kidcare call center assessment kidcare call center assessment
TRANSCRIPT

KidCare Call Center Assessment
March 18, 2003
KidCare Call Center Assessment
March 18, 2003
Submitted by:Submitted by:
KidCare Call Center Assessment
March 18, 2003
KidCare Call Center Assessment
March 18, 2003
Submitted by:Submitted by:
KidCare Call Center Assessment
March 18, 2003
KidCare Call Center Assessment
March 18, 2003
Submitted by:Submitted by:
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Table of Contents
Page i ©2003 BearingPoint, Inc.
TABLE OF CONTENTS
1.0 EXECUTIVE SUMMARY.........................................................................................................................1
1.1 REPORT FORMAT.......................................................................................................................................2 1.2 OPERATIONAL ELEMENTS .........................................................................................................................3 1.3 RECOMMENDATIONS .................................................................................................................................3
2.0 BACKGROUND .........................................................................................................................................5
2.1 ASSESSMENT BACKGROUND .....................................................................................................................5 2.2 ASSESSMENT APPROACH...........................................................................................................................6 2.3 KIDCARE BACKGROUND...........................................................................................................................7
3.0 CALL CENTER OPERATIONAL ELEMENTS ..................................................................................11
3.1 MANAGEMENT.........................................................................................................................................12 3.2 WORKFORCE MANAGEMENT...................................................................................................................13 3.3 TRAINING.................................................................................................................................................14 3.4 QUALITY MONITORING ...........................................................................................................................14 3.5 CUSTOMER SERVICE REPRESENTATIVE (CSR) .......................................................................................15 3.6 REPORTING..............................................................................................................................................15 3.7 TECHNOLOGY ..........................................................................................................................................16
4.0 INDIVIDUAL CALL CENTER ANALYSIS AND RECOMMENDATIONS....................................18
4.1 ASSESSMENT SUMMARY .........................................................................................................................18 4.2 ANALYSIS AND RECOMMENDATIONS......................................................................................................19
4.2.1 Member Services (DHACS).............................................................................................................20 4.2.2 KidCare Medicaid (DCF) ...............................................................................................................26 4.2.3 KidCare Outreach (ACS) ................................................................................................................31 4.2.4 Enrollment Enhancement (ACS) .....................................................................................................36 4.2.5 MediKids (ACS) ..............................................................................................................................42
5.0 KIDCARE PROGRAM ANALYSIS.......................................................................................................48
5.1 ANNUAL CALLS HANDLED......................................................................................................................50 5.2 ANNUAL CALLS OFFERED VS. ANNUAL CALLS HANDLED.....................................................................52

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Table of Contents
Page ii ©2003 BearingPoint, Inc.
5.3 AVERAGE CALL HANDLE TIME...............................................................................................................54 5.4 ANNUAL CALLS HANDLED VS. AVERAGE NUMBER OF CSRS ................................................................57 5.5 SERVICE LEVEL: 80% OF CALLS HANDLED IN “Y” SECONDS ................................................................60 5.6 AVERAGE TIME IN QUEUE VS. ABANDONMENT RATE............................................................................62 5.7 CSR TO SUPERVISOR RATIO ...................................................................................................................64 5.8 LENGTH OF NEW CSR TRAINING PERIOD VS. ANNUAL CSR TURNOVER RATE ....................................66
6.0 KIDCARE PROGRAM RECOMMENDATIONS ................................................................................68
7.0 CREDIT CARD PAYMENTS CALL CENTER ANALYSIS AND RECOMMENDATIONS .........78
7.1 OVERVIEW OF CURRENT OPERATIONS....................................................................................................78 7.2 HISTORICAL TRANSACTION VOLUME .....................................................................................................80 7.3 OVERALL RECOMMENDATION ................................................................................................................81 7.4 CONSIDERATIONS ....................................................................................................................................81
APPENDICES
A. DIAGNOSTIC TOOL SAMPLE ............................................................................................................................1
B. BENCHMARKING DATA SOURCES ................................................................................................................23
C. CALL CENTER GLOSSARY .............................................................................................................................24

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 1 – Executive Summary
Page 1 ©2003 BearingPoint, Inc.
1.0 Executive Summary
BearingPoint, formerly KPMG Consulting, was engaged by the Florida Healthy Kids Corporation to
conduct a call center assessment of five separate call centers that provide KidCare customer service.
The goal of the assessment was to assess current operational performance of each call center and
identify opportunities to increase customer satisfaction through process improvements and use of
enabling technologies.
The five call centers included in this assessment are:
Member Service (DHACS)
KidCare Medicaid (DCF)
KidCare Outreach (ACS)
Enrollment Enhancement (ACS)
MediKids (ACS)
As illustrated above, the call centers are referenced by their name, as well as the entity that operates the
call center in parentheses. In some instances, the call center operations are contracted out to an external
organization, such as the Member Services line being operated by a Third Party Administrator, DHACS.
In other instances, the call center is operated by the same administering organization, such as the case
with the KidCare Medicaid call center, which is operated internally by the Department of Children and
Families (DCF).
During the course of this engagement, a sixth call center, Credit Card Payments (FHK), which operates
internally at the Florida Healthy Kids Corporation, was added to the scope of this assessment. This call
center began as a pilot in February 2002 and was implemented without many standard call center
operational elements, processes and technologies. Thus, due to the fact that the call center is
operationally distinct from the original five call centers, the Credit Card Payments (FHK) Call Center
assessment and recommendations are addressed separately in Chapter Seven.
To perform an effective assessment, BearingPoint visited each call center to interview employees and
observe daily operations. In addition, a diagnostic tool was completed by each call center and various
call center materials were requested, gathered and analyzed.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 1 – Executive Summary
Page 2 ©2003 BearingPoint, Inc.
1.1 Report Format
This report is divided into seven chapters and three appendices as follows:
Chapter Number and Name Description of Chapter Content
1.0 - Executive Summary Contains a summary of project goals, approach, methodology
2.0 - Background Provides assessment background, assessment approach and KidCare programs and call centers information
3.0 - Call Center Operations Overview
Identifies, illustrates and explains the seven operational elements used for this assessment
4.0 - Individual Call Center Analysis and Recommendations
Provides a detailed analysis of each call center and also provides recommendation and strength areas
5.0 - KidCare Program Analysis Provides benchmarking information for each call center and includes industry averages for: Federal Government, State Government, and Health Care Industry call centers
6.0 - KidCare Program Recommendations
Provides short-term and long-term recommendations for the overall KidCare program
7.0 - Credit Card Payments (FHK) Assessment and Recommendations
Provides overview, considerations and recommendations for the Credit Card Payments (FHK) call center.
Appendices A. Diagnostic Tool Sample
B. Sources of Benchmarking Data
C. Glossary of Call Center Terms

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 1 – Executive Summary
Page 3 ©2003 BearingPoint, Inc.
1.2 Operational Elements
Seven major call center operational elements were identified to assess each call center. These
elements make up the seven most commonly found operational elements of a call center. Each
center was assessed and measured against industry best practices in each of the following
operational element areas:
Management
Workforce Management
Training
Quality Monitoring
Customer Service Representatives
Reporting
Technology
1.3 Recommendations
Recommendations for each individual call center are found in Chapter Four. The Credit Card
Payments (FHK) Call Center opportunities for improvement are found in Chapter Seven of this
report.
Chapter Six provides recommendations for increasing the Customer Relationship Management
(via call center) function for the KidCare program as a whole. The recommendations made are
mutually exclusive and can be implemented stand-alone or in conjunction with one another.
The recommendations are as follows:
Recommendation 6.1: Create one set of call center performance metrics that all KidCare
call centers will use as a standard to meet.
Recommendation 6.2: Conduct monthly call calibration sessions at the All Call Center
meetings.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 1 – Executive Summary
Page 4 ©2003 BearingPoint, Inc.
Recommendation 6.3: Standardize call center names and transfer protocol when CSRs
are speaking to callers.
Recommendation 6.4: Implement a single phone number for KidCare Customer Service
and link all call centers off of the IVR menu.
Recommendation 6.5: Identify one single entity to administer all of the KidCare call
centers.
Recommendation 6.6: Perform a phased consolidation of KidCare call centers so that one
contracted entity operates all of the call centers.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 2 – Background
Page 5 ©2003 BearingPoint, Inc.
2.0 Background
Chapter Two is intended to provide readers with an understanding of the purpose of this assessment, the
methodology and approach used, and the overall KidCare program. The related subsections are as
follows:
2.1: Assessment Background – describes the purpose for performing this assessment
2.2: Assessment Approach – provides the approach to collecting, compiling and analyzing
information
2.3: KidCare Background – provides information on the KidCare program, as well as the KidCare
call centers
2.1 Assessment Background
BearingPoint was engaged by the Florida Healthy Kids Corporation to assess five separate call
centers providing KidCare customer service. Because these call centers operate separately,
there are inconsistencies in call center structure, processes, technology and CSR performance
measures. Disparate call centers and operating systems cause caller frustration because of the
multitude of phone numbers required to perform different services related to the KidCare
program. In addition, the time involved in obtaining assistance via the phone can be lengthy.
BearingPoint was contracted to assess call center operations and provide recommendations to
improve customer service across the KidCare program.
During the course of this engagement, a sixth call center, Credit Card Payments (FHK), was
added to the scope of the project. Administered and run internally by the Florida Healthy Kids
Corporation, this call center processes credit card payments for program members paying
premiums. In addition, it also processes credits for families if insurance coverage was
purchased for future months and the child becomes disenrolled in a KidCare program, thus, not
able to use the purchased coverage. This call center began as a pilot in February 2002 and has
grown at a rapid rate since program inception. Since this call center was quickly implemented,
many standard call center operational processes and technologies were not developed and are
currently not performed or used. Thus, due to the fact that this call center is operationally
distinct from the original five call centers, the Credit Card Payments (FHK) Call Center
assessment and recommendations are addressed separately in Chapter Seven.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 2 – Background
Page 6 ©2003 BearingPoint, Inc.
2.2 Assessment Approach
In order to meet the objectives of this assessment, the following activities were conducted for
information gathering and research purposes:
Call Center Site Visits – The following five call centers were visited during the course of this
assessment to gain an in-depth understanding of call center operations and functions:
KidCare Outreach (ACS): November 5-6, 2002
Enrollment Enhancement (ACS): November 5-6, 2002
Credit Card Payments (FHK): November 6, 2002
Member Services (DHACS): November 12-13, 2002
KidCare Medicaid (DCF): November 18-19, 2002
MediKids (ACS): March 10, 2003 1
Diagnostic Distribution – All call centers assessed were given a diagnostic survey that asked
for basic call center performance data and in-depth data related to the analysis of this
assessment. Appendix A of this report provides a sample of the diagnostic each call center
was asked to complete. KidCare Outreach (ACS), Enrollment Enhancement (ACS), and
MediKids (ACS) declined to answer certain questions in the diagnostic. In certain instances,
the lack of information prevented this assessment from being able to benchmark all call
centers. When this occurred, the reason for the exclusion of a call center is annotated in the
“Notes” section of every benchmarking exhibit in Chapter Five. The following is a list of the
questions that the call centers declined to answer in the diagnostic. Please see Appendix A
to reference the specific question:
KidCare Outreach (ACS): declined to answer questions D2-D3, D6-D9, D15-D16, D42,
I1-I9 (The answer to question D1 was provided; however, BearingPoint was asked not to
publish the answer in this assessment.)
1 The Contractor (ACS) allowed a limited two-hour site visit with no CSR shadowing. All other call center site
visits averaged eight hours and included CSR shadowing.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 2 – Background
Page 7 ©2003 BearingPoint, Inc.
Enrollment Enhancement (ACS): declined to answer questions D2-D3, D6-D9, D15-D16,
D42, F26-F47, I1-I9 (The answer to question D1 was provided; however, BearingPoint
was asked not to publish the answer in assessment.)
MediKids (ACS): declined to answer questions B5, B7-B9, D2, D3, D5, D6-D9, D14-D16,
D19-D42, E1-E9, F1-F66, E1-E5, I1-I9 (The answers to questions B4 and B6 were
provided by the AHCA Contract Administrator for this call center)
Call Center Materials – Various call center materials, such as quality monitoring scorecards
and additional call center statistics, were also given to BearingPoint for purposes of
assessment and discovery. A list of initial materials requested is cited in section I of the
diagnostic survey in Appendix A. KidCare Outreach (ACS), Enrollment Enhancement (ACS)
and MediKids (ACS) declined to provide call center materials.
2.3 KidCare Background
The Florida KidCare Program was established in 1998 to provide health insurance for qualifying
uninsured children who reside in the state of Florida. Although the term ‘KidCare’ is used as the
official name of the program, four separate programs act as a partnership to provide services to
Florida families.
Exhibit 2.1 below illustrates KidCare’s four separate programs:
MediKids - health insurance program for children ages 1-4, administered by the Agency for
Health Care Administration (AHCA)
Florida Healthy Kids - health insurance program for children ages 5-18, administered by
Florida Healthy Kids Corporation (FHK)
KidCare Medicaid - free health insurance program for children ages 0-18, administered by
the Department of Children and Families (DCF)
Children’s Medical Services Network (CMSN) - a program for children ages 0-18 who have
special behavioral or physical health needs or on-going medical conditions, administered by
the Department of Health (DOH)

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 2 – Background
Page 8 ©2003 BearingPoint, Inc.
Exhibit 2.1 – KidCare Programs
Florida KidCareProgram
FloridaHealthy Kids
Children'sMedicalServicesNetwork
KidCareMedicaidMediKids
Although KidCare is comprised of the four programs above, there are six call centers assessed
in this study that provide KidCare program information and customer service to current and
prospective members. Some call centers, such as MediKids (ACS), provide services for
program members in only one of the KidCare programs. In other cases, a call center such as
Member Services (DHACS) provides services to all four KidCare program members.
The six call centers are administered by four separate entities, with some entities managing one
call center, while others manage up to three separate call centers. Two call centers operate
within their administering agency or non-profit organization and the remaining four contract their
call center functions to an external entity (ACS) or a Third Party Administrator (DHACS). The
summary descriptions below describe who administers each call center, which program(s) the
call center assists, as well as a brief description of their services.
Member Services (DHACS) - Administered by the Florida Healthy Kids Corporation, this call
center is operated by the Third Party Administrator, Dental Health Administrative and
Consulting Services (DHACS), and serves as the primary source of information for
MediKids, Florida Healthy Kids and CMSN programs. It provides assistance on information
pertaining to application status, eligibility determination, the enrollment process, cancellation
letters, late payments, premium payments, collections and posting.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 2 – Background
Page 9 ©2003 BearingPoint, Inc.
KidCare Outreach (ACS) - This call center is administered by DOH, who contracts services
to Affiliated Computer Services, Inc. (ACS). The main functions of this call center are to
provide general KidCare program information, distribute KidCare applications and file
complaints and grievances. The KidCare Outreach (ACS) call center phone number is
printed on all KidCare outreach materials.
MediKids (ACS) - Administered by AHCA, this call center, like KidCare Outreach, is also
contracted to ACS. The main function of this facility is to assist MediKids callers in HMO
choices, if requested, and enter decision information into the system.
KidCare Medicaid (DCF) - This call center is administered and maintained internally by the
Department of Children and Families. CSRs help solve problems between KidCare
programs and families and provide general KidCare Medicaid information to callers, in
addition to application status and explanations for approval or denial of KidCare Medicaid
benefits.
Enrollment Enhancement (ACS) - This call center is administered by FHK and is also
contracted to ACS. There are two main functions of this call center:
New Enrollee Calls: Customer Service Representatives (CSRs) call all Florida Healthy
Kids newly enrolled families to welcome them to the program, answer questions,
encourage timely premium payment, and update family information when needed. A
total of five attempts are made to contact newly enrolled families.
Birthday Calls: CSRs make one attempt to call Florida Healthy Kids families whose child
has a birthday in that month. CSRs wish the child a happy birthday and inform parents
of seasonal preventative health measures, such as cold and flu season awareness and
immunization shots.
Credit Card Payments (FHK) - Administered and run internally by the Florida Healthy Kids
Corporation, this call center processes credit card payments for program members paying
premiums. In addition, it also processes credits for families if insurance coverage was
purchased for future months and the child becomes disenrolled in a KidCare program, thus,
not able to use the purchased coverage. Information pertaining to the assessment of and
recommendations for this call center are found in Chapter Seven of this report.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 2 – Background
Page 10 ©2003 BearingPoint, Inc.
Exhibit 2.2 below displays basic information pertaining to each call center assessed.
Exhibit 2.2 – KidCare Call Centers Summary
KidCare Call Centers
General Information
Member Services (DHACS)
KidCare Medicaid (DCF)
KidCare Outreach (ACS)
Enrollment Enhancement
(ACS) MediKids (ACS)
Administrator Florida Healthy Kids Corporation
Department of Children and Families
Department of Health
Florida Healthy Kids Corporation
Agency for Health Care Administration
Contractor/ TPA DHACS N/A ACS ACS ACS
Phone Number 1-800-821-5437 1-888-993-9083 1-888-540-5437 N/A 1-877-506-0578
Hours of Operation
8am-6pm EST 8am-5pm EST 8am-8pm EST 11am-8pm EST 8am-6pm EST
Inbound/Outbound Inbound Inbound Inbound Outbound Inbound
Average Number of CSRs
31 5 Declined from having this data printed in assessment
Declined from having this data printed in assessment
13
Annual Calls Handled
603,284 88,694 287,341 426,331 90,900
Average Call Talk Time
03:49 03:18 02:14 01:11 04:01
Average After Call Work Time
00:30 N/A 00:00 00:00 00:43
Abandonment Rate
3.00% 15.33% 3.60% N/A 2.43%
Notes: * The name of the contractor, if applicable, of each call center is written in parentheses after each call center name. For example, ACS is the contractor in the case of the MediKids call center. * Total Calls Handled and Number of CSRs are from the period of 12/01/01-11/30/02. * Number of CSRs is an average of the number of full-time equivalent employees for the duration of one year (12/02/02-11/30/02). * KidCare Medicaid (DCF) does not track average After-Call Work Time. * The Member Services call center run by Affina had an average of 46 CSRs and 3 Supervisors over the period of 12/01/01-11/30/02. * All other data in Exhibit 2.2 is derived from the diagnostic survey answers.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 3 – Call Center Operational Elements
Page 11 ©2003 BearingPoint, Inc.
3.0 Call Center Operational Elements
Exhibit 3.1 is a visual representation of the major call center operational elements and their interaction
with the customer in the call center environment. This illustration is not meant to be representative of
any of the KidCare program call centers; instead, it serves as a generic representation of the operational
elements of most full-scale call centers.
Exhibit 3.1 - Call Center Operational Elements
As Exhibit 3.1 illustrates, there are varying call center operations that precede the actual servicing of a
customer. Good customer service is dependent upon each of the seven elements being properly
planned and carried out. The arrows that move from one operational area to another in Exhibit 3.1
illustrate how there is always a degree of integration and influence between the operational areas of a
call center. While BearingPoint recognizes that there is interdependence of the operational elements,
Customer (Not an operational element)
Customer Service Representative
Workforce Management Training Quality
Monitoring
Technology
7 Major Operational Elements of a Call Center
Rep
ortin
g
Management
Customer (Not an operational element)
Customer Service Representative
Workforce Management Training Quality
Monitoring
Technology
7 Major Operational Elements of a Call Center
Rep
ortin
g
ManagementManagement

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 3 – Call Center Operational Elements
Page 12 ©2003 BearingPoint, Inc.
this report has assessed the call centers in each area separately in order to effectively illustrate
improvement areas that are detailed enough to be actionable.
This chapter describes each operational element and its interaction with other elements in a call center.
3.1 Management
Description. Management of a call center is a broad term that captures the high and low level
personnel that influence call center operations. High-level personnel may include decision
makers, such as a State Agency Contract Administrator or the President of a private call center
outsourcing company. Despite the fact that their day-to-day contact with the call center may be
rare, these individuals are included in this category because their management philosophy and
decisions will ultimately affect the operations of the call center.
In a more closely related position to the daily activities of a call center are Call Center Managers
and Supervisors. Their direct leadership and guidance with the CSR influences the performance
of the call center as a whole. The Call Center Manager and Supervisor are often managing in an
environment guided by the mandates of a Contract Administrator or President of a company.
Call centers sometimes have Managers leading functional departments such as training and
quality monitoring. These Managers may be peers or subordinates of the Call Center Manager.
They have direct influence over department processes affecting the success of the call center.
Interaction. As indicated in Exhibit 3.1, management drives and influences other operational
elements such as workforce management, training and quality monitoring. Management
controls budgetary and strategic decisions that flow down to influence other functions, such as,
but not limited to, staffing and scheduling for workflow estimations, training requirements, and
quality monitoring standards.
In addition, management also directly influences the work of CSRs, as they have CSR oversight
and may interact with them on a daily basis. Management is the element that sets the pace and
tone for all other operational elements. The quantitative results of the call center’s performance
are communicated back to management through reporting applications, which in turn, allows

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 3 – Call Center Operational Elements
Page 13 ©2003 BearingPoint, Inc.
management to adjust or reinforce their decisions and pass them down through the continuous
flow of operations.
3.2 Workforce Management
Description. Workforce management (WFM) is a two-step process. The first step is forecasting
anticipated call volume at a call center taking inbound calls and forecasting the number of calls
to be made for outbound call centers. The second step is the creation of a CSR staffing
schedule to handle forecasted call volume while maintaining performance metrics. There is
usually a small group or a single individual that handles the full time job of WFM analysis. The
most challenging aspect of WFM is forecasting call volume. Accurate forecasting requires a
balance of mathematical analytics, historical call volume data, as well as experienced
premonition. One of the most commonly used formulas to forecast call volume is the Erlang C
equation. This equation improves the accuracy of call volume forecasts by accounting for
random call arrival patterns when predicting call wait times. Furthermore, it predicts call wait
times based on the following elements:
The number of agents
The number of callers waiting to be serviced
The average amount of time it takes to serve each caller
Erlang C can also predict the resources required to keep call wait times within target limits.
Erlang C is widely available in the form of free or low cost PC based “calculators”, and is
currently built into virtually all of the full-blown workforce management software packages.
Interaction. As Exhibit 3.1 demonstrates, WFM is heavily influenced by management decisions.
Call center performance metrics set by management serve as the ruler that WFM staff must
consider when creating staffing schedules. At the same time, budgets set by management can
potentially restrict the amount of staff that can be deployed to reach performance goals. In turn,
CSRs are directly affected by the schedules created by WFM Managers, while customers are
indirectly affected by their decisions.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 3 – Call Center Operational Elements
Page 14 ©2003 BearingPoint, Inc.
3.3 Training
Description. The traditional philosophy behind call center training departments is a focus on
CSR performance, as it has a direct influence on customer service. CSRs are trained in
program specific knowledge, technology, and other CSR specific skills. However, the call center
training industry is expanding to include courses geared toward call center management and
specific analytics, such as call forecasting, in addition to the traditional focus on CSRs.
Interaction. Budgetary and strategy mandates set by management determine the scope of
training carried out by a call center Training department. Training also works closely with the
Quality Monitoring department to retrain CSRs that have deficiency areas identified by the
quality monitoring process.
3.4 Quality Monitoring
Description. Quality monitoring is the process of randomly selecting live phone calls handled
by CSRs and listening to them to assess CSR performance. Quality monitoring is designed to
increase customer service levels of a call center. Quality monitoring is especially important
when CSRs have access to private information or are dealing with sensitive issues, such as
healthcare. In situations such as these, compliance to the performance standards set by a call
center is extremely important. Through quality monitoring, a call center can effectively assess
the level of compliance for CSRs. More advanced quality monitoring technology enables the
monitor to view a recording of the CSR’s desktop screen actions. Thus, the CSR can also be
assessed in appropriate use of the desktop functionality. Examples of elements that are usually
graded in quality monitoring include, but are not limited to: accuracy of content given,
politeness/professionalism, pace of speech, and call talk time.
Interaction. The frequency of quality monitoring is often determined or approved by the
management of a call center. Management will also influence the strictness of quality monitoring
standards and grading. Quality Monitoring departments will also interact with Training
departments to communicate observed deficiency areas of CSRs. In addition, it is important for
Quality Monitoring staff to be regularly trained on CSR technical and knowledge skills so they
can appropriately assess CSRs. Depending on the responsibilities of Supervisors or the

