kastango usp 797 795 nd final - since...
TRANSCRIPT

4/5/2014
1
USP 797 and USP 795: The “Why” behind the USP compounding chapters
Eric S. Kastango, MBA, RPh, FASHPClinical IQ, LLC and CriticalPoint, LLC
Madison, New Jersey
North Dakota Pharmacy ConventionApril 5, 2014
Learning and Performance Objectives
2
At the end of this session, learners will be able to:
Summarize the evolution of the practice of sterile compounding including
misadventures that shaped pharmacy regulation.
Explain current and upcoming national and state laws and standards as it pertains to compounding.
Describe essential elements of performance described in USP Chapters <795> and <797> respectively as they relate to non sterile and sterile compounding.
List the performance elements required of healthcare personnel performing
limited sterile compounding outside of a controlled pharmacy compounding environment.
Define the importance of achieving and maintaining a state of control as it relates to sterile compounding.
Year State Description
1990 Nebraska 4 patients died of a bacterial infection from non-sterile cardioplegia solution compounded in a hospital.
1990 Pennsylvania 2 patients lost their vision after becoming infected by Pseudomonas aeruginosa found in indomethacin eye drops compounded in a drug store even though commercial non-steroidal drops were available at the time.
1998 California 11 children became septic—10 tested positive for Enterobactercloacae bloodstream infections associated with contaminated prefilled saline syringes.
2001 California 11 patients contracted Serratia marcescens infections following the injection of betamethasone compounded at a community pharmacy.
2001 Missouri 4 children contracted Enterobacter cloacae infections from IV ranitidine compounded in a hospital pharmacy.
Brutal Facts
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Year State Description
2002 North Carolina, South Carolina
5 patients developed Exophiala infections from contaminated injectable methylPREDNISolone that was prepared by a compounding pharmacy; one patient died.
2002 Michigan Pharmacy preparing injectable methylPREDNISolone and baclofen recalled the products because of contamination with Penicillium mold, Methylobacterium, and/or Mycobacterium chelonae.
2003 Missouri Bacteria contamination with Burkholderia cepacia found in at least 2 batches of a compounded inhalant solution used by 19,000 patients with chronic lung diseases.
2004 Texas, New York, Michigan, Missouri
36 patients developed Pseudomonas bloodstream infections after receiving heparin/saline flushes from multiple lots of preloaded syringes.
Brutal Facts
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Year State Description
2005 New Jersey, California
Up to 25 patients contracted Serratia marcescens infections due to contaminated magnesium sulfate mini-bags prepared by a compounding pharmacy.
2005 Minnesota 2 patients were blinded after receiving a compounded trypanblue ophthalmic injection contaminated with Pseudomonas aeruginosa and Burkholderia cepacia; the injectable product is a commercially available product.
2005 California Sterile talc vials with unwashed stoppers were not sterility tested before distribution from an outsourcing compounding pharmacy.
2005 Maryland 10 patients died after exposure to cardioplegia solution from 2 lots contaminated with gram-negative rods.
Brutal Facts
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Year State Description
2006 Ohio 1 child died after a compounding error led to administration of chemotherapy in 23.4% sodium chloride injection instead of 0.9% sodium chloride.
2007 Washington, Oregon
2, possibly 3, patients died after receiving an intravenous colchicine product compounded at a concentration higher than standard (4 mg/mL vs. 0.5 mg/mL) in a compounding pharmacy.
2009 Florida 21horses died after receiving a compounded substitute vitamin supplement containing vitamin B, potassium, magnesium, and selenium (product not approved in the US).
2010 Illinois 1 child died after receiving more than 60 times the amount of sodium chloride prescribed due to a compounding error in a hospital pharmacy.
Brutal Facts
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
2
Year State Description
2011 California, Florida,
Tennessee
16 patients being treated for wet macular degeneration developed severe eye infections due to contamination of AVASTIN (bevacizumab) during compounding; one patient blinded, another patient developed brain infection.
2011 Alabama 9 patients among 19 died when parenteral nutrition solutions that were administered were contaminated with Serratia marcescensduring compounding using non-sterile components to prepare amino acids.
2012 California 9 patients developed fungal endophthalmitis after use of the compounded product Brilliant Blue-G (BBG) or receiving injections of triamcinolone-containing products dispensed from the same compounding pharmacy.
2012 Nationwide More than 750 patients contracted fungal meningitis after receiving methylPREDNISolone acetate injection prepared by a compounding pharmacy that was contaminated with Exserohilum rostratum (a brown-black mold) & Aspergillus.
Brutal FactsThe compounded drug at the center of the NECC contamination
case was which of the following?
Betamethasone
17-α hydroxyprogesterone (17-P)
Methylprednisolone
Potassium chloride
A
B
C
D
Methylprednisolone
• A synthetic glucocorticoid or corticosteroid drug.
• All injectable dosage forms have preservatives which is contraindicated intrathecally.
“Corticosteroids may exacerbate systemic fungal infections and therefore should not be used in the presence of such infections unless they are needed to control drug reactions”
Used with permission, APP Pharmaceuticals, LLC
Exserohilum rostratum
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Image courtesy www.cdc.gov
New England Compounding Center (NECC) Meningitis Outbreak
Date September 21, 2012 (on-going) – October 23, 2013
Location USA (23 States)
Cause Fungal meningitis contamination of steroid medication
Injuries
751Total Case Count, 379 meningitis and Spinal Infection, 6 Stroke, 288 Paraspinal/Spinal infection, 30 Peripheral Joint Infection,
Some patients recovering from the meningitis are falling ill again. Sufferers of the new infection are now coping with epidural abscesses and infections near the injection site.
Death(s) 64
Litigation More than 20 lawsuits filed against NECC
The scale of the meningitis outbreak makes this event the worst among a series of fatal or harmful infections and overdoses linked to pharmacy
compounding practices in the US rivaling other key drug safety issues in the past that have led to substantial drug safety legislation.
Persons with Fungal Infections Linked to Steroid Injections, by State
4/5/2014 12
Source: http://www.cdc.gov/hai/outbreaks/meningitis-map-large.html

4/5/2014
3
“Study the past if you would
define the future”Confucius
History of Compounding
� Pharmacy compounding is simply the art and science of preparing customized medications that are not otherwise commercially available.
� Compounding is performed by or under the supervision of a pharmacist pursuant to an order from a licensed prescriber for an individual patient.
� Compounding is an essential element of pharmacy.
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
History of Compounding
� All states license pharmacists to compound
� States laws vs. Federal laws (FDA)
� The federal government, through the FDA, is arguing that patient safety is in jeopardy
� Each state has varying degrees of regulations and oversight and enforcement of compounding practices
� 22 states require direct compliance with USP 797 after 10 years
� Until USP <797>, no consistent and enforceable compounding standard of practice existed
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
History of Sterile Compounding
� Despite the chapter’s uniform sterile compounding standards, schools of pharmacy may not always include sterile compounding
� Only 1 in 6 graduates are prepared for sterile compounding work*
*Helmus M, Alverson, SP, Monk-Tutor, MR. Instruction on compounded sterile preparations at U.S. schools of pharmacy. AJHP. Volume 64, Nov 1, 2007: 2267-74.
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
1975 • NCC LVP
1990
• FDA Alert Letter• ASHP Urgent Attention Letter
1991• ASHP National Survey
1993• ASHP TAB
1995
• USP <1206>• ASHP National Survey
1998• FDAMA signed into law by President
Clinton
2000• ASHP Guidelines revised
2002• ASHP National Survey
Yesterday…
2004• January 1, USP 797 first published
2004• November, NIOSH Alert first published
2008• USP Chapter <797> revised, new standard effective
June 2008
1993• ASHP TAB
2011• 1st CriticalPoint National USP 797 Compliance
Survey
2012
• CDC and CMS recognizes USP Chapter <797>• NECC tragedy
• 2nd CriticalPoint USP 797 Compliance Survey
Today…

