la terapia nel «setting» adiuvante e neoadiuvante 6 maggio...gemcitabine vs 5-fu before and after...
TRANSCRIPT

Laterapianel«setting»adiuvanteeneoadiuvante
CarloBaroneDirettoreUOCOncologiaMedicaUniversitàCattolicadelS.Cuore
Summary
• Introduction• Adjuvant therapy
– Trialsonchemoradiation– Trialsonchemotherapywithout chemoradiation
• Meta-analyses ofadjuvant therapy• Neoadjuvant therapy• Recommendations• Futuredirections

PancreaticCancerStageDistributionandSurvivalintheUnitedStates
• Relapseoccursinapproximately80%- 85%ofpatientsafterresection,underscoringtheimportanceofadjuvanttherapy4-7
– Amargin-freeresection(R0)isassociatedwithbettersurvivaloutcomescomparedwithinvolvedmargins8,9
– Marginstatushasalsobeenshowntobeassociatedwiththeincidenceoflocalrecurrence,butnotrecurrencetolymphnodes ordistantorgans10
1. SEER Stat Fact Sheets: Pancreas. http://seer.cancer.gov /statfac ts/html/pancreas .html. Accessed September 24, 2015. 2. NCCN Clinical Practice Guidelines in Oncology, V2.2015. 3. Vincent A, et al. Lancet 2011; 4. Liao WC, et al. Lancet Oncol 2013; 5. Siegel R, et al. CA Cancer J Clin 2013; 6. Oettle H, et al. JAMA 2007; 7. Sener SF, et al. J Am Coll Surg 1999; 8. Bilimoria KY, et al. J Am Coll Surg 2008; 9. Winter JM, et al. J Gastrointest Surg 2006; 10. Sugiura T, et al. Surgery 2013.
27,1
10,7
2,44,4
051015202530
Localized Regional Distant Unstaged
Prop
ortio
n of
Su
rviv
al, %
5-YearRelativeSurvival1 • Surgery is the only potentially curative treatment option for pancreatic cancer2
• At the time of diagnosis ≈ 10% of patients have resectable(Stages 0-IIB) and ≈ 10% have borderline resectable (Stage III) disease3

ClinicalClassificationofPancreaticCancer
1. NCCN Clinical Practice Guidelines in Oncology, V2.2015. 2. Vincent A, et al. Lancet 2011.
Classification1,2 Stage Features Resectable(≈ 10%)
0, IA, IB, IIA, IIB
• No distant metastases• No evidence of SMV or portal vein abutment, distortion, tumor
thrombus, or venous encasement• Clear fat planes around the celiac axis, hepatic artery, and SMA
Borderline resectable(≈ 10%)
III • No distant metastases• SMA encasement < 180°; SMV/portal impingement• Short-segment SMV occlusion • Celiac encasement < 180° (tail)• Abutment/encasement of hepatic artery
LAPC(≈ 30%)
III • No distant metastases• SMA encasement > 180°• SMV/portal vein occlusion• Any celiac abutment (head) or celiac encasement > 180°
(body/tail)• Aortic invasion or encasement; lfn mts beyond field of resection
MPC (≈ 60%) IV • Presence of metastatic disease in distant organs

Chemoradiation vsObservation:GITSG
• Ofthe21treatedpatients,3(14%)hadsevereleukopenia• Nocasesoftreatment-relateddeathsorlife-threateningadverseevents
Kalser MH, et al. Arch Surg 1985.
Efficacy Observation 5-FU + Radiation P ValueMedian DFS, months 9 11 0.01Median OS, months 11 20 0.03

Chemoradiation vsObservation:EORTC40891
• Thirty-fivepatients(44%)received3daysof5-FUinthesecondcourseduetograde1or2acutetoxicity• Nograde≥3leukopenia orthrombocytopeniawasobserved• Theonlymajortoxicitywas1caseofduodenal ulcer2
a Periampullary = tumor in the distal common bile duct, papilla of Vater, or duodenum.b The course of therapy weeks 5 - 6 consisted of 0 (if grade ≥ 3 toxicity), 3 (if grade 1/2 toxicity), or 5 (if no toxicity) days of 5-FU
Efficacy2 Observation 5-FU + Radiation HR P ValueMedian PFS, years 1.2 1.5 0.94 0.663
Median OS, years (primary endpoint) 1.6 1.8 0.91 0.540
1. Klinkenbijl JH, et al. Ann Surg 1999; 2. Smeenk HG, et al. Ann Surg 2007.
**mg/kg

CRTvsCTvsCRT→CTvsObservation:ESPAC-1(2×2FactorialDesign)
Grade≥3AEs:hematologic(2patientsintheCT-alonegroupand5intheCRT→CTgroup),stomatitis(4intheCT-alonegroupand5intheCRT→CTgroup),diarrhea(2intheCT-alonegroupand4intheCRT→CTgroup)
1. Neoptolemos JP, et al. Lancet 2001; 2. Neoptolemos JP, et al. N Engl J Med 2004.
EfficacyRandom Assignment to CRT Random Assignment to CT
CRT (n = 145) No CRT (n = 144) CT (n = 147) No CT (n = 142)Median OS, months(primary endpoint) 15.9 17.9 20.1 15.5
HR (95% CI) 1.28 (0.99 - 1.66) 0.71 (0.55 - 0.92)P value 0.05 0.009

