knowledge translation: developing evidence - c.ymcdn.comc.ymcdn.com/sites/ · knowledge...
TRANSCRIPT

Knowledge Translation: Developing Evidence‐Based Clinicians in Home Care
Speaker(s): Matt Janes, PT, DPT, MHS, OCS, CSCS
Derek Nordman, MPT, ATC Laurie Otis, PT, MBA, MHA, GCS, COS‐C Patricia Scheets, PT, DPT, MHS, NCS
Session Type: Educational Sessions Session Level: Multiple Level This information is the property of the author(s) and should not be copied or otherwise used without the express written permission of the author(s).
www.homehealthsection.org
Home Health Section of the American Physical Therapy Association
Page 1 of 20 total pages

KT - Janes, Nordman, Otis, Scheets 1
Knowledge Translation:
Developing Evidence-Based
Clinicians in Home Care
Matt Janes, PT, DPT, MHS, OCS, CSCS
Derek Nordman, PT, MPT, ATC
Laurie Otis, PT, MBA, MHA, GCS, COS-C
Patty Scheets, PT, DPT, MHS, NCS
Disclosure
• Matt Janes - No relevant financial relationship exists
• Derek Nordman - No relevant financial relationship exists
• Laurie Otis - No relevant financial relationship exists
• Patty Scheets - No relevant financial relationship exists
Objectives
• At the end of this section, the participant will: – Understand the systematic approach of KT applied in the
initiative and the intent of accelerating optimal use of the best available research evidence
– Describe rehabilitation as a means for developing skill in home health practice
– Describe evidence-based task-specific training principles
– Apply observational analysis during the patient examination when identifying the cause of the patient’s activity limitations
– Recognize the value of using standardized tests in clinical practice
– Identify strategies to increase intensity of a treatment session in order to maximize progress
Company
• Gentiva Health Services
• 40 States
• Greater than 200 locations nationwide
• Over 350,000 patients served/year
• Over 2500 therapy clinicians
• Proprietary Specialty offerings
• Oversight by Rehab Director
The Need
• Not unlike most Home Health Agencies – “Do more with
less.”
• Efficiency and Consistency in clinical care
• Increase the utilization of EBP
– Evaluation
– Activity and Participation Limitation Identification
(by task specific practice)
– Proper Intensity of the Intervention
– Leading to proper documentation of patient progress and
outcome
• Pre-training clinical documentation review conducted within 5 branches
to allow post-training analysis.
The Aim
Support and re-energize our therapy
field leaders and clinicians by
delivering immediate updates to
specialty content and clinical skills
based on latest science, in a way
that allow for immediate adoption into practice.

KT - Janes, Nordman, Otis, Scheets 2
The Formula
• Five questions to be answered as posed by
Grimshaw et al
1. What knowledge should be transferred?
2. To whom should the research knowledge be
transferred?
3. By whom should the knowledge be transferred?
4. How should the knowledge be transferred?
5. With what effect should knowledge be
transferred?
Grimshaw et al. Knowledge translation of research findings. Implementation Science. 2012 7:50.
What knowledge should be transferred?
• Evidence Based Best Practice
• Skilled Examination and Evaluation
• Task Specific Practice
• Intervention Intensity
• Documentation
To whom should the research
knowledge be transferred?
• Direct to consumer! – Alternative to “Train the Trainer”
1. Clinical Leaders
(Branches with Rehab Director oversight)
2. Direct to Clinician
By whom should the knowledge be
transferred?
• Company Experts (controlled consistency)
oMatt Janes, PT, DPT, MHS, OCS, CSCS
o Laurie Otis, PT, MBA, MHA, GCS, COS-C
o Patty Scheets, PT, DPT, NCS
o Jennifer Ellis, PT, DPT, MS, GCS, COS-C
– Did allow secondary trainings at the clinician level via
Directors of Clinical Operations and Rehab Directors
How should the knowledge be
transferred?
• Stakeholder Buy-in
• Virtual Classroom
• Bite size doses
• Over a 5 month period (June through September)
• Knowledge checks modules (virtual feedback/response)
• Application learning – Mini “Labs”
• Clinical Support Tool “Gentiva Therapy Guide”
• Recorded Sessions for availability – Module 1 – 2758
– Module 2 – 2441
– Module 3 – 2146
• Post-training follow up
With what effect should knowledge be
transferred?
• Behavior Change
– Adoption of Evaluative Testing
– Activity and Participation Limitation Identification
(by task specific practice)
– Inclusion of Intensity Validation
– Post training documentation analysis

