laboratory diagnosis & treatment of parasitic diseases bradford mcgwire, md, phd division of...
TRANSCRIPT

Laboratory Diagnosis & Treatment of Parasitic Diseases
Bradford McGwire, MD, PhDDivision of Infectious DiseasesCenter for Microbial Interface [email protected]

Learning Objectives
Describe and differentiate the principles of laboratory diagnosis for parasitic diseases
Recognize general classes of anti-parasitic agents, describe their underlying mechanisms of action, predict their clinical side effect profiles, and accurately evaluate their role in the therapy of parasitic infections
Laboratory Methods for Diagnosing Parasitic Disease
Macroscopic examination
Microscopic examination Wet mountPermanent stainsStool concentrates
Serologic examination Antibody responseAntigen detection
Nucleic acid hybridization Probes and amplification techniquesDetectionIdentification
Culture
Animal inoculation
Xenodiagnosis
Body Sites, Specimen Collection & Diagnostic Procedures for Selected Parasitic Infections – Blood, bone marrow and CNS
Infecting Organism Specimen Options Collection Methods Diagnostic Procedure
Blood
Plasmodium spp., Babesia spp., filaria, Leishmania, Toxoplasma, Trypanosoma spp.
Whole blood, anticoagulated Venipuncture
Microscopic examination (Giemsa stain) or acridine orange fluorescent stain
Thin filmThick film
Blood concentration (filaria)Serology
AntibodyAntigen
PCR
Bone Marrow
Leishmania spp., Trypanosoma cruzi
Aspirate Sterile Microscopic examination (Giemsa stain)Culture
Serum Venipuncture Serology (antibody)
PCR
Central Nervous System
Acanthamoeba spp., Naegleria spp.,trypanosomes,Toxoplasma gondii
Spinal fluid Sterile
Microscopic examination Wet mountPermanent stain
CultureSerology (antibody)PCR
Serum Venipuncture

Blood Films: “Thin” & “Thick” Preparations
This Giemsa stained slide depicts an example of properly prepared thick and thin film blood smears to be examined. Gustav Giemsa (1867 – 1948) was by trade both a chemist and a pharmacist. It was in 1902 that he developed a staining technique that was useful in the identification of malarial parasites such as Plasmodium falciparum.

“Thin” Blood Films: P. vivax & P. falciparum
These thin film Giemsa stained micrographs show ring-form Plasmodium vivax and P. falciparum trophozoites. As the parasite increases in size, the ring morphology of the early trophozoite disappears, and becomes what is referred to as a mature trophozoite, which undergoes further transformation maturing into a schizont.
CDC/ Steven Glenn, Laboratory & Consultation Division

“Thick” Blood Film: P. malariae & P. falciparum
This thick film Giemsa stained micrograph reveals a mixed P. falciparum and P. malariae parasitic infection. In the field of view note the presence of a growing Plasmodium malariae trophozoite (Lt), and a Plasmodium falciparum gametocyte (Rt), indicative of a mixed Plasmodium spp. infection.
CDC/ Steven Glenn, Laboratory & Consultation Division
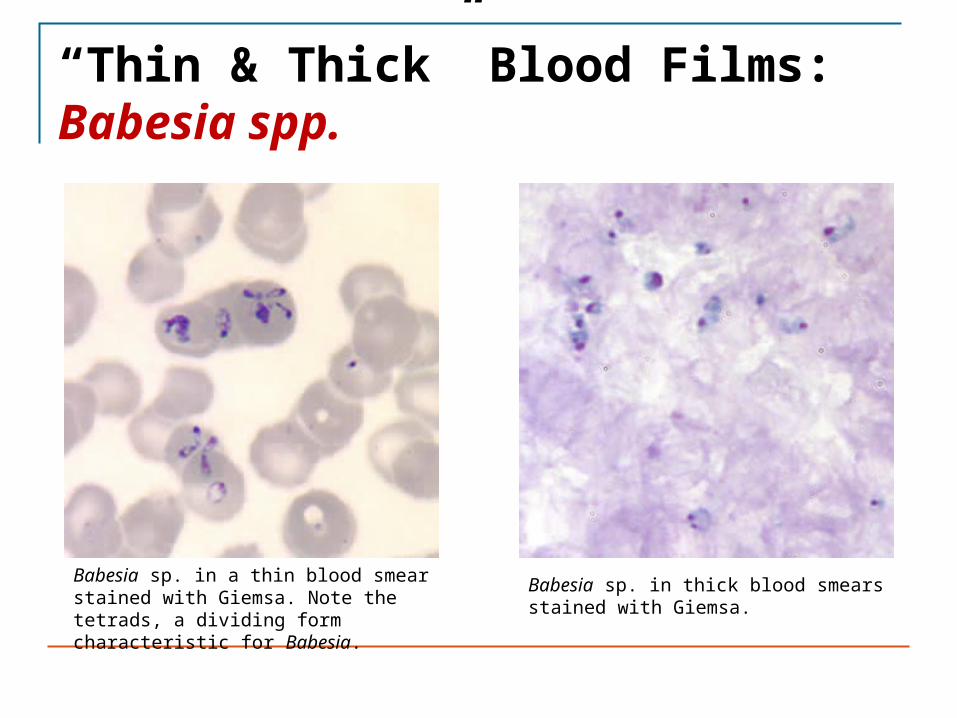
“Thin & Thick” Blood Films: Babesia spp.
Babesia sp. in a thin blood smear stained with Giemsa. Note the tetrads, a dividing form characteristic for Babesia.
Babesia sp. in thick blood smears stained with Giemsa.

