keep moving! the benefits of exercise for cancer patients · pdf filekeep moving! the benefits...
TRANSCRIPT

3/15/2016
1
Keep moving! The Benefits of
Exercise for Cancer Patients
Rob Newton
PHYSICAL ACTIVITY, EXERCISE & THE CANCER CONTROL FRAMEWORK
prediagnosis postdiagnosis
prescreening screening
prevention/detection
DIAGNOSIS
CANCER CONTROL CATEGORIES
treatmentpreparation
recovery disease prevention
palliation survival
pretreatment treatment survivorship end of life
treatmenteffectiveness
cancer-related time periods
Courneya and Friedenreich Sem Onco Nurs 2007;23:242-52
Specific phases along the cancer continuum
Physical activity and cancer risk
•Physically inactive - nearly twice as likely to develop colon cancer1
•Active - 30% reduction in the risk of women of all ages developing breast cancer2
•Reduces prostate cancer incidence of advanced forms and in older men - 70% reduction if >3 hours vigorous per week3
• 20 % reduction in risk of Lung cancer4
1.Colditz et al. Cancer Causes Control. 8(4):649-67.19972.Thune & Furberg. Med Sci Sports Exerc. 33(6 Suppl):S530-50. 20013. Patel et al. Cancer Epidemiol Biomarkers Prev. 14(1):275-9. 20054. Lee & Oguma. Cancer Epidemiology and Prevention. 3rd ed. University Press, 2006
PHYSICAL ACTIVITY AND EXERCISE
• World Health Organisation defines physical activity as “any bodily movement produced by skeletal muscles that requires energy expenditure”.
• WHO is explicit that the term “physical activity” should not be used interchangeably with “exercise”.
EXERCISE
• Exercise, is a subcategory of physical activity that is planned, structured, repetitive, and purposeful in the sense that the improvement or maintenance of one or more components of physical fitness (capacity, structure, function, homeostatis) is the objective.”
EXERCISE MEDICINE
• “Exercise medicine” is the physical assessment and prescription of exercise specifically for the prevention or treatment of injury or illness.
• Specific exercise drives endogenous “medicine”
– Hormones and cytokines
• Direct structural adaptation and repair
• Facilitates other therapies
3/15/2016
2
Galvão & Newton. J Clinical Oncology 2005;23:899-909
By June 2004 – 26 trials; majority of studies with breast cancer using cardiovascular exercise
• Overwhelmingly positive effects despite quite sub-optimal exercise prescription
• Researchers and clinicians not drawing on vast knowledge of exercise and human performance
461 citations in 11 years
Survival!
Cancer Survival: Time to Get Moving? DataAccumulate Suggesting a Link Between Physical Activity and Cancer Survival
Demark-Wahnefried W. Editiral. Journal of Clinical Oncology. 24(22):3517-8. 2006.
EXERCISE AND BREAST CANCER SURVIVAL
• 2987 female nurses who were diagnosed with breast cancer
• RR of death 0.5 to 0.6 < 3 MET‐hours per week compared 9 or more.
• One MET‐hour is equivalent to approximately 20 minutes walking at a normal pace (4 kph).