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 3 – Call Center Operational Elements
Page 15 ©2003 BearingPoint, Inc.
Training department, quality monitoring staff may retrain CSRs directly, or at least discuss
monitored scores with them in person.
3.5 Customer Service Representative (CSR)
Description. CSRs are often the first and only line of communication for a call center. The
quality of CSRs skills is a reflection of the quality of that call center. There is a comprehensive
set of operations that operate behind the scenes at a call center in order to facilitate the CSRs’
ability to offer good customer service. When evaluating the CSR category of a call center, this
assessment considered the CSR working environment, call processes, job complexity and actual
performance observed.
Interaction. As Exhibit 3.1 illustrates, call center management, workforce management, training
and quality monitoring are all elements that directly influence the activities of a CSR. The
interaction of these elements with the CSRs facilitates the ability to offer good customer service
when on the phone with a caller. In turn, the ability of the CSRs to translate all of their training
and monitoring into good service is measured by various reporting devices within the call center.
3.6 Reporting
Description. Call center reports are most often generated by one of two possible pieces of
basic call center technology, either an automatic call distributor (ACD) or a predictive dialer.
ACDs and predictive dialers both enable call centers to control the flow of calls either arriving or
departing the call center. The difference between the two pieces of technology is whether they
control inbound or outbound calls. At an inbound call center, the ACD routes calls into a queue
for the calls to wait until a CSR can handle them. At an outbound call center, a predictive dialer
controls the dialing of phone numbers and routes successfully dialed calls to the CSRs for
handling. Thus, due to the fact that ACDs and predictive dialers are the primary technologies
that handle routing calls, they can easily track the volume and statistical characteristics of the
calls at the call center.
ACD and predictive dialer reports reflect basic call statistics, such as call volume, call handling
times, average speed of answer, abandonment rate, talk time and hold time. Depending on the
sophistication of the ACD and the reporting software used, a call center may be able to report

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 3 – Call Center Operational Elements
Page 16 ©2003 BearingPoint, Inc.
other in-depth call statistics. Beyond ACD and predictive dialer reporting, call centers may also
produce reports from other applications or manual records, such as:
CSR training test scores reports
WFM forecast reports
WFM forecast accuracy reports
WFM schedules
Training content changes reports
Quality monitoring reports
CSR schedule adherence reports
Customer satisfaction reports
All of these reports illustrate different aspects of daily performance, as well as call center trends.
Subsequently, management is able to utilize the reports to adjust or reinforce operational
techniques.
Interaction. Primary reporting is created from CSR interaction with callers. Thus, since ACDs
or predictive dialers are essential to the CSR and caller interaction, they are the main technology
to capture report data. Other reporting software may interface with the switch or ACD to create
more easily read reports that will be utilized by call center management to check performance
status and create forecasts for the call center. Applications specific to call center departments,
such as training software, WFM software, or quality monitoring software may directly produce
reports that are given to management on a regular basis.
3.7 Technology
Description. Technology underlies most call center functionality and serves as the backbone of
the call center. Some typical call center technologies are:
Interactive Voice Response (IVR) Unit - This recording usually serves as the first line of
communication to callers when they reach a call center and it responds to caller entered
digits or speech recognition in menu form.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 3 – Call Center Operational Elements
Page 17 ©2003 BearingPoint, Inc.
Automatic Call Distributor (ACD) - This specialized telephone system is used in incoming call
centers to answer, queue and distribute calls. It can also play an announcement after callers
have been in queue for a set amount of time. Most ACDs can produce reports about basic
statistics of a call center. Some call centers choose to print reports directly from the ACD or
will use reporting technology to integrate with the ACD to produce clearer reports.
Quality Monitoring (QM) Applications - QM applications are used to assist the call center in
quality monitoring. QM applications usually have the ability to automatically record and store
calls for later retrieval and may have the ability to view the CSR’s desktop navigation on a
call. In addition, some applications may also house QM scorecards online.
Workforce Management (WFM) Applications - WFM applications are used to assist the call
center in forecasting and CSR scheduling. WFM applications usually use built in analytics
with the Erlang C equation to derive accurate call volume forecasts and can also consider
historical call patterns.
E-Learning or Training Applications - E-Learning and training applications facilitate the
education of call center personnel through easily updated and individualized training
courses. Some E-learning applications are web-based and accessible at any desktop with
Internet access.
Interaction. Call center technology can enhance the centers’ performance levels, as well as
directly influence the customer experience. Thus, as represented in Exhibit 3.1, technology is an
operational layer that touches upon all other operational elements of the call center. It is directly
affected by management decisions, as well as used by management to carry out their job
responsibilities. Other departments within the call center and corporation rely on technology to
facilitate their actions. Ultimately, the performance of a call center’s technology will affect the
perceived level of customer service by customers.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 18 ©2003 BearingPoint, Inc.
4.0 Individual Call Center Analysis and Recommendations
In order to assess the KidCare program, an in depth understanding of each call center’s operations is
necessary. This chapter analyzes the individual call centers based on the seven major call center
operational elements discussed in Chapter Three. In addition, recommendations for opportunity areas
and identified strengths are provided for each call center.
This chapter is organized in the following manner:
4.1: Assessment Summary – displays comparison of individual call center performance in chart
format
4.2: Analysis and Recommendations – provides analysis of and recommendations for individual
call centers in the following subsections:
4.2.1: Member Services (DHACS)
4.2.2: KidCare Medicaid (DCF)
4.2.3: KidCare Outreach (ACS)
4.2.4: Enrollment Enhancement (ACS)
4.2.5: MediKids (ACS)
4.1 Assessment Summary
Exhibit 4.1 summarizes each call center’s overall ratings in the seven operational areas
described in Chapter Three. While BearingPoint recognizes that there is interdependence of the
operational elements, this report has assessed the call centers in each area separately to
effectively illustrate improvement areas that are detailed enough to be actionable. The results of
this exhibit are justified in detail for each call center in Sections 4.2.1 through 4.2.5.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 19 ©2003 BearingPoint, Inc.
Exhibit 4.1 – Call Center Assessment Summary
KidCare Call Centers
Operational Element
Member Services (DHACS)
KidCare Medicaid (DCF)
KidCare Outreach (ACS)
Enrollment Enhancement
(ACS) MediKids (ACS)
Management Medium High High High Medium
Workforce Management Low Low High Medium Low
Training High Low Medium High Medium
Quality Monitoring Low Low Medium Medium Medium
CSR High Low Medium Medium *Could not determine
Reporting High Low High High Medium
Technology Medium Low High Medium Medium
Notes: * The Contractor (ACS) of the MediKids (ACS) call center allowed a limited two-hour site visit with no CSR shadowing. Due to the lack of CSR shadowing, no formal rating could be made in the operational element area of CSR for purposes of this assessment. All other call centers permitted CSR shadowing, which allowed for an appropriate assessment of the CSR category.
4.2 Analysis and Recommendations
This chapter contains the analysis for each call center assessed and is divided into following
sections:
Special Considerations - lists call center specific information that was considered during the
assessment
Call Center Overview - lists major call center characteristics, providing a basic understanding
of the call center’s operating environment
Recommendation Areas - contains identified opportunity areas for each call center

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 20 ©2003 BearingPoint, Inc.
Operational Strength Areas - contains identified strengths of each call center
Operational Performance Assessment - provides ratings by operational category based on
key findings discovered in call center site visits, review of diagnostic tools and various call
center materials
4.2.1 Member Services (DHACS)
This section provides detailed information pertaining to the Member Services (DHACS)
call center.
4.2.1.1 Special Considerations The Member Services (DHACS) call center is currently located in Lisle,
Illinois. There is discussion that Member Services (DHACS) will open a
second Member Services call center in Tallahassee, Florida in 2003.
DHACS currently subcontracts to Affina to handle part of the call volume
for the Member Services line. The Affina site is located in El Paso,
Texas. There is a controlled split of calls where Affina handles 70% of
call volume and DHACS handles 30%.
Florida Healthy Kids agreed to DHACS’ decision not to include Affina
data or a site visit for this assessment. Thus, this engagement only
assessed and gathered detailed information regarding the DHACS
portion of the Member Services line.
4.2.1.2 Call Center Overview - Member Services (DHACS)
Purpose Serves as primary source of information for KidCare programs (MediKids, Florida Healthy Kids, CMSN); provides information on application status, eligibility determination, enrollment process, premium payments, collections and postings, cancellation letters, late payments and rate increases
Category Inbound call center, Contracted to Third Party Administrator, DHACS
Administrator Florida Healthy Kids Corporation
Service Hours 8am-6pm EST, 1-800-821-5437

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 21 ©2003 BearingPoint, Inc.
Average Number of CSRs 31
Supervisors 1
Annual Calls Handled 603,284
Average Call Talk Time 3 minutes, 49 seconds
Average After Call Work Time 30 seconds
Abandonment Rate 3.00%
Average Speed of Answer 35 seconds steady rate, 40 seconds peak state
Notes: *Average number of CSRs and calls handled is from the period of 12/01/01-11/30/02. *All other data is from the diagnostic survey. *The Affina location for the Member Services line handled 485,491 calls during the period of 12/01/01-11/30/02. *The Affina location for the Member Services call center had an average of 3 Supervisors and 46 CSRs for the period of 12/01/01-11/30/02.
4.2.1.3 Recommendation Areas - Member Services (DHACS)
Recommendations Area: Management Responsibilities
Observation: Best Practice/Recommendation: Risk:
Call Center Manager: The Call Center Manager’s primary responsibility is workforce management. A great of time the Manager’s time is spent dealing with tasks related to this responsibility.
It is important that the Call Center Manager spends the majority of time overseeing all operational aspects of the call center, such as supervising, training, quality monitoring and workforce management. Workforce management is a full time responsibility that is usually given to a dedicated WFM employee that is subordinate to the Call Center Manager.
When a Call Center Manager’s primary responsibility is workforce management, while overseeing a large call center, there may not be enough time to oversee other operational aspects of the call center. The result is that other operational elements may not work in a cohesive, strategic manner and may operate in functional silos.
Call Center Manager: The Call Center Manager does not have instant access to call center activities at the Affina site and must rely upon emails or telephone calls to receive information about their current performance of call queues. It was also suggested that the Call Center Manager would oversee the Tallahassee, FL call center location, as well the Lisle, IL site, when they are both operational.
Call Center Managers should be responsible for and aware of the daily operations of the call center on a real-time basis. This requires constant monitoring of the center’s call queue status via a real time ACD, various reports and being physically located in the call center.
If the Call Center Manager continues to not have real time status of the Affina call center queue or floor events, it does not allow that person to react to unanticipated call spikes and operational emergencies in a prompt and effective manner.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 22 ©2003 BearingPoint, Inc.
Recommendations Area: Management Responsibilities (cont.)
Observation: Best Practice/Recommendation: Risk:
CSR Team Leads: Four CSR Team Leads are handling caller complaints and only send callers to the Supervisor when they cannot resolve the issue.
CSR Team Leads should not handle the Supervisor responsibility of handling caller complaints. For legal reasons, a Supervisor should be the only person handling caller complaints in order to have consistent caller treatment and carry out possible CSR disciplinary action.
Having different CSR Team Leads handle caller complaints risks having an inconsistent process of caller complaint resolution. In addition, if the call complaint warrants CSR disciplinary action, this should be handled directly by a Supervisor, not a CSR Team Lead.
Recommendations Area: Workforce Management (WFM)
Observation: Best Practice/Recommendation: Risk:
DHACS has indicated that they will be implementing a workforce management application in the future. However, at the moment all call volume forecasting is based on manual calculations and does not utilize the Erlang C equation.
Effective workforce management does not have to be carried out by computer applications. However, even if it is determined by manual calculations, an Erlang C chart should be utilized to factor in the variance of “randomly arriving call patterns” in order to make accurate call forecasts.
WFM forecasts that do not employ the Erlang C equation or computer simulation are not able to factor in the random call arrival pattern. Thus, the forecasts are not as accurate as they could be and efficient staffing may be jeopardized.
Recommendations Area: Quality Monitoring
Observation: Best Practice/Recommendation: Risk:
Quality monitoring is carried out by three separate entities: Supervisors, Trainers, and the Delta Dental (parent company) Internal QM team. These entities do not have calibration sessions to encourage consistency of monitoring, develop QM expectations or standardize the scorecard grading system.
If quality monitoring is carried out by separate entities within a call center, it is necessary to have calibration sessions at least once a month. Calibration sessions consist of having all persons who monitor calls listen to and individually score the same call. Then, all respective scores are shared and rationale for scoring is discussed. This process facilitates having a consistent quality standard for CSRs.
Without calibration sessions, there may be inconsistency in QM scoring. CSRs may begin to recognize that different monitors score with varying strictness. This erodes the overall value of the monitoring process and may cause CSR dissatisfaction when they feel that one call can result in different scores depending on the person monitoring.
Only the Delta Dental internal QM team records monitored calls. These records are discarded after approximately one week of existence.
All monitored calls should be recorded so that, if needed, CSRs can listen to their calls and identify their deficiency areas. In addition, if a CSR disagrees with a score it is necessary to have a recorded call to revalidate or dispute a score.
Not recording calls makes it more difficult for CSRs to identify their problem areas. In addition, CSRs may feel that there is no un-biased evidence that can allow them to dispute a score. Without a call record, it becomes the CSR’s opinion versus the monitor’s opinion.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 23 ©2003 BearingPoint, Inc.
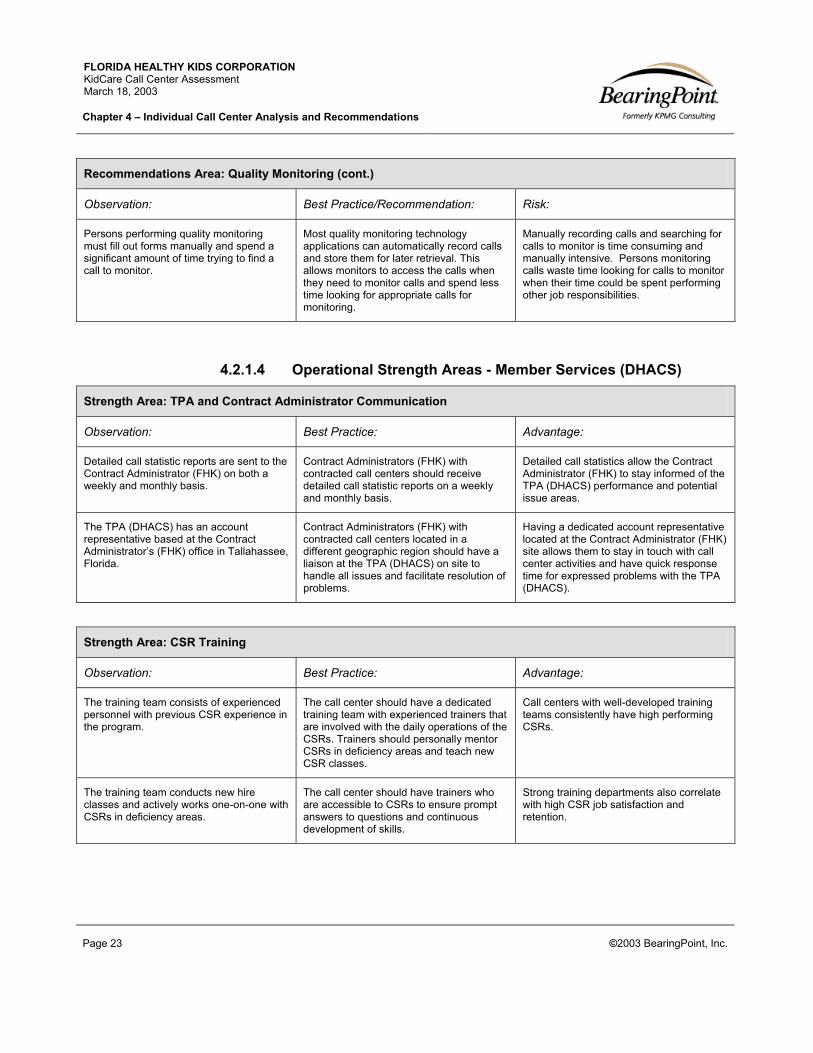
Recommendations Area: Quality Monitoring (cont.)
Observation: Best Practice/Recommendation: Risk:
Persons performing quality monitoring must fill out forms manually and spend a significant amount of time trying to find a call to monitor.
Most quality monitoring technology applications can automatically record calls and store them for later retrieval. This allows monitors to access the calls when they need to monitor calls and spend less time looking for appropriate calls for monitoring.
Manually recording calls and searching for calls to monitor is time consuming and manually intensive. Persons monitoring calls waste time looking for calls to monitor when their time could be spent performing other job responsibilities.
4.2.1.4 Operational Strength Areas - Member Services (DHACS)
Strength Area: TPA and Contract Administrator Communication
Observation: Best Practice: Advantage:
Detailed call statistic reports are sent to the Contract Administrator (FHK) on both a weekly and monthly basis.
Contract Administrators (FHK) with contracted call centers should receive detailed call statistic reports on a weekly and monthly basis.
Detailed call statistics allow the Contract Administrator (FHK) to stay informed of the TPA (DHACS) performance and potential issue areas.
The TPA (DHACS) has an account representative based at the Contract Administrator’s (FHK) office in Tallahassee, Florida.
Contract Administrators (FHK) with contracted call centers located in a different geographic region should have a liaison at the TPA (DHACS) on site to handle all issues and facilitate resolution of problems.
Having a dedicated account representative located at the Contract Administrator (FHK) site allows them to stay in touch with call center activities and have quick response time for expressed problems with the TPA (DHACS).
Strength Area: CSR Training
Observation: Best Practice: Advantage:
The training team consists of experienced personnel with previous CSR experience in the program.
The call center should have a dedicated training team with experienced trainers that are involved with the daily operations of the CSRs. Trainers should personally mentor CSRs in deficiency areas and teach new CSR classes.
Call centers with well-developed training teams consistently have high performing CSRs.
The training team conducts new hire classes and actively works one-on-one with CSRs in deficiency areas.
The call center should have trainers who are accessible to CSRs to ensure prompt answers to questions and continuous development of skills.
Strong training departments also correlate with high CSR job satisfaction and retention.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 24 ©2003 BearingPoint, Inc.
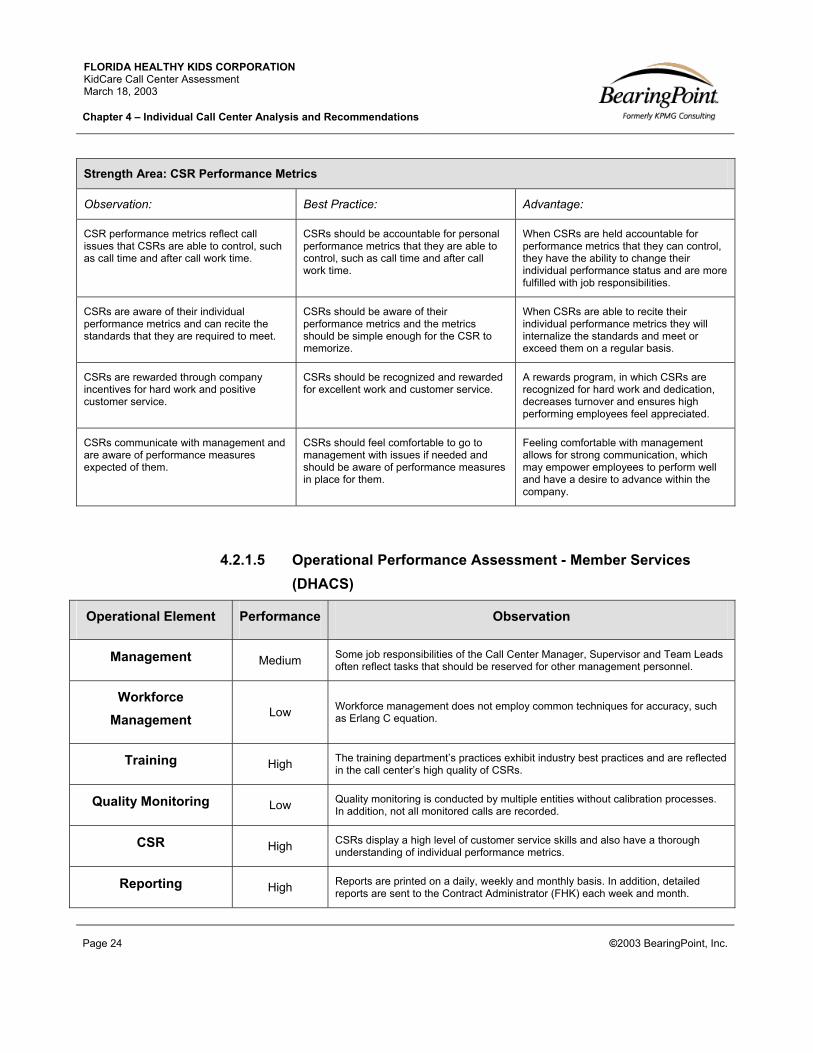
Strength Area: CSR Performance Metrics
Observation: Best Practice: Advantage:
CSR performance metrics reflect call issues that CSRs are able to control, such as call time and after call work time.
CSRs should be accountable for personal performance metrics that they are able to control, such as call time and after call work time.
When CSRs are held accountable for performance metrics that they can control, they have the ability to change their individual performance status and are more fulfilled with job responsibilities.
CSRs are aware of their individual performance metrics and can recite the standards that they are required to meet.
CSRs should be aware of their performance metrics and the metrics should be simple enough for the CSR to memorize.
When CSRs are able to recite their individual performance metrics they will internalize the standards and meet or exceed them on a regular basis.
CSRs are rewarded through company incentives for hard work and positive customer service.
CSRs should be recognized and rewarded for excellent work and customer service.
A rewards program, in which CSRs are recognized for hard work and dedication, decreases turnover and ensures high performing employees feel appreciated.
CSRs communicate with management and are aware of performance measures expected of them.
CSRs should feel comfortable to go to management with issues if needed and should be aware of performance measures in place for them.
Feeling comfortable with management allows for strong communication, which may empower employees to perform well and have a desire to advance within the company.
4.2.1.5 Operational Performance Assessment - Member Services (DHACS)
Operational Element Performance Observation
Management Medium Some job responsibilities of the Call Center Manager, Supervisor and Team Leads often reflect tasks that should be reserved for other management personnel.
Workforce Management Low Workforce management does not employ common techniques for accuracy, such
as Erlang C equation.
Training High The training department’s practices exhibit industry best practices and are reflected in the call center’s high quality of CSRs.
Quality Monitoring Low Quality monitoring is conducted by multiple entities without calibration processes. In addition, not all monitored calls are recorded.
CSR High CSRs display a high level of customer service skills and also have a thorough understanding of individual performance metrics.
Reporting High Reports are printed on a daily, weekly and monthly basis. In addition, detailed reports are sent to the Contract Administrator (FHK) each week and month.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 25 ©2003 BearingPoint, Inc.
Technology Medium The call center has CSR desktops, an ACD and an IVR, which are all industry standards. Member Services (DHACS) should consider implementing quality monitoring and workforce management applications.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 26 ©2003 BearingPoint, Inc.
4.2.2 KidCare Medicaid (DCF)
This section provides detailed information pertaining to the KidCare Medicaid (DCF) call
center.
4.2.2.1 Special Considerations The KidCare Medicaid (DCF) call center is not contracted out and is
managed and run internally at the Department of Children and Families.
The KidCare Medicaid (DCF) call center is managed in conjunction with
another unit at DCF, called the Client Registration Unit. This unit is the
application-processing unit for KidCare Medicaid applications. All CSRs
in the KidCare Medicaid (DCF) call center are cross-trained to work in
the Client Registration Unit when they are not taking phone calls. In
turn, when the KidCare Medicaid CSRs are absent from their offices,
such as during lunch or sick leave, or when there is call overflow, the
Client Registration Unit Supervisor and other employees may handle
calls as back-up CSRs.
Because this call center is managed and run internally at DCF, the CSR
hiring process is different from a traditional call center. CSRs may be
out of the office for a prolonged amount of time, for maternity leave, for
example, and the department is not able to replace them with other
CSRs to handle calls.
4.2.2.2 Call Center Overview - KidCare Medicaid (DCF)
Purpose Once an individual is referred to DCF, the call center provides application status information, as well as general KidCare Medicaid information and explanations for approval or denial of KidCare Medicaid benefits.
Category Inbound call center, Not contracted out
Administrator The Department of Children and Families
Service Hours 8am-5pm, 1-888-993-9083