4/5/2014
4
� Three national surveys
� ASHP: every 3 years
� CriticalPoint’s online USP <797> Compliance Study (annually since 2011)
� Pharmacy Purchasing & Products every year
How Compliant Are We?
Copyright © 2008-2014 CriticalPoint® - All rights reserved
State of Compliance
71.6%
73.9%
73.0%
76.6%
75.3%
78.6%
73.9%
77.2%
68%
70%
72%
74%
76%
78%
80%
2011 2013
Compliance Scores 2011 vs. 2013 based on State Regulatory Requirements
States have no sterile compounding req States have some sterile compounding req
States Req Compliance with 797 Overall Compliance
N=1045
N=1148
Source: Douglass K, Kastango E, Cantor P, et al. The 2013 USP <797> compliance study. Pharm Purch Prod. Oct 2013
State Board of Pharmacy Position on USP 797
The Drug Quality and Security Act (DQSA) Drug Quality and Security Act (DQSA)
� Current status: signed into law by President Obama on November 27, 2013
� Divided into 2 major sections called Titles
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
The Drug Quality and Security Act (DQSA)
� Title I – Compounding Quality Act
� Eliminates the unconstitutional provisions of 503A that “…created uncertainty regarding the laws governing compounding.”
� Requires FDA to engage in two-way communication with state regulators – identified as a major deficiency in FDA’s response to the meningitis outbreak.
� Preserve and protect the practice of Traditional Pharmacy compounding in community pharmacies.
* FDA Guidance for Industry - Interim Product Reporting for Human Drug Compounding Outsourcing Facilities under 503B of FDCA – DEC 2013
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
� Title 1: Compounding Quality Act: 503B -Outsourcing Facilities.
� Permit entities engaged in compounding of sterile drugs to register as “Outsourcing Facilities.”
� Under Section 503B, pharmacy outsourcers to voluntarily register as “outsourcing facilities,” making them subject to good manufacturing practices, risk-based inspection and other standards
The Drug Quality and Security Act (DQSA)
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
5
� Title 2: Drug Supply Chain Security Act
� Track and Trace Program
� The development of the system will be phased in with new requirements over a 10-year period.
� These requirements will include placing unique product identifiers on individual drug packages and providing product and transaction information at each sale with lot level information, in paper or electronic format.
Source: http://www.fda.gov/drugs/drugsafety/drugintegrityandsupplychainsecurity/drugsupplychainsecurityact/default.htm
The Drug Quality and Security Act (DQSA) The Drug Quality and Security Act (DQSA)
� Section 503A (21USC353a) - Traditional compounding
� State-based regulations – State Boards of Pharmacy
� Traditional, individualized prescriptions
� Section 503B (21USC353b) - Outsourcing facilities
� FDA jurisdiction; registration; reporting; cGMPs
� Manufacture and interstate shipment of larger quantities of compounded drugs without prescriptions
� Under direct supervision on a pharmacist
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
503A standards (continued)
� Use bulk from FDA registered facility only
� May not compound those on list of drugs removed from the market
� No inordinate amounts of what are “essentially copies of commercially available drug products”
� Not a product identified as presenting demonstrable compounding difficulties
� Metered dose inhalers
� Transdermal systems, others?
� Subject to inspection by FDA if not in compliance with USP chapters on compounding
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Section 503A
� Health-systems are exempt from registration with the FDA
� Insourcing/regionalizing is possible in some states
Health System Regionalization
Prohibited by SBOP Permitted by SBOP
Virginia New Jersey
Massachusetts California
Ohio Wisconsin
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Registered Outsourcing Facilities
� Firms Registered As Human Drug Compounding Outsourcing Facilities Under Section 503B of the Federal Food, Drug, and Cosmetic Act (FD&C Act)
� Thirty-eight (38) registered establishments As 503B
� http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/PharmacyCompounding/ucm378645.htm
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
The Drug Quality and Security Act (DQSA) -
� The “Risk based system” for FDA inspections –
� Compliance History of the Outsourcing Facility
� Record, History, and Nature of the recalls linked to the Facility
� The “inherent risk” of the drugs compounded at the facility.
� Inspection frequency within the last 4 years by FDA.
� Whether the facility intends to compound a drug under section 506 E (drug shortage item).
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
6
The Drug Quality and Security Act (DQSA)
� Prohibited Acts –
� Wholesaling -
� There is a carve-out for “drugs used in a healthcare setting.”
� Intentional Falsification of Prescriptions
� Failure to report ADRs
� Misbranding of Drugs
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
The Drug Quality and Security Act (DQSA)
� The “Missing Parts” –
� A complete list of FDA approved API suppliers.
� The FDA’s Bulk Drug Substance list
� The FDA’s Drug Shortage list (506 E).
� The list of “Drugs presenting demonstrable difficulties for compounding”
� A complete FDA DO NOT Compound list.
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
FDA Information
� Outsourcing Registration List� http://www.fda.gov/drugs/guidancecomplianceregulatoryinfor
mation/pharmacycompounding/ucm378645.htm
� Inspections; Recalls; other Actions� http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryIn
formation/PharmacyCompounding/ucm339771.htm
� Regulatory Policy Information� http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryIn
formation/PharmacyCompounding/ucm166743.htm
� Compounding FDA Web page� http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryIn
formation/PharmacyCompounding/default.htm
USP Compounding Standards
� USP Chapter <797>: Sterile Compounding became official on January 1, 2004� Revised chapter official on June 1, 2008
� Nationally enforceable
� 23 states require compliance, more states are modifying regulations
� Codify USP <797>
� Adopt portions
� Develop own regulations
� No action
� Shall vs. Should: Appendix I
� USP Chapter <795>: Nonsterile Compounding
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
� USP <797> applies to all personnel who compound sterile preparations
� Pharmacists
� Pharmacy Technicians
� Nurses
� Physicians
� Anesthesia Personnel
� Other hospital clinicians
� Veterinarians
� Veterinary Technicians
Who Compounds Sterile Preparations?
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
7
Where are CSPs Compounded?
� Pharmacies
� Hospitals
� Home Care
� Nuclear
� Community
� Hospital departments
� Long-term care and rehab facilities
� Ambulatory offices and clinics
� Imaging
� Allergy
� Oncology
� Surgical centers
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Types of CSPs� Large volume parenterals
� Small volume parenterals
� Piggyback bags
� Syringes
� Irrigations
� Ophthalmics
� Parenteral nutrition (PN)
� Inhalations
� Allergen extracts
� Radiopharmaceuticals
Image: Courtesy CriticalPoint, LLC
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Not in Scope of USP <797>
� Manufactured products
� FDA labeling
� Administration of medications
� <797> applies up to the point of administration
� CDC provides guidance on “hang time”
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Manufactured Products
Premixed IVs
Vial and Bag Systems
CSP Microbial Risk Levels
• True emergency situations
• Compounded outside of a hood
• Expectations: Handwashing
• 6 Criteria which all must be met
High Risk
Medium Risk
Low Risk
Low Risk with 12 h BUD
Immediate Use
1. Compounding is continuous and is no longer than one hour
2. Aseptic technique is followed3. Administration begins within 1 hour of start of
preparation 4. Appropriately labeled
1. Simple transfer ≤ 3 commercially manufactured non-hazardous products
2. Not > 2 entries into any container
3. Compounding continuous/not > 1 hour
4. Aseptic technique is followed
5. Admin begins ≤ 1 hour from start of compounding
6. Appropriately labeled
Example: initial dose of norepinephrine drip in ICU after pharmacy hoursNurses prepare 14-16% of IV doses from vials and ampules (2011 AJHP Dispensing and Administration)
Copyright © 2013-2014 CriticalPoint’s Sterile Compounding Boot Camp™ - All rights reserved
CSP Microbial Risk Levels (continued)
• Segregated Compounding Area
� CSPs made in a hood that is not placed in a cleanroom
• Cannot be used for hazardous drugs
• Expectations still include
� Hand hygiene and garbing
� Daily & monthly cleaning
� Environmental sampling
Copyright © 2013-2014 CriticalPoint’s Sterile Compounding Boot Camp™ - All rights reserved
High Risk
Medium Risk
Low Risk
Low Risk with 12 h BUD
Immediate Use
Example: initial dose of norepinephrine
compounded in satellite pharmacy in the ER

