kidney transplant case
DESCRIPTION
Kidney transplant case. Niels Marcussen Hans Dieperink Odense University Hospital. Risc factors for the graft. Male_1961. Nephrotic syndrome 2004 MGUS Membranoproliferative glomerulonephritis, with kappa-chains deposits Peritoneal dialysis 2006 Renal transplant 16SEP2008 - PowerPoint PPT PresentationTRANSCRIPT
Kidney transplant caseNiels Marcussen
Hans Dieperink
Odense University Hospital

Risc factors for the graft
Male_1961
• Nephrotic syndrome 2004• MGUS• Membranoproliferative glomerulonephritis, with
kappa-chains deposits• Peritoneal dialysis 2006• Renal transplant 16SEP2008• Living donor, mismatch 4:1• Immediately decreasing s-creatinine • Simulect, Sandimmun, CellCept
Male_1961
• Suspected acute cellular rejection 19SEP2008, s-creatinine rose to 623 µmol/l
• Methylprednisolon intravenously, Prograf replaced Sandimmune
• Graft biopsy delayed to 25SEP2008 due to high MAP. Biopsy 1…..
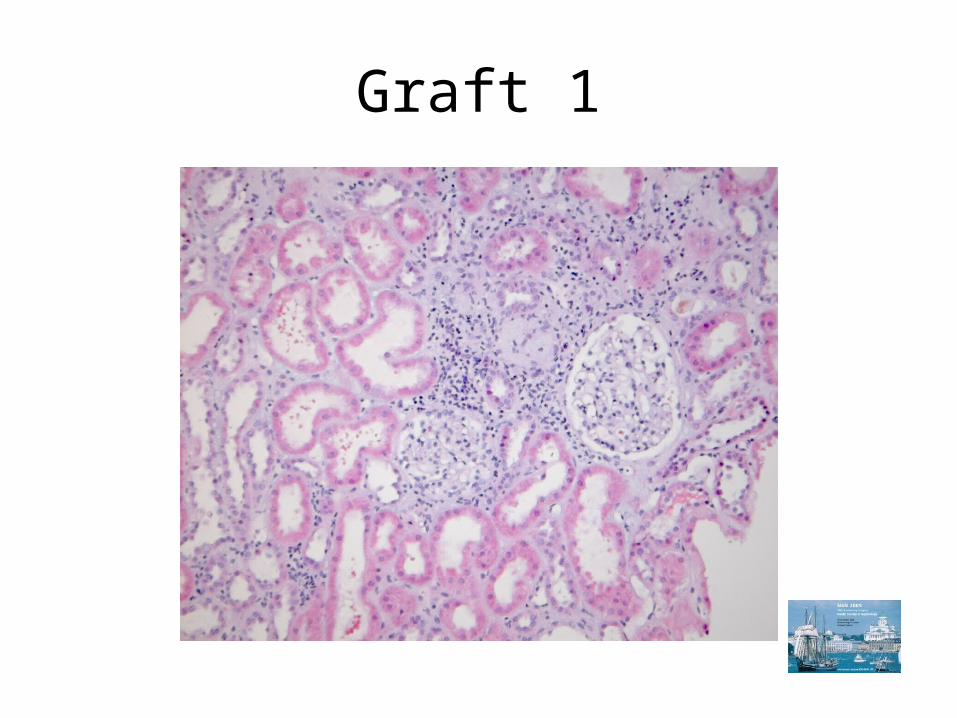
Graft 1
Male_1961
• 08OCT2008 s-creatinine 164 µmol/l
• 14OCT2008: s-creatinine 234 µmol/l; No serum or urine M-komponent
• Graft biopsy 2….
• 24OCT2008: s-creatinine 293 µmol/l, graft biopsy 3….