• 9 Met‐hours = 3 hours walking or 77 mins jogging
Holmes MD, Chen WY, Feskanich D, Kroenke CH, Colditz GA. Physical activity and survival after breast cancer diagnosis. JAMA. 293(20):2479-86. 2005
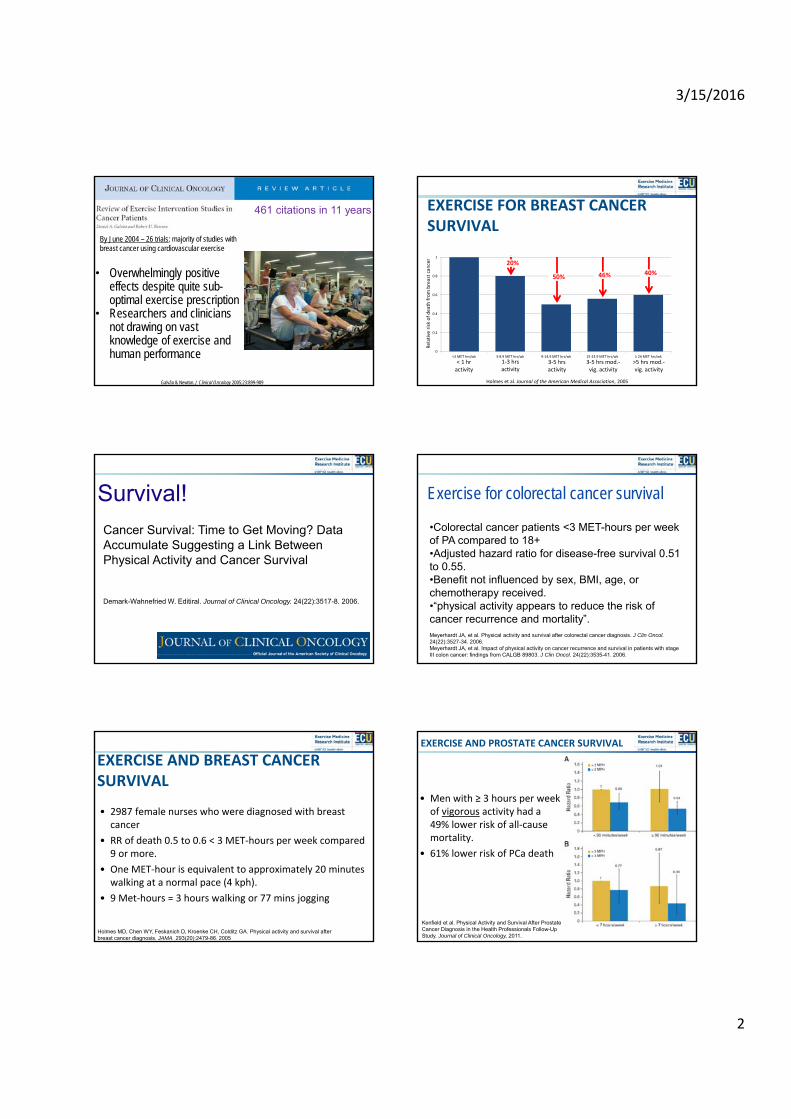
EXERCISE FOR BREAST CANCER SURVIVAL
Holmes et al. Journal of the American Medical Association, 2005
0
0.2
0.4
0.6
0.8
1
<3 MET hrs/wk 3‐8.9 MET hrs/wk 9‐14.9 MET hrs/wk 15‐23.9 MET hrs/wk ≥ 24 MET hrs/wk
Relative risk of death from breast can
cer
< 1 hr activity
1‐3 hrs activity
3‐5 hrs activity
3‐5 hrs mod.‐vig. activity
>5 hrs mod.‐vig. activity
20%
50% 46% 40%
•Colorectal cancer patients <3 MET-hours per week of PA compared to 18+•Adjusted hazard ratio for disease-free survival 0.51 to 0.55. •Benefit not influenced by sex, BMI, age, or chemotherapy received. •“physical activity appears to reduce the risk of cancer recurrence and mortality”.Meyerhardt JA, et al. Physical activity and survival after colorectal cancer diagnosis. J Clin Oncol.24(22):3527-34. 2006.Meyerhardt JA, et al. Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: findings from CALGB 89803. J Clin Oncol. 24(22):3535-41. 2006.
Exercise for colorectal cancer survival
• Men with ≥ 3 hours per week of vigorous activity had a 49% lower risk of all‐cause mortality.
• 61% lower risk of PCa death
EXERCISE AND PROSTATE CANCER SURVIVAL
Kenfield et al. Physical Activity and Survival After Prostate Cancer Diagnosis in the Health Professionals Follow-Up Study. Journal of Clinical Oncology, 2011.
3/15/2016
3
Compared to Chemotherapy
•Data from these studies suggest a reduced risk of recurrence or death of 50% to 60%.
“Such an effect parallels that of trastuzumab for HER-2–positive breast cancer patients, an agent heralded by the oncologic care community and by the Director of the National Cancer Institute, Andrew C. von Eschenbach, MD, as “a major advance andturning point in eliminating suffering and death from cancer.”
Demark-Wahnefried W. Journal of Clinical Oncology. 24(22):3517-8. 2006.
