lakeshore regional entity managed care … rfp document… · release date: march 15, 2018 . 2 ......
TRANSCRIPT

LAKESHORE REGIONAL ENTITY
Managed Care Administrative Functions Medicaid Managed Specialty Supports and Services
Concurrent 1915(b)(c) Waiver Program
Request for Proposals
Release Date: March 15, 2018

2
Table of Contents I. Definitions ............................................................................................................................................ 4
II. General Information ............................................................................................................................. 8
A. Description of Michigan’s Current Service Delivery and Financing System for Behavioral Health and Services and Supports for Persons with Developmental Disabilities .............................................. 8
1) Medicaid Managed Specialty Supports and Services Waiver Program(s), the Healthy Michigan Program, the Flint 1115 Waiver and Substance Use Disorder Community Grant Programs ............... 8
2) Michigan’s Medicaid Health Plans (MHP) ..................................................................................... 9
B. Evolving Initiatives in Michigan’s Medicaid Service Delivery and Financing System .................. 10
1) Section 298 Pilot(s) – Medicaid Physical-Behavioral Health Full Financial Integration .............. 10
2) Pathway to Integration - Michigan’s 1115 Waiver Proposal for Persons with Severe Mental Illness, Substance Use Disorders, Intellectual and Developmental Disabilities and Children with Severe Emotional Disturbances .......................................................................................................... 11
C. The Lakeshore Regional Entity ....................................................................................................... 11
1) Vision & Values ........................................................................................................................... 12
2) MDHHS Request for Audit and Subsequent recommendations ................................................. 12
D. Purpose of the RFP ......................................................................................................................... 13
1) Select a managed care partner to: .............................................................................................. 13
2) Target Population(s), funds and covered services ...................................................................... 13
E. Term of Contract ............................................................................................................................ 14
F. Minimum Offeror Eligibility Criteria .............................................................................................. 14
G. Resources in Bidder Library ........................................................................................................... 15
H. Schedule of Events ......................................................................................................................... 16
I. Single Point of Contact ................................................................................................................... 16
J. Request for Proposals Guidelines .................................................................................................. 16
K. Proposal Submission and Format .................................................................................................. 17
L. Copies of Proposal Required for Submission ................................................................................ 17
M. Public Disclosure of Proposals ................................................................................................... 18
N. Economy of Presentation ............................................................................................................... 18
III. Information Required from the MBHO/MCO Offeror (Scope of Work) ....................................... 18
A. Cover Letter (Page Limit – 5 Pages) ............................................................................................... 18
B. Information about the offeror (Page Limit – 2 Pages) .................................................................. 19
C. Organizational Structure, Legal Standing, & Litigation History (Page Limit – 1 Page, excluding attachments) .......................................................................................................................................... 19

3
D. Solvency & Financial Integrity (Page Limit – 1 Pages, excluding attachments) ........................... 20
E. Relevant Managed Care Experience (Page Limit – 18 Pages, excluding attachments) ................ 20
F. Offeror’s Proposed Organizational Structure (Page Limit – 6 Pages, excluding attachments) ... 21
G. Distribution of Funds & Risk Corridor Assumption (Page Limit – 5 Pages) .................................. 21
H. Implementation of Administrative Functions ............................................................................... 23
H.1 Member Services (Page Limit – 6 Pages) ...................................................................................... 23
H.2 Provider Network Services (Page Limit – 9 Pages) ....................................................................... 24
H.3 Management Information Services (non-claims related) (Page Limit – 10 Pages, excluding system diagrams and process flow charts) ......................................................................................... 25
H.4 Financial Management System (Page Limit – 8 Pages) ................................................................ 27
H.5 Claims Management System (Page Limit – 7 Pages) .................................................................... 28
H.6 Quality Assurance / Performance Improvement Program (QAPIP) (Page Limit – 7 Pages, excluding attachments) ....................................................................................................................... 29
H.7 Service and Utilization Management (Page Limit – 9 Pages) ....................................................... 30
I. Plan for Overall Transition and Timeline (Page Limit – 10 Pages, excluding attachments) ........ 31
VI. Contractor Performance Measures ............................................................................................... 32
VII. Criteria for Selection ...................................................................................................................... 33
VIII. Pricing Proposal .............................................................................................................................. 34
4
I. Definitions Appropriations Act: The annual appropriations act adopted by the State Legislature that governs MDHHS funding.
Capitated Payments: Monthly payments based on the Capitation Rate that are payable to the PIHP by the MDHHS for the provision of Medicaid services and supports pursuant to Part II (A) Section 8.0 of this contract.
Capitation Rate: The fixed per person monthly rate payable to the PIHP by the MDHHS for each Medicaid eligible person covered by the Concurrent 1915(b)/1915(c) Waiver Program, regardless of whether or not the individual who is eligible for Medicaid receives covered specialty services and supports during the month. There is a separate, fixed per person monthly rate payable for each eligible person covered by the Healthy Michigan Program. The capitated rate does not include funding for beneficiaries enrolled in the Medicaid 1915(c) Children’s Waiver, children enrolled in Michigan's separate health insurance program (MiChild) under Title XXI of the Social Security Act.
Clean Claim: A clean claim is one that can be processed without obtaining additional information from the provider of the service or a third party. It does not include a claim from a provider who is under investigation for fraud or abuse, or a claim under review for medical necessity.
Community Mental Health Services Program (CMHSP): A program operated under Chapter 2 of the Michigan Mental Health Code - Act 258 of 1974 as amended.
Contractor: See PIHP.
Cultural Competency: is an acceptance and respect for difference, a continuing self-assessment regarding culture, a regard for and attention to the dynamics of difference, engagement in ongoing development of cultural knowledge, and resources and flexibility within service models to work toward better meeting the needs of minority populations.
Customer: In this contract, customer includes all Medicaid eligible individuals located in the defined service area who are receiving or may potentially receive covered services and supports. The following terms may be used within this definition: clients, recipients, enrollees, beneficiaries, consumers, individuals, persons served, Medicaid Eligible.
Early and Periodic Screening, Diagnosis, and Treatment Program (EPSDT): EPSDT is Medicaid's comprehensive and preventive child health program for beneficiaries under age 21.
Flint 1115 Demonstration Waiver: The demonstration waiver expands coverage to children up to age 21 years and to pregnant women with incomes up to and including 400 percent of the federal poverty level (FPL) who were served by the Flint water system from April 2014 through a state-specified date. This demonstration is approved in accordance with section 1115(a) of the Social Security Act, and is effective as of March 3, 2016 the date of the signed approval through February 28, 2021. Medicaid-eligible children and pregnant women who were served by the Flint water system during the specified period will be eligible for all services covered under the state plan. All such persons will have access to Targeted Case Management services under a fee for service contract between MHDDS and Genesee Health Systems (GHS). The fee for service contract shall provide the targeted case management services in

5
accordance with the requirements outlined in the Special Terms and Conditions for the Flint Section 1115 Demonstration, the Michigan Medicaid State Plan and Medicaid Policy.
Health Care Professional: A physician or any of the following: podiatrist, optometrist, chiropractor, psychologist, dentist, physician assistant, physical or occupational therapist, therapist assistant, speech-language pathologist, audiologist, registered or practical nurse (including nurse practitioner, clinical nurse specialist, certified registered nurse anesthetist, and certified nurse midwife), registered/certified social worker, registered respiratory therapist, and certified respiratory therapy technician.
Health Insurance Portability and Accountability Act of 1996 (HIPAA): Public Law 104-191, 1996 to improve the Medicare program under Title XVIII of the Social Security Act, the Medicaid program under Title XIX of the Social Security Act, and the efficiency and effectiveness of the health care system, by encouraging the development of a health information system through the establishment of standards and requirements for the electronic transmission of certain health information.
The Act provides for improved portability of health benefits and enables better defense against abuse and fraud, reduces administrative costs by standardizing format of specific healthcare information to facilitate electronic claims, directly addresses confidentiality and security of patient information - electronic and paper. HIPAA was amended by the Health Information Technology for Economic and Clinical Health Act of 2009 (HITECH Act), as set forth in Title XIII of Division A and Title IV of Division B of the American Recovery and Reinvestment Act of 2009. The United States Department of Health and Human Services (DHHS) promulgated administrative rules to implement HIPAA and HITECH, which are found at 45 C.F.R. Part 160 and Subpart E of Part 164 (the “Privacy Rule”), 45 C.F.R. Part 162 (the “Transaction Rule”), 45 C.F.R. Part 160 and Subpart C of Part 164 (the “Security Rule”), 45 C.F.R. Part 160 and Subpart D of Part 164 (the “Breach Notification Rule”) and 45 C.F.R. Part 160, subpart C (the “enforcement Rule”). DHHS also issued guidance pursuant to HITECH and intends to issue additional guidance on various aspects of HIPAA and HITECH compliance. Throughout this contract, the term “HIPAA” includes HITECH and all DHHS implementing regulations and guidance.
Healthy Michigan Plan: The Healthy Michigan Plan is a new category of eligibility authorized under the Patient Protection and Affordable Care Act and Michigan Public Act 107 of 2013 that began April 1, 2014.
Healthy Michigan Plan Beneficiary: An individual who has met the eligibility requirements for enrollment in the Healthy Michigan Plan and has been issued a Medicaid card.
Intellectual/Developmental Disability: As described in Section 330.1100a of the Michigan Mental Health Code.
Internal Service Fund: DHHS established method for securing funds as part of the overall strategy for covering risk exposure under the Medicaid Managed Specialty Supports and Services Concurrent Waiver Programs Contract (Contract). The ISF minimum level is set to assure that the overall level of Prepaid Inpatient Health Plan (PIHP) funds are directed toward consumer services.
Medicaid Abuse: Provider practices that are inconsistent with sound fiscal, business or medical practices and result in an unnecessary cost to the Medicaid program, or in reimbursement for services that are not medically necessary or that fail to meet the professionally recognized standards for health care. 42 CFR 455.2