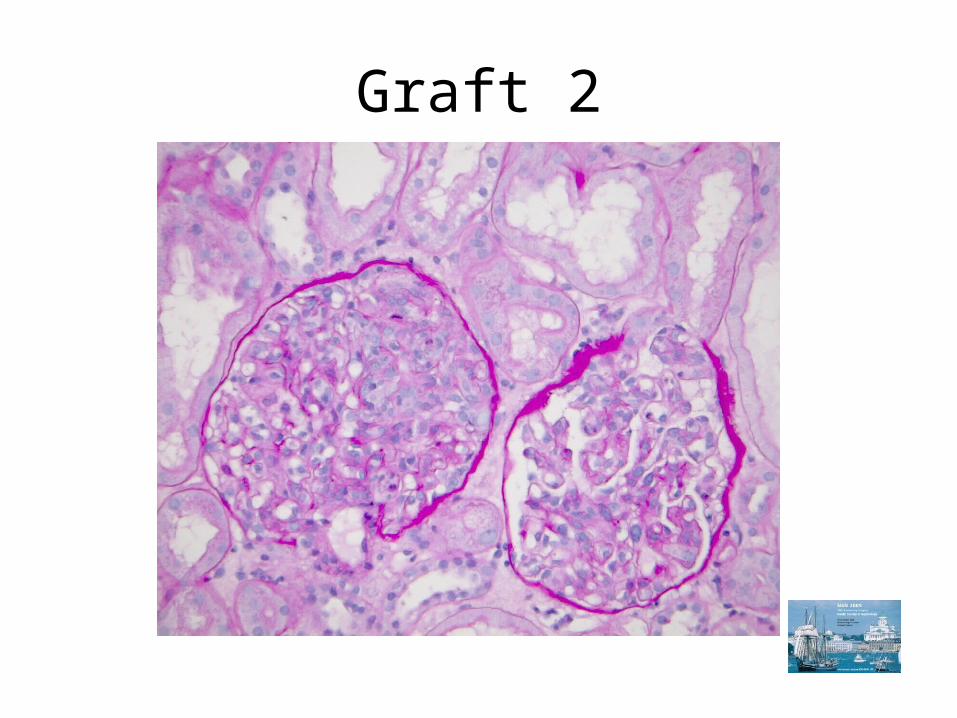
Graft 2
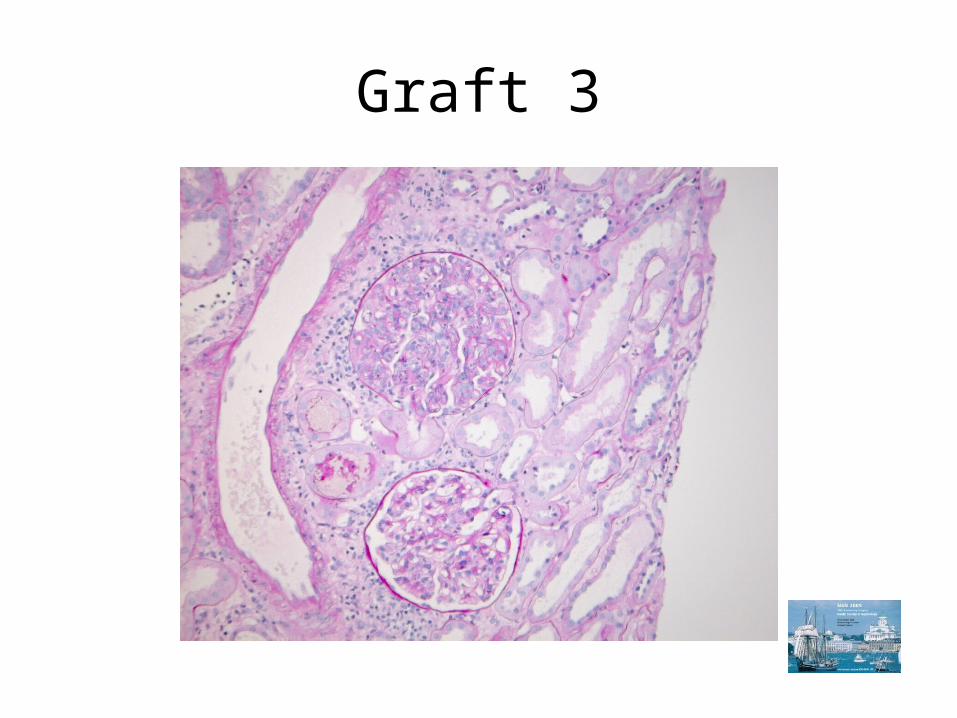
Graft 3
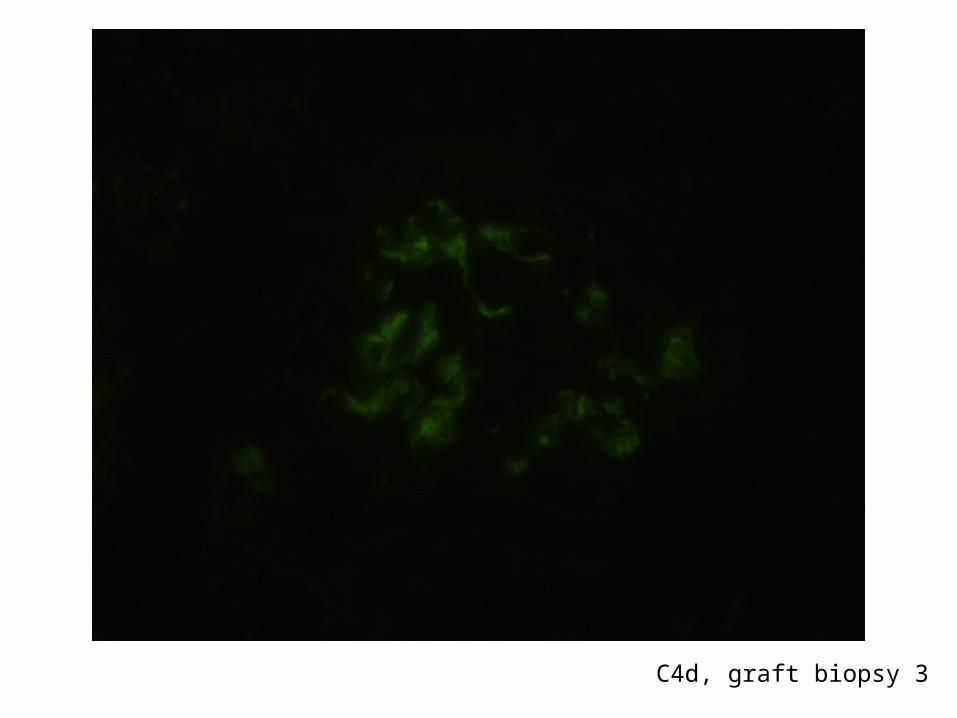
C4d, graft biopsy 3
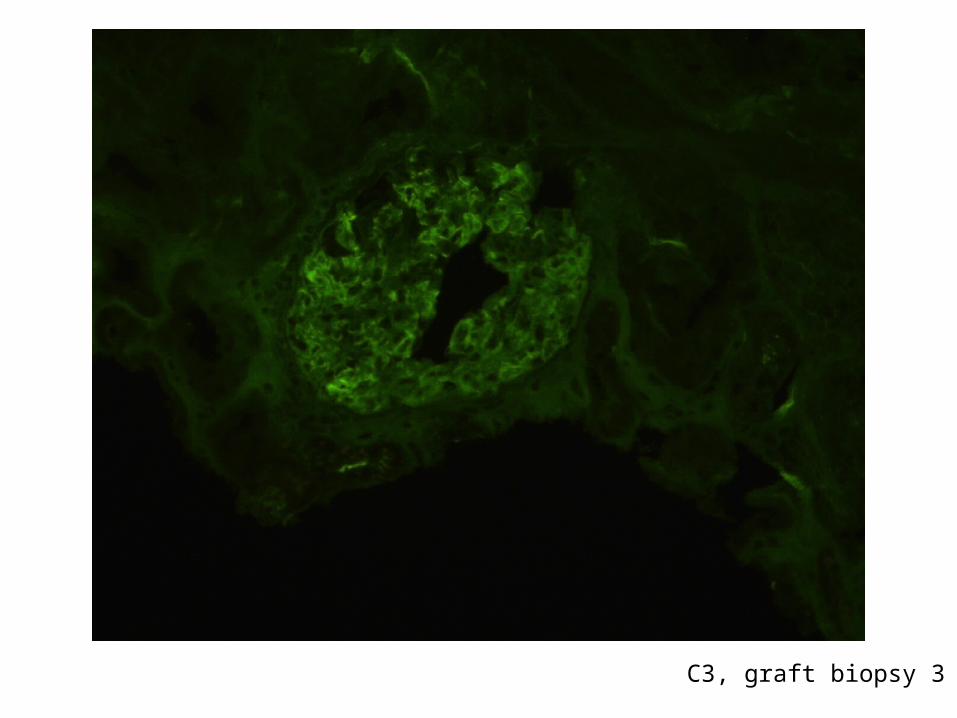
C3, graft biopsy 3
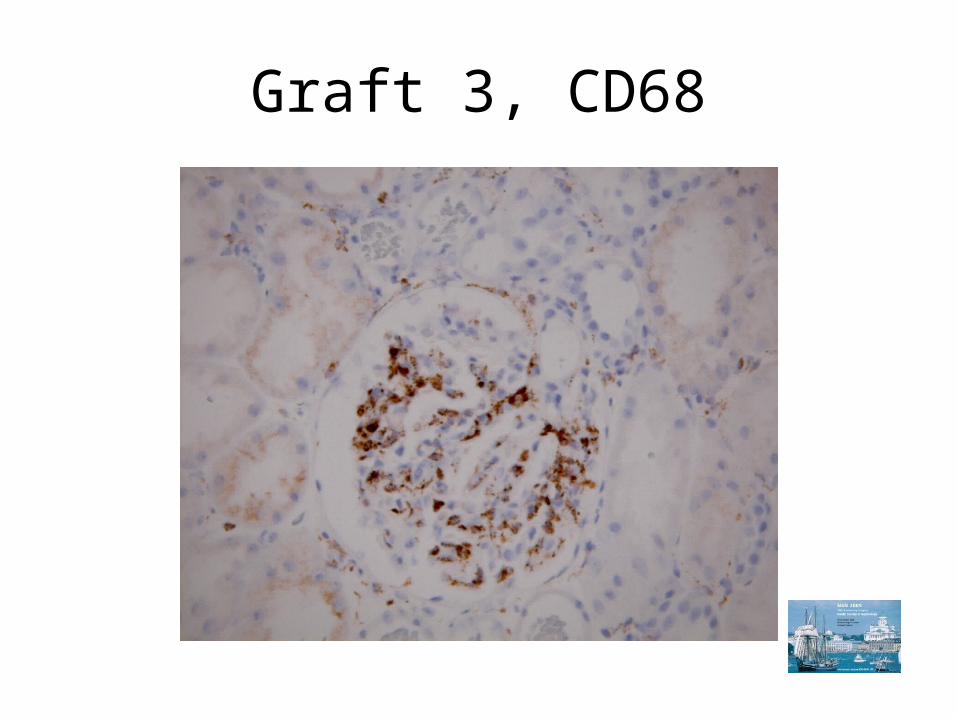
Graft 3, CD68
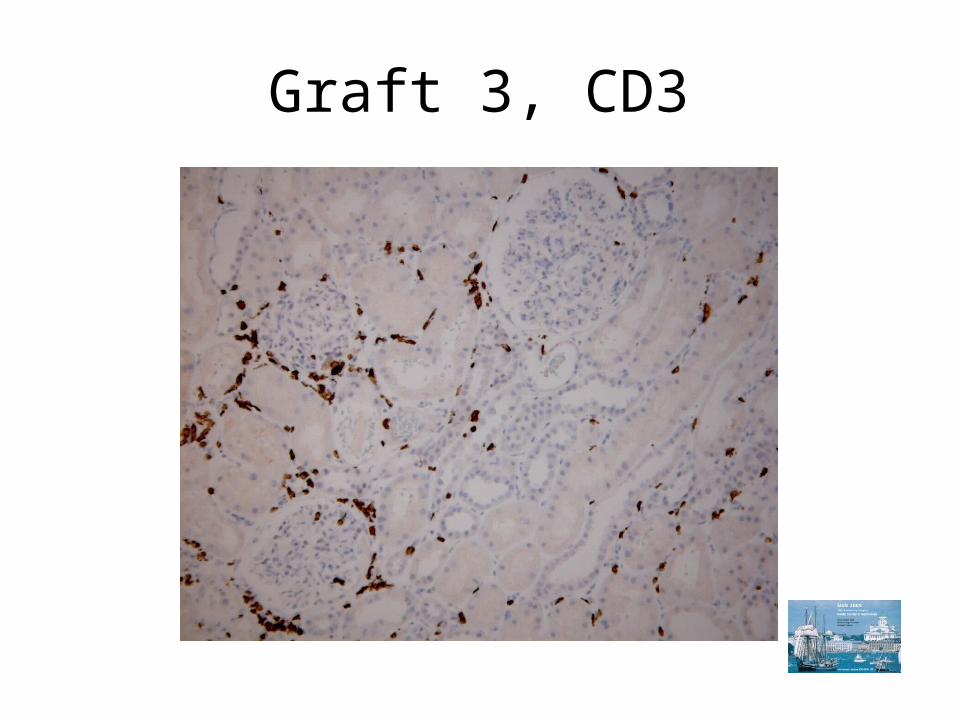
Graft 3, CD3
Male_1961
• 24 OCT2008 Methylprednisolone intravenously