TheESPACstudy withafactorial design
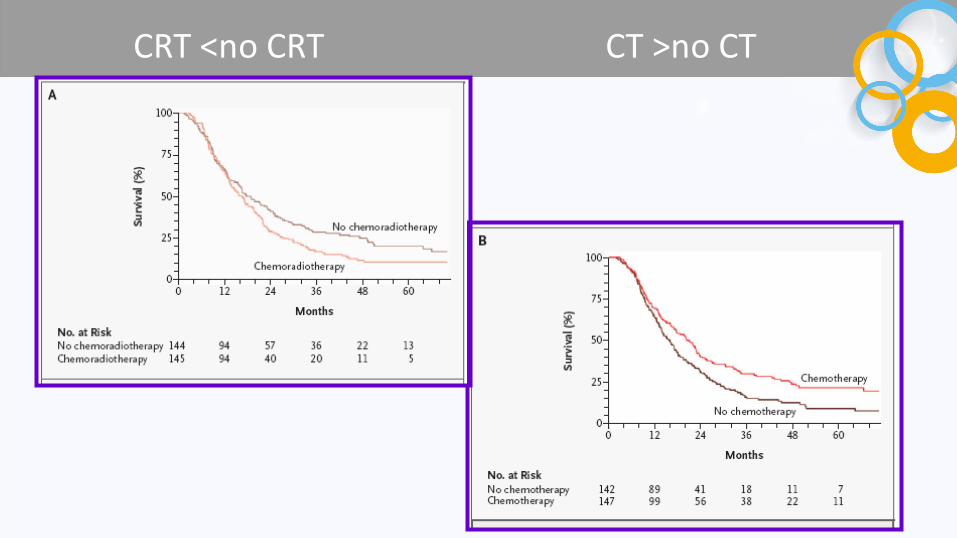
CRT<noCRT CT>noCT

Gemcitabinevs5-FUBeforeandAfterCRT:RTOG97041,2
• Grade4hematologictoxicitywasmorecommoninthegemcitabinearm(14%vs1%;P<0.001);ratesofnonhematologic toxicityweresimilar betweenthe2arms;1patientinthegemcitabinearmdiedofnonneutropenic infection1
a The co-primary endpoints were OS for all patients and OS for patients with tumors of the pancreatic head
Efficacy2,a 5-FU Gemcitabine HR P ValueMedian OS, months NR NR 0.933 0.51
Patients with tumors of the pancreatic head
n = 20117.1
n = 18720.5 0.838 0.12
1. Regine WF, et al. JAMA. 2008;299:1019-1026. 2. Regine WF, et al. Ann Surg Oncol. 2011;18:1319-1326.

TheRTOGtrial:CRTwithFUorGEM?
Surgery
FU ci x 3 w
RT 50.4 Gy + FU ci
FU ci x 3 m(4 + 4 w)
GMC 1000/w x 3
RT 50.4 Gy + FU ci
GMC 1000/w x 3 m
270 pts 268 pts
SM 20.5 vs 17 mSM 18.8 vs 17 m
Nosignificant improvementwithGEMinpancreatic headcancer
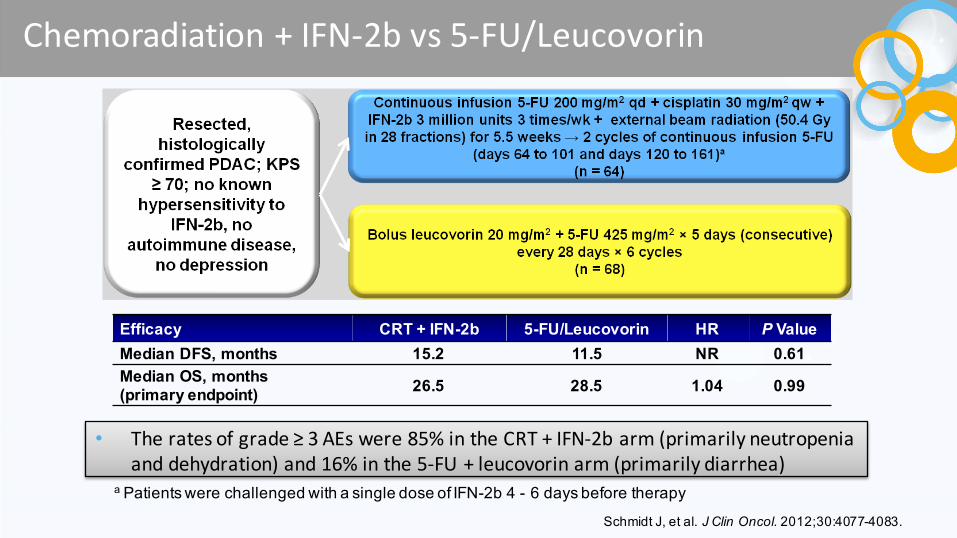
Chemoradiation +IFN-2bvs5-FU/Leucovorin
• Theratesofgrade≥3AEswere85%intheCRT+IFN-2barm(primarilyneutropeniaanddehydration)and16%inthe5-FU+leucovorin arm(primarilydiarrhea)
a Patients were challenged with a single dose of IFN-2b 4 - 6 days before therapy
Efficacy CRT + IFN-2b 5-FU/Leucovorin HR P ValueMedian DFS, months 15.2 11.5 NR 0.61Median OS, months(primary endpoint) 26.5 28.5 1.04 0.99
Schmidt J, et al. J Clin Oncol. 2012;30:4077-4083.

GemcitabinevsObservation:CONKO-0011,2
• Twenty-sixpatients(14%)inthegemcitabinearmand15(8%)observationarmexperiencedaseriousadverseevent;5ofthesepatients(19%)hadeventsconsideredtobegemcitabine-related1
Efficacy Observation Gemcitabine HR P ValueMedian DFS, months(primary endpoint) 6.7 13.4 0.55 < 0.001
Median OS, months 20.2 22.8 0.76 0.01
1. Oettle H, et al. JAMA. 2007;297:267-277. 2. Oettle H, et al. JAMA. 2013;310(14):1473-1481.
qw 3/4 = the first 3 of 4 weeks

CONKO– 001trial
13.4mvs6.7mHR0.55(0.44-0.69)
22.8mvs20.2mHR0.76(0.61-0.95)

GemcitabinevsObservation:JSAP-2
• Inthegemcitabinearm,grade≥3leukopeniaandneutropeniaoccurredin25%and70%ofpatient,respectively; nograde≥3AEswerereportedintheobservationgroup
• 2patientsinthegemcitabinearmand1patientintheobservationarmdiedduringtreatment
a Except intraoperative radiotherapy
Efficacy Observation Gemcitabine HR P ValueMedian DFS, months 5.0 11.4 0.60 0.01Median OS, months(primary endpoint) 18.4 22.3 0.77 0.19
Ueno H, et al. Br J Cancer. 2009;101:908-915.