6
Medicaid Fraud: The intentional deception or misinterpretation made by a person with the knowledge that the deception could result in some unauthorized benefit to himself or another person. 42 CFR 455.2.
Michigan Medicaid Provider Manual-Mental Health/Substance Abuse Chapter: The Michigan Department of Health and Human Services periodically issues notices of proposed policy for the Medicaid program. Once a policy is final, MDHHS issues policy bulletins that explain the new policy and give its effective date. These documents represent official Medicaid policy and are included in the Michigan Medicaid Provider Manual: Mental Health Substance Abuse section.
Per Eligible Per Month (PEPM): A fixed monthly rate per Medicaid eligible person payable to the PIHP by the MDHHS for provision of Medicaid services defined within this contract.
Persons with Limited English Proficiency (LEP): Individuals who cannot speak, write, read or understand the English language at a level that permits them to interact effectively with health care providers and social service agencies.
Post-stabilization Services: Covered specialty services specified in Section 2.0 that are related to an emergency medical condition and that are provided after a beneficiary is stabilized in order to maintain the stabilized condition, or, under the circumstances described in 42 CFR 438.114(e) to improve or resolve the beneficiary's condition.
Practice Guideline: MDHHS-developed guidelines for PIHPs and CMHSPs for specific service, support or systems models of practice that are derived from empirical research and sound theoretical construction and are applied to the implementation of public policy.
Prepaid Inpatient Health Plan (PIHP): In Michigan and for the purposes of this contract, a PIHP is defined as an organization that manages Medicaid specialty services under the state's approved Concurrent 1915(b)/1915(c) Waiver Program, on a prepaid, shared-risk basis, consistent with the requirements of 42 CFR Part 438. (In Medicaid regulations Part 438., Prepaid Health Plans (PHPs) that are responsible for inpatient services as part of a benefit package are now referred to as "PIHP" The PIHP also known as a Regional Entity under MHC 330.1204b or a Community Mental Health Services Program also manages the Autism iSPA, Healthy Michigan, Substance Abuse Treatment and Prevention Community Grant and PA2 funds. "
Regional Entity: An entity established by a combination of community mental health services programs under section 204b of the Michigan Mental Health Code- Act 258 of 1974 as amended.
Sentinel Events: Is an “unexpected occurrence” involving death (not due to the natural course of a health condition) or serious physical or psychological injury or risk thereof. Serious injury specifically includes permanent loss of limb or function. The phrase “or risk thereof” includes any process variation for which recurrence would carry a significant chance of a serious adverse outcome. (JCAHO, 1998) Any injury or death that occurs from the use of any behavior intervention is considered a sentinel event.
Serious Emotional Disturbance: As described in Section 330.1100c of the Michigan Mental
Health Code, a serious emotional disturbance is a diagnosable mental, behavioral, or emotional disorder affecting a minor that exists or has existed during the past year for a period of time sufficient to meet diagnostic criteria specified in the most recent diagnostic and statistical manual of mental disorders
7
published by the American Psychiatric Association and approved by the MDHHS, and that has resulted in functional impairment that substantially interferes with or limits the minor's role or functioning in family, school, or community activities. The following disorders are included only if they occur in conjunction with another diagnosable serious emotional disturbance:
• A substance use disorder • A developmental disorder • A "V" code in the diagnostic and statistical manual of mental disorders
Serious Mental Illness: As described in Section 330.1100c of the Michigan Mental Health Code, a serious mental illness is a diagnosable mental, behavioral, or emotional disorder affecting an adult that exists or has existed within the past year for a period of time sufficient to meet diagnostic criteria specified in the most recent diagnostic and statistical manual of mental disorders published by the American Psychiatric Association and approved by the MDHHS and that has resulted in functional impairment that substantially interferes with or limits one or more major life activities. Serious mental illness includes dementia with delusions, dementia with depressed mood, and dementia with behavioral disturbances, but does not include any other dementia unless the dementia occurs in conjunction with another diagnosable serious mental illness.
Sub-Contractor: A person, business or organization which has a contract with the PIHP to provide some portion of the work or services which the PIHP has agreed to perform within this contract.
Substance Use Disorder (SUD): The taking of alcohol or other drugs as dosages that place an individual’s social, economic, psychological, and physical welfare in potential hazard or to the extent that an individual loses the power of self-control as a result of the use of alcohol or drugs, or while habitually under the influence of alcohol or drugs, endangers public health, morals, safety, or welfare, or a combination thereof.
SUD Community Grant: A combination of the federal grant received by the State from the Substance Abuse and Mental Health Services Administration (SAMHSA) and the general fund dollars appropriated by the legislature for the prevention and treatment of SUD.
Technical Advisory: MDHHS-developed document with recommended parameters for PIHPs regarding administrative practice and derived from public policy and legal requirements.
Technical Requirement: MDHHS/PIHP contractual requirements providing parameters for
PIHPs regarding administrative practice related to specific administrative functions, and that are derived from public policy and legal requirements.
8
II. General Information
A. Description of Michigan’s Current Service Delivery and Financing System for Behavioral Health and Services and Supports for Persons with Developmental Disabilities
1) Medicaid Managed Specialty Supports and Services Waiver Program(s), the Healthy Michigan Program, the Flint 1115 Waiver and Substance Use Disorder Community Grant Programs
Public behavioral health services in Michigan are delivered through county-based Community Mental Health Services Programs (CMHSPs), which are public entities that are created by county governments to provide a comprehensive array of mental health and services and supports to persons with intellectual disabilities to meet local needs, regardless of an individual’s ability to pay. These services are provided either directly or through contracts with community providers. Persons served include children with severe emotional disturbance, adults with serious mental illness, children and adults with intellectual/developmental disabilities and persons with substance use disorders.
Under approval granted by the Centers for Medicare and Medicaid Services (CMS), the Michigan
Department of Health and Human Services (MDHHS) operates a Section 1915(b) Medicaid Managed Specialty Services and Support Program Waiver. Under this waiver, selected Medicaid state plan specialty services related to mental health and developmental disability services, as well as certain covered substance abuse services, have been “carved out” (removed) from Medicaid primary physical health care plans and arrangements. The 1915(b) Specialty Services Waiver Program operates in conjunction with Michigan's existing 1915(c) Habilitation Supports Waiver for persons with developmental disabilities. Such arrangements have been designated as “Concurrent 1915(b)/(c)” Programs by CMS. In addition, CMS has approved an 1115 Demonstration project titled the Healthy Michigan Plan which provides health care coverage for adults who become eligible for Medicaid under section 1902(2) (10) (A)(i)(VIII) of the Social Security Act.
The Concurrent 1915(b)/(c) Programs and the Healthy Michigan Plan are managed on a shared
risk basis by specialty Prepaid Inpatient Health Plans (PIHPs), selected through the Application for Participation (AFP) process. PIHPs may include a single county CMHSP (Macomb, Oakland and Detroit-Wayne) or be a Regional Entity. A Regional Entity is defined as an entity established by a combination of county-based Community Mental Health Services Programs (CMHSPs) under section 204b of the Michigan Mental Health Code, Act 258 of 1974, as amended. The Lakeshore Regional Entity is such an organization.
MDHHS contracts with 10 Prepaid Inpatient Health Plans (PIHP). (This contract can be found in
the RFP Bidder Library.) “The purpose of the MDHHS contract is to obtain the services of the selected PIHP to manage the Concurrent 1915(b)/(c) Programs, the Healthy Michigan Plan and SUD Community Grant Programs, and relevant I Waivers in a designated services area and to provide a comprehensive array of specialty mental health and substance abuse services and supports. The PIHP shall manage its responsibilities in a manner that promotes maximum value, efficiency and effectiveness consistent with state and federal statute and applicable waiver standards. These values include limiting managed care administrative duplication thereby reducing avoidable costs while maximizing the medical loss ratio. The

9
PIHP shall actively manage behavioral health services throughout its service area using standardized methods and measures for determination of need and appropriate delivery of service. The PIHP shall ensure that cost variances in services are supported by quantifiable measures of need to ensure accountability, value and efficiency. The PIHP shall minimize duplication of contracts and reviews for providers contracting with multiple CMHSPs in a region.”1 The PIHPs were required to submit an Application for Participation (AFP) to be selected. That AFP may be found as Attachment P 13.0B in the MDHHS/Lakeshore Regional Entity Contract in the Bidder Library. All requirements of the PIHP in that AFP (and associated other Attachments) apply to the contract and the delegated scope of work of this solicitation.
This solicitation requires that prospective Offerors bear claims risk within the shared risk model
that is defined in the MDHHS/PIHP contract, section 8.6.1.
“The shared risk arrangements shall cover all Medicaid 1915, 1915(b)(3), 1115 Healthy Michigan Plan capitation and 1915(c) Habilitation Supports Waiver payments. The risk corridor is administered across all services, with no separation for mental health and substance abuse funding.
A. The PIHP shall retain unexpended risk-corridor-related funds between 95% and 100% of said funds. The PIHP shall retain 50% of unexpended risk-corridor related funds between 90% and 95% of said funds. The PIHP shall return unexpended risk-corridor-related funds to the MDHHS between 0% and 90% of said funds and 50% of the amount between 90% and 95%. B. The PIHP may retain funds noted in 8.6.1.A, except as specified in Part 1, section 16.0 “Closeout”. C. The PIHP shall be financially responsible for liabilities incurred above the risk corridor related operating budget between 100% and 105% of said funds contracted. D. The PIHP shall be responsible for 50% of the financial liabilities above the risk corridor related operating budget between 105% and 110% of said funds contracted. E. The PIHP shall not be financially responsible for liabilities incurred above the risk corridor-related operating budget over 110% of said funds contracted. The assumption of a shared-risk arrangement between the PIHP and the MDHHS shall not permit the PIHP to overspend its total operating budget for any fiscal year. “
2) Michigan’s Medicaid Health Plans (MHP) Services for individuals with mild to moderate mental illness are covered by Michigan’s
Medicaid Health Plans (MHP) separate from the PIHPs. MHPs have developed a network of private providers to serve the needs of those with mild to moderate behavioral health problems. Mild to moderate behavioral health services are a benefit that is provided as part of the contracting process for Medicaid health services, including physical health services, by MDHHS. Some of the CMHSPs provide this services under contract with the MHPs and all are required to have coordination agreements with
1 MI Medicaid Specialty Supports and Services Concurrent 1915(b)(c) Waiver Program 2018 Contract – p14

