laparoscopic management of choledochal cysts: technique and outcomes—a retrospective study of 35...
TRANSCRIPT

LToCRP
CtstnphsTc
DPm2
RFPCg6
©P
aparoscopic Management of Choledochal Cysts:echnique and Outcomes—A Retrospective Studyf 35 Patients from a Tertiary Centerhinnusamy Palanivelu, MCh, FRCS, FACS, Muthukumaran Rangarajan, MS, DipMIS, FACS,amakrishnan Parthasarathi, MBBS, Vennapusa Amar, MS, DNB(GenSurg), MRCS,alanisamy Senthilnathan, MS, DNB(GenSurg), DNB(GISurg), MRCS
BACKGROUND: Choledochal cysts are congenital dilations of the biliary tree. The accepted mode of treatmentis total excision with hepaticojejunostomy. In this retrospective study, we present our techniqueand results of laparoscopic choledochal cyst excision.
STUDY DESIGN: We retrospectively studied 35 patients who had undergone laparoscopic choledochal cyst exci-sion in our institute from 1996 to 2008. Data about age, gender, type of choledochal cyst,symptoms, surgical technique, conversion rate, morbidity, and mortality were analyzed.
RESULTS: There were Type 1B choledochal cysts in 27 patients (77%) and Type IVA in 8 patients (23%).An anomalous pancreatobiliary junction was found in 40%. Mean operative time was 295 min-utes. Total cyst excision could be done in 26 patients. The conversion rate in our series was8.5%. The overall morbidity rate was 14.3%, the reoperation rate was 8.5%, the mortality ratewas 0%, and the incidence of carcinoma was 8.5%.
CONCLUSIONS: To minimize the risk of malignancy, total excision of the cyst is ideal, but a small proximal cuffof cyst is retained for small-size ducts to aid in the hepaticojejunostomy anastomosis. A slit onone end of the small ducts will render the anastomosis in an oblique orientation, widening thelumen. Dissecting the posterior cyst wall from the underlying portal vein is the most crucial partof the procedure. Morbidity and mortality rates after laparoscopic management are comparablewith published results of the open procedure. Laparoscopic surgery for choledochal cysts isfeasible, safe, and even advantageous. (J Am Coll Surg 2008;207:839–846. © 2008 by the
American College of Surgeons)vs1rl
MWl1cbguafa(
holedochal cysts are congenital dilations of the biliaryree that typically affect the pediatric population.1 Thistudy deals with only cysts of the extrahepatic biliary sys-em. Although up to 60% of choledochal cysts are diag-osed in the patient’s first decade, about 20% to 30% ofatients go undiagnosed until adulthood.2 These patientsave a high risk of biliary tract malignancy developing andhould be treated to prevent additional complications.3
he currently accepted mode of treatment for choledochalysts is total excision with hepaticojejunostomy by the con-
isclosure Information: Nothing to disclose.resented at the 10th World Congress of Endoscopic Surgery, Berlin, Ger-any, 2006, and the Teleconferencing Live Surgery to Leeds University, UK,
007.
eceived May 20, 2008; Revised July 22, 2008; Accepted August 4, 2008.rom the Department of GI and Minimal Access Surgery, GEM Hospital &ostgraduate Institute, Ramnathapuram, Coimbatore, India.orrespondence address: Dr Chinnusamy Palanivelu, GEM Hospital & Post-raduate Institute, 45-A, Pankaja Mill Rd, Ramnathapuram, Coimbatore
a41045, India.
8392008 by the American College of Surgeons
ublished by Elsevier Inc.
entional approach. Laparoscopic choledochal cyst exci-ion has been reported in children and adults since the early990s and has been considered safe and feasible.4,5 In thisetrospective study, we present our technique and results ofaparoscopic choledochal cyst excision.
ETHODSe retrospectively studied 35 patients who had undergone
aparoscopic choledochal cyst excision in our institute from996 to 2008. Data about age, gender, type of choledochalyst, symptoms, surgical technique, conversion rate, mor-idity, and mortality were analyzed. The following investi-ations were performed in all patients: liver function tests,ltrasonographic examination, CT scan of the abdomen,nd magnetic resonance cholangiopancreatogram. Twenty-our (68.5%) patients had an anomalous pancreatobili-ry junction. Presenting symptoms were abdominal pain58%), jaundice (29%), cholangitis (19.3%), and pancre-
titis (6.4%). Patients with jaundice, cholangitis, and pan-ISSN 1072-7515/08/$34.00doi:10.1016/j.jamcollsurg.2008.08.004

cwpidnaa
OUscpAciT5stqrtc
DTotets
oiwvpca(etnpwaofcaaacbawsudnssat
Fc
Fs
840 Palanivelu et al Laparoscopic Excision of Choledochal Cysts J Am Coll Surg
reatitis were assessed carefully, and coagulation parametersere normalized if they were altered. A laparoscopic ap-roach was proposed for all patients after obtaining annformed consent. We considered malignancy a contrain-ication for laparoscopy. Prophylactic antibiotics (combi-ation of a third generation cephalosporin with nitroimid-zole) were administered immediately before induction ofnesthesia and continued postoperatively for 5 to 7 days.
