know ledge and attitudes of rural adolescent girls regarding...
TRANSCRIPT
124
HP2 and 02- by uraemics may also be responsible for impairedbactericidal activity.
Lysosomal enzymes which are responsible for bactericidalkilling within the phagolysosomes are involved in oxygen-inde-pendent microbicidal mechanisms of PMN and are associatedwith digestion of killed microbes. Stinavage et al.20have demon-strated that under anaerobic conditions lysosomal enzymes inneutrophils are involved in the killing of S. typhimurium. Werecorded enhanced activity of cathepsin D and acid phosphatasein the PMN of CRF patients compared to controls. The lysozymelevel was found to be unaltered in our study. Cohen et al. haveshown that degranulation of PMN is impaired in uraemicpatients.' This is likely to explain the increased levels of intra-cellular lysosomal proteases observed in the PMN of uraemics inour study.
Our results indicate that defective PMN function may be thebasis of immune dysfunction in uraemic patients. Little is knownabout the mechanism leading to neutrophil dysfunction. How-ever, Vanho1der et al. have identified the presence of two differentcompounds in the plasma of uraemic patients that depress thehexose monophosphate shunt activity relating to phagocytosis-associated respiratory burst in neutrophils." Cohen et al. sug-gested that the presence of p-cresol in uraemic serum impairs therespiratory burst activity of PMN.4 However, the definite mecha-nism which causes neutrophil dysfunction in uraemic patients isnot yet known.
REFERENCESMailloux LU, Bellucci AG, Wilkes BM, Napolitano B, Mossey RT, Lesser M, et al.Mortality in dialysis patients: Analysis of the causes of death. Am J Kidney Dis1991 ;8:326--35.
2 Keane WF, Maddy MF. Host defenses and infectious complications in maintenancehemodialysis patients. In: Maher IF (ed). Replacement of renal function by dialysis.Boston:Kluwer Academic Publishers, 1989:865-80.
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. 13, NO.3, 2000
3 Lewis SL, VanEpps DE. Neutrophil and monocyte alterations in chronic dialysispatients. Am J Kidney Dis 1987;9:381-95.
4 Cohen G, Haag-Weber M, Horl WHo Immune dysfunction in uremia. Kidney Int1997;62 (Suppl):S79-582.
5 Haag-Weber M, Horl WHo Uraemia and infection: Mechanisms of impaired cellularhost defense. Nephron 1993;63:125-31.
6 Abrutyn E, Cassizzi A, Root RK. Inhibited chemotaxis in uraemia. c/in Res 1977;25:371A.
7 Ritchey EE, Wallin JD, Shah SV. Chemiluminescence and superoxide anion pro-duction by leukocytes from chronic hemodialysis patients. Kidney lnt 1981;19:349-58.
8 Leigh PJ, Vanfurth R, Bazivet TL. In vitro determination of phagocytosis andintracellular killing by polymorphonuclear and mononuclear phagocytes. In: WeirDM (ed). Handbook of immunology. Vol. II. Oxford: Blackwell Scientific, 1986:563-4.
9 Wood SM, WhiteAG. A micro-method for the estimation of killing and phagocytosisof Candida albicans by human leucocytes. J Immunol Methods 1978;20:43-52.
10 Babior BM. Oxygen-dependent microbial killing by phagocytes. N Engl J Med1978;298:659-68.
II Thurman RG, Ley HG, Scholz R. Hepatic microsomal ethanol oxidation: Hydrogenperoxide formation and the role of catalase. Eur J Biochem 1972;25:420-30.
12 Klebanoff SJ. Antimicrobial mechanisms in neutrophilic polymorphonuclear leuko-cytes. Semin Hematol 1975;12:117-42.
13 Spitzwagel JK. Antibiotic proteins of human neutrophils. J CUn Invest 1990;86:1318-20.
14 Vanholder R, Ringoir S. Polymorphonuclear cell function and infection in dialysis.Kidney Int 1992;38 (Suppl 42):S91-595.
15 Mahajan S, Kalra OP, Tripathi AK, Chakrabarty AK. Polymorphonuclear phagocyticfunction in patients with chronic renal failure and effect of acute haemodialysis.Indian J NephroI1999;4:164-7.