KT - Janes, Nordman, Otis, Scheets 3
Knowledge-to-Action Process
Graham ID, Logan J, Harrison MB, et al J of Cont Education for Health Professions. 2006; 26: 13-24.
Knowledge Translation:
Task Specific Training
Laurie Otis, PT, MBA, MHA, GCS, COS-C
Skill Acquisition
Consistency
• Performance over multiple trials or sessions
Flexibility
• Performance under a variety of conditions
Efficiency
• Performance with a certain level of energy expenditure
Independent and Skilled?
DAILY ACTIVITY
• Picks up the newspaper after 7:00 AM and the mail
before 4:00 PM if delivered timely
• Ambulating with a single point cane without assistance to
and from the mailbox at the end of a 50’
driveway
• Negotiates 2 steps to go in and out of the
house
– Grasps door frame for balance and support
– Rests in a chair after negotiating the steps
• Completes the entire activity in 20 minutes
• Rates the activity a 13 on the BORG
(perceived exertion)
Task-Specific Training Defined
• What is a Task?
– Space between Body Structure/Function and Activity
• Body Structure/Function = muscle performance, timing, and balance
• Activity = walking from the living room to the kitchen for dinner and
returning to the living room
• What is Task-Specific Training?
– Goal directed
– Coordinated movements and/or sustained postures
– Replicate some component of daily activities
– Aim towards reconstruction of the whole activity
– Reinforced with positive and timely feedback
ICF Model
Common language and nomenclature for
functioning, disability and health (WHO)

KT - Janes, Nordman, Otis, Scheets 4
Task Specific Training Continuum
Activity Limitation Walk down steps and transfer into senior
citizens’ van UB grooming and dressing
Task Space
Stair Tap Containers and Lids
Impairment
Hip Abductor Weakness Impaired Spatial Organization
Principle - Task Selection
Task Selection
Meaning and Fit
Applicable to the
Patient
Goal Directed
Targeted to Impairment
Sufficient Challenge
Principle - Task Delivery
Task Delivery
Set the Task Parameters
Focus on the desired impairment
Remediation or
Compensation
Tasks Need to Be Practiced
Monitor Response
Progress the
Challenge
Task Specific options
Sit to Stand
• Task used in wide range of activities
• Task demands:
– Force production at initiation
– Control of inter-segmental movement and shifting COM during
execution
– Ability to stabilize in a new position at termination
Sit to stand patient profiles
• Cardiopulmonary Demand
• Task Parameters • Raise seat height to diminish demand on
skeletal muscle; Repeated trials
• Borg RPE; Total min tolerated; Vitals; Dyspnea level
Cardiopulmonary - CHF
• Strength and ROM Demand
• Task Parameters • Strengthening Paradigm
• BORG RPE; Time to Complete; Timed; Pain
Musculoskeletal – Spinal Stenosis with Functional
Decline
• Balance and Strength Demand
• Task Parameters • Compliant surface to increase balance
demand
• 2-3 trials interspersed w/other activities (balance paradigm)
• X LOB; BoS; Time to Complete; Timed
Neuromuscular - DM with
Peripheral Neuropathy

KT - Janes, Nordman, Otis, Scheets 5
Group Question - Sit to Stand Task
Musculoskeletal
• TKA – Quad weakness
• Strength Demand
• Remediation
1. Which phase of the task has the greatest strength demand?
2. What surface height is most appropriate to encourage
quad recruitment, High Medium or Low?
3. Will you allow UE support, Yes or No?
4. What will you monitor?
5. How will you progress the task?
Task - Stair Tap
• Preparation for obstacle
negotiation, stairs, and change of
direction during ambulation
• Task demands:
– Stance limb: force production
(isometric) of extensors and balance
– Swing limb: force production of hip
flexors and timing to place foot on
step
Patient Profile – Stair Tap
• Cardiopulmonary Demand
• Task Set Up • Adjust step height; Alternate sides
• Duration focus
Cardiopulmonary - CHF
• Posture and Timing Demand
• Task Set Up • Adjust step height; Fewer repetitions
• Cues for trunk stabilization
• Sit between sets
Musculoskeletal - Functional Decline with
Spinal Stenosis
• Balance and Timing Demand
• Task Set Up
• Alternate sides; compliant surface
• Cues for postural correction
Neuromuscular - DM with
Peripheral Neuropathy
More LE Task Ideas
Tandem Balance: Step
Up / Up; Down / Down
Step Over
Step Up / Up; Down / Down
UE Tasks
• Variability in what we do with our hands
– Reach
– Grasp
– Move or manipulate
– Release
• What is realistic for the patient’s ability given their
impairment
– Grade task so that it takes 8-15 s
TASK - Object Transport
• Element common across many
ADL/IADLs
• Task demands:
– ROM and strength proximally
(including trunk)
– Isolated movement distally
– Cardiopulmonary demand with
repeated UE movement
– Problem solving