4/5/2014
8
CSP Microbial Risk Levels (continued)
• Not > 3 sterile drug packages used (including diluent)
• Using sterile equipment
• Compounded in an ISO Class 5 device usually in an ISO Class 7 environment
• Limited, basic, closed-system aseptic transfers and manipulations
• Expectations: all QA components with annual aseptic media fill and GFS
Copyright © 2013-2014 CriticalPoint’s Sterile Compounding Boot Camp™ - All rights reserved
High Risk
Medium Risk
Low Risk
Low Risk with 12 h BUD
Immediate Use
Example: 1 dose of 1000 mL D5W with 30 mEq potassium chloride added
CSP Microbial Risk Levels (continued)
• Using 4 or more sterile ingredients, complex aseptic manipulations
• No bacteriostatic additive and administered over several days
• For multiple patients (anticipatory batch compounding) OR
• For 1 patient on multiple occasions (patient-specific batch)
Copyright © 2013-2014 CriticalPoint’s Sterile Compounding Boot Camp™ - All rights reserved
High Risk
Medium Risk
Low Risk
Low Risk with 12 h BUD
Immediate Use
Example: Parenteral Nutrition or Batch of IV minibags/syringes
CSP Microbial Risk Levels (continued)
• Made with non-sterile ingredients and/or using non-sterile containers, devices or equipment
• Prepared from sterile ingredients but exposed to < ISO Class 5 air
• > 6 hour delay from compounding to sterilization
• Purity of components is assumed but cannot be verified by documentation
Copyright © 2013-2014 CriticalPoint’s Sterile Compounding Boot Camp™ - All rights reserved
High Risk
Medium Risk
Low Risk
Low Risk with 12 h BUD
Immediate Use
Example: Morphine sulfate from nonsterile powder for PCA
Single/Multiple Dose Vials
� Definitions of SDV and MDV are in the USP General Notices and Requirements
� Single dose vials: � Opened or punctured in ISO 5
environment may be used for up to 6 hours.
� Opened or punctured in worse than ISO 5 must be used within 1 hour or discarded.
� Single dose ampules must be discarded after opening and not stored for any time period
Copyright © 2008-2014 CriticalPoint® - All rights reserved
Image courtesy www.flickr.com
Multiple Dose Vials
� Multiple dose vials – Contain antimicrobial preservative(s)
� Designed for entry on multiple occasions. � BUD: 28 days after initial entry
unless specified otherwise by the manufacturer.
� Based on USP <51> Antimicrobial Preservative Testing
� Expiration date on vial is based on an unopened, properly stored vial.
Image courtesy of www.pfizerinjectables.ca
Copyright © 2008-2014 CriticalPoint® - All rights reserved
Pharmacy Bulk Package (PBP)� USP <1> Injections
� Sterile preparation for parenteral use that contains many single doses
� Restricted to the preparation of admixtures for infusion or filling empty sterile syringes
� Closure penetrated only once
� Used in a suitable work area such as a laminar flow hood
� Includes a statement limiting the time frame in which the container may be used once it has been entered
Image courtesy of http://www.hospira.com
Copyright © 2008-2014 CriticalPoint® - All rights reserved

4/5/2014
9
Beyond-Use Dating (BUD)
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Parameters for Establishing BUD
� Recognizes the probability of contamination even under best conditions:� Optimal employee performance
� 0.1% (1 contaminated dose out of 1,000)
� Contamination rates published in the literature� 0.3% – 16%
� Patient Safety: Protect patients from dangerous or even fatal overgrowths of microorganisms that may have been accidentally introduced
� Storage time: needs to be greater than zero but less than positive infinity*� (> 0 and < +∞)
* Personal conversation with Dr. David W. Newton, September 30, 2009
Copyright © 2008-2014 CriticalPoint® - All rights reserved
Microbiological Beyond Use Dating
Copyright © 2008-2014 CriticalPoint® - All rights reserved
Achieving a State of Control
� Hand Hygiene, Garbing, Aseptic technique
� Training
� Facility design, Environmental Control
� Environmental Sampling
� Cleaning
� Standard Operating Procedures
� Components
� Sterilization, Quality Release Checks
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
� Hand washing is defined as the vigorous, rubbing together of all surfaces of soap lathered hands (30 sec.), followed by rinsing under a
stream of water.
� The process of hand washing mechanically removes microorganisms of the hands.
� The single most important way to reduce the risk of transmitting microorganisms causing
infections.
� Even after using antimicrobial soap, there is still
about 20,000 microbes per sq. mm left on the hands.¹
Hand Hygiene - USP <797>
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
K1
Ability of Hand Hygiene Agents to Reduce Bacteria on Hands
Adapted from: Hosp Epidemiol Infect Control, 2nd Edition, 1999.
0.0
1.0
2.0
3.0 0 60 180 minutes
0.0
90.0
99.0
99.9log%
Bac
teria
l Red
uctio
n
Alcohol-based handrub(70% Isopropanol)
Antimicrobial soap(4% Chlorhexidine)
Plain soap
Time After Disinfection
Baseline
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

