la inmunoterapia y sus fÁrmacos
TRANSCRIPT

LA INMUNOTERAPIA Y
SUS FÁRMACOS
Rosario García Campelo
Servicio de Oncología Médica
Complejo Hospitalario Universitario A Coruña
XXXIX REUNION ANUAL DE LA SOCIEDAD ESPAÑOLA DE ANATOMIA PATOLOGÍA Y
DIVISION ESPAÑOLA DE LA ACADEMIA INTERNACIONAL DE PATOLOGÍA

Should I tell
you
everything?

Tumors Create Chaos
Disordered
•Blood flow and vascular distribution
•Stroma and immune milieu
Immune shaping
•Creates selection pressure so that cancers can evade immune
destruction
•Malignant “evolution”
Jain RK. Adv Drug Deliv Rev. 2001;46:149-168.
Tumors go to great lengths
to evade or subvert the immune response

Therapies in Active Development Likely to Increase Response to Immune Checkpoint Inhibitors

ANTICANCER INMUNOTHERAPY…a whole universe
Galuzzi L, et al. Oncotarget 2014

Therapeutic vaccines
6
Immunotherapy involving cancer vaccines aims to
generate or augment the innate or adaptive antitumour
immune response with the use of a biologically active
whole-cell or specific protein antigen preparation
Anagnostou – Clin Can Res 2015

Sipuleucel-T (PROVENGE): in metastatic prostate cancer
First FDA-approved therapeutic cancer vaccine (Apr. 2010)
Kantoff et al., NEJM 2010
Cheever et al. CCR 2011
Sipuleucel-T is an active cellular
immunotherapy, a type of therapeutic
cancer vaccine, consisting of autologous
peripheral-blood mononuclear cells
(PBMCs), including antigen-presenting
cells (APCs), that have been activated ex
vivo with a recombinant fusion protein
(PA2024)
PA2024 consists of a prostate antigen,
prostatic acid phosphatase, that is fused
to granulocyte–macrophage colony-
stimulating factor, an immune-cell
activator.

Robert H.I. Andtbacka et al. JCO 2015;33:2780-2788
Oct. 2015 : FDA approval for T-VEC (AMGEN)
Talimogene laherparepvec in unresected melanoma (local injections)
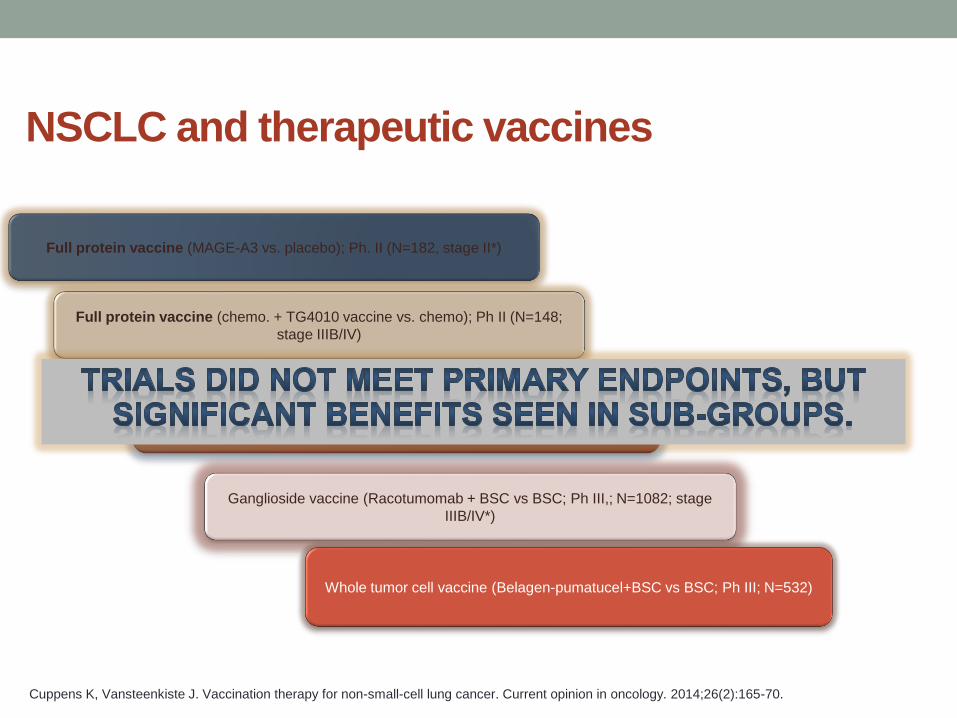
NSCLC and therapeutic vaccines
Full protein vaccine (MAGE-A3 vs. placebo); Ph. II (N=182, stage II*)
Peptide (L-BLP25 vaccine vs placebo; Ph III; N=1514, stage III)
Ganglioside vaccine (Racotumomab + BSC vs BSC; Ph III,; N=1082; stage
IIIB/IV*)
Whole tumor cell vaccine (Belagen-pumatucel+BSC vs BSC; Ph III; N=532)
Full protein vaccine (chemo. + TG4010 vaccine vs. chemo); Ph II (N=148;
stage IIIB/IV)
Cuppens K, Vansteenkiste J. Vaccination therapy for non-small-cell lung cancer. Current opinion in oncology. 2014;26(2):165-70.