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 27 ©2003 BearingPoint, Inc.
Average Number of CSRs 5
Supervisors 1
Annual Calls Handled 88,694
Average Call Talk Time 3 minutes, 18 seconds
Average After Call Work Time N/A
Abandonment Rate 15.33%
Average Speed of Answer 1 minute, 51 seconds
Notes: *Average number of CSRs and calls handled is from the period of 12/01/01-11/30/02. * KidCare Medicaid (DCF) does not track average After Call Work Time. *All other data is from the diagnostic survey.
4.2.2.3 Recommendation Areas - KidCare Medicaid (DCF)
Recommendations Area: Workforce Management
Observation: Best Practice/Recommendation: Risk:
KidCare Medicaid (DCF) is not able to employ flexible staffing based on forecasted call volume because hiring a new CSR is difficult and can take several weeks for approval. In addition, CSRs work standard hours each day regardless of call volume and patterns.
Call Centers should have flexible staffing to ensure it is capable of handling high call volume peaks and low call volume dips.
Customer service levels are at risk when flexible staffing is not in place because there is no difference to the ways in which the call center deals with high call volume versus low or steady call volume. This could cause the call center to have long average speed of answer times, thus, resulting in lower levels of customer service.
Recommendations Area: Training
Observation: Best Practice/Recommendation: Risk:
The call center does not have a dedicated trainer. Supervisor and Senior CSRs assist in training of new hires.
Each call center should have a dedicated Training Coordinator to ensure new CSR training, management training and ongoing training, as needed.
Having no dedicated trainer means the Call Center Supervisor and Senior CSRs have to informally train CSRs, which takes time away from their normal job responsibilities. For a call center of this size, there could be sharing of a trainer that works for other departments within the Department of Children and Families, as well.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 28 ©2003 BearingPoint, Inc.
Recommendations Area: Training (cont.)
Observation: Best Practice/Recommendation: Risk:
The call center has an informal training process where new CSRs sit with the Supervisor to read over the call center manual and then shadow experienced CSRs until they feel comfortable to begin answering calls independently.
Each call center should have a formal training program in which all new CSRs attend to learn call center etiquette, as well as specific KidCare program knowledge.
Because new CSRs do not get formally trained upon arrival to the KidCare Medicaid (DCF) call center, they are not taught consistent call center etiquette or even detailed program knowledge. Because of this lack of training, CSRs may not be performing to call center or program standards that would otherwise be discussed in a formal training session.
Recommendations Area: Quality Monitoring
Observation: Best Practice/Recommendation: Risk:
Quality monitoring is conducted by having the Supervisor sit next to the CSR with the caller on speakerphone.
The majority of quality monitoring should be conducted in a blind format where CSRs are not aware that they are being monitored. This results in a more accurate observation of average CSR performance.
CSR knowledge of being monitored allows them to adjust the quality of performance on the call. In addition, callers having to speak to CSRs on speakerphone can result in an uncomfortable or irritating experience for the caller.
The quality monitoring form does not list standard monitoring elements for customer service. Instead, the form provides an area to check subject of the call and a notes section for all other comments.
Quality monitoring forms should list specific customer service elements for scoring such as pace of speech, politeness, and accuracy of information.
If the quality monitoring form does not list specific customer service qualities in which CSRs are graded, the monitor may not be looking for customer service skills, which may decrease customer service levels.
Recommendations Area: CSR Performance
Observation: Best Practice/Recommendation: Risk:
CSRs in this call center have a variety of performance metrics to meet on a daily basis. However, their main performance metric is to handle 60 calls a day.
CSR performance metrics should be based on call elements that CSRs can directly control; such as call time length and average hold times.
The volume of calls to the KidCare Medicaid (DCF) call center allows the CSRs to regularly handle over 60 calls a day. Thus, their main performance metric of 60 calls is easily attained and does not rely on high customer service skills. Not setting or focusing on performance metrics, such as call time length or average hold times, does not encourage the CSRs to maintain a high level of customer service.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 29 ©2003 BearingPoint, Inc.
Recommendations Area: CSR Performance (cont.)
Observation: Best Practice/Recommendation: Risk:
CSRs are located in separated offices and the Supervisor is located in an office at the end of the hall.
CSRs should be located in an open cube area with the Supervisor, who is also in an open cube, able to see CSRs actions at all times.
The nature of call centers requires CSRs to be in a highly organized and monitored environment. CSRs should not be in separate offices where their time management cannot be directly observed.
Recommendations Area: Reporting
Observation: Best Practice/Recommendation: Risk:
The call center currently has only one terminal with report metrics, which is housed in the office of the Supervisor.
Call Center Managers and Supervisors should be able to see the real-time status of the call queue at their desks to stay aware of issues and make decisions to guarantee a certain level of customer service throughout the day.
Because only one person can view reports at this call center, it is possible the call queue could be at high wait times for several minutes before that one person notices, causing callers to become frustrated.
Reports cannot be printed and management must manually transcribe them.
Note: At the time of this assessment, the department was waiting for their warranty budget to be approved, which would enhance their reporting capabilities.
Reports should be available for printing to ensure no lost time for management.
The process of manually transcribing reports is time consuming and it takes away time from management’s normal job responsibilities.
Recommendations Area: Technology
Observation: Best Practice/Recommendation: Risk:
The call center does not have a disaster recovery plan.
Call centers should have a documented disaster recovery plan that sets up a process for re-routing calls to a back-up center in cases of natural disasters.
Not having a disaster recovery plan risks loss of service for extended periods of time in cases of natural disaster.
The call center does not have an IVR. If all CSRs are handling calls, the caller receives a “call ringing” tone until a CSR is able to answer.
Note: At the time of this assessment, the department was pursuing both an IVR and call center voicemail.
If a call center receives enough call volume to where most callers may have to wait to reach a CSR, the center should have an IVR for announcing hold status to callers.
If callers are hearing a “call ringing” tone for extended periods of time when trying to reach CSRs, the frustration level of the caller is increased by the time a CSR answers. This experience can create a low customer service level impression before a caller even reaches the CSR.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 30 ©2003 BearingPoint, Inc.
4.2.2.4 Operational Strength Areas - KidCare Medicaid (DCF)
Strength Area: Management
Observation: Best Practice: Advantage:
The Call Center Manager has daily interaction with CSRs and directly assists with difficult calls.
Call Center Managers should have daily contact with CSRs. A Manager’s ability to work with CSRs to handle difficult calls keeps the Manager knowledgeable of realistic pressures of the CSR’s job.
When management maintains a close relationship with CSRs, they are able to quickly gauge CSR issues, monitor how policies affect CSRs and react to CSR emergencies.
The Call Center Manager conducts monthly training sessions and tests CSRs.
CSRs should be retrained on a monthly basis and tested on learned information.
CSRs working in health policy-related environments should be retrained regularly in order to retain knowledge. Regular retraining allows CSRs to keep up to date with recent issues or policy changes.
4.2.2.5 Operational Performance Assessment - KidCare Medicaid (DCF)
Operational Element Performance Observation
Management High The Call Center Manager maintains a close relationship with CSRs and closely oversees daily operations of the call center.
Workforce Management Low
The call center is not able to employ flexible staffing based on forecasted call volume because hiring a new CSR is difficult and can take several weeks to be approved. In addition, CSRs work standard hours each day regardless of call volume and patterns.
Training Low The call center does not have a dedicated trainer. Because of this, the Call Center Supervisor and Senior CSRs assist in training of new hires. In addition, training for new CSRs is informal and consists of mostly shadowing experienced CSRs until they are ready to answer calls independently.
Quality Monitoring Low The quality monitoring form used at KidCare Medicaid (DCF) does not grade common customer service elements. In addition, quality monitoring is not performed blind to the CSR.
CSR Low Although CSRs may have a variety of performance measures, they do not seem to focus on metrics based on industry standards.
Reporting Low The call center currently has only one terminal with report metrics, which is housed in the office of the Supervisor, but not the Call Center Manager. In addition, reports cannot be printed from this technology and management must manually transcribe them.
Technology Low The call center does not have an IVR or WFM application. In addition, KidCare Medicaid (DCF) does not have the technology for the Supervisor to anonymously listen to or record calls during quality monitoring.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 31 ©2003 BearingPoint, Inc.
4.2.3 KidCare Outreach (ACS)
This section provides detailed information pertaining to the KidCare Outreach (ACS) call
center.
4.2.3.1 Special Considerations Call center functions have been contracted out through the Department
of Health to ACS. Another KidCare call center, Enrollment Enhancement
(ACS), is also contracted to ACS through Florida Healthy Kids. Both of
these call centers are housed in the same building and have the same
management in many areas.
Call volume associated with this call center directly correlates with
KidCare outreach and various media campaigns. Since the KidCare
Outreach (ACS) call center phone number is printed on program
materials, call center volume increases with outreach distribution.
The Contractor (ACS) declined to answer certain diagnostic survey
questions and did not provide requested call center materials.
4.2.3.2 Call Center Overview – KidCare Outreach (ACS)
Purpose Provides general program information and distributes KidCare applications
Category Inbound call center, Contracted out by DOH
Administrator Department of Health
Service Hours 8am-8pm EST, 1-888-540-5437
Average Number of CSRs The Contractor (ACS) declined from having this data printed in the assessment
Supervisors 1
Annual Calls Handled 287,341
Average Call Talk Time 2 minutes, 14 seconds

