la rehabilitation rapide en chirurgie de...
TRANSCRIPT

LA REHABILITATION RAPIDE EN CHIRURGIE DE L’OBESITE
Elie CHOUILLARD Department of General & Minimally Invasive Surgery
Poissy/Saint-Germain-en-Laye(FRANCE)
For The Intercontinental Society of Natural, Orifice, Endoscopic, and Laparoscopic Surgery (i-NOELS)

Introduction
Chirurgie, traitement de référence pour l’obésité pathologique.
2000-2015: Innovations techniques anesthésiques visant à accélérer le rétablissement, sans compromettre la sécurité
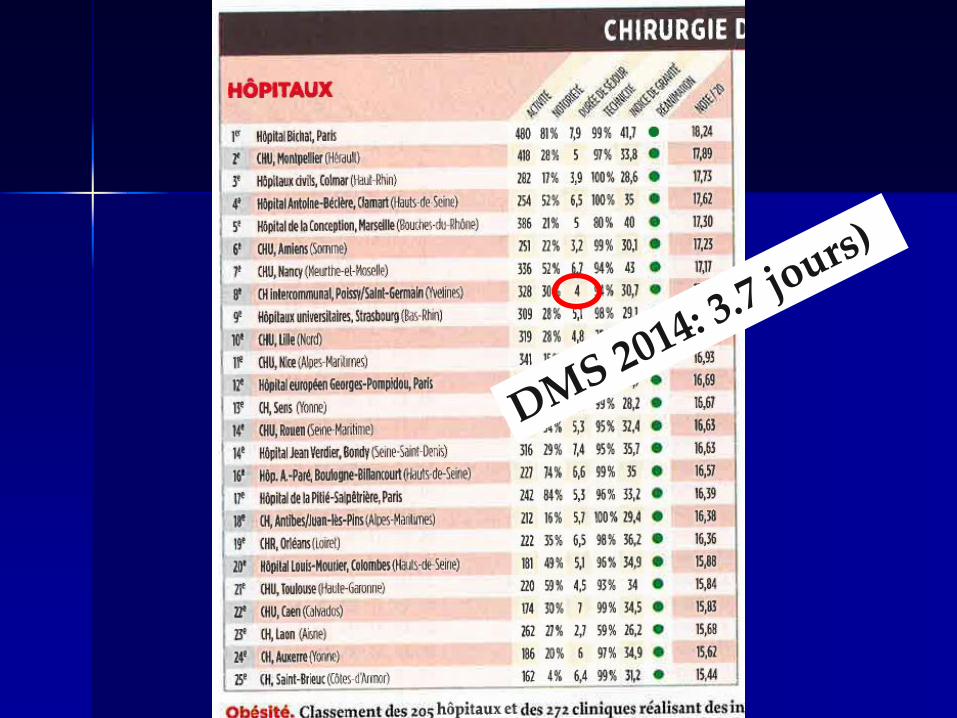
⬇ durée de séjour 300 % en 20 ans.

Fast Track: Definition
A fast-track pathway indicates a multidisciplinary strategy to enhance postoperative recovery and decrease
morbidity by reducing surgical stress and its consequences (stress-free surgery)
Slim K. Fast-track surgery: the next revolution in surgical care following laparoscopy. Colorectal Dis 2011;13:478–480

Fast Track: Definition
A fast-track pathway indicates a multidisciplinary strategy to enhance postoperative recovery and decrease
morbidity by reducing surgical stress and its consequences (stress-free surgery)
Slim K. Fast-track surgery: the next revolution in surgical care following laparoscopy. Colorectal Dis 2011;13:478–480

Fast Track: Definition
A fast-track pathway indicates a multidisciplinary strategy to enhance postoperative recovery and decrease
morbidity by reducing surgical stress and its consequences (stress-free surgery)
Slim K. Fast-track surgery: the next revolution in surgical care following laparoscopy. Colorectal Dis 2011;13:478–480

Fast Track: Definition
A fast-track pathway indicates a multidisciplinary strategy to enhance postoperative recovery and decrease
morbidity by reducing surgical stress and its consequences (stress-free surgery)
Slim K. Fast-track surgery: the next revolution in surgical care following laparoscopy. Colorectal Dis 2011;13:478–480

