kranti custody medicine - whatdotheyknow.com
TRANSCRIPT
Role of FMERole of FMECustody MedicineCustody Medicine
DrDr Kranti HiremathKranti HiremathMBBS, DRCOG, MFFP,MBBS, DRCOG, MFFP, DipFMDipFM
Forensic Medical ExaminerForensic Medical Examiner
Who is an FME /Who is an FME /Forensic PhysicianForensic Physician
•• Forensic Medical Examiner/ PoliceForensic Medical Examiner/ PoliceSurgeonSurgeon
•• Registered medical practitionerRegistered medical practitioner
•• Extra postgraduate qualifications inExtra postgraduate qualifications inother fields of medicineother fields of medicine
•• Forensic medicineForensic medicine
Duties of FMEDuties of FME
•• Medical care of detaineesMedical care of detainees
•• Forensic examinations ofForensic examinations of
•• Adults (victims and accused)Adults (victims and accused)
•• ChildrenChildren
•• Road traffic act (section 4 and 5)Road traffic act (section 4 and 5)
•• Liaising with fiscals, labs, other medicsLiaising with fiscals, labs, other medicssocial workerssocial workers
Liaison with the Forensic Physician regardingLiaison with the Forensic Physician regarding
the reason for attendancethe reason for attendance
•• Ideally the person with the query regarding a detained prisonerIdeally the person with the query regarding a detained prisoner shouldshould
call the FME (Forensic Medical Examiner)call the FME (Forensic Medical Examiner)
•• The FME will enquire why they are being called e.g. fitness to bThe FME will enquire why they are being called e.g. fitness to bee
detained / fitness to be interviewed / medication and whether thdetained / fitness to be interviewed / medication and whether there areere are
any other particular concern in order to asses the urgency of thany other particular concern in order to asses the urgency of the calle call
•• Priorities will be given to head injuries, drunks with head injuPriorities will be given to head injuries, drunks with head injuries,ries,
victims, medical problems, suspicious deaths and drink drivevictims, medical problems, suspicious deaths and drink drive
procedures etcprocedures etc
Briefing on arrivalBriefing on arrival
•• Discuss reason calledDiscuss reason called –– physical, mental illness, medication orphysical, mental illness, medication or
injuryinjury
•• Obtain details from the custody record including reason for arreObtain details from the custody record including reason for arrestst
•• Other information from custody sergeant and where appropriateOther information from custody sergeant and where appropriate
arresting officer regarding circumstances of arrestarresting officer regarding circumstances of arrest
•• Whether any force was used such as handcuffs, CS spray, batonsWhether any force was used such as handcuffs, CS spray, batons
etcetc