• 17NOV2008: s-creatinine 564 µmol/l, repeat X-match negative, no circulating Class I or II antibodies. Graft biopsy 4…
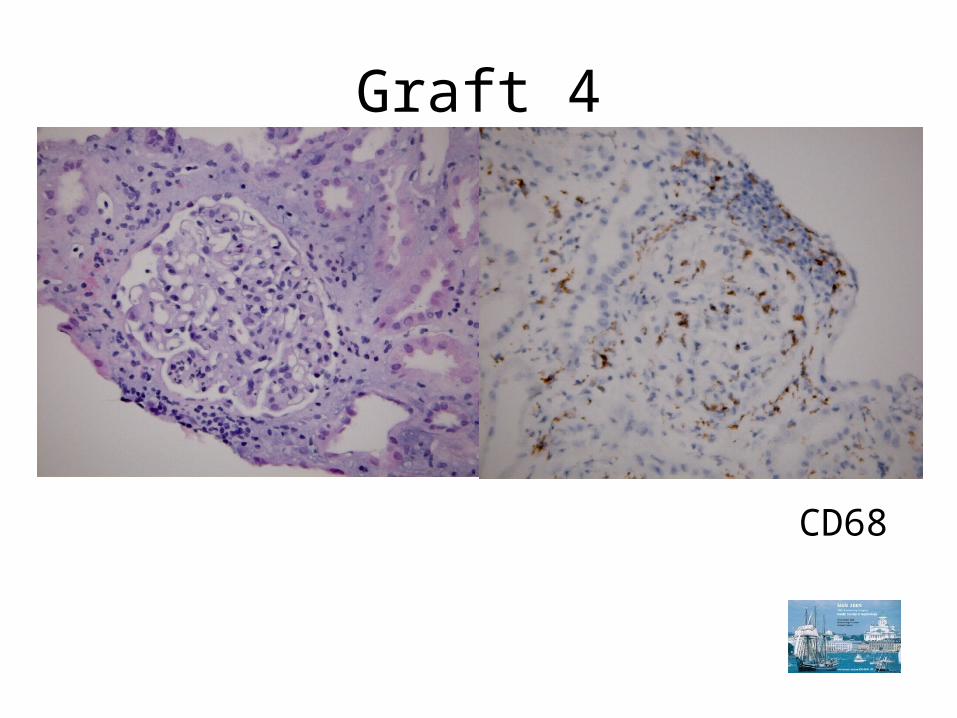
Graft 4
CD68
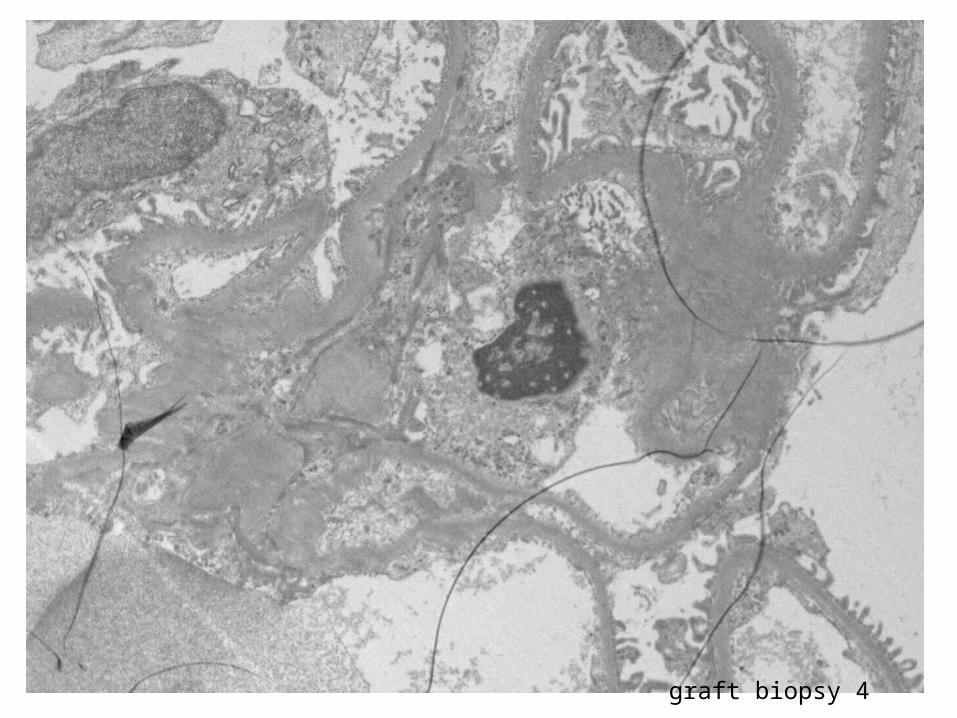
graft biopsy 4
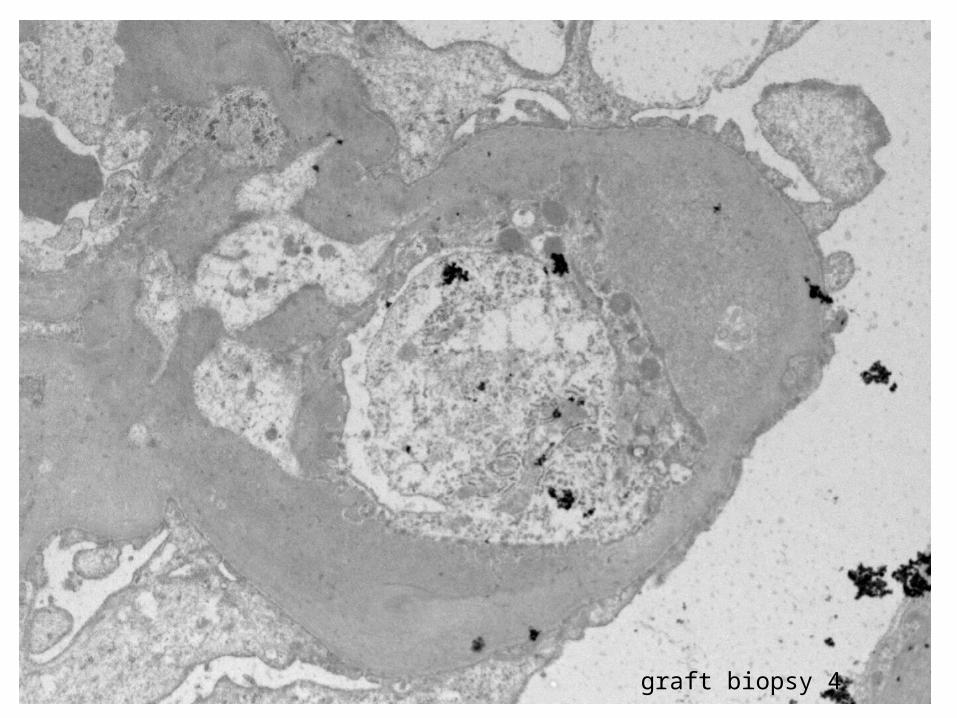
graft biopsy 4
Male_1961
• Intravenous Immunoglobulin 24 gram *2
• 26NOV2008: peritoneal dialysis