“Thick” Blood Film: Wuchecheria bancrofti
This is a micrograph of a Wuchereria bancrofti microfilaria in a thick blood smear using Giemsa stain technique. W. bancrofti, the most common filarial parasite in humans, is one of the causative agents for lymphatic filariasis. Lymphatic filariasis affects an estimated 120 million people in tropical areas of the world.
CDC/Dr. Mae Melvin
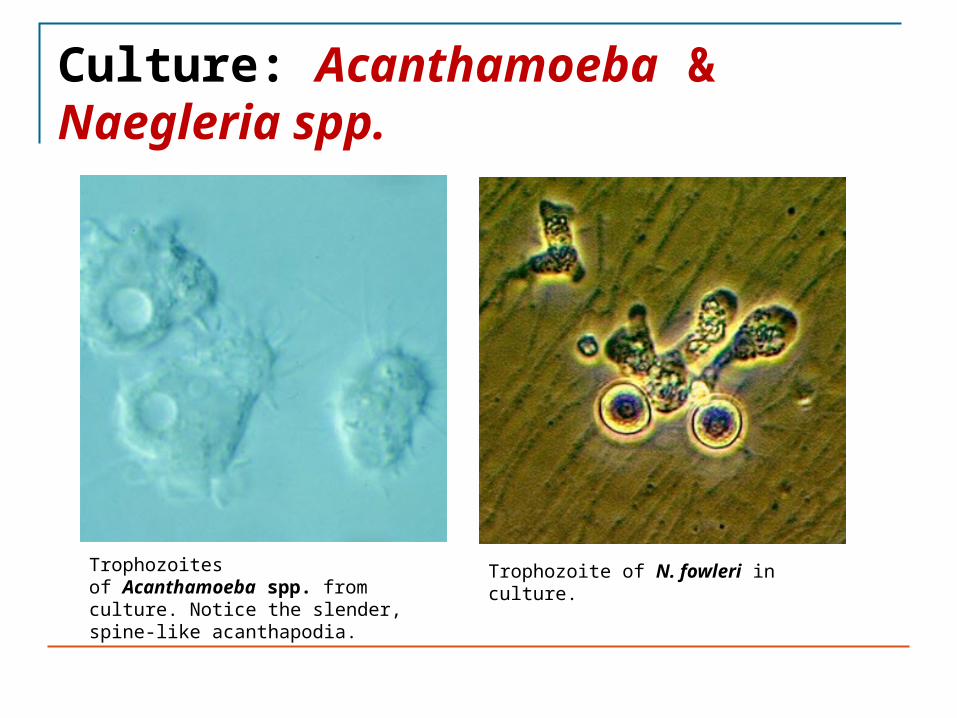
Culture: Acanthamoeba & Naegleria spp.
Trophozoites of Acanthamoeba spp. from culture. Notice the slender, spine-like acanthapodia.
Trophozoite of N. fowleri in culture.
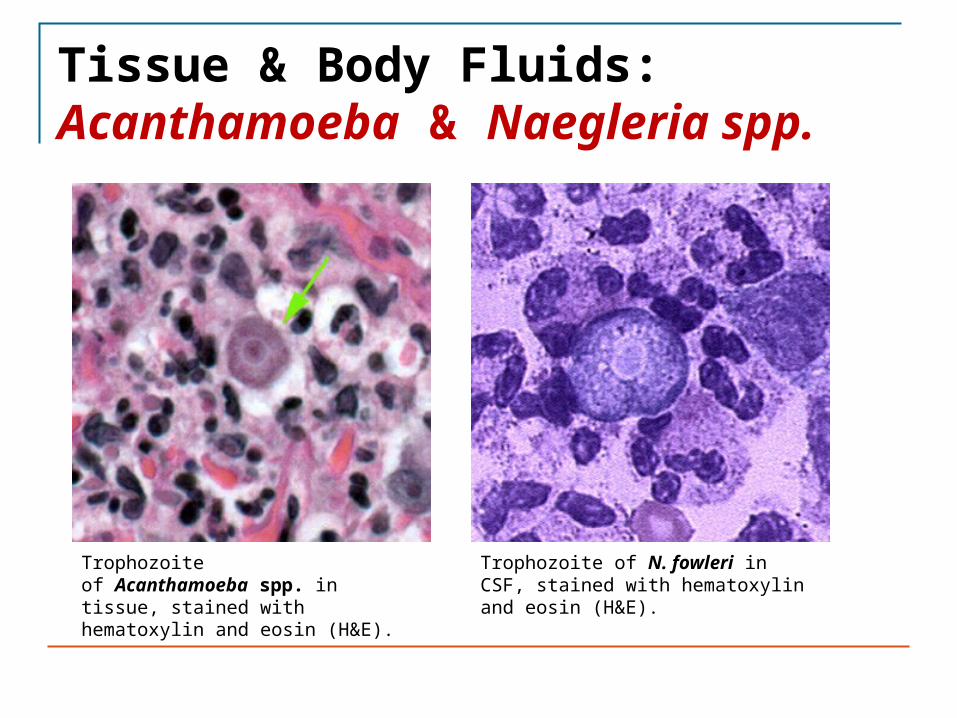
Tissue & Body Fluids: Acanthamoeba & Naegleria spp.
Trophozoite of Acanthamoeba spp. in tissue, stained with hematoxylin and eosin (H&E).
Trophozoite of N. fowleri in CSF, stained with hematoxylin and eosin (H&E).