•• Whether anything was found in the detained prisonerWhether anything was found in the detained prisoner’’s property ors property or
when searched (medication, illicit drugs)when searched (medication, illicit drugs)
•• Police National Computer checks regarding mental illness, violenPolice National Computer checks regarding mental illness, violencece
and drugsand drugs
•• Information from General Practitioner, hospital, friends andInformation from General Practitioner, hospital, friends and
relatives as appropriaterelatives as appropriate
•• Any concerns regarding detained prisoners behaviour regardingAny concerns regarding detained prisoners behaviour regarding
Management PlanManagement Plan
•• Fitness for detentionFitness for detention
•• Fitness for interviewFitness for interview
•• Medical advice to detained prisonerMedical advice to detained prisoner
•• Medical advice to custody staffMedical advice to custody staff
•• RousingRousing
•• Medical advice to colleaguesMedical advice to colleagues
•• Need for appropriate adultsNeed for appropriate adults
•• Information regarding medicationInformation regarding medication
Appropriate AdultsAppropriate Adults
•• JuvenileJuvenile
•• Mentally disorderedMentally disordered
•• Learning disabilitiesLearning disabilities
•• Responsibility custody officerResponsibility custody officer’’ss
•• FME may make a recommendationFME may make a recommendation
Administration of medicationAdministration of medication
•• Detained prisoners own medication should be obtained if at allDetained prisoners own medication should be obtained if at allpossible (from home) for confirmationpossible (from home) for confirmation
•• The FME should leave clear instructions preferably verbally andThe FME should leave clear instructions preferably verbally and ininwritingwriting
•• Giving medication to a detained prisoner should be witnessed byGiving medication to a detained prisoner should be witnessed byanother officeranother officer
•• Detained prisoner should be observed taking medication to prevenDetained prisoner should be observed taking medication to preventthoardinghoarding
•• Consideration should be given to supervision of all injections bConsideration should be given to supervision of all injections by they theFMEFME
•• Medication logged in custody record when givenMedication logged in custody record when given
•• Refusal should be logged and the FME informedRefusal should be logged and the FME informed
•• Unused medication should be disposed of as instructedUnused medication should be disposed of as instructed
•• Medication should be kept in a locked cupboardMedication should be kept in a locked cupboard
•• Private prescriptions will be issuedPrivate prescriptions will be issued
•• Controlled drugs i.e. Methadone(exceptional cases only) must beControlled drugs i.e. Methadone(exceptional cases only) must beadministered by an FMEadministered by an FME