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 32 ©2003 BearingPoint, Inc.
Average After Call Work Time 0 minutes, 0 seconds
Abandonment Rate 3.60%
Average Speed of Answer 26 seconds
Notes: *Average number of CSRs and calls handled is from the period of 12/01/01-11/30/02. *All other data is from the diagnostic survey.
4.2.3.3 Recommendation Areas – KidCare Outreach (ACS)
Recommendations Area: Contract Administration Interaction
Observation: Best Practice/Recommendation: Risk:
The Contract Administrator (DOH) does not regularly shadow the quality monitoring process or perform monitoring independently.
The Contract Administrator (DOH) should closely manage their contracted call centers and should perform quality monitoring on a monthly basis.
Because quality monitoring is not performed or observed by the Contract Administrator (DOH), there is no way to gauge the actual level of customer service provided by the Contractor (ACS).
Recommendations Area: Quality Monitoring
Observation: Best Practice/Recommendation: Risk:
The quality monitoring contractual performance standard is 97%, which is extremely high for all CSRs to reach in a realistic call center setting where CSRs will normally have varying levels of performance.
Quality monitoring scores should realistically show how CSRs are handling calls. The industry standard for the QM scorecard goal is 85%.
If calls that are quality monitored are given too high a score, or the scoring in itself is too lenient, customer service levels may appear to be higher than they are in reality.
Persons performing quality monitoring must fill out forms manually and spend a significant amount of time trying to find a call to monitor.
Quality monitoring technology applications can automatically record calls and store them for later retrieval. These systems also automatically create a recording of the call that is easily forwarded to other monitors.
Manually recording calls and searching for calls to monitor is time consuming and manually intensive. Persons monitoring calls waste time looking for calls to monitor, when their time could be spent performing other duties.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 33 ©2003 BearingPoint, Inc.
4.2.3.4 Operational Strength Areas – KidCare Outreach (ACS)
Strength Area: Call Center Management
Observation: Best Practice: Advantage:
The Call Center Manager communicates effectively with the Supervisor, Training Coordinator and Workforce Manager.
Call center management has open communication with a solid hierarchy.
Open communication among management ensures a productive and collaborative working environment for those associated with the call center. A positive work environment at the management level filters to CSRs to create a positive work environment at that level, as well.
The Call Center Manager, Supervisor, Training Coordinator and Workforce Manager all have appropriate daily tasks and responsibilities given their respective positions.
Appropriate levels of responsibility should be designated to each management position.
Having appropriate responsibilities and daily tasks delegated to management allows for effective and efficient work in their specific area and in CSR interaction. In addition, CSRs are aware of whom to go to with issues when needed.
Strength Area: Workforce Management
Observation: Best Practice: Advantage:
The Workforce Manager compares forecasted volume with actual call center volume on a daily basis.
The Workforce Manager should determine forecasting accuracy by comparing forecasted volume to actual call volume.
When the Workforce Manager forecasts and schedules accurately, the correct number of CSRs are available and average speed of answer and blocked calls are minimal, ensuring high levels of customer service.
The call center uses an advanced application, Blue Pumpkin, to schedule and forecast call volume.
Call centers should use the Erlang C equation or Computer Simulation to perform scheduling and forecasting.
Using an application like Blue Pumpkin ensures more accurate scheduling and forecasting without human error. Strong forecasting and scheduling tools ensure the call center is prepared to accommodate all calls made to the center.
The Workforce Manager receives ongoing training and attends conferences.
The Workforce Manager should receive ongoing training as needed to increase knowledge on operational and technical best practices.
When Workforce Managers receive ongoing training, they become up to date on industry standards and best practices to forecast calls accurately and staff the call center appropriately.
The Workforce Manager is in constant communication with management and acts as a Supervisor, if needed.
The Workforce Manager should have a good understanding of management skills and the organizations’ hierarchy.
When the Workforce Manager is in constant communication with management, and is kept aware of call center operations from that level, they can more appropriately schedule CSRs and forecast call volume.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 34 ©2003 BearingPoint, Inc.
Strength Area: CSR Environment
Observation: Best Practice: Advantage:
CSRs sit in an open cube work environment.
An open cube environment is necessary in call centers to assess CSR time management and facilitate quick accessibility to Supervisors.
Having all CSRs in an open environment ensures efficiency and productivity among workers, which adds value to the call center by increasing overall customer satisfaction.
CSRs are rewarded through company incentives for hard work and positive customer service.
CSRs should be recognized and rewarded for excellent work and customer service.
A rewards program, in which CSRs are recognized for hard work and dedication, decreases turnover and ensures high performing employees feel appreciated.
CSRs communicate with management and are aware of performance measures expected of them.
CSRs should feel comfortable to go to management with issues, if needed, and should be aware of performance measures in place for them.
Feeling comfortable with management allows for strong communication, which may empower employees to perform well and have a desire to advance within the company.
CSRs are aware of their own daily call statistics, as well as their peers.
CSRs should view their own daily statistics, as well as their peer’s statistics, in order to gauge their overall performance in comparison to their peers.
Making CSRs aware of their statistics and how they compare with others allows them to improve their own performance, which leads to higher levels of customer service.
Strength Area: Reporting
Observation: Best Practice: Advantage:
Reports are generated daily, weekly and monthly.
Basic ACD statistics should be reported, monitored and used constantly at an efficient call center.
When reports are generated frequently, management can analyze the data to site trends and can use the information to hire more staff, address certain performance measures that are not being met and be certain the call center is running efficiently.
The Call Center Manager, Workforce Manager, Supervisor and CSR Lead all have access to an effective reporting application, Centervu.
Using applications that assist in identifying and translating information to readable information allows the call center to be aware of performance and trends.
Centervu is used to identify and translate information to readable information for both the Contractor (ACS) and Contract Administrator (DOH). When this information is used properly, it allows both parties to be aware of daily call center performance.
Monthly reports are submitted to the Contract Administrator (DOH) with monthly call center statistics.
The Contract Administrator (DOH) should be kept abreast of call center issues and statistics on a regular basis.
Keeping the Contract Administrator (DOH) informed of statistics and arisen issues helps to bridge the gap between the Contractor (ACS) and the Contract Administrator (DOH).
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 35 ©2003 BearingPoint, Inc.
4.2.3.5 Operational Performance Assessment – KidCare Outreach (ACS)
Operational Element Performance Observation
Management High Call center management is strong and communicates well with each other. In addition, staff is aware of the hierarchy of the call center and positions are tasked with the appropriate responsibilities.
Workforce Management High
The Workforce Manager is trained on an as-needed basis and forecasting accuracy is assessed daily. In addition, the Workforce Manager is in constant communication with call center management.
Training Medium
New employees receive 2 ½ days of soft skills training, which includes company information and benefits paperwork, in addition to general call center information and positive customer service delivery tactics. After this, KidCare program specific training is then performed over a 2-day period. A Training Coordinator teaches soft skills while specific KidCare training is provided by a technical trainer (CSR). Despite the fact that the Contract Administrator (DOH) does not provide KidCare training directly to CSRs, the technical trainer (CSR) uses the DOH manual to educate new CSRs and is aware of the KidCare program as a current CSR.
Quality Monitoring Medium
KidCare Outreach (ACS) monitors and records calls regularly and averages them for CSR performance reviews. However, the process to monitor calls is slow and manually intensive and scoring standards are extremely high. In addition, the Contract Administrator (DOH) does not observe or perform any independent quality monitoring.
CSR Medium
CSRs are in an open, positive work environment, with an established rewards program. They seem to be aware of their performance standards and daily stats. The environment provided for the CSR operations was exemplary. However, direct shadowing of CSRs indicated that their actual call handling techniques were average in comparison to call center best practices.
Reporting High Reports are generated daily, weekly and monthly and Centervu is used to identify and translate data. Monthly reports are provided to the Contract Administrator (DOH).
Technology High The following technology is used at the KidCare Outreach (ACS) call center: ACD, IVR, Centervu, Blue Pumpkin. Although ACS does have online monitoring, the technology is not used for this particular call center contract.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 36 ©2003 BearingPoint, Inc.
4.2.4 Enrollment Enhancement (ACS)
This section provides detailed information pertaining to the Enrollment Enhancement
(ACS) call center.
4.2.4.1 Special Considerations Enrollment Enhancement (ACS) is an outbound call center, in which
CSRs make the following two types of calls to Florida Healthy Kids
program families each month:
New Enrollee: CSRs welcome newly enrolled families, answer
questions, encourage timely premium payment, and update family
information when needed.
Birthday: CSRs wish children a happy birthday and inform parents
of seasonal preventative health measures, such as cold and flu
season awareness and immunization shots.
Call center functions have been contracted through the Florida Healthy
Kids Corporation to ACS. Another KidCare call center, KidCare
Outreach (ACS) through the Department of Health, is also contracted to
ACS. Both of these call centers are housed in the same building and
have the same management in many areas.
The Contractor (ACS) declined to answer certain diagnostic survey
questions and did not provide requested call center materials.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 37 ©2003 BearingPoint, Inc.
4.2.4.2 Call Center Overview – Enrollment Enhancement (ACS)
Purpose
The objective of the call center is to make calls to the following two groups within the Florida Healthy Kids Program:
New Enrollee – CSRs call new enrollee families to welcome them to the program, answer questions, encourage timely premium payments and stress the importance of preventative health measures.
Birthday – CSRs call families to wish them a happy birthday when a child has a birthday in that corresponding month. CSRs also remind parents about preventative measures and answer questions.
Category Outbound call center, Contracted out by Florida Healthy Kids
Administrator Florida Healthy Kids Corporation
Service Hours 11am-8pm EST
Average Number of CSRs The Contractor (ACS) declined from having this data printed in the assessment
Supervisors 1
Annual Calls Handled 426,331
Average Call Talk Time 1 minute, 11 seconds
Average After Call Work Time 0 minutes, 0 seconds
Abandonment Rate N/A for an outbound call center
Average Speed of Answer N/A for an outbound call center
Notes: *Average number of CSRs and calls handled is from the period of 12/01/01-11/30/02. *All other data is from the diagnostic survey.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 38 ©2003 BearingPoint, Inc.
4.2.4.3 Recommendation Areas – Enrollment Enhancement (ACS)
Recommendations Area: Quality Monitoring
Observation: Best Practice/Recommendation: Risk:
The quality monitoring contractual performance standard is 97%, which is extremely high for all CSRs to reach in a realistic call center setting where CSRs will normally have varying levels of performance.
Quality monitoring scores should realistically show how CSRs are handling calls. The industry standard for the QM scorecard goal is 85%.
If calls that are quality monitored are given too high a score, or the scoring in itself is too lenient, customer service levels may appear to be higher than they are in reality.
Persons performing quality monitoring must fill out forms manually and search to find a call to monitor.
Forms should be completed online, which alleviates the manual process of form completion and finding an appropriate call to monitor.
Manually recording calls and searching for calls to monitor is time consuming and manually intensive. Persons monitoring calls waste time looking for calls to monitor, when their time could be spent performing other duties.
4.2.4.4 Operational Strength Areas – Enrollment Enhancement (ACS)
Strength Area: Call Center Management
Observation: Best Practice: Advantage:
The Call Center Manager communicates effectively with Supervisor and Training Team.
Call center management has open communication with a solid hierarchy.
Open communication among management ensures a productive and collaborative working environment for those associated with the call center. A positive work environment at the management level filters to CSRs to create a positive work environment at that level, as well.
The Call Center Manager, Supervisor, and Training Team all have appropriate daily tasks and responsibilities given their respective positions.
There are appropriate levels of responsibility designated to each management position.
Having appropriate responsibilities and daily tasks delegated to management allows for effective and efficient work in their specific area and in CSR interaction. In addition, CSRs are aware of whom to go to with issues when needed.
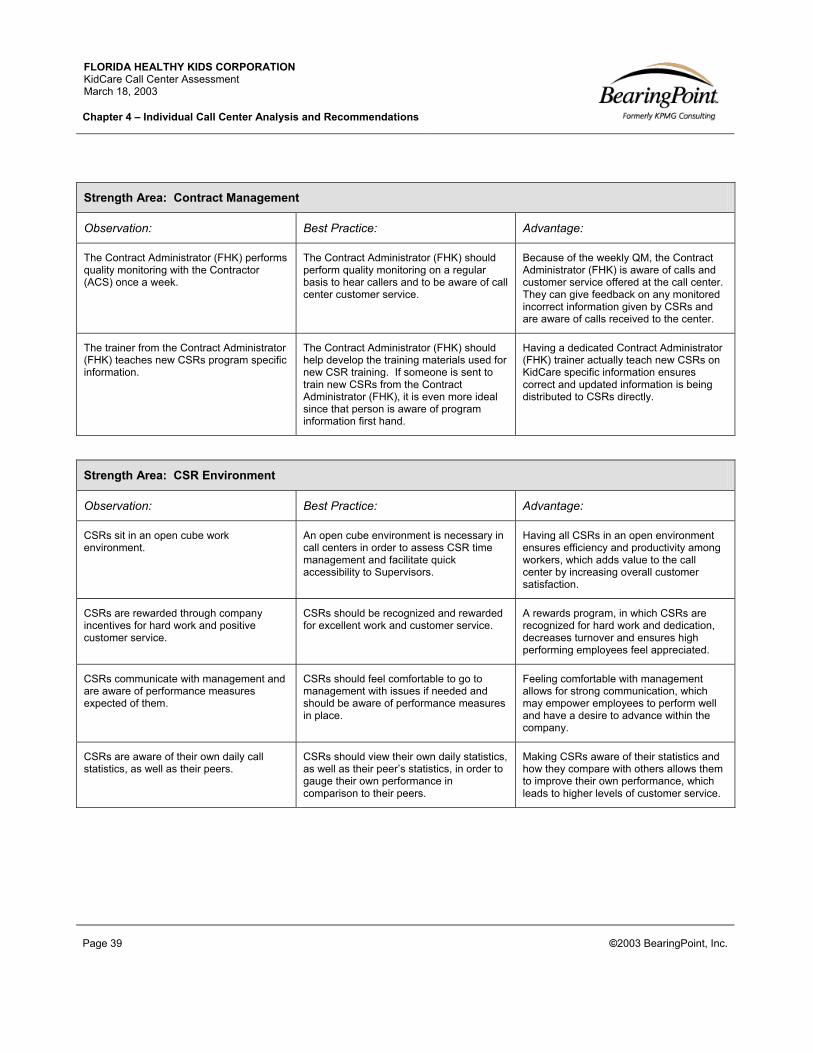
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 39 ©2003 BearingPoint, Inc.
Strength Area: Contract Management
Observation: Best Practice: Advantage:
The Contract Administrator (FHK) performs quality monitoring with the Contractor (ACS) once a week.
The Contract Administrator (FHK) should perform quality monitoring on a regular basis to hear callers and to be aware of call center customer service.
Because of the weekly QM, the Contract Administrator (FHK) is aware of calls and customer service offered at the call center. They can give feedback on any monitored incorrect information given by CSRs and are aware of calls received to the center.
The trainer from the Contract Administrator (FHK) teaches new CSRs program specific information.
The Contract Administrator (FHK) should help develop the training materials used for new CSR training. If someone is sent to train new CSRs from the Contract Administrator (FHK), it is even more ideal since that person is aware of program information first hand.
Having a dedicated Contract Administrator (FHK) trainer actually teach new CSRs on KidCare specific information ensures correct and updated information is being distributed to CSRs directly.
Strength Area: CSR Environment
Observation: Best Practice: Advantage:
CSRs sit in an open cube work environment.
An open cube environment is necessary in call centers in order to assess CSR time management and facilitate quick accessibility to Supervisors.
Having all CSRs in an open environment ensures efficiency and productivity among workers, which adds value to the call center by increasing overall customer satisfaction.
CSRs are rewarded through company incentives for hard work and positive customer service.
CSRs should be recognized and rewarded for excellent work and customer service.
A rewards program, in which CSRs are recognized for hard work and dedication, decreases turnover and ensures high performing employees feel appreciated.
CSRs communicate with management and are aware of performance measures expected of them.
CSRs should feel comfortable to go to management with issues if needed and should be aware of performance measures in place.
Feeling comfortable with management allows for strong communication, which may empower employees to perform well and have a desire to advance within the company.
CSRs are aware of their own daily call statistics, as well as their peers.
CSRs should view their own daily statistics, as well as their peer’s statistics, in order to gauge their own performance in comparison to their peers.
Making CSRs aware of their statistics and how they compare with others allows them to improve their own performance, which leads to higher levels of customer service.
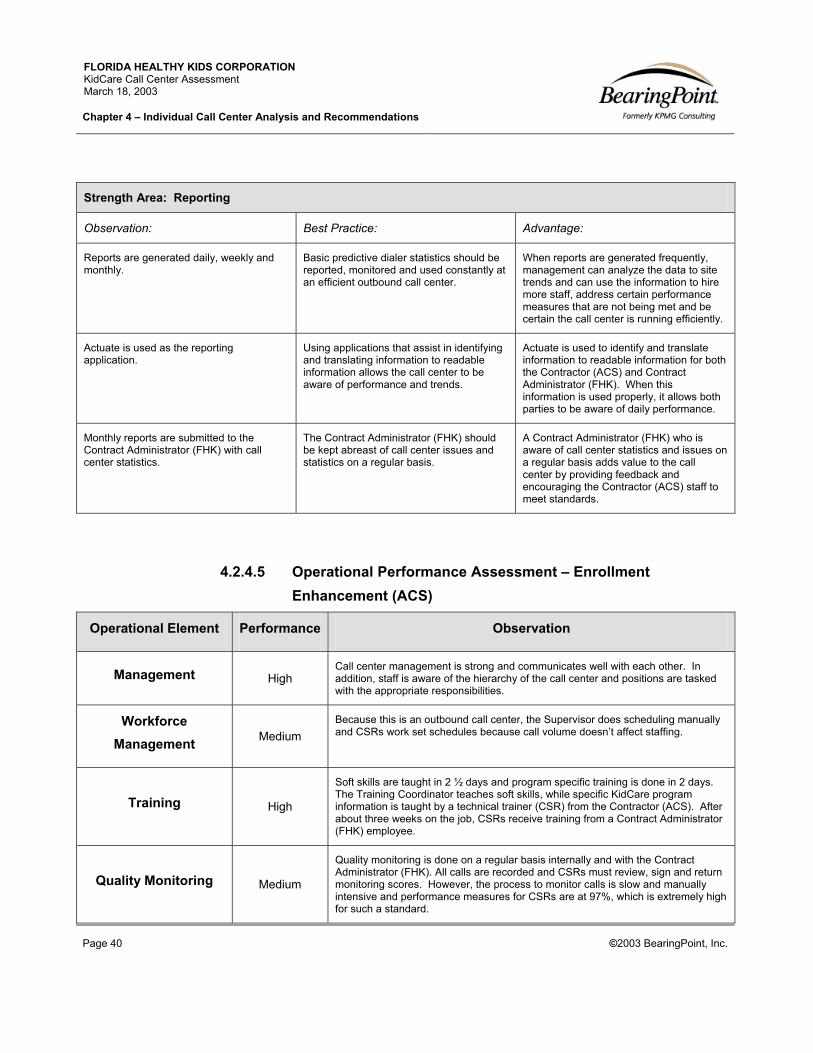
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 40 ©2003 BearingPoint, Inc.
Strength Area: Reporting
Observation: Best Practice: Advantage:
Reports are generated daily, weekly and monthly.
Basic predictive dialer statistics should be reported, monitored and used constantly at an efficient outbound call center.
When reports are generated frequently, management can analyze the data to site trends and can use the information to hire more staff, address certain performance measures that are not being met and be certain the call center is running efficiently.
Actuate is used as the reporting application.
Using applications that assist in identifying and translating information to readable information allows the call center to be aware of performance and trends.
Actuate is used to identify and translate information to readable information for both the Contractor (ACS) and Contract Administrator (FHK). When this information is used properly, it allows both parties to be aware of daily performance.
Monthly reports are submitted to the Contract Administrator (FHK) with call center statistics.
The Contract Administrator (FHK) should be kept abreast of call center issues and statistics on a regular basis.
A Contract Administrator (FHK) who is aware of call center statistics and issues on a regular basis adds value to the call center by providing feedback and encouraging the Contractor (ACS) staff to meet standards.
4.2.4.5 Operational Performance Assessment – Enrollment Enhancement (ACS)
Operational Element Performance Observation
Management High Call center management is strong and communicates well with each other. In addition, staff is aware of the hierarchy of the call center and positions are tasked with the appropriate responsibilities.
Workforce Management Medium
Because this is an outbound call center, the Supervisor does scheduling manually and CSRs work set schedules because call volume doesn’t affect staffing.
Training High
Soft skills are taught in 2 ½ days and program specific training is done in 2 days. The Training Coordinator teaches soft skills, while specific KidCare program information is taught by a technical trainer (CSR) from the Contractor (ACS). After about three weeks on the job, CSRs receive training from a Contract Administrator (FHK) employee.
Quality Monitoring Medium
Quality monitoring is done on a regular basis internally and with the Contract Administrator (FHK). All calls are recorded and CSRs must review, sign and return monitoring scores. However, the process to monitor calls is slow and manually intensive and performance measures for CSRs are at 97%, which is extremely high for such a standard.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 41 ©2003 BearingPoint, Inc.
CSR Medium
CSRs work in an open, positive work environment, with an established rewards program. They seem to be aware of their performance standards and daily stats. The environment provided for the CSR operations was exemplary. However, direct shadowing of CSRs indicated that their actual call handling technique was average in comparison to call center best practices.
Reporting High Reports are generated frequently and Actuate is used to identify and translate data. Reports are given to the Contract Administrator (FHK) on a weekly and monthly basis.
Technology Medium While Enrollment Enhancement (ACS) uses Actuate for reporting, there is no predictive dialer used for CSRs. Although ACS does have online monitoring, the technology is not used for this particular call center contract.
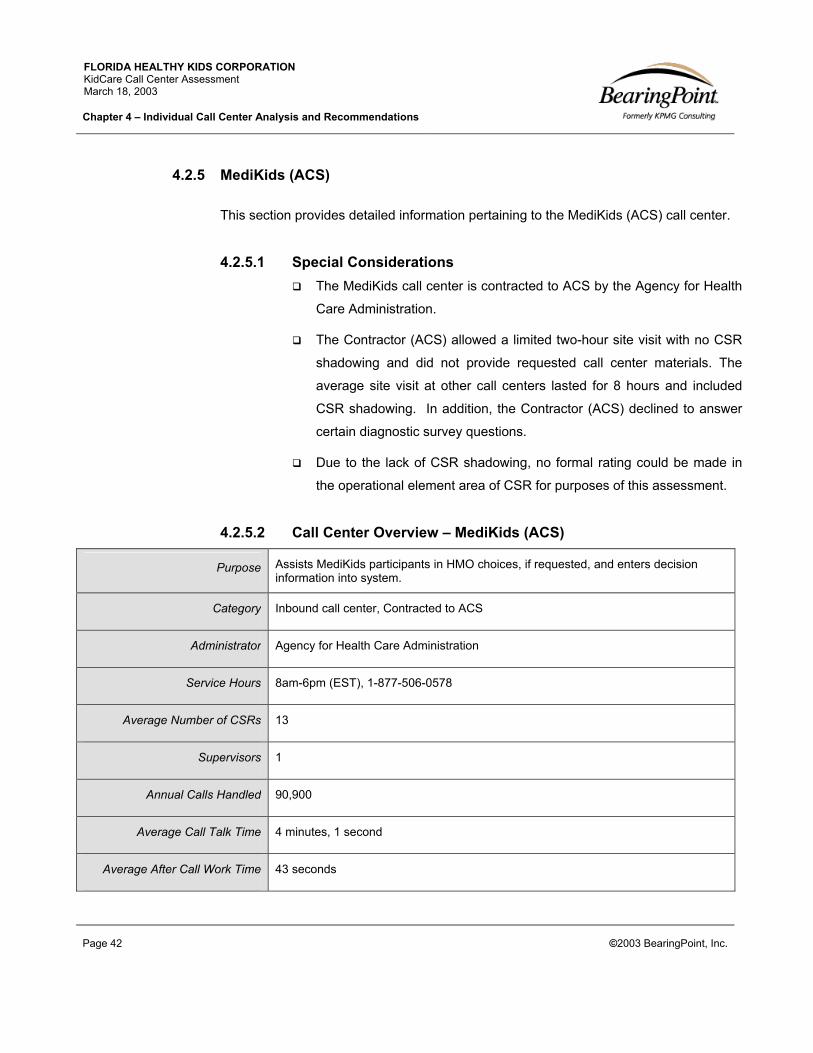
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 42 ©2003 BearingPoint, Inc.
4.2.5 MediKids (ACS)
This section provides detailed information pertaining to the MediKids (ACS) call center.
4.2.5.1 Special Considerations The MediKids call center is contracted to ACS by the Agency for Health
Care Administration.
The Contractor (ACS) allowed a limited two-hour site visit with no CSR
shadowing and did not provide requested call center materials. The
average site visit at other call centers lasted for 8 hours and included
CSR shadowing. In addition, the Contractor (ACS) declined to answer
certain diagnostic survey questions.
Due to the lack of CSR shadowing, no formal rating could be made in
the operational element area of CSR for purposes of this assessment.
4.2.5.2 Call Center Overview – MediKids (ACS)
Purpose Assists MediKids participants in HMO choices, if requested, and enters decision information into system.
Category Inbound call center, Contracted to ACS
Administrator Agency for Health Care Administration
Service Hours 8am-6pm (EST), 1-877-506-0578
Average Number of CSRs 13
Supervisors 1
Annual Calls Handled 90,900
Average Call Talk Time 4 minutes, 1 second
Average After Call Work Time 43 seconds

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 43 ©2003 BearingPoint, Inc.
Abandonment Rate 2.43%
Average Speed of Answer 27 seconds
Notes: *Average number of CSRs and calls handled is from the period of 12/01/01-11/30/02. *All other data is from the diagnostic survey.
4.2.5.3 Recommendation Areas - MediKids (ACS)
Recommendations Area: Quality Monitoring
Observation: Best Practice/Recommendation: Risk:
Current quality monitoring calibration sessions are conducted in a manner where the Supervisor listens to recorded calls that the ‘Quality Assurance’ unit has scored and either disagrees or agrees with the scoring. The resolution is based upon research of the correct answer and the two parties agree upon the final score for the CSR.
Quality monitoring calibration should be conducted by having all quality monitoring entities listen to the same recorded call at the same time and score it without knowledge of the other parties’ opinion. Once each party has scored the call, the separate scoring rationales should be thoroughly discussed.
When multiple parties conduct quality monitoring and they do not regularly calibrate their scoring standards, it risks an inconsistent scoring methodology. CSRs may notice the difference in scoring methodology and apply less value to feedback from their quality monitoring.
Persons performing quality monitoring must fill out forms manually and spend a significant amount of time trying to find a call to monitor.
Quality monitoring technology applications can automatically record calls and store them for later retrieval. These systems also automatically create a recording of the call that is easily forwarded to other monitors.
Manually recording calls and searching for calls to monitor is time consuming and manually intensive. Persons monitoring calls waste time looking for monitoring opportunities, when their time could be spent performing other duties.
The current quality monitoring scorecard is based upon a Pass/Fail grade, not a 100% scale.
The call center industry standard for quality monitoring scorecards is based on weighted averages that can equal up to 100% score.
Simplifying scorecards to simply equal a pass/fail grade may not allow the call center to properly observe differences in CSR performance. Two CSRs that receive a pass grade may practice levels of customer service that are significantly different, whereas a score of 85% versus 90% displays the degree of difference.
Recommendations Area: Workforce Management (WFM)
Observation: Best Practice/Recommendation: Risk:
The Supervisor performing workforce management does not compare forecasted volume with actual call center volume on a daily basis.
The Supervisor performing workforce management should determine forecasting accuracy by comparing forecasted volume to actual call volume.
When the Supervisor performing workforce management does not conduct a daily comparison of estimated versus actual call volume, it is difficult to clearly observe if estimates are inaccurate or on-target.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 44 ©2003 BearingPoint, Inc.
Recommendations Area: Workforce Management (WFM) (cont.)
Observation: Best Practice/Recommendation: Risk:
Call volume forecasting is based on manual calculations and does not utilize the Erlang C equation.
Effective workforce management does not have to be carried out by computer applications. However, even if it is determined by manual calculations, an Erlang C chart should be utilized to factor in the variance of “randomly arriving call patterns” in order to make accurate call volume forecasts.
WFM forecasts that do not employ the Erlang C equation are not able to factor in the random call arrival pattern. Thus, the forecasts are not as accurate as they could be and efficient staffing may be jeopardized.
Recommendations Area: CSR Training
Observation: Best Practice/Recommendation: Risk:
Although new CSRs are placed in a half-day week-long training program to learn about company policies, they do not receive classroom training to learn about the KidCare program, call center etiquette or the computer desktop system. Instead, new CSRs rely on an informal process of shadowing Senior CSRs until they are deemed “ready” to begin answering calls on their own. In addition, they are given a MediKids manual to learn from, but are not presented the material in a classroom setting.
Each call center should have a formal training program in which all new CSRs attend to learn specific KidCare program knowledge, call center etiquette and technology functionality.
Due to the lack of formal training at MediKids, CSRs may not be practicing consistent call center etiquette or dispensing consistent program knowledge. For example, CSRs are not formally taught MediKids program knowledge and are required to read a manual on their own, and learn from taking phone calls. This method does not have proper quality controls and increases the risk of wrong or inconsistent data given to customers.
Recommendations Area: CSR Performance Metrics
Observation: Best Practice/Recommendation: Risk:
Meeting a set quality monitoring score is not part of the CSR performance metrics.
CSRs at a call center should be aware of a set quality monitoring score that is part of their performance metrics. The industry standard for the QM scorecard goal is 85% out of 100%.
If a goal quality monitoring score is not part of the CSRs’ performance metrics, then they may not have as much incentive to overcome quality issues that are discovered during quality monitoring.
A report documenting CSR adherence to performance metrics is given to CSRs privately, but does not allow them to see their rank in comparison to other CSRs.
The call center industry encourages the practice of allowing CSRs to see how their performance stands in comparison to other CSRs, which often motivates them to improve their performance. Displaying ID numbers that only allow an individual to know where they rank, as opposed to viewing where specific people rank, is an encouraged practice.
If CSRs do not understand how their meeting of performance metrics ranks amongst their peers, they may not have a clear understanding of how their performance needs to improve or how it affects total call center performance.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 45 ©2003 BearingPoint, Inc.
Recommendations Area: CSR Performance Metrics (cont.)
Observation: Best Practice/Recommendation: Risk:
The Call Center Manager, Supervisor and Senior CSRs are unable to recite CSR performance metric standards from memory.
CSR standard performance metrics should be understood by all call center operational personnel to the degree of knowing the metrics by memory.
If call center operational personnel are unable to instantly recognize when a CSR does or does not meet a performance metric, it is more difficult to make quick adjustments to the CSR’s actions in order to meet standards.
4.2.5.4 Operational Strength Areas - MediKids (ACS)
Strength Area: CSR Career Path
Observation: Best Practice: Advantage:
CSRs have a clear career path and are able to expand into leadership roles within the company. In addition, verbal discussions from the site visit highlighted a low turnover rate within the call center.
Call centers should offer career advancement opportunities and define CSR career paths.
CSRs who feel like they can grow and advance in the company or call center are more dedicated and interested in providing customer service because they have a vested interest in advancement. In addition, CSRs who feel like they are able to expand their skills are less likely to leave the call center, reducing turnover, and increasing overall staff knowledge.
Strength Area: CSR Environment
Observation: Best Practice: Advantage:
CSRs sit in an open cube work environment with the Supervisor and Senior CSRs seated throughout the call center.
An open cube environment is necessary in call centers to assess CSR time management and facilitate quick accessibility to Supervisors. In addition, having Senior CSRs scattered throughout the call center insures CSRs can quickly ask for help from experienced co-workers.
Having all CSRs in an open environment with the Supervisor and Senior CSRs ensures efficiency and productivity among workers, which adds value to the call center by increasing overall customer satisfaction.
CSRs are rewarded through company incentives for hard work and positive customer service.
CSRs should be recognized and rewarded for excellent work and customer service.
A rewards program, in which CSRs are recognized for hard work and dedication, increases motivation and ensures high performing employees feel appreciated.
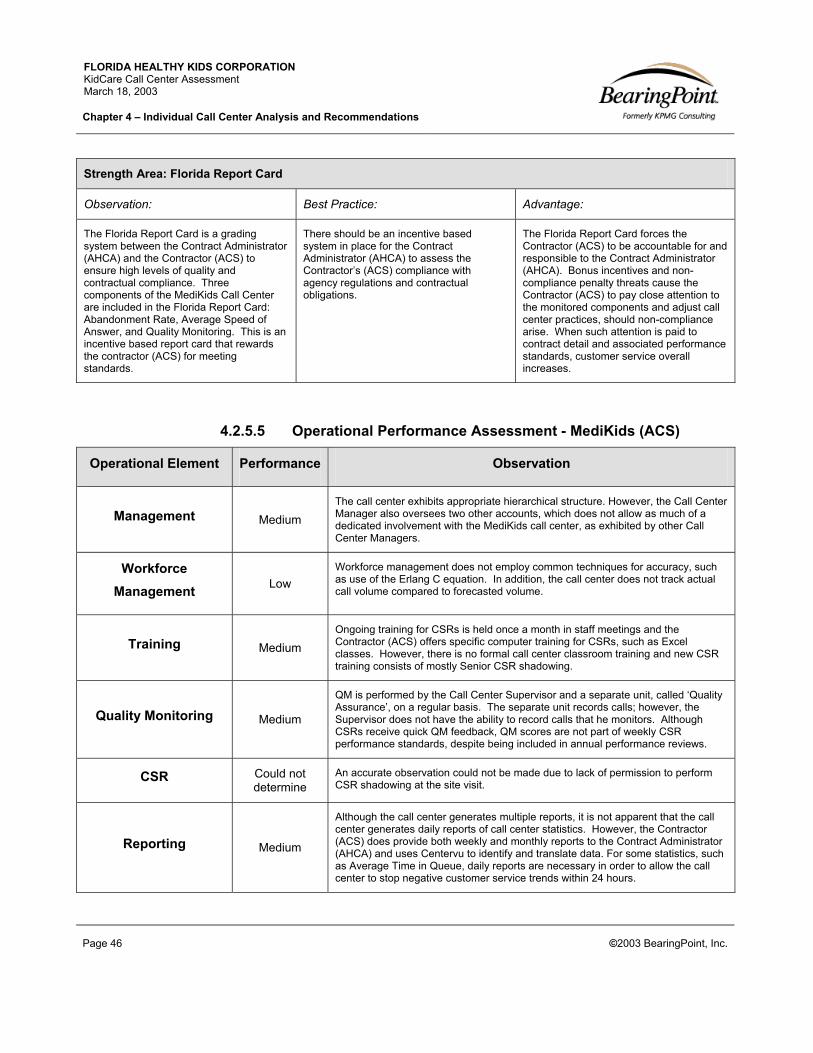
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 46 ©2003 BearingPoint, Inc.
Strength Area: Florida Report Card
Observation: Best Practice: Advantage:
The Florida Report Card is a grading system between the Contract Administrator (AHCA) and the Contractor (ACS) to ensure high levels of quality and contractual compliance. Three components of the MediKids Call Center are included in the Florida Report Card: Abandonment Rate, Average Speed of Answer, and Quality Monitoring. This is an incentive based report card that rewards the contractor (ACS) for meeting standards.
There should be an incentive based system in place for the Contract Administrator (AHCA) to assess the Contractor’s (ACS) compliance with agency regulations and contractual obligations.
The Florida Report Card forces the Contractor (ACS) to be accountable for and responsible to the Contract Administrator (AHCA). Bonus incentives and non-compliance penalty threats cause the Contractor (ACS) to pay close attention to the monitored components and adjust call center practices, should non-compliance arise. When such attention is paid to contract detail and associated performance standards, customer service overall increases.
4.2.5.5 Operational Performance Assessment - MediKids (ACS)
Operational Element Performance Observation
Management Medium The call center exhibits appropriate hierarchical structure. However, the Call Center Manager also oversees two other accounts, which does not allow as much of a dedicated involvement with the MediKids call center, as exhibited by other Call Center Managers.
Workforce Management Low
Workforce management does not employ common techniques for accuracy, such as use of the Erlang C equation. In addition, the call center does not track actual call volume compared to forecasted volume.
Training Medium Ongoing training for CSRs is held once a month in staff meetings and the Contractor (ACS) offers specific computer training for CSRs, such as Excel classes. However, there is no formal call center classroom training and new CSR training consists of mostly Senior CSR shadowing.
Quality Monitoring Medium
QM is performed by the Call Center Supervisor and a separate unit, called ‘Quality Assurance’, on a regular basis. The separate unit records calls; however, the Supervisor does not have the ability to record calls that he monitors. Although CSRs receive quick QM feedback, QM scores are not part of weekly CSR performance standards, despite being included in annual performance reviews.
CSR Could not determine
An accurate observation could not be made due to lack of permission to perform CSR shadowing at the site visit.
Reporting Medium
Although the call center generates multiple reports, it is not apparent that the call center generates daily reports of call center statistics. However, the Contractor (ACS) does provide both weekly and monthly reports to the Contract Administrator (AHCA) and uses Centervu to identify and translate data. For some statistics, such as Average Time in Queue, daily reports are necessary in order to allow the call center to stop negative customer service trends within 24 hours.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 4 – Individual Call Center Analysis and Recommendations
Page 47 ©2003 BearingPoint, Inc.
Technology Medium The following technology is used at the MediKids Call Center: ACD, IVR, and Centervu. MediKids should consider implementing a workforce management application for scheduling and a Quality Monitoring application to auto record calls.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 48 ©2003 BearingPoint, Inc.
5.0 KidCare Program Analysis
Although the KidCare program is a partnership of multiple state agencies and one not-for-profit
organization, the public and its beneficiaries often perceive KidCare as one entity. For example, if a
parent calls the KidCare Outreach (ACS) phone number and is then transferred to the Member Services
(DHACS) line, the parent may not understand that they are dealing with separately run call centers,
administered in separate locations through different organizations. As this example illustrates, KidCare’s
customer service reputation is a collective average of all of the related call centers providing some form
of KidCare service.
Given this understanding of the public’s experience, this chapter analyzes the collective performance of
the KidCare program. When possible, the individual performance of each call center is also broken out
to illustrate how the performance of each center affects the KidCare score. Chapter Six, KidCare
Program Recommendations, will offer recommendations for the overall KidCare Program based on the
analysis illustrated in this chapter.
Benchmarking is commonly used in the call center industry to compare the services and processes of
one call center to others of comparable service in order to identify improvement opportunities and new
ideas. This chapter analyzes the KidCare program through this benchmarking methodology. The
following exhibits will illustrate the performance of the KidCare program using the following statistics:
Exhibit 5.1: Annual Calls Handled
Exhibit 5.2: Annual Calls Offered vs. Annual Calls Handled
Exhibit 5.3: Average Handle Time (Average Call Talk Time and Average After Call Work Time)
Exhibit 5.4: Annual Calls Handled vs. Average Number of CSRs
Exhibit 5.5: Service Level: 80% of Calls Handled in “Y” seconds
Exhibit 5.6: Average Time in Queue vs. Abandonment Rate
Exhibit 5.7: CSR to Supervisor Ratio
Exhibit 5.8: Length of New CSR Training Period vs. Annual CSR Turnover Rate
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 49 ©2003 BearingPoint, Inc.
The benchmarking exhibits listed above illustrate KidCare program performance in three ways:
1. Benchmark the individual KidCare call centers against each other
2. Benchmark the overall KidCare program against industry averages (Federal Government, State
Government, or Healthcare)
3. Benchmark data against the call center industry best practice standard
It is important to note that these exhibits will not always include a comparison of every individual KidCare
call center. The reason for this discrepancy is because some call centers declined providing answers for
certain questions on the diagnostic survey, which was the source for benchmarking data. Please see the
”Notes” section at the end of every benchmarking discussion for a detailed explanation of why certain
call centers are not included in the exhibits.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 50 ©2003 BearingPoint, Inc.
5.1 Annual Calls Handled
Exhibit 5.1.1 Small Sized Call Center Medium Sized Call Center Large Sized Call Center
Federal Gov. Industry Ave. 1,207,670
Healthcare Industry Ave. 4,603,897
Call Center Industry Standard Small call centers handle less than 100,000 calls in a year
Medium call centers handle 100,000 to 500,000 calls in a year
Large call centers handle over 500,000 calls a year
Overall KidCare Total: 1,496,550
Member Services (DHACS) 603,284
KidCare Medicaid (DCF) 88,694
KidCare Outreach (ACS) 287,341
Enrollment Enhancement (ACS) 426,331
MediKids (ACS) 90,900
1,2 0 7,6 70
4 ,6 0 3 ,8 9 7
1,4 9 6 ,550
6 0 3 ,2 8 4
8 8 ,6 9 4 2 8 7,3 4 1
4 2 6 ,3 3 1
9 0 ,9 0 0
0
50 0 ,0 0 0
1,0 0 0 ,0 0 0
1,50 0 ,0 0 0
2 ,0 0 0 ,0 0 0
2 ,50 0 ,0 0 0
3 ,0 0 0 ,0 0 0
3 ,50 0 ,0 0 0
4 ,0 0 0 ,0 0 0
4 ,50 0 ,0 0 0
5,0 0 0 ,0 0 0
Num
ber o
f Cal
ls
F ed eral Go v.Ind ust ry A ve.
Healt hcareInd ust ry A ve.
Overal lKid C are
T o t al
M emb erServices( D HA C S)
Kid C areM ed icaid
( D C F )
Kid C areOut reach
( A C S)
Enro llmentEnhancement
( A C S)
M ed iKid s( A C S)
Exhibit 5.1- Annual Calls Handled