Slide 53
K1 Add reference on where this data is from.Keith, 3/16/2014

4/5/2014
10
Compounding Personnel� Hair net
� Beard cover and face mask
� Gown
� Nonsterile
� Gloves
� Sterile
� Shoe covers
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Critical Factors in Aseptic Technique
Synder SL, Van Scoik S, et al. Assessing Contamination Rates of Medium-Risk Compounding With Sterile vs. Non-sterile Gloves in a community Hospital-2011 ASHP MCM Poster-NOLA
Critical Factors in Aseptic Technique
Synder SL, Van Scoik S, et al. Assessing Contamination Rates of Medium-Risk Compounding With Sterile vs. Non-sterile Gloves in a community Hospital-2011 ASHP MCM Poster-NOLA
6% contamination-sterile gloves
24% contamination-nonsterile gloves
Importance of Garbing
Used with permission: Particle Measuring Systems
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Is this an example of USP 797 compliant garbing ?
Yes
No
A
B
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Appearance of Personnel
� Neat, clean
� In good health
� No visible piercing
� No makeup
� No long or artificial nails
� Properly garbed
� Cleanroom vs. other areas
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
11
Compounding Personnel� Hair net
� Beard cover and face mask
� Gown
� Nonsterile
� Gloves
� Sterile
� Shoe covers
ClinicalIQ Content Copyright 1999-2013 ClinicalIQ, LLC - all rights reserved
Personnel
� Compounding supervisor
� Compounding personnel
� Orientation
� Training
� Didactic
� Hands-on
� Tests
� Written
� Related to compounding practices
� Skills assessment
Image: Courtesy CriticalPoint, LLC
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Personnel Monitoring
Aseptic Media Fill Testing
Gloved Fingertip
Testing
Surface Sampling
Images courtesy of CriticalPoint, LLC
Media Fill
� Demonstrates the ability to aseptically mix a CSP
� Must reflect the most complex process performed
Image courtesy of CriticalPoint, LLC
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Gloved Fingertip Test
� Demonstrates the ability to garb aseptically
� USP <797> Appendix III
� Requires
� Appropriate agar plates
� Personnel garbed, including sterile gloves
� Control plate
� Performed in cleanroom or
anteroom immediately after donning sterile gloves but before cleansing them with
sterile 70% IPA
Image courtesy of CriticalPoint, LLC
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Facilities & Environmental Control

4/5/2014
12
Environmental Controls
� Aimed at creating ISO 5, 7, and 8 environments
� ISO 5 – LAFW, BSC, CAI, CACI are “Primary Engineering Controls”
� Must maintain ISO 5 during dynamic (in use) working conditions
� Unidirectional airflow required
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Environmental Controls
� ISO 7 buffer area and ISO 8 ante area – are “Secondary engineering controls”
� Must maintain ISO 7 or 8 during dynamic (in use) working conditions
� Airflow and balance testing required at the installation site
� Only personnel and materials essential for compounding and cleaning are permitted
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Primary Engineering Controls
Direct Compounding Area (DCA)
ISO Class 5Primary Engineering Control (PEC)
Laminar Air Flow Workbench (“Hood”)
Biological SafetyCabinet (“Hood”)
Compounding Aseptic Isolator(“Glovebox”)
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Air Cleanliness
� ISO classification� The smaller the number, the
cleaner the air
� Refers to number of particles allowed per volume of air
� PEC = ISO 5� Buffer area = ISO 7� Ante area
� ISO 8 if it opens only into a positive pressure cleanroom
� ISO 7 if it opens into a negative pressure cleanroom
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Cleanliness Classification Comparison
� Class limits for sterile compounding based on the number of particles ≥ 0.5µm per m3 (ISO) or per ft3 (former Federal
Standard 209E)• Count locations are determined based on room size and
classification and are measured under dynamic operating conditions.
ISO Class US FS 209E ISO m3 FS 209e (ft3)
3 Class 1 35.2 1
4 Class 10 352 10
5 Class 100 3500 100
6 Class 1000 35,200 1000
7 Class 10,000 352,000 10,000
8 Class 100,000 3,520,000 100,000
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
LAFW
Facility Design� If differential pressure design, then pressure
gauges installed and monitored at least daily:
� Buffer � anteroom (0.02” w.c. positive or 0.01” negative)
� Anteroom �non-classed (0.02” w.c. positive)
� If open concept (air displacement design):
� Velocity across entire opening maintains 40 feet/minute and verified by smoke
� Not allowed if HD compounding
� Air Cleanliness
� Buffer ISO Class 7
� Anteroom ISO Class 7/8
� Air Exchanges
� Buffer room: at least 30 ACPH with 15 of those from HEPA filtered air supplied to room
� Ante-area: no requirement but at least 20 ACPH common
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
4/5/2014
13
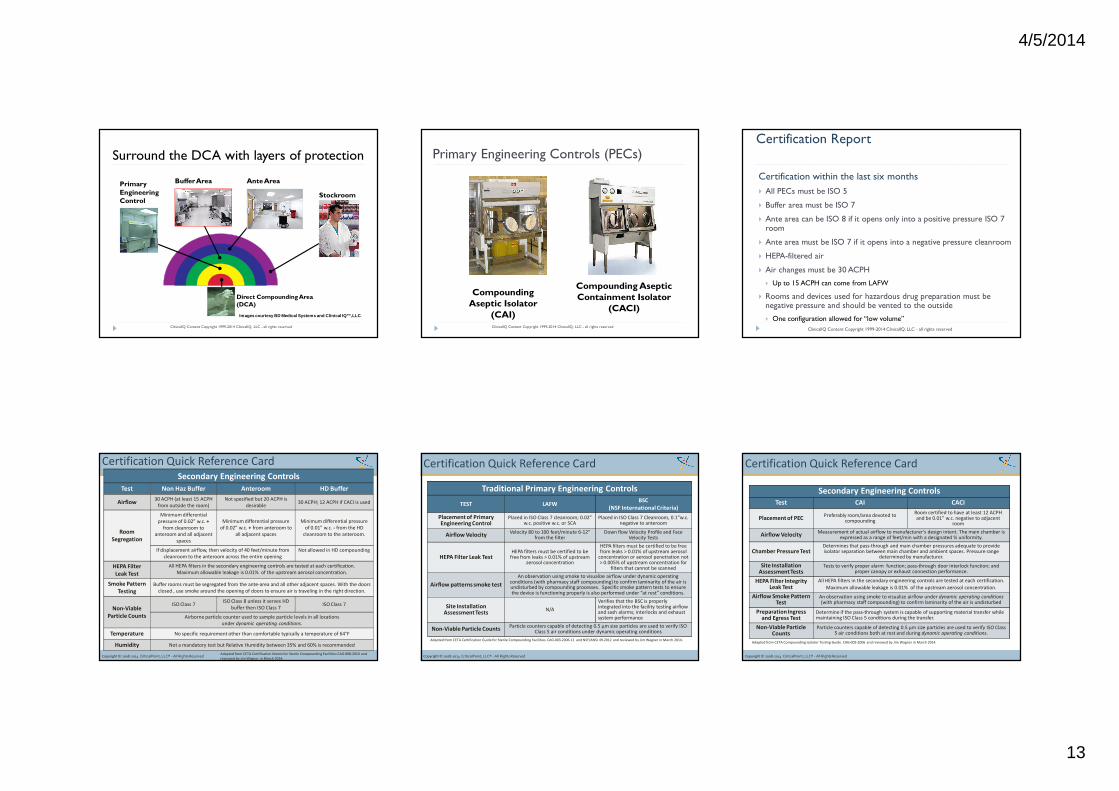
Surround the DCA with layers of protection
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Ante AreaBuffer AreaPrimary Engineering Control
Stockroom
Direct Compounding Area (DCA)
Images courtesy BD Medical Systems and Clinical IQ™, LLC .
Primary Engineering Controls (PECs)
Compounding Aseptic Isolator
(CAI)
Compounding Aseptic Containment Isolator
(CACI)
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
� Certification within the last six months
� All PECs must be ISO 5
� Buffer area must be ISO 7
� Ante area can be ISO 8 if it opens only into a positive pressure ISO 7 room
� Ante area must be ISO 7 if it opens into a negative pressure cleanroom
� HEPA-filtered air
� Air changes must be 30 ACPH
� Up to 15 ACPH can come from LAFW
� Rooms and devices used for hazardous drug preparation must be negative pressure and should be vented to the outside
� One configuration allowed for “low volume”
Certification Report
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Copyright © 2008-2014 CriticalPoint, LLC® - All Rights Reserved
Certification Quick Reference Card
Secondary Engineering Controls
Test Non Haz Buffer Anteroom HD Buffer
Airflow30 ACPH (at least 15 ACPH
from outside the room)
Not specified but 20 ACPH is
desirable30 ACPH; 12 ACPH if CACI is used
Room
Segregation
Minimum differential
pressure of 0.02” w.c. +
from cleanroom to
anteroom and all adjacent
spaces
Minimum differential pressure
of 0.02” w.c. + from anteroom to
all adjacent spaces
Minimum differential pressure
of 0.01” w.c. - from the HD
cleanroom to the anteroom.
If displacement airflow, then velocity of 40 feet/minute from
cleanroom to the anteroom across the entire opening
Not allowed in HD compounding
HEPA Filter
Leak Test
All HEPA filters in the secondary engineering controls are tested at each certification.
Maximum allowable leakage is 0.01% of the upstream aerosol concentration.
Smoke Pattern
Testing
Buffer rooms must be segregated from the ante-area and all other adjacent spaces. With the doors
closed , use smoke around the opening of doors to ensure air is traveling in the right direction.
Non-Viable
Particle Counts
ISO Class 7ISO Class 8 unless it serves HD
buffer then ISO Class 7ISO Class 7
Airborne particle counter used to sample particle levels in all locations
under dynamic operating conditions.
Temperature No specific requirement other than comfortable typically a temperature of 64°F
Humidity Not a mandatory test but Relative Humidity between 35% and 60% is recommended
Adapted from CETA Certification Matrix for Sterile Compounding Facilities CAG-008-2010 and
reviewed by Jim Wagner in March 2014.Copyright © 2008-2014 CriticalPoint, LLC® - All Rights Reserved
Certification Quick Reference Card
Adapted from CETA Certification Guide for Sterile Compounding Facilities. CAG-003-2006-11 and NSF/ANSI 49-2012 and reviewed by Jim Wagner in March 2014.
Traditional Primary Engineering Controls
TEST LAFWBSC
(NSF International Criteria)
Placement of Primary Engineering Control
Placed in ISO Class 7 cleanroom; 0.02” w.c. positive w.c. or SCA
Placed in ISO Class 7 Cleanroom, 0.1”w.c. negative to anteroom
Airflow VelocityVelocity 80 to 100 feet/minute 6-12”
from the filterDown flow Velocity Profile and Face
Velocity Tests
HEPA Filter Leak TestHEPA filters must be certified to be
free from leaks > 0.01% of upstream aerosol concentration
HEPA filters must be certified to be free from leaks > 0.01% of upstream aerosol
concentration or aerosol penetration not > 0.005% of upstream concentration for
filters that cannot be scanned
Airflow patterns smoke test
An observation using smoke to visualize airflow under dynamic operating conditions (with pharmacy staff compounding) to confirm laminarity of the air is undisturbed by compounding processes. Specific smoke pattern tests to ensure the device is functioning properly is also performed under “at rest” conditions.
Site InstallationAssessment Tests
N/A
Verifies that the BSC is properly integrated into the facility testing airflow and sash alarms; interlocks and exhaust system performance
Non-Viable Particle CountsParticle counters capable of detecting 0.5 μm size particles are used to verify ISO
Class 5 air conditions under dynamic operating conditions
Copyright © 2008-2014 CriticalPoint, LLC® - All Rights Reserved
Certification Quick Reference Card
Adapted from CETA Compounding Isolator Testing Guide. CAG-002-2006 and reviewed by Jim Wagner in March 2014.
Secondary Engineering Controls
Test CAI CACI
Placement of PECPreferably room/area devoted to
compounding
Room certified to have at least 12 ACPH and be 0.01” w.c. negative to adjacent
room
Airflow VelocityMeasurement of actual airflow to manufacturer’s design intent. The main chamber is
expressed as a range of feet/min with a designated % uniformity.
Chamber Pressure TestDetermines that pass-through and main chamber pressures adequate to provide isolator separation between main chamber and ambient spaces. Pressure range
determined by manufacturer.
Site InstallationAssessment Tests
Tests to verify proper alarm function; pass-through door interlock function; and proper canopy or exhaust connection performance.
HEPA Filter IntegrityLeak Test
All HEPA filters in the secondary engineering controls are tested at each certification.
Maximum allowable leakage is 0.01% of the upstream aerosol concentration.
Airflow Smoke PatternTest
An observation using smoke to visualize airflow under dynamic operating conditions (with pharmacy staff compounding) to confirm laminarity of the air is undisturbed
Preparation Ingress and Egress Test
Determine if the pass-through system is capable of supporting material transfer while maintaining ISO Class 5 conditions during the transfer.
Non-Viable Particle Counts
Particle counters capable of detecting 0.5 μm size particles are used to verify ISO Class 5 air conditions both at rest and during dynamic operating conditions.