CTLA-4 = cytotoxic T-lymphocyte-associated protein 4PD-1 = programmed death 1; PD-L1 = programmed death ligand 1Please note that atezolizumab has not received regulatory approval in any country yet
1. Mellman, et al. Nature 20112. Chen & Mellman. Immunity 2013
7
Killing of cancer cells
(immune and cancer cells)
Anti-CTLA-4CTLA-4 is a major negative regulator of T cell activation and
inhibition of CTLA-4 can enhance T cell stimulation, resulting in
more potent anti-tumour responses1
Ipilimumab
Tremelimumab
Anti-PDL1/PD1PD-L1 expression on tumour cells and tumour-infiltrating
immune cells can inhibit T cell activity via its receptor PD-1,
dampening the anti-tumour immune response. Inhibition of
PD-L1 or its receptor PD-1 may restore T cell effector function2
Nivolumab (anti-PD1)
Pembrolizumab (anti-PD1)
Atezolizumab (anti-PDL1)
Durvalumab (anti-PDL1)
Avelumab (anti-PDL1)
CD28
OX40
GITR
CD137
CD27
HVEM
CTLA-4
PD-1
TIM-3
BTLA
VISTA
LAG-3
T cell targets for modulating activity
Activating
Receptors
Inhibitory
Receptors
T cell
stimulation
Agonistic
Antibodies
Blocking
Antibodies
T cell
Inmune Checkpoint antibodies you need to remember…
Today…

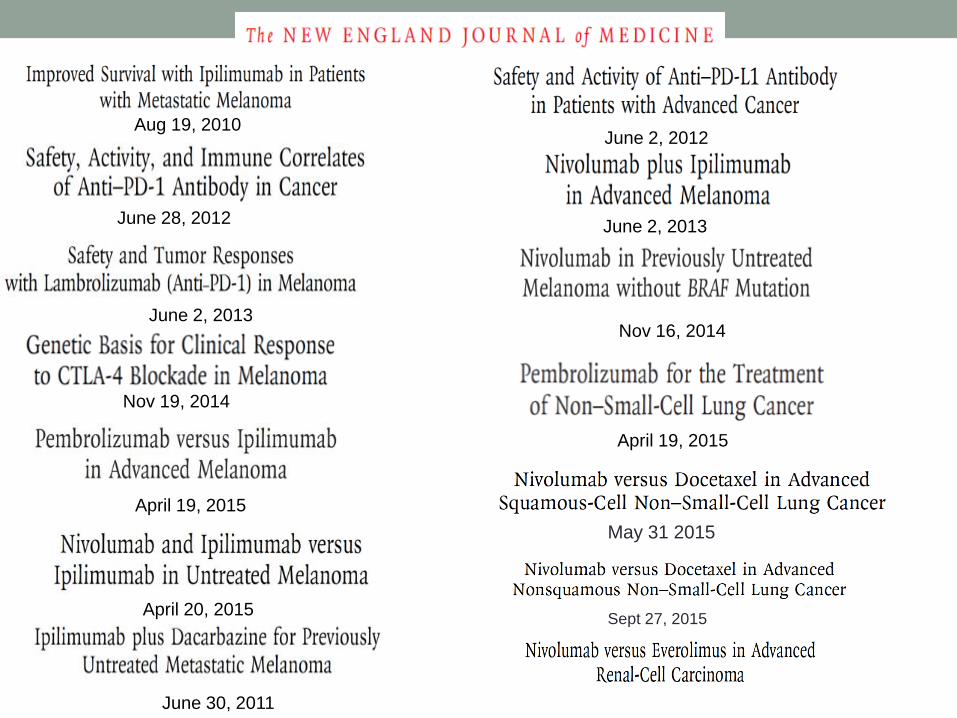
April 19, 2015
April 20, 2015
April 19, 2015
June 2, 2013
June 2, 2013
Nov 19, 2014
June 30, 2011
Nov 16, 2014
Aug 19, 2010June 2, 2012
June 28, 2012
May 31 2015
Sept 27, 2015