Exercise is NOT an alternative to
chemotherapy but a critical synergistic medicine
National/International Position Stands – Exercise and Cancer
American Cancer SocietyExercise Sports Science Australia American College of Sports Medicine
2009 2010 2011
Every Week• 75-150 minutes moderate to
vigorous aerobic exercise• 2 or more resistance training
sessions for all major muscle groups
• Polypharmacy?
Generic to Tailored Prescription• Important start given majority of cancer
survivors sedentary• 86% of Australian men with PCa do not
meet guidelines• However – greater effectiveness and
compliance with targeted exercise medicine
A - overwhelming data from RCTsB - few RCTs existC - uncontrolled, nonrandomized and/or observational studiesD - insufficient for categories A-C
Focus on adult cancers and sites with the most evidence
Evaluation of Evidence A-D*Breast, Prostate, Colon, Hematological, Gynecological
American College of Sports Medicine. Med Sci Sports Exerc. 2010;42(7):1409-1426 *National Heart Lung and Blood Institute
•Evidence category A – Safety•Evidence category A – Aerobic Fitness •Evidence category A – Muscle Strength •Evidence category B – Body Size/Composition•Evidence category B – Quality of Life•Evidence category B – Fatigue•Evidence category B – Anxiety
During chemotherapy or radiation Results from 22 RCTs
Evidence for Breast Cancer
American College of Sports Medicine. Med Sci Sports Exerc. 2010;42(7):1409-1426
• Evidence category A - Safety• Evidence category A - Aerobic Fitness • Evidence category A - Muscle Strength • Evidence category A - Flexibility• Evidence category A - Physical Function• Evidence category A - Safety Lymphedema Onset or Worsening• Evidence category B - Body Size/Composition • Evidence category B - Quality of Life• Evidence category B - Fatigue/Energy/Vitality• Evidence category B - Depression/Anxiety• Evidence category B - Body Image• Evidence category C - Symptoms/Adverse Effects and Pain
Following treatment Results from 32 RCTs
Evidence for Breast Cancer
American College of Sports Medicine. Med Sci Sports Exerc. 2010;42(7):1409-1426
IMPACT EXERCISE FOR BONE HEALTH

3/15/2016
4
LUMBAR SPINE BMD (% CHANGE OVER 6 MONTHS)
Newton et al 2013 World Prostate Cancer Congress
World first for ECU
EXERCISE FOR PATIENTS WITH BONE METASTASES
SAFE AND EFFECTIVE
World first for ECU
SAFETY
Adverse events during the exercise sessions 0
Attendance (out of 24 sessions) 20.2 ± 7.6
Compliance (% of successfully completed sessions) 93.2 ± 6.3
Perceived tolerance of the exercise sessions (0 = intolerable; 7 = highly tolerable)
6.1 ± 0.7
Perceived exercise intensity (session RPE) 13.8 ± 1.5
Severity of bone pain at the start of each session (average of all sessions; 0 = no pain; 10 = very severe pain)
0.6 ± 0.7
Incidence of bone pain negatively affecting the ability to undertake ADL between exercise sessions
0
• No between‐group difference in bone pain (p = 0.602)
• No change in use of pain medication throughout 12 weeks
‐10
‐5
0
5
10
15
20
25
MuscleStrength
AerobicFitness
Ambulation Lean Mass PhysicalAcitivty Level
p = 0.602
EFFICACY
Adjusted Group Difference in Mean Change Over 12 weeks*
p = 0.016p < 0.001
p = 0.010
p = 0.026
*Between group change by ANCOVA adjusted for baseline valuesaIncludes adjustment for use of pain medication
p = 0.003
Bone Paina
Muscle Strength
Physical Activity Level
Percen
t Difference (%)
Favours Exercise
Favours
Usual CareAerobic
Fitness
1.7 kg
DELIBERATE LOADING OF BONE METS?