CommonCommon ProblemsProblems
•• EpilepsyEpilepsy
•• AsthmaAsthma
•• ClaustrophobiaClaustrophobia
•• DiabetesDiabetes
•• Heart diseaseHeart disease
•• Sickle cellSickle cell
•• InjuriesInjuries
•• AlcoholAlcohol
•• DrugsDrugs
•• Mental healthMental health
•• Infectious diseasesInfectious diseases
•• Fitness for interview,detention,release and court . oftenFitness for interview,detention,release and court . oftencombination of abovecombination of above
EpilepsyEpilepsy
•• Regular medicationRegular medication
•• Epilepsy or fits associated with alcohol / drug withdrawalEpilepsy or fits associated with alcohol / drug withdrawal
•• Fit in known epileptic / first fit everFit in known epileptic / first fit ever
EpilepsyEpilepsy
•• GeneralisedGeneralised seizuresseizures
•• Partial seizurePartial seizure
•• Type of epilepsy and frequency of fitsType of epilepsy and frequency of fits
•• Last fit medicationLast fit medication
•• ReliabilityReliability
•• Last doseLast dose
•• Appropriate treatment during custodyAppropriate treatment during custody
EpilepsyEpilepsy
•• Signs and symptomsSigns and symptoms
•• Management of a fitManagement of a fit
•• StatusStatus epilepticusepilepticus
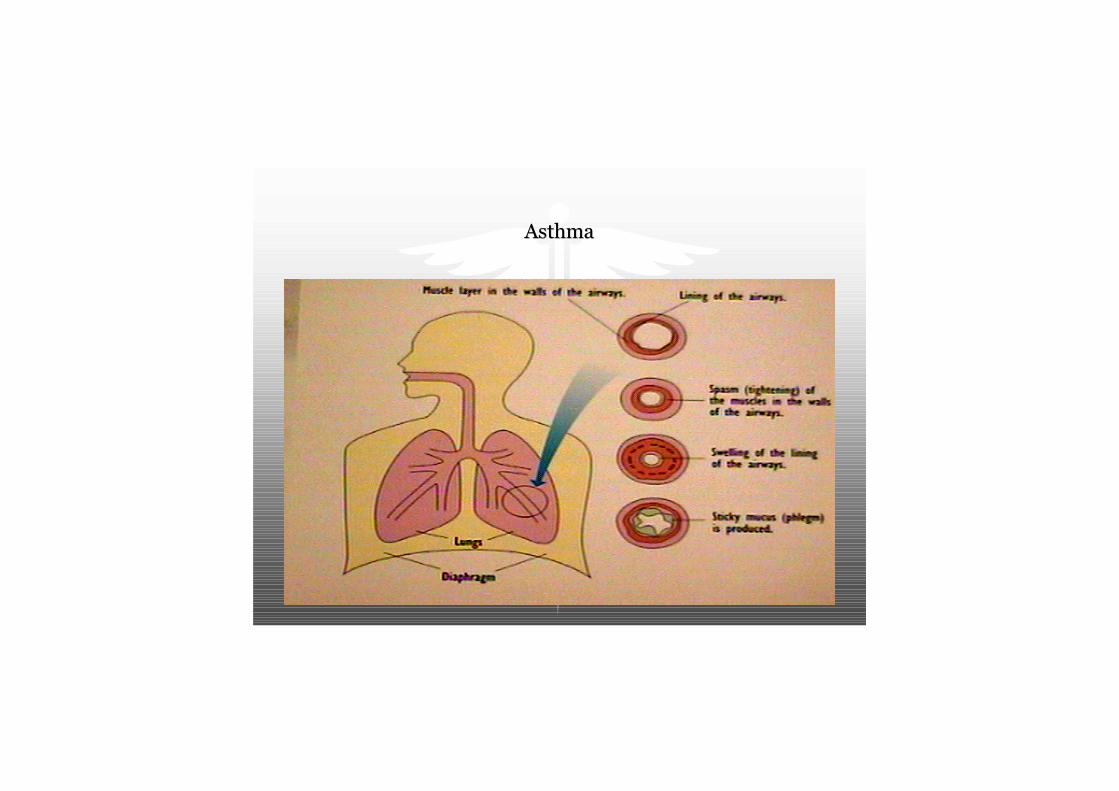
AsthmaAsthma
AsthmaAsthma
•• Wheeze and breathlessnessWheeze and breathlessness
•• Signs of concernSigns of concern
•• Repeated use of inhalers not relieving symptomsRepeated use of inhalers not relieving symptoms
•• Not able to speak easilyNot able to speak easily
•• Use of neck and shoulder musclesUse of neck and shoulder muscles
•• Less wheeze but increasing distressLess wheeze but increasing distress
AsthmaAsthma
•• THE SILENT ASTHMATIC IS A SICK ASTHMATICTHE SILENT ASTHMATIC IS A SICK ASTHMATIC
•• InhalersInhalers
•• Instructions on other medication if requiredInstructions on other medication if required
Panic AttacksPanic Attacks
•• Diagnosis on history (avoidance behaviour)Diagnosis on history (avoidance behaviour)
•• ReassuranceReassurance
•• Rarely medicationRarely medication
•• May affect fitness to interviewMay affect fitness to interview

InsulinInsulin

DiabetesDiabetes
•• TypesTypes -- IDDM and NIDDMIDDM and NIDDM
•• ComplicationsComplications
•• Major risks in custodyMajor risks in custody
•• HypoglycaemiaHypoglycaemia (low blood sugar)(low blood sugar)
•• HyperglycaemiaHyperglycaemia (high blood sugar)(high blood sugar)
•• TreatmentTreatment
DiabetesDiabetes
•• Using insulinUsing insulin –– obtain if possible and other medicationobtain if possible and other medication
•• Access to foodAccess to food
•• Consideration to the supervision of insulin injection. IDDM patiConsideration to the supervision of insulin injection. IDDM patientsents
should be seen by the Doctor.should be seen by the Doctor.
