journal of issn 1998-2062 - painsa · 2018-06-01 · issn 1998-2062 volume 13 number 1 2018...
TRANSCRIPT

Journal of
The South African Chapter of the IASP
ISSN 1998-2062
Volume 13 Number 1
2018
Surgical interventions for the treatment of painful neuroma: a comparative meta-analysis
Transition from acute to chronic pain after surgery
Innovative treatments for back pain
Day-to-day experience in resolution of pain after surgery
Acute pain management in patients with drug dependence syndrome
The gap between knowledge and practice


Journal of The South African Chapter of the IASPVolume 13 Number 1
Editorial
All correspondence to the editor should be addressed to: [email protected]
The recent “year of” campaign highlighted the need to control post-operative pain. I featured several articles and updates covering this subject and trust that the message reached out to all our members.
It is obvious that in the majority of cases we were dealing with acute nociceptive pain. What was not discussed was the potential development of chronic post-surgical pain (CPSP) syndromes.
The idea that acute pain and chronic pain are two distinct entities has now become outdated. What we now believe is that pain is a continuum from acute to chronic. The old definition of chronic pain commencing at three months has
been replaced with the idea that chronic pain is developing when the expected time period for normal resolution of pain is exceeded.
Is there anything that we as clinicians can do about this problem? The simple answer to this is yes!
There are many factors that can predict CPSP and many of these we can do absolutely nothing about. This includes the age of the patient, the sex of the patient, and the genetic makeup of the patient. We can also have a high index of suspicion that CPSP may develop in catastrophisers and in patients with pre-existing chronic pain syndromes.
Where we can make a difference is ensuring that patients do not experience severe post-operative pain. These patients have a higher probability of developing CPSP than those who have little or no post-operative pain.
Similarly, we need to mange pre-operative pain in patients who are already suffering from pain prior to surgery. These patients also need good pain management prior to the commencement of surgery.
It is beyond the scope of this Editorial to prescribe pain therapy and so I have included paper by Patricia Lavand-homme. The author deal with all the concepts I have highlighted and discusses improvements and advances in the prevention, detection, and management of CPSP.
It is clear that we as clinicians have an essential role to play in not only managing the immediate post-operative pain of our patients, but also the long-term wellbeing of these patients in that we can and must apply our clinical knowledge to ensure that the incidence of CPSP decreases.
Dr. Milton RaffBSc MB ChB FFA(SA)
1

EDITORDr M Raff
BSc (WITS), MBChB (Pret), FFA (SA)
EDITORIAL BOARDProf H Meyer
MBChB(Pret) MPraxMed(Pret) MFGP(SA)
Prof C L Odendaal MBChB, MMed(Anest),
GFN(SA)
Prof D MitchellBSc Hons, MSc, PhD
(all University of the Witwatersrand)
Dr S BaumannBA. Mb.Ch.B.(U.C.T.),
P.G.C.E.(University College of Wales), M.R.C.Psych.(London),
F.C.Psych (S.A.)
Mrs P BergerBSc Physio (Wits), Acup (SA)
Prof E FrohlichMD(Tel-Aviv), DA(SA),
FCA(SA), Master (Med) Pain Management (Syd)
This work is subject to copyright. All rights are reserved, whether the whole or part of the material is concerned, specifically the rights for translation, reprinting reuse of illustrations, broad-casting, reproduction of CD-Rom, microfilm, online publication, or in any other way, and storage in data banks.
The use of registered names trademarks etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt for the relevant laws and regulations and therefore free for general use.
Product liability: the publishers cannot guarantee the accuracy of any information about the publication of medications contained in this publication. In every individual case, the user must check such information by consulting the relevant literature.
PUBLISHER / MEDSPEC PUBLISHING / ADVERTISING & RATES
Reni Rouncivell, Tel: (012) 657 2327 Fax: 086 561 5122, Cell: 082 441 6904, e-mail: [email protected], Private Bag X1036, Lyttelton, South Africa 0140
SUBSCRIPTIONS & ACCOUNTS
Chantal du Toit, Tel: 082 385 5524, e-mail: [email protected]/[email protected]
SYSTEMATIC REVIEW AND META-ANALYSISSurgical interventions for the treatment of painful neuroma: a comparative meta-analysisLouis H. Poppler, Rajiv P. Parikh, Miles J. Bichanich, Kelsey Rebehn, Carrie R. Bettlach, Susan E. Mackinnon, Amy M. Moore
3
BIENNIAL REVIEW OF PAINTransition from acute to chronic pain after surgeryPatricia Lavand’homme
13
BIENNIAL REVIEW OF PAINInnovative treatments for back painG. Lorimer Moseley
18
RESEARCH PAPERDay-to-day experience in resolution of pain after surgeryTimothy T. Houle, Scott Miller, Jason E. Lang, Jessica L. Booth, Regina S. Curry, Lynnette Harris,Carol A. Aschenbrenner, James C. Eisenach
27
PAIN CLINCAL UPDATESAcute pain management in patients with drug dependence syndromeJane Quinlan, Felicia Cox
35
GLOBAL YEAR EXCELLENCE IN PAIN EDUCATIONThe gap between knowledge and practicePaul Wilkinson, Judy Watt-Watson, Daniel B. Carr, Andreas Kopf
42
2
Systematic Review and Meta-Analysis
Surgical interventions for the treatment of painfulneuroma: a comparative meta-analysisLouis H. Popplera, Rajiv P. Parikha, Miles J. Bichanicha, Kelsey Rebehnb, Carrie R. Bettlacha, Susan E. Mackinnona,Amy M. Moorea,*
AbstractA consensus on the optimal treatment of painful neuromas does not exist. Our objectivewas to identify available data and to examinethe role of surgical technique on outcomes following surgical management of painful neuromas. In accordance with the PRISMAguidelines, we performed a comprehensive literature search to identify studies measuring the efficacy of the surgical treatment ofpainful neuromas in the extremities (excluding Morton’s neuroma and compression neuropathies). Surgical treatments werecategorized as excision-only, excision and transposition, excision and cap, excision and repair, or neurolysis and coverage. Data onthe proportion of patients with a meaningful reduction in pain were pooled and a random-effects meta-analysis was performed. Theeffects of confounding, study quality, and publication bias were examined with stratified, meta-regression, and bias analysis. Fifty-four articles met the inclusion criteria, many with multiple treatment groups. Outcomes reporting varied significantly and few studiescontrolled for confounding. Overall, surgical treatment of neuroma pain was effective in 77% of patients [95% confidence interval:73-81]. No significant differenceswere seen between surgical techniques. Among studies with amean pain duration greater than 24months, or median number of operations greater than 2 prior to definitive neuroma pain surgery, excision and transposition orneurolysis and coveragewere significantly more likely than other operative techniques to result in ameaningful reduction in pain (P,0.05). Standardization in the reporting of surgical techniques, outcomes, and confounding factors is needed in future studies toenable providers to make comparisons across disparate techniques in the surgical treatment of neuroma pain.
Keywords: Neuroma, Surgery, Operation, Operate, Reconstruction, Restoration, Procedure, Surgical intervention, Allodynia,Burning, Hyperalgesia, Extremity, Peripheral, Hand, Arm, Leg, Foot, Neurectomy, Transposition, Transpos*, Excision, Excis*, Painrelief, Pain management, Outcome, Analgesia, Treatment outcome, Therapy, Visual analogue scale, VAS, Faces pain scale, Painscale, Quality of life, Health related quality of life, Dash questionnaire, Dash score, Disabilities of the arm shoulder and hand
1. Introduction
Painful neuromas of the peripheral nerves are psychologically andphysically disabling.36 Painful neuroma usually develops followingtrauma or surgery,12,73,92 affecting 2% to 60% of patients witha nerve injury.1,29,34 There is no consensus on the optimaltreatment of painful neuroma. Consequently, numerous modal-ities to treat neuroma pain are described, including pharmaco-logic, psychologic, and physical interventions.66,74,93
The role of surgery in the treatment of painful neuroma remainscontroversial.13,22,30 A wide variety of surgical techniques aredescribed to treat painful neuroma. Studies of these techniques
have been limited by small sample sizes and nonrandomizedcase series study designs; therefore, no definitive answer on theeffectiveness of surgical management of neuroma pain exists.
The purpose of this meta-analysis was to identify and assessthe available information on the outcomes of surgical treatment ofpainful neuromas. Our goals were to determine the overalleffectiveness of surgery, determine whether certain surgicalprocedures are more effective than others, and performconfounding and bias analysis not previously possible becauseof the small patient numbers in most published studies.
2. Methods
2.1. Search strategy
In accordance with the Preferred Reporting Items for SystematicReviews and Meta-Analysis (PRISMA) guidelines, we sought toidentify all clinical studies on surgical treatment of neuroma usinga predesigned protocol for computerized literature search of theonline databases Embase, Scopus, PubMed, Cochrane library,and ClinicalTrials.gov.62 We conducted searches up until June2015 without language restrictions. Search terms were MeSHheadings, text words, and variations of the keywords or phrases:neuroma, pain, peripheral, extremity, operate, management,outcome, visual analogue scale (VAS), quality of life, and theDisabilities of the Arm, Shoulder, and Hand (DASH) question-naire.41 Titles and abstracts were reviewed and articles wereretrieved if they seemed relevant or there was uncertainty.
Sponsorships or competing interests that may be relevant to content are disclosed
at the end of this article.
a Division of Plastic and Reconstructive Surgery, Washington University in St. Louis
School of Medicine, St. Louis, MO, USA, b Department of Orthopaedic Surgery,
Saint Louis University, St. Louis, MO, USA
*Corresponding author. Address: Division of Plastic and Reconstructive Surgery,
Washington University in St. Louis School of Medicine, Campus Box 8238, 660 S.
Euclid Ave, St. Louis, MO 63110, USA. Tel.: 314-454-4894; fax: 314-367-0225.
E-mail address: [email protected] (A.M. Moore).
Supplemental digital content is available for this article. Direct URL citations appear
in the printed text and are provided in the HTML and PDF versions of this article on
the journal’s Web site (www.painjournalonline.com).
PAIN 159 (2018) 214–223
© 2017 International Association for the Study of Pain
http://dx.doi.org/10.1097/j.pain.0000000000001101
214 L.H. Poppler et al.·159 (2018) 214–223 PAIN®
Copyright � 2018 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.3

Retrieved articles were assessed using the inclusion andexclusion criteria, and citation lists of retained articles weresearched for relevant citations.
2.2. Study selection
Studies reporting the efficacy of the surgical treatment of painfulneuromas were included in this meta-analysis. Studies ofneuroma prevalence, primary prevention of neuroma, or mech-anisms of painful neuroma formation were not included in ouranalysis. Studies reporting treatment of neuromas not in theextremities or specifically dealing with nerve compression andMorton’s neuroma (a distinct clinical entity more akin to nervecompression) were excluded. Case-reports, nonsequentialpatient series, and studies only reported in abstract form wereexcluded to reduce selection bias within studies.
Theprimaryoutcomeanalyzedwas theproportionof patientswithmeaningful reduction of pain. Outcomes reporting varied acrossstudies and included patient satisfaction, surgeon examination, andordinal pain scales such as the VAS. Therefore, we defineda meaningful reduction of pain as a pain score reduction of 3 ormore, final visual analogue pain less than 4, or patient or surgeonreport of meaningful improvement as defined in each study.
2.3. Data extraction and validity scoring
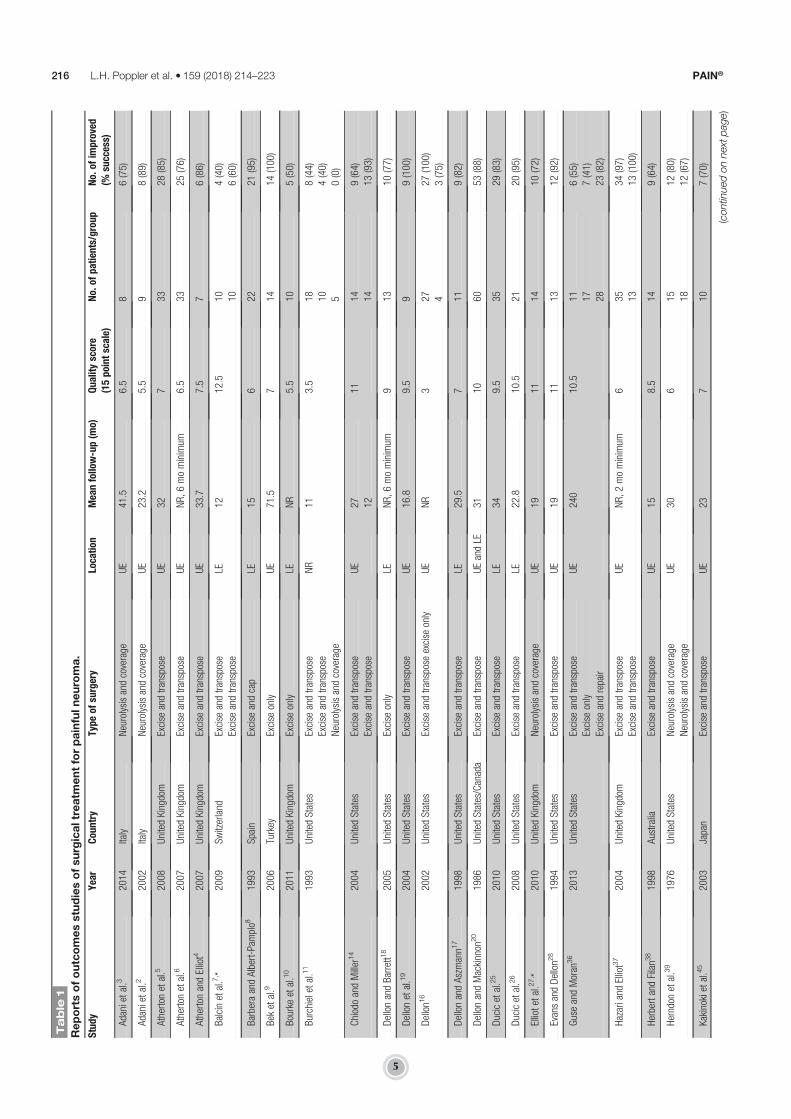
Two authors independently assembled the following informationfor each study: year of publication, period that surgeries wereperformed, surgical technique performed, outcome definition,age range of study population at the time of surgery, duration ofpain symptoms prior to surgery, number of previous neuromapain operations, affected extremity and nerve, and confoundingvariables (socioeconomic status, employment status, workman’scompensation or other litigation, and smoking). Studies weregrouped according to the surgical technique used. Surgicaltechniques were categorized as excision-only, excision and cap(with any device intended to stop regeneration), excision andtransposition (surgical movement of the nerve from its nativecourse into bone, muscle, or vein), excision and repair (direct ornerve graft repair), or neurolysis and coverage with transposedsoft tissue (muscle, fascial, or adipose flap) (Table 1). Wheredisagreement among data extractors arose, adjudication wasaccomplished by a third reader and discussion among authors.
To assess the quality of information in each study, we developeda 15-point scoring technique modeled on the Downs and Blackchecklist for assessing methodological quality of nonrandomizedstudies (Appendix 1, available online as supplemental digitalcontent at http://links.lww.com/PAIN/A506).24 Specifically, weassessed the clarity of the surgery performed, the precision ofthe outcomes reported, whether information on potential con-founders was reported, whether complications of bad outcomeswere reported, and quality of bias analysis. Recognizing thelimitations of quality scoring to account for bias among stud-ies,35,40,43 detailed data were collected on study characteristicsthought most likely to bias study results, namely objectivity of theoutcome reported, follow-up duration, the proportion of patientslost to follow up, and known confounders for successful relief ofpain when available. Using this scale, a higher number equateswith higher quality of information presented.
2.4. Statistical analysis
Raw categorical data from relevant studies were used to calculateproportions with 95% confidence intervals (CIs) of patients who
experienced a meaningful reduction of pain. Individual proportionswere combined by means of DerSimonian-Laird random-effectsmodels, given the variety of surgical techniques, geographiclocations, and patient populations among studies.21,65 A continuitycorrection of 0.1 was used for studies with a proportion of 0 or 1.Cochran Q and Higgins I2 tests were used to assess heterogeneityamong studies. Given the modest statistical power of these tests,we considered heterogeneity as significant if P, 0.1 or I2 . 30%.
We explored sources of heterogeneity with stratified analysis ofgroup differences when significant heterogeneity was notedamong studies for a confounder and when more than 15 studiesreported the confounder of interest. Stratified analyses examiningsurgical group differences were performed for confoundingvariables. For studies with multiple surgical groups, confoundinginformation for each surgical group was used when available.Otherwise, mean or median data from each study as a whole wasapplied to each group to allow categorization. Analysis ofvariance was performed using a Bonferroni correction tocompare multiple groups.
Meta-regression was also used to explore sources ofheterogeneity. After calculating the log odds ratio of patientswith meaningful reduction of pain and standard error of the logodds ratio, a forward, step-wise meta-regression was performedwith potential confounding variables as covariates. Confounderswere considered significant in the model if they altered theb-coefficient for surgery type by more than 10%.58 We assessedpublication bias graphically using Hunter’s method for creatingfunnel plots and formally tested funnel asymmetry using Peters’test.42,71 All statistical analyses were performed using StataIC 13(StataCorp, College Station, TX) and the METAPROP, META-REG, and METAFUNNEL software packages.
3. Results
3.1. Sources
Our electronic literature search and review of bibliographiesidentified 1328 studies. After abstract review excluding duplica-tions and studies not relevant to the subject of interest, 85 full-textstudies were reviewed. After exclusion of studies not meeting theinclusion criteria, 54 studies reporting 74 treatment groups andresults for 1381 patients were included in the final analysis (Fig. 1).
The reviewed studies were conducted over a period of morethan 30 years (1976-2015), in 16 countries, reflecting a variety ofmedical practices and reporting techniques. Among the 54included studies, 4 studies (7%) were conducted prospectively.Thirty-nine (72%) studies reported outcomes for a single surgicaltechnique, 11 (20%) reported outcomes for 2 techniques, 3 (6%)presented 3 techniques, and 1 (2%) reported 4 techniques. Ingeneral, each technique correlated with a treatment group;however, 6 studies described multiple techniques that werecategorized into the same treatment group. Excision andtransposition was the most commonly reported technique fortreating neuroma, with 34 studies (63%) including this group.Nineteen studies (35%) included an excision-only group, 11studies (20%) included a neurolysis and coverage group, 10studies (19%) included an excise and repair group, and 4 studies(7%) included an excise and cap group (Table 1).
Thirty-five studies (65%) reported treatment of neuromas in theupper extremity, 12 (22%) reported on lower extremity neuromas,and 6 (11%) reported on neuromas in both upper and lowerextremities. One study (2%) did not specify neuroma location butdid include intraoperative photographs of the upper extremities.Thirty-six studies (67%) reported results after treatment of
February 2018·Volume 159·Number 2 www.painjournalonline.com 215
Copyright � 2018 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.4
Table
1
Reportsofoutcomesstudiesofsurgicaltreatm
entforpainfulneuroma.
Study
Year
Country
Type
ofsurgery
Location
Meanfollow-up(m
o)Qualityscore
(15pointscale)
No.of
patients/group
No.of
improved
(%success)
Adanietal.3
2014
Italy
Neurolysisandcoverage
UE
41.5
6.5
86(75)
Adanietal.2
2002
Italy
Neurolysisandcoverage
UE
23.2
5.5
98(89)
Athertonetal.5
2008
UnitedKingdom
Excise
andtranspose
UE
327
3328
(85)
Athertonetal.6
2007
UnitedKingdom
Excise
andtranspose
UE
NR,6mominimum
6.5
3325
(76)
AthertonandElliot4
2007
UnitedKingdom
Excise
andtranspose
UE
33.7
7.5
76(86)
Balcinetal.7, *
2009
Switzerland
Excise
andtranspose
LE12
12.5
104(40)
Excise
andtranspose
106(60)
BarberaandAlbert-Pamplo8
1993
Spain
Excise
andcap
LE15
622
21(95)
Bek
etal.9
2006
Turkey
Excise
only
UE
71.5
714
14(100)
Bourkeetal.10
2011
UnitedKingdom
Excise
only
LENR
5.5
105(50)
Burchieletal.11
1993
UnitedStates
Excise
andtranspose
NR
113.5
188(44)
Excise
andtranspose
104(40)
Neurolysisandcoverage
50(0)
ChiodoandMiller14
2004
UnitedStates
Excise
andtranspose
UE
2711
149(64)
Excise
andtranspose
1214
13(93)
DellonandBarrett1
82005
UnitedStates
Excise
only
LENR,6mominimum
913
10(77)
Dellonetal.19
2004
UnitedStates
Excise
andtranspose
UE
16.8
9.5
99(100)
Dellon1
62002
UnitedStates
Excise
andtransposeexcise
only
UE
NR
327
27(100)
43(75)
DellonandAszmann1
71998
UnitedStates
Excise
andtranspose
LE29.5
711
9(82)
DellonandMackinnon
20
1986
UnitedStates/Canada
Excise
andtranspose
UEandLE
3110
6053
(88)
Ducicetal.25
2010
UnitedStates
Excise
andtranspose
LE34
9.5
3529
(83)
Ducicetal.26
2008
UnitedStates
Excise
andtranspose
LE22.8
10.5
2120
(95)
Elliotetal.27, *
2010
UnitedKingdom
Neurolysisandcoverage
UE
1911
1410
(72)
EvansandDellon2
81994
UnitedStates
Excise
andtranspose
UE
1911
1312
(92)
GuseandMoran
36
2013
UnitedStates
Excise
andtranspose
UE
240
10.5
116(55)
Excise
only
177(41)
Excise
andrepair
2823
(82)
Hazariand
Elliot37
2004
UnitedKingdom
Excise
andtranspose
UE
NR,2mominimum
635
34(97)
Excise
andtranspose
1313
(100)
HerbertandFilan3
81998
Australia
Excise
andtranspose
UE
158.5
149(64)
Herndon
etal.39
1976
UnitedStates
Neurolysisandcoverage
UE
306
1512
(80)
Neurolysisandcoverage
1812
(67)
Kakinokietal.45
2003
Japan
Excise
andtranspose
UE
237
107(70)
(contin
uedonnext
page)
216 L.H. Poppler et al.·159 (2018) 214–223 PAIN®
Copyright
�2018
bytheInternationalAssociatio
nfortheStudy
ofPain.
Unauthorizedreproductio
nof
thisarticle
isprohibited.
5