TheJASP-2trial

GemcitabinePlusErlotinib vsGemcitabine:CONKO-005
• Moregrade3/4rashwithgemcitabine+erlotinib vsgemcitabine(7%vs<1%;P <0.001)
a Adjuvant therapy started within 8 weeks after surgical resection
Efficacy Gemcitabine + Erlotinib Gemcitabine HR P Value
Median DFS, months 11.6 11.6 0.89 0.291Median OS, months (primary endpoint) 24.6 26.5 0.90 0.406
Sinn M, et al, ASCO 2015 [Abstract 4007]

5-FUPlusLeucovorin vsGemcitabine:ESPAC-3v2a,1,2
• Differencesingrade≥3toxicityforthe5-FUandgemcitabinearmsincluded,respectively,leukopenia(6%vs10%;P =0.01),thrombocytopenia (0%vs1.5%;P =0.003),stomatitis(10%vs0%;P <0.001),anddiarrhea(13%vs2%;P <0.001)
a Originally a 3-arm trial, but the observation arm was stopped after the results of ESPAC-1 supported CT over observation.
Efficacy 5-FU/leucovorin Gemcitabine HR P ValueMedian PFS, months 14.1 14.3 0.96 0.53Median OS, months(primary endpoint) 23.0 23.6 0.94 0.39
1. Neoptolemos JP, et al. JAMA. 2010;304:1073-1081. 2. Neoptolemos JP, et al. Lancet. 2001;358:1576-1585.

Gemcitabine vsS1:JASPAC-01trial
Resectedhistologically
confirmed PDAC;noneoadjuvantchemotherapy orradiotherapy;PS0-2;adequate bonemarrow function
S180mg/m2/day,d1-28 q6wx4cycles
Gemcitabine 1000mg/m2 d1,8,15every 29days x6cycles
Primary Endpoint:non-inferiority inOS
Treatment Pts 2yrs Survival HR p
Gemcitabine 193 53% 0.56(95%CI.42-.74) <0.0001non-inferiority
S1 192 70% <0.001 superiority
• QoL better withS1;G3/4toxicity similar,except forleukopenia lower inS1Fukutomi A,ASCO2013

5-FUPlusLeucovorin vsObservation:Meta-AnalysisofESPAC-1,ESPAC-1+,andESPAC-31,2
q Theresultsof3ESPACtrialswerepooledtocompareobservationvs5FU/leucovorina
q Allpatientshadresected,histologicallyconfirmedPDAC;noevidenceoflocalspreadordistantmetastasis;lifeexpectancy>3months
q Safetydatawerenotreported
1. Neoptolemos JP, et al. Br J Cancer. 2009;100:246-250. 2. Neoptolemos JP, et al. Lancet. 2001;358:1576-1585.
Trial Observation 5-FU/LeucovorinESPAC-1, n 69 75ESPAC-1+, n 95 97ESPAC-3, n 61 61Total, n 225 233Efficacy Observation 5-FU/Leucovorin HR P Value
Median OS, months 16.8 23.2 0.70 0.003
1 year OS rate, %2 year OS rate, %5 year OS rate, %
633714
774924
— —

SummaryofPhaseIIIAdjuvantStudiesinPCMedian OS, months
Trial CRT Obs 5-FU Gem Gem + Erl S1 P
Value
GITSG 20 11 — — — — 0.03EORTC 40891 21.6 19.2 — — — — 0.540ESPAC-1 15.9 — 20.1 — — — NRa
RTOG 9704 — — 17.1a 20.5a — — 0.12CRT + IFN alfa-2b vs CT 26.5 — 28.5 — — — 0.99CONKO-001 — 20.2 — 22.8 — — 0.01JSAP-02 — 18.4 — 22.3 — — 0.19CONKO-005 — — — 26.5 24.6 — 0.406ESPAC-3 (v2) — — 23.0 23.6 — — 0.39
— — — 53%b — 70%b <.001
a Values reported here are for the set of patients with tumors of pancreatic headb Non-inferiority/superiority trial; reported values refer to 2 year survival

CRTvsCT:Meta-Analysis
Ø Ameta-analysisof10articles(including9trials)examinedtheinfluenceof5adjuvantPCtreatmentsonsurvivalandtoxicityØ Observation(n=670)Ø 5-FU(n=876)Ø Gemcitabine(n=774)Ø Chemoradiation (n=169)Ø CRT+5-FU(n=323)Ø CRT+gemcitabine(n=221)
Ø Authors’interpretationofresultsØ CTwith5-FUorgemcitabineistheoptimumadjuvanttreatmentforPCandreduces
mortalityaftersurgerybyaboutathirdØ CRT+CTislesseffectiveinprolongingsurvivalandismoretoxicthanCT
Liao W-C, et al. Lancet Oncol. 2013;14:1095-1103.
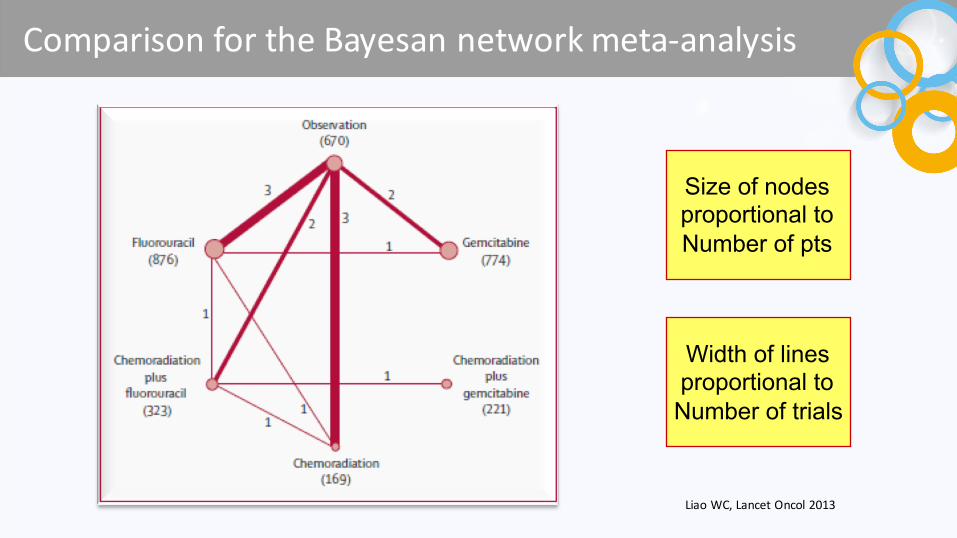
Comparison fortheBayesan networkmeta-analysis
Liao WC,LancetOncol 2013
Width of linesproportional toNumber of trials
Size of nodesproportional toNumber of pts