perative techniquender general anesthesia, the patient was placed in the
upine position, and pneumoperitoneum was created by alosed Veress needle technique through the umbilicus. Theort position and team set-up were identical to the Northmerican position for laparoscopic cholecystectomy ex-ept an extra 5-mm port for duodenal retraction was placedn the left lumbar area, along the left midclavicular line.he left lobe of the liver was retracted cranially with a-mm grasper holding the gallbladder fundus. A generalurvey of the abdomen was performed to assess the status ofhe liver and to look for signs of portal hypertension. Ade-uate exposure of the working area was achieved by cranialetraction of the gallbladder and caudal traction of theransverse colon and duodenum. The gallbladder was de-ompressed in case of gross distention.
issection of the cysthe peritoneum over the cyst just superior to the first partf the duodenum was incised and continued laterally up tohe inferior vena cava. The inferior part of the cyst was thenxposed by dissecting the superior and posterior parts ofhe first part of the duodenum off the cyst using ultrasonic
igure 1. By dissecting the duodenum (D) off from the choledochalyst (arrow), the lower limit is exposed. GB, gallbladder.
hears (Fig. 1). A careful inspection was done for indicators m
f malignancy, such as papillary projections, and vascularnvolvement using laparoscopic ultrasonography. If thereas any suspicion of malignancy, the procedure was con-erted to a laparotomy. The cyst was then decompressed byercutaneous aspiration and the bile sent for culture. In thease of a large cyst, a transverse incision was made on thenterior wall and the debris and sludge were evacuatedFig. 2). The transverse incision over the anterior wall wasnlarged toward the left to dissect the medial cyst wall fromhe right hepatic artery. Blunt dissection with a suctionozzle was useful for this step of the operation. The nextart of the dissection was separation of the posterior cystall from the portal vein. In our technique, this was
chieved by posteriorly extending the transverse incisionn the medial cyst wall. The portal vein was then separatedrom the entire length of the cyst. The posterior wall of theyst was retracted with a grasper from the epigastric port toid in this part of the dissection. In patients with recurrentttacks of cholangitis, injury to the portal vein is possible ifttempts are made to remove the entire posterior wall of theyst. An arbitrary submucosal dissection plane was createdy injecting saline, and this plane was carefully extended bycombination of blunt and sharp dissection. Dissectionas then extended cranially up to the level of the normal-
ized hepatic ducts, and the cyst was excised in toto. Thissually required clipping of the cystic duct junction. Theistal bile duct was divided at the level where it was oformal caliber, and it was sutured with 4.0 Vicryl (Ethicon)utures (Fig. 3). An attempt was always made to demon-trate the junction of the choledochal cyst and the pancre-tic duct in cases of anomalous pancreatic duct biliary junc-ion. In patients with smaller cysts, the entire cyst was
igure 2. Anterior cyst wall is opened and stones and debris areucked out.
obilized circumferentially without decompression. In pa-
twh
RTndth3util
HTfefciwdimadmt
Rota
ROmya(aap
F(
Fe(b
841Vol. 207, No. 6, December 2008 Palanivelu et al Laparoscopic Excision of Choledochal Cysts
ients with IVA type cysts, the proximal line of resectionas extended up to the confluence of the right and leftepatic ducts.