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 51 ©2003 BearingPoint, Inc.
“Calls handled” refers to live calls handled by CSRs and voice mails that are resolved by CSRs
either by calling the caller back or carrying out the requested service without calling the caller
back. A call center may choose to separately measure the CSR calls handled and the voice mail
calls handled. However, for this benchmark, the CSR and voice mail calls handled for the call
centers have been integrated into the single statistic “calls handled.”
The annual volume of calls handled at a call center is commonly used as a gauge for
categorizing call centers into small, medium and large size categories. Small call centers handle
100,000 or less calls in a year. Medium sized call centers handle between 100,00 and 500,000
calls in a year, while large call centers handle 500,000 or more calls in a year.
The average federal government and healthcare industry call centers fall into the large
category of call centers.
The average healthcare industry call center is four times larger than federal government call
centers.
The overall KidCare call center is considered a large call center.
The KidCare Medicaid (DCF) and MediKids (ACS) call centers fall into the small category.
Call centers of this size usually exhibit ad-hoc processes and are operated with a necessary
and less strategic emphasis.
The KidCare Outreach (ACS) and Enrollment Enhancement (ACS) call centers are
considered medium sized call centers and should exhibit processes that are part of the
administering organization’s business objectives.
The Member Services (DHACS) call center is considered a large call center and should
exhibit service differentiating customer service skills and technology.
Notes: * The annual calls handled for Member Services (DHACS), KidCare Outreach (ACS), Enrollment Enhancement (ACS), MediKids (ACS), and KidCare Medicaid (DCF) was for the period of 12/01/01 – 11/30/02. * The annual calls handled for the Member Services (Affina) call center during the period of 12/01/01-11/30/02 was 485,491. Thus, the total call volume for the Member Services call center (DHACS and Affina) during this period was 1,088,775. * The Overall KidCare total calls handled, including the Affina location of the Member Services call center, is 1,982,041 for the period of 12/01/02-11/30/02.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 52 ©2003 BearingPoint, Inc.
5.2 Annual Calls Offered vs. Annual Calls Handled
Exhibit 5.2.1 Annual Calls Offered - Annual Calls Handled = Annual Calls Not Handled
Call Center Industry
Standard
“Annual calls offered” and “Annual calls handled” do not illustrate a call center’s customer service performance as stand alone metrics. However, a consideration of “Annual calls not handled” allows the call center to observe the number of customers that hang up when trying to reach a call center. There is no industry standard for “Annual calls not handled”. Call centers must determine on an individual basis what they consider to be acceptable for this metric. A closely related metric, “Abandonment rate”, is discussed in Section 5.6.
Overall KidCare Total 1,173,931 1,070,219 103,712
Member Services (DHACS) 656,543 603,284 53,259
KidCare Medicaid (DCF) 107,308 88,694 18,614
KidCare Outreach (ACS) 297,258 287,341 9,917
MediKids (ACS) 112,822 90,900 21,922
Exhibit 5.2- Annual Calls Offered vs. Annual CSR Calls Handled
1,0 70 ,2 19
6 0 3 ,2 8 4
8 8 ,6 9 4
2 8 7,3 4 1
9 0 ,9 0 0
6 56 ,54 3
1,173 ,9 3 1
10 7,3 0 8112 ,8 2 2
2 9 7,2 58
0
2 0 0 ,0 0 0
4 0 0 ,0 0 0
6 0 0 ,0 0 0
8 0 0 ,0 0 0
1,0 0 0 ,0 0 0
1,2 0 0 ,0 0 0
1,4 0 0 ,0 0 0
Overal l Kid C areT o t al
M emb er Services( D HA C S)
Kid C are M ed icaid( D C F )
Kid C are Out reach( A C S)
M ed iKid s ( A C S)
Num
ber o
f Cal
ls

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 53 ©2003 BearingPoint, Inc.
“Calls offered” refers to the total number of calls that reach a call center. These calls may end up
with varying results; some callers may hang up before reaching a CSR; some callers may leave
a message in a voice mailbox; or some callers may speak to a CSR. All of these scenarios are
considered “calls offered”. As discussed previously in Exhibit 5.1, “calls handled” refers to calls
handled live by CSRs, as well as voice mail calls that are addressed and satisfactorily completed
by CSRs.
Call centers often measure their number of calls offered versus their number of calls handled.
The subtraction of calls handled from calls offered allows for an estimation of the number of calls
that may not have received service. However, when considering the number that is derived from
this basic equation it is important to also consider a statistic called “IVR calls handled”. IVR calls
handled refers to the number of calls that reach an IVR menu, and are completed by receiving
information obtainable from pre-recorded messages in the IVR. If a call center does not track
“IVR calls handled”, but has the capability to complete calls over the IVR, their number of calls
not handled may be skewed higher due to not subtracting the IVR calls handled from this
statistic.
Notes: *The annual calls handled and calls offered statistics for Member Services (DHACS), KidCare Outreach (ACS), MediKids (ACS), and KidCare Medicaid (DCF) was for the period of 12/01/0 – 11/30/02. * MediKids (ACS) is not included in Exhibit 5.2 because they declined to provide their annual calls offered statistic. * Enrollment Enhancement (ACS) is not included on Exhibit 5.2 because they are an outbound call center and the calls offered statistic is not relevant. * The calls offered for the total Member Services (Affina) call center during the period of 12/01/01-11/30/02 was 502,049. Thus, the total calls offered for the Member Services call center (DHACS and Affina) during this period was 1,158,592. * The calls handled for the total Member Services (Affina) call center during the period of 12/01/01-11/30/02 was 485,491. Thus, the total call handled for the Member Services call center (DHACS and Affina) during this period was 1,088,775. * The calls not handled for the total Member Services call center (DHACS and Affina) during the period of 12/01/01-11/30/02 was 69,817. * The Overall KidCare total calls offered, including the Affina location of the Member Services call center, is 1,675,980. * The Overall KidCare total calls handled, including the Affina location of the Member Services call center, is 1,555,710. * The Overall KidCare total calls not handled, including the Affina location of the Member Services call center, is 120,270.
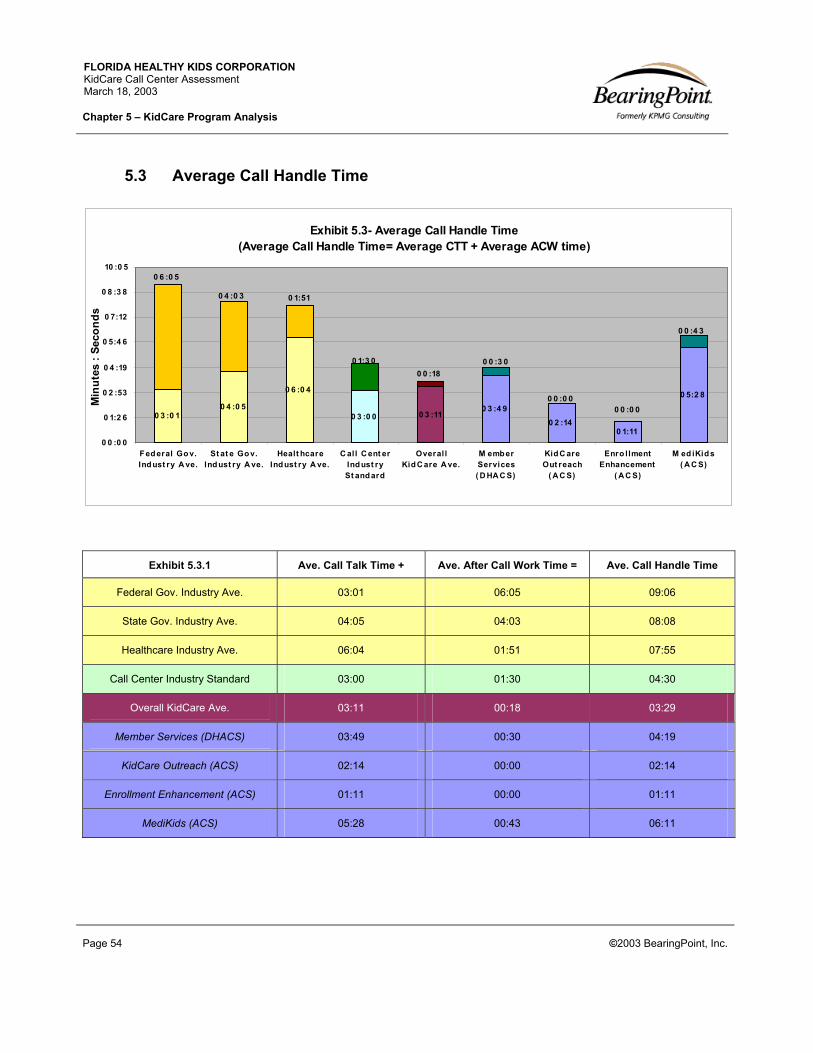
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 54 ©2003 BearingPoint, Inc.
5.3 Average Call Handle Time
Exhibit 5.3.1 Ave. Call Talk Time + Ave. After Call Work Time = Ave. Call Handle Time
Federal Gov. Industry Ave. 03:01 06:05 09:06
State Gov. Industry Ave. 04:05 04:03 08:08
Healthcare Industry Ave. 06:04 01:51 07:55
Call Center Industry Standard 03:00 01:30 04:30
Overall KidCare Ave. 03:11 00:18 03:29
Member Services (DHACS) 03:49 00:30 04:19
KidCare Outreach (ACS) 02:14 00:00 02:14
Enrollment Enhancement (ACS) 01:11 00:00 01:11
MediKids (ACS) 05:28 00:43 06:11
Exhibit 5.3- Average Call Handle Time (Average Call Handle Time= Average CTT + Average ACW time)
0 3 :0 10 4 :0 5
0 6 :0 4
0 3 :0 0 0 3 :110 3 :4 9
0 2 :140 1:11
0 5:2 8
0 0 :4 3
0 6 :0 5
0 4 :0 3 0 1:51
0 0 :0 00 0 :0 0
0 1:3 00 0 :18
0 0 :3 0
0 0 :0 0
0 1:2 6
0 2 :53
0 4 :19
0 5:4 6
0 7:12
0 8 :3 8
10 :0 5
F ed eral Go v.Ind ust ry A ve.
St at e Go v.Ind ust ry A ve.
Healt hcareInd ust ry A ve.
C all C ent erInd ust rySt and ard
Overal lKid C are A ve.
M emb erServices( D HA C S)
Kid C areOut reach
( A C S)
Enro llmentEnhancement
( A C S)
M ed iKid s( A C S)
Min
utes
: Se
cond
s

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 55 ©2003 BearingPoint, Inc.
Average call talk time (CTT) is the average amount of time a CSR is on a call servicing a
customer. After call work (ACW) time is the amount of time a CSR spends doing work related to
the call after hanging up with the customer, but before beginning a new call. The combination of
average call talk time and after call work time associated with a call is what is considered the
average call handle time. In order for a call center to effectively schedule CSR staffing, it is
important for it to consider the average call handle time required by a CSR. When forecasting
data such as the total minutes of an hour that a CSR is handling calls (see Exhibits 5.4 and 5.5),
it is important to calculate the average call handle time.
It is an industry best practice to track after call work time for CSRs. Most CSR telephone
extension systems have a button labeled as “After Call Work (ACW)” or similar terminology, that
a CSR is required to press when performing any after call work. However, it is common for call
centers to not track after call work time for CSRs because CSRs will often continue to finish up
work related to one call while answering another call or keep their phone extension on
“available” (indicating they are available to take calls) while finishing after call work. Call centers
should train their CSRs to use the ACW button and not integrate finishing up a call while
answering another or taking advantage of slow call volume to do after call work. Because of
this, a call center may claim to not have after call work time, when CSRs are performing this task
in reality. This may be an indication of improper training in usage of the ACW button. Failing to
train CSRs to appropriately use the ACW button may result in forecasts that underestimate the
true total call time for a call center.
The Overall KidCare average call handle time is 3 minutes and 29 seconds, composed of 3
minutes and 11 seconds of average call time and 18 seconds of average after call work time.
The call center industry standard for call talk time is approximately 3 minutes. However this
is an industry standard for the average call center. Call centers located in the healthcare
industry are known to require longer call talk times, such as displayed in Exhibit 5.3 by the 6
minute and 4 second healthcare industry average. The industry standard and healthcare
industry average should both be used as a starting point for determining appropriate call talk
times for the KidCare call centers.
The average after call work time for the call center industry is 1 minute and 30 seconds. The
overall KidCare average falls below this standard. As discussed above, this may be an
indication of incorrectly tracking ACW for CSRs.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 56 ©2003 BearingPoint, Inc.
Notes: * KidCare Medicaid (DCF) is not included in Exhibit 5.3 because they do not capture after call work time. Their average talk time is currently 3 minutes and 18 seconds. * The average CTT and average ACW time listed in this benchmark is derived from the answers to questions C5 and C7 in the diagnostic survey.
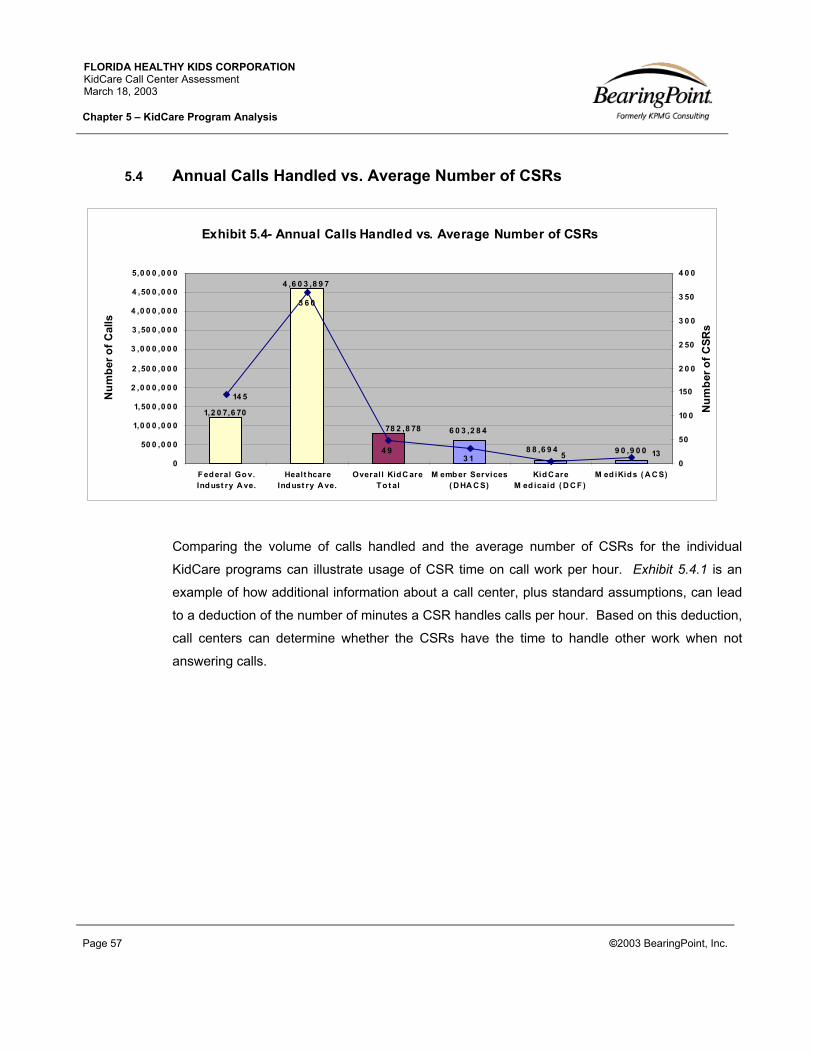
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 57 ©2003 BearingPoint, Inc.
5.4 Annual Calls Handled vs. Average Number of CSRs
Comparing the volume of calls handled and the average number of CSRs for the individual
KidCare programs can illustrate usage of CSR time on call work per hour. Exhibit 5.4.1 is an
example of how additional information about a call center, plus standard assumptions, can lead
to a deduction of the number of minutes a CSR handles calls per hour. Based on this deduction,
call centers can determine whether the CSRs have the time to handle other work when not
answering calls.
Exhibit 5.4- Annual Calls Handled vs. Average Number of CSRs
6 0 3 ,2 8 4
9 0 ,9 0 08 8 ,6 9 4
78 2 ,8 78
4 ,6 0 3 ,8 9 7
1,2 0 7,6 70
14 5
3 6 0
4 93 1 5 13
0
50 0 ,0 0 0
1,0 0 0 ,0 0 0
1,50 0 ,0 0 0
2 ,0 0 0 ,0 0 0
2 ,50 0 ,0 0 0
3 ,0 0 0 ,0 0 0
3 ,50 0 ,0 0 0
4 ,0 0 0 ,0 0 0
4 ,50 0 ,0 0 0
5,0 0 0 ,0 0 0
Federal Gov.Indust ry A ve.
Healt hcareIndust ry A ve.
Overal l KidC areTo t al
M ember Services( D HA C S)
KidC areM ed icaid ( D C F)
M ed iKids ( A C S)
Num
ber o
f Cal
ls
0
50
10 0
150
2 0 0
2 50
3 0 0
3 50
4 0 0
Num
ber o
f CSR
s