KT - Janes, Nordman, Otis, Scheets 6
Patient Profile – Object Transport
• Cardio Demand
• Task Set Up • Weight of object; Movement height
• Unilateral or Bilateral; Repeated Trials
Cardiopulmonary - CHF
• Posture Demand
• Task Set Up • UE Movement Pattern
• Weight of object; Trunk position
Musculoskeletal – Functional Decline
with Spinal Stenosis
• Balance and Timing Demand
• Task Set Up • Compliant surface
• Movement speed; COM displacement
Neuromuscular – DM with Peripheral
Neuropathy
Overall Considerations for
Task Specific Training
• Progress the challenge based
on desired outcome
• Monitor response to treatment
in a single session and across
sessions
• Identify overall progress
towards functionally based
goals using objective
measures
Challenge of the task
Task Performance (consistency; flexibility; efficiency)
Making it Work for YOU in Your Practice
• Adopt a new routine
1. Rehabilitation is about skill acquisition
• Maximize consistency, flexibility and efficiency
2. Make Task-Specific Training your priority intervention
• Differentiate what you do in treatment
from the home program
3. Develop a new task that fits with your
patient’s specific needs
Take a Closer Look
Patty Scheets, PT, DPT, MHS, NCS
The Therapist’s Clinical Examination
• Quantitative Analysis
• Qualitative Analysis
• Body Functions and Structures
• Systems Review
• Drug Regimen Review
Health Status
Impairment Tests
Standardized Measures
Observational Analysis
Standardized Measures
Baseline data for scoring
Interpretative comments from observational analysis
TUG • Sit ↔ stand; Turn to change direction
BERG
• Stair tap; Pick object up from the floor
SPPB • Sit ↔ stand; Standing balance progression

KT - Janes, Nordman, Otis, Scheets 7
Observational Analysis
• Kinematic analysis
• Changes in joint angles and limb displacement
• Timing, range of motion, speed, inter-segmental relationships
Systematic Observation
• Initiation, Execution, Termination
Phases
• Proximal to distal
Each Joint
Which Tasks to Observe?
Varying Demands
Demands can be Generalized to other Tasks
Sufficient Challenge
Overlap with Items on Standardized Tests
• Quiet Sitting, Quiet Standing (EO/EC), STS, Stair Tap, Walking, Walking with Head Turning, Step Over, Change Direction, Reach, Grasp
Recommendations
Sit to Stand
Identifying Faulty Movement
Performance Sit to Stand Example

KT - Janes, Nordman, Otis, Scheets 8
Sit to Stand Example Stand to Sit Example
Stand to Sit Example Sit to/from Stand Documentation
Alternate Stair Tap Identifying Faulty Movement
Performance

KT - Janes, Nordman, Otis, Scheets 9
Cardiopulmonary Patient Cardiopulmonary Patient Example
Cardiopulmonary Patient
Documentation Musculoskeletal Patient
Musculoskeletal Patient Example Musculoskeletal Patient Documentation

KT - Janes, Nordman, Otis, Scheets 10
Neuromuscular Patient Neuromuscular Patient Example
Neuromuscular Patient Documentation Making it Work for YOU
• Adopt a new routine
– Be thorough in your systems review
• Complete the OASIS
• Drug regimen review
– Do a complete examination
• Baseline status
• Understand the nature of the patient’s problem
• Be specific in your observations
– Develop a specific plan of care
Treatment Ideas
Bring it On!
Matt Janes, PT, DPT, MHS, OCS, CSCS

KT - Janes, Nordman, Otis, Scheets 11
Tests and Measures
• A standardized test or measure promotes
reliability and validity through the procedures of
administering, scoring and interpreting results in
a consistent and predetermined standard
• Tests and measures are used as a measure of a
patient’s progress or relative outcome
Standardized Tests and Measures
Short Physical Performance Battery (SPPB)
2 Minute Walk Test (2MWT)
Borg Scale (Rating of Perceived Exertion (RPE))
Dyspnea Scale (Rating of Perceived Exertion (RPE))
Short Physical Performance Battery
(SPPB)
• Measures:
– Functional status
– Physical performance
– Focus on Lower
Extremities
• High correlation:
– Mobility disability
– Hospitalization
– Institutionalization
– Mortality
2MWT
• 2 minute walk test (2MWT)
• Correlation:
– function, morbidity, and mortality
• MDC90 (older adults) = 15 meters or 49.2 feet
• Equipment:
– Stopwatch or second hand
– Tape measure
– BP cuff
– Chair
k
Perception
Performance Physiology
Perceived Exertion
Perceived Exertion
Physiological variables
Physical work capacity

KT - Janes, Nordman, Otis, Scheets 12
Rating of Perceived Exertion (RPE)
Dyspnea Scale Borg Scale
2 Minute Walk Test
PT Documentation Example
Exercise and Activity Prescription
• Progressive age related loss of
strength
• 1% to 5% loss of strength each
year after 30
• 3% to 5% loss of strength each
year after 60
• Loss of strength = loss of function
• Effective strength practice
Building LE Strength
Exercise and Activity Prescription
Modified
Scale
Ordinal Borg RPE
Scale
Percent
Effort
Perceived
Work Load
6 20%
7 30%
8 40%
1 9 50%
2 10 55%
11 60%
12 65%
13 70%
14 75%
5 15 80%
6 16 85%
7 17 90%
8 18 95%
9 19 100%
10 20 Exhaustion
Hard
Very Hard
Very, very hard
3
4
Very, very light
Very light
Fairly light
Moderatly light
Exercise and Activity Prescription
• Maximum Heart Rate (Max HR) = 220 – age
155 Max HR = 220 – 65
• Target Heart Rate (THR)
= Percentage of Max HR
93 THR = 155(60%)
• Heart Rate Reserve (HRR)
= Max HR – Resting HR
85 HRR = 155 – 70
• Target Heart Rate Range (THRR) = [ (Max HR – Resting HR) x % Intensity ] + Resting HR
A = [ (155 - 70) x 60% ] + 70 and B = [ (155 - 70) x 80% ] + 70
121 – 138 THRR