oux-en-Y loop creationhe duodenojejunal flexure was identified and the jeju-um, at the level of the first good vascular arcade, wasivided with an Endo-GIA linear cutter. At least 40 cm ofhe long limb was used for anastomosis with the proximalepatic duct. The jejunojejunostomy was established at the0-cm level by a side-to-side intracorporeal anastomosissing endostaplers. The Roux loop was constructed en-irely intracorporeally and brought up for the anastomosisn a retrocolic fashion, so that the long limb lay close to theateral abdominal wall.
epaticojejunostomyhe hepaticojejunostomy was performed in an end-to-side
ashion by intracorporeal suturing (Fig. 4). During ourarly experience (11 patients), the anastomosis was per-ormed in a single layer using continuous 4.0 Vicryl (Ethi-on) sutures if the common hepatic duct size was � 1.5 cm;nterrupted sutures were used if ducts were � 1.5 cm. Nowe use interrupted sutures in all patients, regardless of theuct size. For small ducts (� 1.5 cm) only, a cuff of prox-
mal cyst was retained to aid in anastomosis. Also, a slit wasade on one side of the duct so that the anastomosis lay in
n oblique orientation, providing a wide lumen. An 18-Fecompression tube was placed at the level of the anasto-osis. The end of the decompression tube was brought out
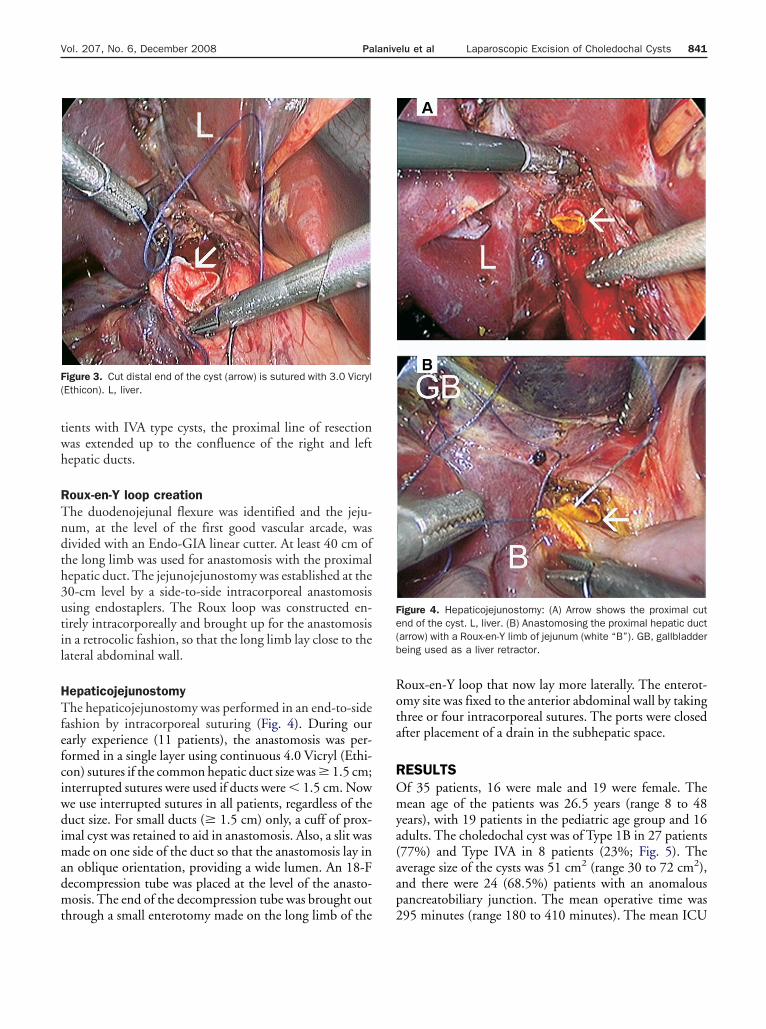
igure 3. Cut distal end of the cyst (arrow) is sutured with 3.0 VicrylEthicon). L, liver.
hrough a small enterotomy made on the long limb of the 2
oux-en-Y loop that now lay more laterally. The enterot-my site was fixed to the anterior abdominal wall by takinghree or four intracorporeal sutures. The ports were closedfter placement of a drain in the subhepatic space.
ESULTSf 35 patients, 16 were male and 19 were female. Theean age of the patients was 26.5 years (range 8 to 48
ears), with 19 patients in the pediatric age group and 16dults. The choledochal cyst was of Type 1B in 27 patients77%) and Type IVA in 8 patients (23%; Fig. 5). Theverage size of the cysts was 51 cm2 (range 30 to 72 cm2),nd there were 24 (68.5%) patients with an anomalousancreatobiliary junction. The mean operative time was
igure 4. Hepaticojejunostomy: (A) Arrow shows the proximal cutnd of the cyst. L, liver. (B) Anastomosing the proximal hepatic ductarrow) with a Roux-en-Y limb of jejunum (white “B”). GB, gallbladdereing used as a liver retractor.
95 minutes (range 180 to 410 minutes). The mean ICU
stodp6poaaot(tpco
ectt
ahpe2dodtawoja
TonaodanncpfcpwthF
j
842 Palanivelu et al Laparoscopic Excision of Choledochal Cysts J Am Coll Surg
tay for these patients was 1.3 days. Patients were allowed toake liquids on the second postoperative day, after passagef flatus. The mean hospital stay was 6.5 days (range 4 to 9ays). Followup was planned by performing ultrasonogra-hy and liver function tests after 4 weeks and everymonths thereafter for 2 years. In four patients (Fig. 6), theosterior wall of the cyst was so adherent because of previ-us episodes of cholangitis that Lilly’s technique wasdopted. In one patient, Lilly’s technique was ineffectivend a cuff of posterior cyst wall was retained, so fulgurationf the retained mucosa was done using bipolar electrocau-ery. It was possible to excise the entire cyst in 28 patients80%). In two patients, the cyst extended caudally behindhe duodenum, so the duodenum along with the head ofancreas had to be mobilized to visualize the lower limit ofyst. The cyst extended proximally beyond the confluencef the hepatic ducts in five patients, but we limited our
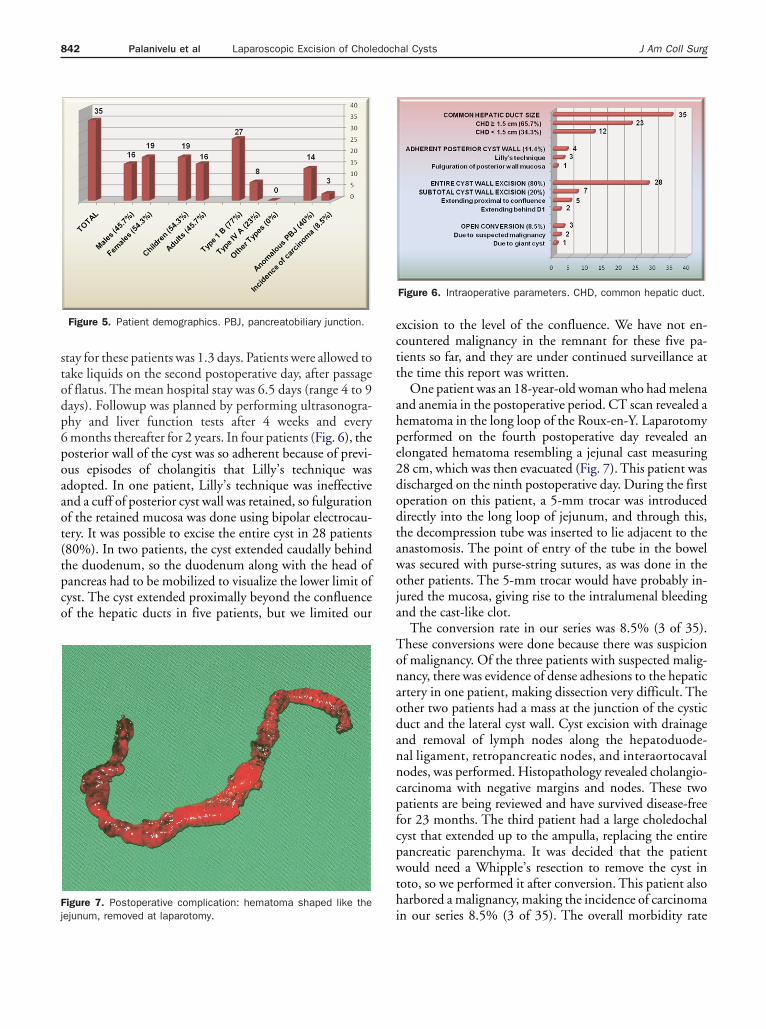
igure 7. Postoperative complication: hematoma shaped like the
Figure 5. Patient demographics. PBJ, pancreatobiliary junction.
