knowledge matters volume 7 issue 1
DESCRIPTION
A new issue of Knowledge Matters for a new era of the NHS. Featuring: Mental health Safety Thermometer Developments in the World of Insight Case Management The Vanguard Programme Plus all the regular featuresTRANSCRIPT

issuu.com/SECQO
twitter.com/SECSHAQO
www.QualityObservatory.nhs.uk http://www.networks.nhs.uk/nhs-networks/sec-qo
Volume 7 Issue 1 April 2013
“O brave new world, that has such people in’t”
That Shakespeare fellow really does have a quote for every occasion. For here we are in the brave new world of the NHS. Gone are the SHA’s and PCTs and we can usher in the new dawn of NHS England, and welcome the birth, af-ter a long and difficult gestation period, of CCGs and CSUs.
It’s appropriate to be talking of birth and new things, now that spring has tentatively sprung. We’ve got a couple of arti-cles in this issue on new developments. A number of us went to the Central Southern CSU team away day, and we report back on how they’re planning to develop and grow in the future.
Many of you will be aware of the Safety Thermometer programme. Not only has that been growing, but it’s also started reproducing! We have a report on the pilot phase of one of its offspring – the Mental Health Safety Thermometer. Even we at the Quality Observatory have to change and develop too – that means looking for new customers and clients. You can find out about how we did at the Healthcare Innovation Expo earlier this year. Also in this issue is an article from Oxfordshire asking if case management can really make a difference.
However in the midst of these new and exciting developments it’s good to have something that’s staying the same to hold onto, so here’s this issue of Knowledge Matters, with the same mixture of articles, opinions, news and terrible poetry as ever. Just to make you feel at home we’ve still got Samantha writing for us, and you can read her first article as Director of Insight for NHS England.
So I’ll leave you to settle into this issue with a bit more of The Bard:
“Once more unto the breach, dear friends, once more,
…
Cry 'God for Harry, England, and Saint George!'”
Welcome to Knowledge Matters
Inside This Issue :
Mental Health Safety Thermometer 2 Skills Builder 8 News 15
Developments in the World of Insight 4 Healthcare Innovation Expo 2013 10
Central Southern CSU launch 6 Does Case management Make A Differ-ence? Evaluating Findings in Oxfordshire
12
Analysis Ancient and Modern 7 The Vanguard Program 14

2
[email protected] www.QualityObservatory.nhs.uk
Mental Health Safety Thermometer
by Nicola Clark, Kurt Bramfitt & Adam Cook
Many of you are aware of the National Safety Thermometer. It is an audit based tool that measures the prevalence of harm from Pressure Ulcers, Falls, UTIs (in patients with a catheter) and VTE across all NHS funded care providers. This has been running for nearly three years now and during this time much interest has been expressed to further develop Safety Thermometers to measure harm in different specialities one of which being Mental Health.
The Mental Health Thermometer (MHST) national pilot data collection has been run between January and April 2013.
New measures have been developed and tested to make the Mental Health Safety Thermometer applicable and specific to mental health services focusing on the vulnerability of the patients and potential risk from harm.
The harms chosen were;
Self-Harm, Falls, Violence and aggression, and Medications errors
The first three categories were looked at in terms of when the harm occurred (i.e. before or after admission) and the severity of the harm. The question on violence and aggression was also divided into whether people felt at risk of violence/aggression, and actual harm from violence/aggression.
Results were collected fortnightly from participating trusts. There was excellent engagement on this, and 17 trusts regularly sent in information – these trusts were from all across the country, and provided information for both community and inpatient settings. Over the 6 test periods data for over 5000 patients was collected, an average of about 850 per test period. This was significantly more than had been expected.
The results were fed back to the testing faculty who provided valuable insight and commentary. As with any pilot testing some issues were raised, and after consultation were corrected for subsequent tests. One particular issue was around Medication Omissions – instead of trying to categorise the severity of harm from an omission, it was decided that it would be better to examine the reasons for the omission, as many of these could have valid clinical reasons, and harm is difficult to measure in a test intended to take no longer than tem minutes to complete at the patients chairside or bedside. Subsequent changes to the tool were more minor and looked at ways of producing consistent terminology for the
various settings of care. Many of the errors that came through with filling in the template were minor and should the project be taken forward would be eliminated by a web based data collection template. For the last test a more major change was implemented around the ‘risk of violence/aggression’ question.