The challenge…

The challenge…
Unique Biology
• Patient selection
Unique drug development
• Patient selection
Unique Activity Patterns
• Patient management
• Go vs no-go decision
Unique toxicity
• Patient management

Adapted from The Cancer Genome Atlas Project: Govindan & Kondath et al Nature 2013
1 / Mb
10 / Mb
100 / Mb
0.1 / Mb
81 64 38 316 100 17 82 28n=109 119 21 40 20
Hematologic &
Childhood Cancers
Carcinogen-induced Cancers
?
?
Ad
en
oca
Squ
am
ous
Ovarian, Breast,
Prostate Cancers
Mutations
Per Mb DNA
UNIQUE BIOLOGY…Magnitude of Genomic Derangement Is Greatest In Melanoma and Lung
Cancer. This may contribute to increased inmunogenicity

UNIQUE DRUG DEVELOPMENTPembrolizumab Phase I Study as an illustration
• PN-001, Phase I study, began in 2011
• Initially a 32 patient study
• Actually enrolled over 1260 patients
• Became basis for FDA Breakthrough designation in
melanoma + lung cancer

UNIQUE ACTIVITY PATTERNS…
Ascierto AL, Frontiers in Oncol 2015

Tail of the curve best describes benefit
• Landmark or Milestone OS rates are better descriptors than mOS
• “Separation of the Curves” effect represents non-proportional HR
• Plateau typically begins about 18-24 mo and “flattens” by 36-48 mo
• Implications for Trial Design
• Better agents (combinations?) and/or selection of pts using predictive biomarkers may ultimately drive the best trial results
1. Adapted from Ribas A, presented at WCM, 2013
2. Ribas A, et al. Clin Cancer Res 2012;18:336–341
3. Drake CG. Ann Oncol 2012;23(suppl 8):viii41–viii46

CTLA-4 INHIBITORS:
IPILIMUMAB
TREMELIMUMAB

IPILIMUMAB

Immune Checkpoint Blockade: OS Demonstrated in Patients
With Advanced Melanoma
Anti-CTLA-4
T cell
CTLA-4PD-1
Anti-PD-1
aFor illustrative purposes; only select checkpoint molecules, select agents, and select data from 2 clinical trials are shown. OS, overall survival.
1. Hodi FS, et al. N Engl J Med. 2010;363:711-723. 2. Atkinson V et al. Presented at SMR 2015.
Phase 3 data with IPI1
Ipilimumab + gp100 (n=403)
Ipilimumab (n=137)
Gp100 (n=136)
Pa
tie
nts
Ali
ve (
%)
Years
0
20
40
60
80
100
0 1 2 3 4
In pretreated patients

Advanced melanoma: ipilimumab
Schadendorf JCO 2015
3 yr OS rate: 22%

CTLA-4 Immune Checkpoint Inhibition for
Advanced Melanoma
• Ipilimumab is the only approved CTLA-4 checkpoint
inhibitor1
• Data showed durable, long-term survival benefit in patients
with advanced melanoma2,3
• Antitumor activity across patient subgroups and irrespective
of prior therapy or BRAF status4,5
• Associated with immune-mediated adverse reactions that
can be serious, but most are reversible using established
management guidelines5
1. Camacho LH. Cancer Med 2015;4:661-672. 2. Schadendorf D, et al. J Clin Oncol. 2015;33:1889-1894. 3. Maio M, et al. J Clin Oncol. 2015 33:1191-1196. 4. Page DB, et al. Curr Oncol Rep. 2013;15:500-508. 5. Wolchok JD, et al. Ann NY Acad Sci. 2013;1291:1-13.

