l11 12.pulmonary tb
TRANSCRIPT

PULMONARY TUBERCULOSIS
DR.Bilal Natiq Nuaman,MD CABM,FIBMS,DIM 2016-2017
1

• Tuberculosis (TB) is caused by infection with Mycobacterium tuberculosis (MTB)
Burden of TB • TB is the seventh leading cause of death worldwide
2

• M. tuberculosis can cause disease in any organ of the body. •Multi-drug resistance (MDRTB) present in 102 of 109 countries surveyed from 1994-2003
3

Mycobacterium tuberculosis are gram positive aerobes and facultative intracellular pathogens, usually infecting mononuclear phagocytes.
Due to high lipid content in the cell wall, they are relatively impermeable and stain only weakly with Gram-stain. Where stained with dye combined with phenol and washed with acidic organic solvents, they resist decolorization and therefore are termed ‘acid-fast bacilli’.
4

5
Transmission• M. tuberculosis is spread by the inhalation
of aerosolized droplet nuclei from other infected patients. Once inhaled, the organisms lodge in the alveoli and initiate the recruitment of lymphocytes and macrophages.
6
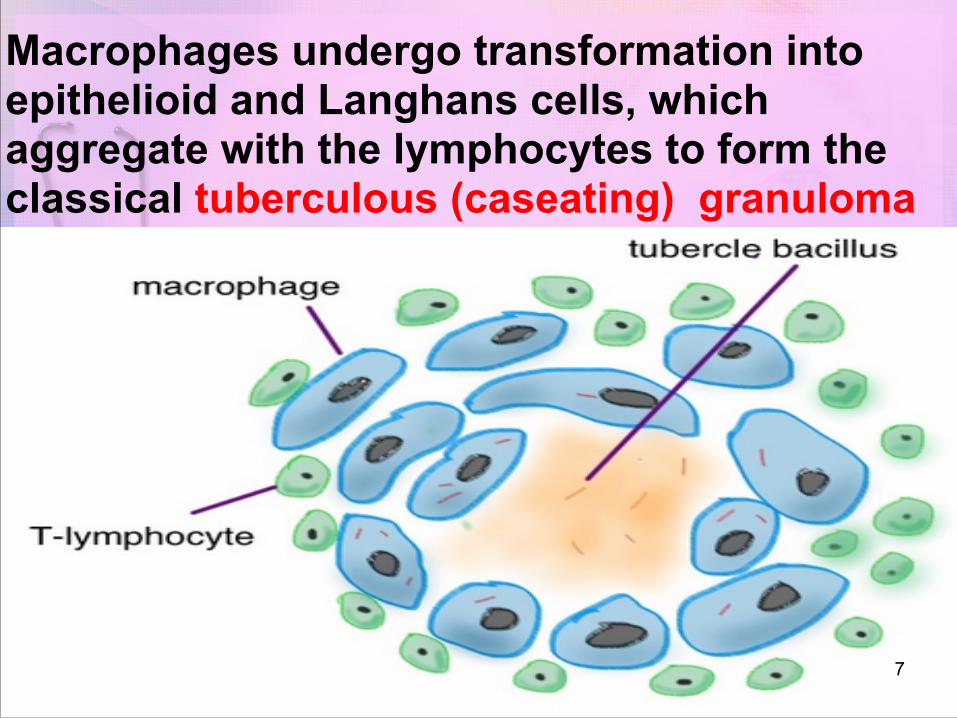
Macrophages undergo transformation into epithelioid and Langhans cells, which aggregate with the lymphocytes to form the classical tuberculous (caseating) granuloma
7

8

Inhalation of M. tuberculosis and deposition in the lungs leads to one of four possible outcomes:
• Immediate clearance of the organism (no disease)
• Latent infection • Immediate onset of active disease (primary
disease) • Onset of active disease many years
following exposure (reactivation disease)
9

Definitions● TB infection
● TB bacilli live inside the person, but the bacilli do not cause pathological destruction of organs
● No signs or symptoms of disease ● TB disease
● TB bacilli progressively invade an organ(s) ● Signs and symptoms of disease appear
10

● Pulmonary TB ● Disease involves the lung parenchyma ● Smear-positive: visible TB bacilli in
sputum ● Smear-negative: no visible TB bacilli in
sputum ● Extra-pulmonary TB
● Disease involving an organ other than the lung parenchyma
● Includes pleural TB11
Risk of Infection from Exposure• Exposure to:
• Persons who cough • Persons with sputum positive for acid-fast
bacilli • Persons not on TB treatment • Persons just started on TB treatment • Persons with a poor response to TB treatment
• Close contact, for long amounts of time, outside of natural sunlight (e.g., PRISON)
12

13

Diagnosis of TBMedical history
Physical examination
Investigations: Bacteriologic or histologic exam Mantoux tuberculin skin test Chest radiograph
14

MEDICAL HISTORY• Symptoms of disease
• History of TB exposure, infection.
• Past TB treatment
• Risk factors and Medical conditions that increase risk for TB disease.
15