Cutaneous Ulcers
Leishmania spp., Acanthamoeba spp.
Aspirate Sterile plus smears Microscopic examination (Giemsa stain)CultureSerology (antibody)PCR
BiopsySterile, nonsterile to
histology
Serum Venipuncture
Eye
Acanthamoeba spp., Loa loa Microsporidia
Corneal scrapingsSterile saline, air-dried
smear
Microscopic examination Wet mountPermanent stain
Corneal biopsy Sterile saline Culture
Infecting Organism Specimen Options Collection Methods Diagnostic Procedure
Body Sites, Specimen Collection & Diagnostic Proceduresfor Selected Parasitic Infections

Tissue & Corneal Scraping: Leishmania spp. & Acanthamoeba spp.
Leishmania spp. amastigotes in a Giemsa-stained tissue scraping.
Trophozoites of Acanthamoeba spp. in a corneal scraping, stained with H&E.
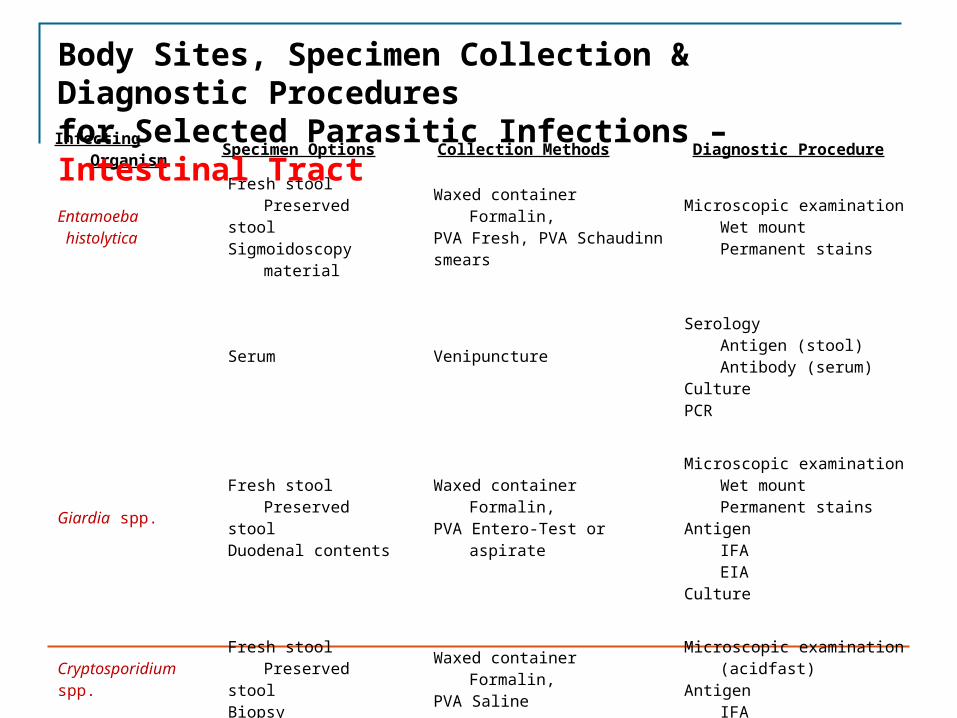
Entamoeba histolytica
Fresh stool Preserved stool Sigmoidoscopy material
Waxed container Formalin, PVA Fresh, PVA Schaudinn smears
Microscopic examination Wet mountPermanent stains
Serum VenipunctureSerology
Antigen (stool)Antibody (serum)
CulturePCR
Giardia spp. Fresh stool Preserved stool Duodenal contents
Waxed container Formalin, PVA Entero-Test or aspirate
Microscopic examination Wet mountPermanent stains
Antigen IFAEIA
Culture
Cryptosporidium spp.
Fresh stool Preserved stool Biopsy
Waxed container Formalin, PVA Saline
Microscopic examination (acidfast)Antigen
IFAEIA
Infecting Organism Specimen Options Collection Methods Diagnostic Procedure
Body Sites, Specimen Collection & Diagnostic Proceduresfor Selected Parasitic Infections – Intestinal Tract

MicrosporidiaFresh stool Preserved stool
Duodenal contents Biopsy
Waxed container Formalin, PVA Aspirate Saline
Microscopic Giemsa stainGram stainChromotrope stain
Pinworm Anal impression smear Cellophane tape Macroscopic examinationMicroscopic examination(eggs)
Helminths Fresh stool Preserved stool Waxed container Formalin, PVA Macroscopic examination(adults)Microscopic examination(larvae and eggs)
Infecting Organism Specimen Options Collection Methods Diagnostic Procedure
Body Sites, Specimen Collection & Diagnostic Proceduresfor Selected Parasitic Infections – Intestinal Tract
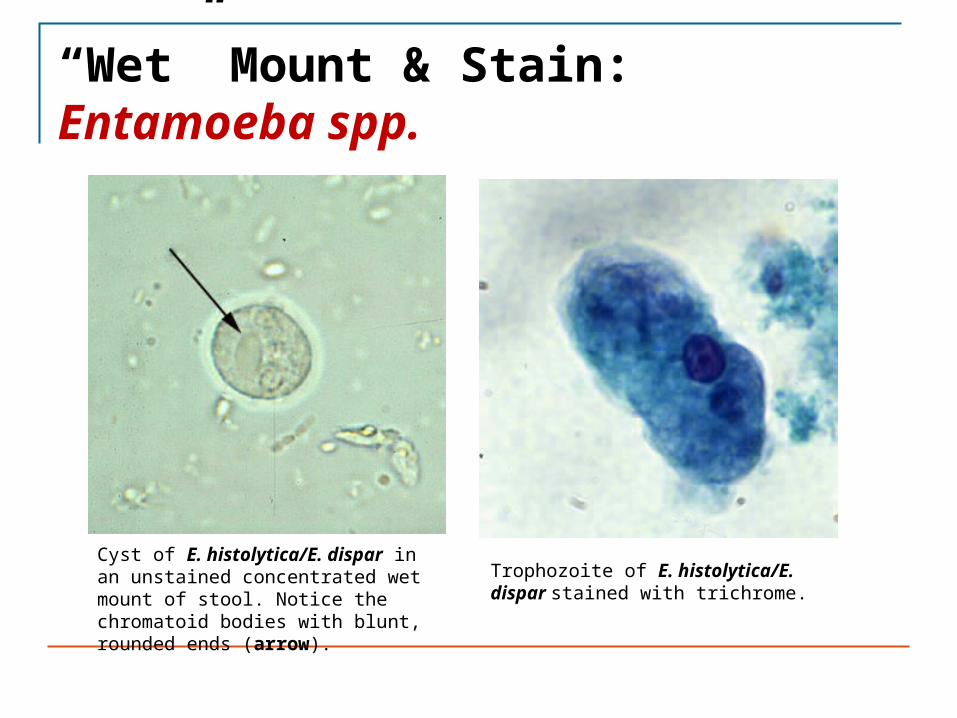
“Wet” Mount & Stain: Entamoeba spp.
Cyst of E. histolytica/E. dispar in an unstained concentrated wet mount of stool. Notice the chromatoid bodies with blunt, rounded ends (arrow).
Trophozoite of E. histolytica/E. dispar stained with trichrome.

