jy douillard, md, phd, cmo esmo preceptorship programme the role of maintenance treatment...
TRANSCRIPT
ESMO Preceptorship Programme
The role of Maintenance treatmentAppropriate endpoints according to ESMO consensus
JY Douillard, MD, PhD, CMO ESMO
Colorectal Cancer– Singapore-October 20-22 2016

MAINTENANCE THERAPY
• Most patients with mCRC have no hope for cure and will receive several lines of chemo +/-targeted therapies with a median Overall Survival of 30 months
• For patients fit for intensive induction chemotherapy, the optimal sequence and duration are unknown, reduction of treatment intensity is often required for toxicity or patient request
• Quantity of life has improved and Quality of life should be considered
• Maintenance treatment apply after induction to maintain benefit as long as possible
• With lower toxicity regimen
• Improvement of disease control (PFS)
• Not at the detriment of QoL
• Several strategies are available

Available strategies in clinical practice
Induction phase 4-6 months with
controlled disease
Continuous with dose reduction according to toxicity
Intermittent with treatment breaks
Maintenance with less toxic drugs
Disease Progression
Re-induction
2nd – Line
2nd – Line

CONTINUED VS: INTERMITTENT CHEMO
Maughan TS et al. The Lancet 2003 361, 457-464
Induction phase 12 w5FU-based (GM, Lockich)Or Raltitrexed
ORSTB
Continue until PD
STOP and restart PD
Primary endpoint: Overall Survival (OS)
n=354
Comparison of intermittent and continuous palliative chemotherapy for advanced colorectal cancer: a multicentre randomised trial
TS Maughan, MD, RD James, MRCP, DJ Kerr, FRCP, JA Ledermann, MD, MT Seymour, MD, C Topham, MD, C McArdle, FRCS, D Cain, PhD, Mr RJ Stephens
The LancetVolume 361, Issue 9356, Pages 457-464 (February 2003)
DOI: 10.1016/S0140-6736(03)12461-0
CR06

The Lancet 2003 361, 457-464DOI: (10.1016/S0140-6736(03)12461-0) Copyright © 2003 Elsevier Ltd Terms and Conditions
Intermittent Continued
OS median* 10.8 11.3 m ns1y OS % 46 452y OS % 19 13PFS 3.7 4.9 m ns*since randomization

The Lancet 2003 361, 457-464DOI: (10.1016/S0140-6736(03)12461-0) Copyright © 2003 Elsevier Ltd Terms and Conditions

Folfiri Continuous vs Intermittent2 months on/2months off -Stop and Go-
337 patients randomized
• 147 in the final analysis
continuous Folfiri
• 146 in the final analysis
Intermittent Folfiri
ORR : 34 vs.42% (int/cont) (NS)
DCR: 67 Vs. 76% (NS)
Labianca R et al, Annals Oncol 22: 1236-1242, 2011

In this study, discontinuing chemotherapy resulted in: Similar PFS and OS Slightly better QoL Reduced toxicity 10 week less chemotherapy Same incidence of exposure to second line
“Interpretation: Our findings provided no clear evidence of a benefit in continuing therapy indefinitely until disease progression. They showed that it is safe to stop chemotherapy after 12 weeks and re-start the same treatment on progression in patients with chemosensitive advanced colorectal cancer.”
Lancet 2003; 361: 457–64
CONTINUED VS: INTERMITTENT CHEMO
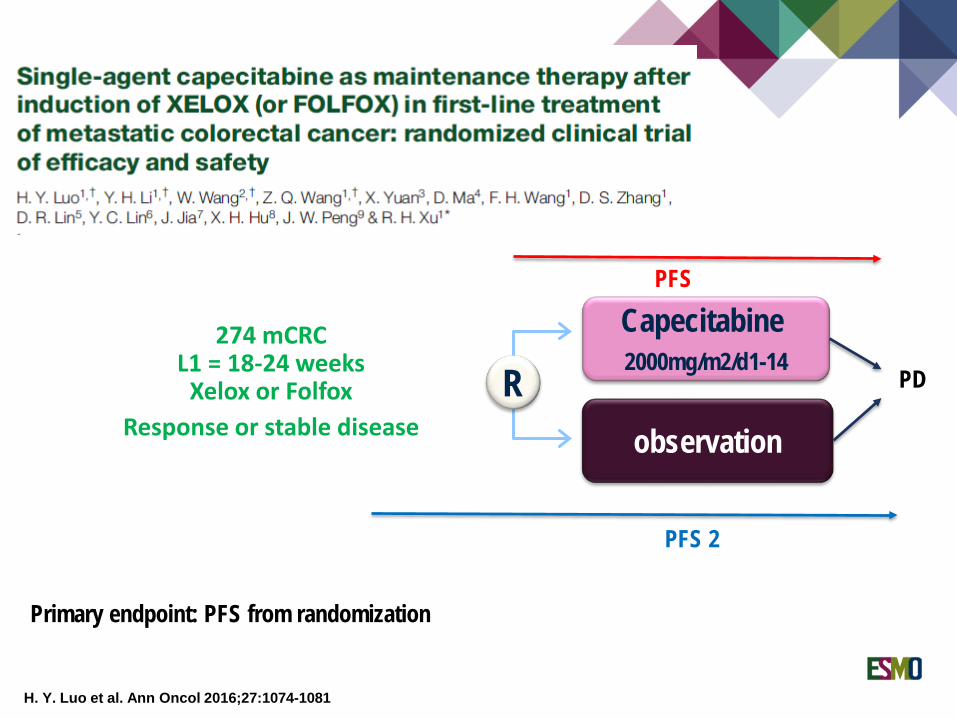
H. Y. Luo et al. Ann Oncol 2016;27:1074-1081
R274 mCRC
L1 = 18-24 weeksXelox or Folfox
Response or stable disease observation
Capecitabine2000mg/m2/d1-14
Primary endpoint: PFS from randomization
PD
PFS
PFS 2