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 58 ©2003 BearingPoint, Inc.
Exhibit 5.4.1 (Annual calls handled)
Divided by (Average number
of CSRs) =
Divided by (# of working
weeks in a year) = (assume 52
weeks)
Divided by (# of working days
in a week) = (assume 5 days)
Divided by (CSR daily hours of work at a call
center) = (assume 8 hours)
Multiply (Average call
handle time) by (# of calls an hour)
=
Federal Gov. Industry Ave.
8,329 CSR calls handled in a year per CSR
160 calls handled a week per CSR
32 calls handled a day per CSR
4 calls an hour per CSR
(Assumes CSR works 8 hours a day)
Approximately 36 total minutes of call talk and work time per hour for a CSR
(Assumes CTT-3:01 + ACW-6:05 = ACHT-9:06)
Healthcare Industry Ave.
12,789 CSR calls handled in a year per CSR
246 calls a handled week per CSR
49 calls a handled day per CSR
6 calls an hour per CSR
(Assumes CSR works 8 hours a day)
Approximately 48 total minutes of call talk and work time per hour for a CSR
(Assumes CTT-6:04 + ACW-1:51 = ACHT-7:55)
Call Center Industry Standard
There is no industry standard for the amount of time a CSR spends on call related work in an hour. Call centers must determine what they consider to be acceptable for this metric on an individual basis. When choosing their standard for this metric, call centers should consider the stress level of the calls handled by CSRs and the amount of non-call work that the call center wants the CSRs to complete in an hour.
Overall KidCare Ave.
15,977 CSR calls handled in a year per CSR
307 calls handled a week per CSR
61 calls handled a day per CSR
8 calls an hour per CSR
(Assumes CSR works 8 hours a day)
Approximately 36 total minutes of call talk and work time per hour for a CSR
(Assumes CTT-3:55 + ACW-0:37 = ACHT-4:32)
Member Services (DHACS)
19,461 calls handled in a year per CSR
374 calls handled a week per CSR
75 calls a day per CSR
8 calls an hour per CSR
(Assumes CSR works 9 hours a day)
Approximately 35 total minutes of average handle time per hour for a CSR
(Assumes CTT-3:49 + ACW-0:30 = ACHT-4:19)
MediKids (ACS) 6,992 calls handled in a year per CSR
134 calls handled a week per CSR
27 calls a day per CSR
3 calls an hour per CSR
(Assumes CSR works 9 hours a day)
Approximately 19 total minutes of average handle time per hour for a CSR
(Assumes CTT- 5:28 + ACW-0:43 = ACHT-6:11)

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 59 ©2003 BearingPoint, Inc.
In Exhibit 5.4.1, the Healthcare industry averages illustrates that their CSRs spend the
majority of an hour performing call related work. This indicates that at these call centers the
CSRs should not be expected to perform other work not related to handling calls. If the
CSRs were to be put in a scenario where they are expected to handle other work and
continue to have call related work metrics as illustrated, the call centers would risk over
utilizing the CSRs and high turn over rates.
The Overall KidCare average of 26 minutes an hour spent on call related work is acceptable
and illustrates that it would be realistic to assign other non-call related work to CSRs at the
Member Services (DHACS) and MediKids (ACS) call centers.
Notes: *The annual calls handled and CSR number in this benchmark is for the period of 12/01/01-11/30/02. * For Exhibit 5.4, the KidCare Outreach (ACS) and Enrollment Enhancement (ACS) call centers are not included because they asked that their total number of CSRs not be published in this assessment. * For Exhibit 5.4.1, the KidCare Medicaid (DCF) call center is not included because they do not calculate their ACW time.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 60 ©2003 BearingPoint, Inc.
5.5 Service Level: 80% of Calls Handled in “Y” Seconds
Exhibit 5.5.1 X% Y Seconds
Federal Gov. Industry Ave. 80% 42 Seconds
State Gov. Industry Ave. 80% 35 Seconds
Healthcare Industry Ave. 80% 60 Seconds
Call Center Industry Standard 80% 20 Seconds
Overall KidCare Ave. 80% 27 Seconds
Member Services (DHACS) 80% 27 Seconds
MediKids (ACS) 80% 27 Seconds
The best practice for describing service levels at a call center is to state it in the terms of ”X% of
calls handled in Y seconds”. The rationale behind why this is considered the most effective way
to illustrate service level is because it gives the clearest indication of a caller’s experience when
they call the call center by considering a majority of the callers (“X” %) and the speed of their
service (“Y” seconds). In other words, this expression captures the majority of callers and allows
an analyst to understand how long callers have to wait before reaching a CSR. The call center
4 2 3 5 6 0 2 0 2 7 2 7 2 7
0
10
2 0
3 0
4 0
50
6 0
Seco
nds
F ed eralGo v.
Indust ryA ve.
St at e Gov.Ind ust ry
A ve.
Healt hcareInd ust ry
A ve.
C al l C ent erIndust rySt and ard
Overal lKid C are
A ve.
M emb erServices( D HA C S)
M ed iKids( A C S)
Exhibit 5.5- Service Level: 80% of Calls Handled in "Y" Seconds

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 61 ©2003 BearingPoint, Inc.
industry often uses the standard of “80% of calls handled in 20 seconds” as a benchmark. In
reality, this benchmark should be a starting point for call centers when determining their Service
Level goal. The specific “X” and “Y” should be determined by each individual call center and is
highly dependent upon the specific environment of the industry, the call center technology, and
other program dependencies.
Setting service levels by number of calls handled, or average speed of answer, is not as
effective as this method because they only indicate the average caller experience, as opposed to
the majority’s experience. The number of calls handled does not illustrate how long the caller
had to wait before being serviced. At the same time, average speed of answer is exactly that, an
average and not a majority. A call center could have one morning of two-second speed of
answers, but an afternoon of three-minute speed of answers. The use of average speed of
answer to illustrate service level would not be an accurate display of the service that the majority
of callers experienced. Instead, it would be a display of the average caller experience. The
KidCare call centers should move to uniformly track their service levels by the “X% of calls
handled in Y seconds” method.
Only the Member Services (DHACS) and MediKids (ACS) call centers measure their service
level by the formula “X% of calls in Y seconds”.
The average KidCare service level does not perform as well as the call center industry
standard. However, it is much better than the federal government, state government, and
healthcare industry averages.
Notes: * The data reflected in Exhibit 5.5 is derived from the answer to question C1 in the diagnostic. * KidCare Medicaid (DCF) and KidCare Outreach (ACS) are not included in Exhibit 5.5 because they do not track their service level based on this formula. * Enrollment Enhancement (ACS) is not included in Exhibit 5.5 because this level of service does not apply to outbound call centers.
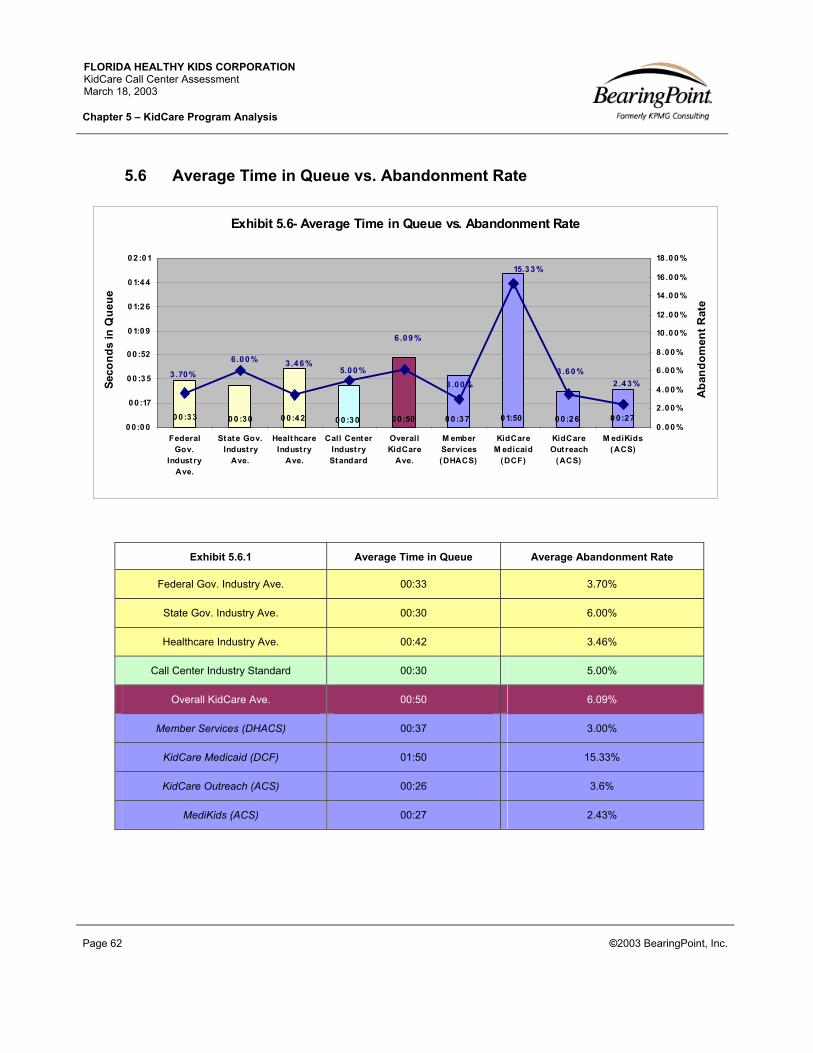
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 62 ©2003 BearingPoint, Inc.
5.6 Average Time in Queue vs. Abandonment Rate
Exhibit 5.6.1 Average Time in Queue Average Abandonment Rate
Federal Gov. Industry Ave. 00:33 3.70%
State Gov. Industry Ave. 00:30 6.00%
Healthcare Industry Ave. 00:42 3.46%
Call Center Industry Standard 00:30 5.00%
Overall KidCare Ave. 00:50 6.09%
Member Services (DHACS) 00:37 3.00%
KidCare Medicaid (DCF) 01:50 15.33%
KidCare Outreach (ACS) 00:26 3.6%
MediKids (ACS) 00:27 2.43%
Exhibit 5.6- Average Time in Queue vs. Abandonment Rate
0 0:33 0 0 :270 0 :2 601:500 0 :3700 :5000 :3 00 0 :420 0 :30
3 .0 0%
6 .09 %
5.00 %3 .4 6%6.00 %
3 .70%
15.3 3 %
3 .6 0 %2 .4 3%
0 0:0 0
0 0 :17
00 :3 5
00 :52
0 1:0 9
0 1:2 6
0 1:4 4
0 2 :01
FederalGov.
Indust ryAve.
Stat e Gov.Indust ry
Ave.
HealthcareIndust ry
Ave.
Call CenterIndust ryStandard
OverallKidCare
Ave.
M emberServices(DHACS)
KidCareM edicaid
(DCF)
KidCareOutreach
(ACS)
M ediKids(ACS)
Seco
nds
in Q
ueue
0 .00 %
2.00 %
4.00 %
6.00 %
8.00 %
10 .00 %
12 .00 %
14 .00 %
16 .00 %
18 .00 %
Aba
ndom
ent R
ate

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 63 ©2003 BearingPoint, Inc.
The time in queue represents the amount of time a caller will wait before reaching a CSR. The
abandonment rate represents the percentage of calls that hang up before reaching a CSR.
There is usually a direct correlation between a call center’s time in queue and the overall
abandonment rate. Abandonment of a call is interpreted by the call center industry as a gauge
of customer frustration, and hence an experience of low customer service. The industry
standard is to achieve an abandonment rate of 5 percent or less.
One of the most relevant factors that determines abandonment rate at a call center is the
tolerance level of a caller. While this factor cannot be controlled by a call center, it can be
gauged by using ACD reports that illustrate abandonment rates and average time to abandon.
Once a call center understands what the average time to abandon is at the call center, it can
staff appropriately to achieve a 5% abandonment rate.
Of the KidCare call centers that track abandonment rate, Member Services (DHACS),
KidCare Outreach (ACS) and MediKids (ACS) illustrate better than industry standard
performance.
KidCare Medicaid (DCF)’s abandonment rate and wait time are significantly higher than
other KidCare call centers and industry standards.
The overall KidCare program does not perform as well as the industry standard for
abandonment rate and average time in queue, mostly due to the performance of the KidCare
Medicaid (DCF) call center.
Notes: * The data illustrated in Exhibit 5.6 is derived from the answer to questions C3, C10 and C11 in the diagnostic. *The Enrollment Enhancement (ACS) call center is not included in Exhibit 5.6 because the statistics are not applicable to an outbound call center.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 64 ©2003 BearingPoint, Inc.
5.7 CSR to Supervisor Ratio
Exhibit 5.7.1 “X” CSRs to 1 Supervisor
Federal Gov. Industry Ave. 15
State Gov. Industry Ave. 17
Healthcare Industry Ave. 18
Call Center Industry Standard 15
Overall KidCare Ave. 16
Member Services (DHACS) 31
KidCare Medicaid (DCF) 5
MediKids (ACS) 13
15 17 18 15 16 3 1 5 130
5
10
15
2 0
2 5
3 0
3 5
Num
ber o
f CSR
s
F ed eralGo v.
Ind ust ryA ve.
St at e Go v.Ind ust ry
A ve.
Healt hcareInd ust ry
A ve.
C all C ent erInd ust rySt and ard
OverallKid C are
A ve.
M emb erServices( D HA C S)
Kid C areM ed icaid
( D C F )
M ed iKid s( A C S)
Exhibit 5.7- CSR to Supervisor Ratio ("X" CSRs to 1 Supervisor)

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 65 ©2003 BearingPoint, Inc.
The industry standard for CSR to Supervisor ratio is 15 to 1. This is considered the ideal ratio
where a Supervisor is able to appropriately distribute his/her time between each CSR to provide
individual coaching and assessment. It is important to also recognize that some call centers will
use experienced CSRs to perform common tasks of Supervisors, such as coaching a CSR in
weak areas.
The average state government and healthcare industry call centers are worse than the call
center industry standard CSR to Supervisor ratio.
The overall KidCare program CSR to Supervisor ratio of 16 to 1 almost meets the industry
standard.
The KidCare Medicaid (DCF) call center has an extremely low CSR to Supervisor ratio of 5
to 1 when compared to the industry standard of 15 to 1.
The Member Services (DHACS) call center has 4 Team Leads who are experienced CSRs
that perform many Supervisory tasks, such as mentoring their own team of CSRs. Due to
the fact that the Team Leads are not officially Supervisors, and do not perform all
Supervisory tasks, they were not included in Member Services (DHACS)’ total number of
Supervisors. If they had been included, Member Services (DHACS)’ CSR to Supervisor
Ratio would be 10 to 1.
Notes: * The number of CSRs and Supervisors in Exhibit 5.7 is from the period of 12/01/01-11/30/02. * The KidCare Outreach (ACS) and Enrollment Enhancement (ACS) call centers are not included in Exhibit 5.7 because they declined to offer this information in the assessment diagnostic survey. * The Affina location for the Member Services call center had a CSR to Supervisor Ratio of 15 to 1 for the period of 03/01/02-12/30/02.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 66 ©2003 BearingPoint, Inc.
5.8 Length of New CSR Training Period vs. Annual CSR Turnover Rate
Exhibit 5.8.1 New CSR Training Period Annual CSR Turnover Rate
Federal Gov. Industry Ave. 98 30.00%
State Gov. Industry Ave. 186 35.00%
Healthcare Industry Ave. 237 24.00%
Call Center Industry Standard No call center industry standard for this metric. It is dependent upon the type of call center and the industry it serves.
25%
Overall KidCare Ave. 68 43.15%
Member Services (DHACS) 80 26.30%
KidCare Medicaid (DCF) 100 60.00%
Exhibit 5.8- New CSR Training Hours vs. Annual CSR Turnover Rate
10 08 06 82 3 718 69 8
2 4 .0 0 % 2 6 .3 0 %
3 5.0 0 %3 0 .0 0 %
4 3 .15%
6 0 .0 0 %
0
50
10 0
150
2 0 0
2 50
F ed eral Go v.Ind sut ry A ve.
St at e Go v. Ind ust ryA ve.
Healt hcare Ind ust ryA ve.
Overal l Kid C areA ve.
M emb er Services( D HA C S)
Kid C are M ed icaid( D C F )
New
CSR
Tra
inin
g H
ours
0 .0 0 %
10 .0 0 %
2 0 .0 0 %
3 0 .0 0 %
4 0 .0 0 %
50 .0 0 %
6 0 .0 0 %
70 .0 0 %
CSR
Tur
nove
r Rat
e

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 5 – KidCare Program Analysis
Page 67 ©2003 BearingPoint, Inc.
New CSR Training hours for the healthcare industry is often one of the highest of all industries
because of the need for CSRs to understand complicated and changing health policies. Thus,
the average education level and years of work experience also tends to be higher for healthcare
industry CSRs. As a result, the turnover rate of CSRs in this industry usually falls lower than the
industry standard because the CSRs become skilled workers.
The call center industry standard for CSR turnover rate is 25%. The average federal
government and state government call centers do not meet this industry standard. However,
the average healthcare industry call center does have a CSR turnover rate that is better than
the call center industry standard.
The average KidCare turnover rate (43.15%) falls below the call center industry standard
(25%) by 18.15%. This is mostly due to the KidCare Medicaid (DCF) call center turnover
rate of 60%.
The average amount of new CSR training for the KidCare program falls below the call center
industry average by 169 hours, or approximately 4 weeks.
Notes: * The data illustrated in Exhibit 5.8 is derived from the answers to questions D8 and D19 in the diagnostic survey. * The Enrollment Enhancement (ACS) and KidCare Outreach (ACS) call centers are not included in Exhibit 5.8 because they declined to provide turnover rate data in the diagnostic survey. Both centers reported 36 hours of new CSR training. * MediKids (ACS) is not included in Exhibit 5.8 because they declined to answer both training and turnover rate in the diagnostic assessment survey. * The Member Services (DHACS) turnover rate includes negative and positive turnover. Their statistics are not separated to distinguish between the two. * The KidCare Medicaid (DCF) training hour of 100 is an average based on their diagnostic answer of 80-120 total training hours in the diagnostic.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 68 ©2003 BearingPoint, Inc.
6.0 KidCare Program Recommendations
This chapter provides recommendations for increasing the customer service function of the KidCare
program as a whole through call center operations. Chapter Four identifies opportunities for
improvement for each specific call center analyzed during this project. In turn, this chapter is focused on
the inter-relationship of the call centers providing KidCare customer service and recommends changes
that affect all of the call centers.
The recommendations in this chapter are mutually exclusive and can be implemented stand-alone or in
conjunction with one another. The recommendations are as follows:
Recommendation 6.1: Create one set of call center performance metrics that all KidCare call
centers will use as a standard to meet.
Recommendation 6.2: Conduct monthly call calibration sessions at the All Call Center meetings.
Recommendation 6.3: Standardize call center names and transfer protocol when CSRs are
speaking to callers.
Recommendation 6.4: Implement a single phone number for KidCare Customer Service and link all
call centers off of the IVR menu.
Recommendation 6.5: Identify one single entity to administer all of the KidCare call centers.
Recommendation 6.6: Perform a phased consolidation of KidCare call centers so that one
contracted entity operates all of the call centers.
The following exhibits in this chapter provide details regarding each of the recommendations provided
above. Each exhibit includes:
Description of our observation of the current process
Detailed explanation of the recommendation
Potential timeline for implementation
Risks for not implementing the recommendation