Pooled hazard ratios fordeath
ØFirst line: crude HRØ2° line (red): HR adjusted for percentage
of LN positivityØBayesan p-values <.05 in blue if crudeØBayesan p-values <.05 in green if adjusted
Liao WC,LancetOncol 2013


Rankingoftreatments interms ofOSbenefitandoverall G3-4toxic effects
ØCT with 5FU or GMC is the optimum adjuvant treatmentØIt reduces mortality by about a thirdØAdding CRT to CT provides little further survival benefit, but increases toxicity

Raigani S,JGastroint Surg 2014
Community Hospitals, 2003-2010 Teaching Hospitals, 2003-2010
SO = Surgery onlySC = Surgery + CTSRC = Surgery + RT + CT
Trendsintreatmentofpancreatic cancerNationalCancer Database– StageI
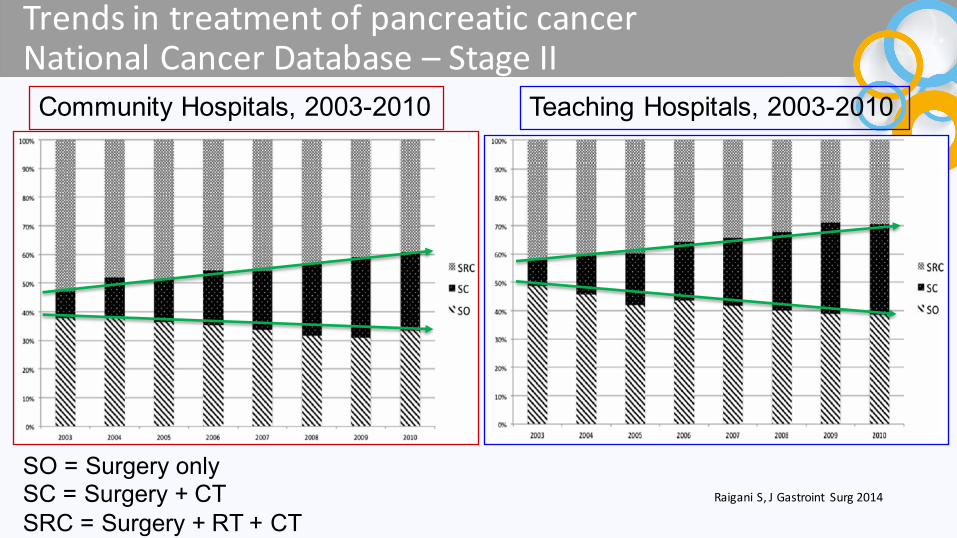
Trendsintreatmentofpancreatic cancerNationalCancer Database– StageII
Community Hospitals, 2003-2010 Teaching Hospitals, 2003-2010
SO = Surgery onlySC = Surgery + CTSRC = Surgery + RT + CT
Raigani S,JGastroint Surg 2014

• Neoadjuvant therapy– Resectable tumors (RPC)
• Endpoint– Toincrease survival incomparison toadjuvant therapy
– Borderlineresectable tumors (BRPC)• Endpoints
– Toincrease R0resectability andsurvival
• Induction therapy– Locally advanced unresectable tumors (LAPC)
• Endpoints– Toconvert somepatient toresectability– Toincrease local andsystemic disease
Neoadjuvant therapy:aconfounding term

Rationale insupport ofneoadjuvant therapy
• Increasing thelikelihood ofmargin-negativeresection• Increasing thelikelihood ofcompletion ofmultimodality
therapy• Increasing theefficacy ofradiotherapy• Minimizing pancreatic leak (without increasingcomplications)• Determination ofindeterminant lesions• Declaration ofdistantmetastases• Decreasing«open-and-close»rates• Allowing apatient’s functional statustodeclare itself• Improved cost-effectiveness (?)

Concerns inneoadjuvant therapy
• Inaccuracyofstaging• Imprecisecontinuumbetween radiologically andtechnically
resectable andunresectabledisease• Erroneous histology• Difficulty indistinguishingPCfromintrapancreaticbileduct
ADC• Potential increase inoperativemorbidity andmortality• Possibility ofmetastases orunresectability during therapy• Difficult assessmentofresponse
– Clinical criteria:clinical benefit(pain),noCTprogression,Ca19-9• Uncommon radiographicdown-staging inBRPC

Resectable PC:selected prospective studies - CT
Author Pts Treatment Resectionrate
R0 Survival
Palmer‘07 50 GEM 38% - mOS 9.9m
GEM+CDDP 70% - mOS 15.6m
Heinrich‘08 28 GEM+CDDP 93% 71% mOS 19.1 m(res)
Tajima ‘12 34 S1(13pts)vsUpfront surgery (21pts)
100%100%
84.6%85.7%
2yrs 55.6%2yrs 29.6%
Mizuma ‘14 36 GEM+S1 - 87% 2yrs 45.7%
O’Reilly ‘14 38 GEMOX→Surg →GEM 71% - mOS 27.2