This was always a difficult and contentious question for some organisations. Measuring an individual’s perception of something is always hard to do, and the results will always be subjective. An additional complicating factor is the patients’ medical conditions – for many of whom feeling at risk of violence or aggression is an actual symptom of their diagnosis. It became clear both through the results of the pilot tests, and through feedback via the testing faculty that this question was something that many staff were finding difficult to ask, and patients were finding difficult to answer in some case, particularly those with conditions such as Dementia. However data collection showed that this was an interesting measure, and although staff were uncomfortable asking it, a real issue was highlighted in the early data.
Organisation
Ward/ team
Set ting
Service/specialty
Date of survey
Number of patients surveyed
Pati
ent
no. Gender Age group
Q1: Has the patient
self harmed in the
last 72 hours?
Q2: Does the
pat ient have harm
f rom this event?
Q3: Did the self
harm occur before
admission to your
organisation?
Q4: Has the patient
fallen in the last 72
hours?
Q5: Does the
patient have harm
from this fall?
Q6: Has the patient
felt at risk of
violence or
aggression in the
last 72 hours?
Q7: Did this occur
before admission
to your
organis ation?
Q8: Has the patient
been a vict im of
violence or
aggression in the
last 72 hours?
Q9: Does the
pat ient have harm
f rom this event?
Q10: Did the
violence or
aggression occur
before admiss ion
to your
organisation?
Q11: Has the
pat ient had an
omitted dose in the
last 24 hours?
Medication omissionsVictim of violenceRisk of violence or aggressionSelf harm Falls
Organisations
945
886
708
422
343
243219
200 199170
138 133 129 123 11587
40
0
100
200
300
400
500
600
700
800
900
1000
Kent & Medway
Coventry & Warwickshire
Bradford District Care
SWLSTG
Mersey Care
Manchester MH&ST
South London & Maudsley
Penine Care
Norfolk & Suffolk
5 Boroughs
Oxford Health
Avon & Wiltshire
Plymouth Community Care
Berkshire Health Care
Southern Health
Dorset Healthcare
2Gether

3
[email protected] www.QualityObservatory.nhs.uk
After much deliberation it was decided to change this from a straight forward Yes/No response and to add another category. The extra category was “Patient not able to understand ques-tion” – as it was felt that this best cap-tured the problems that had been ex-perienced, for patients with cognitive deficits. Further testing will be needed to establish a stable proportion for this measure.
The results of the pilot for each test showed the median number of patients receiving harm free care was 89.5%. Medication omissions was excluded from the harm free care calculation as it was not possible to measure an im-mediate harm from an omission, in-
stead this was classed as a measure of incomplete care. Medication Omission was the most likely of all the recorded events to happen to a patient, (a median of 10.4% of patient having one of more medication omissions.)The vast major-ity of these omissions were down to patient refusal.
Of the three remaining harms the most frequently recorded harm that resulted in actual harm was self-harm – in fact this is the only one of the categories where a severe harm occurred. Receiving harm from violence/aggression was low with a median of 0.5%. Patients receiving harm from a fall was even lower, but there were very small numbers of patients in this group. Only 19 patients out of the group of 5305 actually being in this category. The pilot has been an excellent op-portunity to test and fine tune a Safety Thermometer tool for Mental Health services, however to truly understand the burden of harm from these measures a large scale series of tests will further needed.
Where does the MHST go from here?
Currently discussions are being held with NHS England to continue this pilot and carry out a further 6 large scale tests which will allow the Mental Health Safety Thermometer to establish a base rate of data and a more accurate proportions of harm from a tool that is now stable and not subject to any further changes. It is hoped that this work will be carried forward later this year.
Whichever of these options is chosen this MHST pilot has proven to be a useful and fascinating project for all con-cerned.
Colleagues from Greater Manchester AHSN attending this years IHI & BMJ International Forum in Quality and Safety
in Healthcare in London have put to-
gether a video examining some of the
thorny issues around the measurement
of safety and the impact of financial in-
centives. World leaders in quality im-
provement have their say and snuck in
there somewhere is the QO’s very own
Kate Cheema with words to say about
the use of prevalence measures. You
can see the video at: www.haelo.nhs.uk It’s guaranteed to start a discussion!