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 69 ©2003 BearingPoint, Inc.
Recommendation 6.1 Create one set of call center performance metrics that all KidCare call centers will use as a
standard to meet.
Current Observation:
All of the call centers currently have different categories and standards of performance metrics they set for the objective of their call center service levels. However, there is no indication that the different metrics were derived from one set of ideal standards for the KidCare program. For example, some service levels written into the Member Services (DHACS) call center are as follows: 80% calls answered in 30 seconds, 90% average quality monitoring score, 5% or less abandonment rate, 98% voice mails answered within 24 hours. At the same time, the KidCare Medicaid (DCF) call center has two main call center performance standards, which are an overall abandonment rate of 15% or less and CSRs answering at least 60 calls a day. The KidCare call centers should all begin with one standard set of performance metrics for the entire program, and then adjust the metrics for each call center according to their environment and requirements.
Recommendation:
STEP 1: Use the monthly All Call Center Meeting to decide on KidCare call center performance standards, which should be based on call center industry best practices below. The Call Center Managers should decide if, based on the specific KidCare environment and budget, they should adjust any of the best practices to more reasonable for the different KidCare call centers.
Abandonment Rate: 5% or less
Service Level: X% of calls handled in Y seconds
CSR to Supervisor Ratio: 15 to 1
Average Time in Queue: No industry standard, should be based on industry environment
Average Call Handle Time: (CTT + ACW) see next two metrics
Average Call Talk Time should be based on industry environment
Average After Call Work Time should be based on industry environment
Quality Monitoring Score: 85%
STEP 2: All call centers should report these metrics to one contact person a week before the All Call Center Meetings. At the All Call Center meeting, there should be one summary chart that displays the results of the call centers. This chart should be the source of a discussion described in Step 3.
STEP 3: Each call center representative at the All Call Center Meeting should present their own results and discuss the reason(s) behind why data either deviates from the norm or falls below the set standard.
STEP 4: Other call centers should be able to discuss any recommendations for improving performance with the presenting call center.
STEP 5: All of these performance metrics goals should be written into Contractor contracts as performance requirements in order to ensure the performance metrics become program standard that are maintained by Contractors.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 70 ©2003 BearingPoint, Inc.
Recommendation 6.1 (cont.)
Create one set of call center performance metrics that all KidCare call centers will use as a standard to meet.
Potential Timeframe For Implementation:
1 Day: Standard performance measures are proposed and discussed. This should take place during one All Call Center Meeting.
2 Weeks: Representatives from the All Call Center meeting return to their call centers and propose the standards to their superiors and peers for discussion. They also propose any particular change to the standard based on their specific call center environment.
1 Day: Second meeting with call center representatives takes place to finalize and agree upon performance goals for individual call centers. Call centers should verify if different metrics for other call centers are justifiable.
2 Months: Implementation of standards at call centers may require change in staffing and technology.
Continuous: Discussion of individual call center performance goal results should occur at every subsequent All Call Center meeting.
Risk of Not Implementing Recommendation:
The ability to compare the performance of the call centers across the KidCare program will continue to be difficult due to inconsistent metrics.
Call centers that are under performing will not be forced to improve their performance.
Callers will continue to receive disparate levels of customer service from the call centers and will contribute this disparity to an overall low level of customer service from the KidCare program.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 71 ©2003 BearingPoint, Inc.
Recommendation 6.2 Conduct monthly call calibration sessions at the All Call Center meetings.
Current Observation:
Call Center Managers and Supervisors from the KidCare call centers are not aware of the call handling techniques of CSRs from the other KidCare call centers. There is currently no evidence of call center management visiting or regularly calling and conducting fake calls to other centers to assess their own CSR abilities. At most, the call centers will report disparate statistics at the All Call Center meeting in an attempt to measure their CSR performance, but as discussed in Recommendation 6.1, this process is not always effective. The KidCare call centers should listen to calls from each call center together to gauge CSR performance and to be made aware of levels and quality of customer service at each call center.
Recommendation:
STEP 1: Call Center Managers should agree on recording at least one quality monitored call a month.
STEP 2: Each month, the All Call Center meeting should listen to a taped call from 2 different call centers, rotating the centers that are listened to each month. The calibration session should comment on the following aspects of the call:
Politeness
Pace of conversation
Accuracy of information given
Accurately determining caller problem
Apologizing to caller when placing on hold
Hold time
Call time
STEP 3: The representatives should comment on any deficiency and strength areas they noted from the call.
STEP 4: The meeting representatives should use this calibration session as a source for understanding the type of calls other call centers are handling and translate this into educating their CSRs in order to improve the CSR’s knowledge of the other program services.
STEP 5: Quality monitors from the various KidCare call centers should be present during the All Call Center meeting that reviews their call center. Feedback from the participants of the meeting should serve to improve the quality of monitoring conducted at that call center.
ALTERNATIVE METHOD: If all call centers use an ACD system, it is possible to set-up a remote dial-in number in most ACDs that will select the next incoming call for blind monitoring. Currently, the KidCare Medicaid (DCF) call center does not have an ACD. If it were to install one at its call center, the monthly calibration meeting could simply dial into two call center ACDs for each meeting and listen to a randomly selected call from each center. However, if all call centers do not have an ACD this method is not recommended because it would give the non-ACD call center an unfair advantage by allowing them to record calls of their choosing for calibration.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 72 ©2003 BearingPoint, Inc.
Recommendation 6.2 (cont.)
Conduct monthly call calibration sessions at the All Call Center meetings.
Potential Timeframe For Implementation:
None to 6 Months: Some call centers are already able to record their monitored calls. Others do not have the current technology to record these calls and will have to purchase appropriate equipment.
Continuous: Calibration of calls should occur at every subsequent All Call Center meeting.
Risk of Not Implementing Recommendation:
The ability to compare the performance of the call centers across the KidCare program will continue to be difficult because the call centers do not regularly hear how other program CSRs perform.
Call center CSRs that are under performing will not be forced to improve their performance.
Callers will continue to receive disparate levels of customer service from the call centers and will contribute this disparity to an overall low level of customer service from the KidCare program.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 73 ©2003 BearingPoint, Inc.
Recommendation 6.3 Standardize call center names and transfer protocol when CSRs are speaking to callers.
Current Observation:
KidCare CSRs often transfer callers to other call centers because the caller needs information that the particular call center is not able to handle. Often, this is because callers do not understand what call centers they need to call for certain services. In other instances this is because CSRs are able to serve one part of the customer’s problem, but lack account access or information to serve another part of a customer problem. Currently, CSRs from different call centers will often use different names to describe other call centers. For example, site visits discovered that the Member Services call center was referred to as “Member Services”, “Accounts Department”, and “Healthy Kids” by different CSRs at different call centers. The rate of call transferring or referral is high and the inconsistency in referencing call centers leads to increased caller frustration and confusion.
Recommendation:
STEP 1: Create a standard name for each KidCare call center when a CSR is speaking to a caller. The list should include a one to two sentence description of the services of this call center that can be read to a caller.
STEP 2: Create a standard transfer and referral script for CSRs. The script should say the following for whenever a CSR refers or transfers a call:
Use the correct name of the center
Give the phone number of the center (even if they are transferring the call)
Give the hours of operation of the call center
Give a brief description of the call center’s services
STEP 3:The script should be approved by all call centers.
STEP 4: Implement the new script.
STEP 5: Proper call center referencing and transferring protocol should become an additional element on all quality monitoring scorecards.
Potential Timeframe For Implementation:
1 Week: Create standard call center names and descriptions
1 Week: Create a transfer and referral script for CSRs
2 Weeks: Approve new script by all call centers
Risk of Not Implementing Recommendation:
Callers may continue to be frustrated and confused due to inconsistent call center descriptions and names.
CSRs may continue to misunderstand the services offered by other call centers and relay that information to callers.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 74 ©2003 BearingPoint, Inc.
Recommendation 6.4 Implement a single phone number for KidCare Customer Service and link all call centers off of the IVR menu.
Current Observation:
Currently, individuals wanting to inquire about the KidCare program or their account information are required to call different phone numbers for different programs and services. Discussions with CSRs reveal that this is a consistent source of caller dissatisfaction and confusion. The result is that beneficiaries are not served as well as they could be due to the complexity created by multiple telephone numbers.
Recommendation:
STEP 1: Create one phone number for all KidCare related services and programs. This phone number should have a multi-tiered IVR that transfers callers to the appropriate call center.
STEP 2: Call centers should not continue to use separate telephone numbers once a single phone number is created. The existence of multiple ways to reach a call center will only lead to added confusion for the callers.
STEP 3: CSRs at call centers should be able to transfer callers to another call center so that the caller does not have to hang up and redial the same number only to choose another IVR option.
Potential Timeframe For Implementation:
6 months to 1 year: A single telephone number will be implemented and call centers will be integrated through telephony lines. Some call centers have networks that can easily integrate into another phone number. However, other call centers have less advanced networks and may require upgrades or implementation.
Risk of Not Implementing Recommendation:
Callers may continue to be frustrated due to multiple telephone numbers for different services.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 75 ©2003 BearingPoint, Inc.
Recommendation 6.5 Identify one single entity to administer all of the KidCare call centers.
Current Observation:
Currently each call center has different call center-wide performance metrics, resulting in greatly varying levels of customer service. One reason why this is occurring is because there is not consistency in the administration of the call centers by each Contract Manager and Call Center Manager. This situation is understandable, given that the Contract Manager and Call Center Manager work for different entities.
Recommendation:
Ultimately, the most effective way for the KidCare program to achieve consistent levels of customer service is to have one entity handle the management of all KidCare call centers. This recommendation does not require consolidation of the call centers. The benefits of single management will be realized as long as the entity consistently contracts and manages internal KidCare call centers. If a single entity is responsible for the customer service levels of the entire KidCare program, there will be more accountability for poor customer service performance.
STEP 1: Determine which existing partner in the KidCare program would be most appropriate to manage all of the call centers.
STEP 2: The entity will have to seek within the organization or hire personnel knowledgeable in call center management to oversee all of the call centers.
STEP 3: Use a phased approach to transfer all call centers under the management of one entity. Do not add a call center until the current phased-in centers are meeting performance standards and management is stabilized.
STEP 4: Single entity management of the call center requires monthly communication meetings with representatives of the different programs in order to stay abreast of program changes and issues.
*NOTE: Recommendation 6.5 is mutually exclusive from Recommendation 6.6 because it focuses on the management of the call center, whereas 6.6 is focused on the operations of the call center. However, 6.5 can also be implemented as an initial phase to Recommendation 6.6.
Potential Timeframe For Implementation:
2 months: Study to determine the best managing entity for KidCare customer service
2 months: Create transfer plan
2 years: Transfer call centers under one managing entity in a phased approach
Risk of Not Implementing Recommendation:
Customer service levels and operating procedures across KidCare call centers will continue to be disparate.
The challenge to standardize performance metrics with different administering and managing bodies at the call centers will still exist.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 76 ©2003 BearingPoint, Inc.
Recommendation 6.6 Perform a phased consolidation of KidCare call centers so that one contracted entity operates all of the call centers.
Current Observation:
There are currently three state agencies and one non-profit organization managing the KidCare call centers. This is a result of the fact that the different KidCare programs are administered through these different entities. However, not every call center handles services for only one of the programs. For example, the Member Services call center provides account status for many of the programs, but is administered by only one of the partners in the KidCare program. This example serves as evidence that a call center does not require a Contract Administrator to handle inquiries related to that particular program or entity. In addition, there are disparate call center data applications currently used to capture call notes and details from program participants and perform activities resulting from a call, such as KidCare application distribution.
Recommendation:
It is suggested that the KidCare program move toward a phased consolidation of call centers and data applications to be handled by a single Contractor. The rationale for recommending the outsourcing of call center functions is because the various KidCare entities do not have in-house call center expertise. Rather, management in the KidCare partner entities has expertise in the programs in which they administer. Call Center Contractors can provide physical call center site locations and the inherent expertise of managing call centers.
When each call center is mentioned below, it is intended to refer to the actual functions and data application of that particular center. Therefore, this recommendation does not make any assumptions as to who the Contractor or TPA will be upon implementation.
STEP 1: Procurement Process – determine the best contractor to operate the call centers
STEP 2: Consolidation Plan Development - Requires a detailed, multi-year consolidation plan that considers technology issues, such as multiple technology application and data integration, as well as network architecture development. This plan should be created by the new Contractor in conjunction with the existing Contractors/Contract Administrators of the call centers.
STEP 3: Consolidate the KidCare Outreach and Enrollment Enhancement call centers into the call center handling Member Services. The CSR knowledge required to handle these two call centers already exists in Member Services CSRs. The consolidation of these call centers into Member Services would only require process training, as opposed to knowledge training.
STEP 4: Consolidate the MediKids call center into either a joint call center with KidCare Medicaid, or into the call center created in Step 3. The services offered at the MediKids call center require the CSRs to be knowledgeable of the MediKids program and comfortable with providing HMO information. In addition, MediKids CSRs must enter HMO choices of MediKids participants; therefore, this level of service does require MediKids specific training and overall HMO familiarity. However, the MediKids CSRs will often refer callers to the Member Services call center for more detailed account information or inquiries. It is suggested that the services provided at the MediKids site be integrated into an advanced tier of CSRs at the Member Services call center that handle specific MediKids inquiries.
STEP 5: Consolidation of the KidCare Medicaid call center into either a joint call center with MediKids, or into the call center created in Step 3. The services offered at the KidCare Medicaid call center require the CSRs to be knowledgeable of the KidCare Medicaid program and familiar with DCF standards and procedures. Since this level of service requires specific training, it is suggested that the services provided at the KidCare Medicaid site be integrated into an advanced tier of CSRs at the Member Services call center that handle specific KidCare Medicaid inquiries.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 6 – KidCare Program Recommendations
Page 77 ©2003 BearingPoint, Inc.
Recommendation 6.6 (cont.)
Perform a phased consolidation of KidCare call centers so that one contracted entity operates all of the call centers.
Potential Timeframe for Implementation:
3 months: Complete the procurement process of determining the best Contractor to operate the consolidated call center
3 months: Create the consolidation plan
2 Years: Perform a phased consolidation of the KidCare call centers
Risk of Not Implementing Recommendation:
There will be continued disparity in customer service levels across KidCare call centers since call centers and data applications run separately.
The challenge to standardize performance metrics with different administering and managing bodies at the call centers will still exist.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 7 – Credit Card Payments Call Center Analysis and Recommendations
Page 78 ©2003 BearingPoint, Inc.
7.0 Credit Card Payments Call Center Analysis and Recommendations
This chapter contains the analysis performed and the recommendations developed for the Credit Card
Payment (FHK) Call Center. The related subsections are as follows:
7.1: Overview of Current Operations – describes general information regarding the call center’s
current operations
7.2: Historical Transaction Volume – illustrates the growth in transactions and dollars assessed
since program inception
7.3: Overall Recommendation – describes the overall recommendation made to the Credit Card
Payments (FHK) call center given the analysis performed
7.4: Considerations – describes some considerations that must be addressed given the
recommendation found in Section 7.3
7.1 Overview of Current Operations
The Credit Card Payments (FHK) call center processes credit card payments for program
members paying premiums. In addition, it also processes credits for families if insurance
coverage was purchased for future months and the child becomes disenrolled in a KidCare
program, thus, not able to use the purchased coverage. The call center is open from 8:00 am –
4:30 pm, Monday – Friday, with the exception of all file run days. Callers dial the Florida Healthy
Kids Corporation toll-free phone number, 1-888-352-5437, and follow IVR instructions to make a
credit card payment over the phone. This is currently the only access point for the call center.
Although this call center began as a pilot, it has become an important aspect of KidCare
customer service and is often referred to customers by CSRs from other call centers.
The volume of calls to the credit card payment call center is steady throughout the month. Some
families prefer to use the credit card payment line and do so on a regular basis. For Healthy
Kids, MediKids and CMSN, late payment letters are distributed to families on the 7th day of the
month and cancellation letters are distributed on the 20th or 21st of the month. When families
receive these letters, they often call Member Services (DHACS) regarding their accounts and
are subsequently referred to the credit card payment line to make immediate credit card
payments to remain active in the corresponding program. Although monthly data shows steady

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 7 – Credit Card Payments Call Center Analysis and Recommendations
Page 79 ©2003 BearingPoint, Inc.
call volume, there is evidence of call spikes the last two days of the month that may be attributed
to cancellation letters.
This call center is staffed as follows:
1 Call Center Manager
1 Call Center Supervisor
4 CSRs
The CSR’s primary responsibility is to take credit card payment information from callers over the
phone. This call center is using staff from the Healthy Kids Research Unit for this pilot. The
Research Unit CSRs still have all of their previous responsibilities, despite having only 10% of
the time to complete them. Thus, important processes, such as custody and citizenship issues,
various research items and address verifications are often delayed for weeks due to the dual
responsibility of the CSRs.
Due to the fact that the Credit Card Payments (FHK) call center began as a pilot, many standard
call center operational areas are not a part of the call center. Exhibit 7.1 describes operational
functions that are not performed at this call center.
Exhibit 7.1 - Credit Card Payments (FHK) Call Center - Missing Operational Functions
Training Formal Training Course - New CSRs receive one week of Florida Healthy Kids organization training. For specific call center training, CSRs are initially debriefed by the Supervisor and shadow other CSRs until they are ready to independently answer calls.
Performance Standards
CSR Performance Standard Facilitators
No Script Development or Usage
No Performance Metrics
No CSR Rewards Program
Quality Monitoring
The closest element to quality monitoring currently is having the Supervisor sit in a cube located in the middle of the 4 CSRs.
Workforce Management
No Forecasting of Call Volume
No Scheduling of CSRs based upon call volume and fluctuations

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 7 – Credit Card Payments Call Center Analysis and Recommendations
Page 80 ©2003 BearingPoint, Inc.
The credit card payment call center uses TermNet, an online credit card payment tool, and a
reporting application through TermNet, called Skip Jack. In addition, Language Line is available
to CSRs when they need assistance with foreign language callers. There are two CSRs who are
currently bilingual in Spanish and English.
7.2 Historical Transaction Volume
The Credit Card Payments (FHK) call center began in February 2002 as a pilot for the KidCare
program to accept credit card payments for its members. In the first month of the pilot, the call
center processed 756 transactions, including 68 declined attempts, and processed
approximately $28,760 in premiums. As illustrated in Exhibit 7.2 below, the number of monthly
transactions has increased 860% to approximately 6,541 transactions and $195,505 in
payments in September 2002.
Exhibit 7.2 - Credit Card Payments (FHK) Call Center Transactions
Month Total
Transactions Declined
Transactions
Percent of Declined
Transactions
Total Transaction
Amount
Month over Month Growth
Rate
February 756 68 9.0% $ 28,761.09 -
March 1,452 110 7.6% $ 50,926.51 92%
April 1,907 160 8.4% $ 62,379.10 31%
May 2,627 169 6.4% $ 87,822.50 38%
June 4,000 259 6.5% $ 126,298.00 52%
July 4,804 301 6.3% $ 148,411.99 20%
August 5,584 334 6.0% $ 167,682.50 16%
September 6,541 385 5.9% $ 195,505.00 17%
Total 27,671 1,786 6.5% $ 867,786.69

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 7 – Credit Card Payments Call Center Analysis and Recommendations
Page 81 ©2003 BearingPoint, Inc.
7.3 Overall Recommendation
The significant growth in use of the credit card payment line is proof that there is a purpose and
need for this process. It is recommended the credit card payment call center be fully automated
into a stand-alone touchtone payment line.
When the Member Services call center is mentioned below, it is intended to refer to the actual
functions of that particular center. Therefore, this recommendation does not make any
assumptions as to who the contractor or TPA will be when this recommendation is implemented.
This recommendation is based on the following reasons:
The growth in popularity of this call center service either demands more CSRs or
automation.
The industry that provides technology for automated credit card services is mature enough
to offer mid-sized organizations a scalable and affordable solution.
Automated telephone credit card payments are common processes, which most individuals
have used before and feel comfortable using.
Automated telephone credit card payments reduce the chance of identity fraud because they
do not involve the use of live CSRs to input payment data.
Current Research Unit staff should be able to return to their prior job responsibilities because
their research work is of high importance in facilitating access to the KidCare services for
families.
7.4 Considerations
In choosing to implement an automated system, the following considerations must be
addressed:
Forecast Future Call Volume Growth – The future volumes of calls must be forecasted to
ensure the appropriate technology is purchased. Based on the growth rate of this call
center, the system should be robust and able to accommodate an increasing number of
calls.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 7 – Credit Card Payments Call Center Analysis and Recommendations
Page 82 ©2003 BearingPoint, Inc.
Administration Determination – The KidCare administrator for this system must be
determined. It is recommended that since this process is currently administered by the
Florida Healthy Kids Corporation, it should remain in this arena under the supervision of
Member Services since the payments processing function is housed here.
Conduct Industry Research - Industry research should be conducted to determine the first
time completion rate for automated credit card transactions. This research will determine if a
Stand-Alone system is sufficient or if CSRs are needed to back up the automated function:
Stand-Alone System: If the industry success rate is high, additional CSRs will not be
needed to provide assistance to callers since the system would complete credit card
payments in most instances. In the situation where transactions are declined, members
would be required to send payment by check in the traditional payment format. This
research is suggested because the automated line must assess if it is worth retraining
Member Services CSRs to handle these payments. It must also consider the added
expenses associated with giving callers the option to reach a CSR through the
automated line. Based on the information in Exhibit 7.2, the declined transactions rate
for the current credit card payments system currently is 6.5%, which leads to the
assumption that the industry research will show a high success rate.
CSR Back Up: If research determines that a high percentage of automated credit card
transaction lines incur first time problems, CSR backup may be necessary. CSR backup
would take form in allowing an option to access a live agent if the caller is having
problems completing their transaction. The CSRs would then complete the transaction
by asking for the credit card or check information; much in the same manner that is
currently being performed. CSRs will require training to handle this sensitive information
and will need to be quality monitored on a regular basis. In addition, CSRs should have
background checks and some form of a work bond/insurance because of the sensitivity
level of credit card payments. If CSRs are needed for back up, they should be housed
in the Member Services call center so they can access account information in addition to
the credit card payment system. One option is for existing Member Services CSRs to be
trained in this capability since they are already trained in accessing and dealing with
account issues.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 7 – Credit Card Payments Call Center Analysis and Recommendations
Page 83 ©2003 BearingPoint, Inc.
Determine Call Center Processes – If industry research predicts high success rates in
automation, there will not be a need to be a live CSR assistance option for the credit card
payment line. Instead, callers will simply call the automated payment line and enter their
credit card account information through the touch pad on the phone. Since there will not be
the possibility for CSR interaction, associated process changes will be minimal. However, if
CSRs are needed for back up in the instance when credit cards are declined, Member
Services will be required to develop a CSR script and will need to perform training sessions
for that script and overall program requirements. In addition, quality monitoring will have to
be performed, as well as additional report generation.
Change KidCare Policy – The impact on KidCare policy changes should be assessed. If the
KidCare program purchases the technology to perform these payment tasks, KidCare policy
may be changed to increase the amount of families paying premium payments via credit
card.
Encourage Automated Payment Education – All KidCare CSRs must be instructed to
educate callers about the credit card payment process. Again, if the technology is going to
be purchased and used for automation of credit card payments, members should be
encouraged to use this service. All KidCare CSRs should be trained to distribute information
verbally to callers over the phone informing them of this service, such as the appropriate
referral process. In addition, marketing this process to the public to increase awareness
may be considered.
Check By Phone Functionality – The idea of also accepting automated check by phone
payments can be addressed and decided upon. This expansion of payment capabilities
would mean members would call one telephone line to make automated credit card or check
payments. If it is decided that members will be able to pay for KidCare coverage via check
by phone, in addition to the current form of credit card payment, members should be made
aware of this enhancement via CSRs and developed scripts, as well as outreach materials.
To assess the added value of this service, industry research should be done to assess the
number of KidCare families that would use this service if the check by phone functionality
were made available.
Web Credit Card Payment – It was noted that many callers inquire about paying for KidCare
coverage over the Internet. An option for future advancement is to consider moving to an
online self-pay venue once the telephone self-pay functionality is being used smoothly. To

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Chapter 7 – Credit Card Payments Call Center Analysis and Recommendations
Page 84 ©2003 BearingPoint, Inc.
accommodate this function, the general KidCare website could contain a link to make
payments over the Internet and would allow KidCare program members to pay for insurance
through self-service, thus, providing CSRs with more time to dedicate to other job
responsibilities.
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
1
A. Diagnostic Tool Sample BearingPoint CRM Solutions Group Call Center Diagnostic Tool
The information provided below will be used for benchmarking purposes only and will not be disclosed or
available for distribution outside of BearingPoint. BearingPoint agrees not to disclose identifying information of
any participating organization, without prior approval. BearingPoint will not audit or verify the data that is
submitted (except when expressly requested by participant) and therefore will not express any opinion as to the
validity of the participant’s response. It is the sole responsibility of each participant to ensure that the data
provided is accurate and reliable to the best of their knowledge.
Instructions: Please provide responses for the information requested in the following pages. When necessary,
make duplicate copies to provide information for multiple departments or locations. A glossary of acronyms is
included at the end of the document. Attach diagrams or other materials as necessary to illustrate. If there is a statistical/data request in this document that is not applicable or tracked by your center, please indicate it.
SECTION A. PARTICIPANT INFORMATION......................................................................................2 SECTION B. GENERAL OPERATIONAL INFORMATION .................................................................4 SECTION C. CALL STATISTICS .........................................................................................................5 SECTION D. PEOPLE ..........................................................................................................................6 SECTION E. PROCESS .....................................................................................................................10 SECTION F. TECHNOLOGY..............................................................................................................11 SECTION G. STRATEGY...................................................................................................................19 SECTION H. CUSTOMER ..................................................................................................................20 SECTION I. REQUEST FOR INFORMATION....................................................................................21 SECTION J. GLOSSARY ...................................................................................................................22
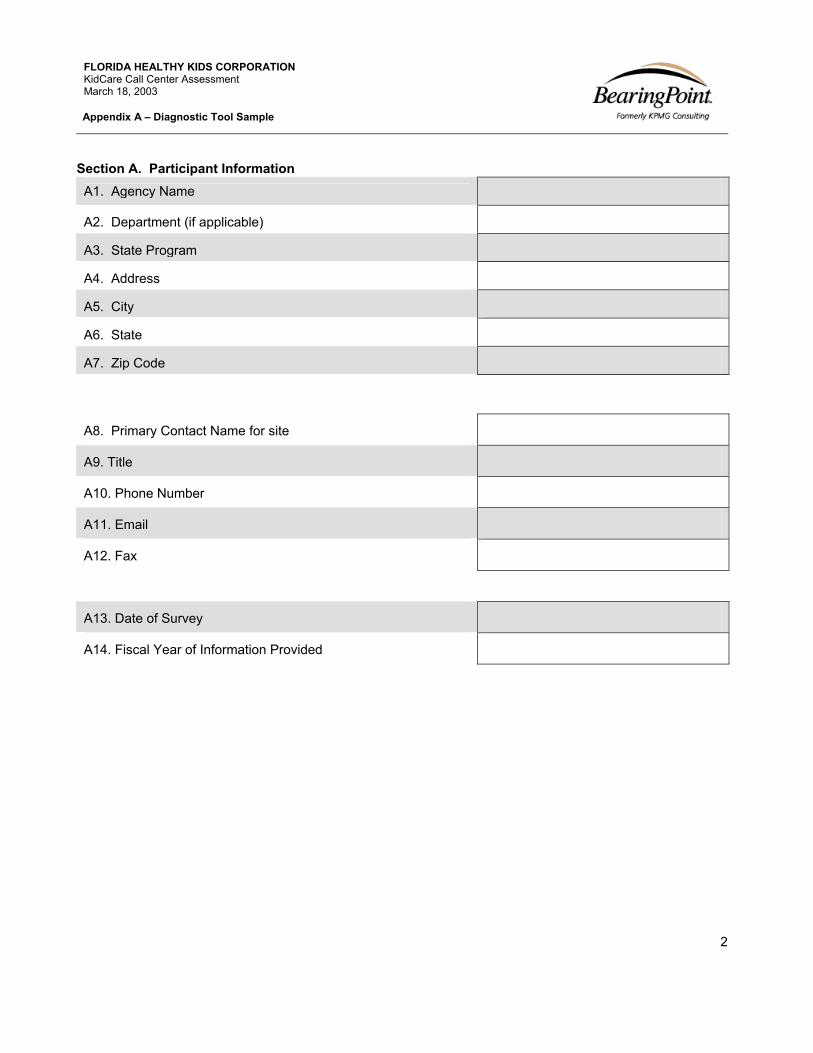
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
2
Section A. Participant Information A1. Agency Name
A2. Department (if applicable)
A3. State Program
A4. Address
A5. City
A6. State
A7. Zip Code
A8. Primary Contact Name for site
A9. Title
A10. Phone Number
A11. Email
A12. Fax
A13. Date of Survey
A14. Fiscal Year of Information Provided