16 Vanholder R, De Smet R, Jacobs V, Van Landschoot N, Waterloos MA, VogeleereP, et al. Uraemic toxic retention solutes depress polymorphonuclear response tophagocytosis. Nephrol Dial Transplant 1994;9:1271-8.
17 Porter CJ, Burden RP, Morgan AG, Daniels I, Fletcher J. Impaired bacterial killingand hydrogen peroxide production by polymorphonuclear neutrophils in end-stagerenal failure. Nephron 1997;77:479-81.
18 Ward RA, McLeish KR. Polymorphonuclear leukocyte oxidative burst is enhancedin patients with chronic renal insufficiency. JAm Soc NephroI1995;5:1697-702.
19 PorterCJ, Burden RP, Morgan AG, Daniels I, Fletcher J. Impaired polymorphonuclearneutrophil function in end-stage renal failure and its correction by continuousambulatory peritoneal dialysis. Nephron 1995;71:133-7.
20 Stinavage P, Martni LE, Spitznagel JK. 0 antigen and lipid A phosphoryl groups inresistance of Salmonella typhimurium LT-2 to nonoxidative killing in humanpolymorphonuclear neutrophils. Infect Immun 1989;57:3894-900.
Know ledge and attitudes of rural adolescent girls regardingreproductive health issues
D. PATTANAIK, J. LOBO, S. K. KAPOOR, P. S. N. MENON
ABSTRACTIJdckground. Adolescent girls (10-19 years old) comprise
about 22% of women in India. They are the mothers oftomorrow and the burden of planned reproduction rests on
All India Institute of Medical Sciences, New Delhi 110029, IndiaD. PATTANAIK, J. LOBO, S. K. KAPOOR
Centre for Community MedicineP. S. N. MENON Department of Paediatrics
Correspondence to P. S. N. MENON
© The National Medical Journal of India 2000
them. Yet very little is known about their knowledge and attitudestowards reproductive health issues-a crucial aspect if India is toachieve the net reproduction rate of 1 by AD 2016. This studyaimed to gather information on areas required for the planningof family life education strategies.
Methods. This cross-sectional study was conducted in thegovernment schools and anganwadi premises of three villages ofthe primary health centre, Chhainsa, under the ComprehensiveRural Health Services Project Area (CRHSP), Ballabgarh, Haryana.The participants were 254 girls aged 13 to 17 years, who had

PATTANAIK et al. : RURAL ADOLESCENT GIRLS AND REPRODUCTIVE HEALTH 125
attained menarche. A pre-tested interview schedule was admin-istered to each girl after taking permission from the principals andparents and with the consent of the participants. The knowledgeand attitudes regarding age at marriage, concept of small familynorm, family size and preference for a son were assessed.
Results. All the giriswere aware that there Isa law regardinglegal age of marriage but only 165 (65%) of them knew thecorrect legai age. Early marriage was preferred by 19 (7.6%).Though 214 (84.3%) girlswere aware of the small family norm,only 19 (8.8%) knew the exact norm. A preferred family sizeoftwo or lesswas reported by 151 (59.2%). Preference for a sonwas reported by 233 (91.7%).
Conduslon. Ail the girlswere aware of the small family norm,but few could correctly define It. Though most girls preferred atwo-child family, almost all of them had a preference for at leastone son. This preference for a son could dominate their futuredecision-making. As attitude development isa long-term process,there is Indeed a long way to go.Natl Med J India 2000; 13: 124-8
INTRODUCTIONThe current world population of young people aged between 10and 19 years is over one billion. 1 In India, adolescent girls (10-19years) comprise about 22% of women.' Marriage at a younger ageputs them at a greater risk of giving birth to a stillborn child or onewho is premature or has low birth-weight. They are also moreprone to complications of delivery.' The percentage contributedby 15-19-year-olds to the total fertility rate (TFR) varies between4% and 15% in South-east Asia.' In India, 10% of the birthsreported are amongst girls less than 20 years of age. The report ofthe Registrar General of India on national fertility stated that girlswho marry before the age of 18 years gave birth to a larger numberof children than those who married later. Some demographershave estimated that if marriages were postponed to 20-21 years ofage, the birth rate would decrease by 20%-30%.5
Family well-being depends on the age at marriage and pre-ferred number of children, thus making the adolescent's percep-tion of reproductive health important for planners.