10
health plans in their area. A model coordination agreement may be found as Attachment P 7.3.1 in the MDHHS/Lakeshore Regional Entity Contract in the Bidder Library.
B. Evolving Initiatives in Michigan’s Medicaid Service Delivery and Financing System 1) Section 298 Pilot(s) – Medicaid Physical-Behavioral Health Full Financial Integration Section 298 of Public Act 107 of 2017 instructs the Michigan Department of Health and Human
Services (MDHHS) to “…implement up to 3 pilot projects to achieve fully financially integrated Medicaid behavioral health and physical health benefit and financial integration demonstration models. These demonstration models shall use single contracts between the state and each licensed Medicaid Health Plan (MHP) that is currently contracted to provide Medicaid services in the geographic area of the pilot project.” This legislation also explicitly states that: “The department shall work with a willing CMHSP in Kent County and all willing Medicaid health plans in the county to pilot a full physical and behavioral health integrated service demonstration model.”
On December 20, 2017, MDHHS released Request for Information No. 1800000000003. This RFI
as amended may be found in Bidder Library. This RFI has the potential to impact this current Lakeshore Request for Proposals due to the following considerations:
• The Kent County CMHSP, one of the Lakeshore Regional Entity’s members, is designated as developing an integrated service demonstration program.
• Only CMHSPs may be offerors, not PIHPs. Therefore, any of the other LRE members may submit a proposal for a full financial integration pilot.
• HealthWest and West Michigan CMHSPs have submitted pilot proposals. • If a CMHSP is selected for the full financial integration pilot, all Medicaid PMPM funding for
members enrolled with the MHP will flow to the MHP and away from the LRE. • In addition, for those Medicaid members in the CMHSPs geographic area who are not
enrolled with a MHP (e.g., dual eligible Medicaid/Medicare, nursing facility residents, PACE enrollees, newly eligible pending assignment/choice enrollment and spend-down eligible) will have their specialty behavioral health services and supports managed by a still to be determined method. “MDHHS is currently analyzing multiple options for the management of specialty behavioral health benefits for this population during the pilot(s).”2 It is unknown if the option selected by MDHHS will be announced before proposals to this solicitation will be due.
Responses to the RFI were due February 20, 2018 and the awards were made on March 9, 2018. Two of the 5 CMHSPs (HealthWest and Western Michigan CMH) within the LRE region received awards and therefore will be pulled from the scope of this contract. Since the exact impact of that process is uncertain at this time, the utilization data provided in the Bidder Library has been delineated by CMHSP for use by the offeror. The State provides notice regarding updates to the 298 Initiative at the following web address:
http://www.michigan.gov/mdhhs/0,5885,7-339-71550_2941_76181---,00.html
2 Michigan Department of Health and Human Services, Request for Information (RFI) No. [RFI-180000000003] 298 Pilot(s) – Medicaid Physical-Behavioral Health Full Financial Integration, February 2018

11
2) Pathway to Integration - Michigan’s 1115 Waiver Proposal for Persons with Severe Mental Illness, Substance Use Disorders, Intellectual and Developmental Disabilities and Children with Severe Emotional Disturbances
MDHHS has a pending 1115 waiver request resting with the Centers for Medicare and Medicaid Services (CMS). (See the Bidder Library for a copy of the waiver application.) The request to CMS is to “... combine under a single waiver authority all services and eligible populations served through its 1915(b), 1915(i) and its multiple 1915(c) waivers. Under this broad consolidated waiver authority, Michigan is seeking broad flexibility to develop quality, financing and integrated care (physical and behavioral health care) initiatives for all Specialty Service populations on a statewide basis.”
The waiver request does not change eligibility requirements for any of the waiver programs, so membership is not anticipated to be impacted. However, the result of possible CMS Terms and Conditions or other factors may require some changes in the MDHHS contract upon which this RFP’s scope of work is based. Depending upon the timing of the waiver approval, any known changes to this RFP’s scope of work would be transmitted to all prospective Offerors who returned a mandatory Letter of Intent. The State provides notice regarding updates to the Pathway to Integration 1115 Waiver at the following web address:
http://www.michigan.gov/mdhhs/0,5885,7-339-71550_2941_4868-387341--,00.html
C. The Lakeshore Regional Entity Lakeshore Regional Entity (LRE) is the PIHP created in the Western Region (MDHHS Region 3) to
manage specialty carved out Medicaid mental health, developmental disability, and substance use disorder services for Medicaid and Healthy Michigan enrollees in Lake, Mason, Oceana, Muskegon, Ottawa, Kent, and Allegan counties (i.e., the Western Region). The LRE has five diverse CMHSPs members, including Allegan County Community Mental Health, HealthWest (formerly Muskegon County Community Mental Health), Kent County Mental Health Authority d/b/a Network180, Ottawa Community Mental Health, and West Michigan Community Mental Health.
Currently each CMHSP member appoints one person from their respective board to serve on the Executive Committee of the Lakeshore Regional Entity Board of Directors. The Executive Committee then selects 10 at-large Board members as recommended by the Member boards. Distribution of the at-large positions is based upon the size of the population size of the member CMHSP counties. An Operations Committee serves in an advisory capacity to the LRE Board of Directors and the Chief Executive Officer. The Operations Committee consists of the Chief Executive Officers/Executive Directors of the Members and the Chief Executive Officer of the Entity. Other staff from the Members or the Entity may attend as requested by the Board of Directors or the Entity Chief Executive Officer in a support capacity. The LRE is considering further potential modifications to its governance structure. Initially the selected Offeror will be a subcontractor to the PIHP, but the PIHP may explore a new “partnership” in which the managed care entity partners with the public PIHP board through a negotiated redesign of our governance model and a risk sharing agreement as permissible under Michigan law and the MDHHS contract.
To understand the relationships between the LRE and its member CMHSPs, please see the
following documents which are provided in the Bidder Library LRE Bylaws, LRE Operating Agreement – 8-2017 and LRE Common Contract.
12
The LRE had 262,356 covered lives in the Program as of December 2017. For additional information on the last two fiscal years of membership, utilization and administrative expenditures in the following resources in the Bidder’s Library: CMHSP/PIHP Administrative Cost Report (FY 2016 & 2017); the Medicaid Unit Net Cost Report (FY 2016 & 2017); the LRE Funding by Year Report (FY 2016 & 2017); Membership Count by Service Group; and the Count by Service Unit Report.
1) Vision & Values The Vision of the Lakeshore Regional Entity is to promote the efficiency and effectiveness of the
Members by jointly serving as the PIHP for Medicaid Specialty Behavioral Health Services for the region. Behavioral Health Services include services for persons with developmental disabilities, adults with mental illness, children with emotional disturbance and persons with substance use disorders. The Lakeshore Regional Entity seeks to build upon and maximize the unique strengths of the individual Member Boards serving Allegan, Kent, Lake, Mason, Muskegon, Oceana and Ottawa Counties, while establishing a regional organization and identity that supports an essential standard for services. The Lakeshore Regional Entity will promote performance that supports and advocates for and is informed by the needs of the individuals the Entity serves across the region.
Our Values include:
Public Dollars Responsibility for the appropriate use of public dollars and accountability to the Members for the use of those dollars
Successes Accountability for the successes and/or failures of the Entity Mental Health System Commitment to trust, honesty, openness, and commitment
concerning the public mental health system in Michigan with the understanding that respect and transparency informs relationships and our dealings with and amongst Members
Communities/Members Commitment to keeping the promises made to Region 3 communities and the promises made to Members
Persons Served Commitment to ensuring that the voice of Persons Served, families and the supporters of Persons Served is heard, honored, and reflected in the work of Lakeshore Regional Partners in a meaningful and substantive manner
Person-Centered Commitment to a person-centered, family centered approach, with emphasis upon self-determination, the rights of the persons served and the opportunity to engage in community living that has meaning and value for the person
Growth Commitment to resolving conflicts that may arise as part of the Entity’s growth
Integrity Commitment to achieving performance, ethically, effectively and professionally, in accordance with the Partner's Conflict of Interest Policy
2) MDHHS Request for Audit and Subsequent recommendations (See the following resources in the Bidder Library – MDHHS Letter to LRE, Program Audit Lakeshore Regional Entity PIHP, and Most recent CAP Report to MDHHS)
13
In July 2015, the LRE notified the State that it estimated overspending by $13.9 million for fiscal year 2014– 15. In addition, MDHHS was potentially concerned regarding the lack of centralization and consistency of the managed care functions within the Region. Since some managed care functions were delegated to the LRE’s member CMHSPs potential duplication of and variation in processes and services across the CMHSPs, had a potential negative effect on the experience of consumers, family members and providers. MDHHS retained an independent managed behavioral health organization (Beacon Health Options) to conduct a program audit.
The result of the program audit, its recommendations and the LRE’s most recent Corrective
Action Plan Status Report may be found in Bidder Library.
D. Purpose of the RFP 1) Select a managed care partner to:
a. Consolidate and provide managed care administrative services functions as delineated below consistent with the requirements in the MDHHS/Lake Shore Contract
b. Provide Risk Protection for the LRE within the contractual risk corridor (7.5%) while maintaining a medical loss ratio of 85%.
c. Accelerate the compliance with the LRE’s Corrective Action Plan with MDHHS. d. Provide Technical Assistance/Training/Consultation as necessary to the LRE and its
member Community Mental Health Services Programs
2) Target Population(s), funds and covered services a. Target Population: all Medicaid beneficiaries in the LRE Service Area who are eligible
and/or enrolled for specialty supports and services under i. 1915(b) Specialty Services Waiver
ii. the Healthy Michigan Plan iii. the Flint 1115 Waiver or Community Block Grant iv. enrolled in the 1915(c) Habilitations Supports Waiver v. Enrolled in MIChild program; or
vi. Persons whom the PIHP has assumed or been assigned County of Financial Responsibility status under Chapter 3 of the Michigan Mental Health Code.
vii. Individuals covered under the SUD Community Grant b. Funding streams to be managed
i. Medicaid – TANF/DAB ii. Medicaid – Autism
iii. Medicaid – Healthy Michigan iv. Medicaid – 1915 (c) Habilitation v. Medicaid – Flint 1115 Waiver
vi. DHS Incentive Payments (DHIP) c. Funding streams to be administered
i. Substance Abuse Prevention and Treatment (SAPT) Block Grant ii. PA2 Liquor Tax Funding
iii. Other Grant Funding d. Medicaid Covered Services (All covered services are found at this website:
https://www.mdch.state.mi.us/dch-medicaid/manuals/MedicaidProviderManual.pdf).