iejunum, removed at laparotomy.
xcision to the level of the confluence. We have not en-ountered malignancy in the remnant for these five pa-ients so far, and they are under continued surveillance athe time this report was written.
One patient was an 18-year-old woman who had melenand anemia in the postoperative period. CT scan revealed aematoma in the long loop of the Roux-en-Y. Laparotomyerformed on the fourth postoperative day revealed anlongated hematoma resembling a jejunal cast measuring8 cm, which was then evacuated (Fig. 7). This patient wasischarged on the ninth postoperative day. During the firstperation on this patient, a 5-mm trocar was introducedirectly into the long loop of jejunum, and through this,he decompression tube was inserted to lie adjacent to thenastomosis. The point of entry of the tube in the bowelas secured with purse-string sutures, as was done in thether patients. The 5-mm trocar would have probably in-ured the mucosa, giving rise to the intralumenal bleedingnd the cast-like clot.
The conversion rate in our series was 8.5% (3 of 35).hese conversions were done because there was suspicionf malignancy. Of the three patients with suspected malig-ancy, there was evidence of dense adhesions to the hepaticrtery in one patient, making dissection very difficult. Thether two patients had a mass at the junction of the cysticuct and the lateral cyst wall. Cyst excision with drainagend removal of lymph nodes along the hepatoduode-al ligament, retropancreatic nodes, and interaortocavalodes, was performed. Histopathology revealed cholangio-arcinoma with negative margins and nodes. These twoatients are being reviewed and have survived disease-freeor 23 months. The third patient had a large choledochalyst that extended up to the ampulla, replacing the entireancreatic parenchyma. It was decided that the patientould need a Whipple’s resection to remove the cyst in
oto, so we performed it after conversion. This patient alsoarbored a malignancy, making the incidence of carcinoma
Figure 6. Intraoperative parameters. CHD, common hepatic duct.
n our series 8.5% (3 of 35). The overall morbidity rate
(rpvl1latpmtrmptOjcstwp
DCpCdtpccteRad
icpbsaeam3mu
tfhCpmotctprmrtftlbsptloadtp
elsediyh
843Vol. 207, No. 6, December 2008 Palanivelu et al Laparoscopic Excision of Choledochal Cysts
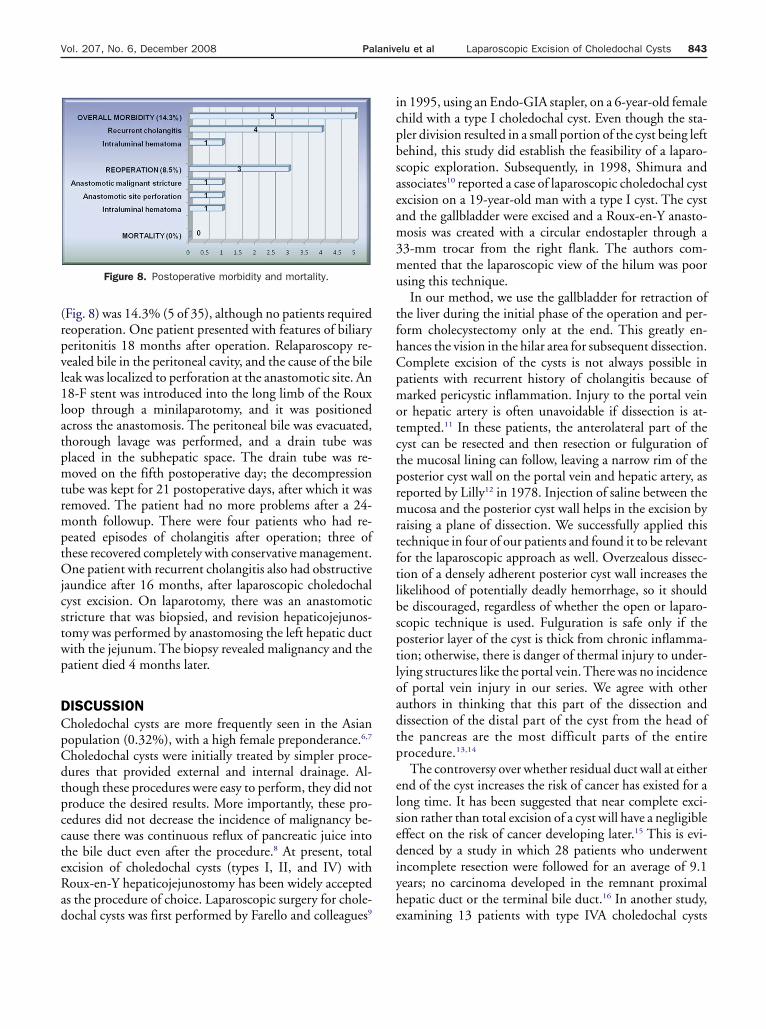
Fig. 8) was 14.3% (5 of 35), although no patients requiredeoperation. One patient presented with features of biliaryeritonitis 18 months after operation. Relaparoscopy re-ealed bile in the peritoneal cavity, and the cause of the bileeak was localized to perforation at the anastomotic site. An8-F stent was introduced into the long limb of the Roux
oop through a minilaparotomy, and it was positionedcross the anastomosis. The peritoneal bile was evacuated,horough lavage was performed, and a drain tube waslaced in the subhepatic space. The drain tube was re-oved on the fifth postoperative day; the decompression
ube was kept for 21 postoperative days, after which it wasemoved. The patient had no more problems after a 24-onth followup. There were four patients who had re-