Table
1(continued)
Study
Year
Country
Type
ofsurgery
Location
Meanfollow-up(m
o)Qualityscore
(15pointscale)
No.of
patients/group
No.of
improved
(%success)
Kakinokietal.44
2008
Japan
Excise
andrepair
UE
1710
99(100)
Kandenweinetal.46
2006
Germany
Excise
andrepair
UE
518
30(0)
Excise
andtranspose
81(13)
KimandDellon4
72001
Korea/UnitedStates
Excise
andtranspose
LE18.5
9.5
1613
(81)
Koch
48
2011
Austria
Excise
andtranspose
UEandLE
43.6
825
23(92)
Koch
etal.49
2003
Austria
Excise
andtranspose
UEandLE
26.5
823
20(87)
Krishnan
etal.51
2005
Germany
Neurolysisandcoverage
excise
only
UEandLE
18.3
103
3(100)
15.3
44(100)
Labordeetal.52
1982
UnitedStates
Excise
only
UE
NR
232
13(41)
Excise
andtranspose
64(67)
Excise
andrepair
42(50)
Neurolysisandcoverage
88(100)
LanzettaandNolli53
2000
Italy
Excise
only
UE
NR,6mominimum
77
7(100)
Lohetal.55
1998
England
Excise
only
UE
NR
66
5(83)
Mackinnon
andDellon5
61987
UnitedStates/Canada
Excise
andtranspose
UE
NR
1052
42(81)
Martinsetal.59
2014
Brazil
Excise
andrepair
UE
28.3
10.5
77(100)
Masqueletetal.60
1987
France
Excise
andtranspose
UE
NR
520
18(90)
NahabedianandJohnson6
3, *
2001
UnitedStates
Excise
andtranspose
LE28
10.5
2521
(84)
NoordenbosandWall67
1981
Netherlands/England
Excise
andrepair
UEandLE
NR,20
mominimum
8.5
51(20)
Excise
only
20(0)
Novak
etal.68
1995
UnitedStates/Canada
Excise
andtranspose
UE
6010.5
7045
(64)
Resiman
andDellon7
51983
UnitedStates
Neurolysisandcoverage
UE
22.1
712
11(92)
Roseetal.76
1996
UnitedStates
Neurolysisandcoverage
UE
246.5
88(100)
Sarrisetal.77
2002
UnitedStates
Excise
andtranspose
UE
268
88(100)
Sehirliogluetal.78
2007
Turkey
Excise
only
LE33.6
675
75(100)
Souzaetal.80
2012
UnitedStates
Excise
only
LE25.7
77
6(86)
Spauwen
andHartman
81
1999
Netherlands
Neurolysisandcoverage
UE
248
109(90)
Stahland
Rosenberg83
2002
Israel
Excise
only
UE
610
32(66)
Excise
andtranspose
99(100)
Stahland
Goldberg8
21999
Israel
Excise
andcap
UE
NR
82
2(100)
Excise
andrepair
99(100)
Stokvisetal.84, *†
2010
Netherlands
Excise
andtranspose
UE
228.5
197(37)
Excise
andrepair
63(50)
Tennentetal.85
1998
England
Excise
only
LENR
43
3(100)
(contin
uedonnext
page)
February 2018·Volume 159·Number 2 www.painjournalonline.com 217
Copyright
�2018
bytheInternationalAssociatio
nfortheStudy
ofPain.
Unauthorizedreproductio
nof
thisarticle
isprohibited.
6

cutaneous sensory nerve neuromas, 11 studies (20%) reportedresults after treatment of major nerve (e.g., ulnar, median, sciatic)neuromas, and 5 studies (9%) reported results for both. Twostudies (4%) did not specify if major or cutaneous nerve weretreated.
In the included studies, the mean age of patients was 41.6 67.1 years. The median follow-up was 24 months (interquartilerange [IQR]: 17-31), and the median duration of symptoms priorto surgery reported was 21 months (IQR: 10-41). The medianpercentage of patients who had one or more prior operations forneuroma pain among studies was 29% (IQR: 0-1).
3.2. Patient identification
Forty-eight studies (89%) reported clearly how they diagnosedneuromas in their patients. In all cases, the physical examinationwasthe primary method of neuroma identification. Twenty-nine studies(54%) supplemented this with a diagnostic nerve block. Threestudies (6%) also used an MRI or ultrasound to aid in diagnosis.
3.3. Outcomes reporting
Outcomes reporting and duration of follow-up varied widelyacross studies. Many studies reported numerous outcomes.Thirty-eight studies (70%) used a nonstandard ordinal scale suchas no pain, mild pain, moderate pain, or severe pain as theirprimary outcome. Only 15 studies (28%) included a 10-point VASto report pain, and only 8 (15%) used it as a primary outcome.Four studies (8%) used patient satisfaction as a primary outcome.Four studies (8%) reported a reduction in pain on physicalexamination or improved functional status as the primaryoutcome. One study (2%) reported only that all patients hadcomplete pain relief and were able to return to normal activities.One study (2%) determined success of treatment fromdecreaseduse of analgesic pain medication.
Forty-four studies (81%) explicitly reported partial vs completepain relief. Five studies (9%) reported scores on the DASH scalebefore and after treatment. Fifteen studies (28%) reported patientsatisfaction. Most studies (40 of 54 [74%]) reported only meanfollow-up duration rather than the timing of outcome assessment.Three studies (6%) reported only a follow-up range, and 2 studies(4%) reported minimum follow-up only. Only one study (2%)reported the exact time of outcome assessment.
3.4. Quality of studies
Among the 54 studies included, the quality of informationreported was inconsistent, limiting our ability to analyze con-founding variables as sources of heterogeneity. On a scale from0 to 15, with 0 representing no important information presentedand 15 representing most important information presented, themedian score was 8.0 (IQR: 6.4-10.0). Studies consistentlyreported their aims, hypotheses, patient identification criteria, andsurgical technique. Patient selection, outcomes assessment, andcomplications were rarely clearly reported.
3.5. Sources of confounding bias
Based on the literature review, we considered the followingconfounding variables important when assessing outcomes fortreatment of painful neuromas: sex, age, duration of symptoms,timing of outcome assessment, number of prior neuroma painoperations, nerve involved, employment status, workers’ com-pensation claims or pending litigation, smoking status, body
Table
1(continued)
Study
Year
Country
Type
ofsurgery
Location
Meanfollow-up(m
o)Qualityscore
(15pointscale)
No.of
patients/group
No.of
improved
(%success)
Thom
asetal.86
1994
England
Excise
andrepair
UEandLE
126.5
203(15)
Thom
senandMackinnon
87
2010
France
Excise
andrepair
UE
11.8
7.5
1010
(100)
Tupperetal.89
1976
UnitedStates
Excise
only
UE
12.1
3.5
153
98(64)
Excise
andcap
24.6
177(41)
Excise
andcap
1728
19(68)
Vaientietal.91
2013
Italy
Excise
andtranspose
UE
1211
84(50)
*Prospectivestudy.
†Randomized
trial.
LE,lowerextrem
ity;NR,notreported;UE,upperextrem
ity.
218 L.H. Poppler et al.·159 (2018) 214–223 PAIN®
Copyright � 2018 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.7

mass index, and socioeconomic status. No study reported all ofthese variables and no study reported why or how confounderswere selected. Among studies reporting confounders, only 9studies (17%) considered confounding in their analysis.
3.6. Meaningful reduction of pain by surgery type
Among all studies, the proportion of patients with a meaningfulreduction in pain was 77% (95%CI: 73-83).When stratified by thetreatment group, there were no significant differences betweentreatment groups in the outcome of meaningful reduction in pain(P . 0.05). However, the excision and transposition group hadthe highest proportion of patients with a meaningful painreduction (81% [95% CI: 75-86]) and the most consistent results.Despite this, a large amount of heterogeneity was observed in alltreatment groups, I2 range 85.7% to 95.6% (Fig. 2).
3.7. Stratified analyses
To tease out possible guidelines for future surgical treatment ofneuromas, stratified analyses examining surgical group differenceswere performed for confounding variables. These included age,follow-up duration, symptom duration prior to definitive neuromasurgery, proportion of patients with 1 or more prior neuroma painsurgeries, neuroma location, affected nerve caliber (major nerve vscutaneous nerve), primary outcome, study quality, and studypublication year. Study groups were categorized according to themean symptom duration reported prior to neuroma surgery into:duration less than 12 months, duration of 12 to 23 months,duration greater than 24months, and not reported. Among groups
with mean symptoms duration greater than 24 months, excisionand transposition (74%patients improved [95%CI: 0.65-0.83]) andneurolysis and coverage (91% patients improved [95% CI: 0.80-1.00]) were significantly better than excision and repair (20%patients improved [95% CI: 0.05-0.34]), P , 0.05 for bothcomparisons. Among groups with mean symptom duration lessthan 12 months, or 12 to 23 months, there were no significantdifferences between surgery types.
Study groups were categorized according to the proportion ofpatients who had one or more surgeries for neuroma pain prior tothe reported surgery (0%-15%, 16%-30%, 31%-45%, 46%-60%, and greater than 60%). Among studies with greater than60% patients with one or more prior surgeries specifically forneuroma pain, excision and transposition (78% patients im-proved [95% CI: 0.66-0.90]) and neurolysis and coverage (96%patients improved [95% CI: 0.90-1.00]) were significantly betterthan excision-only (30% patients improved [95% CI: 0.02-0.59]),P , 0.05 for both comparisons. No significant differences wereseen between surgery types in groups with less than 60%patients with one or more prior operations for pain. No significantdifferences in the proportion of patients with a meaningful painreduction among study groups were seen regardless of age,follow-up duration, location (upper vs lower extremity), affectednerve caliber, primary outcome used, study quality, or publicationyear.
3.8. Regression analysis
Meta-regression was performed to examine for confoundingeffects of mean age, mean follow-up duration, mean symptomduration, proportion of patients with one ormore prior operations,nerve caliber, and primary outcome reported. Within the multipleregression models, the primary outcome reported, mean patientage, and proportion of patients with 1 or more prior operationsaltered the effect estimate of surgery type on proportion ofpatients with meaningful improvement after neuroma surgery bymore than 10%, suggesting that these factors do confoundtreatment effect.
3.9. Bias analysis
Funnel plot analysis of study groups was symmetric, suggestingthat there was no publication bias among studies (Appendix 2,available online as supplemental digital content at http://links.lww.com/PAIN/A506). Peters’ test for publication bias confirmedthese results (P 5 0.24).
4. Discussion
Awide variety of surgical techniques are described in the literatureto treat painful neuroma. Thus, the goal of thismeta-analysis of 54studies reporting outcomes after surgical treatment of painfulneuromas was to evaluate surgical effectiveness, establisha hierarchy of effective techniques, and delve into the impact ofconfounders on effective surgical treatment. When evaluating thestudies that met the inclusion criteria, our data demonstrate thatclinically meaningful improvement of pain can be achieved withsurgical intervention. However, the most effective surgicaltechnique was not elucidated, as we found no significantdifferences between the various surgical techniques. Further,the overall quality of most of the studies reviewed was low andexcitement for these results must be tempered.
Despite the low quality of most of the studies, the large numberof studies, surgical groups, and patients included in this meta-
Figure 1. Study selction process.
February 2018·Volume 159·Number 2 www.painjournalonline.com 219
Copyright � 2018 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.8

Figure 2. Fifty-four studies describing 74 groups were included in this meta-analysis of the proportion of patients successfully treated with surgery for neuromapain. Overall, 77% (95% confidence interval: 73-83) of patients had a meaningful reduction in pain. The type of surgery performed did not make a significantdifference to the proportion of patients successfully treated. Square grey boxes with a dot represent the reported proportion of patients with pain reduction. Theline surrounding this box represents the 95% confidence interval for that proportion. The blue diamonds represent the estimate of proportion of patients withreduction in pain for each surgery type, and overall, derived from the study groups included using random-effects meta-analysis of proportion.
220 L.H. Poppler et al.·159 (2018) 214–223 PAIN®
Copyright � 2018 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.9

analysis allowed for exploration of the role of confoundingvariables on neuroma surgery outcomes. There was no evidenceof publication bias, suggesting that the reported outcomes arereliable. Our categorization schema and subdividing patients intosurgical groups by technique is a reflection of the surgicalliterature, descriptions, and experience. This meta-analysiscannot assess if our categorization schema by technique wasmeaningful and this is a limitation to the study. Subtle differencesin technique are not well addressed with a meta-analysis andwould require a well-designed trial to flush out. Therefore, werecommend ongoing thoughtful analysis of outcomes andtechnique by surgeons in conjunction with pain specialists.
Overall, our data suggest that most patients with a painfulneuroma deemed appropriate surgical candidates by thesurgeon will have a meaningful decrease in pain with surgicalintervention and that in appropriately selected cases, the dogmathat “operating for pain will only result in more pain” may notapply.12,13,67 No information is included about patients withpainful neuromas that were not offered surgery. Therefore, anyconclusions about the effectiveness of surgery have to be limitedto patients deemed appropriate for surgical management, ie,indicated for surgery by the surgeon. We believe that patientselection and careful attention to correct diagnosis is the key tosuccessful outcomes.
When evaluating patients with painful neuromas, it isessential to distinguish between neuropathic pain becauseof compression neuropathy, direct nerve injury, or both,bearing in mind the distinct possibility of an associateddouble-crush phenomenon.90,94 Surgical treatment will varysignificantly for compression and neurotmetic injury.15,69 Thedistinction requires a detailed history and physical examina-tion. Identifying the appropriate nerve(s) involved in paingeneration is critical, especially considering overlap of nervedermatomes and frequent plexus formation between cuta-neous nerves.23,54,79 The importance of active patientparticipation in correct diagnosis cannot be overempha-sized.32 Further, a multidisciplinary approach to thesepatients with pain is essential. We recommend the involve-ment of pain management specialists, physical therapists,and psychological therapists in coming to the diagnosis anddecision for surgical intervention. In our experience, mis-diagnosis coupled with surgery can make a patient’s painworse.
Stratified analyses revealed 2 interesting findings. The firstwas that excision of a neuroma and transposition of the distalnerve end into muscle, bone, or vein or neurolysis of a neuromaand coverage with healthy vascularized tissue were superior toexcision-only or excision and capping in patients who hadneuroma pain for more than 2 years and in patients who hadmore than one previous surgery specifically to deal withneuroma pain. Why these procedures are superior in thesepatient populations cannot be answered by this meta-analysisand deserves further study. However, these populations arebelieved to be the most recalcitrant to surgical treatmentbecause of centralization of their pain.20,30 Therefore, becauseof their severity, these groups may allow the best evaluation ofthe surgical treatments.
Numerous authors have suggested that the microenvironmentcan affect painful neuroma formation.33,45,72,96 Placing the cutnerve end into muscle is shown to decrease neuroma size andmyofibroblast infiltration, potentially decreasing pain signal-ing.57,95 Placing the cut nerve end deep within a muscle or undera vascularized flap also protects it from external stimuli and blocksaxon regeneration to the skin.50,57 Skin may serve as both
a mechanical and biological irritant, especially in an inflamed,multiply operated wound bed.61,70 Other mechanical irritantsshould also be carefully observed by limiting tension and motionon the cut nerve end.20 Our clinical experience with vascularizedtissue coverage of a neuroma has not been positive unless thesource of neuroma pain is addressed with neuroma excision orneuroma excision and repair.88
The results of this study are consistent with previously publishedwork stating that 20% to 30% of neuromas will be refractory totreatment, regardless of the type of surgery performed.36,64 Initialresults can be misleading, and reoperation rates as high as 65%have been reported in some studies.36,37,52 Unfortunately, reopera-tion rates can be difficult to track and were rarely reported in theincluded studies. Studies also suggest that neuroma location or sizecan affect outcomes.20,31,36 In this study, neuroma location in thelower vs upper extremity made no difference. Neuroma size wasrarely reported, which precluded a meaningful interpretation of itsimpact.
As with all systematic reviews and meta-analyses, our ability todraw conclusions is limited by the quality of information in theprimary studies included. Studies only reported amedian of 8, outof 15 possible, key factors pertinent to patient outcome. Allstudies failed to include at least one important factor, and moststudies failed to report or perform any bias analysis with theirresults. Although included data were sufficient to performstratified and multivariate regression analysis, our inability todetect significant differences among treatment groups does notconfirm equivalence of these techniques. Rather, this lack ofdifference is likely an indication of the granularity of our data andheterogeneity in outcomes and confounding variables reportingamong studies.
Therefore, one of the major conclusions of this study that is wemust improve the quality of data reporting in the literature toimprove the acceptance and validity of surgical treatment forpainful neuromas. In particular, studies need to include cleardescriptions of how a neuroma is diagnosed, clear inclusion andexclusion criteria, and data about confounders such as age,ethnicity, smoking status, socioeconomic status, employmentstatus, and litigation or workers’ compensation claims. Thesedata should include precision estimates and not just ranges.Similarly, outcomes reporting should be standardized. Wesuggest using a pre- and post-operative VAS in conjunction witha pain diagram and list of pain adjectives. We use a standardizedpain assessment sheet at every visit (Appendix 3, available onlineas supplemental digital content at http://links.lww.com/PAIN/A506). It is essential that future studies collect long-term follow-up data on patients and include nonbiased reporting ofreoperative rates and treatment failures.
5. Conclusions
Surgical management of painful neuromas led to clinicallymeaningful improvement of pain in approximately 77% of casesregardless of surgical technique used. Although no techniqueproved to be clearly superior, these data demonstrate thatsurgical intervention should be considered in the treatmentalgorithm for patients suffering from painful neuroma refractory tomedical management. Future studies evaluating the surgicaltreatment of neuroma, or those comparing surgical techniques,need to be careful to define their treatment, outcomes, inclusion/exclusion criteria, and should account for confounding variablesto provide meaningful data and to facilitate the evidence-basedtreatment of our patients with painful neuromas.
February 2018·Volume 159·Number 2 www.painjournalonline.com 221
Copyright � 2018 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.10