4/5/2014
14
What’s Wrong with This Picture?
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Environmental Sampling
Environmental Sampling Dilemma:
� One of the most contentious section of USP Chapter <797>
� Since the 1980’s, the US Centers for Disease Control (CDC) has not advocated routine microbial environmental culturing (sampling) of inanimate surfaces in the absence of an outbreak situation
� The US Food and Drug Administration requires sterile processing operations in manufacturing facilities to perform daily monitoring of viable air, surface and personnel glove fingertip samples
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Environmental Sampling
� Environmental Sampling section has been separated into a facility-related performance metric and a personnel –related performance metric
� Facility-related Environmental Sampling� Viable air sampling via volumetric method (impaction) to
occur at least every 6 months
� Personnel-related Environmental Sampling � Personnel fingertip sampling during initial training, with
media fills and as a competency assessment tool
� Surface sampling for viable microorganisms
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
General Environmental Sampling “Shalls”� Detailed written PnP on
all aspects of environmental sampling
� Sampling occurs in all ISO areas from cleanest to dirtiest ISO 5 � ISO 7 �ISO 8
� CFU Action Levels established
� Evidence of logical plan of action in the event sampling exceeds Action Levels
CFU/m3 air/plate(1000 liters) If < 1000 liters air sampled, convert to equivalent AL (e.g., 400 liter sample in ISO Class 7 then AL = >4 CFU/plate)
Classification
Volumetric
Air Sample
Required*
ISO Class 5 > 1
ISO Class 7 > 10
ISO Class 8 > 100
Table 2 in Chapter <797>
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Growth Media� Soybean Casein Digest Media
(Trypticase Soy Broth/Agar) to support the growth of bacteria
� Malt Extract Agar or other media
that supports the growth of fungi
� Must use plates with lecithin and polysorbate 80 which are
chemicals that neutralize cleaning agents when performing:
� Surface sampling
� Personnel glove sampling associated with MFUs
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Sampling for Air Viable Organisms� Volumetric air sampling is required
� Predefined amounts of air
� Settling Plates cannot be the only method of evaluating air viable organisms
� Not qualitative
� Settling of particles influenced by size of particle and air movement
Courtesy of MSI, Inc. Houston, TX(www.microbiologyspecialists.com)
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
15
Environmental Sampling
� Designed to demonstrate that the primary and secondary engineering controls, disinfecting procedures, and work practices result in a suitable environment for aseptic compounding
� Utilizes several approaches to assess and evaluate:� Total particle counts
� Air viable organism cfu
� Surface viable organism cfu
� Finger touch plates
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Environmental Monitoring Trending
Courtesy of msi®
86 ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Environmental Sampling
“Regardless of the number of cfuidentified in the pharmacy, further corrective actions will be dictated by the identification of micro-organisms recovered (at least the genus level) by an appropriate credentialed laboratory of any microbial bioburden…”
USP Chapter <797> USP 34-NF 29
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
CFU Identification and Sources
Microorganisms (gram stain/ morphology)
Indication
• Staphylococcus/ Micrococcus
• Personnel habits or gowning problems
• Gram negative rods • Water condensation, leaking, aerosols
• Bacillus species • Dust, dirt, floor traffic, possible air handling
• Molds • Influx of unfiltered air, mold from street clothing or mold-contaminated cardboard, water reservoir, i.e. incubator humidification system
• Yeast • Possible outdoor air influx; clothing-borne, especially in late summer/ fall; possible human contaminant
• Diptheroids/ coryneforms • Poor air conditioning (leading to sweating and personnel discharge from gowns)
Source: Microbiological Environments (www.microbioenv.com)
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Cleaning and Disinfection
� Routine cleaning & disinfection decreases the overall bioburden in the compounding area therefore reducing the risk of contamination to CSPs.
� It is one part of an overall quality management plan. Other components include:� Design/function of primary and
secondary engineering controls
� Material/component handling procedures
� Personnel hand hygiene and garbing
� Environmental sampling/testing
Images courtesy ClinicalIQ™, LLC.
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
What is the difference between cleaning, sanitization and disinfection?
� Cleaning
� Cleaning is the removal of visible soil (e.g., organic and inorganic material) from objects and surfaces and normally is accomplished manually or mechanically using water with detergents or enzymatic products.
� Sanitizing
� Chemical process of reducing the number of disease-causing germs on cleaned surfaces to a safe level.
� Disinfecting
� Disinfection describes a process that eliminates many or all pathogenic microorganisms, except bacterial spores, on inanimate objects.
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
16
Use of Disinfectants
� Must be germicidal detergent
� Dilution of agent is critical to its efficacy
� Contact time
� Storage conditions: light or temperature sensitive
� Follow manufacturer instructions
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
What cleaning supplies do you recommend using?
� Cleaning & disinfecting agents
� Mop(s) and, if necessary, bucket(s)
� Non-shedding, non-linting wipes
� Pre-saturated and dry
� Polyester knit fabrics
� Nylon fabrics
� Isolator cleaning tools
� Equipment should be dedicated!!
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
More than Daily* Daily MonthlyISO Class 5 PEC & work surfaces
• Beginning of day/shift
• Prior to each batch
• Every 30 min
• When visibly soiled
• As spills occur
• Suspect contamination
Empty trash as needed
Empty trash
ISO Class 5 PEC**
Easily cleanable horizontal surfaces in ante and cleanrooms (including pass-through counter)
Restock daily supply cart
Floors from furthest location in cleanroom out thru anteroom (including pass-through floor)
Empty trash
Ceiling
Walls, Pass-throughs
Every surface
• Outside of PECs
• All carts (top, bottom, wheels, etc.)
• Supply bins
• Doors, handles, vents
ISO Class 5 PEC**
Restock supply cart
Floors (same as daily)
Clean refrigerators, freezers, incubators, etc.
* Clean PEC with sterile 70% IPA** Clean with germicidal detergent diluted with SWf Irrigation followed by sterile 70% IPA; use decontamination first agent if HD PECRed represents best practice recommendation; Black indicates 797 required
Cleaning and Disinfection
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
"For 42 years, I made small, regular deposits of education, training and experience ... and the expe rience balance was sufficient that on January 15th I could make a sudden, large withdrawal”
Chesley Sullenberger
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Standard Operating Procedures or Policies and Procedures
� Available to staff
� Evidence of review
� Reflects current practice and regulatory requirements
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Quality Assurance Plan
� Facilities
� Daily logs
� Certification report
� Variances and actions taken
� Gap analysis
Images courtesy of ClinicalIQ, LLC
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
17
� Sterility Testing
� High risk level CSPs prepared in groups > 25 identical individual SDCs or in MDC for administration to multiple patients
� High risk level CSPs prepared and exposed for > 12 hours to temperatures of 2-8°C or > 6 hours at temperatures > 8°C before they are sterilized.
� When assigned BUDs exceed the storage times published in USP Chapter 797 (regardless of compounding risk level)
� Endotoxin (pyrogen)
� Required for all above except inhalation and ophthalmic dosage forms
Testing Required
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Understanding all of the elements
ASSUMPTION!CSP is stored at its optimal temperature at all times.
Risk Level
Beyond-Use Dating(point in time)
Chemical Stability
Aseptic technique
Microbial Stability
Due to the inherent low probability that a Sterility Test can detect low levels of contamination in a batch, sterility assurance must always be based on process design and control.
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Garbing� Head, face, shoe covers� Hand hygiene� Gown/Frock� Application of alcohol
based hand rub w/persistent activity
� Sterile Gloves� Sterile Alcohol
Filter integrity testing
Sterilization Cycle Verification
Calibration & Use
Final release checks
Process verification with media
Process Control Metrics
TrainingEnvironment
Related Metrics
Components & Materials
Cleaning & Disinfection
Main
tain
ing a
Ste
rile C
om
po
un
din
g S
tate
of C
on
trol
Component Type (sterile/nonsterile, PBP, SDV, MDV, bulk API)
Material Handling Processes� Formulary Development� Drug/Supply Procurement� Standardization of
compounding practices and batch records
� Inventory control� Staging/Double-check� Sanitize components� Area Clearance� Reconciliation� Labeling, Storage, Transport
CSP Testing� Strength (Potency) Testing� Sterility Testing� Bacterial Endotoxin Testing
Personnel Related Metrics
Documentation
Selection cleaning and disinfecting agents
Equipment and supplies
Program of cleaning activities
Documentation
Equipment
Non Viable Particle Counts
Training & Competency Verification� Fundamental Principles� Aseptic Technique/Media Fill
Units with GFS� Hand Hygiene/Garbing/GFS� Conduct inside ISO
environments� Cleaning/Material handling� SOPs
Facility
Air Cleanliness via HEPA, ACPH, & Pressure Differential/Displacement
Design Requirements
Materials/ConstructionPrimary/Secondary Engineering Control Certification
Viable Sampling1.Gloved Fingertip Sampling (GFS)
2.Surface Sampling
3.Volumetric Air Sampling
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
� NIOSH Hazardous
� Not EPA hazardous
� Separate area
� Negative pressure
� 12 ACPH
� Can be inside negative pressure buffer area
Storage – Hazardous Drugs Major Differences between USP <797> and Proposed <800>
USP <797>Pharmaceutical Compounding
-Sterile Preparations
Proposed New Chapter USP <800>Hazardous Drugs
-Handling in Healthcare Settings
Applies to sterile compounding onlyApplies to sterile and nonsterile
compounding
Applies from receipt of inventory up to drug administration
Wider continuum of timeApplies from receipt of inventory through
drug administration
All HDs must be stored separatelyin area with 12 ACPH and
0.01” negative to adjacent space
Antineoplastic HDs must be stored separately from non-HDs in an area with 12 ACPH and 0.01” negative to adjacent
space unless coated, final-manufactured dosage forms are clearly labeled as HDs and safety strategies are detailed in PnPs
Exemption for low volume compounding No low volume exemption
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved
Major Differences between USP <797> and Proposed <800>
USP <797>Pharmaceutical Compounding
-Sterile Preparations
Proposed New Chapter USP <800>Hazardous Drugs
-Handling in Healthcare Settings
CSTD use is a “should”CSTD use is a “shall” during administration as
long as dosage form permits
Defines PECs for HDsterile compounding
Defines PECs for nonsterile and sterile HD compounding; allows for manipulation of HDs
that do not produce aerosols (e.g., coated
tablets or capsules) outside of a C-PEC
Prohibits SCA for HD compounding; Requires BSC to be housed in ISO
class 7 room air that is
0.01” w.c. negative
Permits SCA for HDs provided CACI/BSC in area that has 12 ACPH and 0.01” w.c. negative;
Maximum BUD 12 hours
Does not require environmental and medical surveillance
Requires environmental and medical surveillance
ClinicalIQ Content Copyright 1999-2014 ClinicalIQ, LLC - all rights reserved