eated episodes of cholangitis after operation; three ofhese recovered completely with conservative management.ne patient with recurrent cholangitis also had obstructive
aundice after 16 months, after laparoscopic choledochalyst excision. On laparotomy, there was an anastomotictricture that was biopsied, and revision hepaticojejunos-omy was performed by anastomosing the left hepatic ductith the jejunum. The biopsy revealed malignancy and theatient died 4 months later.
ISCUSSIONholedochal cysts are more frequently seen in the Asianopulation (0.32%), with a high female preponderance.6,7
holedochal cysts were initially treated by simpler proce-ures that provided external and internal drainage. Al-hough these procedures were easy to perform, they did notroduce the desired results. More importantly, these pro-edures did not decrease the incidence of malignancy be-ause there was continuous reflux of pancreatic juice intohe bile duct even after the procedure.8 At present, totalxcision of choledochal cysts (types I, II, and IV) withoux-en-Y hepaticojejunostomy has been widely accepteds the procedure of choice. Laparoscopic surgery for chole-
Figure 8. Postoperative morbidity and mortality.
ochal cysts was first performed by Farello and colleagues9 e
n 1995, using an Endo-GIA stapler, on a 6-year-old femalehild with a type I choledochal cyst. Even though the sta-ler division resulted in a small portion of the cyst being leftehind, this study did establish the feasibility of a laparo-copic exploration. Subsequently, in 1998, Shimura andssociates10 reported a case of laparoscopic choledochal cystxcision on a 19-year-old man with a type I cyst. The cystnd the gallbladder were excised and a Roux-en-Y anasto-osis was created with a circular endostapler through a
3-mm trocar from the right flank. The authors com-ented that the laparoscopic view of the hilum was poor
sing this technique.In our method, we use the gallbladder for retraction of
he liver during the initial phase of the operation and per-orm cholecystectomy only at the end. This greatly en-ances the vision in the hilar area for subsequent dissection.omplete excision of the cysts is not always possible inatients with recurrent history of cholangitis because ofarked pericystic inflammation. Injury to the portal vein
r hepatic artery is often unavoidable if dissection is at-empted.11 In these patients, the anterolateral part of theyst can be resected and then resection or fulguration ofhe mucosal lining can follow, leaving a narrow rim of theosterior cyst wall on the portal vein and hepatic artery, aseported by Lilly12 in 1978. Injection of saline between theucosa and the posterior cyst wall helps in the excision by
aising a plane of dissection. We successfully applied thisechnique in four of our patients and found it to be relevantor the laparoscopic approach as well. Overzealous dissec-ion of a densely adherent posterior cyst wall increases theikelihood of potentially deadly hemorrhage, so it shoulde discouraged, regardless of whether the open or laparo-copic technique is used. Fulguration is safe only if theosterior layer of the cyst is thick from chronic inflamma-ion; otherwise, there is danger of thermal injury to under-ying structures like the portal vein. There was no incidencef portal vein injury in our series. We agree with otheruthors in thinking that this part of the dissection andissection of the distal part of the cyst from the head ofhe pancreas are the most difficult parts of the entirerocedure.13,14