International Forum on Quality and Safety in Healthcare
Proportion of patients that
have self harmed with a
resulting harm
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
Test
1
Test
2
Test
3
Test
4
Test
5
Test
6
Proportion of patients that have had a
fall which resulted in harm
0.00%
0.10%
0.20%
0.30%
0.40%
0.50%
0.60%
0.70%
Test 1 Test 2 Test 3 Test 4 Test 5 Test 6
Proportion of patients feeling at risk of
violence/aggression
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
Test 1 Test 2 Test 3 Test 4 Test 5 Test 6
Before admission Since admission
Proportion of patients that
have been a victim of
violence/aggession and
resulted in harm
0.0%
0.1%
0.2%
0.3%
0.4%
0.5%
0.6%
0.7%
0.8%
Test
1
Test
2
Test
3
Test
4
Test
5
Test
6
Proportion of patients that have had
one or more omitted doses of
medication
0%
2%
4%
6%
8%
10%
12%
14%
Test 1 Test 2 Test 3 Test 4 Test 5 Test 6
Proportion of patients that are receiving
harm free care
0%10%
20%
30%40%
50%60%
70%80%
90%100%
Test 1 Test 2 Test 3 Test 4 Test 5 Test 6
No Harm 1 Harm 2 Harms

4
[email protected] www.QualityObservatory.nhs.uk
Hello Knowledge Matters readers – I hope that you have had a good last couple of months. Although I’ve moved into a
new role with NHS England, I’m sure that there’s lots involved in my new role which will be of interest to all of you. So,
I am intending (if the new editor allows me) to continue with a regular article in Knowledge Matters. As a quick re-
minder, I now cover the annual survey programme, PROMs, Friends and Family Test and insight more generally.
So, on 16th April did you know that the Inpatient Survey results for 2012 were published by the CQC? The survey
looked at the experience of 64,500 and achieved a 51%
return rate. The findings in the survey were generally posi-
tive with progress made in key areas, however (as always)
there does still remain far too much variation across (and I
imagine within) providers. Here are headlines for the 2012
survey: -
• the overall patient experience measure is in-creased from the previous year;
• the overall CQUIN measures of patient experi-ence is increased from the previous year;
• trust in doctors and nurses has increased from the previous year;
• free text comment has been included for the first time in this year’s CQC report.
The inclusion of free text comments is a good move in my view – free text comments can provide a really rich source of data which provide more insight into the experience of patients. Here’s the link to all of the documents related to the inpatient survey – I would encourage you to go and have a look http://www.cqc.org.uk/public/reports-surveys-and-reviews/surveys/inpatient-survey-2012
I’m hoping that Knowledge Matters readers are aware that the Friends and Family Test for A&E and inpatients went live from 1
st April. This means that patients being discharged from A&E or a ward should be asked whether they would
recommend services to friends and family if they required similar care or treatment. (As an aside, I presented at a con-ference last week on FFT and was concerned with the low level of awareness of what it is, and that it is being imple-mented now – so a key priority going forward will be communication). Anyway, in addition, many Trusts are providing patients with the opportunity to provide free text comments to explain why they have scored as they have. You may have seen and heard views that the Friends and Family Test is flawed in a variety of ways (I’m not going to go into this now but will cover the concerns raised in a future article and outline plans later this year to undertake a review of the
methodology, implementation and learning). Last month I spent the day visiting two Trusts which have been undertaking fantastic work on patient experience for many years and were clear that the Friends and Family Test had added value and was a very useful high level indicator. The first of these was the Heart of England NHS Trust who have been utilising the approach for a number of years. Here’s the link to a video of how wards are using the results to improve services. I posted this link previously but it is so good I think it’s worth draw-ing your attention to it again http://www.youtube.com/watch?v=9DGA1zJ1KRA
Developments in the World of Insight
By Samantha Riley, Direct of Insight, NHS England

5
[email protected] www.QualityObservatory.nhs.uk
The same day I visited Birmingham Children’s Hospital who are also undertaking fantastic work in patient experience and feedback. I learnt about the new app which they are using to gain feedback from patients and parents. The app was really simple – that’s why it was so good. Even more impressive was that actioning and responding to comments made via the app were made a core component of the role of the responsible sister/department head. Most of the comments left are positive which has provided a real boost to staff. Negative comments are dealt with promptly. The really impressive thing was that the Trust has really embraced transparency and publishes all comments and responses on their website. Here’s the link to their website for you to have a look at the feedback and a short video describing how it works. I’d encourage you all to have a look http://www.bch.nhs.uk/feedback/app/landing Final thing on the Friends and Family Test is that the
guidance for maternity will be published imminently,
possibly by the time that Knowledge Matters is published. So keep your eyes open for this. Friends and family for
maternity needs to be introduced from October this year.