Fast Track: Definition
A fast-track pathway indicates a multidisciplinary strategy to enhance postoperative recovery and decrease
morbidity by reducing surgical stress and its consequences (stress-free surgery)
Slim K. Fast-track surgery: the next revolution in surgical care following laparoscopy. Colorectal Dis 2011;13:478–480

Fast Track: Definition
A fast-track pathway indicates a multidisciplinary strategy to enhance postoperative recovery and decrease
morbidity by reducing surgical stress and its consequences (stress-free surgery)
Slim K. Fast-track surgery: the next revolution in surgical care following laparoscopy. Colorectal Dis 2011;13:478–480

Fast Track: Definition
A fast-track pathway indicates a multidisciplinary strategy to enhance postoperative recovery and decrease
morbidity by reducing surgical stress and its consequences (stress-free surgery)
Slim K. Fast-track surgery: the next revolution in surgical care following laparoscopy. Colorectal Dis 2011;13:478–480


La durée du séjour hospitalier est significativement réduite en
comparaison avec la prise en charge tradiotionnelle
Ansari D, Gianotti L, Schroder J, Andersson R.
Fast-track surgery: procedure-specific aspects and future direction. Langenbecks Arch Surg 2013;398:29–37
Fast Track: Finalité


❒ Pousser le principe de la réduction de la durée de séjour au maximum…
❒ Récupération fonctionnelle plus accelérée et délocalisée
❒ Réduire le séjour hospitalier à sa plus simple expression: Moins d’une journée!
Hemmerling TM, Romano G, Terrasini N, Noiseux N.
Anesthesia for off-pump coronary artery bypass surgery. Ann Card Anaesth. 2013;16(1):28–39
Ultra Fast Track: Définition
❒
❒ Application to bariatrics allows favorable outcomes, equivalent to traditional management strategies
❒ Implementation of this pathway is based on the following three elements:
• Features of the surgery • Particularities of patients • Optimization of perioperative care
Elliott JA, Patel VM, Kirresh A, et al. Fast-track laparoscopic bariatric surgery: a systematic review. Updates Surg. 2013;65:85–94.
Wasowicz-Kemps DK, Bliemer B, Boom FA, et al. Laparoscopic gastric banding for morbid obesity: outpatient procedure versus
overnight stay. Surg Endosc 2006;20:1233–1237
Fast Track in Bariatrics

☞Information du patient
☞Préparation nutritionnelle
☞Protocoles dédiés d’anesthésie
☞Chirurgie de + en + mini-invasive
☞Morbilisation précoce Lemanu DP, Srinivasa S, Singh PP, et al. Optimizing perioperative care in bariatric surgery patients.
Obes Surg. 2012;22(6):979–990 Raeder J. Bariatric procedures as day/short stay surgery: is it possible and
reasonable? Curr Opin Anaesthesiol 2007;20:508–512
Fast Track: Philosophie Collaboration Multidisciplinaire (Chirurgiens, Anesthésistes,
Paramédicaux, Kinésithérapeute, ….et…SURTOUT LE PATIENT

