keratoconus and related non- inflammatory thinning disorders timothy t. mcmahon, od department of...
TRANSCRIPT

Keratoconus and Related Non-Inflammatory Thinning Disorders
Timothy T. McMahon, OD
Department of Ophthalmology and Visual Sciences
University of Illinois at Chicago

Non-Inflammatory Thinning Disorders
Keratoconus Pellucid Marginal Degeneration Posterior Keratoconus Keratoglobus Terrien’s Marginal Degeneration Senile Marginal Furrowing
Keratoconus
Non-inflammatory Central and Paracentral Thinning Steepening, Principally Central and Inferior M>F, (60% M) Prevalence - Approx. 230/100,000 96% Bilateral Types: Nipple, Oval, Globoid

Demographics: Prevalence
Range: 4 to 600 per 100,000 Most Common: 230/100,000

Demographics: Gender
% Female Range 22-56% Mean % Female 38.7% 6255 Patients (2423 Females) 10 Studies M:F Ratio 1.58:1

Demographics: Bilaterality
Prior to Topography: 85.% Bilateral After Topography: 96% Bilateral
Demographics: Race
No Racial Predilection

Demographics: Age
Age <20 20-29 30-39 40-49 50-59 60-69 >70
Percent of Sample
4
26
33
25
8
3
1
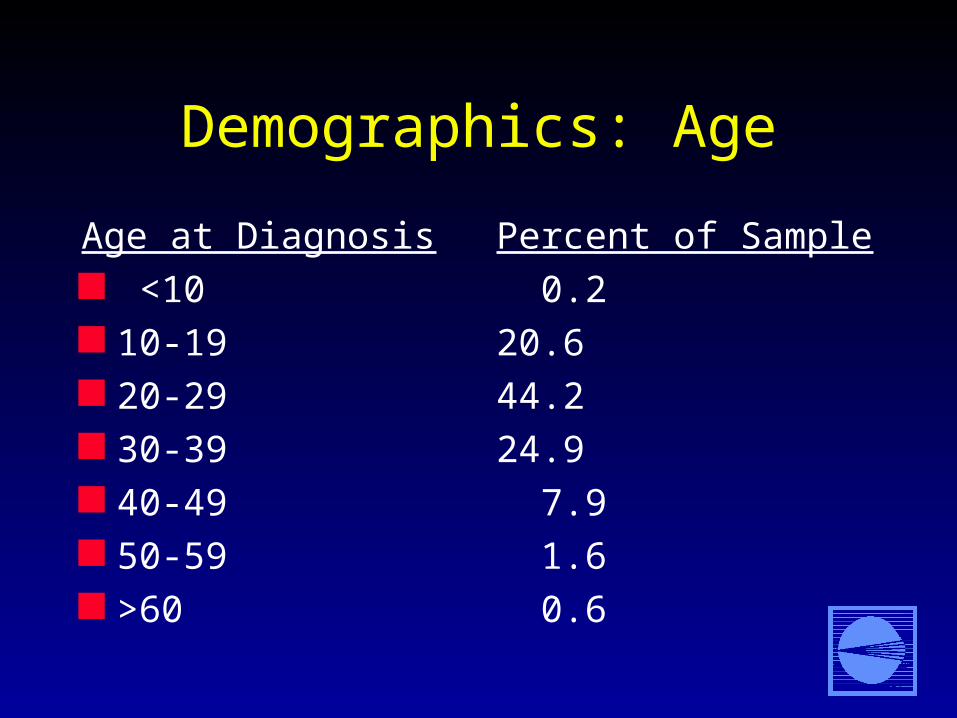
Demographics: Age
Age at Diagnosis <10 10-19 20-29 30-39 40-49 50-59 >60
Percent of Sample
0.2
20.6
44.2
24.9
7.9
1.6
0.6