KT - Janes, Nordman, Otis, Scheets 13
Exercise and Activity Prescription Exercise and Activity Prescription
Building UE Strength Exercise and Activity Prescription
Frail elderly: RPE of 11-13, 20 minutes each day, 3 days/week
Cardiac patients: RPE 11-16, multiple short sessions, 4-7 days/week
Respiratory patients: RPE 3-5, two,15-minute or one, 30-minute sessions, 4-5 days/week
Vital Sign Baseline Normative Values
American Heart Association (AHA) Standards
– Blood Pressure (BP) : Systolic 90-140 mmHg
Diastolic 60-90 mmHg
– Heart Rate (HR) : 60-90 beats per minute (bpm)
– Respirations (R) : 12-16 breaths per minute
– Oxygen Saturation (O2 Sat) : ≥ 90%
Vital Sign Response to Exercise

KT - Janes, Nordman, Otis, Scheets 14
Normal Blood Pressure Response to
Exercise
• Increases with increasing workload
• Flattens out/decreases slightly as maximum work capacity is reached
Systolic Pressure
• Demonstrates no change and/or
• Slightly increases or decrease
Diastolic Pressure
Abnormal Blood Pressure Response to
Exercise
• Demonstrates little or no response with increasing workload,
• Slight fall, then rise with increased workload,
• Normal rise which abruptly falls
Systolic Pressure
• Increases with increasing workload and/or increase is prolonged after exercise is stopped
Diastolic Pressure
Building Activity Tolerance Building Activity Tolerance
PT Documentation Example
Indications for Termination of Exercise
• Chest pain of any type
• Severe shortness of breath
• Dizziness or faintness
• New onset or increase in mental confusion
• Sudden onset of sweating, pallor, cyanosis
• Sign of irregular heart rhythm
• Patient request to stop
• Drop in systolic BP > than 10 mmHg from baseline, despite increase in workload
• O2 saturation 85-89% & symptomatic, absolute cutoff is 85%
• Hypertensive response
• Systolic blood pressure > 210 mmHg and/or
• Diastolic blood pressure >115 mmHg
• Leg cramps or increase in leg pain
• Fatigue, shortness of breath, increased wheezing
Bring it on!
• Adopt a new routine – Utilize tests and measures for examining
exertional ability and functional performance
– Prescribe a level of optimal intensity appropriate for your
patient
– Develop a plan of care that promotes functional activity
tolerance and independence
– Monitor response to exercise
and activity

KT - Janes, Nordman, Otis, Scheets 15
Knowledge-to-Action Process
Outcomes
Outcomes
Measures of clinician empowerment, engagement, support,
“energy” and adoption into practice
– Number of OT and PT staff who completed training
• Target: ≥ 50% of target audience
– Result: average attendance across all 3 modules 67.7%
– 2966 employees completed one or more of the modules
– “I feel I will be able to apply this information to my practice.”
• Target: ≥ 70% Agree or Strongly Agree
– Result: average across all 3 modules 89.8%
Chart Audit Results
Convenience Sample
• 4 therapists from each region
Reviewed 5 completed records prior to training and 5 completed records after training
16 behaviors associated with the first 3 modules
Calculated an adherence score for each record; averaged for each clinician
• Possible adherence scores range from 1.0 to 0.0
Home Health Section
Platform Presentation
Friday, February 6
3:00 – 5:00 pm
• 3:20 – 3:40 pm
Opportunities
• Present < 50% of the time after training
– A 2-minute walk test was completed during the Physical
Therapist’s evaluation
– Strength training was implemented using an intensity of at least
60% of a 1-repetition maximum identified using the Borg RPE
scale to identify the intensity
– An RPE rating was provided for at least 1 activity from the
Physical Therapist’s evaluation
– Sessions are of appropriate duration and intensity (using Borg
or HR) to build CP capacity if documented as a problem
– Standardized tests are used when reporting progress
Additional Opportunities
• Increase prevalence of task-specific training in post-
operative cases
• Progress strength training by adding resistance (intensity)
rather than adding repetitions
• Summarize progress in terms of skill consistency,
flexibility, and efficiency rather than advancement of
exercises
• Do more gait speed training rather than gait endurance
training