Resectable PC:perioperative therapy
O’Reilly EMetal,AnnSurg 2014

Resectable PC:selected prospective studies - CRT
Author Pts Treatment Resectionrate
R0 Survival
Evans‘08 86 GEM+RT 75% 66% mOS 22.7m(res)
Varadhachary ’08 90 GEM+CDDP→GEM/RT 66% 62% mOS 17.4m(res)
LeScodan ‘’08 41 FU+CDDP+RT 67% - mOS 9.4m(res)
Turrini’10 34 TXT+RT 50% 10% mOS 32m(res)
Shimoto ’13 26 CarboionRT 81% - 5yrs 42%

Resectable andBRPC:selected studies
Author Pts Treatment Resectionrate
R0 Survival
Sho ’13* 22res+39BR GEM+CRT 97% 92% NR
VanBuren ‘13 30 res+29BR GEM+Bev +CRT 72.8% 64% mOS 19.7m(res)
*Retrospective study;important biases fromthelack ofpre-neoadjuvanthistological confirmation forsomepatient andtheadministraton ofadjuvant CTtosomeothers

BRPC:selected prospective studies
Author Pts Treatment Resectionrate
R0 Survival
Patel ‘11 17 GTX→FU/RT 64.7% 47% mOS 15.6m
Stokes ‘11 40 Cap/RT 46% 40% mOS 23m
Landry ‘10 10 GEM/RT 30% 19.4% -
11 GEM+CDDP/RT 22% 13% -
Leone‘13 39 GEMOX→GEM/RT 28% 28% mOS 16.7m
Christians ‘14 18 FOLFIRINOX→CRT 67% 67% 2yr S:39%

BRPC:selected retrospective studies
Author Pts Treatment Resectionrate
R0 Survival
Faris ‘13 25 FOLFIRINOX 33% 10% -
Boone ‘13 22 FOLFIRINOX 26% - -
Christians ‘14 18 FOLFIRINOX 67% - -
Hattori ‘14 28 S1 76% - -
Rose‘14 64 GEM+TXN orFU+OXA 48% - mOS 23.6m(res)
Katz‘08 160 CT→CRT 63% --
mOS 18mmOS 40m*
*66out160patients who completed theprogram

LAPC:selected prospective studies
Author Pts Treatment Resectionrate
R0 Survival
Kunzmann ‘13 8 NabT →FOLFIRINOX 37% - -
Huguet ‘07 167 PCTseq vsGEMOX→RT - - mOS 13.1m
Reni’09 91 PEFG/PEXGorPDXG→RCT
14%ORR47%
- mOS 16.2m
Polistina ‘10 23 GEM→GEM+RT 8% 0.9% mOS 10.6m
Mukerjee ‘13 3836
GEM→CRTCap→CRT
--
--
mOS 15.2mmOS 13.4m
Sherman ‘15 34(art)11(ven)
GTX→CRT→SurgGTX→Surg (R1→CRT)
85.3%100%
69%7.5%
mOS 29mmOS n.r.*
*n.r.=not reached

LAPC:selected retrospective studies
Author Pts Treatment Resectionrate
R0 Survival
Gunturu ‘13 16 FOLFIRINOX ORR50% - -
Nitsche ‘15 14 FOLFIRINOX 29% - -
Greer ‘08 102 FU+CDDP→GEM+RT 41% - -
Khushman‘15
51 FOLFIRINOX→CRT(not res)FOLFIRINOX→CH(res) 53% 40% mOS 35.4m*
*All patients
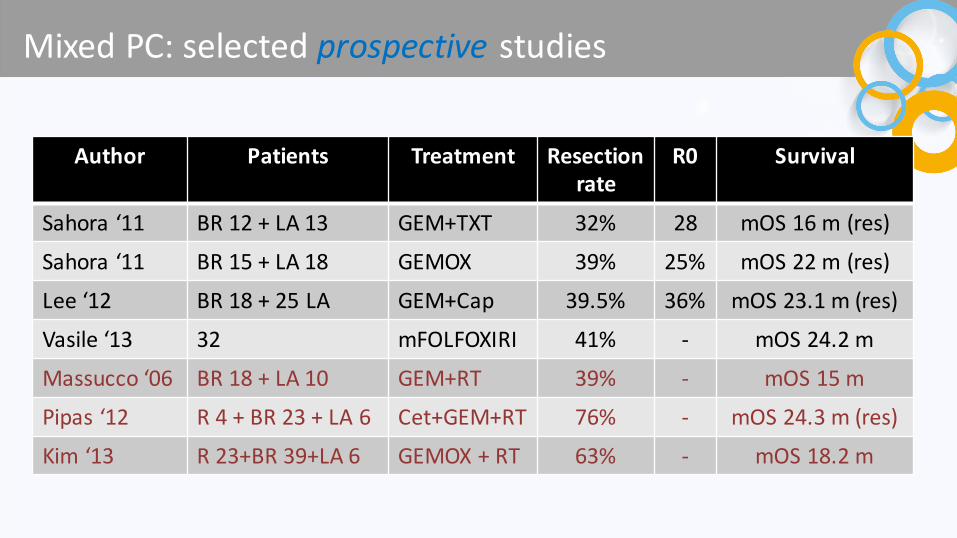
MixedPC:selected prospective studies
Author Patients Treatment Resectionrate
R0 Survival
Sahora ‘11 BR12+LA13 GEM+TXT 32% 28 mOS 16m(res)
Sahora ‘11 BR15+LA18 GEMOX 39% 25% mOS 22m(res)
Lee‘12 BR18+25LA GEM+Cap 39.5% 36% mOS 23.1m(res)
Vasile‘13 32 mFOLFOXIRI 41% - mOS 24.2m
Massucco ‘06 BR18+LA10 GEM+RT 39% - mOS 15m
Pipas ‘12 R4+BR23+LA6 Cet+GEM+RT 76% - mOS 24.3m(res)
Kim ‘13 R23+BR39+LA6 GEMOX+RT 63% - mOS 18.2m