Corneal Thinning

Fleischer Ring

Corneal Nerve Fibers More Visible

Munson’s Sign
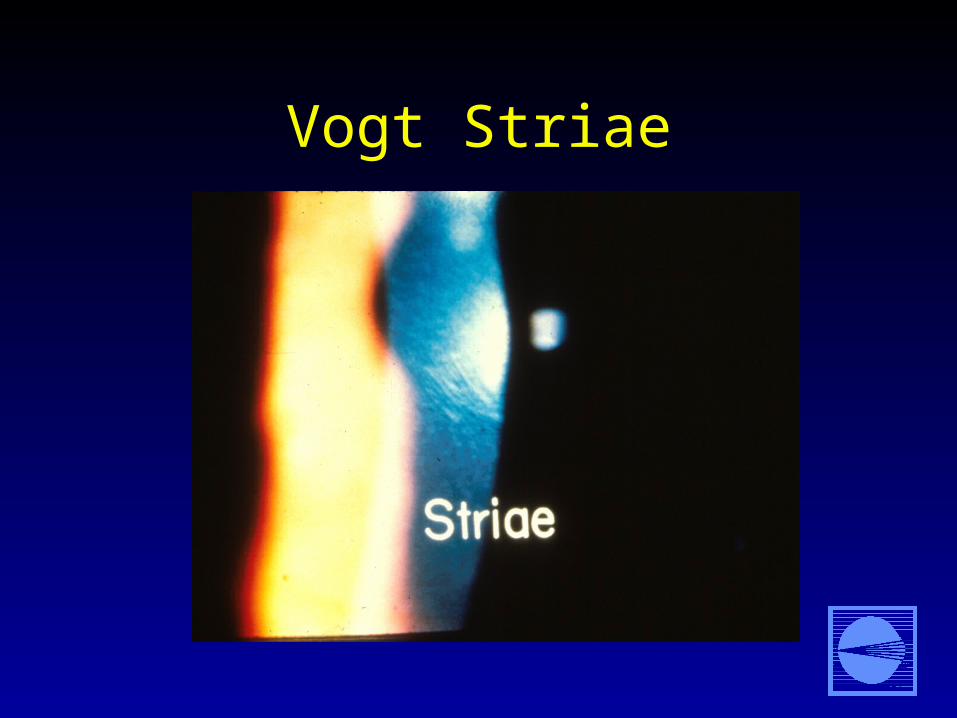
Vogt Striae

Corneal Hydrops

Corneal Hydrops




Hurricane (Whorl) Keratopathy

Ophthalmoscopy Reflex

Ophthalmoscopy Reflex

Slit Lamp FindingsEye
___________
Vogt’sStriae___________
Fleischer’sRing___________
CornealScarring___________
Neither 48% 36% 57%
One Eye 23% 21% 23%
Both Eyes 29% 43% 20%