KT - Janes, Nordman, Otis, Scheets 16
Strengths of the KT Project
• Recognized need company-wide • Therapist engagement
• Therapy practice
• Re-stabilization in company structure • Therapist in senior leadership
• Local structure for therapy support determined
• Operational support for training • Wanted to see behavior change
• Trust in the product to be produced
• Senior leadership support • Resource allocation
• Enthusiasm among local therapy leaders
• Available technology and technological expertise
• The “Therapy Guide”
Limitations of the KT Project
• Short timeline for development
• Inexperience with virtual classroom for clinical teaching
• Activities to reinforce learning were optional • Few local leaders implemented follow-up activities
• Competing priorities • EMR
Sustain
Sustainability
• Modules made available for CEUs
• Reinforced concepts and use of “Therapy Guide” in other
projects
• Intermittent chart audits • RPE ratings more consistently used now
Summary of Key Points
Large scale KT Intervention
Training converted theoretical constructs to concrete
behaviors
Clinicians did change behavior
Organization support critical
Competing priorities are a factor
Consistent clinical message with lasting clinical support
tools increases likelihood of sustaining change

KT - Janes, Nordman, Otis, Scheets 17
Selected References • American College of Sports Medicine, ed. ACSM’s Guidelines for Exercise Testing and Prescription. 8th
ed. Baltimore MD: American College of Sports Medicine; 2010.
• American College of Sports Medicine, Chodzko-Zajko WJ, Proctor DN et al. American college of sports medicine position stand. Exercise and physical activity for older adults. Med Sci Sport Exerc. 2009;41:1510-30.
• Avers D, Brown M. White paper: strength training for the older adult. J Geri Phys Ther. 2009;32(4):148-152.
• Birkenmeier RL, Prager EM, Lang CE. Translating animal doses of task-specific training to people with chronic stroke in 1-hour therapy sessions: a proof-of-concept study. Neurorehabil Neural Repair. 2010;24(7):620-630.
• Boulay MR, Simoneau JA, Lortie G, Bouchard C. Monitoring high-intensity endurance exercise with heart rate and thresholds. Med Sci Sports Exerc. 1997;29(1):125-32.
• Brooks D, Davis AM, Naglie G. The feasibility of six-minutes and two-minute walk tests in in-patient geriatric rehabilitation. Can J Aging. 2007;26(2):159-62.
• Burtin C, Saey D, Saglam M, et al. Effectiveness of exercise training in patients with COPD: the role of muscle fatigue. Eur Respir J. 2012;40(2):338-44.
• Coleman E, Chalmers S. The Care Transitions Intervention, Results of a Randomized Controlled Trial. Arch Intern Med; 2006; 166.
• Connelly DM, Thomas BK, Cliffe SJ, Perry WM, Smith RE. Clinical utility of the 2-minute walk test or older adults living in long-term care. Physiother Can. 2009;61:78-87.
• DeJong G, Hsieh CH, Putman K, et al. Physical therapy activities in stroke, knee arthroplasty, and traumatic brain injury rehabilitation: their variation, similarities, and association with functional outcomes. Phys Ther. 2011:91(12):1826-37.
• DeJong S., Schaefer SY, Lang CE. Need for speed: better movement quality during faster task performance after stroke. Neurorehabil Neural Repair. 2012;26(4):362-73.
• de Vreede PL, van Meeteren NL, Samson MM, Wittink HM, Duursma SA, Verhaar HJ. Functional tasks exercise versus resistance to improve daily function in older women: A feasibility study. Arch Phys Med Rehab. 2004;85:1952-61.