MixedPC:selected retrospective studies
Author Patients Treatment Resectionrate
R0 Survival
Hosein ‘12 18(BR+LA) FOLFIRINOX 39% 20% 1yr PFS83%
Lee‘12 BR18+25LA GEM+Cap 39.5% 36% mOS 23.1m(res)
Peddi ‘12 23(BR+LA) mFOLFIRINOX ORR34% - 1yr PFS75%
Blazer‘14 43(BR+LA) mFOLFIRINOX 53.8% 42% mPFS 18.4 m(res)
Nanda‘15 BR14+15LA FOLFIRINOX→CRT 41.3% 31% 1yr S65.5%Kharofa ‘14 R 30
BR39CRT→Surg →RTCT→CRT→Surg →RT
70% 65% mOS 20m
Mellon‘15 BR110+49LA CT(FOLFIRINOXin21LA) 51% 48% mOS 34.2(res)
Blazer‘15 BR18+25LA FOLFIRINOX→CRT 51% 45% -
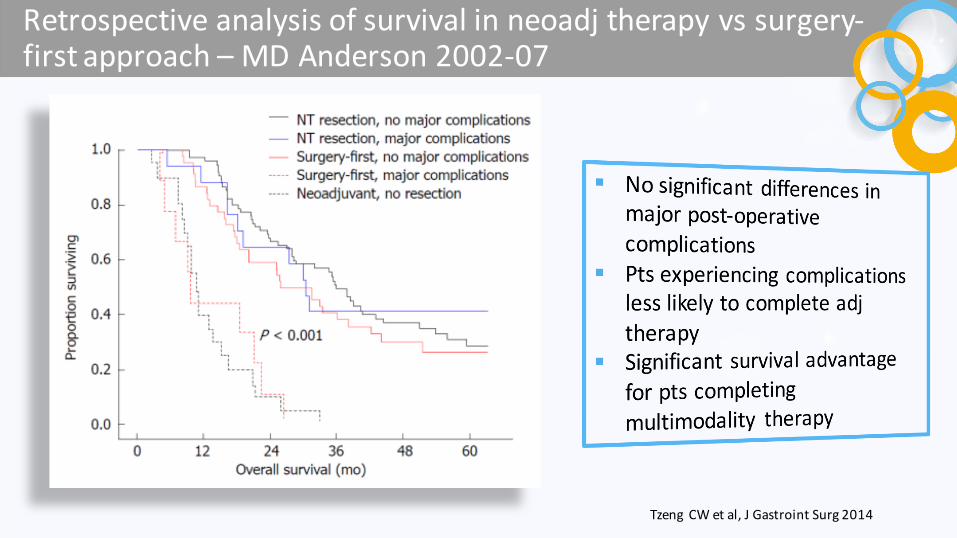
Retrospective analysis ofsurvival inneoadj therapy vssurgery-firstapproach – MDAnderson2002-07
Tzeng CWetal,JGastroint Surg 2014

Summary ofmeta-analyses:localized,BRandLAPC
Author Studies Treatment Patients Resection rate Survival
Petrelli’14 2phase II11retrosp
FOLFIRINOX+CRT
BR+LA 43% -
Xu ’14 1prosp2retrosp
Adj CRTvsNeoadj CRT
LPC - P =0.62
Festa’13 5phase II5prosp
CT± RT BR 80%(of69%*)
1yr S61%2yr S44%
Andriulli ’13 7phase I/II10phase II3prosp
GEM± RTGEM± RT
LPCBR+LA
82%(of91%*)68%(of39%*)
2 yr S67.2%2yr S54.2%
Assifi ‘11 14phase II CT± RTCT± RT
LPCBR+LA
65%31%
mOS 23mmOS 22.3m
*Percentage ofexplored patients

Limitsofmeta-analyses forneoadjuvant therapy• Different types ofstudies
– Phase IIorI– Retrospective– Cohort– Casereports
• Different settings– Resectable tumors– Borderlineresectable tumors– Locally advanced uresectable tumors
• Low size samples– Less than 50patients inprospective studies
• Different schedules– Monotherapy (FluoropyrimidineorGemcitabine orTaxanes)– Combinationtherapy (GEMOX,GEM+CDDP, FOLFIRINOX,GTX,S1+GEM,others)
• Different measures ofoutcome• Mixedtreatmentstrategies
– CTalonefollowed bysurgery followed ornot byRTorCT– CTfollowed byRTorRCTfollowed bysurgery– CRTfollowed bysurgery followed ornot byCT

RecommendationsforAdjuvantPCTreatment
• Forsurveillance, theNCCNrecommendshistoryandphysicalexam(cat2A),CA19-9(cat2B),orCTscan(cat2B)every3- 6months for2years,andthenannually
a For NCCN guidelines, chemotherapy before or after chemoradiation. Chemoradiation can be fluoropyrimidine- or gemcitabine-based.b The ESMO guidelines state that chemoradiation in the adjuvant or additive setting should only be performed within randomized controlled trials (cat IB).c Not specified in guidelines whether leucovorin should be included or whether the recommendation differs by bolus vs continuous infusion.1. NCCN Clinical Practice Guidelines in Oncology, V2.2015; 2. Ducreux M, et al. Ann Oncol 2015; 3. Yamaguchi K, et al. Jpn J Clin Oncol 2011.
NCCN 20151 ESMO 20152,b JPS 20113
Chemotherapy alone
Gemcitabine 1 I A B5-FU/leucovorin 1 I Ac —Continuous infusion 5-FU 2A I Ac —Capecitabine 2B — —
Chemotherapy plus chemoradiationa
Gemcitabine 2A — —5-FU/leucovorin 2A — —Continuous infusion 5-FU 2A — —
Chemoradiation alone Gemcitabine — — C1