“mechanical loading dramatically reducedosteolysis and tumor formation and
increased tibial cancellous mass due to trabecular thickening”
Basis of a new Exercise Trial in Breast Cancer led by Dr Nicolas Hart

3/15/2016
5
EXERCISE FOR LYMPHOEDEMA
• Lymphoedema affects ~20‐30% of breast cancer survivors
• Historically upper body exercise has been discouraged for women who have or are at risk of lymphoedema for fear of exacerbating the condition
Bioimpedence Spectroscopy
Heavier Weights Lighter Weights No Exercise
Ch
ang
e in
L-D
ex
Sco
re
-6
-4
-2
0
2
4
6
Bioimpedence Spectroscopy
Pre
Immediately Post
24 hours Post
72 hours Post
L-D
ex
Sco
re
0
10
20
30
40
50Heavier WeightsLighter Weights
Acute Impact of Exercise on Lymphoedema
Impact of Regular Exercise on Lymphoedema
EXERCISE FOR LYMPHOEDEMA
• A bout of resistance exercise does NOT cause an increase in swelling or worsening of symptom severity
– This is the case for both heavier & lighter weights
• Regular resistance exercise over 3 months results in:
– ↔ swelling (i.e. does NOT increase swelling)
– ↑ strength
– ↑ physical func on
– Similar effects observed for both heavier & lighter weights
Chest Press 1RM
Heavier Weights Lighter Weights No Exercise
Pe
rce
nt C
hang
e (
%)
0
20
40
60
80
Seated Row 1RM
Heavier Weights Lighter Weights No Exercise
Per
cen
t C
han
ge (
%)
0
10
20
30
40
50
*
*
*
*
World first for ECU
• Tailored exercise prescription for patients during radiation and/or chemotherapy
• Assessment and prescription by our Accredited Exercise Physiologists – trained and experienced in exercise oncology
• Implementing latest research from our clinical trials into best practice patient support
• World first in terms of proximity to therapy
• Convenience, stress reduction, acute exercise effects
• Efficacy, tolerance, effectiveness pilot trial
GENESIS CANCER CARE:EXERCISE CLINIC
• 176 consultations completed• 74 patients have commenced an exercise program• 35 patients completed pre & post‐testing• Average program length 4‐6 weeks• Preliminary outcomes:
– balance +7.08%– chest press +13.4%– leg press +36.4%– seated row +8.15%– aerobic fitness +3.53%– Lean mass ‐1.11%– %fat ‐0.24% (change in average body fat percentage)– systolic BP ‐3.23%– normal walk speed +4.17% and fast walk +1.78%
• During a treatment phase expected to severely negatively impact health and fitness!
OUTCOMES TO DATE
CHEMO COMPLETION
Waart et al. J Clin Oncol. 2015 Apr 27. 2014.59.1081. [ahead of print]