The controversy over whether residual duct wall at eithernd of the cyst increases the risk of cancer has existed for aong time. It has been suggested that near complete exci-ion rather than total excision of a cyst will have a negligibleffect on the risk of cancer developing later.15 This is evi-enced by a study in which 28 patients who underwent
ncomplete resection were followed for an average of 9.1ears; no carcinoma developed in the remnant proximalepatic duct or the terminal bile duct.16 In another study,
xamining 13 patients with type IVA choledochal cysts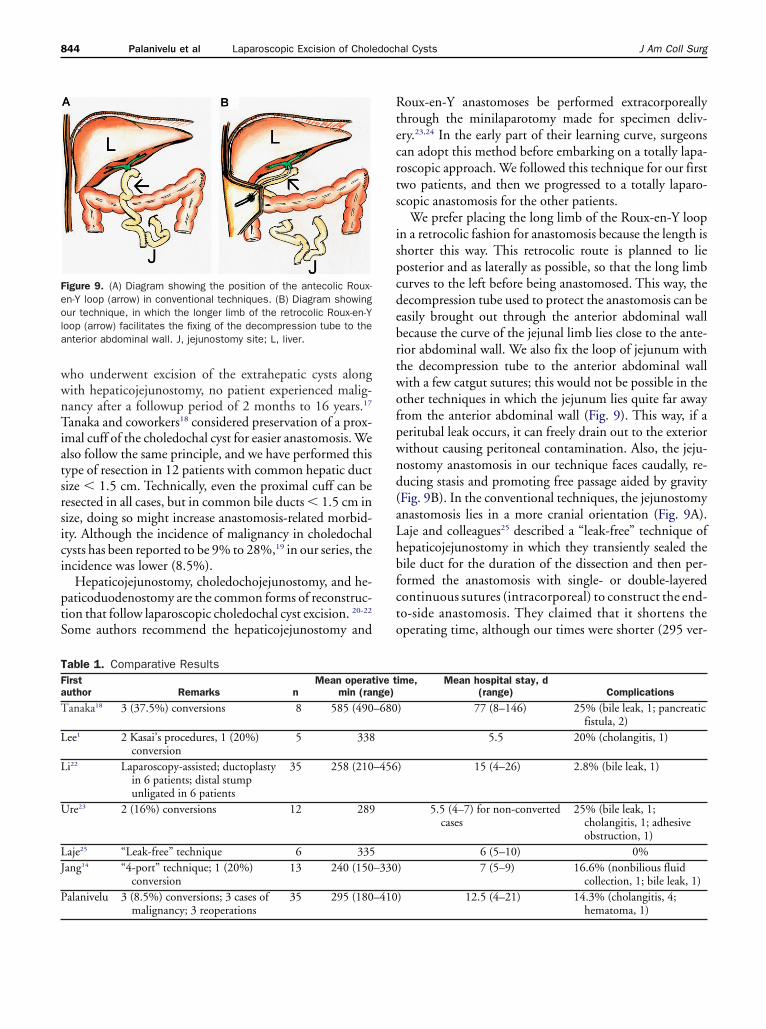
wwnTiatsrsici
ptS
Rtecrts
ispcdebrtwofpwnd(aLhbfcto
Feola
TFa
T
L
L
U
LJ
P
844 Palanivelu et al Laparoscopic Excision of Choledochal Cysts J Am Coll Surg
ho underwent excision of the extrahepatic cysts alongith hepaticojejunostomy, no patient experienced malig-ancy after a followup period of 2 months to 16 years.17
anaka and coworkers18 considered preservation of a prox-mal cuff of the choledochal cyst for easier anastomosis. Welso follow the same principle, and we have performed thisype of resection in 12 patients with common hepatic ductize � 1.5 cm. Technically, even the proximal cuff can beesected in all cases, but in common bile ducts � 1.5 cm inize, doing so might increase anastomosis-related morbid-ty. Although the incidence of malignancy in choledochalysts has been reported to be 9% to 28%,19 in our series, thencidence was lower (8.5%).
Hepaticojejunostomy, choledochojejunostomy, and he-aticoduodenostomy are the common forms of reconstruc-ion that follow laparoscopic choledochal cyst excision. 20-22
ome authors recommend the hepaticojejunostomy and
igure 9. (A) Diagram showing the position of the antecolic Roux-n-Y loop (arrow) in conventional techniques. (B) Diagram showingur technique, in which the longer limb of the retrocolic Roux-en-Y
oop (arrow) facilitates the fixing of the decompression tube to thenterior abdominal wall. J, jejunostomy site; L, liver.
able 1. Comparative Resultsirstuthor Remarks n
Mean operatmin (ra
anaka18 3 (37.5%) conversions 8 585 (490
ee1 2 Kasai’s procedures, 1 (20%)conversion
5 338
i22 Laparoscopy-assisted; ductoplastyin 6 patients; distal stumpunligated in 6 patients
35 258 (210
re23 2 (16%) conversions 12 289
aje25 “Leak-free” technique 6 335ang14 “4-port” technique; 1 (20%)
conversion13 240 (150
alanivelu 3 (8.5%) conversions; 3 cases of 35 295 (180
malignancy; 3 reoperationsoux-en-Y anastomoses be performed extracorporeallyhrough the minilaparotomy made for specimen deliv-ry.23,24 In the early part of their learning curve, surgeonsan adopt this method before embarking on a totally lapa-oscopic approach. We followed this technique for our firstwo patients, and then we progressed to a totally laparo-copic anastomosis for the other patients.