The TFR is higher in rural than in urban areas. It is 4 childrenper woman or higher in the states of Uttar Pradesh, Bihar, Haryanaand Arunachal Pradesh. According to the National Family HealthSurvey (NFHS) report of 1992-93, the TFR for India was 3.4 perwoman, which is slightly lower than the Sample RegistrationSystem estimate of 3.6 for 1991.6 The women-to-men ratio hasdeclined from 934:1000 in 1981 to 927:1000 in 1991. The genderratio is considerably lower in the National Capital Territory ofDelhi (824), Rajasthan (880) and Haryana (888).6.7
To control the population explosion, the Government of Indiaformulated its population policy in 1976 and modified it in 1977.The reviewed national population policy of 1986 aimed to achievea net reproduction rate (NRR) of 1 by the year AD 2016 (initially2000, then 2006).8 This revision indicates that the reduction inpopulation growth requires more than just the introduction offamily planning methods. First, a change in the attitude of womenand men is essential. Second, an understanding of the knowledgeand attitudes of adolescent girls regarding reproductive health isnecessary to help plan appropriate education strategies. We as-sessed the knowledge and attitudes regarding age at marriage,concept of small family norm, family size and preference for a sonamong adolescent rural girls of Haryana.
SUBJECTS AND METHODSThis cross-sectional study was conducted in government schoolsand anganwadi premises of selected villages under the PrimaryHealth Centre (PHC) at Chhainsa, district Faridabad, Haryanawhich falls under the Comprehensive Rural Health ServicesProject (CRHSP) of the All India Institute of Medical Sciences(AIIMS), New Delhi. Of the 9 villages under PHC Chhainsa, 3were selected for the study as they were comparable with respectto the socio-economic and literacy status of the population. Thetotal population of the 3 villages was 18750. This study was partof a larger study on sexual maturity rating of rural adolescent girls8-17 years of age. The sample size was 500 with 50 girls fromeach age group. All eligible students were covered till the requirednumber of 50 in each group was achieved. Two hundred and fifty-four girls who were in the age group of 13-17 years and girls lessthan 13 years of age who had already attained menarche wereincluded in this study.
Consent was taken from each individual who fulfilled theselection criteria, and permission for interviews was obtainedfrom the principals and parents. The purpose of the interview wasexplained to all the girls and confidentiality assured. They wererequested not to disclose the questions or answers to their col-leagues till the completion of the study. This was done to avoid acontamination effect.
A structured pre-tested close-ended interview schedule wasadministered to each subject at school or in the anganwadipremises. The interview focused on the age at marriage, smallfamily norm and preference for a son. Subjects who were absenton the day of the visit were contacted by other students or teachersand requested to be present in school on the next visit of theinvestigator. Girls aged 16 and 17 years, if not found in schoolsin adequate numbers (because of a high drop-out rate), werecontacted at home with the help of the local health worker. Thegirls were asked to assemble in the respective anganwadis duringthe afternoon on specified days. As both the investigator andMedical Officer of Chhainsa were women, the girls were comfort-able during the interview.
RESULTSA total of 254 girls were evaluated regarding their knowledge andattitudes towards future reproductive health issues.
Legal age at marriageAll the girls were aware that there was a minimum legal age formarriage for girls, but only 165 (65%) could accurately define theage as 18 years, as stated in the Marriage Restraint Act. 10 Therewere 4 girls who were already married at the time of interview andwere among the 35% girls who did not know the minimum age atmarriage.
Preferred age for marriageTo find out their attitude towards early marriage, unmarried girlswere asked at which age they would like to get married. Only 19(7.6%) preferred marriage before the legal age of 18 years, while27 (10.8%) wanted to leave the decision regarding age of marriageto their parents. Though the correct awareness response for legalage was only 65%, the responsible attitude for preferred age ofmarriage was 74% among these rural girls, There were 15girls outof 165 who had the knowledge but could not reflect the positiveattitude. On the other hand, 35 girls without the knowledgeshowed a responsible attitude (Table I).