IPILIMUMAB IN NSCLC
R Phase II CA184-041
Lynch T, J Clin Oncol 2012
Phased ipilimumab regimen improved irPFSand OS in patients with squamous histology: HR: 0.55 (95% CI, 0.27-1.12) also in WHO-PFS
Ipilimumab for NSCLC: Randomized Phase II Study Design
• Primary Endpoint: Immune-related PFS (irPFS)
• Exclusion Criteria – Prior treatment for lung cancer
– Brain metastases
– Autoimmune disease
– P/C: 175 mg/m2 paclitaxel + AUC = 6 carboplatin q 3 weeks x 6 doses
– Concurrent ipilimumab: 10 mg/kg q 3 weeks x 4 doses
– Phased ipilimumab: Placebo q 3 weeks x 2 doses followed by IPI q 3 weeks x 4 doses
Chemotherapy
-naïve stage
IIIB/IV NSCLC
(N = 204)
R A N D O M I Z E
Concurrent ipilimumab
+ P/C (n = 70)
Phased ipilimumab
+ P/C (n = 68)
Placebo + P/C (n = 66)
1:1:1
Ipilimumab q 12 weeks
Ipilimumab q 12 weeks
Placebo q 12 weeks
Lynch TJ, et al. J Clin Oncol. 2012;30(17):2046-2054.
Maintenance

PD-1 AND PD-L1 INHIBITORS:NIVOLUMAB
PEMBROLIZUMAB
ATEZOLIZUMAB
DURVALUMAB
AVELUMAB

NIVOLUMAB

Nivolumab Antitumor Activity
Melanoma
(n = 272)[1]
1. Weber JS, et al. Lancet Oncol. 2015;16:375-384. 2. Rizvi NA, et al. Lancet Oncol. 2015;16:257-265
3. McDermott DF, et al. J Clin Oncol. 2015;[Epub ahead of print]. 4.Ansell SM, et al. N Engl J Med. 2015;372:311-319.
Advanced NSCLC
(N = 117)[2]
Advanced RCC
(N = 34)[3]
Hodgkin’s Lymphoma
(N = 23)[4]
125100
7550250
-25-50-75
-100Ma
x C
ha
ng
e i
n T
arg
et
Le
sio
ns
Fro
m B
L (
%)
Pts
100
75
50
25
0
-25
-50
-75
-100Ma
x C
ha
ng
e i
n T
arg
et
Le
sio
ns
Fro
m B
L (
%)
Pts
Alive
Dead
Confirmed responders
100
50
0
-59
-100Ma
x C
ha
ng
e i
n T
um
or
Bu
rde
n F
rom
BL
(%
) 150
1 mg/kg nivolumab
10 mg/kg nivolumab
Pts
100
-50-60
-40
-70-80-90
-100Ma
x C
ha
ng
e i
n T
um
or
Bu
rde
n F
rom
BL
(%
)-30-20-10
Pts
Stable
DiseasePartial Response
Complete
Response

Immune Checkpoint Blockade: OS Demonstrated in Patients
With Advanced Melanoma
Anti-CTLA-4
T cell
CTLA-4PD-1
Anti-PD-1
aFor illustrative purposes; only select checkpoint molecules, select agents, and select data from 2 clinical trials are shown. OS, overall survival.
1. Hodi FS, et al. N Engl J Med. 2010;363:711-723. 2. Atkinson V et al. Presented at SMR 2015.
2-yr OS=26.7%
Pro
ba
bil
ity
of
Su
rviv
al
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0 3 6 9 12 15 18 21 24 27 30
Overall Survival (Months)
2-yr OS=57.7%
NIVO 3 mg/kg Q2W (n=210)
Dacarbazine (n=208)
Phase 3 data with NIVO2
In treatment-naïve patients

RENAL CANCER
Motzer et al. NEJM 2015

NSCLCOS in Nivolumab phase 1 (3yrs FU)
• Pts were heavily pretreated; 54% had 3–5 prior
therapiesGettinger, JCO. 2015.