14
Due to size of the report, (e.g., 2008 pages), it is recommended that Offerors use the bookmarked website for information.)
i. 1915(b) Services Described in the Michigan Medicaid Provider Manual: Mental Health – Substance Abuse Section (See Bidder Library)
ii. 1915(b)(3) Services All Medicaid services in included in the Described in the Michigan Medicaid Provider Manual: Mental Health – Substance Abuse Section (Behavioral Health and Intellectual Disability Supports and Services, page 303)
iii. 1915(c) Services Described in the Michigan Medicaid Provider Manual: Mental Health – Substance Abuse Section
iv. Autism Services under the iSPA and 1915(b) waiver as described in the Michigan Medicaid Provider Manual.
v. All Healthy Michigan Plan additional Substance Use Disorder and Supports described in the Medicaid Provider Manual.
e. Substance Abuse Prevention and Treatment Block Grant Services (all covered services can be found in the LRE SUD Services Provider Manual located in the Bidder Library).
i. Initial Assessment ii. Outpatient Treatment
iii. Medication Supported Services iv. Intensive Outpatient Treatment v. Residential Substance Abuse Services
vi. Sub-Acute Detoxification vii. Acute Detoxification
viii. Specialty Services
E. Term of Contract The initial term of this contract will be for 12months. The contract may be extended in
increments of no more than 12 months, up to a total of 36 months. All extensions will be contingent upon offeror’s performance and continuation of the MDHHS/LRE contract.
F. Minimum Offeror Eligibility Criteria I. Proof of at least five (5) full years of public behavioral health (i.e., mental health and
substance use disorder) managed care experience on a shared or full risk basis II. Proof of experience managing, delivering, or coordinating services for persons with
developmental disabilities. III. Ability to accept financial risk consistent with in the State of Michigan law and
regulation. IV. Submission of an electronic Letter of Intent to submit a proposal (due by 5:00 PM,
March 23, 2018). This letter of intent should provide the name and contract information of the Offeror’s point of contact during the procurement.
V. Submission of the proposal on or before May 15, 2018, 4:00 PM VI. Signed certification statement that neither the BHO/MCO nor any entity with which it is
affiliated or related is under suspension or debarment by Michigan, any other state, or the federal government. This does not limit the BHO/MCO’s duty to disclose all litigation noted below.
15
VII. Agreement that the Offeror shall bear all costs it incurs related to proposal preparation, start-up and readiness review.
VIII. Agreement that the Offeror will not subcontract or delegate any of the managed care functions without prior approval of the LRE.
G. Resources in Bidder Library MDHHS/Lakeshore Regional Entity Contract and Attachments State of Michigan Department of Health and Human Services Request for Information No. [RFI-
1800000000003] 298 Pilot(s) – Medicaid Physical-Behavioral Health Full Financial Integration LRE/CMHSP Contract and Attachments Pathway to Integration: Michigan’s 1115 Waiver Proposal for Persons with Severe Mental
Illness, Substance use Disorders, Intellectual and Developmental Disabilities and Children with Severe Emotional Disturbances
LRE Bylaws LRE Operating Agreement – 8-2017 LRE Common Contract Program Audit of Lakeshore Regional Entity PIHP (2015) Most Recent Corrective Action Plan in Response to Program Audit External Quality Review Organization (EQRO) Reports Michigan Medicaid Provider Manual - Mental Health/Substance Abuse Section LRE SUD Services Provider Manual LRE Prevention Service Provider Manual Key Performance Indicator Dashboard CMHSP/PIHP Administrative Cost Report (FY 2016 & 2017) Medicaid Unit Net Cost Report (FY 2016 & 2017) LRE Funding by Year Report (FY 2016 & 2017) Membership Count by Service Group Count by Service Unit Report CMHSP Assessment Tools Quality Assurance / Performance Improvement Program (QAPIP) Pricing Proposal Template
16
H. Schedule of Events Date and Time Task March 15, 2018 RFP Issued March 23, 2018, by 5:00pm Eastern time
Mandatory Letter of Intent to respond due to LRE by prospective bidders to the LRE Single Point of Contact via e-mail.
March 26, 2018, 10:00am Eastern time
Bidder conference call (for those that submitted timely intent to respond)
March 30, 2018, by 5:00pm Eastern time
Bidder written questions due to LRE
April 6, 2018 LRE to issue written responses to Bidder questions May 15, 2018, by 4:00pm Eastern time
Final proposals from Bidders due
June 8, 2018 Tentative Bidder Oral Presentation June 15, 2018 Notification to successful Bidder of intent to contract June 29, 2018 Contract execution September 28, 2018 Completion of Readiness Review October 1, 2018 Go Live
I. Single Point of Contact All communications regarding this RFP shall be submitted to the following e-mail address:
[email protected]. Phone calls will not be accepted. Please include "Lakeshore RFP" in the subject line for any correspondence. Contact with any other LRE officials, employees, agents or representatives of the LRE, including the member CMHSPs, LRE board members and CMHSP board members, concerning this RFP is grounds for disqualification.
J. Request for Proposals Guidelines It is the policy of the LRE to solicit Proposals with a bona fide intention to award a contract. This
policy notwithstanding, any Proposal submitted in response to this RFP is done so with the following expressed understanding by the submitting entity:
• The LRE has the right, in its sole discretion, to reject any and all Proposals. • The LRE, at its sole discretion, may choose to withdraw this RFP at any point in time
following its release. • The LRE may modify the selection process, the scope of the project, or the required
responses to the RFP. • Solicitations of Proposals and granting of exclusive negotiation rights does NOT commit the
LRE to accept any terms of any Proposal. The final terms of any agreement will be determined by direct negotiation. The LRE may suspend or terminate negotiations at any time that it determines additional negotiations would be unproductive. As such, acceptance of the Proposal from a BH-MCO does not guarantee that the LRE will enter a Subcontract with the MCO.
• The LRE reserves the right, in its sole discretion, to reject all Proposals received as a result of this RFP and/or to negotiate separately with competing BH-MCOs. If all Proposals submitted are unacceptable to the LRE, as determined by its sole discretion, the LRE reserves the right to reject the Proposals and re-issue the RFP.
17
• The LRE reserves the right to renegotiate any financial offers submitted by Offerors in their Proposals and to condition any selection of an offeror on such negotiations.
• The LRE reserves the right to reject a Proposal at any time during the review process. • In addition to the requirements set forth in this RFP, the Subcontract will also include all the
LRE's mandatory required contract provisions.
K. Proposal Submission and Format All Proposals are to be received both electronically and in hard copy no later than May 15, 2018
at 4:00pm EST. LRE will reject late submissions not received by the designated date and time specified in the RFP. It is the Offeror’s responsibility to appropriately mark and deliver the Proposal to LRE by the specified date.
Physical Address for hand delivery and overnight and commercial mail:
Lakeshore Regional Entity ATTN: RFP
5000 Hakes Drive, Suite 500 Norton Shores, MI 49441
All proposals become the property of LRE after submission.
• Proposals are to be in Microsoft Word (Windows 98 or higher), single-spaced, double sided, and on 8 ½ x 11-inch white bond paper, three-hole punched, and placed in sturdy three-ring binders.
• Narrative text must be no smaller than 11-point font. Figures may not incorporate text smaller than 10-point font. All pages must have one-inch margins and page numbering must be sequential per section.
• Proposals must be organized and numbered in a manner that facilitates reference to this RFP and its requirements. Offerors must respond to each item in the order it appears in the RFP. The Offeror’s response must include the text of each question and headings and numbering to match the corresponding section of the RFP. Offerors may place attachments in a separate section, if the section notes that attachments are not included in the page limits specified in the RFP.
L. Copies of Proposal Required for Submission • Offerors must submit one (1) hardbound original and nine (9) hardbound copies of the
Proposal (10 total hardbound copies). Each binder must be labeled clearly with the title of this RFP, the Offeror’s legal name.
• Two (2) complete submissions are to be sent via electronic storage media.
• One (1) additional hard copy of the Proposal must be unbound.