Selected References con’t. • Finger M, Stoll A, Stucki G, Huber E. Identification of intervention categories for physical therapy, based on
the International Classification of Functioning, Disability and Health: a Delphi exercise. Phys Ther. 2006;86:1203–1220.
• Frese EM, Fick A, Sadowsky HS. Blood pressure measurement guidelines for physical therapists. Cardiopulm Phys Ther J. 2011;22(2):5-12.
• Garber CE, Blissmer B, Deschenes MR, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exercise. 2011;43(7):1334-59.
• Graham ID, Logan J, Harrison MB, et al J of Cont Education for Health Professions. 2006; 26: 13-24.
• Horn SD, DeJong G, Smout RJ, et al. Stroke rehabilitation patients, practice, and outcomes: is earlier and more aggressive therapy better? Arch Phys Med Rehabil. 2005;86(2):S101-14.
• Jette DU, Warren RL, Wirtalla C. The relation between therapy intensity and outcomes of rehabilitation in skilled nursing facilities. Arch Phys Med Rehabil. 2005;86(3):373-9.
• Kimberley TJ, Samargia S, Moore LG, et al. Comparison of amounts and types of practice during rehabilitation for traumatic brain injury and stroke. J Rehabil Res Dev. 2010;47(9):851-62.
• Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. J Speech Lang Hearing Res. 2008;51:s225-s239.
• Lang CE, MacDonald JR, Reisman DS, et al. Observation of amounts of movement practice provided during stroke rehabilitation. Arch Phys Med Rehabil. 2009;90:1692-8.
• Lee MJ, Kilbreath SLm Singh MF, Zeman B, Davis GM. Effect of progressive resistance training on muscle performance after chronic stroke. Med Sci Sports Exerc. 2010;42(1):23-34.
• Leung AS, Chan KK, Sykes K, Chan KS. Reliability, validity, and responsiveness of a 2-min walk test to assess exercise capacity of COPD patients. Chest. 2006;130(1):119-25.
• Littbrand H, Carlsson M, Lundinn-Olsson L, et al. Effect of a high-intensity functional exercise program on functional balance: preplanned subgroup analyses of a randomized controlled trial in residential care facilities. J Am Geriatr Soc. 2011;59(7):1274-82.
Selected References con’t. • Maughan KK, Lowry KA, Franke WD, Smiley-Oyen AL. The dose-response relationship of balance training
in physically active older adults. J Aging Phys Act. 2012;20(4):442-55.
• Mayer F, Scharhag-Rosenberger F, Carlsohn A, et al. The intensity and effects of strength training in the elderly. Dtsch Arztebl Int. 2011;108(21):359-64.
• Munin MC, Putman K, Hsieh CH, et al. Analysis of rehabilitation activities within skilled nursing and inpatient rehabilitation facilities after hip replacement for acute hip fracture. Am J Phys Med Rehabil. 2010;89(7):530-40.
• Pak S, Patten C. Strengthening to promote functional recovery poststroke: an evidence-based review. Topics Stroke Rehabil. 2008;15(3):177-199.
• Peterson MD, Rhea MR, Sen A, Gordon PM. Resistance exercise for muscular strength in older adults: a meta-analysis. Aging Res Rev. 2010; 8(3):226-37.
• Quinn, L., Gordon, J. (2010). Documentation for Rehabilitation: A Guide to Clinical Decision Making, 2nd Ed. St Louis, Missouri: Saunders.
• Schaefer SY, Patterson CB, Lang CE. Transfer of training between distinct motor tasks after stroke: implications for task-specific approaches to upper-extremity neurorehabilitation. Neurorehabil Neural Repair. 2013 Apr 2 [Epub ahead of print].