Keratometry
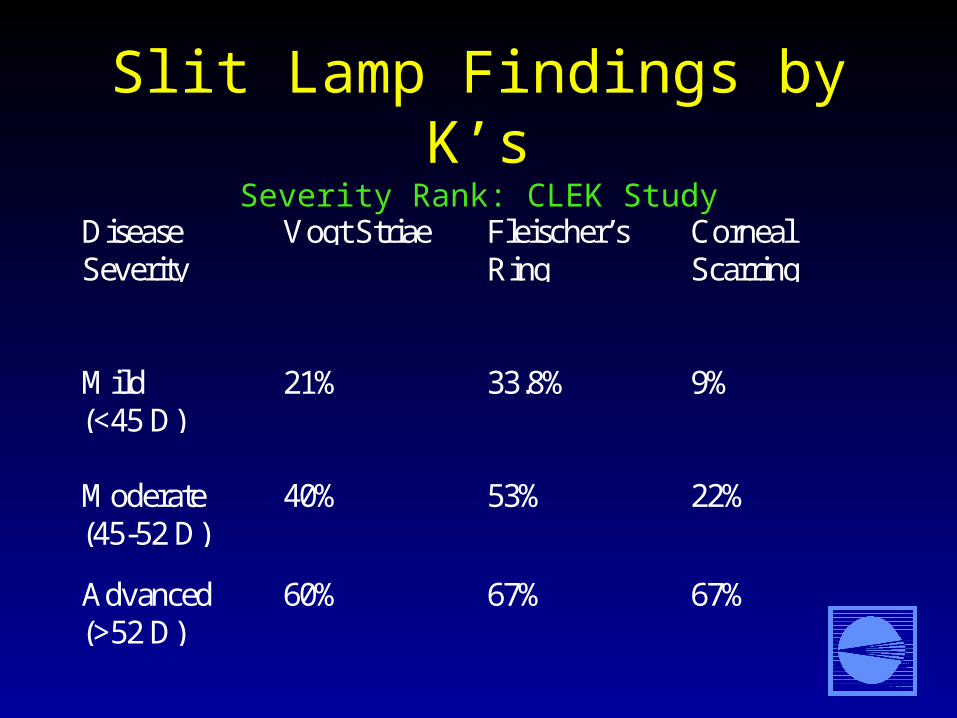
Slit Lamp Findings by K’sSeverity Rank: CLEK Study
DiseaseSeverity___________
Vogt Striae
___________
Fleischer’sRing___________
CornealScarring___________
Mild(<45 D)
21% 33.8% 9%
Moderate(45-52 D)
40% 53% 22%
Advanced(>52 D)
60% 67% 67%
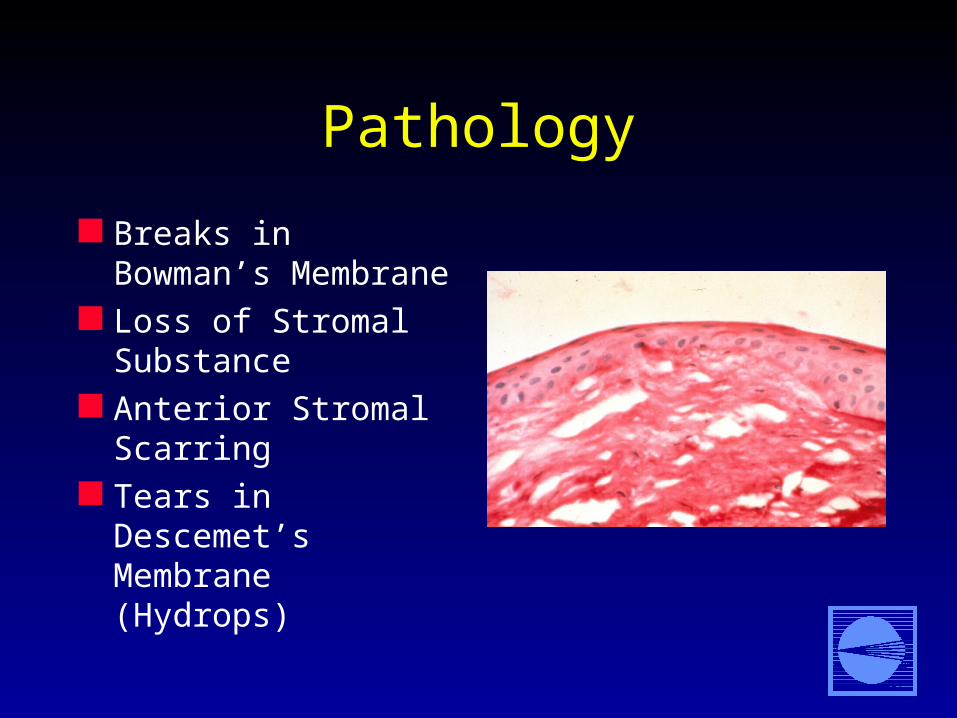
Pathology
Breaks in Bowman’s Membrane
Loss of Stromal Substance
Anterior Stromal Scarring
Tears in Descemet’s Membrane (Hydrops)

Pathology
Reduced Protein Content Reduced Protein and Collagen Production
When Grown in Culture in Some KCN Corneas but not all

Pathology
Elevated Lysosomal Enzymes in the Epithelium and Conjunctiva (but not the Skin)– acid phosphatase– acid esterase
Elevated Lysome Enzymes in the Corneal Epithelium– acid lipase

Pathology
Reduced Levels of Protease Inhibitors in the Epithelium and Stroma– alpha-1-protease inhibitor– alpha-2-macroglobulin

Pathology
Elevated levels of Inflammatory Products in Cultured KCN Corneas– 4X increase IL-1 receptors– 10X increase in Cyclooxygenase Vmax
(kinetics of cytokine system)– 10X increase in PGE2 production– increase in TGF beta

Pathology
Evidence supports the hypothesis that there is an acceleration in cellular degradation processes associated with an increase in degratory enzymes as a result of the suppression of inhibitory enzymes in the corneal epithelium, the conjunctival epithelium, and maybe the stroma.

Pathology
There is evidence of the inflammatory system being involved
It is likely that this is a secondary (response) mechanism
Genetic Disorder Suggested by:
Familial occurrence (13.5% in CLEK) 15-67X greater in 1st degree relatives than in
the general population Twin Studies Bilaterality

Linkage Studies
16q 22.3 – q23.1 Finland
20q 12 Tasmania
21 Utah
20 pII-qII Canada
3p14-q13 Italy
6p 25 Canada

Keratoconus: Complex Genetic Disorder
Multiple genes may come into play Other modifier genes may be involved
Interaction between genetic and non-genetic factors
Treatment Options
Spectacles Soft Lenses Rigid Corneal Lenses Piggy Back Lenses Scleral Lenses Penetrating Keratoplasty