18
M. Public Disclosure of Proposals All information in the MDHHS contract and any proposal submitted in response to this RFP is
subject to the provisions of the Freedom of Information Act, 1976 PA 442, as amended, MCL 15.231, et seq. Should the offeror wish to claim any portion of its proposal as a trade secret or proprietary and confidential, it may submit an electronic redacted copy. However, no assurance of confidentiality can be given. The information will be subject to public disclosure at the time the bids are opened or, in the alternative, at the time the deadline for submission of proposals passes.
N. Economy of Presentation Unnecessarily elaborate Proposals beyond those sufficient to provide a complete and effective
response to this RFP are not desired and may be construed as an indication of the Offeror’s lack of ability to provide efficient work products.
The Offeror must adhere to page limits where specified. Page limits are listed in parentheses at the end of the title of the section to which the page limit applies. A three-page limit, for example, means that the response should not be more than three one-sided pages that meet the size, font, and margin requirements specified in the Proposal Format above. The question text will not be included in the page limit.
LRE reserves the right not to review information provided in excess of the page limits. Offerors need not feel compelled to submit unnecessary text to reach the page limits.
Offerors must not submit information or attachments not explicitly requested in the RFP. Elaborate artwork, expensive paper and bindings, and expensive visual or other presentation aids are neither necessary nor desired.
III. Information Required from the MBHO/MCO Offeror (Scope of Work)
A. Cover Letter (Page Limit – 5 Pages) The cover letter will summarize the offeror’s strengths, skills and capabilities to perform the
services described in this RFP and be signed by the person who is authorized to enter into a contract with the LRE. In addition, the letter shall certify the following:
1. That neither the offeror nor any entity with which it is affiliated or related is under suspension or debarment by Michigan, any other state, or the federal government.
2. That neither the offeror or any entity which is affiliated or related have • not within a three-year period preceding this agreement been convicted of or had a civil
judgment rendered against them for commission of fraud or a criminal offense in connection with obtaining, attempting to obtain, or performing a public (federal, state, or local) transaction or contract under a public transaction;
• violation of federal or state antitrust statutes or commission of embezzlement, theft, forgery, bribery, falsification or destruction of records, making false statements, or receiving stolen property;
19
• Are not presently indicted or otherwise criminally or civilly charged by a government entity (federal, state or local) with commission of any of the offenses enumerated in section 2, and;
• Have not within a three-year period preceding this agreement had one or more public transactions (federal, state or local) terminated for cause or default.
3. The offeror shall comply with all current and potential future modifications of MDHHS contractual requirements and regulations regarding the Michigan Medicaid Managed Specialty Supports and Services Concurrent 1915(b)/(c) waiver programs, the Healthy Michigan Program, the Flint 1115 Waiver and Substance Use Disorder Community Grant Programs.
4. The offeror can accept financial risk consistent with in the State of Michigan law and regulation 5. That the Offeror will not subcontract or delegate any of the managed care functions without
prior approval of the LRE. 6. A statement that the offeror shall assure that it will maintain a medical loss ratio (MLR) of 85
percent of all Medicaid and Healthy Michigan Funds.
B. Information about the offeror (Page Limit – 2 Pages) 1. Company Information
• Company Name • Home Office Address • Local Address in Michigan • FEIN Number • Person Authorized to negotiate a contract with the LRE
o Name o E-mail Address o Company Title o Address o Phone Number o Fax Number
• Person to serve as the Implementation Lead for the Program o Name o E-mail Address o Company Title o Address o Phone Number o Fax Number
2. Provide evidence that the Offeror has the ability to bear insurance risk in the State of Michigan
C. Organizational Structure, Legal Standing, & Litigation History (Page Limit – 1 Page, excluding attachments) 1. Describe your organizational structure (i.e., corporation, partnership, joint venture, etc.) 2. Are you a for-profit or not-for-profit entity?

20
3. Provide, as an attachment, a chart showing your corporate/entity structure, including and parent, brother/sister or subsidiaries that will be performing functions related to this contract and what those functions would be.
4. Attach documentation to support you are registered to do business in Michigan and that you are in good standing
5. Provide a statement disclosing any possible conflicts of interest and/or relationship(s) which of could be viewed as a conflict if the offeror is selected. This includes relationships with the LRE or its member CMHSPs by the offeror, and its affiliated and related entities.
6. List, in an attachment, all outstanding litigation for in which your organization and any proposed affiliate or parent is a defendant and for which the amount of recovery being sought by the plaintiff is more than $50,000. Also list all judgements and settlements more than $50,000 against you, any affiliate that would perform work under this contract, and the parent for the past two years.
D. Solvency & Financial Integrity (Page Limit – 1 Pages, excluding attachments) State your organization's Excess Equity and Liquidity Ratios as described below:
1. Provide the following Liquidity Ratios for your organization, and separately for your parent corporation, for the past two completed fiscal years and the most recent quarter (current assets/current liabilities); defensive interval (days cash on hand); and total cash/claims liability (IBNR & RBUC).
2. Provide, in an attachment, a certified audited copy of your two most recent annual financial statements together with a copy of the balance sheet accompanying said audited financial statements.
E. Relevant Managed Care Experience (Page Limit – 18 Pages, excluding attachments) 1. Provide information on all current, relevant public sector (Medicaid) managed care
contracts. (Page Limit – 10 Pages) For each contract, include: • Contract/customer • Numbers of covered lives/members • Covered services managed • Service populations (persons with mental illness, children and youth with severe
emotional disturbance, persons with intellectual or developmental disabilities, persons with substance use disorders, other)
• Start date of the contract (if a renewal or re-awarded, initial start date) • Specific managed care functions performed (e.g., Utilization Management, Member
Services, Claims Payment, Quality Improvement, etc.) • State/county customer reference, with contact information (phone number and e-
mail address) 2. Describe your experience serving persons with intellectual or developmental disabilities,
and specifically experience with 1915(c) Home and Community Based Waiver Services (Page Limit – 1 Page)
3. Describe your experience in managing substance use disorder services. (Page Limit – 1 Page) 4. Describe your experience in managing autism services. (Page Limit – 1 Page)
21
5. Describe your strategies for incorporating recovery and resiliency principles into the program and how these principles are supported. (Page Limit – 1 Page)
6. Describe your experience with implementing and assuring person-centered planning. (Page Limit – 1 Page)
7. Describe specific activities that have been implemented that demonstrate good collaborative, working relationships with a local or regional governmental customer. (Page Limit – 1 Page)
8. Provide in an attachment a list all corrective action plans required for all Medicaid managed care contracts for the past five years as an attachment.
9. Provide in an attachment a list of the amounts and reasons for performance penalties and liquidated damages related to all Medicaid managed care contracts for the past five years as an attachment.
10. List any contracts that have been terminated prior to the original expiration date. Please specify the reasons for termination. (Page Limit – 1 Page)
11. Disclose any prior debarment, exclusion, suspension, litigation or proceeding within the last five years for the offeror, any relevant affiliate and/or the parent. (Page Limit – 1 Page)
F. Offeror’s Proposed Organizational Structure (Page Limit – 6 Pages, excluding attachments) 1. Describe the overall organizational structure with functional units for the operation of
the Program. Which functions will be performed within the Region? 2. Attach an organizational chart showing overall organization and reporting lines and
prepare sub-chart specific to the organizational structure and reporting lines for the Program.
3. Include a description of any subcontracting entities that are planned to be utilized to perform any of the administrative managed care functions. Include the rationale for subcontracting each function and the offeror’s experience working with the subcontractor providing these services under a similar Medicaid contract. If none, state so.
4. Identify and describe key administrative positions fully dedicated to the program, including but not limited to a Chief Executive Officer/Project Director, Financial Officer, Medical Director, and Quality Improvement Director.
5. For every position to work on the program, please provide by job title, the number of full-time equivalent employees, the percent of time dedicated to this program, and location of the staff. Provide as an attachment.
G. Distribution of Funds & Risk Corridor Assumption (Page Limit – 5 Pages) It has been the intent of the LRE to provide for a funding system that is fair and equitable to all
Medicaid Persons Served in Region 3 and to preserve the fiscal viability of the safety net CMHSPs. Region 3's initial funding distribution for Medicaid 1915(b), 1915(b)(3) and the Habilitation Supports Waiver (HSW) funds provided each Member CMHSP with funding based upon historical spending trends. Starting 10/1/2015, the region began the transition to a Per Member Per Month (PMPM) funding formula with 75% funding based upon historical expenditures and 25% on a PMPM model. On 10/1/2016 the formula was modified to 50% historical and 50% PMPM. The result of this change away from the historical basis resulted in a significant adverse impact on two of the five CMHSP members. Beginning October 1, 2017, the Entity halted the historical/PMPM funding methodology transition at