•• Awareness of hypoglycaemia / hyperglycaemiaAwareness of hypoglycaemia / hyperglycaemia
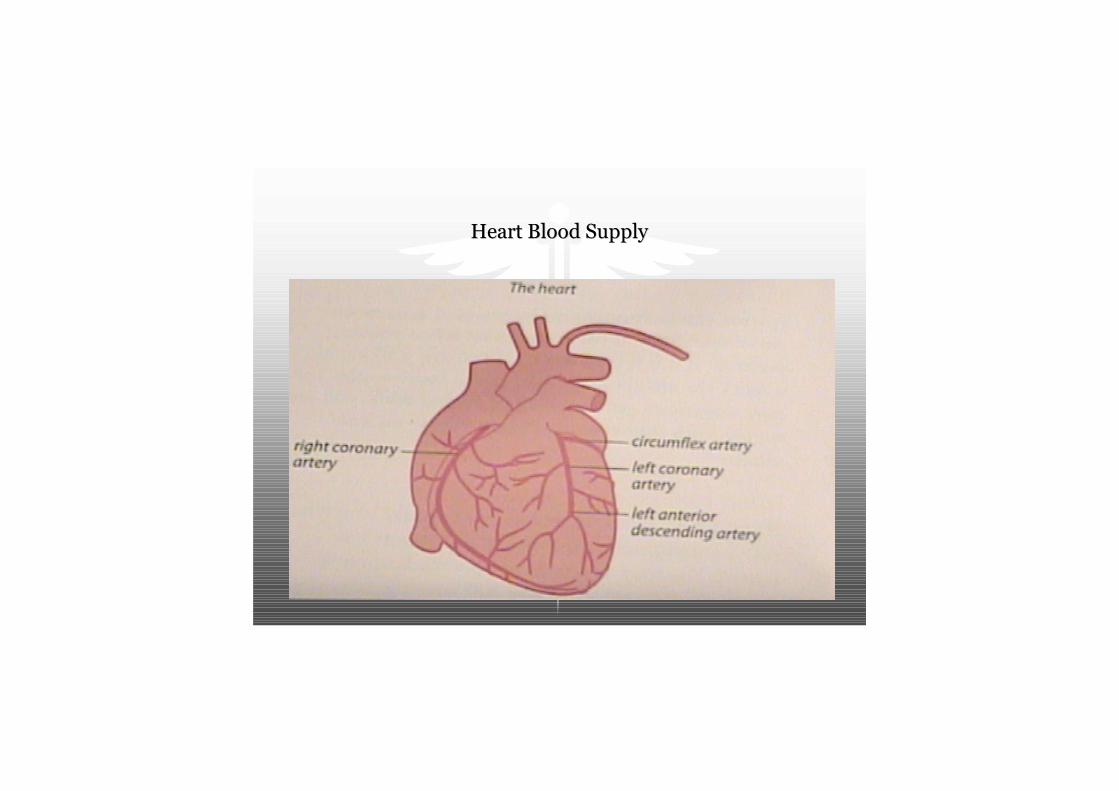
Heart Blood SupplyHeart Blood Supply
AnginaAngina
•• Signs and symptomsSigns and symptoms
•• TreatmentTreatment
Heart DiseaseHeart Disease
•• Access to medication such as GTN tablets or sprayAccess to medication such as GTN tablets or spray
•• If chest pain does not settle hospitalisation may be requiredIf chest pain does not settle hospitalisation may be required
Angina Heart AttackAngina Heart Attack
Sickle cellSickle cell
•• Disease or traitDisease or trait
•• Access to regular fluids (avoid dehydration)Access to regular fluids (avoid dehydration)
•• Avoid coldAvoid cold
•• May need painkillersMay need painkillers

InjuriesInjuries
•• Use of personal safety equipmentUse of personal safety equipment –– CS spray, handcuffs and batonsCS spray, handcuffs and batons
•• Complete accurate documentation important for medical and legalComplete accurate documentation important for medical and legal
reasonsreasons
•• Dog bitesDog bites –– may need hospital treatment, tetanus, antibiotics, follow upmay need hospital treatment, tetanus, antibiotics, follow up

Head injuryHead injury
•• Important to get accurate history from arresting officer beforeImportant to get accurate history from arresting officer before hehe
disappears!disappears!
•• Was there loss of consciousness or bleeding from any orifices?Was there loss of consciousness or bleeding from any orifices?