Linee-GuidaAIOM- 1Qualità
dell’evidenzaSIGN
Raccomandazioneclinica Forzadellaraccomandazione
clinica
C NeitumoriBLèraccomandabileunastrategiaterapeuticacontrattamentoneoadiuvante seguitodaristadiazione edeventualeresezionechirurgica
Positivadebole
D Inmancanzadistudiprospetticineitumoriresecabiliconfattoriprognosticiassociatialimitatasopravvivenzapost-operatoriapuòessereconsiderato untrattamentoneoadiuvante
Positivadebole
A IpzaffettiaADCduttaledelpancreasstadioIa-IIIresecatoR0-R1 conKarnofsky ≥50devono rievere unaCTadiuvanteconFPoGEM
Positivaforte
D* LaRCTpuòessereconsideratadopochirurgiaR0oR1conunadosedialmeno50Gy
Positivadebole
*Opinionediespertiinassenzadistudiconunadeguatolivellodiqualità

Linee-GuidaAIOM– 2MalattialocalmenteavanzataQualità
dell’evidenzaSIGN
Raccomandazioneclinica Forzadellaraccomandazione
clinica
D* IpzconmalattialocalmenteavanzatanonresecabilepotrebberoesseretrattaticonCTsistemica,conglischemidellamalattiaavanzata,seguitadaRCT
Positivadebole
*Opinionediespertiinassenzadistudiconunadeguatolivellodiqualità
Qualitàglobaledelleevidenze
GRADE
Raccomandazioneclinica Forzadellaraccomandazione
clinica
Molto bassa NeipzaffettidaADCnonresecabiledelpancreasinstadioIIIpotrebbeessereeffettuataunaCTcometerapiainiziale
Positivadebole
Bassa Neipz affettidaADCnonresecabiledelpancreasinstadioIIIlacapecitabina puòesseresomministratainconcomitanzaallaRT
Positivadebole

CRTforAdjuvantTreatmentisControversial1
1. Twombly R. J Natl Cancer Inst 2008; 2. NCCN Clinical Practice Guidelines in Oncology. V2.2105. 3. Kalser MH, et al. Arch Surg 1985; 4. Ducreux M, et al. Ann Oncol 2015; 5. Klinkenbijl JH, et al. Ann Surg 1999; 6. Neoptolemos JP, et al. Lancet 2001.

AdjuvantAfterNeoadj TherapyandResection
• AccordingtotheNCCN,datasupportingtheuseofadjuvanttherapyforpatientswhoreceivedneoadjuvanttherapyarelacking1
• Patientswhoreceivedneoadjuvantchemotherapyorchemoradiationmayconsideradjuvanttreatmentanoption pendingmultidisciplinaryreview(responsetoneoadjuvanttherapymayguidetreatmentchoice)
• Apatientwhoundergoesresectionforinitiallyborderlineresectablediseasemayconsideradjuvanttherapy(sametherapyoptionsasforinitiallyborderlineresectable disease)2
1. NCCN Clinical Practice Guidelines in Oncology, V2.2015: 2. Vincent A, et al. Lancet2011.

KeyOngoingPhaseIIIAdjuvantPCTrials- 1
Trial Pts Experimentalarm
Comparator arm PrimaryEndpoint
CONKO-006 NR GEM+SOR GEM DFS
PACT-15(NCT01150630)
370* Adj PEXG±Neoadj PEXG
GEM(adj) OS
NCT01072981 722 GEM± CRT+algenpantucel
GEM± CRT OS
PRODIGE/ACCORD24(NCT01526135)
490 FOLFIRINOX GEM DFS
RTOG08481° randomRTOG08482° random(NCT01013649)
950 GEM+ERLGEM± ERL
GEMGEM± ERL +CRT
OSOS
*This is aphaseII/III trial.N refers tothephase II,which compares adj PEXGwithadj+neoadj PEXC

KeyOngoingPhaseIIIAdjuvantPCTrials- 2
Trial Pts Experimentalarm
Comparator arm PrimaryEndpoint
GIP-2(NCT02355119) 310 FOLFOXIRI GEM DFS
NEPAFOX*(NCT02172976)
126 FOLFIRINOXneoadj andadj
GEM OS
NCT00994721 265 GEM+CRT GEM DFS
ESPAC-4 732 GEM+CAP GEM DFS
APACT(NCT01964430) 800 GEM+NabTXL GEM DFS
*This is aphaseII/III trial.N refers tothephase II
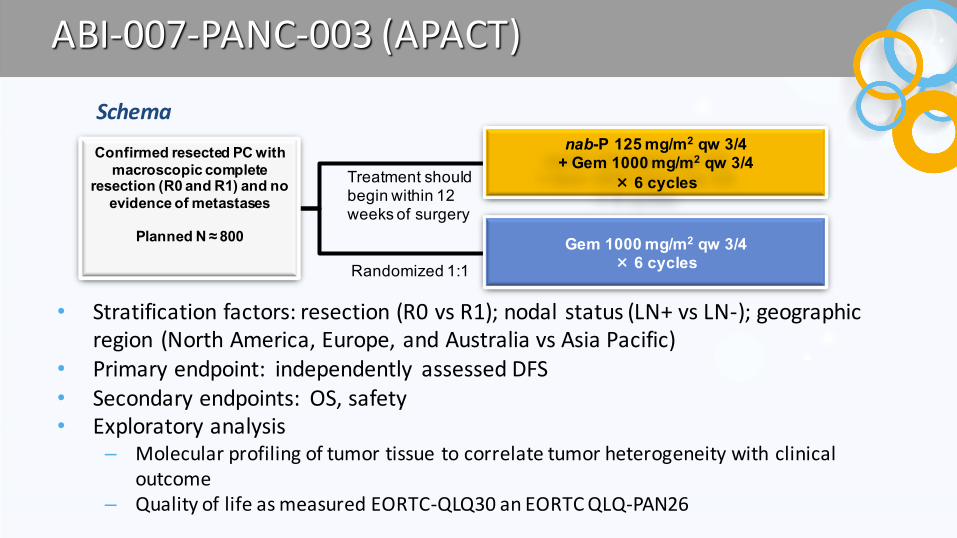
ABI-007-PANC-003(APACT)
nab-P 125 mg/m2 qw 3/4 + Gem 1000 mg/m2 qw 3/4
× 6 cycles
Gem 1000 mg/m2 qw 3/4× 6 cycles
Confirmed resected PC with macroscopic complete
resection (R0 and R1) and no evidence of metastases
Planned N ≈ 800
Treatment should begin within 12 weeks of surgery
Randomized 1:1
Schema
• Stratification factors:resection (R0vsR1);nodal status(LN+vsLN-);geographicregion (NorthAmerica,Europe,andAustraliavsAsiaPacific)
• Primary endpoint: independently assessed DFS• Secondary endpoints: OS,safety• Exploratory analysis
– Molecular profiling oftumor tissue tocorrelatetumor heterogeneity withclinicaloutcome
– Quality oflifeasmeasured EORTC-QLQ30anEORTCQLQ-PAN26
• Tocomparedisease-freesurvivalbetweenpatientsrandomizedtonab-P+GemvsGemalone
ClinicalTrials.gov:NCT01964430
PrimaryObjective
Rationale• NoadjuvantPCregimenshavereceivedregulatoryapprovalintheUS1
• TheNCCNandESMOrecommend5-FU(NCCN:+leucovorin) orGemasadjuvantchemotherapyoptions2,3
• RecurrencerateswithadjuvantGemwere77%and81%inphaseIIItrials,suggesting aneedforimproved therapies4,5
• nab-P+GemdemonstratedsuperiorefficacyvsGemalonefortreatmentofmetastaticPCinthephaseIIIMPACTtrial6
1.LiaoW-Cetal.LancetOncol 2013; 2.TheNationalComprehensiveCancerNetwork.NCCNGuidelinesinOncology,v1.2013.3.Seufferlein Tetal.AnnOncol 2012; 4.Oettle Hetal.JAMA 2013;5.UenoH,etal.BrJCancer 2009; 6.VonHoffDD,etal.NEngl JMed 2013.
APACT:AdjuvantPancreaticAdenocarcinomaClinicalTrial(ABI-007-PANC-003)