• Scheets PL, Sahrmann SA, Norton BJ. Use of movement system diagnoses in the management of patients with neuromuscular conditions: a multiple-patient case report. Phys Ther. 2007;87(6):654-669.
• Schultz AB, Alexander NB, Ashton-Miller JA. Biomechanical analyses of rising from a chair. J Biomechanics. 1992;25(12):1383-1391.
• Schwartz RS: Sarcopenia and physical performance in old age: introduction. Muscle Nerve Suppl5: S10-12, 1997.
• Valenzuela T. Efficacy of progressive resistance training interventions in older adults in nursing homes: a systematic review. J Am Med Dir Assoc. 2012;13(5):418-28.
• Wrentenberg P, Lindberg F, Arborelius UP. Effect of armrests and different ways of using them on hip and knee load during rising. Clin Biomech. 1993;8:95-101.
Mo
du
le 2
La
b
[1
]
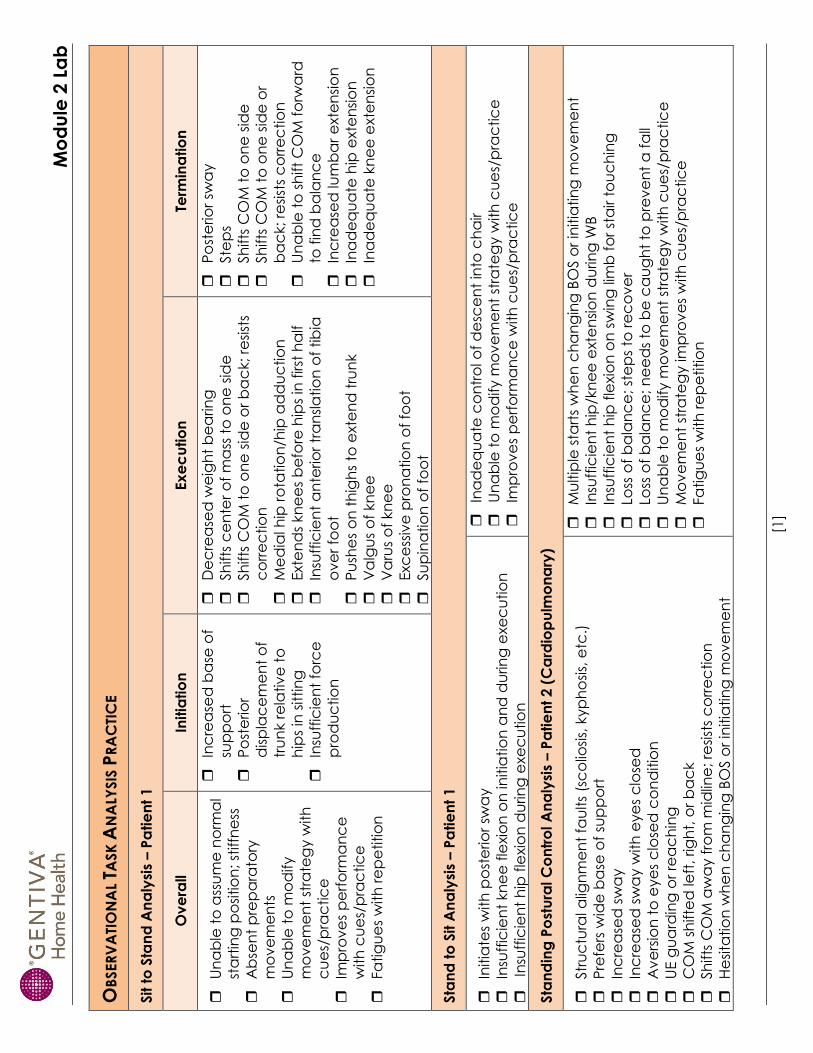
OB
SER
VA
TIO
NA
L TA
SK
AN
ALY
SIS
PR
AC
TIC
E
Sit t
o S
tan
d A
na
lysi
s – P
atie
nt
1
Ov
era
ll In
itia
tio
n
Ex
ec
utio
n
Term
ina
tio
n
Un
ab
le t
o a
ssu
me
no
rma
l
sta
rtin
g p
osi
tio
n; st
iffn
ess
Ab
sen
t p
rep
ara
tory
mo
ve
me
nts
Un
ab
le t
o m
od
ify
mo
ve
me
nt
stra
teg
y w
ith
cu
es/
pra
ctic
e
Imp
rov
es
pe
rfo
rma
nc
e
with
cu
es/
pra
ctic
e
Fa
tig
ue
s w
ith
re
pe
titio
n
Inc
rea
sed
ba
se o
f
sup
po
rt
Po
ste
rio
r
dis
pla
ce
me
nt
of
tru
nk r
ela
tiv
e t
o
hip
s in
sittin
g
Insu
ffic
ien
t fo
rce
pro
du
ctio
n
De
cre
ase
d w
eig
ht
be
arin
g
Sh
ifts
ce
nte
r o
f m
ass
to
on
e s
ide
Sh
ifts
CO
M t
o o
ne
sid
e o
r b
ac
k; re
sist
s
co
rre
ctio
n
Me
dia
l hip
ro
tatio
n/h
ip a
dd
uc
tio
n
Exte
nd
s kn
ee
s b
efo
re h
ips
in f
irst
ha
lf
Insu
ffic
ien
t a
nte
rio
r tr
an
sla
tio
n o
f tib
ia
ov
er
foo
t
Pu
she
s o
n t
hig
hs
to e
xte
nd
tru
nk
Va
lgu
s o
f kn
ee
Va
rus
of
kn
ee
Exc
ess
ive
pro
na
tio
n o
f fo
ot
Su
pin
atio
n o
f fo
ot
Po
ste
rio
r sw
ay
Ste
ps
Sh
ifts
CO
M t
o o
ne
sid
e
Sh
ifts
CO
M t
o o
ne
sid
e o
r
ba
ck; re
sist
s c
orr
ec
tio
n
Un
ab
le t
o s
hift
CO
M f
orw
ard
to f
ind
ba
lan
ce
Inc
rea
sed
lum
ba
r e
xte
nsi
on
Ina
de
qu
ate
hip
exte
nsi
on
Ina
de
qu
ate
kn
ee
exte
nsi
on
Sta
nd
to
Sit A
na
lysi
s – P
atie
nt
1
Initia
tes
with
po
ste
rio
r sw
ay
Insu
ffic
ien
t kn
ee
fle
xio
n o
n in
itia
tio
n a
nd
du
rin
g e
xe
cu
tio
n
Insu
ffic
ien
t h
ip f
lexio
n d
urin
g e
xe
cu
tio
n
Ina
de
qu
ate
co
ntr
ol o
f d
esc
en
t in
to c
ha
ir
Un
ab
le t
o m
od
ify m
ov
em
en
t st
rate
gy w
ith
cu
es/
pra
ctic
e
Imp
rov
es
pe
rfo
rma
nc
e w
ith
cu
es/
pra
ctic
e
Sta
nd
ing
Po
stu
ral C
on
tro
l A
na
lysi
s – P
atie
nt
2 (
Ca
rdio
pu
lmo
na
ry)
Str
uc
tura
l alig
nm
en
t fa
ults
(sc
olio
sis,
kyp
ho
sis,
etc
.)
Pre
fers
wid
e b
ase
of
sup
po
rt
Inc
rea
sed
sw
ay
Inc
rea
sed
sw
ay w
ith
eye
s c
lose
d
Av
ers
ion
to
eye
s c
lose
d c
on
ditio
n
UE g
ua
rdin
g o
r re
ac
hin
g
CO
M s
hifte
d le
ft, rig
ht,
or
ba
ck
Sh
ifts
CO
M a
wa
y f
rom
mid
line
; re
sist
s c
orr
ec
tio
n
He
sita
tio
n w
he
n c
ha
ng
ing
BO
S o
r in
itia
tin
g m
ov
em
en
t
Mu
ltip
le s
tart
s w
he
n c
ha
ng
ing
BO
S o
r in
itia
tin
g m
ov
em
en
t
Insu
ffic
ien
t h
ip/k
ne
e e
xte
nsi
on
du
rin
g W
B
Insu
ffic
ien
t h
ip f
lexio
n o
n s
win
g li
mb
fo
r st
air t
ou
ch
ing
Loss
of
ba
lan
ce
; st
ep
s to
re
co
ve
r
Loss
of
ba
lan
ce
; n
ee
ds
to b
e c
au
gh
t to
pre
ve
nt
a f
all
Un
ab
le t
o m
od
ify m
ov
em
en
t st
rate
gy w
ith
cu
es/
pra
ctic
e
Mo
ve
me
nt
stra
teg
y im
pro
ve
s w
ith
cu
es/
pra
ctic
e
Fa
tig
ue
s w
ith
re
pe
titio
n