We prefer placing the long limb of the Roux-en-Y loopn a retrocolic fashion for anastomosis because the length ishorter this way. This retrocolic route is planned to lieosterior and as laterally as possible, so that the long limburves to the left before being anastomosed. This way, theecompression tube used to protect the anastomosis can beasily brought out through the anterior abdominal wallecause the curve of the jejunal limb lies close to the ante-ior abdominal wall. We also fix the loop of jejunum withhe decompression tube to the anterior abdominal wallith a few catgut sutures; this would not be possible in thether techniques in which the jejunum lies quite far awayrom the anterior abdominal wall (Fig. 9). This way, if aeritubal leak occurs, it can freely drain out to the exteriorithout causing peritoneal contamination. Also, the jeju-ostomy anastomosis in our technique faces caudally, re-ucing stasis and promoting free passage aided by gravityFig. 9B). In the conventional techniques, the jejunostomynastomosis lies in a more cranial orientation (Fig. 9A).aje and colleagues25 described a “leak-free” technique ofepaticojejunostomy in which they transiently sealed theile duct for the duration of the dissection and then per-ormed the anastomosis with single- or double-layeredontinuous sutures (intracorporeal) to construct the end-o-side anastomosis. They claimed that it shortens theperating time, although our times were shorter (295 ver-
ime, Mean hospital stay, d(range) Complications
) 77 (8–146) 25% (bile leak, 1; pancreaticfistula, 2)
5.5 20% (cholangitis, 1)
) 15 (4–26) 2.8% (bile leak, 1)
5.5 (4–7) for non-convertedcases
25% (bile leak, 1;cholangitis, 1; adhesiveobstruction, 1)
6 (5–10) 0%) 7 (5–9) 16.6% (nonbilious fluid
collection, 1; bile leak, 1)) 12.5 (4–21) 14.3% (cholangitis, 4;
ive tnge)
–680
–456
–330
–410
hematoma, 1)
sw
rtmscr8ecsobtps
cppasamtcotjmiacaflfhactcsip
cin
cgcwlvc
A
SAADC
R
1
1
1
1
1
845Vol. 207, No. 6, December 2008 Palanivelu et al Laparoscopic Excision of Choledochal Cysts
us 335 minutes). The leak rates in their study and oursere both 0%.In the case of large cysts, after ruling out malignancy, we
ecommend opening the cyst on its anterior wall for effec-ive decompression, clearing of debris, visualization of theucosa of the cyst to identify malignancy, and to aid dis-
ection of the posterior wall of the cyst. Small or mediumysts need not be opened before excision. The conversionates in published reports range from 0% to 37%; it was.5% in our series.26,27 We believe that with increasing lev-ls of experience with these operations, the conversion ratesan be minimized. The main deterrent to laparoscopy inuch cases is the prolonged operative time; mean durationf the procedure was 600 minutes in the five cases reportedy Tanaka and associates.18 They had suggested that withechnical refinements, they would be able to complete therocedure within 400 minutes. The operative time in oureries was slightly lower than those in the other reports.
The short-term and longterm morbidity rates of theonventional approaches to choledochal cyst have beenublished in the literature.28 Chen and colleagues29 re-orted a morbidity rate of 20% and a mortality of 3.3% inseries of 60 adult patients who underwent conventional
urgery. The complication rate in our study was 17% with0% mortality rate. Although similar reports on longtermorbidity are sadly lacking in the laparoscopic approach,
he short-term morbidity rates that have been publishedlearly show that the results are superior to those of thepen procedures.30 Anastomotic leak rates range from 0%o 20%, as reported in a large study.31 We had a hepaticoje-unal anastomotic leak rate of 0%. These comparisons of
orbidity, mortality, and leak rates show that laparoscopys comparable with the open technique. One of the majordvantages of the laparoscopic approach in choledochalyst surgery is the superior visualization of the structuresround the cyst and hepatic hilum. The magnification con-erred by the laparoscope helps in assessment of neovascu-arity around the cyst, separation of the posterior cyst wallrom the portal vein, and dissection and anastomosis in theilar area. Shimura and coworkers10 found that dissectionnd identification of the narrow intrapancreatic bile ductlose to the anomalous pancreatobiliary junction was rela-ively easy with the magnified laparoscopic view whenompared with the conventional view. The results of ourtudy compare favorably with those from other major stud-es on the laparoscopic management of choledochal cystsublished so far (Table 1).In conclusion, laparoscopic excision of choledochal
ysts, although technically challenging, is safe and feasiblen experienced hands. It requires a greater degree of tech-
ical skill and dexterity, with adequate experience both inomplex biliary operations and advanced laparoscopic sur-ery. These procedures can be performed according to theurrently accepted standards of the conventional approachith minimum conversion and acceptable morbidity. The
aparoscopic approach has the potential to replace the con-entional approach in the near future as the standard ofare.
uthor Contributions
tudy conception and design: Senthilnathancquisition of data: Amarnalysis and interpretation of data: Parthasarathirafting of manuscript: Rangarajanritical revision: Palanivelu
EFERENCES
1. Lee H, Hirose S, Bratton B, Farmer D. Initial experience withcomplex laparoscopic biliary surgery in children: biliary atresiaand choledochal cyst. J Pediatr Surg 2004;39:804–807.
2. Soreide K, Korner H, Havnen J, Soreide JA. Bile duct cysts inadults. Br J Surg 2004;91:1538–1548.
3. de Vries JS, de Vries S, Aronson DC, et al. Choledochal cysts:age of presentation, symptoms, and late complications re-lated to Todani’s classification. J Pediatr Surg 2002;37:1568–1573.
4. Chowbey PK, Katrak MP, Sharma A, et al. Complete laparo-scopic management of choledochal cyst: report of two cases.J Laparoendosc Adv Surg Tech A 2002;12:217–221.