The final area that I would like to cover in this article is the development of an Insight Dashboard which brings together
the various sources of feedback data currently in existence. As Knowledge Matters readers will know, there can be
great value in triangulating different data sets as in many cases this enables you to ask more pertinent questions and
focus on areas of interest or concern. A number of data sets related to patient experience are currently annual, so
once the dashboard is launched later this year, we are intending to focus on different areas within the various annual
survey and complaints data sets to shine the spotlight on different topics. The dashboard will be demoed to the NHS
England Board in May and made available publically later this year so watch this space!
That’s all for now folks!! I’m trying to get into Twitter so if you want to keep updated on developments in between issues of Knowledge Matters follow me @samriley . I’ve also committed to restart my blog….. So if you are interested here is the link: http://samantharileynhs.blogspot.co.uk/
If you would like to get in touch with me please do [email protected]
6
[email protected] www.QualityObservatory.nhs.uk
On Wednesday the 24th April our new hosts, Central Southern CSU had an all staff
away day as a launch event. Four of us (Adam, Fats, Rebecca and Simon) from the Quality Observatory travelled along to Oxford United’s home ground to hear about the vision and the plans that were being put forward.
The day was split into two halves – before lunch the executive team stood up one by one, in front of the 400 plus crowd and expounded the philosophies and plans of the new organisation. The plans were clear, obviously well thought out and should prove to be challenging, but realistic. Ultimately the key message of the event was around supporting and growing the 5 things that CSCSU want to be famous for. These are:
Transforming services for patients and the public
Delivering efficient services
Improving quality for the patient
Helping others run their business
Evidence based decision making
All important and valuable, and importantly they resonate and complement our key values and principles at the Quality Observatory.
After lunch the throng was split into three groups and rotated through three workshops. Two were provided by external people who talked about the principles of good leadership and the importance and achievability of innovation.
The third, and probably most valuable session, was questions and answers with the executive team. The floor was opened to all staff present and the exec team fielded questions on any topic. This was useful not only for the answers given, but also in giving confidence to
staff present that they are being led by an open and honest team, who are working hard not only for the good of the staff, but for patients and the wider NHS.
Central Southern CSU Launch by Adam C. Cook

7
[email protected] www.QualityObservatory.nhs.uk
It’s hard to remember sometimes that we didn’t always have an NHS in this country and that health services were provided by a patchwork of organisations ranging from huge private institutions for the wealthy through voluntary hospitals, funded by donations, and care linked to workhouses. It’s pretty unlikely that there was much of a call for data running through all of this; but there must have been something because everyone has to look after the pennies, right?
Being a bit of a local history aficionado I thought I’d check out what this might have looked like for the health services in my town, not far from QO towers, Horley. I was quite surprised to find that up to 1983 Horley had its own cottage hospital, opened in 1903. In 1912 you could stay in a private room for the heady sum of 3 guineas (£3.15 in decimal money, about £255 allowing for inflation) or have a night nurse for 2 guineas (£2.10, £170 adjusted). Well, that’s all very interesting but it doesn't help in the search for data; what was the hospital’s casemix, their growth in demand and did their financials stack up?
Could there have been a need for a good QIPP scheme in bygone Horley?
Obviously we’re well off the era of the HRG but the annual report of the year’s work for 1937 shows an interesting range of procedures carried out at the hospital, although all firmly in the realms of general surgical daycases as we would understand it today, except the dentistry of course. Of course not all inpatients had a procedure undertaken but there isn’t any detail on what else they did come in for. Also interesting is the year on year growth in activity from 1934 to 1937 and the accompanying shift from being in the black in 1934 to in the red by some £43 pounds in 1937 (admittedly only equivalent to £2,269 in today’s money). Sounds like a QIPP plan would have been a good idea then.
It just shows that the core of our analysis has changed little; we’re interested in activity, finance, growth and casemix as the cornerstones to delivering a service in any health system and so was the system in pre-war Horley.
Shelley J, Lucas J and Brown AGT 2002 Charlwood and
Horley Cottage Hospital 1873-1983. Self-published
Analysis Ancient and Modern– pre-NHS data? by Kate Cheema

8
[email protected] www.QualityObservatory.nhs.uk
April 2013 is an interesting time to be returning to work after a 6 month break. Although it was impossible not to know about the changes taking place in the NHS it is still a bit daunting leaving one NHS world and returning to another, and one of the things I’ve been doing during my first few days back is getting to grips with what this actually means in terms of data analysis.