Conflict of interest statement
The authors have no conflict of interest to declare.R. P. Parikh is supported by a NIH Ruth L. Kirschstein National
Research Service Award Institutional Research Training Grant(T32CA190194, PI Colditz).
Acknowledgements
Theauthors thank theNational Center for Advancing TranslationalSciences for grant UL1 TR000448 that helped make this workpossible.
Appendix A. Supplemental digital content
Supplemental digital content associated with this article can befound online at http://links.lww.com/PAIN/A506.
Article history:Received 29 April 2017Received in revised form 15 October 2017Accepted 26 October 2017Available online 20 November 2017
References
[1] Aasvang E, Kehlet H. Chronic postoperative pain: the case of inguinalherniorrhaphy. Br J Anaesth 2005;95:69–76.
[2] Adani R, Tarallo L, Battiston B, Marcoccio I. Management of neuromas incontinuity of the median nerve with the pronator quadratus muscle flap.Ann Plast Surg 2002;48:35–40.
[3] Adani R, Tos P, Tarallo L, Corain M. Treatment of painful median nerveneuromaswith radial and ulnar artery perforator adipofascial flaps. J HandSurg 2014;39:721–7.
[4] Atherton D, Elliot D. Relocation of neuromas of the lateral antebrachialcutaneous nerve of the forearm into the brachialis muscle. J Hand SurgEur Vol 2007;32:311–15.
[5] Atherton D, Fabre J, Anand P, Elliot D. Relocation of painful neuromasin zone III of the hand and forearm. J Hand Surg Eur Vol 2008;33:155–62.
[6] Atherton D, Leong J, Anand P, Elliot D. Relocation of painful endneuromas and scarred nerves from the zone II territory of the hand.J Hand Surg Eur Vol 2007;32:38–44.
[7] Balcin H, Erba P, Wettstein R, Schaefer D, Pierer G, Kalbermatten D. Acomparative study of two methods of surgical treatment for painfulneuroma. J bone Joint Surg Br 2009;91:803–8.
[8] Barbera J, Albert-Pamplo R. Centrocentral anastomosis of the proximalnerve stump in the treatment of painful amputation neuromas of majornerves. J Neurosurg 1993;79:331–4.
[9] Bek D, Demiralp B, Komurcu M, Atesalp S. The relationship betweenphantom limb pain and neuroma. Acta Orthop Traumatol Turc 2006;40:44–8.
[10] Bourke H, Yelden K, Robinson K, Sooriakumaran S, Ward D. Isrevision surgery following lower-limb amputation a worthwhileprocedure? A retrospective review of 71 cases. Injury 2011;42:660–6.
[11] Burchiel K, Johans T, Ochoa J. The surgical treatment of painful traumaticneuromas. J Neurosurg 1993;78:714–19.
[12] Campbell JN. Neuroma pain. In: Gebhart GF, Schmidt RF, editors.Encyclopedia of pain. 2nd ed. Berlin: Springer-Verlag, 2013. p. 2056–2058.
[13] Cetas JS, Saedi T, Burchiel KJ. Destructive procedures for the treatmentof nonmalignant pain: a structured literature review. J Neurosurg 2008;109:389–404.
[14] Chiodo C, Miller S. Surgical treatment of superficial peroneal neuroma.Foot Ankle Int 2004;25:689–94.
[15] Colbert SH. Painful sequelae of peripheral nerve injuries. In: MackinnonSE, editor. Nerve surgery. New York: Thieme, 2014. p. 591–619.
[16] Dellon A. Invited discussion. Ann Plast Surg 2002;48:158–60.[17] Dellon A, Aszmann O. Treatment of superficial and deep peroneal
neuromas by resection and translocation of the nerves into theanterolateral compartment. Foot Ankle Int 1998;19:300–3.
[18] Dellon A, Barrett S. Sinus tarsi denervation: clinical results. J Am PodiatricMed Assoc 2005;95:108–13.
[19] Dellon A, Kim J, Ducic I. Painful neuroma of the posterior cutaneous nerveof the forearm after surgery for lateral humeral epicondylitis. J Hand Surg2004;29:387–90.
[20] Dellon A, Mackinnon S. Treatment of the painful neuroma by neuromaresection and muscle implantation. Plast Reconstr Surg 1986;77:427–38.
[21] DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled ClinTrials 1986;7:177–88.
[22] Devor M, Tal M. Nerve resection for the treatment of chronic neuropathicpain. PAIN 2014;155:1053–4.
[23] Dorsi MJ, Chen L, Murinson BB, Pogatzki-Zahn EM, Meyer RA, BelzbergAJ. The tibial neuroma transposition (TNT) model of neuroma pain andhyperalgesia. PAIN 2008;134:320–34.
[24] Downs SH, Black N. The feasibility of creating a checklist for theassessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol CommunityHealth 1998;52:377–84.
[25] Ducic I, Levin M, Larson E, Al-Attar A. Management of chronic leg andknee pain following surgery or trauma related to saphenous nerve andknee neuromata. Ann Plast Surg 2010;64:35–40.
[26] Ducic I, Mesbahi A, Attinger C, Graw K. The role of peripheral nervesurgery in the treatment of chronic pain associated with amputationstumps. Plast Reconstr Surg 2008;121:908–14.
[27] Elliot D, Lloyd M, Hazari A, Sauerland S, Anand P. Relief of the pain ofneuromas-in-continuity and scarred median and ulnar nerves in the distalforearm and wrist by neurolysis, wrapping in vascularized forearm fascialflaps and adjunctive procedures. J Hand Surg Eur Vol 2010;35:575–82.
[28] Evans G, Dellon A. Implantation of the palmar cutaneous branch of themedian nerve into the pronator quadratus for treatment of painfulneuroma. J Hand Surg Am 1994;19:203–6.
[29] Fisher GT, Boswick JA Jr. Neuroma formation following digitalamputations. J Trauma 1983;23:136–42.
[30] Flor H, Nikolajsen L. Staehelin Jensen T. Phantom limb pain: a case ofmaladaptive CNS plasticity? Nat Rev Neurosci 2006;7:873–81.
[31] Friscia DA, Strom DE, Parr JW, Saltzman CL, Johnson KA. Surgicaltreatment for primary interdigital neuroma. Orthopedics 1991;14:669–72.
[32] Fuentes J, Armijo-Olivo S, Funabashi M, Miciak M, Dick B, Warren S,Rashiq S, Magee DJ, Gross DP. Enhanced therapeutic alliance modulatespain intensity and muscle pain sensitivity in patients with chronic low backpain: an experimental controlled study. Phys Ther 2014;94:477–89.
[33] Ghilardi JR, Freeman KT, Jimenez-Andrade JM, Mantyh WG, Bloom AP,Kuskowski MA, Mantyh PW. Administration of a tropomyosin receptorkinase inhibitor attenuates sarcoma-induced nerve sprouting, neuromaformation and bone cancer pain. Mol Pain 2010;6:87.
[34] Gotoda Y, Kambara N, Sakai T, Kishi Y, Kodama K, Koyama T. Themorbidity, time course and predictive factors for persistent post-thoracotomy pain. Eur J pain 2001;5:89–96.
[35] Greenland S, O’Rourke K. On the bias produced by quality scores inmeta-analysis, and a hierarchical view of proposed solutions. Biostatistics2001;2:463–71.
[36] Guse D, Moran S. Outcomes of the surgical treatment of peripheralneuromas of the hand and forearm: a 25-year comparative outcomestudy. Ann Plast Surg 2013;71:654–8.
[37] Hazari A, Elliot D. Treatment of end-neuromas, neuromas-in-continuityand scarred nerves of the digits by proximal relocation. J Hand Surg Br2004;29:338–50.
[38] Herbert T, Filan S. Vein implantation for treatment of painful cutaneousneuromas. J Hand Surg Br 1998;23 B:220–4.
[39] Herndon J, Eaton R, Littler J. Management of painful neuromas in thehand. J Bone Joint Surg Am Vol 1976;58:369–73.
[40] Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD,Savovic J, Schulz KF, Weeks L, Sterne JA. The Cochrane collaboration’stool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928.
[41] Hudak PL, Amadio PC, Bombardier C. Development of an upperextremity outcome measure: the DASH (disabilities of the arm, shoulderand hand) [corrected]. The upper extremity collaborative group (UECG).Am J Ind Med 1996;29:602–8.
[42] Hunter JP, Saratzis A, Sutton AJ, Boucher RH, Sayers RD, Bown MJ. Inmeta-analyses of proportion studies, funnel plots were found to be aninaccurate method of assessing publication bias. J Clin Epidemiol 2014;67:897–903.
[43] Juni P, Witschi A, Bloch R, Egger M. The hazards of scoring the quality ofclinical trials for meta-analysis. JAMA 1999;282:1054–60.
[44] Kakinoki R, Ikeguchi R, Atiyya A, Nakamura T. Treatment of posttraumaticpainful neuromas at the digit tip using neurovascular island flaps. J HandSurg Am 2008;33:348–52.
[45] Kakinoki R, Ikeguchi R, Matsumoto T, Shimizu M, Nakamura T.Treatment of painful peripheral neuromas by vein implantation. IntOrthop 2003;27:60–4.
222 L.H. Poppler et al.·159 (2018) 214–223 PAIN®
Copyright � 2018 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.11

[46] Kandenwein J, Richter H, Antoniadis G. Is surgery likely to be successfulas a treatment for traumatic lesions of the superficial radial nerve? [inGerman]. Nervenarzt 2006;77:175–6.
[47] Kim J, Dellon A. Neuromas of the calcaneal nerves. Foot Ankle Int 2001;22:890–4.
[48] KochH. Painful neuroma—mid-term results of resection and nerve stumptransposition into veins. Eur Surg 2011;43:378–81.
[49] Koch H, Haas F, Hubmer M, Rappl T, Scharnagl E. Treatment of painfulneuroma by resection and nerve stump transplantation into a vein. AnnPlast Surg 2003;51:45–50.
[50] Krishnan KG, Pinzer T, Schackert G. Coverage of painful peripheral nerveneuromas with vascularized soft tissue: method and results.Neurosurgery 2005;56(2 suppl):369–78; discussion 369–78.
[51] Krishnan KG, Pinzer T, Schackert G. Coverage of painful peripheral nerveneuromas with vascularized soft tissue: method and results. Comments.Neurosurgery 2005;56(4 suppl):ONS-377–8.
[52] Laborde K, Kalisman M, Tsai T. Results of surgical treatment of painfulneuromas of the hand. J Hand Surg Am 1982;7:190–3.
[53] LanzettaM,Nolli R.Nerve stripping: new treatment for neuromas of thepalmarcutaneous branch of the median nerve. J Hand Surg Br 2000;25:151–3.
[54] Li Y, Dorsi MJ, Meyer RA, Belzberg AJ. Mechanical hyperalgesia after anL5 spinal nerve lesion in the rat is not dependent on input from injurednerve fibers. PAIN 2000;85:493–502.
[55] Loh Y, Stanley J, Jari S, Trail I. Neuroma of the distal posteriorinterosseous nerve. A cause of iatrogenic wrist pain. J Bone Joint SurgBr Vol 1998;80:629–30.
[56] Mackinnon S, Dellon A. Results of treatment of recurrent dorsoradial wristneuromas. Ann Plast Surg 1987;19:54–61.
[57] Mackinnon SE, Dellon AL, Hudson AR, Hunter DA. Alteration of neuromaformation by manipulation of its microenvironment. Plast Reconstr Surg1985;76:345–53.
[58] Maldonado G, Greenland S. Simulation study of confounder-selectionstrategies. Am J Epidemiol 1993;138:923–36.
[59] Martins R, Siqueira M, Heise C, Yeng L, De Andrade D, Teixeira M.Interdigital direct neurorrhaphy for treatment of painful neuroma due tofinger amputation. Acta Neurochir (Wein) 2015;157:667–71.
[60] Masquelet A, Bellivet C, Nordin J. Treatment of painful neuromas of the handby intra-osseous implantation [in French]. Ann Chir Main 1987;6:64–6.
[61] Meyer RA, Raja SN, Campbell JN, Mackinnon SE, Dellon AL. Neural activityoriginating from a neuroma in the baboon. Brain Res 1985;325:255–60.
[62] Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items forsystematic reviews and meta-analyses: the PRISMA statement. AnnIntern Med 2009;151:264–9.
[63] Nahabedian M, Johnson C. Operative management of neuromatous kneepain: patient selection and outcome. Ann Plast Surg 2001;46:15–22.
[64] Nelson AW. The painful neuroma: the regenerating axon verus theepineural sheath. J Surg Res 1977;23:215–21.
[65] Newcombe RG. Two-sided confidence intervals for the single proportion:comparison of seven methods. Stat Med 1998;17:857–72.
[66] Nikolajsen L, Christensen KF, Haroutiunian S. Phantom limb pain:treatment strategies. Pain Manag 2013;3:421–4.
[67] Noordenbos W, Wall P. Implications of the failure of nerve resection andgraft to cure chronic pain produced by nerve lesions. J Neurol NeurosurgPsychiatry 1981;44:1068–73.
[68] Novak C, Van Vliet D, Mackinnon S. Subjective outcome followingsurgical management of upper extremity neuromas. J Hand Surg Am1995;20:221–6.
[69] Novak CB. Evaluation of the patient with nerve injury or nervecompression. In: Mackinnon SE, editor. Nerve surgery. New York:Thieme, 2014. p. 41–58.
[70] Paterson S, Schmelz M, McGlone F, Turner G, Rukwied R. Facilitatedneurotrophin release in sensitized human skin. Eur J Pain 2009;13:399–405.
[71] Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Comparison oftwo methods to detect publication bias in meta-analysis. JAMA 2006;295:676–80.
[72] Pezet S. Neurotrophins and pain [in French]. Biol Aujourdhui 2014;208:21–9.
[73] Rajput K, Reddy S, Shankar H. Painful neuromas. Clin J pain 2012;28:639–45.
[74] Ramachandran VS, Rogers-Ramachandran D. Synaesthesia in phantomlimbs induced with mirrors. Proc Biol Sci 1996;263:377-86.
[75] Reisman N, Dellon A. The abductor digiti minimi muscle flap: a salvagetechnique for palmar wrist pain. Plast Reconstr Surg 1983;72:859–63.
[76] Rose J, Belsky M, Millender L, Feldon P. Intrinsic muscle flaps: thetreatment of painful neuromas in continuity. J Hand Surg Am 1996;21:671–4.
[77] Sarris I, Gobel F, Gainer M, Vardakas D, Vogt M, Sotereanos D. Medialbrachial and antebrachial cutaneous nerve injuries: effect on outcomein revision cubital tunnel surgery. J Reconstr Microsurg 2002;18:665–70.
[78] Sehirlioglu A, Ozturk C, Yazicioglu K, Tugcu I, Yilmaz B, Goktepe A.Painful neuroma requiring surgical excision after lower limb amputationcaused by landmine explosions. Int Orthop 2009;33:533–6.
[79] Sheth RN, Dorsi MJ, Li Y, Murinson BB, Belzberg AJ, Griffin JW, MeyerRA. Mechanical hyperalgesia after an L5 ventral rhizotomy or an L5ganglionectomy in the rat. PAIN 2002;96:63–72.
[80] Souza J, Nystrom A, Dumanian G. Patient-guided peripheral nerveexploration for the management of chronic localized pain. Plast ReconstrSurg 2012;129:221–5.
[81] Spauwen P, Hartman E. Reverse fasciocutaneous forearm flaps areeffective in treating incapacitating neuromas in the hand. Eur J Plast Surg1999;22:107–10.
[82] Stahl S, Goldberg J. The use of vein grafts in upper extremity nervesurgery. Eur J Plast Surg 1999;22:255–9.
[83] Stahl S, Rosenberg N. Surgical treatment of painful neuroma in medialantebrachial cutaneous nerve. Ann Plast Surg 2002;48:154–8.
[84] Stokvis A, van der Avoort D, van Neck J, Hovius S, Coert J. Surgicalmanagement of neuroma pain: a prospective follow-up study. PAIN2010;151:862–9.
[85] Tennent T, Birch N, Holmes M, Birch R, Goddard N. Knee pain and theinfrapatellar branch of the saphenous nerve. J R Soc Med 1998;91:573–5.
[86] Thomas M, Stirrat A, Birch R, Glasby M. Freeze-thawed muscle graftingfor painful cutaneous neuromas. J Bone Joint Surg Br 1994;76:474–6.
[87] Thomsen L, Bellemere P, Loubersac T, Gaisne E, Poirier P, Chaise F.Treatment by collagen conduit of painful post-traumatic neuromas of thesensitive digital nerve: a retrospective study of 10 cases. Chir Main 2010;29:255–62.
[88] Tung TH, Mackinnon SE. Secondary carpal tunnel surgery. PlastReconstr Surg 2001;107:1830–43; quiz 1844, 1933.
[89] Tupper J, Booth D. Treatment of painful neuromas of sensory nerves inthe hand: a comparison of traditional and newer methods. J Hand SurgAm 1976;1:144–51.
[90] Upton AR, McComas AJ. The double crush in nerve entrapmentsyndromes. Lancet 1973;2:359–62.
[91] Vaienti L, Merle M, Battiston B, Villani F, Gazzola R. Perineural fat graftingin the treatment of painful end-neuromas of the upper limb: a pilot study.J Hand Surg Eur Vol 2013;38:36–42.
[92] Watson J, Gonzalez M, Romero A, Kerns J. Neuromas of the hand andupper extremity. J Hand Surg Am 2010;35:499–510.
[93] Whipple RR, Unsell RS. Treatment of painful neuromas. Orthop Clin NorthAmerica 1988;19:175–85.
[94] Wilbourn AJ, Gilliatt RW. Double-crush syndrome: a critical analysis.Neurology 1997;49:21–9.
[95] Yan H, Gao W, Pan Z, Zhang F, Fan C. The expression of alpha-SMA inthe painful traumatic neuroma: potential role in the pathobiology ofneuropathic pain. J Neurotrauma 2012;29:2791–7.
[96] Yan H, Zhang F, Kolkin J, Wang C, Xia Z, Fan C. Mechanisms of nervecapping technique in prevention of painful neuroma formation. PLoS One2014;9:e93973.
February 2018·Volume 159·Number 2 www.painjournalonline.com 223
Copyright � 2018 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.12