EXERCISE MECHANISMS: SURVIVAL AND TUMOUR BIOLOGY
Galvão, Newton et al. Nature Reviews Urology, Published online 8th March 2016
3/15/2016
6
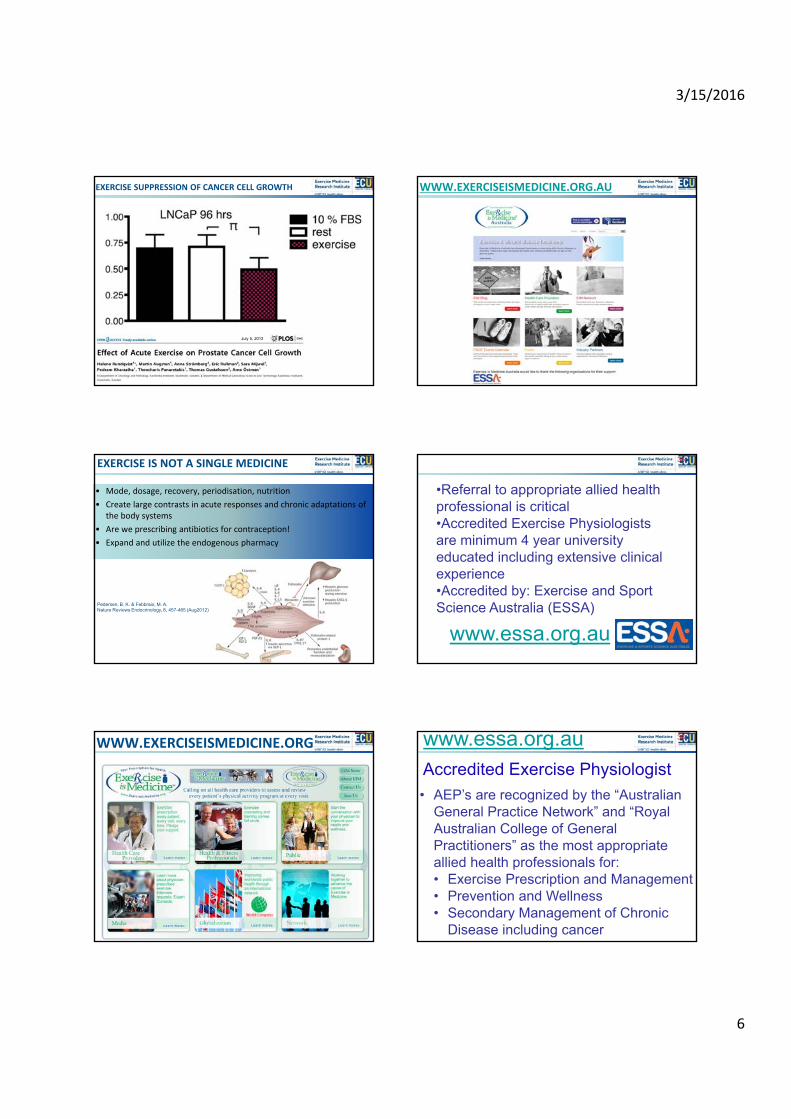
EXERCISE SUPPRESSION OF CANCER CELL GROWTH
• 10 male individuals ‐ 60 minutes cycling
• Serum pre+post
• Prostate cancer cell line LNCaP exposed
• 9 out of 10 individuals growth inhibition
• Pooled exercise serum 31% inhibition
July 5, 2013
EXERCISE IS NOT A SINGLE MEDICINE
• Mode, dosage, recovery, periodisation, nutrition
• Create large contrasts in acute responses and chronic adaptations of the body systems
• Are we prescribing antibiotics for contraception!
• Expand and utilize the endogenous pharmacy
Pedersen, B. K. & Febbraio, M. A. Nature Reviews Endocrinology, 8, 457-465 (Aug2012)
WWW.EXERCISEISMEDICINE.ORG
WWW.EXERCISEISMEDICINE.ORG.AU
Exercise Scientist and Physiologist
•Referral to appropriate allied health professional is critical•Accredited Exercise Physiologists are minimum 4 year university educated including extensive clinical experience•Accredited by: Exercise and Sport Science Australia (ESSA)
www.essa.org.au
35
Exercise Scientist and Physiologist
• AEP’s are recognized by the “Australian General Practice Network” and “Royal Australian College of General Practitioners” as the most appropriate allied health professionals for:• Exercise Prescription and Management• Prevention and Wellness• Secondary Management of Chronic
Disease including cancer
Accredited Exercise Physiologist
36www.essa.org.au
3/15/2016
7
Exercise Scientist and Physiologist
• MBS Chronic Disease Management –GP Services includes referral to AEPs
• Up to 5 consults per calendar year• Many private health insurers now
cover AEP services
Rebates for Exercise Physiology Services
37
EXERCISE MEDICINE RESEARCH INSTITUTE
www.exercisemedicine.org.au
VARIO HEALTH CLINIC
www.exercisemedicine.org.au
Title ‐ target N, months intervention, trial sites
1. Exercise, Sexual health and PCa ‐ 240/6/8
2. Exercise and chemotherapy‐induced cognitive‐impairment ‐ 66/4/5
3. Exercise during adjuvant‐treatment of high‐grade glioma ‐ 30/3/6
4. Exercise as medicine for mesothelioma – 20/3/6
5. Exercise, PCa and bone metastases ‐ 90/3/5
6. LifeNow for cancer survivors – an RCT 100/3/15
7. Breast cancer and bone metastases ‐ 100/35
8. Exercise therapy and pancreatic cancer ‐ 20/6/5
9. Exercise medicine during radiation and chemo therapy – The Genesis Study – 50/3/1
10. Movember GAP4 – CRPC International Trial – 900/24/25
CURRENT TRIALS