Cellulose Tape & “Wet” Mount: Enterobius vermicularis (Pinworm)
Eggs of E. vermicularis in a cellulose-tape preparation. Eggs of E. vermicularis in a wet mount.

Macroscopic Examination & “Wet” Mount: Ascaris lumbricoides
Adult female A. lumbricoides. Unfertilized egg of A. lumbricoides in an unstained wet mount of stool.
Infecting Organism Specimen Options Collection Methods Diagnostic Procedure
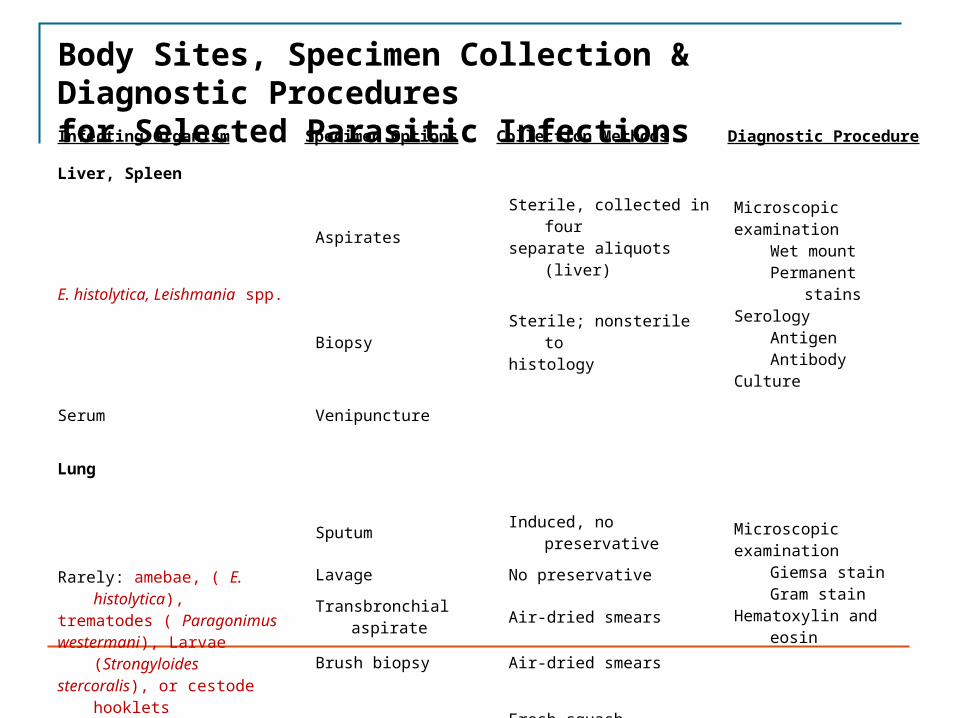
Liver, Spleen
E. histolytica, Leishmania spp.
Aspirates Sterile, collected in four separate aliquots (liver) Microscopic
examination Wet mountPermanent stains
Serology AntigenAntibody
Culture
Biopsy Sterile; nonsterile to histology
Serum Venipuncture
Lung
Rarely: amebae, ( E. histolytica), trematodes ( Paragonimus westermani), Larvae (Strongyloides stercoralis), or cestode hooklets
Sputum Induced, no preservative Microscopic examination
Giemsa stainGram stain
Hematoxylin and eosin
Lavage No preservative
Transbronchial aspirate Air-dried smears
Brush biopsy Air-dried smears
Open lung biopsy Fresh squash preparation; nonsterile to histology
Body Sites, Specimen Collection & Diagnostic Proceduresfor Selected Parasitic Infections
Infecting Organism Specimen Options Collection Methods Diagnostic Procedure
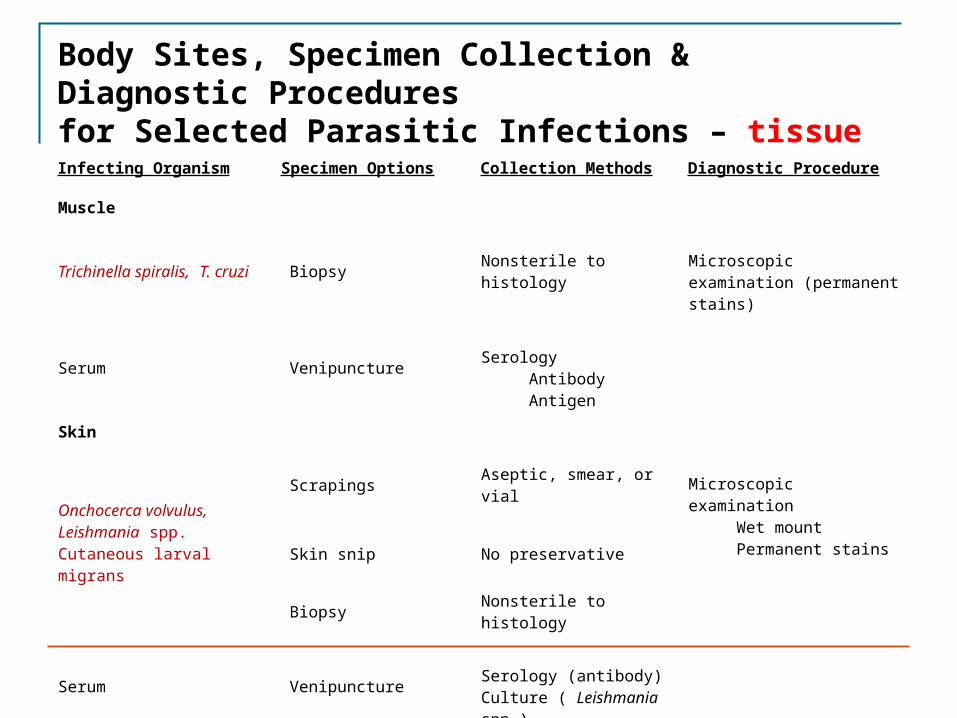
Muscle
Trichinella spiralis, T. cruzi Biopsy Nonsterile to histology Microscopic examination (permanent stains)
Serum Venipuncture Serology AntibodyAntigen
Skin
Onchocerca volvulus, Leishmania spp. Cutaneous larval migrans