• 01DEC2008: graft biopsy 5…
• plasmapheresis * 10 (4 liters, substitution with HA)
• 17DEC2008: CMV PCR positive
• 02JAN2009: graft biopsy 6…
• 10JAN2009: graftectomia
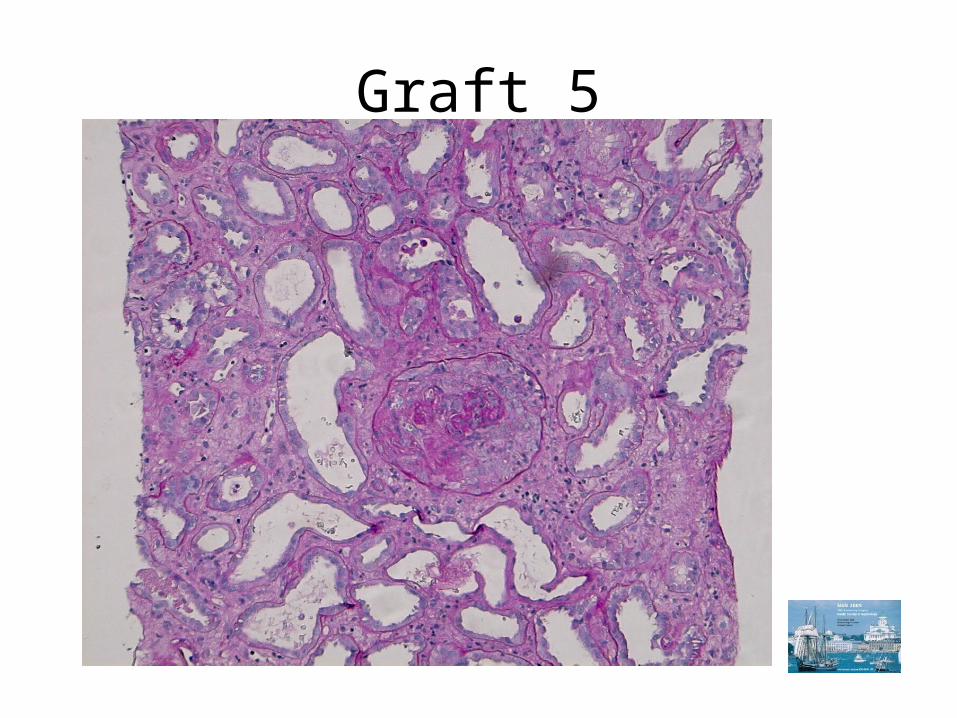
Graft 5
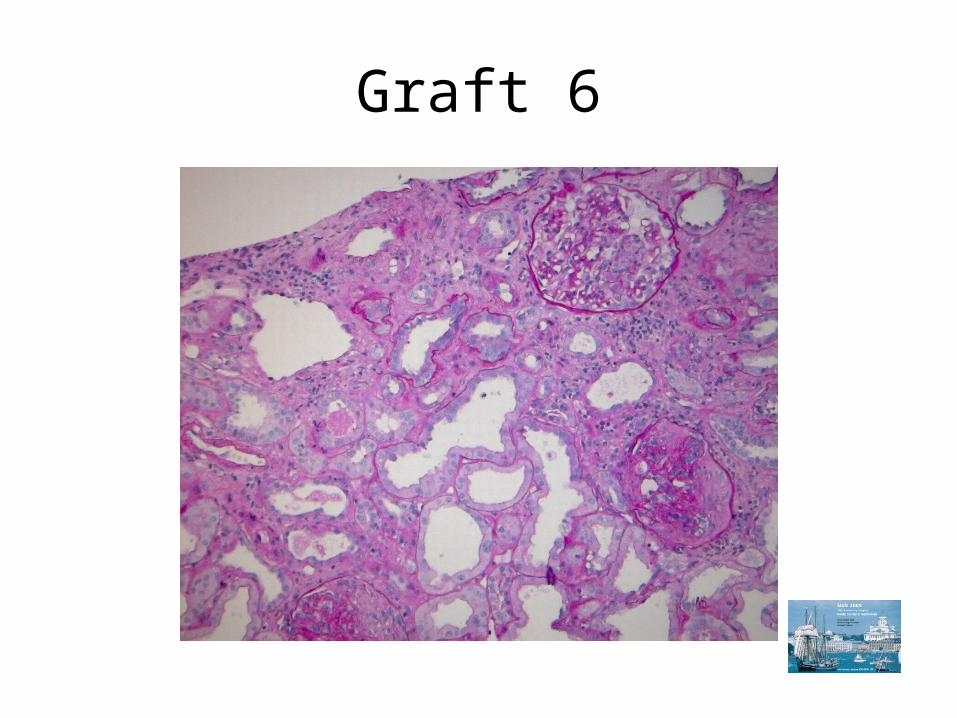
Graft 6
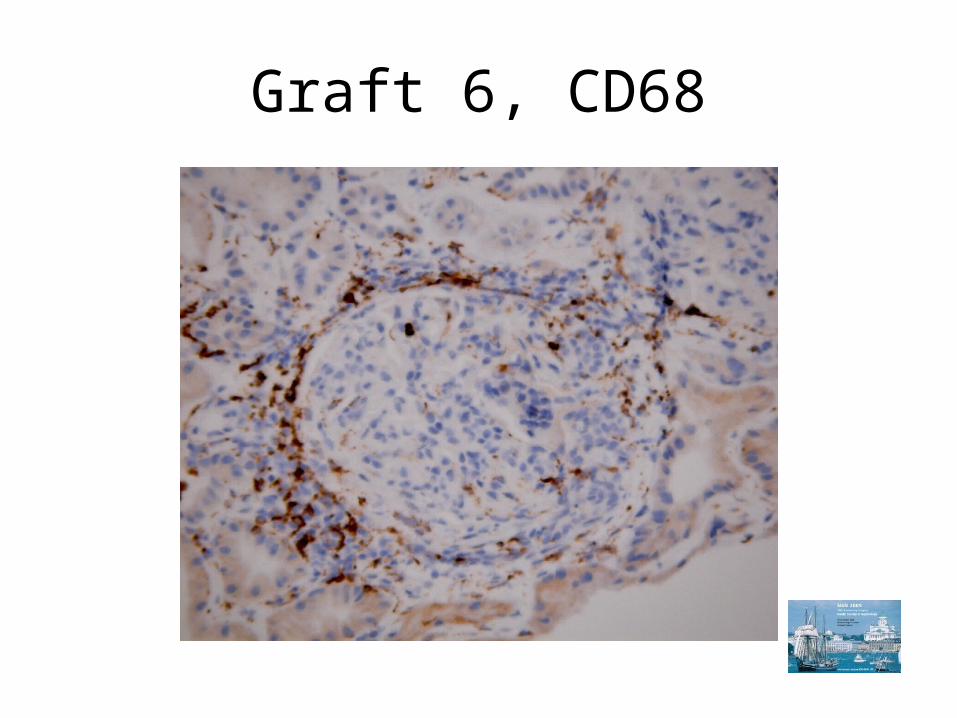
Graft 6, CD68
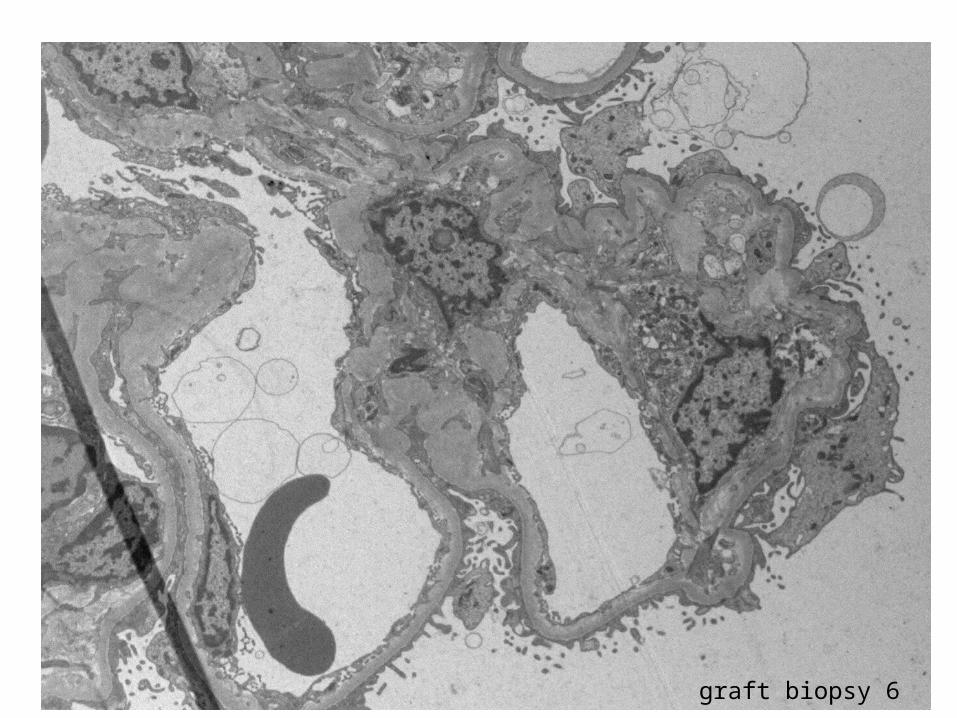
graft biopsy 6
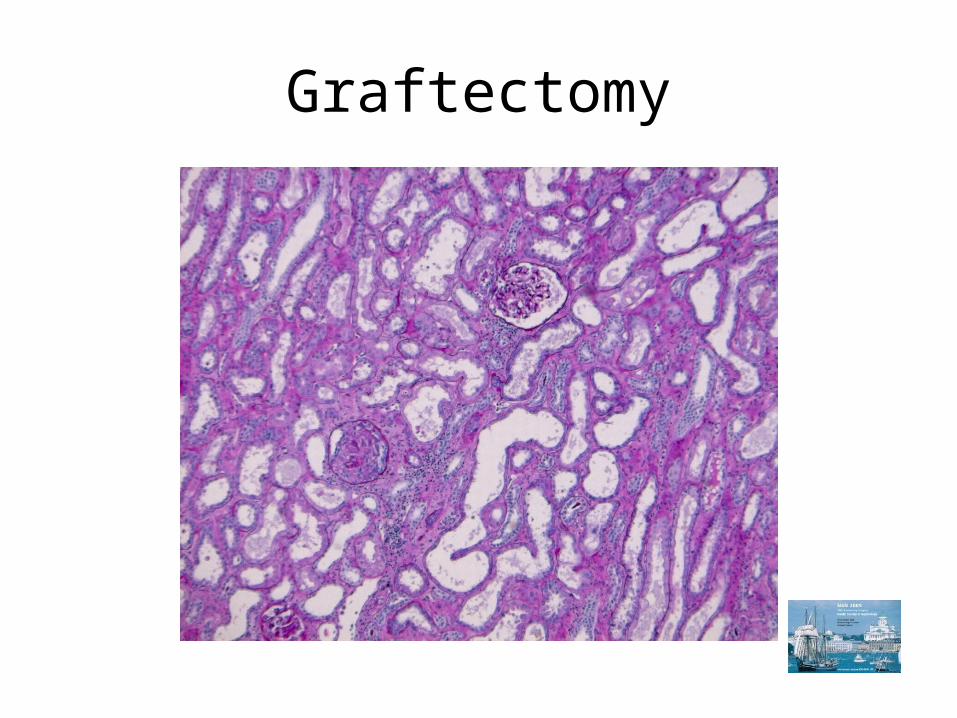