Raeder J. Bariatric procedures as day/short stay surgery: is it possible and reasonable? Curr Opin Anaesthesiol 2007;20:508–512
Joshi GP. The adult patient with morbid obesity and/or sleep apnea syndrome for ambulatory surgery. Presentation at
the American Society of Anesthesiology annual meeting. 2010. http://www.hnanes.org/modjeditor/uploadfile/20101207224350233.pdf. Accessed May 12, 2013
Sasse KC, Ganser JH, Kozar MD, et al. Outpatient weight loss surgery: initiating a gastric bypass and gastric banding
ambulatory weight losssurgery center. JSLS 2009;13:50–5
Type de chirurgie
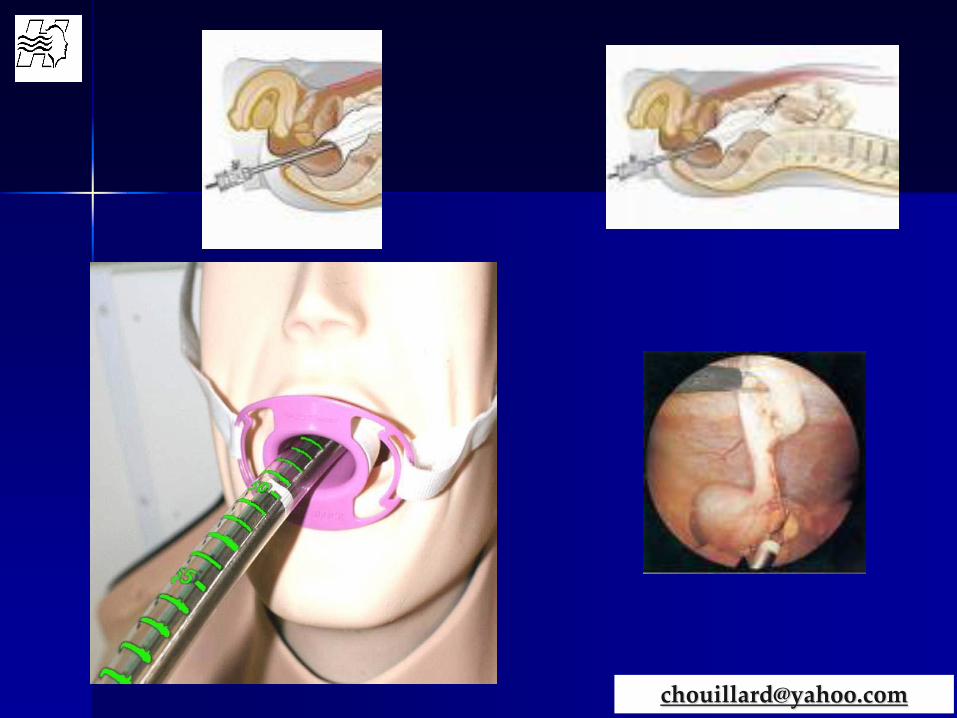
What is NOTES?
Natural Orifice Translumenal Endoscopic Surgery:
- Intentional puncture of one of the viscera (e.g., stomach, rectum, vagina, urinary bladder) to access the abdominal cavity
- With an endoscope (flexible or stiff)
- To perform an intraabdominal operation
Pearl JP, Ponsky JL: J Gastrointest Surg. 2007