22
50% to begin analysis to create a Needs-based Funding Formula that allows for the right services at the right time in the right duration rather than the current Per Member/Per Month (PMPM) funding methodology. All other fund sources have been paid as PMPM since inception of Region 3.
The current flow of funds between the LRE and its member CMHSPs is as follows by funding type included in this RFP:
Distribution of Medicaid Capitation — Healthy Michigan. The LRE distributes the Healthy Michigan dollars, if any, to the CMHSP Members using the same methodology as MDHHS allocates the dollars to the Entity (PMPM).
Distribution of Medicaid Capitation — DAB & TANF (Disabled, Aged and Blind and Temporary Assistance for Needy Families). The LRE retains a small amount for its administrative cost. Fifty (50) percent of the remaining PMPM goes to CMHSPs based upon prior 3 year’s spending to assure stability. The remaining Fifty (50) percent of the PMPM goes to the CMHSP Members using the same methodology as MDHHS allocates the dollars to the Entity (PMPM).
Distribution of Medicaid Capitation — 1915(c) (HAB) Waiver. – Same as DAB & TANF
Distribution of Medicaid Capitation — Autism. The LRE distributes the Autism dollars to the Members using the PMPM received from the MDHHS and gives a 25% higher weighted average for those enrolled with the higher intensity. Distribution of Substance Use Disorder ("SUD") Funding — All Sources. SUD Medicaid and Healthy Michigan will be allocated to the Members using the same methodology as MDHHS allocates the dollars to the Entity. MDHHS Block Grant Dollars will be allocated first by the Allocation set by MDHHS to the splits between Prevention and Treatment Dollars. Prevention is retained by the LRE and used for the centralized prevention functions. This now becomes the responsibility of the Offeror. The Treatment dollars will be divided between the Members based on historic allocations. In the future the distribution would be based on General Fund need. by using the latest Census to get the population for each of the counties. Using the ACS 200% Federal Poverty Level (FPL) (American Community Survey-United States Census Bureau) will be used to determine the base for initial need and subtracting the following: Medicaid Eligible, Healthy Michigan Eligibles and Marketplace Enrollment (Less than or equal to 200% FPL). This method will determine the base for SUD GF Block Grant Distribution. (This is the process MDHHS is planning to use for GF distribution).
Distribution of Public Act 2 (PA 2 Liquor Tax) Funds. Public Act 2 (PA2) Liquor Tax funds will be approved for distribution by the Entity SUD Oversight Policy Board. PA2 funds will be allocated back to the county from which the funds originated. Any surpluses will be sent back to the Entity for distribution in the following years from which the funds originated.
As described above regarding the risk corridor requirements of the contract, Offerors are required to provide risk protection for the full 7.5% of claims risk and maintain an 85% MLR for Medicaid and Healthy Michigan funds.
23
Given the information above, please describe:
1. How you would retain or modify the current flow of funds to the CMHSPs for each funding payment model and on what timeframe?
2. How will the offeror ensure that the payment method implemented does not destabilize the CMHSPs and/or their provider network?
3. Provide evidence that the proposed approach is effective and achievable.
H. Implementation of Administrative Functions H.1 Member Services (Page Limit – 6 Pages)
The 2013 Application for Participation outlined expectations for PIHPs to be selected: “Customer services functions are typically: 1) information services that are compliant with 42 CFR 438.10, 2) maintenance and annual provision of the Customer Services Handbook that has been approved by MDHHS, 3) facilitation of consumer empowerment and participation in PIHP planning and monitoring, 4) customer complaint, grievances and appeals, and 5) community benefit. While functions number one and two are the responsibility of the PIHP, the other three functions may be delegated in part or in full.”
Section 6.3 of the MDHHS/LRE contract delineates the scope of work requirements that the offeror would need to meet on behalf of the LRE. Additional standards for the 24/7 access line are included in Attachment P4.1.1 (Access System Standards). Currently these functions are performed largely by the LRE. The member CMHSPs currently supplement the efforts through community outreach and education.
1. Please briefly describe your experience and performance in delivering these administrative services. Include recent data on the following industry metrics that would reflect your performance in this area under a similar Medicaid contract:
a. Average Speed to Answer b. Average Abandonment Rate c. First Call Resolution
2. Please describe how you would propose to deliver these administrative services, including but not limited to
a. Where the live answer service would be located b. What would be the proposed staffing for these functions c. Will staff be 100% dedicated to this contract? If not describe how staff time will be
determined and allocated d. What will be the strategy for after-hour calls? e. Describe the methods by which the member services staff will be trained on the
Michigan program and the available resources in the Region f. Describe the grievance and appeals process and the methods by which members and
providers will be informed of their appeal and grievance rights. 3. Please describe how you propose to transition these responsibilities from the LRE to the offeror
with minimum disruption. 4. Please describe how you propose to coordinate with the member CMHSPs on related services.
24
H.2 Provider Network Services (Page Limit – 9 Pages) MDHHS’s Application for Participation outlined the expectations for the PIHP: “Provider
Network Management typically includes the functions of 1) network development and procurement (and re-procurement), 2) provider contract management (including oversight), 3) network policy development, 4) credentialing, privileging and primary source verification of professional staff, and 5) background checks and qualifications of non-credentialed staff. The “provider network” of the PIHP includes as applicable, the member CMHSPs, or any other provider with which the PIHP has a direct contract to deliver a covered service. It is the responsibility of the PIHP to perform the functions above, and to assure that its provider network performs these functions in the management of any providers it procures.”
MDHHS is currently considering network adequacy standards (e.g., time and distance) but are not finalized at this time. Section 4.0 of the MDHHS Contract outlines the Access Assurances for this program. Section 7.0, subsections 7.1-7.6 of the same contract and delineates the provider network services scope of work requirements and Attachment P 7.1.1 provides the MDHHS Credentialing and Re-credentialing Processes policy that the offeror would need to meet on behalf of the LRE. Currently, the access assurances are the responsibility of the LRE. The provider network functions are a shared responsibility by the LRE and its member CMHSPs. For example, the LRE holds provider contracts with those CMHSP members that provide direct services and is responsible for credentialing. All member CMHSPs also subcontract and credential other community providers. Therefore, credentialing processes and provider rates are non-uniform across the region. One of the goals of this procurement is to reduce the variability of network management, while retaining a robust network that allows the LRE to meet the required access assurances.
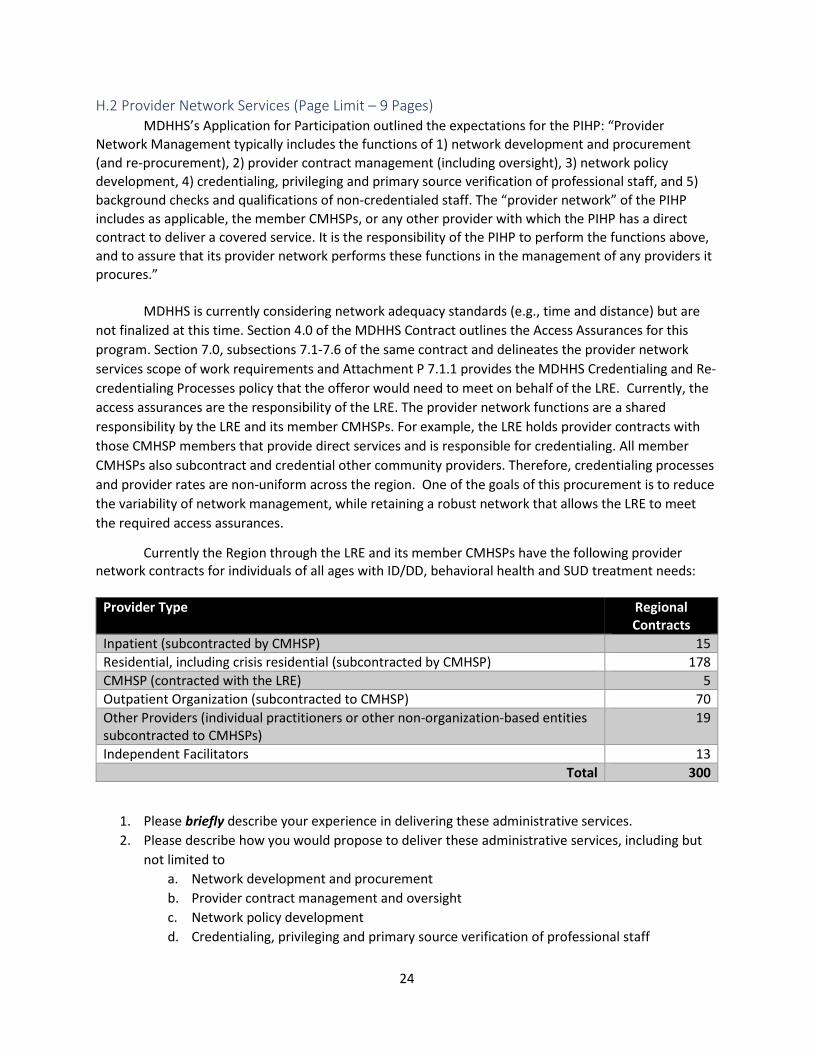
Currently the Region through the LRE and its member CMHSPs have the following provider network contracts for individuals of all ages with ID/DD, behavioral health and SUD treatment needs:
Provider Type Regional
Contracts Inpatient (subcontracted by CMHSP) 15 Residential, including crisis residential (subcontracted by CMHSP) 178 CMHSP (contracted with the LRE) 5 Outpatient Organization (subcontracted to CMHSP) 70 Other Providers (individual practitioners or other non-organization-based entities subcontracted to CMHSPs)
19
Independent Facilitators 13 Total 300
1. Please briefly describe your experience in delivering these administrative services. 2. Please describe how you would propose to deliver these administrative services, including but
not limited to a. Network development and procurement b. Provider contract management and oversight c. Network policy development d. Credentialing, privileging and primary source verification of professional staff