Vision by Correction Type
VA_______________
CL________________
GLASSES________________
20/20 or + 32% 14%
20/21-20/40 56% 44%
20/41-20/60 8% 16%
<20/60 4% 26%

Keratoconus - RGP Corneal Lenses
Fitting Philosophies Fitting Method(s)

Keratoconus - Fitting Philosophies
Flat, Reshape the Cornea Flat, Three Point Touch Steep, Apical Clearance

Notice!
A “bad looking fit” is not a reason to change a lens

When To Change a Lens (General)
To Improve Vision To Improve Comfort To Reduce Physical Insult To Keep the Lens on the Cornea

When To Change a Lens (Specific)
Change in Power > .50 D That Improves VA 1 Line or More
Increasing Discomfort Increasing Lens Dislodgement (>3X/wk) Decreasing Wearing Time That is Fit Related Chronic Epithelial Whorl Staining Development of Subepithelial Nodule

Monitor
Central VA Hx of VA at Night Hx of Light Sensitivity Lens Behavior Epithelial Staining

Contact Lens Failure
43% Poor Visual Acuity 32% Contact Lens Intolerance 12% Peripheral Thinning

Reasons For Surgery
Visual Acuity <20/40, Loss of Function Lens Intolerance Can’t Keep a Lens on the Eye Frequent Corneal Abrasions With Severe
Disease Peripheral Corneal Thinning

Clinical Pearls
Glasses should be considered Use a large RGP for 1st timers with mild
steepening You can’t follow standard fitting protocols Evaluate edge clearance as carefully as you
do the central fitting relationship

Clinical Pearls
Move to a smaller design when you can (8.2-8.6 mm)
You’ll end up fitting much flatter than K as the disease progresses
If it isn’t broken, don’t fix it!

Pellucid Marginal Degeneration
Very uncommon Generally bilateral Onset: Age 10-30
years Inferior arcuate
thinning– width 1-2 mm
– length 4-8 mm
– 1-2 mm from limbus

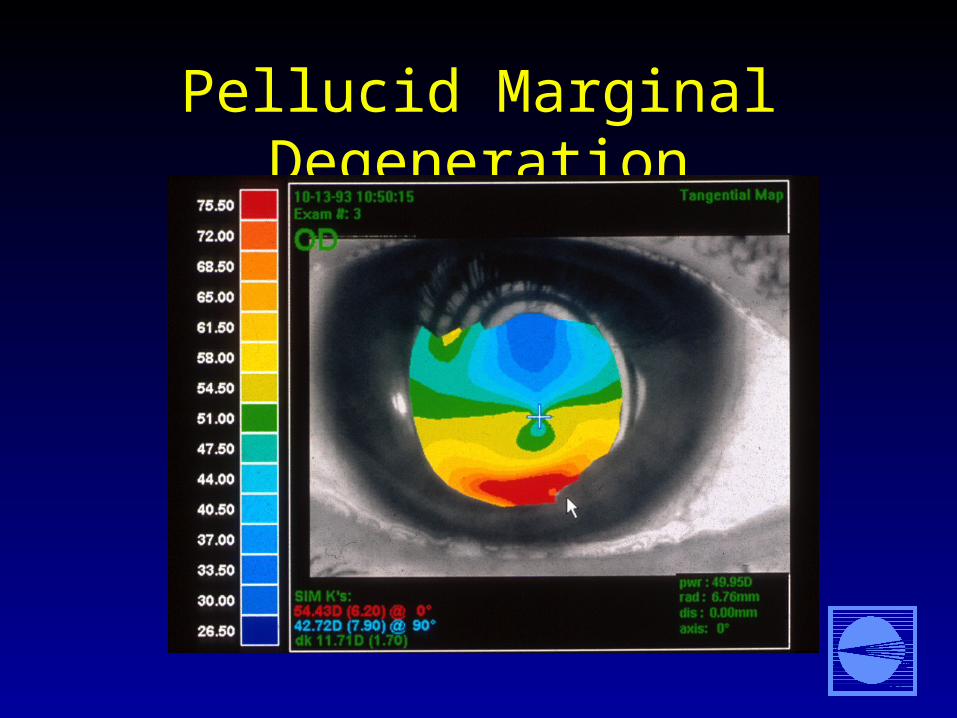
Pellucid Marginal Degeneration
Steepening above the thinned area
Central A/R astigmatism
Inferior W/R astigmatism
Slowly progressive “Inferior keratoconus”
Pellucid Marginal Degeneration
Pellucid Marginal Degeneration