126
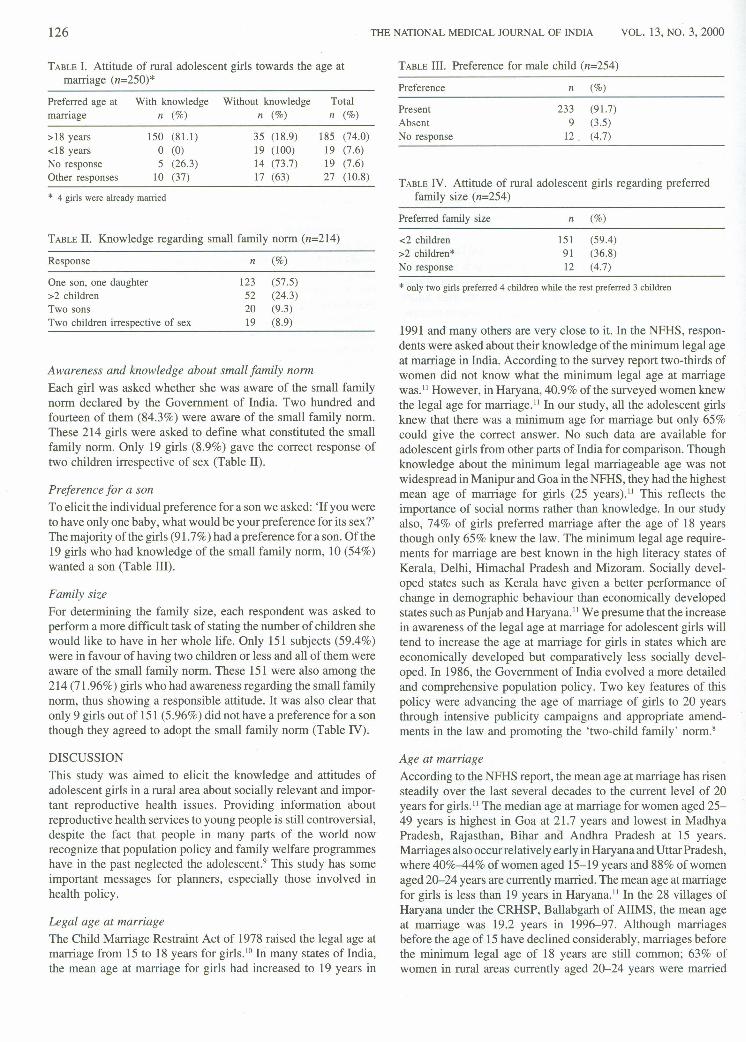
TABLE1. Attitude of rural adolescent girls towards the age atmarriage (n=250)*
Preferred age at With knowledge Without knowledge Totalmarriage n (%) n (%) n (%)
>18 years 150 (81.1) 35 (18.9) 185 (74.0)<18 years 0 (0) 19 (100) 19 (7.6)No response 5 (26.3) 14 (73.7) 19 (7.6)Other responses 10 (37) 17 (63) 27 (10.8)
* 4 girls were already married
TABLEII. Knowledge regarding small family norm (n=214)
Response n (%)
One son, one daughter 123 (57.5)>2 children 52 (24.3)Two sons 20 (9.3)Two children irrespective of sex 19 (8.9)
Awareness and knowledge about small family normEach girl was asked whether she was aware of the small familynorm declared by the Government of India. Two hundred andfourteen of them (84.3%) were aware of the small family norm.These 214 girls were asked to define what constituted the smallfamily norm. Only 19 girls (8.9%) gave the correct response oftwo children irrespective of sex (Table 11).
Preference for a sonTo elicit the individual preference for a son we asked: 'If you wereto have only one baby, what would be your preference for its sex?'The majority of the girls (91.7%) had a preference for a son. Of the19 girls who had knowledge of the small family norm, 10 (54%)wanted a son (Table III).
Family sizeFor determining the family size, each respondent was asked toperform a more difficult task of stating the number of children shewould like to have in her whole life. Only 151 subjects (59.4%)were in favour of having two children or less and all of them wereaware of the small family norm. These 151 were also among the214 (71.96%) girls who had awareness regarding the small familynorm, thus showing a responsible attitude. It was also clear thatonly 9 girls out of 151 (5.96%) did not have a preference for a sonthough they agreed to adopt the small family norm (Table IV).