Biennial Review of Pain
Transition from acute to chronic pain after surgeryPatricia Lavand’homme
1. Introduction
Any tissue trauma can lead to “chronic pain,” which by definition ispain that persists past the normal healing time.40 This type of painis frequent after surgery. In 1998, Crombie et al.8 noted that 22.5%of patients attending pain clinics attributed their pain to a previoussurgery, and since then, numerous original research articles,review articles, and editorials have addressed chronic pain aftersurgery. Long-term pain after surgery causes disability andsuffering associated with reduced quality of life and increaseduse of health care resources. For that reason, chronic postsurgicalpain (CPSP) has become a health priority and will be included inthe new version of the International Classification of Diseases
(ICD-11), as a result of the combined efforts of the World HealthOrganization (WHO) and the IASP.40 Adequate pain treatment isa human right, and the inclusion of CPSP in the ICD-11 isexpected to increase recognition of the problem and promoteinterdisciplinary research in the field. Indeed, CPSP is nowaccepted as an important outcome of surgery. Researchers havedetermined its prevalence in the adult population and examined itsincidence after various procedures. However, while the globalvolume of surgeries is increasing worldwide,41 the occurrence ofCPSP has not really decreased over the years because preventivestrategies are not clearly defined and thereby not applied in clinicalpractice, in contrast to the progress made in basic research in theunderstanding of incisional pain physiology.10
In daily clinical practice, the transition from acute postoperativepain to CPSP is often subtle and unpredictable. Rather thanfocusing on pathophysiological mechanisms, the followingdiscussion will address clinical aspects, ongoing improvementsin management, and future challenges.
2. The “problem” of chronic postsurgical pain:evolution and new approaches
Chronic postsurgical pain may occur irrespective of the type ofprocedure, although some surgeries carry a higher risk in relationto the degree of tissue damage and the potential for a majorinflammatory reaction or nerve injury. An editorial5 dedicated toacute postoperative pain summarized the situation as follows:“CPSP develops in 1 of 10 surgical patients and becomes an
intolerable pain condition after 1 of every 100 operations.” In2016, studies from large cohorts of patients and prospectivestudies still showed the same prevalence (Table 1), despitea significant evolution in surgical techniques. Laparoscopicprocedures and minimally invasive approaches have only slightlymodified the incidence of CPSP, but their impact on the intensityand duration of CPSP deserves further assessment. A recentmulticenter observational study on CPSP in Europe reportsa 12-month incidence of 11.8% for moderate CPSP and 2.2% forsevere CPSP (defined by a score .6 on a numeric rating scaleranging from 0-10).13
The nature of CPSP is often poorly characterized in clinicalstudies. However, a neuropathic component may exist in around35% of cases.40 The reported prevalence of a neuropathiccomponent differs among surgical procedures, depending on thelikelihood of surgical iatrogenic nerve injury and themethod or toolused to assess its presence.11,16 Signs of neuropathic pain areimportant to detect because they are always associated withhigher pain intensity and a poorer quality of life.11–13 Furthermore,neuropathic pain requires a specific therapeutic approach.
For several years, CPSP has been assessed in adulthospitalized patients undergoing major surgical procedures suchas thoracic surgery or limb amputation. Recently, orthopedicprocedures and specifically joint replacements have beenconsidered as a major risk for development of CPSP.13,37 Thevolume of knee and hip arthroplasties is growing because thepopulation is growing older and inflammatory diseases as well asobesity are becoming more frequent. Although outcomes interms of pain relief and mobility are highly successful for mostpatients undergoing joint arthroplasty, 20% of them will developCPSP after knee arthroplasty and 10% after hip arthroplasty.33
The intensity of CPSP is greater after joint arthroplasty than aftervisceral or gynecological surgery.13
It is unfortunate that CPSP data are still missing for specificpopulations and subgroups of patients because they might yieldimportant findings for a better understanding of the chronificationof acute postoperative pain. Only recently, CPSPwas found to bean important problem in children. The prevalence of CPSP islower when surgery is performed at a younger age, perhapsbecause surgical procedures are simpler and recovery is fasterduring childhood.29 Nevertheless, CPSP has a significant impacton any child’s quality of life and is associated with poor long-termoutcomes. Therefore, better understanding of the context ofCPSP development in children is mandatory to prevent painpersistence into adulthood. Furthermore, studying CPSP inchildren is a unique opportunity to assess the role of pain ata critical period of development and to determine the impact ofprotective factors vs risk factors, including hormonal factors andsocial variables such as parental influence.
Studies addressing recovery from CPSP in the context ofoutpatient surgery are scarce.11,18 Although outpatient surgerymight be different in terms of tissue damage and anesthetic
Sponsorships or competing interests that may be relevant to content are disclosed
at the end of this article.
Department of Anesthesiology, Cliniques Universitaires Saint-Luc, University
Catholic of Louvain, Brussels, Belgium
Address: Department of Anesthesiology, Cliniques Universitaires Saint-Luc, University
Catholic of Louvain, Ave Hippocrate 10-1821, B-1200 Brussels, Belgium. Tel.:132 2
7641821; fax:1322 7643699. E-mail address:[email protected]
(P. Lavand’homme).
PAIN 158 (2017) S50–S54
© 2017 International Association for the Study of Pain
http://dx.doi.org/10.1097/j.pain.0000000000000809
S50 P. Lavand’homme·158 (2017) S50–S54 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.13

technique, that it is often associated with suboptimal acutepostoperative pain control, and that its psychological impactmight be lower in outpatients (with less anxiety and lesscatastrophizing), the prevalence and intensity of CPSP do notseem to differ between outpatients and hospitalized patients(Table 1). Today, more and more patients are included in ERAS(enhanced recovery after surgery) programs. However, theoptimal perioperative multimodal care provided in such programsdoes not seem to influence the outcome of patients with CPSP.39
We lack data on the prevalence of CPSP in patients withpsychiatric diseases and in less-developed countries. Findings inthose populations might be important in helping us to betterunderstand the development of CPSP.
3. The resolution of pain after surgery: pointing toa novel definition of chronic postsurgical pain
Fortunately, CPSP resolves over time. Of all patients with CPSP 6months after surgery, 55.8% will be pain free at 12 months,whereas 2.9%of patientswithout pain at 6monthswill report somepain at 12 months.13 Such findings reinforce the fact that CPSPdoes not always develop on a continuum from acute postsurgicalpain; new studies should assess all patients at several time points.Not only the incidence but also the intensity of CPSP decreaseswith time.11 Furthermore, studies focusing on neuropathiccomponents of CPSP have highlighted the variability of theseaspects over time.35 Several problems arise when investigatingCPSP, and the first involves its definition.25 Werner and Kongs-gaard42 proposed an updated definition based on observationsand the most important concerns raised during the last few years(Table 2). These criteria will factor into the definition of CPSP thatwill be included in the ICD-11.40 The major points are as follows:(1) Chronic postsurgical pain is either a continuum of acutepostoperative pain or develops after an asymptomatic period;
(2) Chronic postsurgical pain shows greater intensity or differentpain characteristics than preoperative pain (an important pointregarding CPSP after orthopedic procedures, where preoper-ative pain may affect up to 80% of patients undergoing surgery);
(3) The cutoff for CPSP has now been fixed at 3 months aftersurgery becausehealing times differ amongdifferent procedures;for major orthopedic surgeries such as hip and knee arthroplas-ties, pain reaches its lowest level by 3 months after surgery.28
4. Predictive tools: strengths and weaknesses
Chronic postsurgical pain may develop after any surgical pro-cedure, and the fact that the pain is sometimes disproportionate to
the degree of tissue trauma underlines the major role of individualfactors. In pain clinics, the suffering expressed by patients resultsfrom both pain amplification and psychological distress. Asprevention is always better than a cure, the development ofreliable predictive tools to detect the high-risk patients for CPSP ismandatory. Studies investigating the association of CPSP with 90genetic markers found no evidence for genetic predisposition ina subset of 1000 patients, whereas 6 clinical factors predicted73% of the chronic postsurgical pain that developed.27 Today,despite the hopes and promises of genetic research, which hasrevealed several links between gene polymorphisms and sensi-tivity to pain, clinical risk factors remain the best availablepredictors of CPSP. However, in daily practice, even if the riskfactors are well known, the proposed risk index is still not sensitiveand specific enough to determinewhich patients are atmost risk.2
The chronification of postoperative pain often remains subtle, andthe risk factors involved in the transition from acute to chronicpostsurgical pain probably differ from those involved in maintain-ing chronic pain once it has developed.19 The most important riskfactors involved in the development of CPSP are as follows:(1) the intensity of acute postoperative pain;(2) the presence of preoperative pain in the body part to beoperated on or elsewhere (including coexisting chronic painfulconditions such as fibromyalgia, headache, low back pain, orrestless leg syndrome);
(3) symptoms of psychological distress and major stress such asdepression, extreme anxiety, or catastrophizing.Acute postoperative pain intensity, “recalled pain” in retro-
spective studies, is a highly prominent risk factor although theassociation between acute postoperative pain and CPSP is not
Table 1
Picture of perioperative pain: evolution of the incidence of preoperative pain, acute postoperative pain, and chronic postsurgical
pain in different populations.
Population Preoperative pain Severe acutepostoperative pain
CPSP moderate/severe
Crombie et al,8 Adult patients in pain clinics 22%
Macrae,25 Adult population 10%-50%/4%-10%
Johansen et al, 2012 General adult population 18.3% (6.2% without preoperative pain)
Fletcher et al,13 Adult inpatients 35%-60% 30% 11.8%/2.2%
Hoofwijk et al,18 Adult outpatients 37.7% 26.7% 15.3%/2.3%
Nikolajsen and Brix29 Pediatric population 13% (with NRS . 3)*
* NRS: Numeric rating score on a scale from 0 (no pain) to 10 (worst possible pain).
CPSP, chronic postsurgical pain.
Table 2
Updated definition of chronic postsurgical pain.
Pain developed after a surgical procedure or increased in intensity after the surgical
procedure.
Pain should be of at least 3 mo duration with a significant negative effect on the
quality of life.
Pain is a continuation of acute postoperative pain or may develop after an
asymptomatic period
Pain is localized to the surgical field or to a referred area (eg, innervation territory,
referred dermatoma for visceral surgery).
Other possible causes for the pain have been excluded (eg, infection, cancer
recurrence)
Italic characters concern the modifications proposed and added to the initial definition (from Macrae WA,
2008,25 and Werner MU and Kongsgaard UE, 201442). The current definition of chronic postsurgical pain has
been accepted by the IASP Task Force on Chronic Pain and will be included in ICD-11.
April 2017·Volume 158·Number 4·Supplement 1 www.painjournalonline.com S51
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.14

necessarily a causal one. An estimated 30% of patients enduresevere pain (numeric rating scale . 6) during the first 24 hoursafter surgery, even after minor procedures.14 Fortunately for thepatients, not all of those who experience severe acute post-operative pain will develop CPSP. Conversely, and unfortunatelyfor the patients’ caregivers, optimal control of acute post-operative pain is not a guarantee that CPSP will not develop, ashighlighted by the failure of current perioperative treatments suchas multimodal analgesia and local and regional techniques tosignificantly reduce the incidence of CPSP.6 Indeed, epiduralanalgesia may prevent CPSP after thoracotomy in 1 of 4 patients,and paravertebral block may prevent CPSP after breast cancersurgery in 1 of 5 women, which supports the mandate to targethigh-risk patients and to individualize perioperative manage-ment.22 Postoperative pain and the development of CPSP notonly vary among individuals but are dynamic processes. The factthat a 10% increase in the percentage of time in severe pain isassociated with a 30% increase in the incidence of CPSP at 12months certainly demonstrates that acute postoperative painintensity is a risk factor for some patients.13 However, it does notallow us to determine which patients are at high risk.
The resolution of postoperative pain matters more than theinitial pain intensity. The development of “pain trajectories” shouldallow us to characterize an individual’s postoperative pain andthereby identify abnormal resolution of acute pain.7 In a study thatmapped pain trajectory patterns, and specifically the slope of thetrajectory (ie, pain resolution), during the first week after surgery,25% of patients showed no pain resolution (a flat slope), whereas12% of patients had a greater postoperative pain (a rising slope).In a study on pain after total knee replacement, patients whosepain was increasing a week after surgery were still in severe pain 3months after surgery, and their CPSP had a neuropathiccomponent.23
There are 2 lessons to be learned from these observations.First, the control of acute postoperative pain should includecorrect assessment of pain and early intervention with accuratetreatment. The diagnosis of a neuropathic component in the earlypostoperative period is feasible with the use of adequate tools.Back in 2002, Hayes et al.17 pointed out that acute pain servicesoften neglected to assess neuropathic pain. They reported thatamong the 3% of patients diagnosed with neuropathic pain bytheir acute pain service, 78% had ongoing pain at 6 months and56% at 12 months.17
Second, the characteristics of pain are important in identifyingpatients at high risk for CPSP. Unfortunately, most clinical trials donot provide many details regarding the type of pain, eitherpostoperative or chronic; for example, only 40% of trials assesspain related to mobilization (ie, evoked pain), which plays a majorrole in rehabilitation after surgery.21 After laparoscopic cholecys-tectomy, 3 components contribute to the overall burden of pain:incisional pain (somatic pain), deep abdominal pain (visceral pain),and shoulder pain (referred pain). The 3 components showdistinct pain trajectories, with incisional pain having the highestpain scores.3 Surprisingly, the risk of chronic pain afterlaparoscopic cholecystectomy is significantly related to thevisceral pain response during the first week after surgery.4 Inpatients with osteoarthritis with joint pain, there is a growingrecognition of the importance of distinguishing between pain atrest and pain on movement, owing to different underlying painmechanisms and a different response to analgesic treatments.33
A recent study intended to explore the relationship betweenacute postsurgical pain and preoperative pain on one hand andCPSP on the other hand after knee and hip replacementsecondary to osteoarthritis, considering both pain at rest and
movement-evoked pain.36 The main findings of the study are thepreponderant influence of preoperative pain either at rest (for hiparthroplasty) or on movement (for knee arthroplasty) in predictingthe intensity of postoperative pain at rest or on movement.
Preoperative pain at the surgical site or elsewhere also standsas a major risk factor for persistent pain after surgery. Twoexplanations underlie the phenomenon: the link between painand sensitization to further pain and the impact of takingpreoperative analgesics. Patients taking opioid analgesics beforesurgery report higher acute postoperative pain and are ata greater risk for painful prolonged recovery, particularly afterorthopedic procedures.44 Is sensitization caused by opioid intakethe explanation? The answer is not so simple. Opioid analgesicsare not very effective against evoked pain (ie, pain associatedwithmovement). A prospective study on CPSP in outpatientsscheduled for orthopedic surgery found that in patients achievingeffective pain relief with preoperative analgesics, only 8%developed CPSP. By contrast, 32% of patients taking pre-operative analgesics without achieving effective pain reliefdeveloped CPSP.18 These data underline the complexity of therelationship between preoperative pain, its control, and CPSP.Further studies should focus on preoperative pain control asa preventive measure to reduce both the incidence of severeacute pain and the development of persistent pain after surgery.The experience of pain results from both pain amplification andpsychological distress, and some patients are more prone todevelop severe pain both immediately after tissue lesion andsubsequently. Thereby, progress in preventive strategies isstrongly linked to individualization of treatments based on theknowledge of the patient’s pain phenotype. The use ofquantitative sensory testing allows clinicians to determinea patient’s endogenous pain modulation profile43 and therebymight allow mechanism-based pain management as moreappropriate pain therapy. Around 68% to 82% of patientsscheduled for joint replacement present with preoperative paincaused by osteoarthritis.33 In those patients, nociceptiveperipheral pain is associated with a central sensitization processin 30% of cases, particularly when a neuropathic component ispresent.24,33 However, individualized perioperative treatmentsare rarely provided because the patient’s pain phenotype is nottaken into account.
Mental health has an important impact on the patient’s ability torecover after surgery. There is a vulnerable population ofindividuals with a reduced ability to cope with pain, to anticipatepain, and to control pain when confronted with it. A tendencytoward anxiety, psychological distress such as depression,hypervigilance, and catastrophizing are all risk factors for bothsevere acute postoperative pain and CPSP.1 However, theimportance of these psychological factors varies from onesurgical population to another. Catastrophizing has only a minorimpact on pain after cesarean section in comparison with its rolein pain after breast cancer surgery.35 Models of postoperativepain in children display 2 distinct trajectories: early recovery(49.8%) and late recovery (11.2%).34 While child catastrophizinghas no impact, parental pain catastrophizing before surgerysignificantly predicts late recovery. Furthermore, as time fromsurgery increases, parents exert more and more influence overthe pain response of their children.
Chronic postsurgical pain should be considered a “mixed painsyndrome” in which neuropathic pain represents one of thecomponents that, when present, contributes to pain severity andchronification.11 As a neuropathic component is present in atleast one-third of CPSP cases, determining the factors thatcontribute to whether or not a nerve lesion will become painful is
S52 P. Lavand’homme·158 (2017) S50–S54 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.15

highly relevant. Indeed, not all lesions in the somatosensorysystem lead to neuropathic pain.38 In the first 48 hours aftersurgery, higher pain intensity, a positive neuropathic pain score,and evidence of secondary hyperalgesia (a clinical correlate ofcentral nervous system sensitization) are all predictive of CPSPinvolving a major neuropathic component.26 A history of previousneuropathy is also a risk factor,11 which highlights the role ofgenetic predisposition to less-successful nerve regeneration afterinjury in the development of CPSP.38
5. The subacute pain period: the role of transitionalpain services
After hospital discharge, postoperative pain can last for severalweeks. This “subacute pain” period remains a rather neglectedarea, a “gray zone” of clinical investigations, despite its crucialrole in rehabilitation and the patient’s return to his or herpreoperative status.22 A few prospective studies have underlinedthe predictive value of 30-day or 6-week postoperative painintensity as a risk factor for the development of CPSP, forexample, after inguinal hernia repair and cosmetic breastsurgery.22 In clinical studies using long-term pain trajectoriesafter surgery, analysis conducted between 6 weeks and 3months shows subgroups of patients who will or will not resolvetheir pain after knee arthroplasty.32 The intensity of subacutepain 30 days after knee replacement is a risk factor for severeCPSP at 3 and 6 months.15 Pain intensity may even increaseduring the subacute period, revealing the presence of a neuro-pathic pain process, as observed after hernia repair ororthopedic surgery in rehabilitation units.30 It is worth notingthat not only pain intensity but also pain unpleasantness (theemotional aspect of pain) might be an important predictor ofsubsequent CPSP development, as highlighted in a pediatricpopulation during the subacute period (eg, at 6 weeks).31 In painclinics, patients who attribute their chronic pain to a specificcause often report a higher level of emotional distress and painintensity.8 For a large majority of patients, the worst pain periodoccurs at home (eg, outpatients) and during rehabilitation efforts(eg, orthopedic patients), which supports the implementation oftransitional pain units as an integral part of “perioperativemedicine” to provide the most effective pain treatment and todetect any risk of pain chronification as soon as possible.9,20
6. Conclusions
We currently have a good picture of the prevalence of chronicpain after surgery, a picture that has not changed since the firstreports almost 2 decades ago. Ongoing improvements in thelight of more recent clinical studies are a new more accuratedefinition of CPSP and the inclusion of CPSP in the future versionof the ICD-11 (by theWHO and an IASP task force). The inclusionof CPSP in the ICD-11 is expected to increase recognition of theproblem and further promote research in the field. The year 2017represents IASP’s Global Year Against Pain After Surgery, whichwill help to attract the attention of caregivers, patients, and theirrelatives. As stated above, chronic postsurgical pain resultsfrom pain amplification and emotional distress. Although the riskfactors are well known, they do not allow clinicians to identifypatients at very high risk or to provide effective preventivetreatments. Future challenges include the optimization ofpredictive tools. Screening of new populations includingpediatric patients, the use of pain trajectories includingobservation of patients during the subacute pain period, andthe implementation of transitional pain units as part of
perioperative medicine are exciting projects that should helpcaregivers to find a better approach to the transition from acuteto chronic postoperative pain.
Conflict of interest statement
The author has no conflicts of interest to declare.
Article history:Received 21 October 2016Received in revised form 9 December 2016Accepted 12 December 2016Available online 25 January 2017
References
[1] Althaus A, Arranz Becker O, Neugebauer E. Distinguishing between painintensity and pain resolution: using acute post-surgical pain trajectories topredict chronic post-surgical pain. Eur J Pain 2014;18:513–21.
[2] Althaus A, Hinrichs-Rocker A, Chapman R, Arranz Becker O, Lefering R,Simanski C, Weber F, Moser KH, Joppich R, Trojan S, Gutzeit N,Neugebauer E. Development of a risk index for the prediction of chronicpost-surgical pain. Eur J Pain 2012;16:901–10.
[3] Bisgaard T, Klarskov B, Rosenberg J, Kehlet H. Characteristics andprediction of early pain after laparoscopic cholecystectomy. PAIN 2001;90:261–9.
[4] Blichfeldt-Eckhardt MR, Ording H, Andersen C, Licht PB, Toft P. Earlyvisceral pain predicts chronic pain after laparoscopic cholecystectomy.PAIN 2014;155:2400–7.
[5] Breivik H, Stubhaug A. Management of acute postoperative pain: stilla long way to go! PAIN 2008;137:233–4.
[6] Chaparro LE, Smith SA, Moore RA, Wiffen PJ, Gilron I. Pharmacotherapyfor the prevention of chronic pain after surgery in adults. CochraneDatabase Syst Rev 2013;CD008307.
[7] Chapman CR, Davis J, Donaldson GW, Naylor J, Winchester D.Postoperative pain trajectories in chronic pain patients undergoingsurgery: the effects of chronic opioid pharmacotherapy on acute pain.J Pain 2011;12:1240–6.
[8] Crombie IK, Davies HT, Macrae WA. Cut and thrust: antecedent surgeryand trauma among patients attending a chronic pain clinic. PAIN 1998;76:167–71.
[9] De Kock M. Expanding our horizons: transition of acute postoperativepain to persistent pain and establishment of chronic postsurgical painservices. Anesthesiology 2009;111:461–3.
[10] Deumens R, Steyaert A, Forget P, Schubert M, Lavand’homme P,Hermans E, De Kock M. Prevention of chronic postoperative pain:cellular, molecular, and clinical insights for mechanism-based treatmentapproaches. Prog Neurobiol 2013;104:1–37.
[11] Duale C, Ouchchane L, Schoeffler P, Group EI, Dubray C. Neuropathicaspects of persistent postsurgical pain: a French multicenter survey witha 6-month prospective follow-up. J Pain 2014;15:24 e1–20.
[12] Fletcher D, Pogatzki-Zahn E, Zaslansky R, Meissner W; Pain Out Group.euCPSP: European observational study on chronic post-surgical pain.Eur J Anaesthesiol 2011;28:461–2.
[13] Fletcher D, Stamer UM, Pogatzki-Zahn E, Zaslansky R, Tanase NV,Perruchoud C, Kranke P, Komann M, Lehman T, Meissner W; euCgftCTNgotESoA. Chronic postsurgical pain in Europe: an observationalstudy. Eur J Anaesthesiol 2015;32:725–34.
[14] Gerbershagen HJ, Pogatzki-Zahn E, Aduckathil S, Peelen LM, KappenTH, van Wijck AJ, Kalkman CJ, Meissner W. Procedure-specific riskfactor analysis for the development of severe postoperative pain.Anesthesiology 2014;120:1237–45.
[15] Grosu I, Thienpont E, De Kock M, Scholtes JL, Lavand’homme P.Dynamic view of postoperative pain evolution after total kneearthroplasty: a prospective observational study. Minerva Anestesiol2016;82:274–83.
[16] Haroutiunian S, Nikolajsen L, Finnerup NB, Jensen TS. The neuropathiccomponent in persistent postsurgical pain: a systematic literature review.PAIN 2013;154:95–102.
[17] Hayes C, Browne S, Lantry G, Burstal R. Neuropathic pain in the acutepain service: a prospective study. Acute pain 2002;4:45–8.
[18] Hoofwijk DM, Fiddelers AA, Peters ML, Stessel B, Kessels AG, JoostenEA, GramkeHF, MarcusMA. Prevalence and predictive factors of chronicpostsurgical pain and poor global recovery 1 year after outpatient surgery.Clin J Pain 2015;31:1017–25.
April 2017·Volume 158·Number 4·Supplement 1 www.painjournalonline.com S53
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.16