Capecitabine maintenance
H. Y. Luo et al. Ann Oncol 2016;27:1074-1081
PFS from randomization
PFS from induction treatment (PFS2)
overall survival

Maintenance chemotherapy after induction vs. Continuous chemo until PD
Christophe Tournigand et al. JCO 2006;24:394-400

Chemotherapy regimens: (A) FOLFOX4; (B) FOLFOX7; and (C) simplified LV5FU2.
Christophe Tournigand et al. JCO 2006;24:394-400
A (Folfox 4) until PD
B (Folfox 7) (6 cycles)C (LV5FU2 x12)B (Folfox 7)
OPTIMOX 1
B C B
A
Primary End-Point. Duration of Disease Control

Christophe Tournigand et al. JCO 2006;24:394-400
Duration of disease control
Progression-free survival
Overall survival
ConclusionOxaliplatin can be safely stopped after six cycles in a FOLFOX regimen.No difference in PFS and OS, less grade 3-4 toxicity in arm B
Primary End-Point

Comparison of the proportion of patients who developed a grade 3 or 4 toxicity at each cycle.
Christophe Tournigand et al. JCO 2006;24:394-400
©2006 by American Society of Clinical Oncology
Drug exposure: n patients receiving each cycle
N patients with G3-4 toxicity
Neurotoxicity G3-4

mFOLFOX7 x 6, sLV5FU2 maintenance, mFOLFOX7
mFOLFOX7 x 6, chemo-free interval, mFOLFOX7
n = 99
n = 103
R
OPTIMOX 2
Benoist Chibaudel et al. JCO 2009;27:5727-5733
DDC
PFS
OS
mFOLFOX 7 reintroduced at progression
Primary End-Point: DCC
Optimox 2: conclusion• DCC and PFS are improved• OS is not• Similar toxicity in both arms
mFolfox 7: Oxali 100mg/m2

Treatment discontinuation STOP and GO:
Similar PFS and OS Slightly better QoL Reduced toxicity
Maintenance Capecitabine vs Observation: Improved PFS and PFS 2 No benefit on OS
Maintenance with reduced toxicity regimen OPTIMOX Strategy
No alteration or improved DCC and PFS Less toxicity with maintenance due to Oxaliplatin reduction No survival benefit
MAINTENANCE CHEMOTHERAPYCONCLUSION

CONTRIBUTION OF TARGETED AGENT IN MAINTENANCEBevacizumabCetuximab

D. Koeberle et al. Ann Oncol 2015;26:709-714
RmCRC
L1 = 4-6 monthsCT + bev
Response or stable disease pause
bevacizumab 7.5 mg/kg/3 weeks
Primary endpoint: TTP non inferiority

SAKK 41/06Kaplan–Meier curves for time to progression from randomization.
D. Koeberle et al. Ann Oncol 2015;26:709-714
TTP 4.1 vs. 2.9 mHR 0.74 (0.58-0.96)Non-inferiority not demonstrated
OS 25.4 vs. 23.8mP=0.19