A phase III study (CheckMate 017) of nivolumab vs docetaxel in previously treated advanced or metastatic squamous (SQ) cell non-small cell lung cancer (NSCLC).
Brahmer J et al. N Engl J Med 2015

Nivoluma
b
(n = 292)
Docetax
el
(n = 290)
mOS, mo 12.2 9.4
HR = 0.73 (96% CI: 0.59, 0.89); P =
0.0015
Phase III, randomized trial (CheckMate 057) of nivolumab(NIVO) versus docetaxel (DOC) in advanced non-squamous cell (non-SQ) non-small cell lung cancer (NSCLC).
Nivolumab
(n = 292)Docetaxel
(n = 290)
mPFS,
mo
2.3 4.2
HR = 0.92 (95% CI: 0.77, 1.11); P = 0.3932
Borghaei H, et al. N Engl J Med 2015

OS by PD-L1 Expression

Nivolumab is FDA approved in unresectable or metastatic
melanoma with disease progression following ipilimumab (and
BRAF inhibitor if BRAF V600+) and in metastatic NSCLC on or after
progression with platinum-based chemotherapy and received
Breakthrough Therapy Designation for Hodgkin’s Lymphoma

ATEZOLIZUMAB

ATEZOLIZUMAB

Vansteenkiste et al. Ann Oncol 2015; 26 (suppl 6): abstr 14LBA
Atezolizumab monotherapy vs docetaxel in 2L/3L non-small cell lung cancer:
Primary analyses for efficacy, safety and predictive biomarkers from a
randomized phase II study (POPLAR)
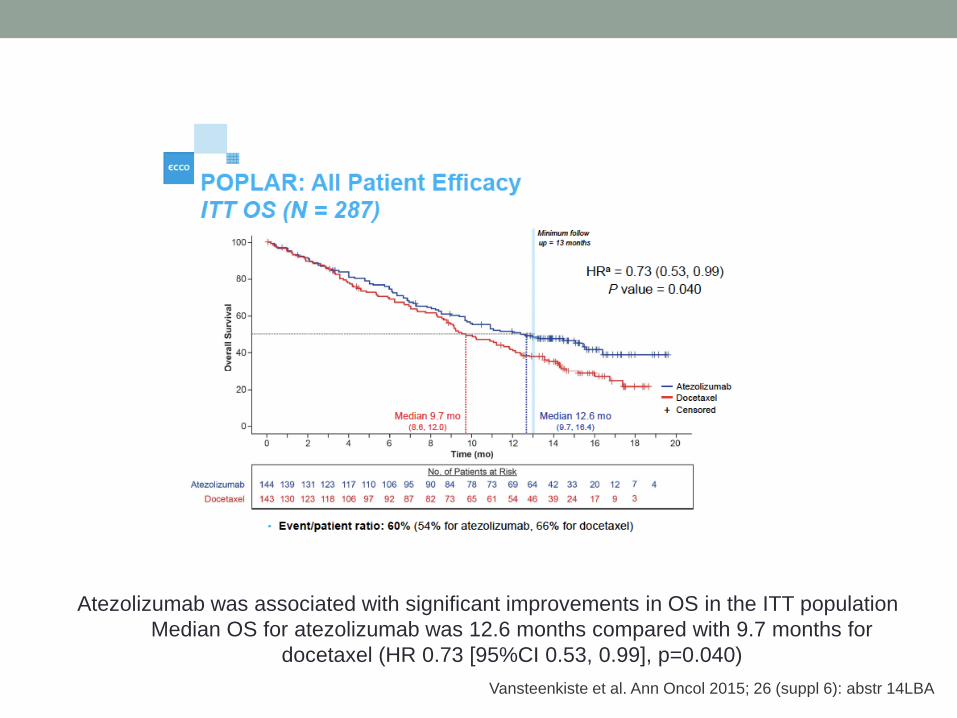
Vansteenkiste et al. Ann Oncol 2015; 26 (suppl 6): abstr 14LBA
Atezolizumab was associated with significant improvements in OS in the ITT population
Median OS for atezolizumab was 12.6 months compared with 9.7 months for
docetaxel (HR 0.73 [95%CI 0.53, 0.99], p=0.040)

• Patients with higher PD-L1 expression demonstrated improved
OS with atezolizumab
• Tumour cells and tumour-infiltrating immune cells were both
independent predictors of survival improvement with
atezolizumab
Vansteenkiste et al. Ann Oncol 2015; 26 (suppl 6): abstr 14LBA