•• Symptoms of concussion (increasingly drowsy, increasing headacheSymptoms of concussion (increasingly drowsy, increasing headache,,
blurred or double vision, vomits, fits, becomes unconscious or oblurred or double vision, vomits, fits, becomes unconscious or otherther
unusual symptoms)unusual symptoms)
•• Remember dangerous combinations e.g. head injury and alcohol andRemember dangerous combinations e.g. head injury and alcohol and
or drugs and other medical problems such as diabetesor drugs and other medical problems such as diabetes
•• Instructions:Instructions: -- Take the patient to hospital by ambulanceTake the patient to hospital by ambulance
AlcoholAlcohol -- IntoxicationIntoxication
•• ConsiderConsider -- use of drugs and other medical problems including a headuse of drugs and other medical problems including a head
injuryinjury
•• If in doubt call an FMEIf in doubt call an FME
•• Check and rouse every half an hourCheck and rouse every half an hour
•• Dependent may sober up very quickly and develop withdrawalDependent may sober up very quickly and develop withdrawal
symptomssymptoms
AlcoholAlcohol -- WithdrawalWithdrawal
•• May be complicated by fitsMay be complicated by fits
•• May need treatment depending on length of detentionMay need treatment depending on length of detention
DrugsDrugs
•• Knowledge of drug trends in your areaKnowledge of drug trends in your area
•• Be aware that substance use and mental illness may coBe aware that substance use and mental illness may co--existexist
•• ProblemsProblems –– Hypoglycaemia, dehydration, polydrug misuse, alcohol,Hypoglycaemia, dehydration, polydrug misuse, alcohol,
nonnon--truthful history and other illnessestruthful history and other illnesses
OpiatesOpiates –– Heroin / MethadoneHeroin / Methadone
•• Main problem medical intoxication (drowsy, decreasing level ofMain problem medical intoxication (drowsy, decreasing level of
consciousness, pinconsciousness, pin--point pupils, respiration level falls, snoring)point pupils, respiration level falls, snoring)
•• Combination with other drugs and alcohol potentially dangerousCombination with other drugs and alcohol potentially dangerous
•• Withdrawal less of a problem but can be treated in custody, mayWithdrawal less of a problem but can be treated in custody, may affectaffect
fitness to be interviewedfitness to be interviewed
•• Intravenous misusers may suffer from abscesses, HIV, Hepatitis BIntravenous misusers may suffer from abscesses, HIV, Hepatitis B andand
Hepatitis CHepatitis C –– Discuss with the FMEDiscuss with the FME
BenzodiazepinesBenzodiazepines
•• Intoxication similar to alcoholIntoxication similar to alcohol
•• Fits may occur with withdrawalFits may occur with withdrawal
StimulantsStimulants –– Cocaine / AmphetamineCocaine / Amphetamine
•• Death may occur from cardiac problems, stroke, cocaine agitatedDeath may occur from cardiac problems, stroke, cocaine agitated deliriumdelirium
•• WithdrawalWithdrawal –– risk of selfrisk of self--harmharm
PregnancyPregnancy
•• Discuss with the FME regarding fitness to be detained especiallyDiscuss with the FME regarding fitness to be detained especially if onif on
medication and in 3medication and in 3rdrd trimester of pregnancytrimester of pregnancy
Infectious diseasesInfectious diseases
•• Hepatitis B vaccination for officersHepatitis B vaccination for officers
•• Risks mainly needle stick injuriesRisks mainly needle stick injuries
•• High risk population for HIV, hepatitis B and C (iv drug users)High risk population for HIV, hepatitis B and C (iv drug users)
•• Observe good clinical practiceObserve good clinical practice –– wear gloves, beware when searchingwear gloves, beware when searching
•• Tuberculosis, other infections diseases continue treatment, consTuberculosis, other infections diseases continue treatment, considerider
hospitalisationhospitalisation
•• Scabies can be treated in custodyScabies can be treated in custody
•• Cells and bedding cleaned professionallyCells and bedding cleaned professionally

Mental HealthMental Health
•• Call an FME if concerns regarding mental healthCall an FME if concerns regarding mental health
•• Risk of selfRisk of self--harmharm –– history of previous attempts and past psychiatrichistory of previous attempts and past psychiatric