Provider data is pretty straightforward as there are no real changes there, although it’s worth checking that you’re picking up all of the community trusts for your area. It’s also worth noting that on any reports from the central data returns, e.g. the weekly A&E reports, that data previously grouped by SHA will now be grouped by Area Team instead for any data after 31st March. So there shoudn’t be any issues with continuing to add to any provider based analysis you have set up.
Commissioner based analysis though is more tricky, due to the organisational changes that came into effect on 1st April. PCTs and SHAs now no longer exist and have been replaced by Clinical Commissioning Groups (CCGs), Area Teams (ATs) and Commissioning Support Units (CSUs), plus other organisations.
So what can you do if you have a nice set of commissoner-based anlyses set up? Do you have to start a new set from scratch and lose all the historical/ benchmarking data that you have? Not necessarily - you’ll have to make some adjustments but it should be possible to come up with something, whatever data you’re working with.
How you want to go about this will largely depend on what your data source is. If you are working with hospital activity data e.g. SUS or HES, then you’ll have all the information you need to re-run your analysis by CCG rather than PCT, so can keep the historical trends in your new CCG analysis. (More on how to do this shortly).
If you have a more restricted set of data, e.g. data returns submitted to Unify2 such as the referral to treatment returns, diagnostic activity, or Monthly Activity returns then your options are more limited as these only have data at PCT level before April 2013, so while data from April onwards will be collected at CCG level there is no way to disaggregate the historical data. If you do want to look at trends over a number of years though, you do have the option of grouping the new data up to PCT level, which will at least give an idea of progress over time in a particular geographical area.
There are a number of resources available to help with this. The NHS England website has a ‘List of proposed CCGs with names, populations, current PCTs and running cost allowances’ which can be used to map CCGs to the old PCT boundaries. http://www.england.nhs.uk/resources/ccg-directory/
The Organisation Data Service page (now available on the Health and Social Care Information Centre website rather than Connecting for Health) has a number of useful files to download, including membership of CCGs by GP practice, lists of CCG, CSU and AT codes and postcode files with details of which CCG covers which post-code. All of these files can be found on the HSCIC website: http://systems.hscic.gov.uk/data/ods/datadownloads
Traditional Analysis: Linking Old and New Data By Rebecca Matthews, Information Analyst

9
[email protected] www.QualityObservatory.nhs.uk
These resources should help in linking pre and post-transition analysis

10
[email protected] www.QualityObservatory.nhs.uk
Healthcare Innovation Expo 2013
Healthcare Innovation Expo 2013
On 13th and 14
th March this year the Quality Observatory had a
stand at the Healthcare Innovation Expo at the Excel centre in London.
With an estimated 10,000 delegates passing through the door, and 200 other exhibitors we had our work cut out for us. This did mean that our stand was very busy (and not just because of the free sweets we had on offer!). All the Quality Observatory team members who manned the stand had aching feet and sore throats at the end of the event!
We were able to demonstrate many of our key products and ser-vices to their best advantage, and to a wide audience—many of whom we wouldn’t normally have been able to reach.
We were very encouraged by, not only the amount of visitors to our stand, but also their response. People were keen to engage and learn about what we do and our ethic of producing good qual-ity, understandable information for improvement purposes.
We shared our stand with the Safety Thermometer team from Sal-ford, and the Enhancing Quality team from South East Coast, both of whom were able to show the improvements that their pro-grammes had made, their plans for the future and of course how the QO team has helped them realise their goals!
The Expo was an opportunity for a wide variety of organisations from inside the NHS and the private sector to get together, and show their new ideas and innovations.
There were over 200 different stands offering an equally wide vari-ety of services from clinical and pharmaceutical, and medical de-vices to technological and managerial solutions.
Much of the new NHS world was represented with zones dedi-cated to Commissioning Support Units, Academic Health Sci-ences networks and NHS England. All setting out their pro-grammes of work, and showing how they will be operating in the new climate.

11
[email protected] www.QualityObservatory.nhs.uk
Healthcare Innovation Expo 2013
MISSING IN ACTION!
We collected a large number of business cards and expressions of interest on the day, in a beautiful vase, as you can see. However when we went to dismantle our stand the next day the vase was empty! (Enthusiastic cleaners? Industrial Espionage? Answers on a post-card…)
So if you had a chat with one of us on the day and are wondering why we haven’t called you then that’s the reason.