[19] Katz J. One man’s risk factor is another man’s outcome: difference in riskfactor profiles for chronic postsurgical pain maintenance vs transition.PAIN 2012;153:505–6.
[20] Katz J,Weinrib A, Fashler SR, Katznelzon R, Shah BR, Ladak SS, Jiang J,Li Q, McMillan K, Mina DS, Wentlandt K, McRae K, Tamir D, Lyn S, dePerrot M, Rao V, Grant D, Roche-NagleG, Cleary SP, Hofer SO,Gilbert R,Wijeysundera D, Ritvo P, Janmohamed T, O’Leary G, Clarke H. TheToronto General Hospital Transitional Pain Service: development andimplementation of a multidisciplinary program to prevent chronicpostsurgical pain. J Pain Res 2015;8:695–702.
[21] Kehlet H, Dahl JB. Assessment of postoperative pain–need for action!PAIN 2011;152:1699–700.
[22] Lavand’homme P. The progression from acute to chronic pain. Curr OpinAnaesthesiol 2011;24:545–50.
[23] Lavand’homme PM, Grosu I, France MN, Thienpont E. Pain trajectoriesidentify patients at risk of persistent pain after knee arthroplasty: anobservational study. Clin Orthop Relat Res 2014;472:1409–15.
[24] Lavand’homme P, Thienpont E. Pain after total knee arthroplasty:a narrative review focusing on the stratification of patients at risk forpersistent pain. Bone Joint J 2015;97-B(10 suppl A):45–8.
[25] Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth 2008;101:77–86.
[26] Martinez V, Ben Ammar S, Judet T, Bouhassira D, Chauvin M, Fletcher D.Risk factors predictive of chronic postsurgical neuropathic pain: the valueof the iliac crest bone harvest model. PAIN 2012;153:1478–83.
[27] Montes A, Roca G, Sabate S, Lao JI, Navarro A, Cantillo J, Canet J,Group GS. Genetic and clinical factors associated with chronicpostsurgical pain after hernia repair, hysterectomy, and thoracotomy:a two-year multicenter cohort study. Anesthesiology 2015;122:1123–41.
[28] Morze CJ, Johnson NR, Williams G, Moroney M, Lamberton T, McAuliffe M.Knee pain during the first three months after unilateral total knee arthroplasty:a multi-centre prospective cohort study. J Arthroplasty 2013;28:1565–70.
[29] Nikolajsen L, Brix LD. Chronic pain after surgery in children. Curr OpinAnaesthesiol 2014;27:507–12.
[30] Padua L, Aprile I, Cecchi F, Molino Lova R, Arezzo MF, Pazzaglia C; DonCarlo Gnocchi Pain-Rehab Group. Pain in postsurgical orthopedicrehabilitation: a multicenter study. Pain Med 2012;13:769–76.
[31] Page MG, Campbell F, Isaac L, Stinson J, Katz J. Parental risk factors forthe development of pediatric acute and chronic post-surgical pain:a longitudinal study. J Pain Res 2013;6:727–41.
[32] Page MG, Katz J, Romero Escobar EM, Lutzky-Cohen N, Curtis K, FussS, Clarke HA. Distinguishing problematic from nonproblematicpostsurgical pain: a pain trajectory analysis after total knee arthroplasty.PAIN 2015;156:460–8.
[33] Petersen KK, Arendt-Nielsen L. Chronic postoperative pain after jointreplacement. PAIN: Clinical Updates 2016;24:1–6.
[34] Rabbitts JA, Zhou C, Groenewald CB, Durkin L, Palermo TM. Trajectoriesof postsurgical pain in children: risk factors and impact of late painrecovery on long-term health outcomes after major surgery. PAIN 2015;156:2383–9.
[35] Richez B, Ouchchane L, Guttmann A, Mirault F, Bonnin M, Noudem Y,Cognet V, Dalmas AF, Brisebrat L, Andant N, Soule-Sonneville S, DubrayC, Duale C, Schoeffler P. The role of psychological factors in persistentpain after cesarean delivery. J Pain 2015;16:1136–46.
[36] Sayers A,Wylde V, Lenguerrand E, Beswick AD, Gooberman-Hill R, PykeM, Dieppe P, Blom AW. Rest pain and movement-evoked pain as uniqueconstructs in hip and knee replacements. Arthritis Care Res (Hoboken)2016;68:237–45.
[37] Simanski CJ, Althaus A, Hoederath S, Kreutz KW, Hoederath P, LeferingR, Pape-Kohler C, Neugebauer EA. Incidence of chronic postsurgicalpain (CPSP) after general surgery. Pain Med 2014;15:1222–9.
[38] Sommers C. When does nerve injury hurt? PAIN 2010;151:561–2.[39] Thienpont E, Lavand’homme P, Kehlet H. The constraints on day-case
total knee arthroplasty: the fastest fast track. Bone Joint J 2015;97-B(10suppl A):40–4.
[40] Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, Cohen M,Evers S, Finnerup NB, First MB, Giamberardino MA, Kaasa S, Kosek E,Lavand’homme P, Nicholas M, Perrot S, Scholz J, Schug S, Smith BH,Svensson P, Vlaeyen JW, Wang SJ. A classification of chronic pain forICD-11. PAIN 2015;156:1003–7.
[41] Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe-Leitz T,Fu R, Azad T, Chao TE, Berry WR, Gawande AA. Size and distribution ofthe global volume of surgery in 2012. Bull World Health Organ 2016;94:201–9F.
[42] Werner MU, Kongsgaard UE. I. Defining persistent post-surgical pain: isan update required? Br J Anaesth 2014;113:1–4.
[43] Yarnitsky D, Granot M, Granovsky Y. Pain modulation profile and paintherapy: between pro- and antinociception. PAIN 2014;155:663–5.
[44] Zywiel MG, Stroh DA, Lee SY, Bonutti PM, Mont MA. Chronic opioid useprior to total knee arthroplasty. J Bone Joint Surg Am 2011;93:1988–93.
S54 P. Lavand’homme·158 (2017) S50–S54 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.17

Biennial Review of Pain
Innovative treatments for back painG. Lorimer Moseley
1. Introduction and what this review is not
Innovation is the introduction or use of new ideas ormethods.63 “Innovative” research is that which asks a novelquestion or seeks to answer an old question in a new way orusing a new technique. We have long known that innovation isneither easy nor necessarily welcomed—“Our wretchedspecies is so made that those who walk on the well-troddenpath always throw stones at those who are showing a new
road.”115 In health care, innovation is one phase in a continualcycle of innovation–testing–dissemination–practice.
To review innovative treatments of back pain, we must firstdetermine the need for such innovation. This is an importantmatter—sooner or later innovation will be needed at other stagesof the cycle–innovative methods of dissemination,4 promotion19
or participant recruitment,55 innovative approaches to qualitycontrol or clinician adherence. In such cases, the treatment maybe excellent and the focus of innovation shifts to optimising theimpact of the treatment on public health.
Do we still have a problem with back pain? The 1990 GlobalBurden of Disease study sought to quantify the burden of nonfatalhealth outcomes, using a metric that captured years of life livedwith “less than ideal health,” termed “years of life lived withdisability” (YLD).91 That study identified low back pain as the singlemost burdensome nonfatal condition globally, and one of the 4most burdensomenonfatal conditions in every country or region forwhich data were available. This startling discovery presumablytriggered industry and government support to solve what wasclearly a massive public health problem. The 2011 Global Burdenof Disease study may have been expected to illuminate the gainsthat had been made over the previous 20 years. Unfortunately,however, low back pain remained the most burdensome nonfatalcondition, by a larger margin than it was 20 years earlier,accounting for 11% of the total YLD (83 million YLD). Low backpain, affecting 1 in 10 people, was 6 times as prevalent as anginaand twice as prevalent as depression.116 The 2015 updatecategorized back and neck pain together, but showed little or nochange in prevalence or burden.
This disappointing situation is not for want of trying. There aremany treatments already available. Treatment approaches haveoften been based on the work of a particularly prominent orcharismatic clinician (or perhaps entrepreneur). In physiotherapy
for example, such approaches have tended to be named afterthe “guru” who developed them–for example the Maitland,69
McKenzie,74 or Mulligan42 approaches. Other treatments havebeen developed on the basis of empirical research that identifiedbehavioural differences between those who have back pain andthose who do not–for example “motor control” approaches.111
Although such treatments are often innovative, almost withoutexception they are vigorously promoted and widely adopted,sometimes to the extent of institutes and even notional“universities” dedicated to their promotion, before their clinicaleffects are tested with scientific methods. Such treatmentsoccasionally have sensible theoretical justification, but theirproponents are often too conflicted to test them with anyrigour. This is not to say “nothing is effective,” but to highlightthat innovative treatments for back pain do exist, but popularityor unsubstantiated claims of their inventors or proponents,were not considered worthwhile reasons for inclusion in thisreview.
This is also not a review of “effective treatments for back pain.”If one were to review “effective” treatments for back pain, thepicture would be rather large but perhaps somewhat under-whelming. There is now amassive body of randomized controlledtrials (RCTs), systematic reviews, and meta-analyses on treat-ments for back pain.49,101,113,114 As noted, review of thatliterature is outside the scope of this article, but the generalpicture is critically relevant–treatments that do exist, regardless ofthe discipline that offers them and regardless of their provenance,offer on average a small benefit or no benefit at all, aside from thenonspecific effects of treatment. The current state of play formany treatments is reflectedwell in a recent Cochrane systematicreview of psychological therapies for chronic pain,124 recom-mending immediate cessation of RCTs of cognitive behaviouraltherapy (CBT) because the evidence of weak to moderate effectsis very unlikely to change as a result. Importantly, this does notmean these treatments are useless–denying patients access tomildly effective treatments would seem unjustifiable—it meansthat if we are to really reduce the burden of back pain, innovativetreatments are still required.
2. Innovative treatments for primary nociceptivecontributions to back pain
Conventionally and perhaps unsurprisingly, most treatments forback pain have targeted a primary nociceptive “source” of thepain (Fig. 1). Surgeons focus on removing (eg, a discectomy1),anaesthetising (eg, a facet joint block112), or denervating (eg,lumbar rhizotomy23) a particular tissue; physiotherapists mightfocus on strengthening muscles of the trunk,99 altering bio-mechanics (eg, the McKenzie method102), or motor controlstrategy46; psychologists might focus on biofeedback or re-laxation to reduce unwanted trunk muscle tension.20 Oneapproach that has only recently been applied to back pain isregenerative medicine.
Sponsorships or competing interests that may be relevant to content are disclosed
at the end of this article.
Sansom Institute for Health Research, The University of South Australia, Adelaide,
South Australia, Australia
Address: Sansom Institute for Health Research, The University of South Australia,
GPO Box 2473, Adelaide, South Australia 5001, Australia. Tel.: 161 8 83022454.
E-mail address: [email protected] (G. L. Moseley).
PAIN 158 (2017) S2–S10
© 2016 International Association for the Study of Pain
http://dx.doi.org/10.1097/j.pain.0000000000000772
S2 G.L. Moseley·158 (2017) S2–S10 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.18

This approach aims to regenerate the intervertebral disk (IVD) byinjecting stem cells, IVD progenitor stem cells, IVD progenitor cells,or transplanted chondrocytes or IVD cells (or alternatively shock-absorbing artificial polymers100) into the IVD. The animal studiesseemed promising: delayed degeneration when compared withplacebo93; positive impact on inflammatory profile77; evidence ofregeneration of the nucleus pulposus.123 Five observationalstudies, involving people with back pain, usually with imagingevidence of disk degeneration (or ageing) (total n 5139),39,75,76,94,125 have also been positive–4 of the 5 reportsymptomatic improvements. Industry jumped on this innovation:between 2013 and 2014, at least 6 industry-sponsored RCTswere registered at ClinicalTrials.gov alone (NCT0177471;NCT01290367; NCT01860417; NCT01640457; NCT01643681;NCT02097862). Interestingly, and perhaps disappointingly, 1 hasalready been terminated (NCT01771471), 2 have stopped recruit-ing (NCT01860417; NCT01640457), and 1 has not been updatedsince March 2014 (NCT01643681).
Another approach to disk pathology that has attracted someattention is that of antibiotic therapy.2,3 The approach is based onthe idea that bacteria enter the bloodstream during teethbrushingand end up infecting the IVD, causing damage and nociception.The indication of such an infection is proposed to be modic signson scans, a finding that is reported in approximately 8% ofasymptomatic people and 40% of people with back pain.126 Apromising pilot study2 was followed up by an RCT3 that reportedlarge effects on disability, back pain, and leg pain. As noted in theBritish Medical Journal—“the media went crazy”73 about thisRCT, perhaps because of careless public relations and non-declaration of interests by the research group, but also, maybe,because it really did represent a new way of approaching an oldproblem. There is no doubt that 100 days of antibiotics would beeasier than regular exercise, surgery, or injections. Perhaps
however, things were not as they seemed. For example, therewas no effect in the placebo group; the study report wasinconsistent with the trial registry report; if teethbrushing was thebacterial entry pathway, the risk of recurrence would presumablybe quite high.56 It is perhaps unsurprising that the study attractedthorough critique in the peer-reviewed literature56 and theblogosphere.92 A subsequent open trial by a separate researchgroup failed to replicate an effect95 and, even if we were topresume that things were as they were reported to be, theimplications of placing up to 40% of patients with back pain ona 3-month course of antibiotics, with no ongoing protectionagainst reinfection, and in an increasingly antibiotic resistantworld, are by no means trivial. One more registered RCT(2013-004505-14) is ongoing.
The final “diskocentric” approach to emerge in the last decadeis that of injecting methylene blue into the IVD.96,97 Methyleneblue is thought to have a neuroablative or possibly antiinflam-matory effect through its action on nitric oxide.36,44 Itsapplication to back pain was outrageously successful. Targetingpeople with low back pain considered diskogenic on the basisof diskography results, a pilot trial97 was followed by an RCT,96
with the treated group showing a drop in mean pain ratings from70/100 to 20/100 and a similar drop in disability. Bogduk’seditorial on the study rightly described the results as out-standing, unprecedented, and unrivalled11 (although the in-novative approach of wearing woolen underwear for back pain53
reported similar remarkable results–in the words of MarcelloTruzzi—“extraordinary claims require extraordinary proof”).Bogduk urged the field to prioritise replication of the methyleneblue study. One observational study seemed positive, althoughnot so magnificently as the original trial.48 An RCT has beenregistered34 and is ongoing; another has failed to show any long-term effects.52
Figure 1. Innovative treatments for back pain that target the intervertebral disk. IVD, intervertebral disk; RCT, randomised clinical trial.
April 2017·Volume 158·Number 4·Supplement 1 www.painjournalonline.com S3
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.19