16

17

18

19

Sputum for AFB and culture
• Zeil Nielson acid stain, 60% sensitivity• For diagnosis of pulmonary TB, obtain three
morning sputum specimens (sent for AFB smear and mycobacterial culture)
• 3 negative smears to assure low infectivity (Does not exclude TB)
• Culture most sensitive and specific test. But need more time 4-6 weeks
20

0.1 mL of 5-TU of purified protein derivative (PPD) solution injected intradermally Produce a wheal that is 6-10mm in diameter Read within 48-72 hours Measure induration, not erythema
Mantoux tuberculin skin test
21

False negatives • Severe TB (25% of cases negative) • Newborn and elderly • HIV (if CD4 count < 200 cells/ml) • Recent infection (e.g. measles) or immunization • Malnutrition • Immunosuppressive drugs • Sarcoidosis
False positives
• BCG vaccination
22

Interferon-gamma release assays (IGRAs)
• They are whole-blood tests that can aid in diagnosing Mycobacterium tuberculosis infection. IGRAs detect T-cell secretion of interferon-gamma (IFN-γ) following exposure to M tuberculosis-specific antigens (ESAT-6, CFP-10).
• They do not help differentiate latent tuberculosis infection (LTBI) from tuberculosis disease.
• IGRAs will replace the tuberculin skin test in low incidence, high-income countries.
23

The advantages of IGRAs • Requires a single patient visit to conduct the test. • Results can be available within 24 hours. • Prior BCG (bacille Calmette-Guérin) vaccination does not
cause a false-positive IGRA test result.
Disadvantages of IGRAs • Higher costs • Sophisticated equipment and need trained personnel.
24

CXR Findings
• Primary TB: • Lower or middle lobe infiltrates
• Reactivated TB: • Apical infiltrates/ cavitations
• Latent TB: • Usually normal
25

26

High ESR(≥50)
27

Clinical Forms of TB• Primary • Secondary or Reactivation • Miliary
28

29

30

31

32

33

Secondary Tuberculosis
• Reactivation occurs in 10-15% of patients; 1/2 within 2 years of primary disease
• The earliest radiological change is typically an ill-defined opacity situated in one of the upper lobes.
34
PrImary Tuberculosis is a typical acute systemic disease of children. secondary Tuberculosis is typically a chronic pulmonary disease of adults and children older than 10. It is due to reactivation of dormant bacilli due to a decrease in immunity or reinfection.The pulmonary lesions are apical and bilateral in distribution arising from bacilli that seeded to this site early in primary tuberculosis, which may have been many years previously. Apical lesions tend to be well ventilated, providing an environment rich in oxygen for the bacilli

35

Secondary Tuberculosis• Slowly Progressive (several months)• Worsening cough with sputum production• Low grade fever, night sweats, fatigue and
weight loss• CXR : apical lordotic apical cavities (without
fluid), • Cavitary disease very infectious. • Isolate all patients.
36

37

Miliary TB• risk for disseminated tuberculosis
1) Teenagers exposed to TB for the first time
2) Elderly patients with a past history of TB exposure
3) HIV patients with a past history of TB exposure.
38

Miliary TB Clinical Manifestations• Symptoms are nonspecific• - Moderate grade fever
Night sweats, Malaise and anorexia Weakness, Weight loss.
• Funduscopic exam - choroid tubercles• Laboratory - leukemoid reaction, anemia
abnormal LFTs• CXR - Micronodular interstitial pattern (millet
seeds)
39

choroid tubercles
40

41

• Diagnosis - blood cultures bone marrow culture Liver biopsy
• Treatment - Early therapy for all suspected cases (4 drugs)
42

Extrapulmonary tuberculosisCan occur in presence or absence of pulmonary TB The most common sites of involvement, in descending
order, are • pleura (with effusion),
• the lymph nodes (scrofula), • skeletal system (T11 and T12 vertebrae are most often
affected) (pott disease), • central nervous system, • Urogenital system • gastrointestinal tract, and
• Skin (lupus vulgaris) 43

44

Patients are not considered infectious if they meet all these criteria: • Received adequate treatment for 2-3
weeks • Favorable clinical response to treatment • 3 consecutive negative sputum smears
results from sputum collected on different days
➢Extrapulmonary TB (including pleural
effusion),and latent TB patients are not infectious
45

46
Treatment of TB Disease

47

Indications of corticosteroids in TBCorticosteroids reduce inflammation and limit tissue
damage, and are currently recommended when treating 1-pericardial or 2-meningeal disease, 3-children with endobronchial disease. 4-TB of the ureter, 5-pleural effusions , 6-extensive pulmonary disease, and 7-can suppress hypersensitivity drug reactions.
48

49

50

Latent TB Infection (LTBI) • Occurs when person breathes in bacteria and it
reaches the air sacs (alveoli) of lung Immune system keeps bacilli contained and under control Person is not infectious and has no symptoms
TB Disease • Occurs when immune system cannot keep bacilli
contained Bacilli begin to multiply rapidly Person develops TB symptoms
51

52

53

THANK YOU
54