DISCUSSIONThis study was aimed to elicit the knowledge and attitudes ofadolescent girls in a rural area about socially relevant and impor-tant reproductive health issues. Providing information aboutreproductive health services to young people is still controversial,despite the fact that people in many parts of the world nowrecognize that population policy and family welfare programmeshave in the past neglected the adolescent." This study has someimportant messages for planners, especially those involved inhealth policy.
Legal age at marriageThe Child Marriage Restraint Act of 1978 raised the legal age atmarriage from 15 to 18 years for girls. 10 In many states of India,the mean age at marriage for girls had increased to 19 years in
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. 13,No.3, 2000
TABLEIII. Preference for male child (n=254)
Preference n (%)
PresentAbsentNo response
233 (91.7)9 (3.5)
12 (4.7)
TABLEIV. Attitude of rural adolescent girls regarding preferredfamily size (n=254)
Preferred family size n (%)
<2 children 151 (59.4)>2 children* 91 (36.8)No response 12 (4.7)
* only two girls preferred 4 children while the rest preferred 3 children
1991 and many others are very close to it. In the NFHS, respon-dents were asked about their knowledge of the minimum legal ageat marriage in India. According to the survey report two-thirds ofwomen did not know what the minimum legal age at marriagewas." However, in Haryana, 40.9% ofthe surveyed women knewthe legal age for marriage. II In our study, all the adolescent girlsknew that there was a minimum age for marriage but only 65%could give the correct answer. No such data are available foradolescent girls from other parts of India for comparison. Thoughknowledge about the minimum legal marriageable age was notwidespread in Manipur and Goa in the NFHS, they had the highestmean age of marriage for girls (25 years ).11 This reflects theimportance of social norms rather than knowledge. In our studyalso, 74% of girls preferred marriage after the age of 18 yearsthough only 65% knew the law. The minimum legal age require-ments for marriage are best known in the high literacy states ofKerala, Delhi, Himachal Pradesh and Mizoram. Socially devel-oped states such as Kerala have given a better performance ofchange in demographic behaviour than economically developedstates such as Punjab and Haryana." We presume that the increasein awareness of the legal age at marriage for adolescent girls willtend to increase the age at marriage for girls in states which areeconomically developed but comparatively less socially devel-oped. In 1986, the Government of India evolved a more detailedand comprehensive population policy. Two key features of thispolicy were advancing the age of marriage of girls to 20 yearsthrough intensive publicity campaigns and appropriate amend-ments in the law and promoting the 'two-child family' norm."
Age at marriageAccording to the NFHS report, the mean age at marriage has risensteadily over the last several decades to the current level of 20years for girls. 11 The median age at marriage for women aged 25-49 years is highest in Goa at 21.7 years and lowest in MadhyaPradesh, Rajasthan, Bihar and Andhra Pradesh at 15 years.Marriages also occurrelatively early in Haryanaand Uttar Pradesh,where 40%-44% of women aged 15-19 years and 88% of womenaged 20-24 years are currently married. The mean age at marriagefor girls is less than 19 years in Haryana. II In the 28 villages ofHaryana under the CRHSP, Ballabgarh of AIIMS, the mean ageat marriage was 19.2 years in 1996-97. Although marriagesbefore the age of 15 have declined considerably, marriages beforethe minimum legal age of 18 years are still common; 63% ofwomen in rural areas currently aged 20-24 years were married

PATIANAIK et al. : RURAL ADOLESCENT GIRLS AND REPRODUCTIVE HEALTH 127
before 18years of age. II It was encouraging to find that 74% of theadolescent girls in this study were in favour of marriage after 18years of age. However, even in this study 4 girls out of 254 0.6%)were already married before the age of 18 years (school going anddrop-outs). Srinivasa et al. in a study conducted in one of theIntegrated Child Development Services Project areas of Pondi-cherry, reported that only 3% of the girls considered less than 18years as the right age for girls to marry. 12Talwar and Mehra in theirstudy of 220 adolescent girls in an urban slum of Delhi, found that18% of the girls were already married and the mean age atmarriage in that area was 16.7 years. 13Doibala et al. in their studyof 213 adolescents in a rural area of Maharashtra, found that themean age at marriage for girls was 16.1 years and 78.2% of girlswere married below the legal age." The situation is far from satis-factory in the South Asian region-25% of girls below 14 yearsare married in Bangladesh and about 35% of girls below 15 yearsin Nepal."