Mo
du
le 2
La
b
[2
]
Sta
nd
ing
Po
stu
ral C
on
tro
l A
na
lysi
s – P
atie
nt
3 (
Mu
scu
losk
ele
tal)
Str
uc
tura
l alig
nm
en
t fa
ults
(sc
olio
sis,
kyp
ho
sis,
etc
.)
Pre
fers
wid
e b
ase
of
sup
po
rt
Inc
rea
sed
sw
ay
Inc
rea
sed
sw
ay w
ith
eye
s c
lose
d
Av
ers
ion
to
eye
s c
lose
d c
on
ditio
n
UE g
ua
rdin
g o
r re
ac
hin
g
CO
M s
hifte
d le
ft, rig
ht,
or
ba
ck
Sh
ifts
CO
M a
wa
y f
rom
mid
line
; re
sist
s c
orr
ec
tio
n
He
sita
tio
n w
he
n c
ha
ng
ing
BO
S o
r in
itia
tin
g m
ov
em
en
t
Mu
ltip
le s
tart
s w
he
n c
ha
ng
ing
BO
S o
r in
itia
tin
g m
ov
em
en
t
Insu
ffic
ien
t h
ip/k
ne
e e
xte
nsi
on
du
rin
g W
B
Insu
ffic
ien
t h
ip f
lexio
n o
n s
win
g li
mb
fo
r st
air t
ou
ch
ing
Loss
of
ba
lan
ce
; st
ep
s to
re
co
ve
r
Loss
of
ba
lan
ce
; n
ee
ds
to b
e c
au
gh
t to
pre
ve
nt
a f
all
Un
ab
le t
o m
od
ify m
ov
em
en
t st
rate
gy w
ith
cu
es/
pra
ctic
e
Mo
ve
me
nt
stra
teg
y im
pro
ve
s w
ith
cu
es/
pra
ctic
e
Fa
tig
ue
s w
ith
re
pe
titio
n
Sta
nd
ing
Po
stu
ral C
on
tro
l A
na
lysi
s – P
atie
nt
4 (
Ne
uro
mu
scu
lar)
Str
uc
tura
l alig
nm
en
t fa
ults
(sc
olio
sis,
kyp
ho
sis,
etc
.)
Pre
fers
wid
e b
ase
of
sup
po
rt
Inc
rea
sed
sw
ay
Inc
rea
sed
sw
ay w
ith
eye
s c
lose
d
Av
ers
ion
to
eye
s c
lose
d c
on
ditio
n
UE g
ua
rdin
g o
r re
ac
hin
g
CO
M s
hifte
d le
ft, rig
ht,
or
ba
ck
Sh
ifts
CO
M a
wa
y f
rom
mid
line
; re
sist
s c
orr
ec
tio
n
He
sita
tio
n w
he
n c
ha
ng
ing
BO
S o
r in
itia
tin
g m
ov
em
en
t
Mu
ltip
le s
tart
s w
he
n c
ha
ng
ing
BO
S o
r in
itia
tin
g m
ov
em
en
t
Insu
ffic
ien
t h
ip/k
ne
e e
xte
nsi
on
du
rin
g W
B
Insu
ffic
ien
t h
ip f
lexio
n o
n s
win
g li
mb
fo
r st
air t
ou
ch
ing
Loss
of
ba
lan
ce
; st
ep
s to
re
co
ve
r
Loss
of
ba
lan
ce
; n
ee
ds
to b
e c
au
gh
t to
pre
ve
nt
a f
all
Un
ab
le t
o m
od
ify m
ov
em
en
t st
rate
gy w
ith
cu
es/
pra
ctic
e
Mo
ve
me
nt
stra
teg
y im
pro
ve
s w
ith
cu
es/
pra
ctic
e
Fa
tig
ue
s w
ith
re
pe
titio
n