Rationale

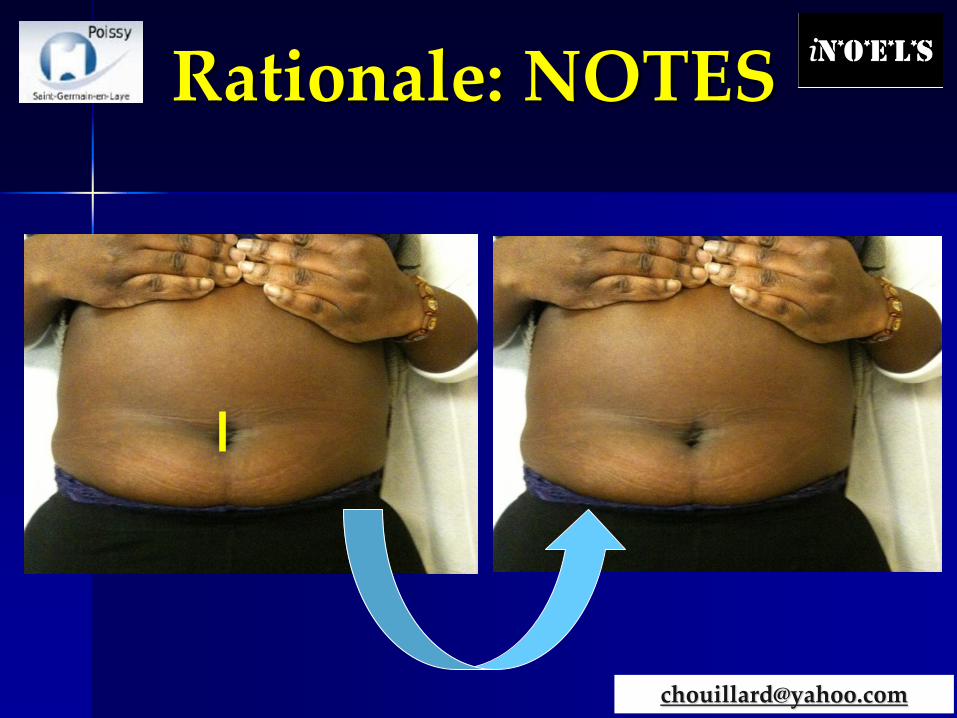

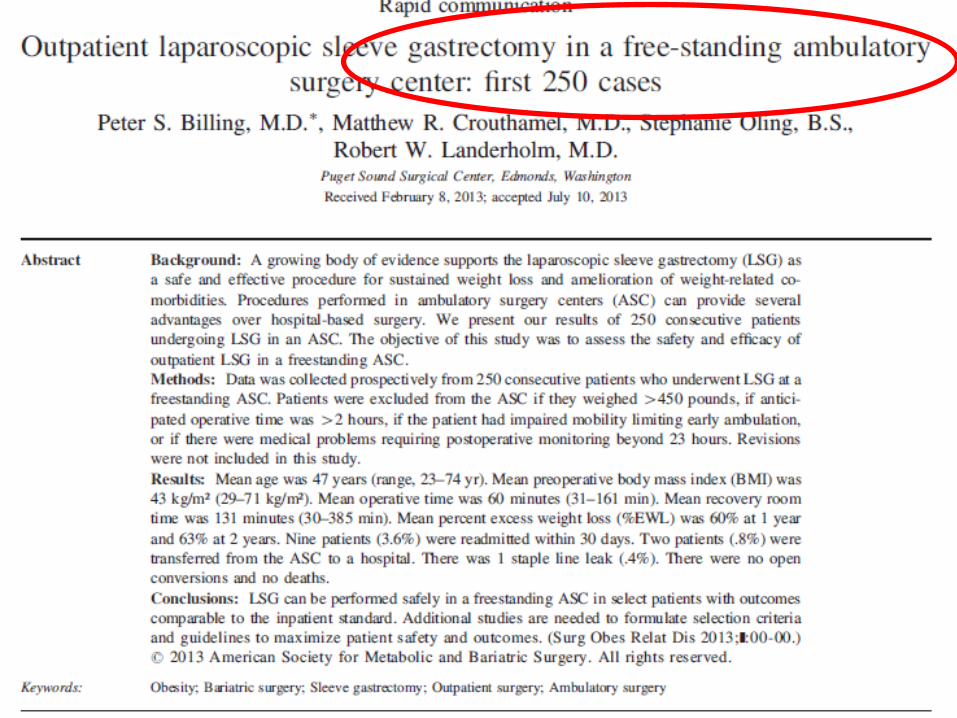
❒ Banding and Roux-en-Y gastric bypass, most frequently associated with ultra fast-track
❒ Sleeve Gastrecctomy (France)
❒ Abdominoplasty
❒ Careful patient selection
❒ Experienced surgical, anesthetic, and nursing
❒ Postoperative observation and follow up
❒ Miscellaneous: Short duration of the surgery High procedure volume Proximity to a tertiary level hospital
Chirurgie

An exemple of specialized Center Regional center of excellence (> 750 procedures 2014)
Large Teaching hospital (1000 beds)
Bariatric program since 1976
Multidisciplinary team
Fast-track logistics since 2011
Procedures per day on one OR (8.00-15.45h)
7 LRYGB
8 LSG
5 Revision surgery
❒ IMC, tout sauf un facteur limitant
❒ Comorbidités, facteur limitant +++++++
❒ Apnée du sommeil +++++
❒ Sélection obligatoire
❒ Adhésion du patient, cruciale
Patients selection

❒ Information détaillée et réitérée
❒ Restriction calorique préopératoire et activité physique oxygénée
❒ Arrêt strict du tabac et de l’alcool > 1 mois
❒ Arrivée entre 6:30 et 8:00
❒ Jeûn préopératoire 2 H pour les liquides et 6 H pour les solides
Prise en charge périopératoire