Children bearing children is a mockery of the system ofplanned parenthood.' Childbearing in India is concentrated in theage group 15-29 years, contributing to more than three-fourths ofthe TFR. 11 Current fertility is characterized by a substantialamount of early childbearing; 17% of total fertility is accountedfor by births to women aged 15-19 years. Goa has a unique patternof childbearing, with very low fertility before 25 years of age asa result of a high average age at marriage and the late initiation ofchildbearing. On the other hand, fertility is 4 children per womanor higher inUttar Pradesh, Bihar, Haryana and Arunachal Pradesh. II
Preferred family sizeIn our study, 96.2% of adolescent girls were able to give a numericresponse to preferred family size, as compared to the NFHS where90% of women responded to this question. In our study, 59.4%responses were in favour of a two-child family. Srinivasa et al.reported that 76% of girls were in favour of the 'two-child norm' YIn the NFHS for two-thirds of women, the ideal number ofchildren fell within the narrow range of 2-3 children, though theTFR was 3.4. Thus, although the 'two-child family' norm cannotbe said to exist in India at this time, the majority of womenconsider a small or moderate size family as ideal rather than a verylarge one. For India as a whole, the TFR would drop by 22% ifunwanted pregnancies could be eliminated. In Haryana, thewanted TFR is at least one child less than the actual TFR. On theother hand, the smallest differences between the wanted TFR andactual TFR are seen in Kerala and Mizoram (0.2 child)." We seemto be far away from the goal especially in rural Haryana. If thefertility preferences of adolescent girls can be moulded to adoptthe small family norm, considerable progress can be made to-wards achieving the population goals.
Preference for a sonTo achieve the national target of net reproduction rate of 1 by theyear 2016, the current emphasis by the Government of India is onthe theme 'son or daughter, two will do'. Parental attitudes andaspirations regarding the gender of their children have attractedconsiderable research interest because of the belief that genderpreferences may sustain higher fertility levels than would be thecase if parents are indifferent to the gender of their children. IS
Researchers argue that childbearing may continue beyond apreferred family size if women desire a particular combination ofsons and daughters. Numerous studies in India including theNFHS have found a strong preference for sons, particularly innorth India. 16-20The preference for a son is stronger in rural than
in urban areas.The preference of rural girls in Haryana is also not different.
The results of the Kanpur survey from north India provideadditional support that women express higher fertility preferencesthan husbands and this is largely the result of their preference fora higher mean number of additional sons." The pronouncedpreference for sons among women in South Asia has been dem-onstrated in a number of studies.20.22.23Both women's strongpreferences for sons and their limited influence in decision-making contribute significantly to higher fertility in patriarchalsocieties." The current age structure and the fertility and mortalitypatterns in India have an in-built momentum for continued popu-lation growth."
It is time that information regarding the population policy andfamily welfare programmes is provided to young adolescent girlsto achieve the national demographic goal in the defined period.Consolidated effort is needed to bridge the prevailing knowledgegap among rural adolescent girls regarding the population policythrough school health programmes or other existing programmes.It is essential to change the attitude, because it is subject to socialpressures. Education about the small family norm needs to beincorporated into the lifestyle of the adolescent girl to ensure thatshe will have a responsible behaviour towards population issuesas well as her own life.
REFERENCESNoble J, Cover J, Yanagishita M. The world's youth 1996. Washington, DC:Population References Bureau, 1996.
2 Government of India. Percentage distribution of population by sex and age groupsduring 1981 Census. In: Health information of India. New Delhi:DirectorateGeneral of Health Services, 1991:12.
3 Friedman HL. The health of adolescents and youth: A global overview. WorldHealth Stat Q 1985:38:256-62.
4 Rogston E, Armstrong S. Preventing maternal deaths. Geneva:Worid HealthOrganization, 1989:33,71,107.
5 Office of Registrar General. Sample Registration System-I99I. NewDelhi:Ministryof Home Affairs, 1993.
6 India International Institute for Population Sciences. National Family HealthSurvey 1992-93, Introductory Report. Bombay, 1993:17.