PEMBROLIZUMAB

Pembrolizumab Antitumor Activity
1. Robert C, et al. Lancet. 2014;384:1109-1117. 2. Garon EB, et al. ESMO 2014. LBA43. 3. Chow LQ, et al. ESMO 2014.
LBA31. 4. O’Donnell P, et al. ASCO GU 2015. Abstract 296. 5. Muro K, et al. ASCO GI 2015. Abstract 03. 6. Nanda R, et al.
SABCS 2014. Abstract S1-09. 7. Moskowitz C, et al. ASH 2014. Abstract 290.
100806040200
-20-40-60-80
-100Ch
an
ge F
rom
Ba
se
lin
e
in S
um
of
La
rge
st
Dia
me
ter
of
Ta
rge
t L
es
ion
s (
%) Melanoma[1] (N = 411)
KEYNOTE-001100806040200
-20-40-60-80
-100
NSCLC[2] (N = 262)
KEYNOTE-001100806040200
-20-40-60-80
-100
HNSCC[3] (N = 61)
KEYNOTE-012
100806040200
-20-40-60-80
-100Ch
an
ge F
rom
Ba
se
lin
e
in S
um
of
La
rge
st
Dia
me
ter
of
Ta
rge
t L
es
ion
s (
%)
Urothelial Cancer[4]
(N = 33)
KEYNOTE-012
100806040200
-20-40-60-80
-100
Gastric Cancer[5]
(N = 39)
KEYNOTE-012
100806040200
-20-40-60-80
-100
TNBC[6] (N = 32)
KEYNOTE-012 100806040200
-20-40-60-80
-100
cHL[7] (N = 29)
KEYNOTE-013

PEMBROLIZUMAB
Estudio Keynote 001
Updated pooled analysis with
665 patients
• PFS: 4.4 meses
• OS: 22.8 meses

Estudio Keynote 001
Treatment-Naïve patients
• PFS: 13,8 meses
• OS: 31,3 meses

Estudio Keynote 006
30% LDH elevada
63% B-RAF WT
80% PD-L1 positivo
35% una línea previa

Estudio Keynote 006. OS (Second Interim Analysis)
1-year estimates of OS:
• 74.1% pembrolizumab 2w (HR 0.63, P<0.0005),
• 68.4% pembrolizumab every 3 weeks (HR 0.69, P = 0.0036)
• 58.2% ipilimumab




Pembrolizumab is FDA approved in unresectable or metastatic
melanoma and in metastatic NSCLC PD-L1 positive on or after
progression with platinum-based chemotherapy

Immune-mediated
adverse reactions
TOXICITY
Immune-mediated adverse reactions
Patient education for early
recognition
Early diagnosis
and appropriate
management essential to
minimise
life-threatening
complications
Systemic high-dose
corticosteroids
may be required for severe
events
Can be severe or
life-threatening; may involve
various organs
Result from increased or
excessive immune activity
Unless an alternate etiology
has been identified,
consider all signs and
symptoms

General health and performance status are important
when considering whether an individual patient
would tolerate one of the higher grade irAEs.
At present there is no test to predict likelihood of
toxicity with immunotherapy.

Let´s see an example
• 61 year old male
• Active smoker 50 packs/year
• May 2014: Stage IV Squamous Cell Lung Cancer
• cT4NxM1b (bilateral adrenal metastasis)
• 1st line: Platinum-Gemcitabine x 6 cycles: PD
• January 2015
• 2nd line Docetaxel: severe acute infusion reaction
• 09/06/2015: 1st dose Nivolumab 3mg/Kg



IN THE NEAR FUTURE...


Several Arguments for Combining
Immunotherapies

MELANOMA COMBO: PFS With the NIVO+IPI Regimen –
ITT Population (CheckMate 067)1,2
NIVO+IPI
(n=314)
NIVO
(n=316)
IPI
(n=315)
Median PFS, months
(95% CI)
11.5
(8.9–16.7)
6.9
(4.3–9.5)
2.9
(2.8–3.4)
HR (99.5% CI)
vs. IPI
0.42
(0.31–0.57)*
0.57
(0.43–0.76)*--
HR (95% CI)
vs. NIVO
0.74
(0.60–0.92)**-- --
*Stratified log-rank P<0.001 vs. IPI
**Exploratory endpoint
No. at Risk
314NIVO+IPI 173 151 65 11 1219 0
316NIVO 147 124 50 9 1177 0
315IPI 77 54 24 4 0137 0
0 6 9 12 15 183 21
NIVO
NIVO+IPI
IPI
Months
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Pro
po
rtio
n a
liv
e a
nd
pro
gre
ssio
n-f
ree
1. Larkin J, et al. N Engl J Med. 2015;373:23-34. 2. Wolchok JD, et al. Presented at ASCO 2015 abstract LBA1.