Pellucid Marginal Degeneration
Spectacles Rigid contact lenses Crescentic lamellar
graft Large central
penetrating graft Combined procedure

Posterior Keratoconus
Rare Normal anterior
curvature (?) Steep posterior
curvature– diffuse or focal
Usually unilateral

Posterior Keratoconus
Posterior scarring Synechiae (sometimes) Present at birth Mesynchemal dysgenesis disorder

Posterior KeratoconusAssociated Conditions
Choroidal and retinal sclerosis Retinal coloboma Optic nerve hypoplasia Lens defects Posterior polymorphous dystrophy Ptosis

Keratoglobus
Rare Bilateral Clear, thin, limbus to
limbus Thinning is greatest
near or at the limbus 1/3 to 1/5 normal
thickness Nonprogressive

Keratoglobus
Present at birth High risk of
perforation (70%) May have Hydrops No association with
congenital glaucoma or megalocornea
Contact lenses are contraindicated

Terrien’s Marginal Degeneration
Any age/mostly middle-older adults
Bilateral (>80%), asymmetric
Slowly progressive Generally painless, but
may have painful episodes

Terrien’s Marginal Degeneration
Increase in cylinder, usually A/R
Flat meridian points to thinned area
20% have oblique pterygium

Senile Marginal Furrowing
Shallow peripheral thinning
Next to limbus Slowly progressive No epithelial defects No pain May have topographic
changes

Senile Marginal Furrowing
No vessels Sloping edges, no
guttering
THANK YOU!

Keratoconus GP Fitting Methods

Keratoconus - Flat, Reshape
Least Common Method Bronstein et al Sphericize the Cornea “Retard Progression” by Tamponade Generally Fit Large and Quite Flat

Flat, Reshape

Keratoconus - Three Point Touch
Most Popular Method No Intention to Change Shape Apical Touch or Bearing Mid-peripheral Bearing Peripheral Edge Clearance

Three-Point Touch

Flat 3-Point Touch

Keratoconus - Apical Clearance
Vaults Corneal Apex Mid-peripheral Bearing/Support Technically, the Most Difficult Method ? Reduces the Likelihood of Scars Forming

Apical Clearance

Keratoconus - SeveritySeverity Rank: McMahon
Average Keratometry Value Mild: 43.00-51.75 Moderate: 52.00-57.00 Severe: 57.25 +

Flat Fitting Method
Three-Point Touch (Flat Bias) Three-Point Touch (Steep Bias)

Mild Cone (Virgin)Flat Bias
Large Diameter (9.4-9.7 mm) Lid Supported Fit on K to 1.00D Flat Tricurve Design Spherical Base Curve

Mild Cone (Veteran)Flat Bias
Moderate Diameter (8.2-8.6 mm) Non-lid Supported Fit on K Tricurve Design Spherical Base Curve

Moderate ConeFlat Bias
Moderate Diameter (8.2-8.6 mm) Non-lid Supported Bispheric Base Design One Peripheral Curve, Flat Fit 1.00 D Flat if Average K = 52.00-54.00 Fit 2.00 D Flat if Average K = 54.25-57.00

Severe Cone Flat Bias
Try Moderate Diameter First (8.2-8.6 mm) Fit 3-4 Diopters Flat If Unstable, Large Diameter (9.4-9.7 mm) Fit 5-6 Diopters Flat Bispheric Design One, Flat Peripheral Curve Non-lid Supported

Mild Cone (Virgin)Steep Bias
Large Diameter (9.4-9.7 mm) Lid Supported Fit on K to 0.50D Steep Tricurve Design Spherical Base Curve

Mild Cone (Veteran)Steep Bias
Moderate Diameter (8.2-8.6 mm) Non-lid Supported Fit .75 D Steeper than K Tricurve Design Spherical Base Curve

Moderate ConeSteep Bias
Moderate Diameter (8.2-8.6 mm) Non-lid Supported Bispheric Base Design One Peripheral Curve, Flat Fit On K if Average K = 52.00-54.00 Fit 1.00 D Flat if Average K = 54.25-57.00

Severe Cone Steep Bias
Try Moderate Diameter First (8.2-8.6 mm) Fit 1-2 Diopters Flat If Unstable, Large Diameter (9.4-9.7 mm) Fit 3-4 Diopters Flat Bispheric Design One, Flat Peripheral Curve Non-lid Supported

Apical Clearance Fitting
Diameter 7.5 to 8.5 mm Use Steep K Find First Definite Apical Clearance Base
Curve (Fluorescein) Two Peripheral Curves (First is Wide)