Graftectomy
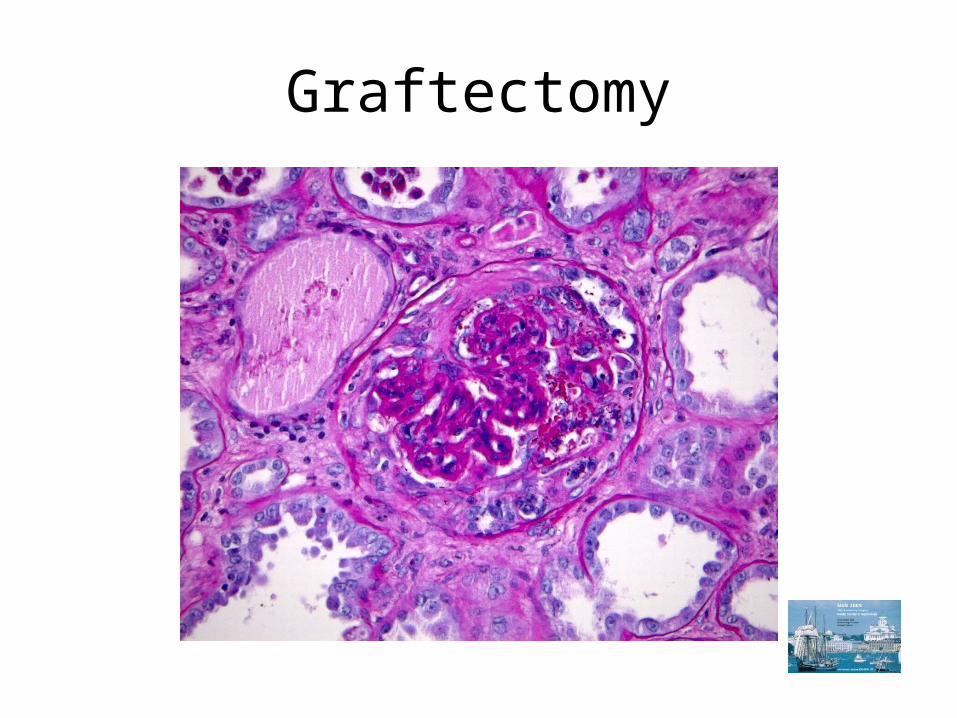
Graftectomy
Your diagnosis?
Glomerulitis in historic perspective
• Richardson et al: Glomerulopathy associated with cytomegalovirus viremia in renal allografts. N Engl J Med 1981
• Olsen S et al. Endocapillary glomerulitis in the renal allograft. Transplantation 1995.
13.5% of biopsies from the first 90 d postTx.