SCLCOverall survival: CheckMate 032
mOS = median OS; OS = overall survival; NR = not reached.
Nivolumab
3
n = 80
Nivolumab 1 +
Ipilimumab 3
n = 47
mOS,
months
(95% CI)
3.55
(2.66, 7.46)
7.75
(3.65, NR)
No. of
events
33 19
1-year OS rate = 47.5%
1-year OS rate = 27.1%
100
90
80
70
60
50
40
30
20
10
0
0 3 6 9 12 15 18
Nivolumab 1 + Ipilimumab 3
Nivolumab 3
Patients at risk
Nivolumab 3 mg/kg 80 26 16 14 6 4 0
47 32 13 6 2 1 0Nivolumab 1 mg/kg +
Ipilimumab 3 mg/kg
Time (Months)
OS
(%
)
Calvo E et al. ESMO 2015. Abstract #3098

If we talk about IO, check your enthusiasm
ONE SIZE DOES NOT FIT ALL
PATIENT SELECTION

How to select patients for IO?
• 62 years old male
• Active smoker 45 paq/year
• Routine medical check:
• Thorax X-ray: RUL mass
• CT scan: 5x3 cm RUL mass and a 13 mm traqueobronchial adenopathy
• PET-CT: multiple uptake sites including right parahilar right nodes, 3rd right rib, 7nd
left rib, lumbar, RUL mass and traqueobronchial adenopathy
• Stage IV Squamous Cell Carcinoma
• First line therapy CDDP/Gem
• Lung and costal progression after 3 cycles of platinum-doublet, ECOG 1

Randomized trials In NSCLC
Main activity data in 2nd line setting
Garon GB et al. Lancet. 2014.
Soria JC et al. Lancet Oncol 2015
Bramer J et al. NEJM. 2015.
Vansteenkiste J, et al. ECC 2015.
Herbst R. Lancet Oncol 2015
Docetaxel+Ram
ucirumab
vs Docetaxel
Revel Phase III
Dcoetaxel+Ninte
danib vs
Docetaxel
LumeLung 1
Phase III
Afatinib vs
Erlotinib
Lux-LUNG 8
Phase III
Nivolumab vs
Docetaxel
CheckMate
017 Phase III
Nivolumab vs
Docetaxel
CheckMate 057
Phase III
Pembrolizumb
vs Docetaxel
KeyNote 010
Phase III
Atezolizumab
vs Docetaxel
Poplar
Phase II
ORR 23 vs 14% 4.7% vs 3.6% 5.5% vs 2.8% 20% vs 9% 19% vs 12% 18% vs 18% 15% vs 15%
PFS m 4.5 vs 3 4 vs 2.8 2.6 vs 1.9 3.5 vs 2.8 2.3 vs 4.2 3.9 vs 4 vs 4 2.7 vs 3
OS m10.4 vs 9.1
9.5 vs 8.2 (SCC)
12.6 vs 10.3
(Adenocarcinoma)7.9 vs 6.8 9.2 vs 6 12.2 vs 9.4m
10.4-12.7 vs 8.5 12.7 vs 9.7
10.1 vs 8.6
(SCC)
HR OS
HR PDL1-
HR PDL1+
0-86
0.883 (SCC)
NA
NA
0.83
NA
NA
0.81
NA
NA
0.59
0.70
0.50
0.73
0.87
0.40
0.71-0.61
NA
0.54-0.50
0.73
1.09
0.49

Toxicity…It can make a difference
Docetaxel+
Ramucirumab
vs Docetaxel
Revel
Afatinib vs
Erlotinib
Lux-Lung 8
Nivolumab vs
Docetaxel
CheckMate 017
Atezolizumab
vs Docetaxel
Poplar
Pembrolizumab
vs Docetaxel
KeyNote 010
Any 98% vs 95% 99.5% vs
97.5%
58% vs 86% 67% vs 88% 63% vs 81%
Gr 3-4 79% vs 71% 57.1% vs
57.4%
7% vs 55% 11% vs 39% 13% vs 35%
Gr 5 5% vs 6% 1.5% vs 1.3% 0 vs 2.1% 1 vs 2% -
Any AEs leading
to discontinuation
15% vs 8,8% 20.2% vs 17% 4% vs 10% 8% vs 22 % 4% vs 10%
Garon GB et al. Lancet. 2014.
Soria JC et al. Lancet Oncol 2015
Bramer J et al. NEJM. 2015.
Vansteenkiste J, et al. ECC 2015
Herbst R et al. Lancet Oncol 2015