We’d love you to get in touch with us to discuss any new projects – just drop an e-mail to [email protected], and we’ll get back to you.
There were a wide variety of speakers giving seminars and master-classes – leaders from the NHS, Social Care and charities were ex-pounding their vision of the NHS, whilst many clinicians and other front-line staff demonstrated their innovations that have had positive effects upon healthcare in the recent few years.
12
[email protected] www.QualityObservatory.nhs.uk
Does Case Management Make A Difference? Evaluating Findings in Oxfordshire Chris Morris, Information Analyst, Central Southern CSU
Background
Oxfordshire PCT had been commissioning a Case Management Service for several years, and the newly-formed
CCG wanted to evaluate how effective this service had been at reducing emergency admissions and other
activity. We looked at all the available data and carried out an analysis to assess the impact of the Case
Management Service.
Methodology
The methodology used was an adaptation of one published by the Nuffield Trust. The analysis utilised a ‘matched
controls’ design whereby each case managed patient in the analysis cohort was matched on key information to a
very similar patient who had not received the service. The difference in outcomes between the ‘case’ (the patient
receiving the service) and their control could then be summed across all cases in order to estimate the overall
impact of the service.
This approach avoids the problems associated with only analysing the case managed patients differences in
outcomes using a ‘before and after’ design, where any reduction in activity following commencement of the
service may only be in part attributable to the service, and in part attributable to other effects (e.g. regression to
the mean).
The variables used for matching were;
• Gender
• Age
• Risk of Emergency Admission (PARR++ score)
• Deprivation score at patients postcode (Index of Multiple Deprivation 2010)
• Long-term condition profile (absence / presence of 7 key LTC’s; long-term Mental Health, Cancer,
Stroke, Coronary Heart Disease, Heart Failure, Chronic Obstructive Pulmonary Disease, and Diabetes)
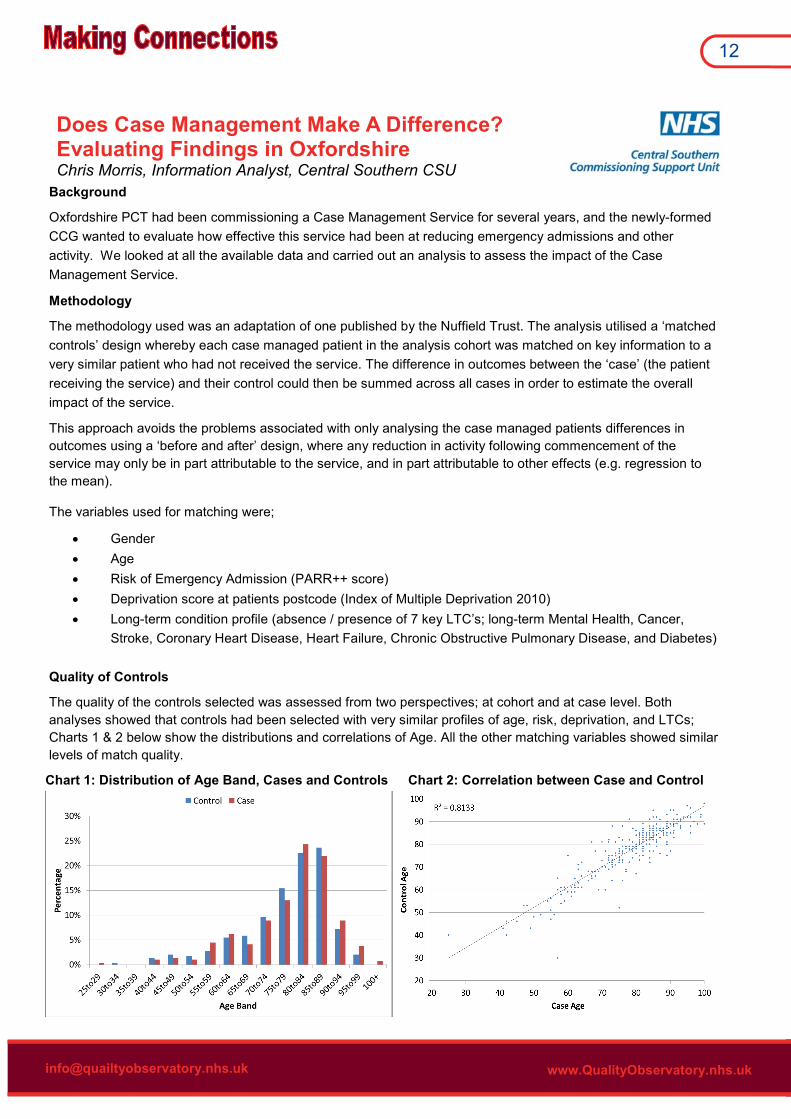
Quality of Controls
The quality of the controls selected was assessed from two perspectives; at cohort and at case level. Both
analyses showed that controls had been selected with very similar profiles of age, risk, deprivation, and LTCs;
Charts 1 & 2 below show the distributions and correlations of Age. All the other matching variables showed similar
levels of match quality.