4/5/2014
18
Review of USP <795> Pharmaceutical Compounding-
Nonsterile Preparations
Eric S. Kastango, MBA, RPh, FASHP
Non-Sterile Compounding
� USP <795> Pharmaceutical Compounding –Nonsterile Preparations
� Other USP Chapters related to compounding
� State regulations concerning compounding
104
USP <795> is a minimum standard – not a guideline
Who Compounds Nonsterile Preparations?
� USP <795> defines compounder as a professional authorized by the appropriate jurisdiction to perform compounding pursuant to a prescription or medication order by a licensed prescriber � Pharmacists� Pharmacy Technicians� Physicians� Veterinarians� Veterinary Technicians� Nurses
105
Status of USP <795>
� Revised Chapter official as of June 2011
� USP Compounding Expert Committee
� Revision process for all new and revised USP chapters
� Published in Pharmacopeial Forum for public comment
� Other related Chapters
� Chapter <800> Hazardous Drugs – Handling in Patient Care Settings – Published for comment on March 28, 2014
� Chapter <1168> Compounding for Investigational Studies – to be proposed in PF 39(5) Sept/Oct 2013
106
Sections of USP <795> …� Introduction
� Definitions
� Categories of Compounding
� Responsibilities of the Compounder
� Compounding Processes
� Compounding Facilities
� Compounding Equipment
� Component Selection, Handling, and Storage
107
… Sections of USP <795>� Stability Criteria and Beyond-Use Dating
� Packaging and Drug Preparation Containers
� Compounding Documentation
� Quality Control
� Patient Counseling
� Training
� Compounding for Animal Patients
108