Scrapings Aseptic, smear, or vialMicroscopic examination
Wet mountPermanent stains
Skin snip No preservative
Biopsy Nonsterile to histology
Serum Venipuncture Serology (antibody)Culture ( Leishmania spp.)
Body Sites, Specimen Collection & Diagnostic Proceduresfor Selected Parasitic Infections – tissue
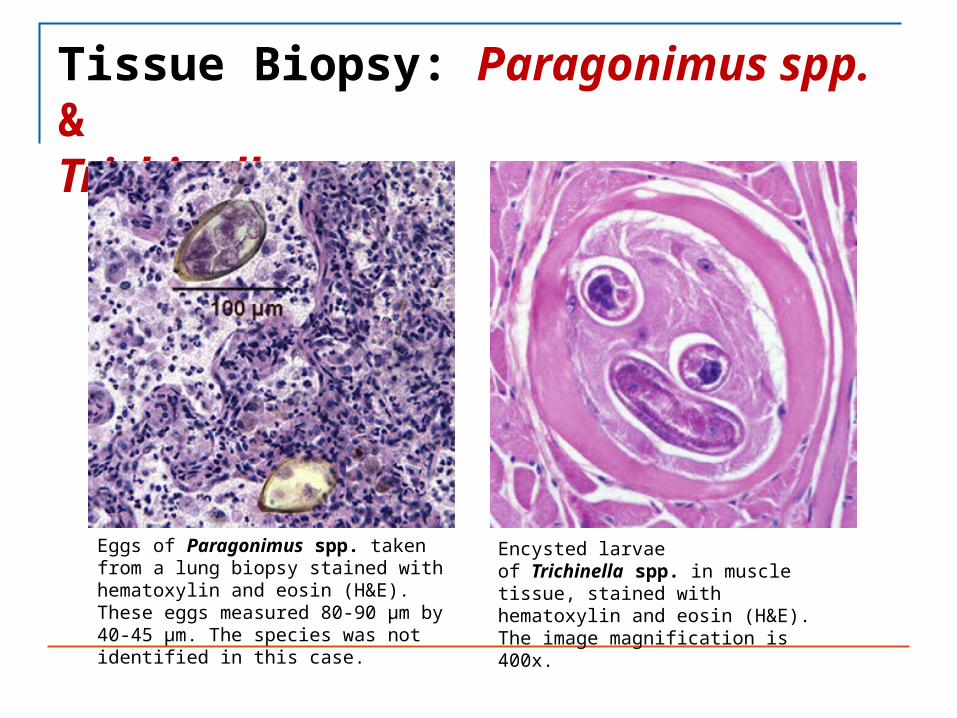
Tissue Biopsy: Paragonimus spp. & Trichinella spp.
Eggs of Paragonimus spp. taken from a lung biopsy stained with hematoxylin and eosin (H&E). These eggs measured 80-90 µm by 40-45 µm. The species was not identified in this case.
Encysted larvae of Trichinella spp. in muscle tissue, stained with hematoxylin and eosin (H&E). The image magnification is 400x.

Infecting Organism Specimen Options Collection Methods Diagnostic Procedure
Urogenital System
Trichomonas vaginalis
Vaginal discharge Saline swab, culture medium Microscopic examination Wet mountPermanent stains
Antigen (IFA)CultureSerology (antibody)Nucleic acid probe
Prostatic secretions Saline swab, culture medium
Urethral discharge Saline swab, culture medium
Schistosoma haematobium Urine Single unpreserved specimen Microscopic examination
Biopsy Nonsterile to histology
Body Sites, Specimen Collection & Diagnostic Proceduresfor Selected Parasitic Infections – urogenital tract

“Wet” Mount: Trichomonas vaginalis & Schistosoma spp.
Trophozoite of T. vaginalis in a vaginal smear, stained with Giemsa.
Egg of S. haematobium in a wet mount of urine concentrates, showing the characteristic terminal spine.