Chart 1: Distribution of Age Band, Cases and Controls Chart 2: Correlation between Case and Control

13
[email protected] www.QualityObservatory.nhs.uk
Outcome Analysis
The outcomes included in the analysis were;
• A&E Attendances
• Emergency Admissions
• Elective Admissions (excluding regular day or regular night admissions)*
• Outpatient Appointments*
*This activity was included in order to sense check any potential findings in the main areas of interest, A&E and
Emergency Admissions; no effect was expected in Elective or Outpatients.
In all cases, the measurement was the difference in activity 12 months post-referral/index date compared to 12
months pre-referral/index, comparing the case to the control on an individual basis. For example, if the case had
had 5 A&E Attendances pre, and 2 post (i.e. -3 Attendances), and the control had had 5 pre and 3 post (i.e. -2
Attendances), the outcome was -1 Attendance; the difference between the case and control.
The data were subject to statistical tests for the significance of any observed differences. Although none of the
data were normally distributed, where the sample size was large enough (n>=100), parametric testing (Paired
Samples T-test) was used. Where the sample was small (n<100), the nonparametric equivalent (Related Samples
Wilcoxon Signed Rank Test) was used. Testing was undertaken at both the full cohort and risk group subset
levels.
None of the outcomes showed a significant difference between cases and controls.
It is useful to visualise the distributions of the outcomes; chart 3 below shows the distribution of change in A&E
Attendances. We can see that the distributions are very similar and reinforce the result of the statistical testing
that found no significant differences.
Chart 3: Distribution of Change in A&E Attendances
Conclusion
There was no evidence, based on the data available, for a systematic impact of Case Management in any of the
outcomes evaluated. Oxfordshire CCG took these findings into consideration when deciding whether to
commission this service going forward.
Contact: [email protected] Information Analyst, Central Southern Commissioning Support Unit
OCCG Project Lead: Karen Kearley, GP and member of Oxfordshire Clinical Commissioning Group

14
[email protected] www.QualityObservatory.nhs.uk
NHS Vanguard Programme By Fatai Ogunlayi, ERP Project Manager / QIPP Analyst
There are 4 things you may not know about the NHS Vanguard Programme. (And if at the end of this article, you
actually knew all 4 things before hand, cross your heart and all that, and you are not an Emerging leader or Sponsor
- contact the QO at [email protected] and 1 lucky winner will be treated to a lunch with the QO team).
The first thing you may or may not know is that NHS South
of England and NHS Yorkshire and Humber commissioned
the NHS Institute for Innovation and Improvement to
provide an accelerated development programme for 200
NHS leaders (100 emerging leaders and their local partner
sponsors). The NHS Vanguard Programme is a six-month
intensive leadership development programme (September
2012 – March 2013), aiming to provide Emerging Leaders and Doctors in training (specialist registrar level) and their
sponsors with the skills to deliver improvements in quality and productivity by building leadership and improvement
skills, the ability to engage others and create energy for change.
The second thing you may or may not know is that I was fortunate to
have applied and be successful in gaining a place in this prestigious
programme. My Vanguard Project was around improving early post-
operative mobilisation following hip/knee surgery for patients across
Kent, Surrey and Sussex. My sponsor for the project was Kay
Mackay – Director of Service Improvement for the AHSN. I chose
this project because it was part of my bigger portfolio of work which
is around getting patients better sooner with fewer complications –
The Enhanced Recovery Programme.