25
e. Background checks and qualifications of non-credentialed staff f. What would be the proposed staffing for these functions. g. Will staff be 100% dedicated to this contract? If not describe how staff time will be
determined and allocated. h. What methods would be used for provider reimbursement. i. Will you propose alternative payment or value-based reimbursement models?
i. Will you propose sub-capitation? 3. Please describe how and when you propose to transition these responsibilities from the LRE and
CMHSPs to the offeror with minimum disruption. 4. Please describe how you propose to coordinate with the member CMHSPs on related services.
H.3 Management Information Services (non-claims related) (Page Limit – 10 Pages, excluding system diagrams and process flow charts)
MDHHS’s Application for Participation outlined the expectations for the PIHP: “The PIHP must have an information management system that supports the core administrative activities of the region including:
a. The ability to accept on behalf of entire region of CMHSPs/CAs, enrollment and revenue files, in HIPAA compliant formats, from the State of Michigan.
b. The ability to accept clinical, financial, utilization, demographic, quality and authorization information from CMHSP/CA sources (including providers) in standard electronic formats (i.e., HIPAA Administrative Simplification X12N). Note if the CMHSP/CA/provider source can send in standard electronic formats, the PIHP must receive via standard electronic means versus requiring direct entry or non-standard format.
c. The ability to accept clinical, financial, utilization, demographic, quality and authorization information through clearinghouses and other viable, secure and efficient means when requested by CMHSP/CA sources and providers.
d. The ability to analyze, integrate and report clinical, financial, utilization, demographic, quality and authorization information.
e. The ability to submit QI and encounter data in compliant formats as specified by MDHHS. Data must pass all required data quality edits prior to being accepted into CHAMPS before it is sent to the warehouse.
f. The ability to identify, analyze and report costs and revenues for service components, including, but not limited to, analysis and reporting by regions and CMHSP/CA sources and providers.
g. The ability to detect and correct errors in data receipt, transmissions and analyses. This includes screening for completeness, logic, and consistency; and identifying and tracking fraud and abuse.
h. The ability (within limits of law) to safely and securely send and receive data to and from other systems. This includes, but is not limited to, the State of Michigan, health plans and providers systems including physical health and non-healthcare support systems of care. (Note: If the PIHP region is selected to participate in Medicaid Health Homes and/or Integrated Care For Dual Eligible demonstrations, the PIHP must be able to interface with health plans and provider systems).”
26
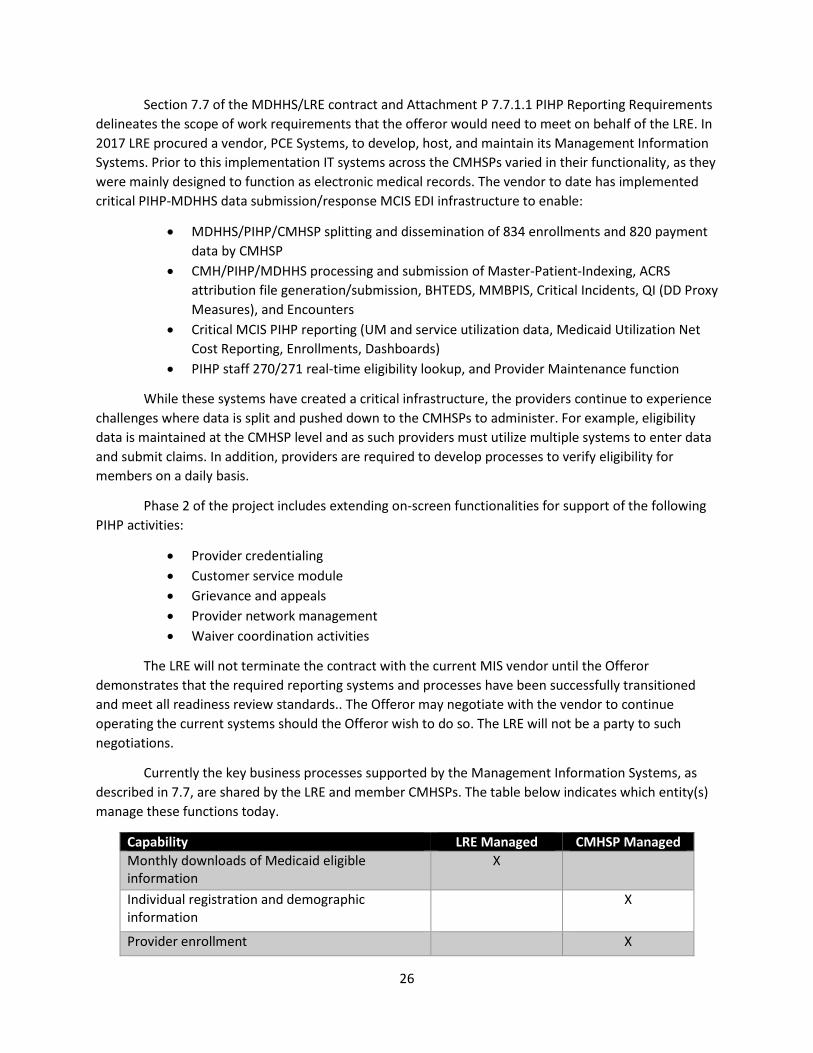
Section 7.7 of the MDHHS/LRE contract and Attachment P 7.7.1.1 PIHP Reporting Requirements delineates the scope of work requirements that the offeror would need to meet on behalf of the LRE. In 2017 LRE procured a vendor, PCE Systems, to develop, host, and maintain its Management Information Systems. Prior to this implementation IT systems across the CMHSPs varied in their functionality, as they were mainly designed to function as electronic medical records. The vendor to date has implemented critical PIHP-MDHHS data submission/response MCIS EDI infrastructure to enable:
• MDHHS/PIHP/CMHSP splitting and dissemination of 834 enrollments and 820 payment data by CMHSP
• CMH/PIHP/MDHHS processing and submission of Master-Patient-Indexing, ACRS attribution file generation/submission, BHTEDS, MMBPIS, Critical Incidents, QI (DD Proxy Measures), and Encounters
• Critical MCIS PIHP reporting (UM and service utilization data, Medicaid Utilization Net Cost Reporting, Enrollments, Dashboards)
• PIHP staff 270/271 real-time eligibility lookup, and Provider Maintenance function
While these systems have created a critical infrastructure, the providers continue to experience challenges where data is split and pushed down to the CMHSPs to administer. For example, eligibility data is maintained at the CMHSP level and as such providers must utilize multiple systems to enter data and submit claims. In addition, providers are required to develop processes to verify eligibility for members on a daily basis.
Phase 2 of the project includes extending on-screen functionalities for support of the following PIHP activities:
• Provider credentialing • Customer service module • Grievance and appeals • Provider network management • Waiver coordination activities
The LRE will not terminate the contract with the current MIS vendor until the Offeror demonstrates that the required reporting systems and processes have been successfully transitioned and meet all readiness review standards.. The Offeror may negotiate with the vendor to continue operating the current systems should the Offeror wish to do so. The LRE will not be a party to such negotiations.
Currently the key business processes supported by the Management Information Systems, as described in 7.7, are shared by the LRE and member CMHSPs. The table below indicates which entity(s) manage these functions today.
Capability LRE Managed CMHSP Managed Monthly downloads of Medicaid eligible information
X
Individual registration and demographic information
X
Provider enrollment X