R
Maintenance with bevacizumab and capecitabine: CAIRO3
Primary endpoint PFS2 = Delay up to 2nd progression after rechallenge with CAPOX-bevacizumab
Secondary endpoints : PFS1, TTP2, OS TTP2 : time to progression or death after first progression, whatever the treatment used
SD or OR(n = 558)
mCRC Non resectable 1st line OMS 0-1
Observation(n = 279)
PFS2
PFS1
Prog
ress
ion
RechallengeCAPOX-bevacizumab
(n = 212 [76 %])
RechallengeCAPOX-bevacizumab
(n = 131 [47 %])
Prog
ress
ion
CAPOX-bevacizumab
(6 cycles)
Capecitabine + bevacizumab *
(n = 279)
* Capecitabine 625 mg/m2 2 x/j en continu + bevacizumab 7,5 mg/kg i.v. every 3 weeks
Phase III trial DCCG (Dutch Colorectal Cancer Group

Figure 2
The Lancet 2015 385, 1843-1852DOI: (10.1016/S0140-6736(14)62004-3)
CAIRO 3: OUTCOMES
Simkens L et al. The Lancet 2015; 385: 1843-52
PFS 1 PFS 2
Time to 2nd PD OS

Figure 1
The Lancet Oncology 2015 16, 1355-1369DOI: (10.1016/S1470-2045(15)00042-X)

Figure 3
The Lancet Oncology 2015 16, 1355-1369DOI: (10.1016/S1470-2045(15)00042-X)
Failure of strategy
PFS
OS

Figure 8
The Lancet Oncology 2015 16, 1355-1369DOI: (10.1016/S1470-2045(15)00042-X) Copyright © 2015 Elsevier Ltd Terms and Conditions
AIO 0207: Quality of Life
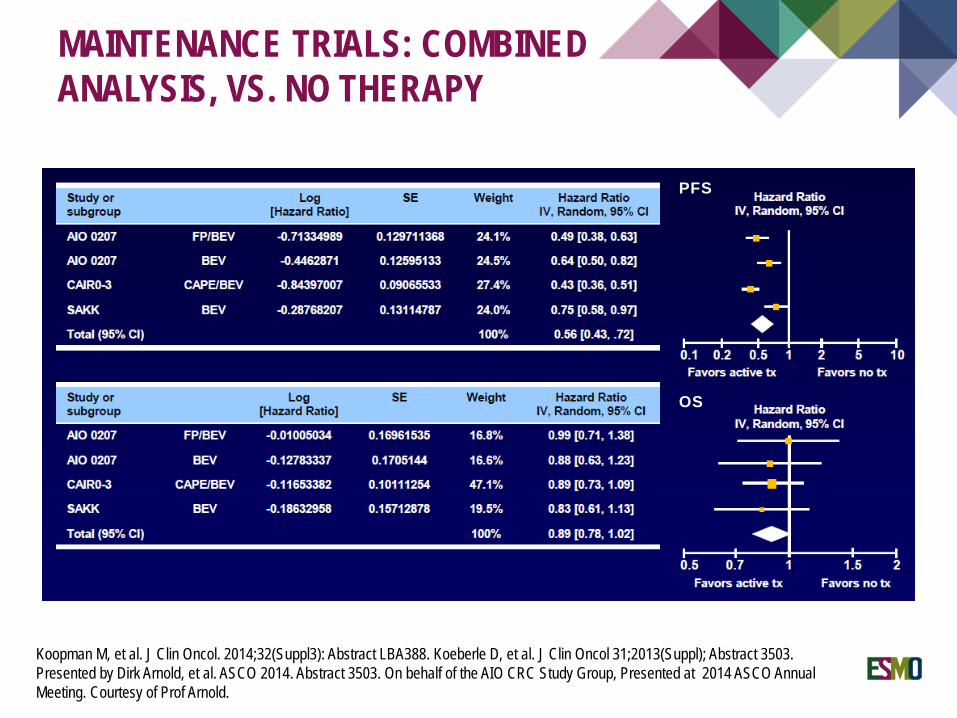
MAINTENANCE TRIALS: COMBINED ANALYSIS, VS. NO THERAPY PFS
PFS
OS
Koopman M, et al. J Clin Oncol. 2014;32(Suppl3): Abstract LBA388. Koeberle D, et al. J Clin Oncol 31;2013(Suppl); Abstract 3503.Presented by Dirk Arnold, et al. ASCO 2014. Abstract 3503. On behalf of the AIO CRC Study Group, Presented at 2014 ASCO AnnualMeeting. Courtesy of Prof Arnold.