history importanthistory important
•• Remove articles that could be used for deliberate selfRemove articles that could be used for deliberate self--harmharm
•• May need constant supervisionMay need constant supervision
•• Liaison with other agencies when detained prisoners transferredLiaison with other agencies when detained prisoners transferred
Mental HealthMental Health
•• Abnormal mental state may have a variety of causes:Abnormal mental state may have a variety of causes:
DepressionDepression
SchizophreniaSchizophrenia
Bipolar disorderBipolar disorder
Personality disorderPersonality disorder
Learning disabilityLearning disability
Substance misuserSubstance misuser
Substantial RiskSubstantial Risk -- TemporaryTemporary
•• DrunkennessDrunkenness
•• Intoxication by drugsIntoxication by drugs
•• Severe drug withdrawalSevere drug withdrawal
•• Severe exhaustion or physical painSevere exhaustion or physical pain
•• Severe physical illnessSevere physical illness
•• Severe mental illness that may be amenable to treatment such asSevere mental illness that may be amenable to treatment such as anan
acute organic reaction or maniaacute organic reaction or mania
•• A state of fear induced by police contactA state of fear induced by police contact
Significant RiskSignificant Risk(Appropriate Adult would be required)(Appropriate Adult would be required)
•• HypomaniaHypomania
•• Schizophrenia and related disordersSchizophrenia and related disorders
•• Depressive illnessDepressive illness
•• Mild or moderate learning disabilityMild or moderate learning disability
•• Mild to moderate dementiaMild to moderate dementia
•• Inability to handle interrogative pressureInability to handle interrogative pressure
•• Significant anxiety induced by custodial environment and other aSignificant anxiety induced by custodial environment and other anxietynxiety
states and phobias, such as fear of being locked in a police celstates and phobias, such as fear of being locked in a police celll
Medical risk factorsMedical risk factors
•• Sickle cell diseaseSickle cell disease
•• Absent spleenAbsent spleen
•• Kidney problemsKidney problems
•• ImmunosuppressedImmunosuppressed
•• Heart conditionHeart condition
•• Lung diseaseLung disease
•• Liver diseaseLiver disease
•• DiabeticDiabetic
•• Drug ingestion(claims overdose and alcohol)Drug ingestion(claims overdose and alcohol)
When to hospitaliseWhen to hospitalise
•• Difficult to give clear guidance for every situation (see below)Difficult to give clear guidance for every situation (see below)
•• If in doubt trust your instincts and call an ambulanceIf in doubt trust your instincts and call an ambulance
•• If not sure call the FME for adviceIf not sure call the FME for advice
•• Err on the side of cautionErr on the side of caution
Remember (Hospitalisation)Remember (Hospitalisation)
•• Chest painChest pain
•• Breathing difficultiesBreathing difficulties
•• Level of consciousnessLevel of consciousness
•• Severe injuriesSevere injuries –– head injuries with loss of consciousness, deformedhead injuries with loss of consciousness, deformed
limbs, wounds that obviously need suturinglimbs, wounds that obviously need suturing
Deaths In Police CustodyDeaths In Police Custody
•• Deliberate self harm single most common cause of deathDeliberate self harm single most common cause of death
•• Substance abuse and medical conditions = another half of deathsSubstance abuse and medical conditions = another half of deaths
•• Police restraint = 6% associated with underlying medical conditiPolice restraint = 6% associated with underlying medical conditionsons
DrugsDrugsAnyone Suspected of ingesting substantial amount ofAnyone Suspected of ingesting substantial amount of
drugs needs to be evaluated at a hospitaldrugs needs to be evaluated at a hospitalThe need isThe need is NOT DIMINISHEDNOT DIMINISHED even if such claims areeven if such claims are
made to avoid detentionmade to avoid detentionViolent, agitated prisoners should be transported toViolent, agitated prisoners should be transported to
hospital in an ambulance especially due to drugshospital in an ambulance especially due to drugs

Clinical well being is the primary concernClinical well being is the primary concern