Organism Gene Target Sensitivity (%) Comment
Plasmodium vivax Circumsporozoite gene 91 – 96 Dried blood-spotted filter paper samples are used.
Leishmania species kDNA minicircle sequence 87 – 100 Results are compared to culture and microscopy of biopsy specimens.
Trypanosoma cruzi kDNA minicircle sequence 100Results are compared to serology and xenodiagnosis of blood samples.
Toxoplasma gondii B1 repetitive gene P30 major surface antigen Recombinant DNA sequences
46 – 99PCR of BAL, blood, CSF, and amniotic fluid show great potential for diagnosis of toxoplasmosis.
Entamoeba histolytica P145 tandem repeat sequence SSU rRNA 96 – >90
Results are compared to microscopic diagnosis of stool samples. Test may distinguish pathogenic from nonpathogenic strains.
Examples of Techniques for Detection of Parasitic Infections Based on PCR Analysis
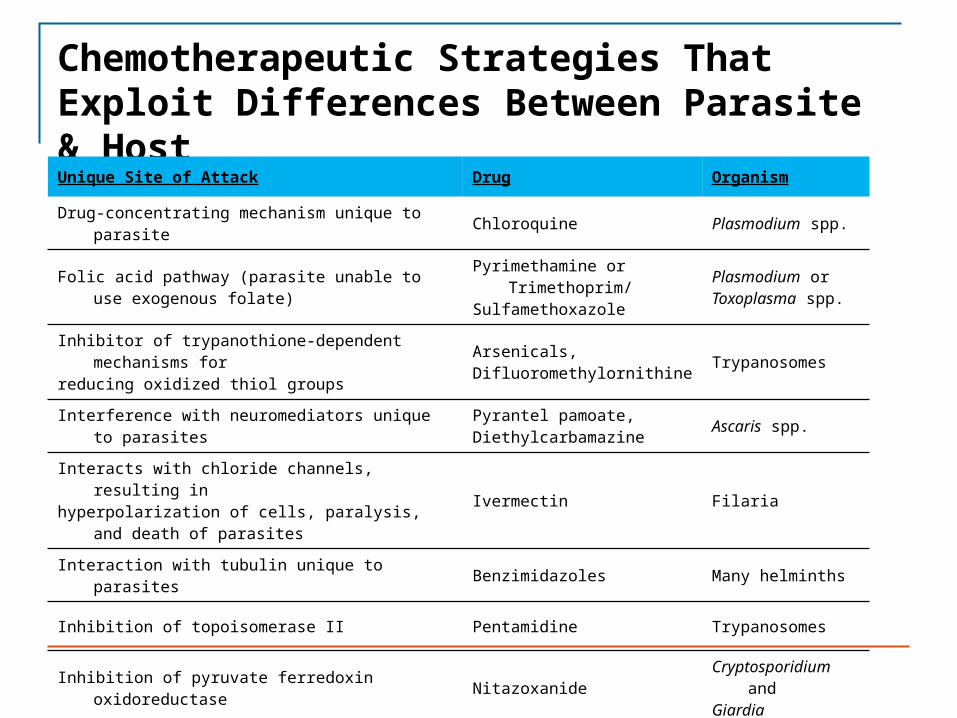
Chemotherapeutic Strategies That Exploit Differences Between Parasite & Host
Unique Site of Attack Drug Organism
Drug-concentrating mechanism unique to parasite Chloroquine Plasmodium spp.
Folic acid pathway (parasite unable to use exogenous folate) Pyrimethamine or Trimethoprim/Sulfamethoxazole
Plasmodium or Toxoplasma spp.
Inhibitor of trypanothione-dependent mechanisms for reducing oxidized thiol groups
Arsenicals,Difluoromethylornithine Trypanosomes
Interference with neuromediators unique to parasites Pyrantel pamoate,Diethylcarbamazine Ascaris spp.
Interacts with chloride channels, resulting inhyperpolarization of cells, paralysis, and death of parasites Ivermectin Filaria
Interaction with tubulin unique to parasites Benzimidazoles Many helminths
Inhibition of topoisomerase II Pentamidine Trypanosomes
Inhibition of pyruvate ferredoxin oxidoreductase Nitazoxanide Cryptosporidium and Giardia