27
Third party liability activity X
Claims payment system and tracking X
Grievance and complaint tracking X
Tracking and analyzing services and costs by population group, and special needs categories
X X
Encounter and demographic data reporting X
Quality indicator reporting X X
HIPAA compliance X X
Individual access and satisfaction X
1. Please briefly describe your experience in delivering these administrative services. 2. Please describe how you would propose to deliver these administrative services, including but
not limited to: a. The Management Information System (MIS) the offeror will implement and
demonstrate that the offeror’s MIS and practices have the capacity to meet the obligations of the contract. The response must address the requirements of Section 7.7. The description should address:
i. Hardware and system architecture specifications; ii. Data and process flows for all key business processes in Section 7.7;
iii. The protection and security features of the information management system to ensure confidentiality, data integrity and protection from intrusion, including the risk mitigation and management procedures for a loss of confidential data or security breach to include notification of affected consumers; and
iv. Attest to the availability of the data elements required to produce required management reports.
b. Describe the policies and procedures that will be used to analyze claims and encounter data to create information about region wide and CMHSP specific service utilization. The response should also address how the Offeror will use that information to inform risk management strategies and other functions.
c. Describe the policies and procedures that will be used to validate that data required under the contract are accurate and complete prior to submission.
d. How the offeror will ensure accuracy, timeliness, and completeness of Encounter Data submissions.
3. Please describe how you propose to transition these responsibilities from the LRE/vendor and CMHSPs to the offeror with minimum disruption. And how the transition and resulting systems will alleviate administrative burden experienced by providers in the region.
H.4 Financial Management System (Page Limit – 8 Pages) MDHHS’s Application for Participation outlined the expectations for the PIHP: “Financial
management functions typically include: 1) budgeting – general accounting and financial reporting, 2) revenue analyses, 3) expense monitoring and management, 4) service unit and recipient-centered, 5) cost analyses and rate-setting, 6) risk analyses, risk modeling and underwriting, 7) insurance, re-
28
insurance and management of risk pools, 8) supervision of audit and financial consulting relationships, 9) claims adjudication and payment, and 10) audits.”
Section 7.8 of the MDHHS/LRE contract delineates the scope of work requirements that the offeror would need to meet on behalf of the LRE. LRE is currently meeting minimum financial management requirements, while all five CMHSPs maintain their own financial management operation. The LRE collects data from the CMHSPs and reports on behalf of the region in accordance with MDHHS financial reporting requirements as specified in the Management Information Systems section of the Contract and accompanying Attachment (P 7.7.1.1). The member CMHSPs manage the process of claims adjudication at the consumer level, and submit required data to the LRE. [The claims management system is addressed in a later section of the RFP.] The CMHSPs ensure compliance with third party resource requirements through identification and collection of third party liabilities and is perceived to be an area of potential significant improvement. One of the goals of this procurement is to reduce administrative duplication and improve the overall efficiency and accuracy of financial management in the region.
1. Please briefly describe your experience and performance in delivering these administrative services. Include recent data on the following industry metrics that would reflect your performance in this area under a similar Medicaid contract:
a. Annual dollars cost-avoided b. Annual dollars recovered
2. Please describe how you would propose to deliver these administrative services, including but not limited to:
a. The accounting system that the offeror will implement, including i. Capacity and processes for reporting specific fund sources as required by the
Contract ii. Cost accounting methodology that will be used to ensure consistent treatment
of costs across different funding sources and assure proper cost allocation b. Describe the policies, processes and positions responsible for maintaining internal
control systems. c. Describe the process for performing Coordination of Benefits (COB) and Third-Party
Liability (TPL) i. If COB and TPL functions are outsourced, provide information on the Material
Subcontractor to be used and oversight processes that will be employed. d. Attach a COB sample report from another State or County contract.
3. Please describe how you propose to transition these responsibilities from the LRE and CMHSPs to the offeror with minimum disruption.
H.5 Claims Management System (Page Limit – 7 Pages) Section 7.8.2 of the MDHHS/LRE contract delineates the scope of work requirements that the
offeror would need to meet on behalf of the LRE. Currently these functions are delegated to the CMHSPs. The member CMHSPs manage the process of claims adjudication at the consumer level, and submit required data to the LRE. Each quarter, the LRE visits each CMHSP to validate the claims, using a Medicaid eligibility verification system. As a result, providers in the region may be submitting claims to multiple CMHSPs. One of the goals of this procurement is to eliminate administrative duplication in the system and reduce administrative burdens on providers.
29
1. Please briefly describe your experience and performance in delivering these administrative services. Include recent data on the following industry metrics that would reflect your performance in this area under a similar Medicaid contract:
a. Percentage of clean claims adjudicated accurately b. Percentage of clean claims adjudicated timely
2. Please describe how you would propose to deliver these administrative services, including but not limited to:
a. System capacity for complying with timely claims payment requirement i. If claims processing and payment functions are outsourced, provide information
for the Material Subcontractor and oversight processes that will be employed b. Processes which will be used to train and support providers for claims submission and
adjudication c. Proposed provider appeal process to promptly and fairly resolve provider-billing
disputes d. Post-payment review methodology and proposed process to verify that services were
provided e. Offeror’s capacity for accepting HIPAA compliant electronic billing
3. Please describe how you propose to transition these responsibilities from the CMHSPs to the offeror with minimum disruption.
H.6 Quality Assurance / Performance Improvement Program (QAPIP) (Page Limit – 7 Pages, excluding attachments)
MDHHS’s Application for Participation outlined the initial expectations if the PIHP. “Quality Management typically includes the following functions: 1) developing an annual Quality Assessment and Performance Improvement Program (QAPIP) plan and report, 2) standard-setting, 3) conducting performance assessments, 4) conducting on-site monitoring of providers in the provider network, 5) managing regulatory and corporate compliance, 6) managing outside entity review processes (e.g., external quality review, PIHP accreditation), 7) conducting research, 8) facility quality improvement process , 9) facility provider education and oversight, and 10) analyzing critical incidents and sentinel events. MDHHS expects that the PIHP will not delegate these functions and understands that some of the functions will be performed in addition by the provider network (member CMHSPs, MCPNs, or core providers).”
Section 7.9 and Attachment P 7.9.1 of the MDHHS/LRE contract delineates the scope of work requirements that the offeror would need to meet on behalf of the LRE. A summary of this reporting is contained in the Executive Key Performance Indicator (KPI) Dashboard which can be found in the Bidder’s Library. Currently the LRE has primary responsibility for these functions. The member CMHSPs support the LRE’s Quality Improvement Plan (QIP) by participating in the development and implementation of the LRE’s performance improvement programs (PIPs) and developing local QIPs that align with the LRE QIP and locally identified quality improvement needs.
1. Is the offeror accredited by a national accreditation body such as NCQA or URAC? If yes, please attached the certificate of accreditation as evidence. If not, what would be the plan for the offeror to become accredited within two years?
30
2. Please briefly describe your experience in delivering these administrative services. Include recent data on the following industry metrics that would reflect your performance in this area under a similar Medicaid contract:
a. Antidepressant Medication Management Acute Phase b. Antidepressant Medication Management Continuation Phase c. Adherence to Antipsychotic Medications for Individuals with Schizophrenia d. Cardiovascular Health Screening for People with Schizophrenia/Bipolar Disorder who are
Prescribed Antipsychotic Medications 3. Please describe how you would propose to deliver these administrative services, including but
not limited to: a. Describe the Quality Management structure, including a table of organization, meeting
structures including participants and feedback processes b. Development of the QAPIP in response to the MDHHS external review, including
infrastructure and resources that will be implemented locally c. Processes used to conduct annual effectiveness review of the QAPIP, including
i. Identifying trends in service delivery and health outcomes and ii. Monitoring progress on PIPs
d. How the annual effectiveness review of the QAPIP will be disseminated annually to network providers and to members upon request
e. Describe a data-driven clinical initiative that the offeror initiated within the past 24 months that have yielded measurable improvement in clinical care for a managed care population comparable to those served by the LRE.
4. Please describe how you propose to transition these responsibilities from the LRE to the offeror with minimum disruption and whether any role would be reserved for the LRE.
5. Please describe how you propose to coordinate with the member CMHSPs on related services.
H.7 Service and Utilization Management (Page Limit – 9 Pages) MDHHS’s Application for Participation outlined the initial expectations if the PIHP. “Utilization
management typically includes the following functions: 1) access and eligibility determination, 2) utilization management protocols, 3) service authorization, and 4) utilization review. The functions may be fully or partially-delegated to the PIHP’s provider network.
Section 7.10 of the MDHHS/LRE contract delineates the scope of work requirements that the offeror would need to meet on behalf of the LRE. Currently these functions are delegated to the CMHSPs. Each CMHSP has its own internal mechanisms to determine service need and authorization. Please see the CMHSP Assessment Toll document in the resource library. Consolidation of these functions is necessary to achieve the goals of the procurement including, creating consistency in service access and utilization management by centralizing practices, reducing provider burden, and improving quality of care by accurately assessing member needs and leveraging evidence-based guidelines to determine medical necessity.
1. Please briefly describe your experience and performance in delivering these administrative services. Include recent data on the following industry metrics that would reflect your performance in this area under a similar Medicaid contract
a. Average number of days to determination b. Appealed denials overturn rate
31
2. Please describe how you would propose to deliver these administrative services, including but not limited to:
a. The proposed staffing that will be employed to perform UM functions, including organizational chart, and position experience, licensing/certification, and location
b. Please describe the medical necessity and/or level care criteria that you use (e.g., ASAM, Interqual, etc.).
c. The UM guidelines the offeror plans to employ, including whether and how the guidelines comply with the standards under the MDHHS/LRE contract
i. If the UM guidelines were developed internally, describe the process by which they were developed and when they were developed or last revised
d. How the UM guidelines will generally be applied to authorize or retrospectively review services
e. Describe the mechanisms that will be used to ensure consistent and appropriate application of approved criteria
f. How providers will be trained on UM guidelines, policies and procedures g. Process for monitoring and addressing over/under utilization at the provider level.
3. Please describe how you propose to transition these responsibilities from the CMHSPs to the offeror with minimum disruption.
I. Plan for Overall Transition and Timeline (Page Limit – 10 Pages, excluding attachments)
1. Provide a Plan and Timeline which shall include significant actions needed for undertaking this program.
2. Describe the start-up process the BH-MCO will utilize for the Program, including, but not limited, to:
a. identifying the local presence of the BH-MCO; b. hiring and training of staff and whether any preference will be given to the hiring of
displaced LRE or CMHSP staff; c. developing working knowledge of local services and resources; d. developing protocols/procedures; e. initiating and developing Provider contracts; f. ensuring continuity of care for Members receiving behavioral health services; and g. conducting outreach and education for Members, families, Providers, and other
organizations. 3. Define the processes which will be used to train and support Providers for claims submission
and adjudication. Include the BH-MCOs procedures for over-seeing and monitoring the Providers' compliance with all legal requirements for billing and collecting for services.
4. Describe the process for assuring on time and routine processing of claims at the start-up of the Program.
5. Describe the process for assuring an adequate flow of funds to the CMHSPs at the start-up of Program.
32
VI. Contractor Performance Measures The Contractor will be monitored for the following outcome measures. Within the Pricing
Template (Section VII.) Offerors are given the opportunity to propose risk arrangements associated with these measures.
Outcome Measures
Cardiovascular Health Screening for People with Schizophrenia/Bipolar Disorder who are Prescribed Antipsychotic Medications Use of Multiple Concurrent Antipsychotics in Children and Adolescents
Antidepressant Medication Management Acute Phase
Antidepressant Medication Management Continuation Phase
Adherence to Antipsychotic Medications for Individuals with Schizophrenia
Initiation of Alcohol and other Drug Dependence Treatment
Engagement of Alcohol and other Drug Dependence Treatment

33
VII. Criteria for Selection
SEC CRITERIA # Questions in Section
Points (5pt/
question) Section Weight
Total Possible Section Score
A Cover Letter Pass/Fail B Information About the Offeror Pass/Fail C Organizational Structure, Legal Standing & Litigation History Pass/Fail D Fiscal Solvency Pass/Fail E Relevant Managed Care Experience 11 55 2 110 F Offer's Proposed Organizational Structure 5 25 1 25 G Distribution of Funds & Risk Corridor Assumption 3 15 20 300 H Implementation of Managed Care Functions H.1 Member Services 9 45 1 45 H.2 Provider Network Services 11 55 1 55 H.3 Management Information Services 9 45 2 90 H.4 Financial Management Services 7 35 2 70 H.5 Claims Management Services 7 35 1.5 52.5 H.6 Quality Assurance/Performance Improvement Program 9 45 1 45 H.7 Service and Utilization Management 9 45 1.5 67.5
I Plan for Overall Transition & Timeline 11 55 1.5 82.5 VIII Pricing (scoring criteria described in template) 100
Bidder Oral Presentation (at the option of the LRE) 50
Criteria Scoring Summary Score Experience and Structure (E, F) 135 Managed Care Functions (H.1-H.7) 425 Transition and Timeline (I) 82.5 Finance and Pricing (G, VIII) 400 Overall Total Possible Score 1042.5

34
VIII. Pricing Proposal Offeror shall complete the grid below, making no marks other than entering the PMPM specific rates requested. Bids should reflect the extent to which services are covered in each of the benefit types listed below.
PRICING
Covered Services Administrative Services
At Risk: Medical and Administrative Costs
i. 1915(b) Services Described in the Michigan Medicaid Provider Manual: Mental Health – Substance Abuse Section (See Bidder Library)
ii. 1915(b)(3) Services All Medicaid services in included in the Described in the Michigan Medicaid Provider Manual: Mental Health – Substance Abuse Section (Behavioral Health and Intellectual Disability Supports and Services, page 303)
iii. 1915(c) Services Described in the Michigan Medicaid Provider Manual: Mental Health – Substance Abuse Section
iv. Autism Services under the iSPA and 1915(b) waiver as described in the Michigan Medicaid Provider Manual.
v. All Healthy Michigan Plan additional Substance Use Disorder and Supports described in the Medicaid Provider Manual.
i. Network Management
ii. Credentialing
iii. Claims Administration
iv. Customer Service
v. Utilization Management
vi. Grievances and Appeals
vii. Quality Management
Administrative Services PMPM = $_______ Covered Services PMPM = $_______ Total PMPM = $_______
1. Please include an attachment with offeror financial guarantees or risk related to performance standards outlined in Section VI. Contractor Performance Measures of this RFP.