3. The elephant in the room: the disconnect betweenstructural imperfections and pain
Bettermethodsof treating specific structures in the back are clearlywelcomed; however, their usefulness is currently limited by theclear disconnect between back pain and evidence of structuralpathology. Although imaging findings are more prevalent in thosewith chronic back pain than in those without,16 2 in every 3asymptomatic 40-year olds have signs of disk degeneration; 1 in 5of facet joint degeneration and 1 in 10 of spondylolisthesis.17
Although longitudinal data that track imaging findings alongside thedevelopment and resolution of backpainwould seemacrucial nextstep, the commonality of positive findings in asymptomaticindividuals and thedifficulty of properly diagnosing agiven structureas causing someone’s back pain cast a long shadow when itcomes to identifying effective treatments directed at a specificspinal tissue pathology. This does not mean tissue-basedproblems are irrelevant for our consideration of back pain, nordoes it mean that diagnostics are totally useless. However, it doesstrongly compel us to critically review the role of imaging findings inan individual’s pain experience.
One innovative way around this problem may be to matchtreatments to patients on the basis of their clinical presentationrather than on the basis of their imaging. Such an approach relieson accurate screening to direct patients to “their” most beneficialpathway. There have been several tools developed for thispurpose (eg, the StartBack tool)40 and some studies seempromising, particularly for minimising inappropriate or excessivetreatment for those who would have recovered anyway.33,41
However, a recent systematic review casts significant doubt overthe accuracy of these tools—all seem poor at delineating patientswho will develop chronic pain from those who will not.50 Thisresult is perhaps not surprising to those who have been critical ofpredictive screening tools both in the peer-reviewed literature38
and the blogosphere (see the provocatively title R.I.P. PrescriptiveClinical Prediction Rules25 for one such account).
The troubling disconnect between evidence of structuralpathology and back pain, and the underwhelming results ofattempts to match patients to treatment pathways based on theirclinical presentation, encapsulate a difficulty that permeates acrossclinical pain conditions—that of the “fearful and wonderful complex-ity of pain.”82 This challenge is prime for those looking for newanalgesics—“the greatest translational barrier lies in the distinctionbetween nociception and pain”12—and may underpin the persis-tence in clinical settings of ineffective but not risk-free treatments,even after RCTs show those treatments to offer no benefit beyondtheir nonspecific effects. Moreover, it is possible that some of thesetreatments are given to patients who should be categorized ina fourth group—those who would have recovered if we had nottreated them. This latter possibility is sufficiently pertinent to foster theidea that a highly innovative approach to back painmight be to “stopproviding ineffective and unnecessary care for back pain, particularlycare that is also expensive, invasive, or potentially harmful (Maher C,personal communication, September 2016).”
4. Shifting sights: innovative approaches to changesin cortical bodily representations
The brain holds multiple bodily and spatial “maps”—multisensoryneural networks that subserve the regulation and protection of thebody and the space around it, networks that have been collectivelytermed “the cortical bodymatrix”.84 The last decadehas seen rapidprogress in our understanding of the relationship between chronicpain and disruptions of these bodily representations (for reviews
see Refs. 71,83,84,121). Regarding back pain, disrupted repre-sentations have been observed in the motor,14,15,109 tac-tile,22,57,60,81 and spatial79,81,120 domains. Broadly speaking,these deficits reflect a loss of precision, as evidenced in alteredfunctional imaging data and altered performance in behaviouraltasks involving the back. For example, patients are unable tovoluntarily move their back without also moving their pelvis, theycannot differentiate 2 separate tactile stimuli unless they are a longway apart,60 and they process stimuli delivered to the affected sideof the body midline more slowly than identical stimuli delivered tothe healthy side, even when the stimuli are delivered to the handsheld near the back, rather than to the back itself.79
The imprecision that characterizes these disruptions of corticalrepresentation can be understood in terms of flattening of“activation probability gradients”78 or reduction in the differencein probability density function of adjacent neurone-to-neuroneconnections.98 That such changesmight be driven by local brain-bound inflammatory mechanisms was mooted some time ago,6
seems supported by the growing evidence of neuroimmunemediators of chronic pain,35 but remains to be clearly demon-strated. Nonetheless, progress in our understanding of themultisensory mechanisms that underpin bodily representationshas revealed potential pathways by which precision might bereinstated in people with back pain. Those pathways fall into 2broad innovations—sensory discrimination training and multi-sensory augmentation (Fig. 2).
Sensory discrimination training was first developed for thetreatment of phantom limb pain in amputees,31 on the basis ofa very strong relationship between phantom limb pain (but notnonpainful phantom limb feelings) and reorganization of theprimary sensory cortex (S1).32 Sensory discrimination traininginvolved a range of different stimuli being delivered to the stumpand the patient discriminating between them on the basis oflocation and quality of the tactile input.31 Patients showedcorrelated improvement in pain and normalization of corticalresponses to tactile stimuli delivered to the face—an area adjacentin primary sensory cortex to the hand. Discovery of corticalreorganization in people with complex regional pain syndrome68—although see Refs. 26,27 for critical clarifications of the initialdata—led to an initial investigation of tactile discrimination trainingin that group, with preliminary data appearing promising.89 S1reorganization is also present in people with back pain.30 Tactilediscrimination training has been attempted as a stand-alonetreatment for back pain7,119. A recent systematic review showedthat most trials show reductions of pain that are statisticallysignificant, suggesting it might be useful as part of multimodalintervention in appropriate patients. The effects seem too smallhowever, to expect clinically meaningful improvement from tactilediscrimination training as a stand-alone treatment.47
Targeting imprecise motor representations was developed asa treatment on the basis of a different theoretical rationale to thatpresented here. We have now learnt that specific contraction ofparticular muscles, most often the lumbar multifidus or thetransversus abdominis, partially normalizes primary motor cortex(M1) disorganization in people with back pain,110 as well as theabnormal activation of thesemuscles during postural tasks.108 Thesymptomatic effects of motor precision training as a stand-alonetreatment seem to be superior to those of minimal or no treatmentand similar to those offered by manual therapy62 or generalexercise.61
Themost parsimonious interpretation of the small but consistenteffects of discrimination training is that imprecise motor or tactilerepresentations are not major contributors to back pain. However,an alternative explanation that should trigger further innovations is
S4 G.L. Moseley·158 (2017) S2–S10 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.20
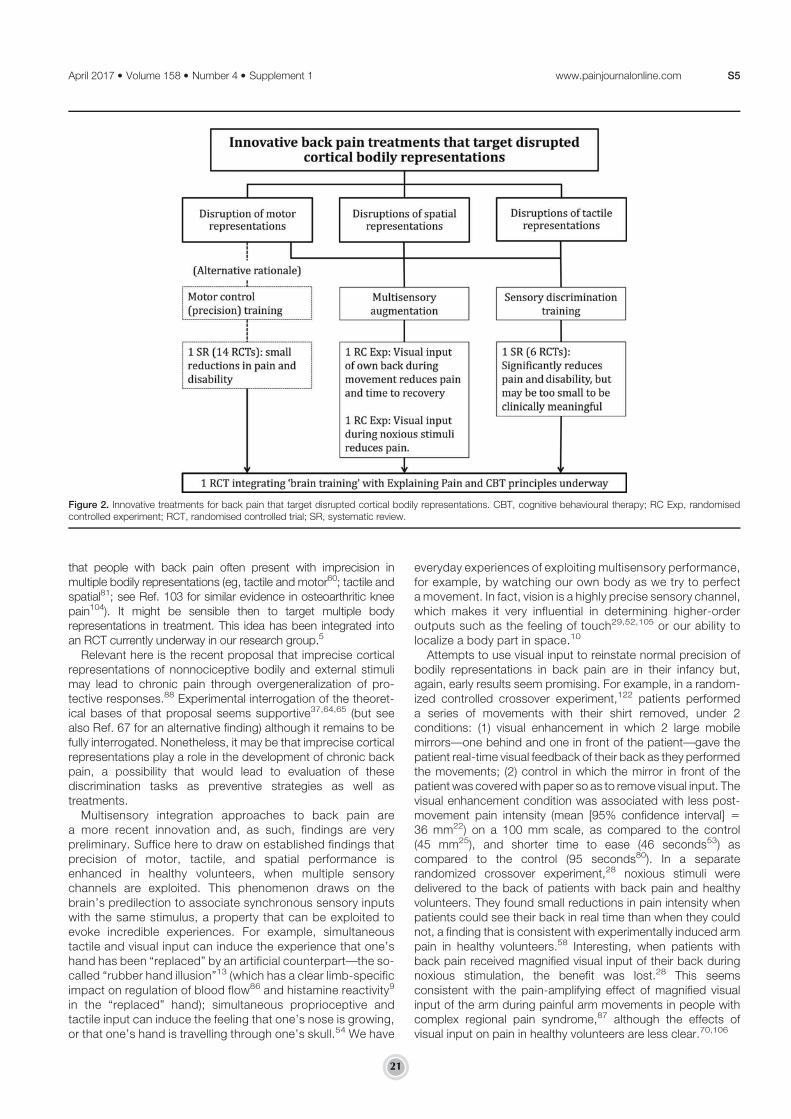
that people with back pain often present with imprecision inmultiple bodily representations (eg, tactile and motor60; tactile andspatial81; see Ref. 103 for similar evidence in osteoarthritic kneepain104). It might be sensible then to target multiple bodyrepresentations in treatment. This idea has been integrated intoan RCT currently underway in our research group.5
Relevant here is the recent proposal that imprecise corticalrepresentations of nonnociceptive bodily and external stimulimay lead to chronic pain through overgeneralization of pro-tective responses.88 Experimental interrogation of the theoret-ical bases of that proposal seems supportive37,64,65 (but seealso Ref. 67 for an alternative finding) although it remains to befully interrogated. Nonetheless, it may be that imprecise corticalrepresentations play a role in the development of chronic backpain, a possibility that would lead to evaluation of thesediscrimination tasks as preventive strategies as well astreatments.
Multisensory integration approaches to back pain area more recent innovation and, as such, findings are verypreliminary. Suffice here to draw on established findings thatprecision of motor, tactile, and spatial performance isenhanced in healthy volunteers, when multiple sensorychannels are exploited. This phenomenon draws on thebrain’s predilection to associate synchronous sensory inputswith the same stimulus, a property that can be exploited toevoke incredible experiences. For example, simultaneoustactile and visual input can induce the experience that one’shand has been “replaced” by an artificial counterpart—the so-called “rubber hand illusion”13 (which has a clear limb-specificimpact on regulation of blood flow86 and histamine reactivity9
in the “replaced” hand); simultaneous proprioceptive andtactile input can induce the feeling that one’s nose is growing,or that one’s hand is travelling through one’s skull.54 We have
everyday experiences of exploiting multisensory performance,for example, by watching our own body as we try to perfecta movement. In fact, vision is a highly precise sensory channel,which makes it very influential in determining higher-orderoutputs such as the feeling of touch29,52,105 or our ability tolocalize a body part in space.10
Attempts to use visual input to reinstate normal precision ofbodily representations in back pain are in their infancy but,again, early results seem promising. For example, in a random-ized controlled crossover experiment,122 patients performeda series of movements with their shirt removed, under 2conditions: (1) visual enhancement in which 2 large mobilemirrors—one behind and one in front of the patient—gave thepatient real-time visual feedback of their back as they performedthe movements; (2) control in which the mirror in front of thepatient was coveredwith paper so as to remove visual input. Thevisual enhancement condition was associated with less post-movement pain intensity (mean [95% confidence interval] 536 mm22) on a 100 mm scale, as compared to the control(45 mm25), and shorter time to ease (46 seconds53) ascompared to the control (95 seconds80). In a separaterandomized crossover experiment,28 noxious stimuli weredelivered to the back of patients with back pain and healthyvolunteers. They found small reductions in pain intensity whenpatients could see their back in real time than when they couldnot, a finding that is consistent with experimentally induced armpain in healthy volunteers.58 Interesting, when patients withback pain received magnified visual input of their back duringnoxious stimulation, the benefit was lost.28 This seemsconsistent with the pain-amplifying effect of magnified visualinput of the arm during painful arm movements in people withcomplex regional pain syndrome,87 although the effects ofvisual input on pain in healthy volunteers are less clear.70,106
Figure 2. Innovative treatments for back pain that target disrupted cortical bodily representations. CBT, cognitive behavioural therapy; RC Exp, randomisedcontrolled experiment; RCT, randomised controlled trial; SR, systematic review.
April 2017·Volume 158·Number 4·Supplement 1 www.painjournalonline.com S5
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.21

5. Theory-driven enhancement of one treatmentby another
The underwhelming evidence with respect to tried and truetreatments for back pain suggests that it might be prudent to stoptesting these treatments and instead look for new ways theireffect might be enhanced by augmenting them with otherinterventions (Fig. 3). Several research teams have takena theory-driven approach to this idea. One particularly innovativeexample is that of cannabis-enhanced extinction training (Flor,PhD, October 2016, unpublished data). This idea was driven bystrong evidence that the cannabinoid receptor plays a major rolein extinction of aversive memories.72 In a randomized, double-blind, placebo-controlled trial that compared extinction trainingplus placebo to extinction training plus cannabis (THC9), thecombination of extinction training and cannabis had a clinicallyimportant benefit in pain intensity and interference.
Other theory-driven approaches look to augment the effect ofCBT, by example, augmenting a CBT programme with preprog-ramme explaining pain. Explaining pain refers to a range ofstrategies that use conceptual change and instructional designtheory to change the patient’s own conceptualization of thebiological cause of their pain.78,82 Explaining pain is different fromconventional education approaches, which have been used asthe control treatment in RCTs of explaining pain80,85,90 (see Ref.82 for an account of key differences in material and delivery). Theidea of preceding CBT with explaining pain was driven by theobservation that CBT relies on taking a truly biopsychosocialapproach to pain—encouraging activity despite pain, but such anapproachmakes no sense if pain is believed to reflect nociceptionor damage. The initial pilot RCT showed a clear advantage ofexplaining pain, and the effect emerged 6 months after theintervention started and increased at 12month follow-up. A largerRCT interrogating the usefulness of a modified version of thisapproach—explaining pain and cognitive reassurance—to im-prove recovery after an acute episode of back pain (thus reducingthe development of chronicity) is currently underway.107 Furtherinnovation in this line of research is leading to the use of hypnotic
suggestion to further enhance the effects of explaining pain.There is a clear and solid theoretical basis for this proposition andpreliminary data show that hypnosis enhances the effects ofcognitive therapy,43 which suggests that further exploration ofthis idea is warranted. Pilot trials are currently underway.
Some caveats and recommendations are appropriate here.There is no doubt that innovative treatments are emerging andpreliminary results seem promising. However, this has been thecase for many treatments across all of health care and many haveturned out to be useless when they are tested in large definitivetrials. This reality highlights the need to prioritise evaluation of a newtreatment with empirical methods over promoting it on the basis ofits promise. It also points to an important aspect of transparencyand replication that is still to bewidely endorsed in our field—that ofregistering and locking study protocols before undertaking thestudy, a practice that might well be applied to pilot studies ofinnovative treatments, not just major clinical trials. Anotherdevelopment that has the potential to be a truly innovativecontribution is that of developing an effective mechanism withwhich to obtain an early reliable signal of the likely benefit of a newtreatment. The disappointment of treatments not living up to theirpromise and the difficulty of winding back popular ineffectivetreatments might thus be avoided. Finally, the possibility remainsthat some of these innovative treatment approaches are of morebenefit to patients than we think they are. That is, a furtherinnovation may be to expand the patient voice in the selection ofresearch methods and outcome variables—we may well discoverthat patients find these treatments to be of greater benefit than ourcurrent outcomes suggest.
6. Mass conceptual change
Wehave long known that pain is not ameasure of tissue state, noreven of nociceptor activity.117,118 Although the endorsement ofthis idea has greatly increased among clinicians,66 the oldconceptualization understandably remains common among thegeneral public. This is very important for the management of painbecause pain is critically dependent onwhat one thinks is causing
Figure 3. Theory-driven enhancement of one treatment by another. RCT, randomised controlled trial; levels of evidence: Level 1a—several meta-analysesshowing consistent effects; Level 1b—a few meta-analyses showing consistent effects; Level 2a several RCTs and a systematic review.
S6 G.L. Moseley·158 (2017) S2–S10 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.22

it (see Ref. 20 for one lay-friendly account). It follows then, that wemay stand to make significant inroads into the massive burdenincurred by back pain by helping the general public change whatthey think pain actually is.
There is precedent for taking a mass conceptual changeapproach to treating back pain. A multimillion dollar mass mediacampaign was undertaken in one state of Australia between 1997and 1999. The campaign aimed to shift public attitudes aboutwhat to do when you experience back pain, centred around theslogan “back pain: don’t take it lying down.” The campaigninvolved television advertisements for the first 12 months andthen again for the final 3 months of the 3-year period. The primaryoutcomes were the targeted attitudes and metrics associatedwith the costs of workers’ compensation claims for back pain.Attitudes were measurably different from those of a neighbouring“control” state, and therewere clear shifts in all the outcomes overthe course of the campaign. Similar campaigns run in othercountries were less successful, potentially because they did notinvolve television (2 of 3 campaigns), invested less money in thecampaign (2 and perhaps 3—the cost of one campaign remainsunknown), or both.18 Alternatively, perhaps the effectiveness ofsuch a campaign in one jurisdiction and context simply does notgeneralize to another.
A final possibility and perhaps a pointer to the innovative nextstep regarding mass conceptual change may well relate to thenature of the targeted conceptual change. Much has changed inthe last 2 decades about our understanding of pain biology andthe effects of teaching patients about it. It may well be time to takean establishedmethod ofmass conceptual change and apply it toa new target. Considering the rapid and sustained positive effectson pain of explaining pain biology to people already experiencingback pain,24,59,82 onemight predict that “pre-emptive” explainingpain biology might have a protective effect against poor recoveryfrom an acute episode of back pain. Other things have changed inthe last 16 years—perhaps a mass conceptual change strategyshould now integrate social media and web-based mechanismsin addition to, or even instead of, conventional mass mediachannels such as television, radio, and newspapers.
7. Perhaps the grandest innovation of all—taking on“the difficult problem”
We recently proposed that chronic pain in general, and chronicback pain in particular, can rightly be considered “the difficultproblem” in health care.8 Not only are there complex biological,psychological, and social contributors to one’s back pain, thereare also complex societal factors that may in fact be maintainingthe prevalence and burden of the condition. There are powerfulstakeholders in the problem of back pain and their influences arereadily visible in the clinical journeys that patients take, thetreatments they seek, the stigma they experience, and thedifficulty they might face in accessing evidence-based care.These are potentially powerful factors, full review of which isbeyond the scope of this article (see Ref. 8 for more thoroughcoverage of the complex politics of chronic pain). In some ways,the politics of back pain are similar to our emerging picture of backpain itself—powerful and complex protective mechanisms formaintaining the equilibrium of the body (politic) have becomemaladaptive and self-defeating.8
It is not unreasonable to suggest that the most innovativetreatment for back pain would involve taking on these complexsocietal and cultural influences. To do so would requirea magnitude of innovation, collaboration, and commitmentgreater perhaps than we can currently envisage. It may also
require courage—after all, most of us are excited about change ifit is about changing other people but rather turned off by change ifit is about changing ourselves, and most of us are sustained insome way by the fact that we have not yet solved the problem ofback pain.
8. Summary
Innovative treatments for back pain are emerging from severalsectors of our community. Regenerative medicine may end upoffering effective methods to help those for whom their back painreflects a primary nociceptive “driver” in pathological tissue. Betterunderstanding of abnormal brain functions may yet lead toinnovative and effective treatments that target normalization ofthose abnormal functions. Clever combinations of different treat-ments to exploit biological mechanisms that underpin them mayyet yield “superadditive” effects that get patients excited about theirimpact. Perhaps, we should channel our imagination and creativitytoward innovation in helping people to change how they thinkabout pain before they sustain an acute episode of back pain.Alternatively, perhaps innovative strategies to change societaldrivers of back pain will completely revolutionise how people withback pain are treated. Only the future will shed light on thesematters. In the meantime, 3 important issues are already clear.
First, we clearly need innovation—the problem of back pain ismore massive now than it was 20 years ago. Second, we shouldencourage innovation by nurturing connections, creating net-works of clinicians and scientists, both basic and clinical, fromacross disciplines, cultures, and professions, and critically, thismultifaceted network must be closely connected with patients—as Steven Johnson, author of “Where good ideas come from: The
natural history of innovation,”45 noted—“it is not the wisdom ofthe crowd, but thewisdomof someone in the crowd. The networkitself is not smart, but individuals get smarter if they are connectedto the network.” Finally, we should not throw stones at thoseshowing a new road, but, equally, those showing a new roadshould not promote it until scientific studies show it to be good.
Conflict of interest statement
The author has received support from Pfizer, Kaiser Permanente,USA; Workers’ Compensation Boards in Australia, NorthAmerica, and Europe; Agile Physiotherapy, USA; ResultsPhysiotherapy, USA; the International Olympic Committee; andthe Port Adelaide Football Club, Australia. He receives royaltiesfor books on pain and rehabilitation, including two books that arecited in this article. He receives speaker fees for lectures on painand rehabilitation.
The author is supported by a Principal Research Fellowshipfrom the National Health &Medical Research Council of Australia.
Acknowledgements
The author acknowledges very helpful suggestions and reviews inthe preparation of the plenary lecture on which this article wasbased, from Dr Neil O’Connell, Brunel University, UnitedKingdom; Prof Benedict Wand, The University of Notre DameAustralia, Fremantle, Australia; Prof Herta Flor, HeidelbergUniversity, Germany; Prof Chris Maher, University of Sydney,Australia; Emma Karran, University of South Australia, Australia;Prof Frank Keefe, Duke University, USA; Prof Marshall Devor,Hebrew University of Jerusalem, Israel; Dr Tasha Stanton,University of South Australia, Australia. The author alsoacknowledges Dr Valeria Bellan, Dr Carolyn Berryman, and
April 2017·Volume 158·Number 4·Supplement 1 www.painjournalonline.com S7
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.23