4/5/2014
19
Compounding Categories
Personnel Facilities Components
Stability Criteria Documentation Quality Control/Assurance
Major Elements of the Chapter
109
Categories of Compounding
� Simple
� Moderate
� Complex
Categories of Compounding
111
Simple Compounding
� Reconstituting or manipulating a commercial product that may require the addition of one or more ingredients as directed by the manufacturer
� A preparation that has a USP compounding monograph or appears in a peer-reviewed article that contains
� Specific quantities for all components
� Compounding procedures and equipment
� Stability data for that formulation with beyond-use date (BUD)
112
USP Compounding Monographs
113
www.usp.org/usp-healthcare-professionals/compounding/compounding-monographs/usp-nf-monographs-compounded-preparations
� Making a preparation that requires special calculations or procedures to determine quantities of components per preparation or per individualized dosage units
� Making a preparation for which stability data for that specific formulation is not available
� Example: mixing two or more manufactured creams when the stability of the mixture is not known
Moderate Compounding
114

4/5/2014
20
� Making a preparation that requires special training, environment, facilities, equipment, and procedures
� Examples
� Transdermal dosage forms
� Modified-release preparations
Complex Compounding
115Image courtesy CriticalPoint, LLC
Responsibilitiesof the Compounder
Responsibility of the Compounder
� The compounder must be proficient in compounding
� The compounder must prepare compounds
� with acceptable strength, quality, and purity
� in accordance with the prescription or medication order
� the finished preparation with appropriate packaging and labeling
� in compliance with established state agencies, state boards of pharmacy, federal law, and other regulatory agencies
117
It’s Not Just USP <795>
118
<LOCATION> TITLE
General Notices
17 Prescription Container Labeling
659 Packaging and Storage Requirements
797 Pharmaceutical Compounding - Sterile Preparations
1066 Physical Environments that Promote Safe Medication Use
1151 Pharmaceutical Dosage Forms
1160 Pharmaceutical Calculations in Prescription Compounding
1163 Quality Assurance in Pharmaceutical Compounding
1178 Prescription Balances and Volumetric Apparatus
1191 Stability Considerations in Dispensing Practice
1265 Written Prescription Drug Information - Guidelines
General Principles of Compounding
119
� Training and documentation
of competence
� Compounding ingredients
� Equipment
� Facilities
� Quality control and assurance
� Error prevention
� Documentation
Image copyright Lisa F Young, 2013
Personnel Training
120

4/5/2014
21
Orientation and Training
� USP <795>
� Other applicable USP Chapters
� Safety Data Sheets (SDS, formerly MSDS)
� Hazardous Drug safety
� Facility policies and procedures
� Oversight by skilled compounder
� Demonstration of verbal and functional knowledge
� Review and approval by compounding supervisor
� Documentation of competence
� Annual review of skills
121
Policies and Procedures
� Available to staff
� Evidence of review
� Reflects current practice and regulatory requirements
122
Component Selection, Handling, and Storage
Definitions
� API: Active Pharmaceutical
Ingredient
� The active ingredient
� Added Substances
� Inactive ingredients, excipients, pharmaceutical ingredients
� Vehicle
� Carrier or diluent in which liquids, semisolids, or solids are
dissolved or suspended
124
API and Other Bulk Substances
� Best option: USP, NF or FCC (Food
Chemical Codex) substances manufactured in an FDA registered facility
� If ingredients from a non-FDA registered facility are required, use professional judgment and obtain a Certificate of Analysis
� Caution with components not of “compendial quality”
� Standards of American Chemical Society (ACS) grade materials are not tested for impurities that might raise patient safety
concerns
125
Certificate of Analysis
126