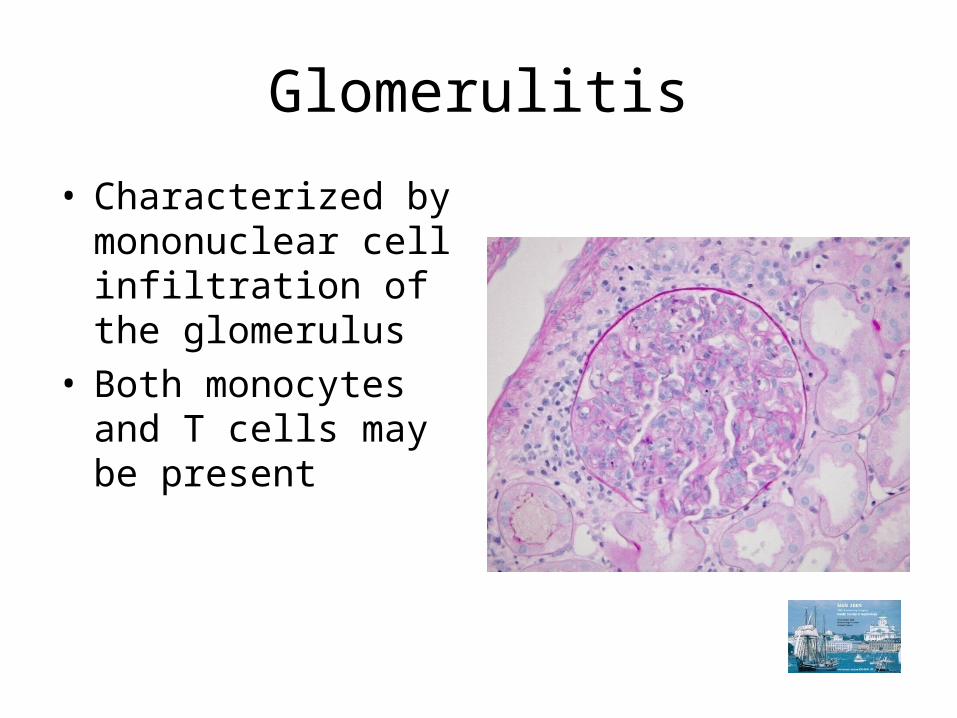
Glomerulitis
• Characterized by mononuclear cell infiltration of the glomerulus
• Both monocytes and T cells may be present
Banff Classification
• g0: No glomerulitis
• g1: Glomerulitis in less than 25% of glomeruli
• g2: Segmental or global glomerulitis in 25% to 75% of glomeruli
• g3: Glomerulitis (mostly global) in more than 75% of glomeruli
The Banff 97 working classification
Differential diagnosis:Recurrent or denovo glomerulonephritisChronic transplant glomerulopathy
Glomerular inflammatory cells Monocytes vs. T cells:Mean monocytes/glomerulus >1 independently predicted poor renal functionat 2 years (Tinckam KJ et al. Kidney Int 68:1866-1874, 2005)
Monocytes is present together with C4d deposition, unlike T cells which are mainly present i cases without C4d deposition (Magil AB, Am
J Kidney Dis 45:1084-1089, 2005)
Correlation to peritubular capillary C4d deposition and to peritubular capillaritis
• Severe glomerulitis was present only in cases with diffuse C4d deposition in the study of 54 renal biopsies by Valente et al.
(Transpl Proceedings 39: 1827-1829, 2007) • 82.8% of biopsies with glomerulitis had
peritubular capillaritis (Gibsin IW et al., Am J Transpl 8:819-825, 2008)
Conclusions
• Glomerulitis was found in 5% of protocol biopsies from stable renal allografts (Gough, Rush et al, NDT 2002;17:1081-1084)
• Glomerulitis was seen in 30-60% of biopsies from patients who had previous positive X-match or previous or current class I or II panel reactive antibodies (Anclicheau et al, Am J Transplant 2007;7:1185-1192).
• Glomerulitis was associated to poor graft outcome when observed in patients with antibody-mediated rejection (Lefaucheur et al, Am J Transplant 2007;7:832-841)
Conclusions
• Glomerulitis, however, did not significantly increase rate of graft loss in patients without evidence of vascular rejection, and was reported not to be an independent predictor of graft survival (Messias et al, Transplantion 2001;72/4:655-660)
• Some degree of glomerulitis is present in most cases of transplant glomerulopathy (i.e., glomerulitis and double contours of GBM)
• Virus, including CMV, may cause glomerulitis (Cathro et al, Am J Kidney Disease 2008;52/1:188-192.)
Conclusions
• Present case was a severe, progressive glomerulitis not related to acute cellular or humoral rejection, to presence of virus in the graft, or to transplant glomerulopathy
• The glomerulitis caused loss of graft function, in spite of conventional anti-rejection therapy, plasmapheresis, and IVIG
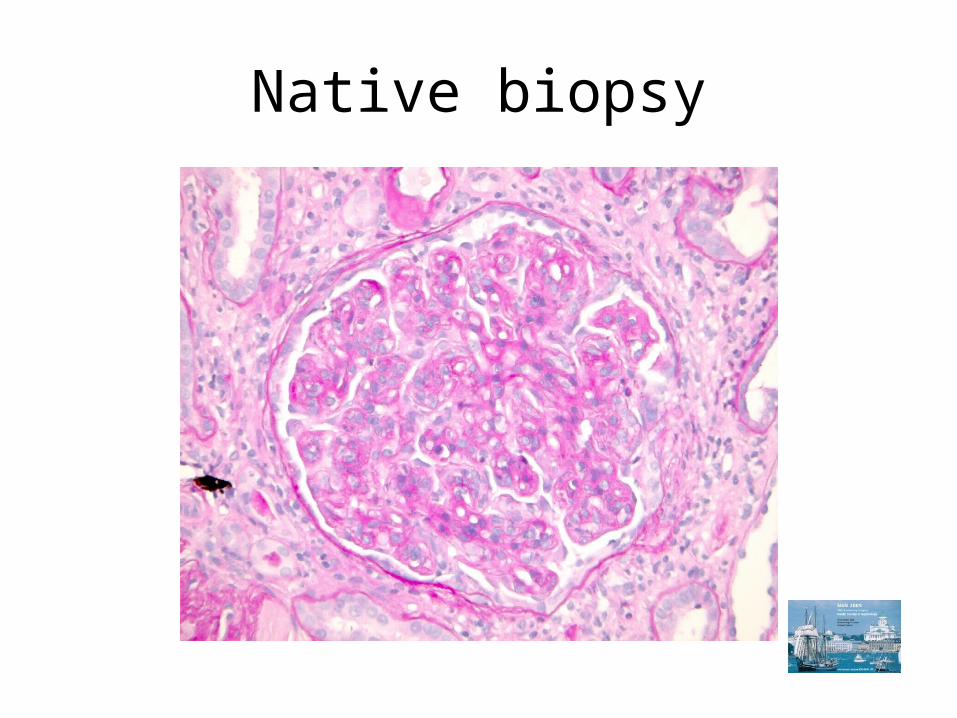
Native biopsy