Histology is not Predictive
RR
SQUAMOUS
CARCINOMA
NON-
SQUAMOUS
NIVOLUMAB 20% 19%
ATEZOLIZUMAB 27% 21%
PEMBROLIZUMAB 23.5% 18.7%
Bramer J et al. NEJM. 2015.
Borghaei H et al. NEJM. 2015.
Soria JC et al. ESMO 2014.
Garón et al. NEJM. 2015.

1L line, 2L line or beyond?
Besse B, et al. ECC 2015
66

SMOKING HISTORY

Rizvi N, et al. Science 2015.
Genomic landscape of lung cancers shape response to
anti-PD-1 therapy
Mutational landscape determines sensitivity
to PD-1 blockade in non-small cell lung cancer
• Whole-exome sequencing of NSCLC treated with Pembrolizumab
• In two independent cohorts, higher nonsynonymous mutation burden
in tumors associated with improved ORR, durable clinical benefit,
and PFS
• Efficacy also correlated with the molecular smoking signature, higher
neoantigen burden, and DNA repair pathway mutations

Oncogene addicted NSCLC
Broghaei et a. NEJM. 2015
Horn et al. WCLC 2013Hellmann et al. WCLC 2015

Human microbiome: gut – influence on
immunotherapeutic efficacy
Sivan. Science. 2015; Vetizou. Science. 2015.
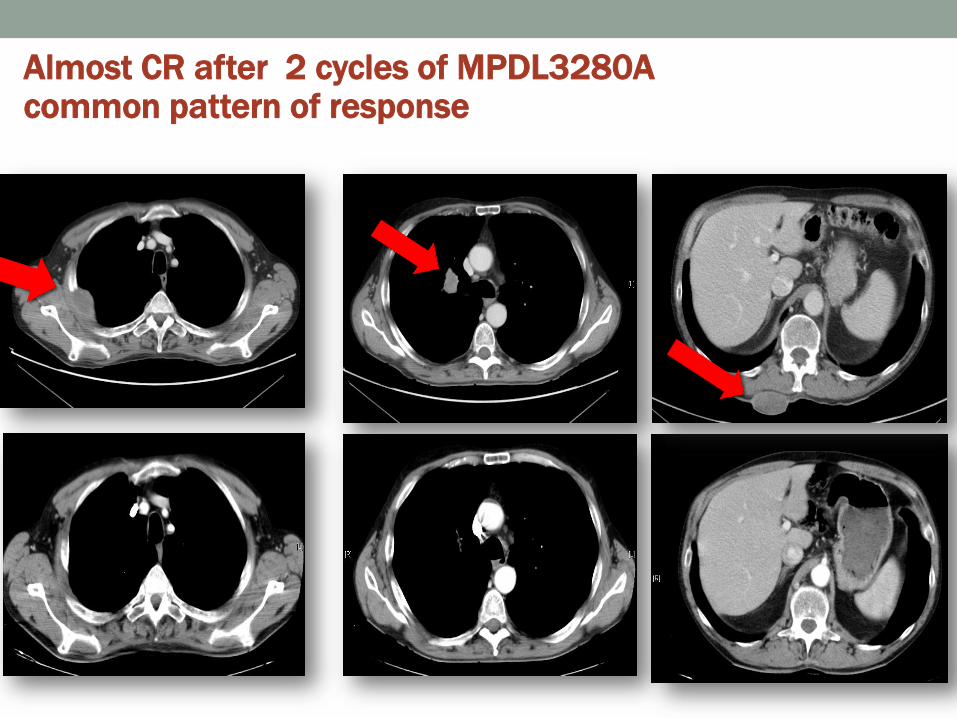
Almost CR after 2 cycles of MPDL3280Acommon pattern of response

Some take home messages
IO, THE CHALLENGE
• IO WORKS…AND IT WORKS REALLY WELL
• Patient selection for therapy: IT´S AN URGENT ISSUE
• Toxicity management:
• Physician education
• Patient education
• Early recognition and consideration: reinforce to patients the
importance of reporting any new or worsening symptoms

Conclusions:
Presented By Leonard Saltz at 2015 ASCO Annual Meeting