CONTRIBUTION OF TARGETED AGENT IN MAINTENANCEBevacizumabCetuximab

Phase II trial, Kras wt exon 2 (later retested for Kras, Nras, Braf)
n=78*
n=91*
• *14/78 and 25/91 did not complete the 12w induction, • result will be expressed on per protocol population, not intent to treat• Imbalanced population for Braf in defavor of the continued arm• 13 patients received Xelox rather than Folfox (5 and 8 in the Contimued arm)
Wasan H et al The Lancet Oncology 2014; 15: 631-39
Primary Endpoint: Failure-Free Survival at 10 months

COIN BFailure Free Survival (Primary Endpoint)
The Lancet Oncology 2014 15, 631-639DOI: (10.1016/S1470-2045(14)70106-8) Copyright © 2014 Wasan et al. Open Access article distributed under the terms of CC BY Terms and Conditions
All Wild-type population:Median FFS (months):Intermittent: 12.3 mContinued: 14.5 m

The Lancet Oncology 2014 15, 631-639DOI: (10.1016/S1470-2045(14)70106-8) Copyright © 2014 Wasan et al. Open Access article distributed under the terms of CC BY Terms and Conditions
COIN BOverall Survival
All Wild-type population:Median OS (months):Intermittent: 18.8 mContinued: 21.7 m

COIN B
Intermittent Folfox-Cetuximab with Cetuximab maintenance: conclusion
• In COIN-B, planned maintenance with cetuximab was associated with• a greater failure-free survival, • a greater progression-free survival, • a greater overall survival, • an improved disease control at 24 weeks, • and a longer chemotherapy-free interval
than was intermittent cetuximab.
• These benefits occurred despite an imbalance of prognostic factors at baseline
• COIN-B was designed as an exploratory, hypothesis generating study to complement COIN.

Bevacizumab with or without erlotinib as maintenance therapy in patients with metastatic colorectal cancer (GERCOR DREAM; OPTIMOX3): a randomised, open-
label, phase 3 trial
Prof Christophe Tournigand, MD, Benoist Chibaudel, MD, Benoit Samson, MD, Prof Werner Scheithauer, MD, Dewi Vernerey, PhD, Paul Mésange, PhD, Gérard Lledo, MD, Frédéric Viret, MD, Jean-François Ramée, MD, Prof Nicole Tubiana-Mathieu, MD, Jérôme Dauba,
MD, Olivier Dupuis, MD, Yves Rinaldi, MD, May Mabro, MD, Nathalie Aucoin, MD, Jean Latreille, MD, Prof Franck Bonnetain, PhD, Prof Christophe Louvet, MD, Annette K Larsen, PhD, Prof Thierry André, MD, Prof Aimery de Gramont, MD
The Lancet OncologyVolume 16, Issue 15, Pages 1493-1505 (November 2015)
DOI: 10.1016/S1470-2045(15)00216-8
Copyright © 2015 Elsevier Ltd Terms and Conditions
Switch maintenance with another EGFR targeting agent

Maintenance: Bev + erlotinib DREAM
Induction, N=700
33
Bevacizumab(7.5 mg/kg /21d)
+ erlotinib(150 mg/d)
until progression
NoProgression
Maintenance, N=446
N=222
Bevacizumab(7.5 mg/kg /21d)
until progression
N=2244.1.07 – 13.10.11
REGISTRATION
mFOLFOX7bevacizumab(59%)
XELOX2bevacizumab(30%)
FOLFIRIbevacizumab(10%)
6 MONTHS
R
Primary Endpoint: PFS after maintenance randomisation (4.5 6.5m)

DREAM OUTCOMES from maintenance
The Lancet Oncology 2015 16, 1493-1505DOI: (10.1016/S1470-2045(15)00216-8) Copyright © 2015 Elsevier Ltd Terms and Conditions
PFS
OS

Berry SR et al, Annals Oncol 26: 477–485, 2015
If maintenance is prefrerred:
ESMO Highlights Copenhagen J.Taïeb

Abst 462

PFS HR 0.63 (0.37-1.08)

41Van Cutsem E et al.

42Van Cutsem E et al.

MAINTENANCE THERAPYIndividualisation and discussion with the patient is essential:
For patients receiving FOLFOX or CAPOX plus bevacizumab-based therapy, consider maintenance therapy after 6–8 cycles with a combination of a fluoropyrimidine plus bevacizumab
Patients receiving FOLFIRI can continue on induction therapy for as long as tumourshrinkage continues and the treatment is tolerable
Bevacizumab as monotherapy is not recommended as maintenance therapy
As overall survival has not been improved by maintenance strategies, treatment holidays are a valid option and should be discussed with the patientPause remains useful in patients with:
Normalisation of CEA Slow-growing tumours Good response to initial therapy…
For patients receiving initial therapy with a single agent fluoropyrimidine (plus bevacizumab) induction therapy should be maintained