❒ Charge sucrée (50 mg dans 400 mL 2 H avant l’intervention): contre la déshydratation améliore l’insulinorésistance
❒ Prophylaxie anthithrombotique (pharmacologique & mécanique): patients à haut risque
❒ Bandes ou chaussettes de cotention + 1 dose préopérqtoire d’anticoagulants (HBPM)
❒ Antibiothérapie prophylactique
❒ Contrôle de l’acidité gastrique
Prise en charge préopératoire
❒ Anesthetic management is based on the S.A.F.E. principle (short acting drugs facilitating fast emergence)
❒ Induction : remifentanil, propofol and rocuronium, or cisatracurium
❒ Opioids: remifentanil, drug of choice
❒ RSI is important in patients with obesity with symptomatic GERD, gastroparesis, emergency surgery, and intestinal obstruction.
Intraoperative Management

❒ Preoxygenation and endotracheal intubation should be performed in the 25-degree, head-up position or the head elevated laryngoscopy position (HELP) ❒ Use ultrasonography selected patients ❒ Pressure-controlled ventilation with a PEEP
Intraoperative Management

❒ Goal-directed fluid therapy (esophageal doppler)
❒ Warming
❒ Avoidance of NG tubes and drains
❒ Postoperative nausea vomiting (PONV) Prophylaxis
❒ Glucocorticoid administration.
❒ A multimodal and opioid sparing approach for postoperative analgesia
❒ Wound infiltration
Other intraoperative measures

Preoperative measures
LMWH evening before surgery
Elastic stockings
Pneumatic stocking for history of DVT
Urinate before surgery (no CAD& no bladder-scan)
Single dose IV-Antibiotic prophylaxis
OR-shirt with front closure
Weight/diet check 1 week before surgery (if incorrect; postpone surgery)

Position & Fixation
Head
Elevated
Laryngoscopy
Position
Information! No premedication
Let the patient install awake (neuropathy)
HELP
Simple, fast & firm fixation

Protocoles dédiés d’anesthésie
Opioïds partition coefficient
oil/water
Ultiva (30) ~ 20
Alfentanil (31) ~ 130
Fentanyl (31) ~ 820
Sufentanil (31) ~ 1730
Hypnotics partition coefficient
oil/gas
Desflurane (33 ) ~ 20
Sevoflurane (33) ~ 45
Isoflurane (33) ~ 90
Halothane (33) ~ 220

Travailler en parallèle et non en série!



Every surgeon uses the same technique
Gastric bypass (linear technique with mesenterial closure)
Sleeve (dorsal SFG-approach)
Standardized surgery
Obes Surg 2012;22:320-9


Surgery & anesthesia finish at the same time
Surgeon leaves OR when the patient is in bed
Surgeon does not leave OR-complex
End of operation
Cleaning in between?
Only if necessary !

❒ Extubated at the end of surgery and transferred awake to the recovery room
❒ Be able to transfer themselves from the operating table
❒ 25- to 30-degree head-up position, monitored and provided with oxygen
❒ In patients with OSA, the duration of the monitoring should be three hours longer than non-OSA patients.
Postoperative measures
❒ Early mobilization 3H / respiratory exercises
❒ Drink some tea or water
❒ Fluid oral intake and short walk
❒ Criteria for the discharge: • No signs of airway obstruction • Saturation at the reoperative level with room air • Sufficient control of pain • No PONV • Full oral liquid intake • Ability to ambulate • Possibility of a follow up (by telephone and presence)
Postoperative measures


❒ Le Fast-Track Bariatrique nécessite des STRUCTURES DÉDIÉES, ainsi que l’implication sans faille de plusieurs spécialités et du patient. ❒ La chirurgie mini-invasive ainsi que la chirurgie sans stress et sans douleur SONT POSSIBLES, permettant une meilleure récupération physiologique. ❒ Si bien pratiqué, avec des patients bien sélectionnés et très bien informés, ce principe est applicable à LA MAJORITEÉ des patients.
Conclusions

Merci de votre attention
POISSY-FRANCE