4/5/2014
22
Dietary and Nutritional Supplements
� Must comply with any federal or state regulations
� Generally, dietary supplements are prepared from ingredients that meet USP, NF, or FCC standards
� If not, must have acceptable food-grade quality
127
Expiration Date of Bulk Components
� If there is no expiration date
� Label with the date of receipt
� Assign a conservative expiration date
� Cannot exceed three years from date of receipt
128
Water
� Potable water
� Hand washing
� Equipment washing
� Purified Water
� Is a “shall” requirement for compounding
� Is a “should” requirement for rinsing equipment and supplies
� Methods of purification include: deionization, distillation, ion exchange,
reverse osmosis, filtration, etc.
129
Image courtesy CriticalPoint, LLC
Storage
� Must be stored as directed by
the manufacturer or according to USP, NF, or FCC monograph requirements
� Appropriate temperature and humidity
� Labeled appropriately
� Off the floor
� Handled and stored to prevent contamination
� Rotated so that oldest stock is used first
130
Image courtesy CriticalPoint, LLC
USP Temperature Ranges
131
Storage TemperaturesDegrees
FahrenheitDegrees
Centigrade
Controlled Room Temperature 68 to 77 20 to 25
Refrigerator 36 to 46 2 to 8
Freezer -13 to 14 -25 to -10
CompoundingFacilities

4/5/2014
23
Facilities
� Adequate space specifically designed for compounding
� Separate and distinct from sterile preparation area
� Clean, orderly, sanitary and in good state of repair
� Orderly placement of equipment and materials
� Designed, arranged, and used to prevent cross-contamination
� Well-lighted
� Appropriate heating, ventilation, air conditioning
133
Facilities
� Hand and equipment washing facilities
� Hot and cold water
� Soap or detergent
� Air-dryer or single-use towels
� Plumbing system
134
Image courtesy CriticalPoint, LLC
Stock
� Component, container, and closure stock stored off the floor
� Rotated so oldest stock used first
135Image courtesy CriticalPoint, LLC
Waste
� Waste held and disposed of in sanitary and timely manner
� In accordance with local, state, and federal guidelines
136 Image courtesy CriticalPoint, LLC
CompoundingEquipment
Equipment and Utensils
� Appropriately designed
� Adequate capacity
� Surfaces that contact components are not reactive, additive, nor sorptive
� Are maintained as directed by the manufacturer
� Refer to USP <1176> Prescription Balances and Volumetric Apparatus
� Routinely inspected
� Calibrated, if necessary
138

4/5/2014
24
Equipment for Special Compounds
� When possible, equipment should be dedicated for specific uses
� Antibiotics
� Cytotoxics
� If not dedicated equipment, the equipment and utensils used are meticulously cleaned
� If possible, disposable items are used to reduce chance of bioburden and cross-contamination
139
Containers and Packaging
Containers and Closures
� Suitable, clean material
� Non-reactive
� Cannot alter quality, strength, or purity
141
Image copyright khuntapol, 2013
USP Standards: Containers and Packaging
142
<LOCATION> TITLE
General Notices and Requirements
Compounding Monographs
659 Packaging and Storage Requirements
660 Containers - Glass
661 Containers - Plastic
671 Performance Testing
681Repackaging into Single-Use Containers and Unit Dose Containers for Nonsterile Solid and Liquid Dosage Forms
1136 Repackaging – Unit-of-Dose
Stability Criteria and BUDs
143
Beyond-Use Dates
144
Traditional Current
Chemical stabilityof the drug
Chemical stability of the compounded preparation
Based on drug-specific & general stability documentation/literature to
reduce potential of falling outside
required USP strength(+/- 10% of labeled content)
Stability in Container
Expected Storage conditions
Competent Personnel

4/5/2014
25
Stability of Compounded Nonsterile Preparations
� Manufacturer’s information
� Package insert
� USP
� Compounding monographs
� All applicable USP General Notices and Chapters
� Peer-reviewed literature
145
BUD by Type of Formulation
�
146
Type of Formulation Maximum BUD
Non-aqueous formulation 6 months
Water-containing oral formulations14 days under refrigeration
Water-containing topical/dermal and mucosal liquid and semisolid formulations
30 days
The BUD cannot exceed the expiration date ofthe API or any other component
Labeling
147
Patient Notification
� The labeling should indicate that “this is a compounded preparation”
148
This is a compounded preparation
Documentation
Required Documentation
� Master Formulation Record
� Compounding Record
� Standard Operating Procedures
� Safety Data Sheets (SDSs, previously MSDSs)
150

4/5/2014
26
Documentation
� Written or electronic
� Comply with record-keeping requirements of State Board of
Pharmacy
� Documentation is not required when preparing a compound
according to the manufacturer’s labeled instructions
� All other compounds require
� Master Formulation Record
� Compounding Record
151
Image courtesy CriticalPoint, LLC
Master Formulation Record
� Official or assigned name, strength, dosage form
� Calculations and doses
� Ingredients and quantities
� Compatibility and stability info and references
� Equipment needed
� Mixing instructions
� Label information
� Container used
� Packaging and storage requirements
� Description of the final preparation
� Quality control procedures and expected results
152
Compounding Record …
� Official or assigned name, strength, and dosage
� Reference to Master Formulation Record
� Names and quantities of all components
� Sources, lot numbers, and expiration dates of components
� Total quantity compounded
� Names of persons who prepared, performed QC, and approved the preparation
153
… Compounding Record
� Date of preparation
� Assigned control or prescription number
� Assigned BUD
� Copy of label
� Description of final preparation
� Results of QC (weight of capsule, pH of liquid)
� Documentation of any QC issues and any ADRs reported by patient
154
Standard Operating Procedures
� SOPs should include
� Facilities for preparation
� Equipment for packaging
� Personnel
� Storage
� SOPs should ensure
� Accuracy
� Quality
� Safety
� Uniformity in compounding
� Accountability
155
Quality Control
156

4/5/2014
27
Quality Assurance Plan
� Quality Control
� Personnel orientation and training
� Variances
� Trends
157
<1163> Quality Assurance in Pharmaceutical Compounding
� Training
� SOPs
� Documentation
� Verification
� Testing
� Cleaning and disinfection
� Containers, packaging, repackaging, labeling, and storage
� Outsourcing
� Responsible Personnel
158
Patient Counseling
159
Shall Statements: Patient Counseling
� The patient or patient’s agent shall be counseled about proper use and instructed to report any adverse event
160
Image copyright Bellingham, 2013
Critique of North Dakota Rules and Regulations North Dakota Board of Pharmacy Rules
162
� 61-02-01-03. Pharmaceutical compounding standards.
� All compounders of sterile and nonsterile products must be in compliance with this rule by January 1, 2015.
� Abbreviated version of USP Chapters <797> and <795>
� Compounding personnel must be familiar with USP standards and North Dakota regulations:…what is the expectation of this statement?
� No guidance on the specific facility requirements except for CACIs used for hazardous drugs
� No air changes per hours
� No pressure differentials (except for HDs)
� No guidance on environment monitoring and acceptance criteria
4/5/2014
28
North Dakota Board of Pharmacy Rules
163
� 61-02-01-03. Pharmaceutical compounding standards.
� No requirement to do air, surface or gloved fingertip except for high-risk level compounding
� Only air sampling (volumetric or gravimetric)
� No requirement for sterile gloves and sterile IPA
� Lacks specificity making compliance difficult and will make enforcement challenging.
� How will the pharmacist know when their operation and facility is operating under a state of control they?
� …was built correctly?
� How will the Board inspectors know when a pharmacy that is compounding is not complying with the regulation?
Thank you
� Eric S. Kastango, MBA, RPh, FASHP
� 235 Main Street, Ste 292
� Madison, NJ 07940