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
3
A15. Name of Subcontractors (if applicable)
A16. Number of customer served by your site (annual)
A17. Number of customers served by Subcontractor (annual)
A18. Primary Contact Name for Subcontractor
A19. Subcontractor Contact Title
A20. Subcontractor Phone Number
A21. Subcontractor Email
A22. Subcontractor Fax
A23. What are your funding sources?
A. Federal
B. State
C. Local
D. Private Sector
E. Non-Profit

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
4
Section B. General Operational Information Please provide information regarding the specific client listed above, unless otherwise noted.
B1. Hours of operation
B2. Total Number of CSRs
B3. What type of calls does your call center handle ? (Please
check all boxes that apply)
Inbound Outbound Blended
B4. Total inbound call volume offered last year
B5. Forecasted inbound call volume offered this year
B6. Total inbound call volume handled last year
B7. Forecasted inbound call volume handled this year
B8. Total outbound call volume last year
B9. Forecasted outbound call volume current year
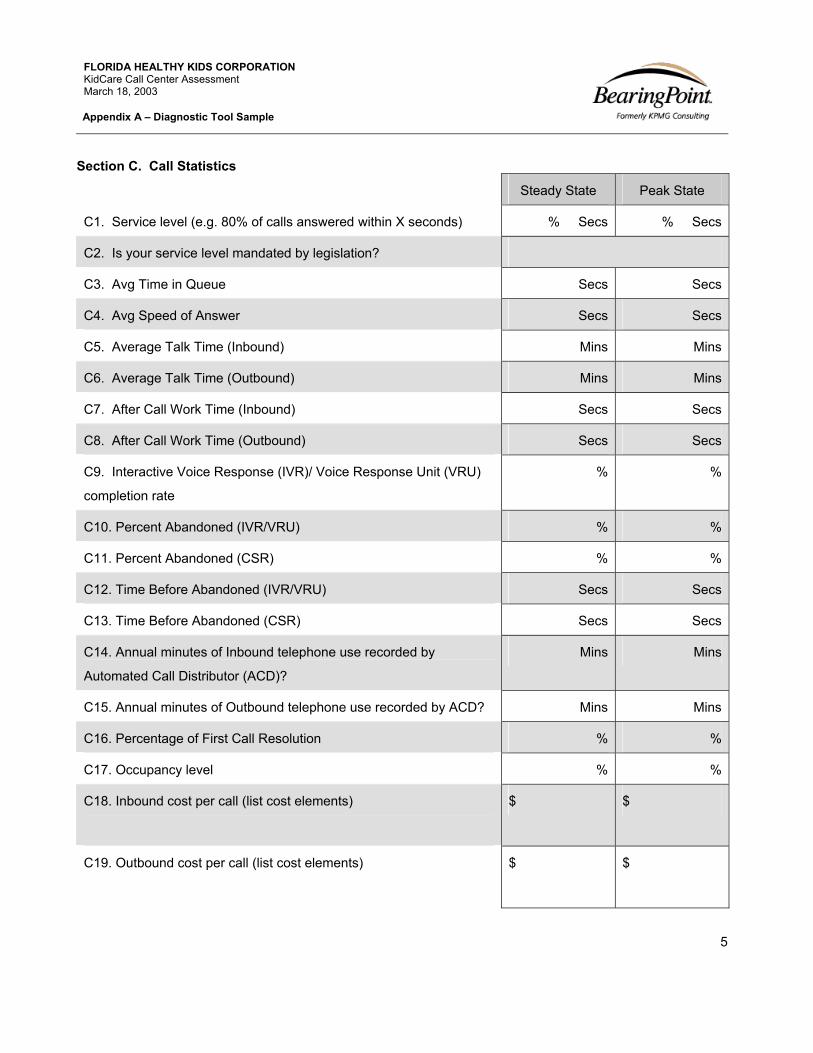
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
5
Section C. Call Statistics
Steady State Peak State
C1. Service level (e.g. 80% of calls answered within X seconds) % Secs % Secs
C2. Is your service level mandated by legislation?
C3. Avg Time in Queue Secs Secs
C4. Avg Speed of Answer Secs Secs
C5. Average Talk Time (Inbound) Mins Mins
C6. Average Talk Time (Outbound) Mins Mins
C7. After Call Work Time (Inbound) Secs Secs
C8. After Call Work Time (Outbound) Secs Secs
C9. Interactive Voice Response (IVR)/ Voice Response Unit (VRU)
completion rate
% %
C10. Percent Abandoned (IVR/VRU) % %
C11. Percent Abandoned (CSR) % %
C12. Time Before Abandoned (IVR/VRU) Secs Secs
C13. Time Before Abandoned (CSR) Secs Secs
C14. Annual minutes of Inbound telephone use recorded by
Automated Call Distributor (ACD)?
Mins Mins
C15. Annual minutes of Outbound telephone use recorded by ACD? Mins Mins
C16. Percentage of First Call Resolution % %
C17. Occupancy level % %
C18. Inbound cost per call (list cost elements)
$ $
C19. Outbound cost per call (list cost elements)
$ $

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
6
Section D. People Statistics Answer
D1. What is the number of CSR FTEs in this department?
D2. What is the number of Supervisors in this department?
D3. What is the number of Managers in this department?
D4. What is the cost of a new CSR hire in this department?
D5. Are your CSRs represented by a labor union? Yes No
Human Resources Answer
D6. What was your unplanned/negative CSR turnover* last
month?
D7. What is your quarterly unplanned/negative CSR turnover
rate?
D8. What is your annual unplanned/negative CSR turnover
rate?*
D9. What is your monthly CSR attendance rate?
D10. Are CSRs hourly or salaried employees?
D11. What is the average hourly rate for CSRs? (convert salary)
D12. What is the average annual salary for Supervisors?
D13. What is the average annual salary for Managers?
D14. Are aptitude tests or civil service exams used to screen
CSR applicants?
Yes No
D15. How many of your staff are dedicated to call answering as
their only job responsibility?
D16. How many of your staff answer calls, but are responsible for
other job functions as well?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
7
CSR Functions (Please check all that apply) Answer
D17. What functions are your CSRs responsible for?
A. Routing Calls B. Complaint Resolution C. Consumer Affairs D. Customer Service E. Dispatching F. Account Inquiries G. Order taking H. Information Requests I. Public Relations J. Reservations K. Technical Support L. Collections M. Customer Satisfaction Surveys N. Outbound Telemarketing O. Follow-up to Inbound Calls P. Market Research Q. Other (please specify)
D18. Which of the following activities do CSRs perform?
A. Inbound Calls B. Outbound Calls C. Email D. Text Chat E. Research F. Fax Response G. Others (Please Specify)

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
8
Training Answer
D19. How many hours of initial training do CSRs receive?
D20. Does initial CSR training include call simulation?
D21. How many hours per month of refresher training do CSRs
receive?
D22. How many hours of cross-functional skill training do CSRs
receive? (i.e. call handling, transcription, content skills, etc.)
D23. How many hours of soft skill training do
Supervisors/Managers receive each year? (mentoring, coaching,
communication, etc)
D24. How many hours of advanced training do
Supervisors/Managers receive each year? (new technology,
management strategy, industry trends, forecasting, etc)
D25. If Email is available, do you use dedicated staff to respond? Yes No
D26. Do CSRs receive specific training on responding to Email?
D27. Are new employees mentored by experienced CSRs?
Performance Measurement Answer
D28. Are CSR performance reviews tied to KPIs?
D29. Have performance measurement standards been
developed and communicated to CSRs?
D30. Is call monitoring part of performance reviews?
D31. How frequently are new CSRs monitored?
D32. How frequently are experienced CSRs monitored?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
9
Job Satisfaction Answer
D33. Do you conduct CSR job satisfaction surveys? Yes No
D34. What percent of CSRs rate their jobs as satisfactory or
better?
D35. Do you conduct Supervisor/Manager job satisfaction
surveys?
Yes No
D36. What percent of Supervisors/Managers rate their jobs as
satisfactory or better?
D37. Do you have an employee feedback process? Yes No
D38. If yes, what processes are in place to implement employee
feedback?
Career Path Answer
D39. How many CSR skill levels do you have?
D40. Do opportunities for upward mobility exist for CSRs?
D41. Do opportunities for horizontal departmental transfers exist
for CSRs?
D42. What is your positive CSR turnover rate? Positive turnover
includes lateral or upward movement within the call center.
*Note: “Positive Turnover” includes lateral or upward movement within the call center.

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
10
Section E. Process
Answer
E1. What is the turnaround time for responding to Email?
E2. Is there a process to match inquiry type and customer to
CSR expertise?
E3. Are there standardized call handling procedures to service
routine calls?
E4. Are there standardized call handling procedures to service
exception calls?
E5. Is there a defined escalation process for escalating calls to
expert resources?
E6. Are there formalized procedures for customer follow-up?
E7. Are standard quantitative measures used to assess agent
performance?
E8. Are standard qualitative measures used to assess agent
performance?
E9. Are call monitoring standards used to assess agent
performance?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
11
Section F. Technology
Which of the following technologies are currently utilized in the
call center?
Answer
A. Integrated private branch exchange (PBX) B. Automated call distributor (ACD) C. Stand-alone ACD D. Network based ACD E. Interactive voice response (IVR) or voice response unit (VRU)
F. Voice over IP G. Computer telephony integration (CTI) H. Predictive Dialing I. Dynamic inbound/outbound calling J. Staff forecasting planning tools K. CSR monitoring/recording system L. Fax response/server M. Voice messaging for external callers N. Voice messaging for internal callers O. Speech recognition P. Remote agents/telecommuting Q. Client-server/database access R. Mainframe database access S. Workstations running Windows T. Mainframe terminals U. Desktop call tracking/management system V. Customer Relationship Management (CRM) tool W. Imaging systems (scanners, etc.) X. Customer call history database Y. Multimedia system (CSR workstations equipped with CD-ROM or video capabilities).

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
12
ACD/PBX Answer
F2. Who are the ACD or PBX manufacturers?
F3. What software release is being used on the ACD/PBX?
F4. Does the ACD/PBX provide enterprise/automated reporting?
F5. Does the ACD/PBX provide real-time management
information?
F6. Does the ACD/PBX provide call routing/virtualization?
IVR Answer
F7. Do you use an IVR/VRU?
F8. Who is the IVR/VRU manufacturer?
F9. What software release is being used on the IVR/VRU?
F10. Do you use speech recognition technology?
F11. If so, is standard or natural language speech recognition
technology being utilized?
F12. Is the IVR available 24/7/365?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
13
CTI
F13. What level of CTI functionality is currently utilized in the call
center?
Answer
A. Inbound screen pop by automatic number identification (ANI)
B. Inbound screen pop by VRU input C. Consultation/conference D. Intelligent routing E. ACD and workstation integrated logon F. Telephony functions on workstation G. Abandoned call ANI capture for callback H. Coordinated call/screen transfer between CSC/CSRs I. Integrated call/database reporting J. Integrated CSR status control K. Integrated messaging L. Call recording M. Predictive dialing N. Integrated messaging

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
14
Desktop Answer
F14. Do you use a scripted/expert desktop system?
F15. Is the desktop system customized or an off-the-shelf tool?
F16. Is your desktop tool Web based?
F17. Is there a CTI interface with the desktop?
F18. Is the desktop integrated with the reporting system?
F19. Are call center statistics available on the desktop?
F20. Is there a softphone on the desktop?
F21. Is there online training on the desktop?
F22. Is Email integrated into the desktop?
F23. Is online reference material available on the desktop?
F24. Are screen pops available on the desktop?
F25. Is the desktop available remotely to CSRs and/or client?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
15
CRM Answer
F26. Are you using a CRM tool in your call center?
F27. Are you using a customized or off-the-shelf CRM tool?
F28. Are you using CRM for campaign or marketing purposes?
F29. Are you using CRM for order entry/status?
F30. Does the CRM tool allow for real time updates?
F31. Does the CRM tool contain error-handling features?
F32. Does the CRM tool allow CTI integration to the call center
telephone and computer platforms?
F33. Does the CRM tool provide an on-line knowledge base that
is accessible real-time to all CSRs?
F34. Does the CRM tool provide tracking of customer orders?
F35. Does the CRM tool provide tracking of product inventory?
F36. Does the CRM tool provide escalation management tools?
F37. Does the CRM tool provide correspondence and literature
fulfillment?
F38. Does the CRM tool provide customer profile capabilities?
F39. Does the CRM tool provide customer history logging?
F40. Does the CRM tool provide the ability to log in multiple calls
for the same service/information request?
F41. Does the CRM tool provide “information push” to
customers?
F42. Does the CRM tool track customer interaction across all
contact channels?
F43. Does the CRM tool keep multiple contacts per customer and
identify type of contact?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
16
F44. Does the CRM track agent feedback?
F45. Does the CRM tool have customer search capabilities?
F46. Does the CRM tool have the ability to communicate with
customer via Internet-based e-mail?
F47. Does the CRM tool allow remote connectivity?
Quality Assurance Answer
F48. Are you using an automated Quality Assurance (QA)
recording tool?
F49. Does the QA tool allow recording to be scheduled for
specific CSRs?
F50. Does the QA tool allow online scoring?
F51. Is there a CTI link to the QA tool?
F52. Does the QA tool allow screen captures?
F53. Does the QA tool allow CSRs to initiate recording?
F54. Does the QA tool allow recording on command?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
17
Scheduling and Forecasting Answer
F55. Do you use a forecasting/scheduling application?
F56. Does the application provide simulation tools?
F57. Is the application browser based?
F58. Does the application integrate with the ACD/PBX platform?
F59. Does the application integrate with the IVR platform?
F60. Does the application integrate with your Email server?
F61. Does the application integrate with the CSR desktop?
F62. Does the application provide schedule adherence data?
F63. Does the application allow manager overrides?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
18
Other Communication Channels (Please check all that apply)
F64. What other communication channels do you offer callers? Answer
A. Website B. Email C. Fax D. Kiosk E. In-person F. Mail G. Internet Chat H. Callback messaging I. Voicemail J. Other (Please Specify)
F65. How many web interactions are handled each year?
F66. What features and services does your website offer?
A. Email B. Internet Chat C. Voice Over IP (VOIP) D. Call Center 800 number E. Frequently Asked Questions F. Complaint resolution G. Service scheduling H. Order taking and tracking I. Publication downloading and printing J. Other (please specify)
F67. Is the data provided in one communication channel provided
to all other channels?
Yes No
F68. Do you use standardized or pre-composed responses to
Email?
F69. Do you send an automatic response to acknowledge receipt
of an Email inquiry?
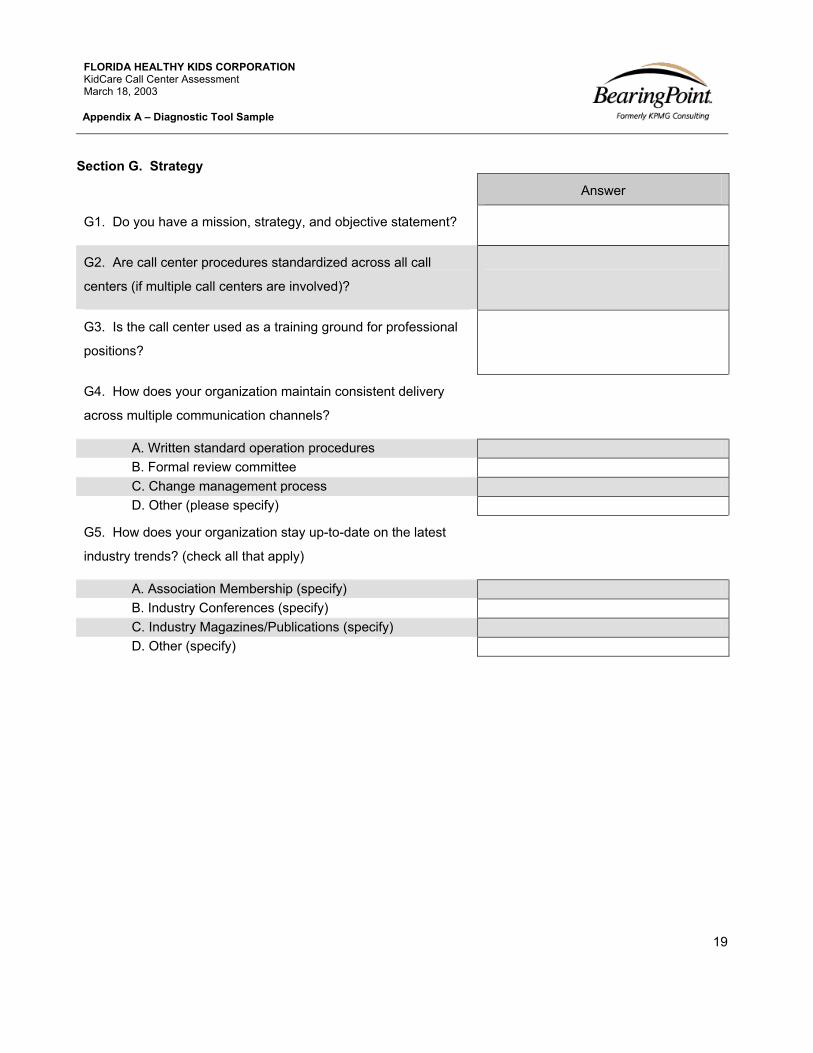
FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
19
Section G. Strategy
Answer
G1. Do you have a mission, strategy, and objective statement?
G2. Are call center procedures standardized across all call
centers (if multiple call centers are involved)?
G3. Is the call center used as a training ground for professional
positions?
G4. How does your organization maintain consistent delivery
across multiple communication channels?
A. Written standard operation procedures B. Formal review committee C. Change management process D. Other (please specify)
G5. How does your organization stay up-to-date on the latest
industry trends? (check all that apply)
A. Association Membership (specify) B. Industry Conferences (specify) C. Industry Magazines/Publications (specify) D. Other (specify)

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
20
Section H. Customer Answer
H1. Do you measure customer satisfaction? Yes No
H2. If Yes, how many surveys do you attempt annually?
H3. How many surveys are completed annually?
H4. What percentage of your callers are surveyed?
H5. What method do you use to survey customers?
A. Post-call B. Return call phone survey C. Mail D. Postcard E. Email F. Others (Please specify)
H6. What method do you use to determine survey sample size?
H7. What method do you use to identify survey participants?
H8. Does your company or a third-party conduct surveys?
H9. If your company conducts surveys, does the same CSR who
provided service conduct the survey?
H10. What percentage of surveys result in a perfect score?
H11. Does your company conduct customer focus groups?
H12. Is customer profile and history maintained in a single
database accessible by CSRs?

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
21
Section I. Request for Information Please mail the following information to the contact person indicated on the front page of this diagnostic: Please check if data provided:
I1. Performance reports and the related performance metrics that
they are matched against
I2. Technical Infrastructure description/ overview map
I3. Call flows/ vector maps
I4. Example of scripts and/or reference books used to answer
caller questions
I5. List of call center staff (Directors, Managers, Supervisors,
CSRs, etc.)
I6. Copies of any customer service survey results conducted by
yourself or a third party
I7. Example of training materials for Managers and/or CSRs
I8. Example of a daily and weekly work flow management print
out
I9. The template/scoring form used for quality monitoring

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix A – Diagnostic Tool Sample
22
Section J. Glossary ACD - Automated Call Distributor
ANI - Automatic Number Identification
CPI -Consumer Price Index
CRM - Customer Relationship Management
CSC - Customer Service Center
CSR(s)- Customer Service Representative(s)
CTI - Computer Telephony Integration
FTE- Full Time Equivalent
GSA - Schedule- Government Services Administration
IVR - Interactive Voice Response
KPI - Key Performance Indicator
OLAP- Online Analytical Processing
Peak State Calls - Description of time period where call center experiences a distinct peak in call volume,
sometimes referred to as “spike time”
PBX - Private Branch Exchange
QA - Quality Assurance
SOP - Standard Operating Procedures
Steady State Calls - Description of time period where call center experiences call volume outside of Peak State
VRU - Voice Response Unit

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix B – Benchmarking Data Sources
23
B. Benchmarking Data Sources Best Practices BearingPoint Global Best Practices
COPC-2002 Standard Report (http://www.copc.com)
ICMI- Call Center Management Review (http://www.incoming.com/s1ccmr.html)
Callcenterbiz.com (http://www.callcenterbiz.com)
Customer Interaction Solutions Magazine
Gartner Professional Business Research (http://www4.gartner.com)
Incoming Call Center Management (ICCM) Institute 2001 Conference Materials
Benchmarking Industry Averages and Standards Purdue University Public Sector Benchmarking Survey
Purdue University Private Sector Benchmarking Database
Benchmarkportal.com (http://www.benchmarkportal.com)

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix C – Call Center Glossary
24
C. Call Center Glossary
Abandoned Calls - Also called lost calls, calls where the caller hangs up before reaching a live agent. This
value is often expressed in the form of percentage of total offered calls that were abandoned by callers,
abandonment rate.
Automatic Call Distributor (ACD) - Specialized telephone system used in incoming call centers to answer
calls, queue calls, distribute calls and plays delay announcements.
After Call Work (ACW) - Work performed by CSRs that is related to calls. May include updating account
records based on call or filling out manual applications and forms.
Customer Service Representative (CSR) - The agents that handle incoming and outgoing calls at a call
center.
Call Talk Time (CTT) - The total amount of time a CSR spends on the phone handling a live call. This is a
description for both incoming and outgoing calls.
Erlang C - Equation used for workforce management that calculates predicted waiting times. For a more
detailed explanation, please refer to the workforce management discussion in Chapter 3.
Handle Time - A sum of call talk time (CTT) plus after call work (ACW) time. This is the total amount of time
it takes to service and complete work related to a call.
Handled Calls - Calls that are handled by either a CSR or Intelligent IVR. It can be further broken into the
categories of CSR Handled Calls or IVR Handled Calls.
Interactive Voice Response (IVR) - An IVR responds to caller-entered digits or speech recognition and
serves as the opening dialogue with a caller. Callers may choose menu options or opt to speak with a live
CSR, if CSRs are linked to the menu.
Offered Calls - All calls made to a call center that either reach the IVR menu or are answered by a CSR.
The total of abandoned call, CSR handled calls and IVR handled calls should be offered calls.
Predictive Dialing - Technology that assists in the placing of outbound calls and delivers answered calls to
agents. For a more detailed discussion of predictive dialing technology please refer to the workforce
management section of Chapter 3.
Quality Monitoring (QM) - Quality monitoring is usually related to the monitoring of CSRs on real calls. Call
center management, or a dedicated quality monitoring department, will rate CSRs on their performance

FLORIDA HEALTHY KIDS CORPORATION KidCare Call Center Assessment March 18, 2003
Appendix C – Call Center Glossary
25
based on a scorecard that lists customer service elements. For a more detailed discussion of quality
monitoring please refer to the Quality Monitoring section of Chapter 3.
Workforce Management (WFM) - The call center process of forecasting call loads, calculating staff
requirements, organizing schedules, and tracking real time performance of individuals and groups.