Simon Kirkegaard, of the University of South Australia, forassistance preparing this article.
Article history:Received 28 October 2016Received in revised form 9 November 2016Accepted 14 November 2016Available online 21 November 2016
References
[1] Ahn Y, Lee SH, Park WM, Lee HY, Shin SW, Kang HY. PercutaneousEndoscopic lumbar discectomy for recurrent disc herniation: surgicaltechnique, outcome, and prognostic factors of 43 Consecutive cases.Spine (Phila Pa 1976) 2004;29:E326–32.
[2] Albert HB, Manniche C, Sorensen JS, Deleuran BW. Antibiotictreatment in patients with low-back pain associated with Modic changesType 1 (bone oedema): a pilot study. Br J Sports Med 2008;42:969–73.
[3] Albert HB, Sorensen JS, Christensen BS, Manniche C. Antibiotictreatment in patients with chronic low back pain and vertebral boneedema (Modic type 1 changes): a double-blind randomized clinicalcontrolled trial of efficacy. Eur Spine J 2013;22:697–707.
[4] Allen HG, Stanton TR, Di Pietro F, Moseley GL. Social media releaseincreases dissemination of original articles in the clinical pain sciences.PLoS One 2013;8:e68914.
[5] Bagg M, Hubscher M, Rabey M, Wand B, O’Hagan E, Moseley G,Stanton T, Maher C, Goodall S, Saing S, O’Connell N, Luomajoki H,McAuley J. The RESOLVE trial for people with chronic low back pain:protocol for a randomised clinical trial. J Physioth 2017;63:47–8.
[6] Banati RB. Brain plasticity and microglia: is transsynaptic glial activationin the thalamus after limb denervation linked to cortical plasticity andcentral sensitisation? J Physiol Paris 2002;96:289–99.
[7] Barker K, Elliot C, Sackley C, Fairbank J. Treatment of chronic backpain by sensory discrimination training. A Phase 1 RCT of a novel device(FairMed) vs TENS. BMC Musculoskelet Disord 2008;9:97.
[8] Barker S, Moseley G. The difficult problem in health care: chronic painand politics of care. Aust Q 2016;87:8–17.
[9] Barnsley N, McAuley J, Mohan R, Dey A, Thomas P, Moseley GL. Therubber hand illusion increases histamine reactivity in the real arm. CurrBiol 2012;21:R945–946.
[10] Bellan V, Gilpin HR, Stanton TR, Newport R, Gallace A, Moseley GL.Untangling visual and proprioceptive contributions to hand localisationover time. Exp Brain Res 2015;233:1689–701.
[11] Bogduk N. A cure for back pain? PAIN 2010;149:7–8.[12] Borsook D, Hargreaves R, Bountra C, Porreca F. Lost but making
progress—where will new analgesic drugs come from? Sci Transl Med2014;6:249sr243.
[13] Botvinick M, Cohen J. Rubber hands “feel” touch that eyes see. Nature1998;391:756.
[14] Bowering KJ, Butler DS, Fulton IJ, Moseley GL. Motor imagery inpeople with a history of back pain, current back pain, both, or neither.Clin J Pain 2014;30:1070–5.
[15] Bray H, Moseley GL. Disrupted working body schema of the trunk inpeople with back pain. Br J Sports Med 2011;45:168–73.
[16] Brinjikji W, Diehn FE, Jarvik JG, Carr CM, Kallmes DF, Murad MH,Luetmer PH. MRI findings of disc degeneration are more prevalent inadults with low back pain than in asymptomatic controls: a systematicreview and meta-analysis. Am J Neuroradiol 2015;36:2394–9.
[17] Brinjikji W, Luetmer PH, Comstock B, Bresnahan BW, Chen LE, DeyoRA,Halabi S, Turner JA, Avins AL, James K,Wald JT, Kallmes DF, JarvikJG. Systematic literature review of imaging features of spinal degenerationin asymptomatic populations. Am J Neuroradiol 2015;36:811–16.
[18] Buchbinder R. Self-management education en masse: effectiveness ofthe back pain: don’t take it lying down mass media campaign. Med JAust 2008;189:S29–32.
[19] Buchbinder R, Jolley D, Wyatt M. Population based intervention tochange back pain beliefs and disability: three part evaluation. BMJ 2001;322:1516–20.
[20] Bush C, Ditto B, Feuerstein M. A controlled evaluation of paraspinalEMG biofeedback in the treatment of chronic low back pain. HealthPsychol 1985;4:307–21.
[21] Butler DS, Moseley GL, Sunyata. Explain pain. Adelaide, Australia:Noigroup Publications, 2013.
[22] Catley MJ, O’Connell NE, Berryman C, Ayhan FF, Moseley GL. Istactile acuity altered in people with chronic pain? A systematic reviewand meta-analysis. J Pain 2014;15:985–1000.
[23] Cho J, Park YG, Chung SS. Percutaneous radiofrequency lumbar facetrhizotomy in mechanical low back pain syndrome. Stereotact FunctNeurosurg 1997;68(pt 1):212–17.
[24] Clarke CL, Ryan CG,Martin DJ. Pain neurophysiology education for themanagement of individuals with chronic low back pain: systematicreview and meta-analysis. Man Ther 2011;16:544–9.
[25] Cook C. R.I.P. Prescriptive clinical prediction rules. Available at:Bodyinmind.org. Accessed November 26, 2016.
[26] Di Pietro F, McAuley JH, Parkitny L, Lotze M,Wand BM, Moseley GL,Stanton TR. Primary somatosensory cortex function in complex regionalpain syndrome: a systematic review and meta-analysis. J Pain 2013;14:1001–18.
[27] Di Pietro F, Stanton TR, Moseley GL, Lotze M, McAuley JH.Interhemispheric somatosensory differences in chronic pain reflectabnormality of the healthy side. Hum Brain Mapp 2015;36:508–18.
[28] Diers M, Zieglgansberger W, Trojan J, Drevensek AM, Erhardt-RaumG, Flor H. Site-specific visual feedback reduces pain perception. PAIN2013;154:890–6.
[29] Eads J, Lorimer Moseley G, Hillier S. Non-informative vision enhancestactile acuity: a systematic review and meta-analysis. Neuropsychologia2015;75:179–85.
[30] Flor H, Braun C, Elbert T, Birbaumer N. Extensive reorganization ofprimary somatosensory cortex in chronic back pain patients. NeurosciLett 1997;224:5–8.
[31] Flor H, Denke C, Schaefer M, Grusser S. Effect of sensorydiscrimination training on cortical reorganisation and phantom limb pain.Lancet 2001;357:1763–4.
[32] Flor H, Elbert T, Knecht S, Wienbruch C, Pantev C, Birbaumer N,Larbig W, Taub E. Phantom-limb pain as a perceptual correlate ofcortical reorganization following arm amputation. Nature 1995;375:482–4.
[33] Foster NE, Mullis R, Hill JC, Lewis M, Whitehurst DG, Doyle C,Konstantinou K,Main C, Somerville S, Sowden G,Wathall S, Young J,Hay EM; team IMBS. Effect of stratified care for low back pain in familypractice (IMPaCT Back): a prospective population-based sequentialcomparison. Ann Fam Med 2014;12:102–11.
[34] Geurts JW, Kallewaard J-W, Kessels A, Willems PC, van Santbrink H,Dirksen C, van Kleef M. Efficacy and cost-effectiveness of intradiscalmethylene blue injection for chronic discogenic low back pain: studyprotocol for a randomized controlled trial. Trials 2015;16:532.
[35] Grace PM, Hutchinson MR, Maier SF, Watkins LR. Pathological painand the neuroimmune interface. Nat Rev Immunol 2014;14:217–31.
[36] Han X, Kobzik L, Zhao YY, Opel DJ, Liu WD, Kelly RA, Smith TW.Nitric oxide regulation of atrioventricular node excitability. Can J Cardiol1997;13:1191–201.
[37] Harvie DS, Broecker M, Smith RT, Meulders A, Madden VJ, MoseleyGL. Bogus visual feedback alters onset of movement-evoked pain inpeople with neck pain. Psychol Sci 2015;26:385–92.
[38] Haskins R, Cook C. Enthusiasm for prescriptive clinical prediction rules(eg, back pain and more): a quick word of caution. Br J Sports Med2016;50:960–1.
[39] Haufe SM, Mork AR. Intradiscal injection of hematopoietic stem cells inan attempt to rejuvenate the intervertebral discs. Stem Cells Dev 2006;15:136–7.
[40] Hill JC, Dunn KM, Lewis M, Mullis R, Main CJ, Foster NE, Hay EM. Aprimary care back pain screening tool: identifying patient subgroups forinitial treatment. Arthritis Rheum 2008;59:632–41.
[41] Hill JC, Whitehurst DG, Lewis M, Bryan S, Dunn KM, Foster NE,Konstantinou K, Main CJ, Mason E, Somerville S, Sowden G, VohoraK, Hay EM. Comparison of stratified primary care management for lowback pain with current best practice (STarT Back): a randomisedcontrolled trial. Lancet 2011;378:1560–71.
[42] Hing W, Hall T, Rivett DA, Vicenzino B, Mulligan BR. The Mulliganconcept of manual therapy textbook of techniques. Sydney, Australia:Churchill Livingstone, 2015.
[43] Jensen MP, Ehde DM, Gertz KJ, Stoelb BL, Dillworth TM, Hirsh AT,Molton IR, Kraft GH. Effects of self-hypnosis training and cognitiverestructuring on daily pain intensity and catastrophizing in individualswith multiple sclerosis and chronic pain. Int J Clin Exp Hypn 2011;59:45–63.
[44] Jesse CR, Savegnago L, Nogueira CW.Role of nitric oxide/cyclic GMP/K(1) channel pathways in the antinociceptive effect caused by 2,3-bis(mesitylseleno)propenol. Life Sci 2007;81:1694–702.
[45] Johnson S. Where good ideas come from: the natural history ofinnovation. New York: Riverhead Books, 2010.
[46] Jull GA, Richardson CA. Motor control problems in patients with spinalpain: a new direction of therapeutic exercise. JManipulative Physiol Ther2000;23:115–17.
S8 G.L. Moseley·158 (2017) S2–S10 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.24

[47] Kalin S, Rausch-Osthoff AK, Bauer CM. What is the effect of sensorydiscrimination training on chronic low back pain? A systematic review.BMC Musculoskelet Disord 2016;17:143.
[48] Kallewaard JW, Geurts JW, Kessels A, Willems P, van Santbrink H,van Kleef M. Efficacy, Safety, and Predictors of intradiscal methyleneblue injection for discogenic low back pain: results of a multicenterprospective clinical series. Pain Pract 2016;16:405–12.
[49] Karjalainen K, Malmivaara A, van Tulder M, Roine R, Jauhiainen M,Hurri H, Koes B. Multidisciplinary biopsychosocial rehabilitation forsubacute low back pain in working-age adults: a systematic reviewwithin the framework of the Cochrane Collaboration Back ReviewGroup. Spine (Phila Pa 1976) 2001;26:262–9.
[50] Karran E,McAuley J, Traeger A, Hillier S,Moseley G. Howaccurate arelow back pain screening instruments at determining chronic pain risk? Asystematic review and meta-analysis. BMC Medicine [in press].
[51] Kennett S, Taylor-Clarke M, Haggard P. Noninformative vision improvesthe spatial resolution of touch in humans. Curr Biol 2001;11:1188–91.
[52] Kim SH, Ahn SH, Cho YW, Lee DG. Effect of intradiscal methylene blueinjection for the chronic discogenic low back pain: one year prospectivefollow-up study. Ann Rehabil Med 2012;36:657–64.
[53] Kiyak E. The impact of wool in the patients with chronic non-specific lowback pain. Coll Antropol 2012;36:623–6.
[54] Lackner J. Some proprioceptive influences on the perceptualrepresentation of body shape and orientation. Brain 1988;111:281–97.
[55] Lee H, Hubscher M, Moseley G, Kamper S, Traeger A, Skinner I,Williams C, McAuley J. An embedded randomised controlled trial ofa teaser campaign to optimise recruitment in primary care. Clin Trials2016. In press.
[56] Lings S. Antibiotics for low back pain? Eur Spine J 2014;23:469–72.[57] Lloyd D, Findlay G, Roberts N, Nurmikko T. Differences in low back
pain behavior are reflected in the cerebral response to tactile stimulationof the lower back. Spine (Phila Pa 1976) 2008;33:1372–7.
[58] Longo MR, Betti V, Aglioti SM, Haggard P. Visually induced analgesia:seeing the body reduces pain. J Neurosci 2009;29:12125–30.
[59] Louw A, Zimney K, Puentedura EJ, Diener I. The efficacy of painneuroscience education onmusculoskeletal pain: a systematic review ofthe literature. Physiother Theory Pract 2016;32:332–55.
[60] Luomajoki H, Moseley GL. Tactile acuity and lumbopelvic motor controlin patients with back pain and healthy controls. Br J Sports Med 2011;45:437–40.
[61] Macedo LG, Latimer J, Maher CG, Hodges PW, McAuley JH, NicholasMK, Tonkin L, Stanton CJ, Stanton TR, Stafford R. Effect ofmotor controlexercises versus graded activity in patients with chronic nonspecific lowback pain: a randomized controlled trial. Phys Ther 2012;92:363–77.
[62] Macedo LG,Maher CG, Latimer J,McAuley JH.Motor control exercisefor persistent, nonspecific low back pain: a systematic review. Phys Ther2009;89:9–25.
[63] Macquarie dictionary, 6th edition. Sydney, Australia: MacmillanPublishers, 2013.
[64] Madden VJ, Bellan V, Russek LN, Camfferman D, Vlaeyen JW,Moseley GL. Pain by association? Experimental modulation of humanpain thresholds using classical conditioning. J Pain 2016;17:1105–15.
[65] Madden VJ, Harvie DS, Parker R, Jensen KB, Vlaeyen JW, MoseleyGL, Stanton TR. Can pain or hyperalgesia be a classically conditionedresponse in humans? A systematic review and meta-analysis. Pain Med2016;17:1094–111.
[66] Madden VJ, Moseley GL. Do clinicians think that pain can bea classically conditioned response to a non-noxious stimulus? Man Ther2016;22:165–73.
[67] Madden VJ, Russek LN, Harvie DS, Vlaeyen JW, Moseley GL.Classical conditioning fails to elicit allodynia in an experimental studywith healthy humans. Pain Med 2016. In press.
[68] Maihofner C, Handwerker HO, Neundorfer B, Birklein F. Patterns ofcortical reorganization in complex regional pain syndrome. Neurology2003;61:1707–15.
[69] Maitland G. Vertebral manipulation. Essex: Butterworth-Heinnemann,1990.
[70] Mancini F, Longo MR, Kammers MP, Haggard P. Visual distortion ofbody size modulates pain perception. Psychol Sci 2011;22:325–30.
[71] Mansour AR, Farmer MA, Baliki MN, Apkarian AV. Chronic pain: therole of learning and brain plasticity. Restor Neurol Neurosci 2014;32:129–39.
[72] Marsicano G, Wotjak CT, Azad SC, Bisogno T, Rammes G, CascioMG, Hermann H, Tang J, Hofmann C, Zieglgansberger W, Di Marzo V,Lutz B. The endogenous cannabinoid system controls extinction ofaversive memories. Nature 2002;418:530–4.
[73] McCartney M. Antibiotics for back pain: hope or hype? BMJ 2013;346:f3122.
[74] McKenzie R, Kubey C. 7 steps to a pain-free life: how to rapidly relieveback and neckpain using theMcKenziemethod.NewYork:Dutton, 2000.
[75] Meisel HJ, Ganey T, Hutton WC, Libera J, Minkus Y, Alasevic O.Clinical experience in cell-based therapeutics: intervention andoutcome. Eur Spine J 2006;15(suppl 3):S397–405.
[76] Meisel HJ, Siodla V, Ganey T, Minkus Y, Hutton WC, Alasevic OJ.Clinical experience in cell-based therapeutics: disc chondrocytetransplantation A treatment for degenerated or damaged intervertebraldisc. Biomol Eng 2007;24:5–21.
[77] Miyamoto T, Muneta T, Tabuchi T, Matsumoto K, Saito H, Tsuji K,Sekiya I. Intradiscal transplantation of synovial mesenchymal stem cellsprevents intervertebral disc degeneration through suppression of matrixmetalloproteinase-related genes in nucleus pulposus cells in rabbits.Arthritis Res Ther 2010;12:R206.
[78] Moseley GL, Butler DS. Explain pain supercharged. Adelaide, Australia:NOIgroup Publishing, 2017.
[79] Moseley G, Gallace A, Iannetti GD. Neglect-like tactile dysfunction inchronic back pain. Neurology 2012;79:327–32.
[80] Moseley GL. Joining forces - combining cognition-targeted motorcontrol training with group or individual pain physiology education:a successful treatment for chronic low back pain. J Man Manip Therap2003;11:88–94.
[81] Moseley GL. I can’t find it! Distorted body image and tactile dysfunctionin patients with chronic back pain. PAIN 2008;140:239–43.
[82] Moseley GL, Butler DS. 15 Years of explaining pain—the past, presentand future. J Pain 2015;16:807–13.
[83] Moseley GL, Flor H. Targeting cortical representations in the treatmentof chronic pain: a review. Neurorehabil Neural Repair 2012;26:646–52.
[84] Moseley GL, Gallace A, Spence C. Bodily illusions in health anddisease: physiological and clinical perspectives and the concept ofa cortical “body matrix”. Neurosci Biobehav Rev 2012;36:34–46.
[85] Moseley GL, Nicholas MK, Hodges PW. A randomized controlled trialof intensive neurophysiology education in chronic low back pain. Clin JPain 2004;20:324–30.
[86] Moseley GL, Olthof N, Venema A, Don S,Wijers M, Gallace A, SpenceC. Psychologically induced cooling of a specific body part caused by theillusory ownership of an artificial counterpart. Proc Nat Acad Sci U S A2008;105:13169–73.
[87] Moseley GL, Parsons TJ, Spence C. Visual distortion of a limbmodulates the pain and swelling evoked by movement. Curr Biol 2008;18:R1047–8.
[88] Moseley GL, Vlaeyen JW. Beyond nociception: the imprecisionhypothesis of chronic pain. PAIN 2015;156:35–8.
[89] Moseley GL, Zalucki NM,Wiech K. Tactile discrimination, but not tactilestimulation alone, reduces chronic limb pain. PAIN 2008;137:600–8.
[90] Moseley L. Combined physiotherapy and education is efficacious forchronic low back pain. Aust J Physiother 2002;48:297–302.
[91] Murray CJ, Lopez AD. Alternative projections of mortality and disabilityby cause 1990-2020: global burden of disease study. Lancet 1997;349:1498–504.
[92] O’Connell N. Clean teeth, bad back? Available at: bodyinmind.org.Accessed March 12, 2013.
[93] Okuma M, Mochida J, Nishimura K, Sakabe K, Seiki K. Reinsertion ofstimulated nucleus pulposus cells retards intervertebral discdegeneration: an in vitro and in vivo experimental study. J Orthop Res2000;18:988–97.
[94] Orozco L, Soler R, Morera C, Alberca M, Sanchez A, Garcia-SanchoJ. Intervertebral disc repair by autologous mesenchymal bone marrowcells: a pilot study. Transplantation 2011;92:822–8.
[95] Palazzo C, Ferrari M, Lefevre-Colau MM, Nguyen C, Rannou F,Poiraudeau S. Lack of effectiveness of antibiotics in chronic low backpain with Modic 1 changes. Joint Bone Spine. doi 10.1016/j.jbspin.2016.08.001 [e-pub ahead of print].
[96] Peng B, Pang X, Wu Y, Zhao C, Song X. A randomized placebo-controlled trial of intradiscal methylene blue injection for the treatment ofchronic discogenic low back pain. PAIN 2010;149:124–9.
[97] Peng B, Zhang Y, Hou S, Wu W, Fu X. Intradiscal methylene blueinjection for the treatment of chronic discogenic low back pain. EurSpine J 2007;16:33–8.
[98] Perin R, Berger TK, Markram H. A synaptic organizing principle forcortical neuronal groups. Proc Nat Acad Sci U S A 2011;108:5419–24.
[99] Risch SV, Norvell NK, Pollock ML, Risch ED, Langer H, Fulton M,Graves JE, Leggett SH. Lumbar strengthening in chronic low back painpatients: physiologic and psychological benefits. Spine (Phila Pa 1976)1993;18:232–8.
[100] Sakai D, Andersson GB. Stem cell therapy for intervertebral discregeneration: obstacles and solutions. Nat Rev Rheumatol 2015;11:243–56.
April 2017·Volume 158·Number 4·Supplement 1 www.painjournalonline.com S9
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.25