ABI-007-PANC-003(APACT)
• HistologicallyconfirmedresectedPCwithmacroscopiccompleteresection(R0andR1)
– Noneuroendocrinetumors• StageT1-3,N0-1,M0• Abletobegintreatment≤12weeksafterresection• Age≥18years• ECOGPS0or1• Adequatehematologicandbloodchemistryparameters,including
– Absoluteneutrophil count≥1500cells/mm3
– Totalbilirubin ≤ULN(patientswithGilbertsyndrome, ≤1.5×ULN)• CA19-9<100U/mLassessedwithin14daysofrandomization
1.CelgeneDataonFile.ProtocolABI-007-PANC-003.2.ClinicalTrials.gov:NCT01964430.
SelectedInclusion Criteria

ABI-007-PANC-003(APACT)
• Assumptionbasedon2previousphaseIIItrials:GemwillresultinamedianDFSof14months1,3,4
• Theestimatedenrollmentofthistrialis800patients1,2– Ifnab-P+GemresultsinamedianDFSof19months,this
wouldrepresentanHRof0.74– Atleast489DFSeventsfrom800patientswouldallow90%
powertodetecttheHRof0.74ata2-sidedsignificancelevelof0.05
1.CelgeneDataonFile.ProtocolABI-007-PANC-003. 2.ClinicalTrials.gov:NCT01964430.3.Oettle H,etal.JAMA 2007;4.Neoptolemos JP, etal.JAMA 2010.
StatisticalDesign

KeyOngoingNeoadjuvantPCTrials- 1
Trial Pts Treatmentgroups PrimaryEndpoint
NEONAX(NCT02047513)
166 Neoadj GEM+NabTXL x2Adj GEM+NabTXL x4Adj GEM+BabTXL x6
DFS
NCT02047474 46 Neoadj FOLFIRINOXx3+AdjFOLFIRINOXx3
DFS
NEOLAP(NCT02125136)*
168 Neoadj GEM+NabTXL x3+NeoadjFOLFIRINOXx2+Adj GEM+NabTXL x3Neoadj GEM+NabTXL x4+Adj GEM+NabTXL x3
Conversionrate
*Including LAPC

KeyOngoingNeoadjuvantPCTrials- 2
Trial Pts Treatmentgroups PrimaryEndpoint
NCT01314027 - Neoadj GEMOX+Adj GEMAdj GEM
DFS
NCT01065870 - Neoadj GTX+RTNeoadj GTX
DFS
NEOPA 410 Neoadj CRT+Adj GEMAdj GEM
DFS

Summaryü Resectionistheonlypotentiallycurativetreatmentoption forPC1
ü Atthetimeofdiagnosis,≈10%ofpatientswithPChaveresectablediseaseand≈10%patientshaveborderline resectable disease2
ü TheuseofCRTforadjuvantPCiscontroversial3ü CurrentUSrecommendationslistCT(Gemor5-FU/leucovorin)asacategory1optionand
CRTacategory2Aoption1ü CurrentESMOguidelines listCT(Gemor5-FU/leucovorin)asacategory1Aoptionbutdo
notrecommendCRToutsideofaclinical trial4ü Resultsofarecentmeta-analysissupportCToverCRT5
ü AnumberofphaseIIItrialsarecurrentlyexploringdifferentadjuvantPCtreatmentoptions6
ü Theroleofneoadjuvantorconversiontherapyispresentlyuncertain;thisstrategyhastobeevaluatedinwell-designedclinicaltrial,butinthepracticemightbeconsidered inBRPCandinLAPCpendingmultidisciplinary review
1. NCCN Clinical Practice Guidelines in Oncology. Pancreatic Adenocarcinoma. Version 2.2015. 2. Vincent A, et al. Lancet. 2011:378:607-620. 3. Twombly R. J Natl Cancer Inst. 2008;23:1670-1671. 4. Ducreux M, et al. Ann Oncol. 2015;23(suppl 5):v56-v68.
5. Liao W-C, et al. Lancet Oncol. 2013;14:1095-1103. 6. Neoptolemos JP, et al. Presented at: ASCO 2013 [abstract 4006].

• Back-up