5. Le DM, Woo RK, Sylvester K, et al. Laparoscopic resection oftype 1 choledochal cysts in pediatric patients. Surg Endosc2006;20:249–251.
6. Tao KS, Lu YG, Wang T, Dou KF. Procedures for congenitalcholedochal cysts and curative effect analysis in adults. Hepato-biliary Pancreat Dis Int 2002;1:442–445.
7. Visser BC, Suh I, Way LW, Kang SM. Congenital choledochalcysts in adults. Arch Surg 2004;139:855–860.
8. Franko J, Nussbaum ML, Morris JB. Choledochal cyst cholan-giocarcinoma arising from adenoma: case report and a review ofthe literature. Curr Surg 2006;63:281–284.
9. Farello GA, Cerofolini A, Rebonato M, et al. Congenital chole-dochal cyst: video-guided laparoscopic treatment. Surg LaparoscEndosc 1995;5:354–358.
0. Shimura H, Tanaka M, Shimizu S, Mizumoto K. Laparoscopictreatment of congenital choledochal cyst. Surg Endosc 1998;12:1268–1271.
1. Martinez-Ferro M, Esteves E, Laje P. Laparoscopic treatment ofbiliary atresia and choledochal cyst. Semin Pediatr Surg 2005;14:206–215.
2. Lilly JR. Total excision of choledochal cyst. Surg Gynecol Obstet1978;146:254–256.
3. Tan HL, Shankar KR, Ford WD. Laparoscopic resection of typeI choledochal cyst. Surg Endosc 2003;17:1495.
4. Jang JY, Kim SW, Han HS, et al. Totally laparoscopic manage-ment of choledochal cysts using a four-hole method. Surg En-
dosc 2006;20:1762–1765.
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
846 Palanivelu et al Laparoscopic Excision of Choledochal Cysts J Am Coll Surg
5. Jordan PH Jr, Goss JA Jr, Rosenberg WR, Woods KL. Someconsiderations for management of choledochal cysts. Am J Surg2004;187:790–795.
6. Ishibashi T, Kasahara K, Yasuda Y, et al. Malignant change in thebiliary tract after excision of choledochal cyst. Br J Surg 1997;84:1687–1691.
7. Chijiiwa K, Komura M, Kameoka N. Postoperative follow-up ofpatients with type IVA choledochal cysts after excision of extra-hepatic cyst. J Am Coll Surg 1994;179:641–645.
8. Tanaka M, Shimizu S, Mizumoto K, et al. Laparoscopicallyassisted resection of choledochal cyst and Roux-en-Y reconstruc-tion. Surg Endosc 2001;15:545–552.
9. Ikoma A, Tanaka K, Koyanagi H, et al. Long-term survival withcarcinoma arising from a congenital choledochal cyst. J Hepato-Biliary-Pancreat Surg 1996;3:74–77.
0. Watanabe Y, Sato M, Tokui K, et al. Laparoscope-assisted min-imally invasive treatment for choledochal cyst. J LaparoendoscAdv Surg Tech A 1999;9:415–418.
1. Vila-Carbó JJ, Lluna González J, Hernández Anselmi E, et al.Congenital choledochal cyst and laparoscopic techniques. CirPediatr 2007;20:129–132.
2. Li L, Feng W, Jing-Bo F, et al. Laparoscopic-assisted total cystexcision of choledochal cyst and Roux-en-Y hepatoenterostomy.J Pediatr Surg 2004;39:1663–1666.
3. Ure BM, Nustede R, Becker H. Laparoscopic resection of
congenital choledochal cyst, hepaticojejunostomy, and exter-nally made Roux-en-Y anastomosis. J Pediatr Surg 2005;40:728–730.
4. Ure BM, Schier F, Schmidt AI, et al. Laparoscopic resection ofcongenital choledochal cyst, choledochojejunostomy, and extra-abdominal Roux-en-Y anastomosis. Surg Endosc 2005;19:1055–1057.
5. Laje P, Questa H, Bailez M. Laparoscopic leak-free technique forthe treatment of choledochal cysts. J Laparoendosc Adv SurgTech A 2007;17:519–521.
6. Aspelund G, Ling SC, Ng V, Kim PC. A role for laparoscopicapproach in the treatment of biliary atresia and choledochalcysts. J Pediatr Surg 2007;42:869–872.
7. Liu DC, Rodriguez JA, Meric F, Geiger JL. Laparoscopic exci-sion of a rare type II choledochal cyst: case report and review ofthe literature. J Pediatr Surg 2000;35:1117–1119.
8. Bulte C, Klaase J, Russel M, Somsen J. Choledochal cyst in anadult. J Am Coll Surg 2007;205:178–179.
9. Chen HM, Jan YY, Chen MF, et al. Surgical treatment of cho-ledochal cyst in adults: results and long-term follow-up. Hepa-togastroenterology 1996;43:1492–1499.
0. Abbas HM, Yassin NA, Ammori BJ. Laparoscopic resection oftype I choledochal cyst in an adult and Roux-en-Y hepaticoje-junostomy: a case report and literature review. Surg LaparoscEndosc Percutan Tech 2006;16:439–444.
1. Srimurthy KR, Ramesh S. Laparoscopic management of pedi-atric choledochal cysts in developing countries: review of ten
cases. Pediatr Surg Int 2006;2:144–149.