The third thing you may or may not know is that I have been successful at my final
assessment of the programme and as an additional icing on top; I was also awarded the
Best in Region award. I was invited to a celebration event in London where I shared with
my fellow Emerging leaders and their Sponsors, my Vanguard journey. While it was a
daunting experience, I felt very privileged to have been amongst the chosen few to speak
on the day. I remember telling them that the Vanguard journey has taken me through a
transformation process beyond my expectation; I shared my analogy of being like a
caterpillar at the start of the programme, full of potential and I have now emerged as a full
fledged butterfly ready to deliver on those potentials. I also shared with them how I have
learnt that in this journey of improving the service we deliver to our patients, we can’t
impose anything on anyone and expect them to be committed. What we need to do is
develop a shared purpose, a shared vision, a contagious environment for change –
engage staff at all levels to achieve commitment rather than compliance, in order to deliver better outcomes for our
patients.
The fourth and final thing you may or may not know about the NHS Vanguard Programme is that all the

15
[email protected] www.QualityObservatory.nhs.uk
NHS England Business Plan Published
The NHS England Business Plan has been published. It outlines an 11 point scorecard by
which progress will be judged .
http://www.england.nhs.uk/wp-content/uploads/2013/04/ppf-1314-1516.pdf
Friends and Family Test Maternity Guidance
The FFT maternity guidance is due to be published on the NHS England website by the end
of April.
New Caldicott Review Published
The new Caldicott Review on Information Governance in the health and social caresystem
was published on April 26th. The review can be downloaded from this link::
https://www.gov.uk/governance/publications/the-information-governance-review
New Anonymisation Standard
As of 30th April a new anonymisation standard for the publication of health and social care
data came into effect
http://www.hscic.gov.uk/article/2741/New-Anonymisation-Standard-for-the-publication-of-
health-and-social-care-data-becomes-effective-on-30-April-2013
NEWS
organisations involved in commissioning and delivering the Programme are, as of 31st March 2013, no longer part
of the new NHS landscape.
It is not yet clear which organisations would deliver these types of trainings in the future:
– it could be The NHS Leadership Academy whose mission is to develop outstanding leadership in health, in
order to improve people’s health and their experiences of the NHS.
– it could also be NHS Improving Quality who will drive transformational change through the promotion of the NHS
Change Model.
In either case, if you think a programme like the NHS Vanguard Programme would be of benefit to you or others
at your organisation, then the power is with you. My suggestion would be to speak to your line manager as a first
step, but it may also be worth enquiring with the NHS Improving Quality and /or NHS Leadership Academy
directly. To put it simply, you need to ask for it.
I have benefited a great deal from this programme, which has been instrumental in delivering improved outcomes
to patients across the Kent, Surrey and Sussex region and I think others should have the same opportunities that
were given to me. If you would like to know more about the Enhanced Recovery Programme across Kent, Surrey
and Sussex or about my Vanguard Project then please contact me on [email protected]
or on twitter @O_LaFatai.

Knowledge matters is the newsletter of NHS South East Coast’s Quality Observatory, to discuss any items raised in this publication, for further information or to be added to our distribution list, please contact:
Hosted by: Central Southern Commissioning Support Unit
E-mail: [email protected]
To contact a team member: [email protected]
Welcome Back Rebecca! This month we welcome back Rebecca Matthews who went on maternity leave in late September
and returned in April. As Rebecca says, “it’s great that we’re now being hosted by Central Southern
CSU as it means I get to come back to working with the Quality Observatory, although very strange
being in the same building but a different office—I have to keep to reminding myself not to sit at my
old desk!. It’s been amazing having the time off with Rosie, but now looking forward to being back at work and get-
ting involved in some completely new projects (and not obsessing over the nursery webcams too much)!
“As well as sorting out what work I’m going to be involved in and catching up with the NHS changes and other re-
cent developments, I’m also going to need a new job title as ‘Performance and Planning Analyst’ is somewhat out
of date now! Maybe that could be a competition in a future edition of Knowledge Matters? For the time being I’m
just calling myself ‘Analyst’”
Welcome back!
Fascinating Facts
On Joining the Central Southern CSU
We went to the CSU,
To show them what we could do,
John and his chums,
Stuck up their thumbs,
And now we’re part of the crew!
On Exhibiting at the Innovation Expo.
At the Expo for health innovation
We went looking for remuneration.
People came to our stand,
And said it was grand,
And helped build on our own reputation
A Pair of Limericks
A hobbit isn’t just a small, ha i r y- f oo ted creature from The Lord Of The Rings books – it also used to be a unit of meas-urement in Wales. A hob-bit measured either volume or weight – how much a hobbit weighed de-pended on what it was made of, so a hobbit of wheat would weigh more than half as much again as a hobbit of oats.
If you want to contribute to future is-
sues of Knowledge Matters then drop
us a line at