7 Nagaraj K. The missing women: The declining sex ratio. Frontline 1991:88-96.8 Central Health Education Bureau (DGHS). Future goals and new approaches in the
new National Family Welfare Strategy. Swasth Hind 1986;30:292.9 Senanayake P. Research needs in adolescent sexual and reproductive health.
Reproductive health research the new directions, Biennial Report, WHO 1996-9725th Anniversary Issue. Geneva:Worid Health Organization, 1998:132-7.
10 Sadashivaiah K, Ramesh AS, Sinha JS. Age at marriage in India-The implicationsof the new legislations in the light of 1971Census data. J Family Welfare 1981;27:39-45.
II India International Institute for Population Sciences. National Family HealthSurvey 1992-93. New Delhi:Ajanta Offset, 1995:77-197.
12 Srinivasa K, Sahai A, Ramalingam G, Premarajan KC. Knowledge and perceptionof adolescents regarding factors affecting family formation. J Family Welfare 1993;39:47-51.
13 Talwar R, Mehra M. Health profile of adolescent girls in an urban slum. Souvenirof the 26th Annual conference of Indian Association of Preventive and SocialMedicine, Surat, 1999 [Abst]:96.
14 Doibala MK, Mahajan SM, Nimale NE, Ankushe RT. Health status of adolescentsin the rural area of Maharashtra state. Souvenir of the 26th Annual Conference ofIndian Association of Preventive and Social Medicine, Surat, 1999 [Abst]:162.
15 Cleland J, Verrall J, Vassen M. Preferences for the sex of children and theirinfluence on reproductive behaviour. In: World Fertility Survey ComparativeStudies (27). Voorburg: International Statistical Institute, 1983.
16 Das Gupta M. Selective discrimination against female children in rural Punjab,India. Population Dev Rev 1987;13:77-101.
17 Miller BD. The endangered sex: Neglect of female children in rural north India.Ithaca, New York:Cornell University Press, 1981.
18 Population Research Centre. People's perception and reproductive behaviour innorthwest India: An interdisciplinary field study of eight districts in Haryana,Himachal Pradesh and Uttar Pradesh. Chandigarh:Centre for Research in Ruraland Industrial Development, 1993.
19 Rastogi SR, Kumari R. Son preference and effectiveness of the Family WelfareProgram in Uttar Pradesh. In: Patil RN (ed). Health environment and population.New Delhi:Ashish Publishing House, 1992:165-79.

128 TIIE NATIONAL MEDICAL JOURNAL OF INDIA
20 Khan ME, Richard A, Ghosh Dastidar SK, Bairathi S. Inequalities between men andwomen in nutrition and family welfare services: An indepth enquiry in an Indianvillage. In: Caldwell JC, Santow G (eds). Selecred reading in culrural, social andbehavioural determinants of healrh. Canberra:Highland Press, 1989:175-99.
21 Michael KA, Gillan FHC. Patriarchy, women's status, and reproductive behaviourin rural north India. Demography India 1992;21:145-66.
VOL. 13, No.3, 2000
22 Ahmed NR. Family size and sex preferences among women in rural Bangladesh.Srudies in Family Planning 1981;12:100--9.
23 Williamson NE. Sons ordaughrers-A cross-cultural survey of 'parental preferences.Beverly Hills, California:Sage Publications, 1976.
24 Registrar General and Census Commissioner (1984). Popularion Projection ofIndia, Paper. New Delhi. 1984.
Attention SubscribersThe subscriptions for The National Medical Journal of India are being servicedfrom the following address:
The Subscription DepartmentThe National Medical Journal of IndiaAll India Institute of Medical SciencesAnsari NagarNew Delhi 110029
The subscription rates of the journal are as follows:
One year Two years Three years
Rs 900$140
IndianOverseas
Rs 500$80
Rs 1300$200
Personal subscriptions paid from personal funds are available at50% discounted rates.
Please send all renewals and new subscriptions along with the payment tothe above address. ChequeslDemand Draft should be made payable toThe National Medical Journal of India. Please add Rs 20 foroutstation cheques.
If you wish to receive the Journal by registered post, please add Rs 60 perannum to the total payment and make the request at the time of subscribing.