Mechanisms of Action & Clinical Indications for the Major Anti-parasitic Agents – Anti-protozoal Agents
Drug Class Mechanism of Action Examples Clinical Indications
Heavy metals: arsenical and antimonials
• Inactivate sulfhydryl groups.• Disrupt glycolysis.
Melarsoprol, sodium stibogluconate, meglumine antimonate
Trypanosomiasis, Leishmaniasis
Aminoquinoline analogues
• Accumulate in parasitized cells.
• Interfere with DNA replication.
• Bind to ferriprotoporphyrin IX.
• Raise intravesicular pH.• Interfere with hemoglobin
digestion
Chloroquine, mefloquine, quinine, primaquine, halofantrine, lumafantrine
Malaria prophylaxis and therapy Radical cure (exoerythrocytic-primaquine only)
Folic acid antagonists• Inhibit dihydropteroate
synthetase and dihydrofolate reductase
Sulfonamides, pyrimethamine,trimethoprim
Toxoplasmosis, malaria, cyclosporiasis
Inhibitors of protein synthesis
• Block peptide synthesis at levelof ribosome
Clindamycin, spiramycin,paromomycin, tetracycline, doxycycline
Malaria, babesiosis, amebiasis, cryptosporidiosis, leishmaniasis, onchocerciasis
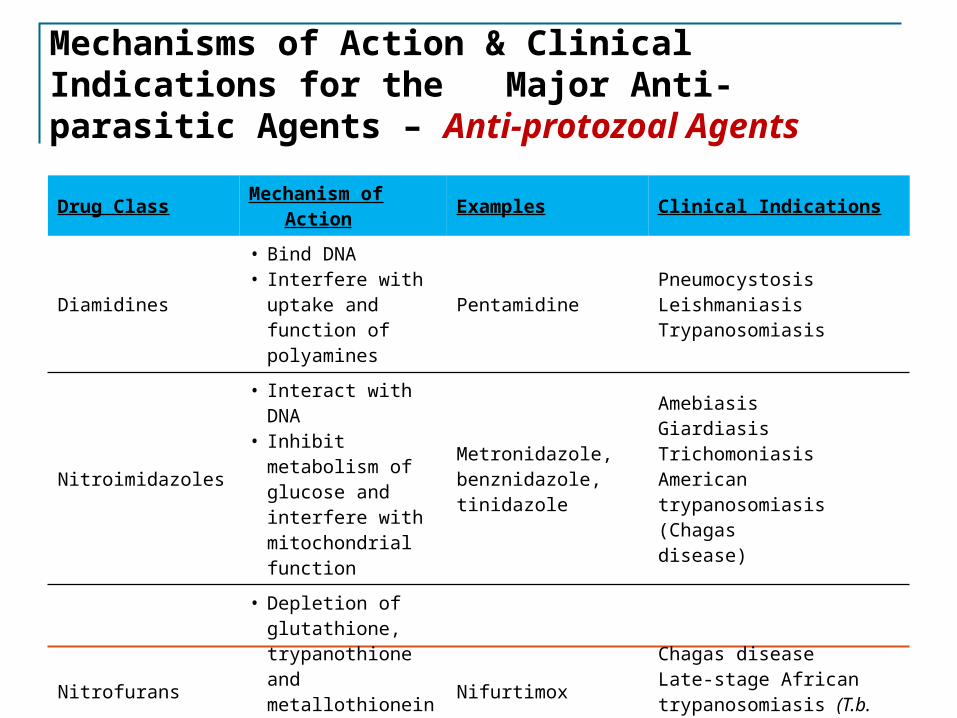
Mechanisms of Action & Clinical Indications for the Major Anti-parasitic Agents – Anti-protozoal Agents
Drug Class Mechanism of Action Examples Clinical Indications
Diamidines• Bind DNA• Interfere with uptake
and function of polyamines
PentamidinePneumocystosisLeishmaniasisTrypanosomiasis
Nitroimidazoles
• Interact with DNA • Inhibit metabolism of
glucose and interfere with mitochondrial function
Metronidazole, benznidazole,tinidazole
AmebiasisGiardiasisTrichomoniasis American trypanosomiasis (Chagas disease)
Nitrofurans
• Depletion of glutathione, trypanothione and metallothionein.
• Oxidative stress.
NifurtimoxChagas diseaseLate-stage African trypanosomiasis (T.b. gambiense)

Mechanisms of Action & Clinical Indications for the Major Anti-parasitic Agents – Anti-protozoal Agents
Drug Class Mechanism of Action Examples Clinical Indications
Sesquiterpenes
• React with heme, causing free-radical damage to parasite membranes (artemisinins).
• Inhibit methionine aminopeptidase type 2 (fumagillin).
• Inhibit RNA and DNA synthesis (fumagillin).
Artemisinin, artemether, artesunate Fumagillin
Malaria (artemisinins) Schistosomiasis Gastrointestinal and ocular microsporidiosis (fumagillin)
Hydroxynaphthoquinone (Atovaquone)+ anti-folate (Proguanil) combination
• Atovaquone Inhibition of electron transport system in mitochondria of parasites, thus blocking nucleic acid synthesis and inhibiting replication
• Proguanil Selective inhibition of plasmodial dihydrofolate reductase. Lowers effective concentration at which atovaquone causes collapse of mitochondrial membrane potential.
Malarone (Atovaquone-Proguanil)
Malaria prophylaxis and therapy(P. falciparum – active against all stages of development; P. vivax and P. ovale – active against erythrocytic stages)
Ornithine analogue • Inhibits ornithine decarboxylase.• Interferes with polyamine metabolism Difluoromethylornithine African
trypanosomiasis

Mechanisms of Action & Clinical Indications for the Major Anti-parasitic Agents – Anti-protozoal Agents
Drug Class Mechanism of Action Examples Clinical Indications
Phosphocholine analogue
• Disruption of lipid metabolism Miltefosine Leishmaniasis
Acetanilide • Unknown Diloxanide furoate Intestinal amebiasis
Sulfated naphthylamine
• Inhibits sn-glycerol-3- phosphate oxidase and glycerol-3-phosphate dehydrogenase causing decreased ATP synthesis
Suramin African trypanosomiasis
Thiazolides• Inhibit pyruvate-
ferredoxin oxidoreductase
Nitazoxanide Cryptosporidiosis,Giardiasis

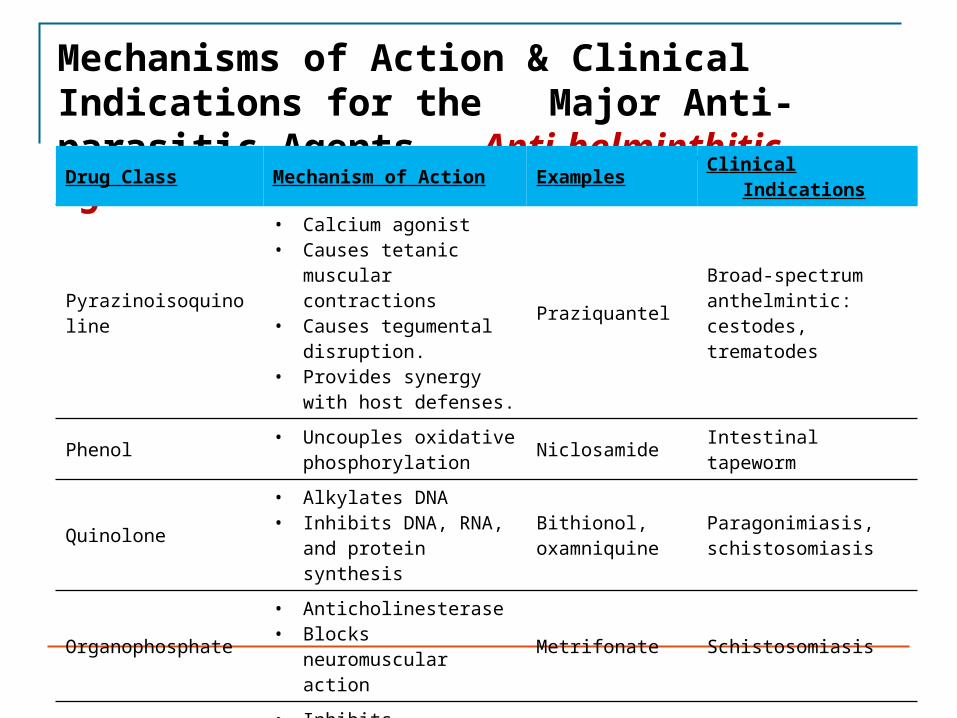
Mechanisms of Action & Clinical Indications for the Major Anti-parasitic Agents – Anti-helminthitic Agents
Drug Class Mechanism of Action Examples Clinical Indications
Benzimidazoles
• Inhibit fumarate reductase.• Inhibit glucose transport.• Disrupt microtubular
function.
Mebendazole,thiabendazole,albendazole
Broad-spectrum anthelmintic: nematodes, cestodes
Tetrahydropyrimidine• Blocks neuromuscular
action• Inhibits fumarate reductase
Pyrantel pamoate Ascariasis, pinworm, hookworm
Piperazines• Cause neuromuscular
paralysis• Stimulates phagocytic cells.
Piperazine,diethylcarbamazine
Ascariasis and pinworm infections
Avermectins• Block neuromuscular action• Hyperpolarize nerve and
muscle cells• Inhibit filarial reproduction
IvermectinFilarial infections, strongyloidiasis, ascariasis, scabies

MOA – Praziquantel
Before exposure to praziquantel, the schistosome is capable of avoiding the numerous antibodies directed toward surface and internally located antigens. A, Cross-section of the dorsal surface of a normal male schistosome. Within 1 to 2 seconds after exposure to praziquantel, the muscles of the schistosome contract because of a drug-induced influx of calcium ions into the schistosome tegument. B, The change in permeability of the schistosome surface toward external ions initiates the appearance of small holes and balloon-like structures, making the parasite vulnerable to antibody-mediated adherence of host leukocytes that kill the helminth.
Mechanisms of Action & Clinical Indications for the Major Anti-parasitic Agents – Anti-helminthitic AgentsDrug Class Mechanism of Action Examples Clinical Indications
Pyrazinoisoquinoline
• Calcium agonist • Causes tetanic muscular
contractions • Causes tegumental
disruption. • Provides synergy with host
defenses.
PraziquantelBroad-spectrum anthelmintic:cestodes, trematodes
Phenol • Uncouples oxidative phosphorylation Niclosamide Intestinal tapeworm
Quinolone• Alkylates DNA• Inhibits DNA, RNA, and
protein synthesis Bithionol, oxamniquine
Paragonimiasis, schistosomiasis
Organophosphate• Anticholinesterase • Blocks neuromuscular
action Metrifonate Schistosomiasis
Sulfated naphthylamidine
• Inhibits glycerophosphate oxidase and dehydrogenase Suramin Onchocerciasis
Lab Diagnosis and Treatment of Parasitic Disease Quiz
Thank you for completing this module
• I hope that I was able to teach the subject clearly.• If you have any questions, write to me: [email protected]
References
Primary Reference Source: -Medical Microbiology, 7th Ed. Murray, Rosenthal & Pfaller; Chapter 76, pages 715 – 721; Chapter 77, pages 722 – 725; Chapter 78, pages 726 – 727; Chapter 79, pages 728 – 736; Chapter 80, pages 737 – 744; Chapter 81, pages 745 – 758; Chapter 82, pages 759 – 777; Chapter 83, pages 778 – 795; Chapter 84, pages 796 – 805; Chapter 85, pages 806 – 816; Chapter 86, pages 823 – 824 (focus on Scabies); Chapter 80, pages 737 – 744.
Survey
We would appreciate your feedback on this module. Click on the button below to complete a brief survey. Your responses and comments will be shared with the module’s author, the LSI EdTech team, and LSI curriculum leaders. We will use your feedback to improve future versions of the module.
The survey is both optional and anonymous and should take less than 5 minutes to complete.
Survey