[101] Staal JB, de Bie RA, de Vet HC, Hildebrandt J, Nelemans P. Injectiontherapy for subacute and chronic low back pain: an updated Cochranereview. Spine (Phila Pa 1976) 2009;34:49–59.
[102] Stankovic R, Johnell O. Conservative treatment of acute low-back pain.A prospective randomized trial: McKenzie method of treatment versuspatient education in “mini back school”. Spine (Phila Pa 1976) 1990;15:120–3.
[103] Stanton T, Lin C, Smeets R, Taylor D, Law R, Moseley G. Spatially-defined disruption of motor imagery performance in people withosteoarthritis. Rheumatology 2012;51:1455–64.
[104] Stanton TR, Lin CW, Bray H, Smeets RJ, Taylor D, Law RY, MoseleyGL. Tactile acuity is disrupted in osteoarthritis but is unrelated todisruptions in motor imagery performance. Rheumatology (Oxford)2013;52:1509–19.
[105] Taylor-Clarke M, Kennett S, Haggard P. Vision modulatessomatosensory cortical processing. Curr Biol 2002;12:233–6.
[106] Torta DM, Legrain V, Mouraux A. Looking at the hand modulates thebrain responses to nociceptive and non-nociceptive somatosensorystimuli but does not necessarily modulate their perception.Psychophysiology 2015;52:1010–18.
[107] Traeger AC, Moseley GL, Hubscher M, Lee H, Skinner IW, NicholasMK, Henschke N, Refshauge KM, Blyth FM, Main CJ, Hush JM,Pearce G, McAuley JH. Pain education to prevent chronic low backpain: a study protocol for a randomised controlled trial. BMJOpen 2014;4:e005505.
[108] Tsao H, Druitt TR, Schollum TM, Hodges PW. Motor training of thelumbar paraspinal muscles induces immediate changes in motorcoordination in patients with recurrent low back pain. J Pain 2010;11:1120–8.
[109] Tsao H, Galea MP, Hodges PW. Reorganization of the motor cortex isassociatedwith postural control deficits in recurrent low back pain. Brain2008;131:2161–71.
[110] Tsao H, Galea MP, Hodges PW. Driving plasticity in the motor cortex inrecurrent low back pain. Eur J Pain 2010;14:832–9.
[111] Tsao H, Hodges PW. Persistence of improvements in posturalstrategies following motor control training in people with recurrent lowback pain. J Electromyogr Kinesiol 2008;18:559–67.
[112] van Kleef M, Barendse GA, Kessels A, Voets HM, Weber WE, deLange S. Randomized trial of radiofrequency lumbar facet denervationfor chronic low back pain. Spine (Phila Pa 1976) 1999;24:1937.
[113] van Tulder MW, Cherkin DC, Berman B, Lao L, Koes BW. Theeffectiveness of acupuncture in the management of acute and chroniclow back pain. A systematic review within the framework of theCochrane Collaboration Back Review Group. Spine (Phila Pa 1976)1999;24:1113–23.
[114] van Tulder MW, Ostelo R, Vlaeyen JW, Linton SJ, Morley SJ,Assendelft WJ. Behavioral treatment for chronic low back pain:a systematic review within the framework of the Cochrane Back ReviewGroup. Spine (Phila Pa 1976) 2001;26:270–81.
[115] Voltaire Woolf HI. Voltaire’s philosophical dictionary. London: Allen &Unwin, 1945.
[116] Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M,Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, AckermanI, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, AndersonLM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-ColloS, Barrero LH, Bartels DH, Basanez MG, Baxter A, Bell ML, BenjaminEJ, Bennett D, Bernabe E, Bhalla K, Bhandari B, Bikbov B, BinAbdulhak A, Birbeck G, Black JA, Blencowe H, Blore JD, Blyth F,Bolliger I, Bonaventure A, Boufous S, Bourne R, Boussinesq M,Braithwaite T, Brayne C, Bridgett L, Brooker S, Brooks P, Brugha TS,Bryan-Hancock C, Bucello C, Buchbinder R, Buckle G, Budke CM,Burch M, Burney P, Burstein R, Calabria B, Campbell B, Canter CE,Carabin H, Carapetis J, Carmona L, Cella C, Charlson F, Chen H,Cheng AT, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S,Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, CortinovisM, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M,Dabhadkar KC, Dahiya M, Dahodwala N, Damsere-Derry J, Danaei G,Davis A, De Leo D, Degenhardt L, Dellavalle R, Delossantos A,Denenberg J, Derrett S, Des Jarlais DC, Dharmaratne SD, Dherani M,Diaz-Torne C, Dolk H, Dorsey ER, Driscoll T, Duber H, Ebel B,Edmond K, Elbaz A, Ali SE, Erskine H, Erwin PJ, Espindola P,Ewoigbokhan SE, Farzadfar F, Feigin V, Felson DT, Ferrari A, Ferri CP,Fevre EM, Finucane MM, Flaxman S, Flood L, Foreman K, ForouzanfarMH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabbe BJ,
Gabriel SE, Gakidou E, Ganatra HA, Garcia B, Gaspari F, Gillum RF,Gmel G, Gosselin R, Grainger R, Groeger J, Guillemin F, Gunnell D,Gupta R, Haagsma J, Hagan H, Halasa YA, Hall W, Haring D, HaroJM, Harrison JE, Havmoeller R, Hay RJ, Higashi H, Hill C, Hoen B,Hoffman H, Hotez PJ, Hoy D, Huang JJ, Ibeanusi SE, Jacobsen KH,James SL, Jarvis D, Jasrasaria R, Jayaraman S, Johns N, Jonas JB,Karthikeyan G, Kassebaum N, Kawakami N, Keren A, Khoo JP, KingCH, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R,Lalloo R, Laslett LL, Lathlean T, Leasher JL, Lee YY, Leigh J, Lim SS,Limb E, Lin JK, Lipnick M, Lipshultz SE, Liu W, Loane M, Ohno SL,Lyons R,Ma J,Mabweijano J,MacIntyre MF,Malekzadeh R,MallingerL, Manivannan S, Marcenes W, March L, Margolis DJ, Marks GB,Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH,McDermott MM, McGill N, McGrath J, Medina-Mora ME, Meltzer M,Mensah GA, Merriman TR, Meyer AC, Miglioli V, Miller M, Miller TR,Mitchell PB, Mocumbi AO, Moffitt TE, Mokdad AA, Monasta L,Montico M,Moradi-Lakeh M,Moran A,Morawska L, Mori R, MurdochME, Mwaniki MK, Naidoo K, Nair MN, Naldi L, Narayan KM, NelsonPK, Nelson RG, Nevitt MC, Newton CR, Nolte S, Norman P, NormanR, O’Donnell M, O’Hanlon S, Olives C, Omer SB, Ortblad K, OsborneR, Ozgediz D, Page A, Pahari B, Pandian JD, Rivero AP, Patten SB,Pearce N, Padilla RP, Perez-Ruiz F, Perico N, Pesudovs K, Phillips D,Phillips MR, Pierce K, Pion S, Polanczyk GV, Polinder S, Pope CA III,Popova S, Porrini E, Pourmalek F, Prince M, Pullan RL, Ramaiah KD,Ranganathan D, Razavi H, Regan M, Rehm JT, Rein DB, Remuzzi G,Richardson K, Rivara FP, Roberts T, Robinson C, De Leon FR, RonfaniL, Room R, Rosenfeld LC, Rushton L, Sacco RL, Saha S, SampsonU, Sanchez-Riera L, Sanman E, Schwebel DC, Scott JG, Segui-Gomez M, Shahraz S, Shepard DS, Shin H, Shivakoti R, Singh D,Singh GM, Singh JA, Singleton J, Sleet DA, Sliwa K, Smith E, SmithJL, Stapelberg NJ, Steer A, Steiner T, Stolk WA, Stovner LJ, SudfeldC, Syed S, Tamburlini G, Tavakkoli M, Taylor HR, Taylor JA, TaylorWJ, Thomas B, Thomson WM, Thurston GD, Tleyjeh IM, Tonelli M,Towbin JA, Truelsen T, Tsilimbaris MK, Ubeda C, Undurraga EA, vanderWerf MJ, van Os J, Vavilala MS, Venketasubramanian N,Wang M,Wang W, Watt K, Weatherall DJ, Weinstock MA, Weintraub R,Weisskopf MG, Weissman MM, White RA, Whiteford H, Wiersma ST,Wilkinson JD, Williams HC, Williams SR, Witt E, Wolfe F, Woolf AD,Wulf S, Yeh PH, Zaidi AK, Zheng ZJ, Zonies D, Lopez AD,Murray CJ.Years lived with disability (YLDs) for 1160 sequelae of 289 diseases andinjuries 1990–2010: a systematic analysis for the Global Burden ofDisease Study 2010. Lancet 2012;380:2163–96.
[117] Wall P, McMahon S. The relationship of perceived pain to afferent nerveimpulses. Trends Neurosci 1986;9:254–5.
[118] Wall PD, McMahon SB. Microneuronography and its relation toperceived sensation. A critical review. PAIN 1985;21:209–29.
[119] Wand BM, Abbaszadeh S, Smith AJ, Catley MJ, Moseley GL.Acupuncture applied as a sensory discrimination training tool decreasesmovement-related pain in patients with chronic low back painmore thanacupuncture alone: a randomised cross-over experiment. Br J SportsMed 2013;47:1085–9.
[120] Wand BM, James M, Abbaszadeh S, George PJ, Formby PM, SmithAJ, O’Connell NE. Assessing self-perception in patients with chroniclow back pain: development of a back-specific body-perceptionquestionnaire. J Back Musculoskel Rehabil 2014;27:463–73.
[121] Wand BM, Parkitny L, O’Connell NE, Luomajoki H, McAuley JH,Thacker M, Moseley GL. Cortical changes in chronic low back pain:current state of the art and implications for clinical practice. Man Ther2011;16:15–20.
[122] Wand BM, Tulloch VM, George PJ, Smith AJ, Goucke R, O’ConnellNE, Moseley GL. Seeing it helps: movement-related back pain isreduced by visualization of the back during movement. Clin J Pain 2012;28:602–8.
[123] Wang H, Zhou Y, Huang B, Liu LT, Liu MH,Wang J, Li CQ, Zhang ZF,Chu TW, Xiong CJ. Utilization of stem cells in alginate for nucleuspulposus tissue engineering. Tissue Eng Part A 2014;20:908–20.
[124] Williams AC, Eccleston C, Morley S. Psychological therapies for themanagement of chronic pain (excluding headache) in adults. CochraneDatabase Syst Rev 2012;11:CD007407.
[125] Yoshikawa T, Ueda Y, Miyazaki K, Koizumi M, Takakura Y. Discregeneration therapy using marrow mesenchymal cell transplantation:a report of two case studies. Spine (Phila Pa 1976) 2010;35:E475–480.
[126] Zhang YH, Zhao CQ, Jiang LS, Chen XD, Dai LY. Modic changes:a systematic review of the literature. Eur Spine J 2008;17:1289–99.
S10 G.L. Moseley·158 (2017) S2–S10 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.26

Research Paper
Day-to-day experience in resolution of painafter surgeryTimothy T. Houlea, Scott Millerb, Jason E. Langc, Jessica L. Boothb, Regina S. Curryb, Lynnette Harrisb,Carol A. Aschenbrennerb, James C. Eisenachb,*
AbstractWe know little about the individual pain experience of patients recovering from surgery in the first weeks after hospital discharge.Here, we examine individual differences in the day-to-day experience after 2major surgeries: lower limb total major joint arthroplasty(TJA) and cesarean delivery (CD). Fifty-five TJA patients and 157 CD patients were recruited to complete questionnaires and recordtheir daily pain experiences after surgery. After hospital discharge, patients recorded their pain intensity once daily for 60 days (CD) ortwice daily for 2 weeks, once daily for 2 weeks, weekly for 8 weeks, andmonthly for 3months (TJA). Pain scores weremodeled usinggrowth curve and Bayesian change-point models. Individual differences in the model fits were examined for evidence of day-to-daydifferences in pain. A log time model was the simplest model that fit the data, but examination of the residuals revealed highautocorrelation representing misspecification. A change-point model fit the data better and revealed that the form of recoveryfundamentally changed between days 10 and 21 after surgery. These data add meaningfully to our understanding of recovery frompain after surgery by extending the period of frequent observations a few days after surgery to a 2-month period. These high timeresolution data suggest that there is a typical experience of pain resolution after surgery, but that meaningful subpopulations ofexperience may exist. They also indicate that a transition occurs within 1 month after surgery from 1 pattern of change in pain overtime to another.
Keywords: Growth curve modeling, Postoperative pain, Recovery, Trajectory, Orthopedics, Obstetrics
1. Introduction
Chronic pain after surgery is a major health problem,9,17 yetresearch on its causes and predictors is hindered by our lack ofknowledge of how pain usually resolves. Many rules of thumb arecommonly communicated to patients (eg, “the pain will start tosubside after 3 days”), but little is known about a typical painexperience after surgery and the variability around this typicalexperience. To examine the pain experience after surgery, weused a statistical technique called growth curve modeling.
Growth curve modeling has been previously applied todescribe patterns of recovery over weeks in patients with acutelow back pain5 and over days in hospitalizedmedical and surgicalpatients.10 Patterns of pain resolution in the first 5 to 6postoperative days have been described and correlated withpersistent pain months later,1,4,14 yet the few studies which havemodeled these patterns have been restricted to short periods (2weeks)3 or included paucity (#6) measures.11,13,15,16 The loneexception is a study of 32 subjects who contributed 16observations over 6 weeks after surgery, but modeling was not
applied.7 In this study, we examined a large group of patientsrecovering after surgery for an extended period of time.
To more precisely measure pain resolution after surgery, painmust be measured frequently immediately after surgery andcontinue for at least the time when most individuals reportcomplete resolution. These assessments can be quite burden-some given that many patients report high levels of painimmediately after surgery, a distracting state that might reduceadherence to data collection procedures. If a common painresolution model could be found, individuals whose pain resolvesat the upper or lower bounds of this model could be identified aseither being at high risk of chronic pain or alternatively amongthose whose pain resolves far quicker than normal; in either case,such identification could better target interventions. It is unclear,however, whether pain after surgery resolves according toa single typical trajectory (with some variability around thistrajectory), or is better characterized as consisting of severaldifferent patterns of trajectories (ie, subpopulations), each withtheir own unique variability. Thus, understanding the bestapproach to model change in pain after surgery is an importantstep from both research and translational standpoints.
Our primary aimwas to examine these 3methodological issues.As such, we tested the feasibility of measuring pain intensity inpatients after major surgery on a daily basis for prolonged periodsafter discharge, examined several different statistical models in thesearch for a common pain resolution model and examined subtledeviations in the calibrations of thebest fitting pain resolutionmodelas initial evidence for different subpopulations of individuals’resolution of pain after surgery. We hypothesized that collectingthis data is feasible with only modest levels of missing data, andthat a commonmodel form could be found to characterize the timecourse in reduction of pain after surgery.
Sponsorships or competing interests that may be relevant to content are disclosed
at the end of this article.
a Department of Anesthesiology, Critical Care, and Pain Medicine, Massachusetts
General Hospital, Boston, MA, USA, Departments of b Anesthesiology and,c Orthopaedics, Wake Forest School of Medicine, Winston-Salem, NC, USA
*Corresponding author. Address:Department of Anesthesiology,Wake Forest School
ofMedicine,Medical Center Blvd,Winston-Salem,NC27157-1009, USA. Tel.: (336)-
716-4182; fax: (336) 716-0288. E-mail address: [email protected] (J.C.
Eisenach).
PAIN 158 (2017) 2147–2154
© 2017 International Association for the Study of Pain
http://dx.doi.org/10.1097/j.pain.0000000000001015
November 2017·Volume 158·Number 11 www.painjournalonline.com 2147
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.27

2. Methods
To address the study’s aims, we examine individual differences inthe day-to-day experience during the resolution of pain after 2major surgeries: lower limb total major joint arthroplasty (TJA) andcesarean delivery (CD). These 2 groups of participants werecollected sequentially as part of our ongoing research programexamining pain resolution after surgery, but none of the datareported in this manuscript have been published elsewhere. Eachsurgical population is described below.
2.1. Lower limb total major joint arthroplasty
After institutional review board approval, adult patients (AmericanSociety of Anesthesiologists physical status 1, 2, or 3) undergoingelective TJA (unicompartmental or total knee replacement or hipreplacement) were recruited from a single center (Wake ForestUniversity Health Sciences) into this observational study. Weexcluded patients who did not understand English and pregnantwomen or thosewithin 1 year of childbirth. The trial was registeredbefore enrollment of the first subject (NCT01390298). Thepurpose of the study was explained, questions were answered,and all patients gave written informed consent. Demographics,medical history, indication for surgery, and current joint functionwere recorded. Many questionnaires were completed 1 to 6weeks before surgery but are not considered here (please see thetrial registration for a complete list).
All surgical procedures occurred at Wake Forest UniversityHealth Sciences, and all patients were followed postoperativelyby the members of the Department of Orthopaedics and theRegional Anesthesia and Acute Pain Service of the Department ofAnesthesiology. Surgical, anesthetic, and postoperative analge-sic care was routine and not used in any of the statistical modelsfor this observational study.
Beginning on the day of discharge, patients completed theShort Form McGill Pain Questionnaire,12 a visual analog scale(VAS) for pain intensity (10-cm line anchored on the left with notpainful at all and on the right with most pain imaginable; separatescores for current, withmovement, andmost intense in the last 24hours), and Stress Inventory2 twice a day for 14 days after hospitaldischarge and daily at the end of the day for the following 2weeks.The SF-MPQ and VAS were then collected weekly until 12 weeksafter discharge and then monthly until 6 months after discharge.The SF-MPQ, VAS, and Stress Inventory were completed inapproximately 10 to 15 minutes.
Patients were allowed to choose between paper and pencildiaries or an electronic diary, using a small hand-held device thathad been programmed to query these outcomes using Pen-dragon Forms VI (Pendragon Software, Corp, Chicago, IL).Patients were introduced before surgery to the diary and thetouch screen, and then allowed time to make several practiceentries. They were also asked to make a diary entry witha predetermined set of responses to ensure that they understoodthe diary system.
2.2. Cesarean section
After institutional review board approval, adult patients (AmericanSociety of Anesthesiologists physical status 1, 2, or 3) undergoingnonemergent CD were recruited from a single center (MayaAngelou Women’s Center) into this observational study. Weexcluded patients who did not understand English. The trial wasregistered before enrollment of the first subject (NCT01996592).The purpose of the study was explained, questions wereanswered, and all patients gave written informed consent.
Demographics, medical history, and indication for surgery wererecorded. Many questionnaires were completed 1 to 5 daysbefore surgery but are not considered here (please see the trialregistration for a complete list).
All surgical procedures occurred at the Maya AngelouWomen’s Health Center, and all patients were followed post-operatively by the members of the Department of Obstetrics andGynecology and the Section on Obstetric Anesthesia of theDepartment of Anesthesiology, Wake Forest Health Sciences.Surgical, anesthetic, and postoperative analgesic care wasroutine and not used in any of the statistical models for thisobservational study. Unless contraindicated or refused by theparturient, patients typically receive subarachnoid anesthesiawith intrathecal hyperbaric bupivacaine 10 to 12 mg, 15 to 20 mgfentanyl, and preservative free morphine 150 to 200 mg.
Beginning on the day of discharge, patients completed a seriesof 7 questions through an online survey, paper and pencil forms,or SMS texting daily until 60 days after surgery. These questionswere as follows: What is today’s date? What is your pain intensityright now? What is your pain unpleasantness right now? Whatwas your worst pain in the past 24 hours? What was your worstpain unpleasantness in the past 24 hours? What was youraverage pain in the past 24 hours? What was your average painunpleasantness in the past 24 hours? Scores were numericalbetween 0 (not painful or unpleasant at all) and 10 (worst pain orunpleasantness imaginable).
2.3. Primary outcome
The TJA and CD studies were not coincident in time and usedminimalist (CD) or extensive (TJA) daily reporting. For the purposeof this analysis, we used a common metric in both studies, theworst pain in the previous 24 hours, as the measure to examinetrajectory of recovery from pain after surgery.
2.4. Sample size
Given the lack of previous knowledge regarding the daily timecourse of recovery from pain after discharge after theseprocedures, we requested a time period of up to 12 months torecruit the convenience sample for each of these 2 surgicalpopulations. Because the goals were to explore the nature of thetime course of recovery and the effect size of predictors of thistime course, formal hypothesis testing was not used to guidesample size estimation.
2.5. Statistical methods
Statistical analyses were conducted using R version 3.2 (RFoundation for Statistical Computing, Vienna, Austria) andRStudio version 0.98.501 (RStudio, Inc). Descriptive statisticswere calculated for all variables such that mean (SD) were usedfor normally distributed variables; median (range) for nonpara-metric data; and frequency (percentage) for count data. For allanalyses, 2-tailed hypothesis testing was used with P , 0.05interpreted for statistical significance.
A data-driven approach was used to explore the resolution ofpain that could be attributed to recovery in both CD and TJAcohorts. The daily worst VAS score was chosen as the primaryoutcome given that it was used in both groups for 60 days aftersurgery. Examination of the raw data suggested a curvilineardecline in pain for most individuals. Linear, quadratic, cubic, andlogarithmic curve fitting was explored based on the intuitive fit ofthese forms to the data. In addition, a Gompertz polynomial
2148 T.T. Houle et al.·158 (2017) 2147–2154 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.28

model was also fit based on the models used to describe thewound recovery rates of pressure ulcers.19 Linear mixed modelswere constructed with lme4 (Bates D, Maechler M, Bolker B,Walker S. lme4: linear mixed-effects models using Eigen and S4.R package version. 2014; 1). To fit the models, pain after surgeryfor each cohort was modeled separately with correlated randomeffects used for intercept and change parameters (ie, slopes)based on individual subjects.
To examine patterns in the residuals that could be indicative ofneglected change processes, the autocorrelation function of themodel residuals was examined for each subject during theprocess of determining the best model fit. The first-orderautocorrelation was plotted to characterize the pattern of errors.Because a high degree of autocorrelation remained in theresiduals even for models that fit the data well, an additionalmodel form was applied to characterize a multi-phased changeprocess. For these models, we applied Bayesian change-pointanalysis using MCMCpack (Martin AD, Quinn KM, Park JH.MCMCpack, Version 1.0-1. 2011). Full data and code areavailable on request.
3. Results
3.1. Participant characteristics and daily diaries
During December 2011 through July 2012, N 5 31 participantswho underwent TJA completed a diary during at least 1measurement occasion of the postoperative assessment period.During May 2013 through June 2014, N 5 155 CD participantscompleted a diary during at least 1 measurement occasion of thepostoperative assessment period. Figure 1 displays the dispo-sition of participants who began each study, dropped out for anyreason, and completed the assessment period. Table 1 displaysthe demographic and surgical characteristics of both samples.Orthopedic surgery participants were women (51.6%), white(83.9%), and African American (16.1%), had an average age of61.1 (10.6) andmean Center for Epidemiological Studies Scale ofDepression total score of 14.5 (10.9). Cesarean deliveryparticipants were all women, white (63%), and African American(31%), had an average age of 30.2 (7.0) and mean PROMISdepression total score of 11.2 (4.1).
There were missing data from the daily diaries. Total majorjoint arthroplasty participants each provided a median (range) of49 (18-51) diary entries (N5 1477), of which there were 2 entriesdaily from date of discharge through day 14 after surgery, thenonce daily for the next 14 days, whereas the remaining were
weekly and monthly assessments. Cesarean delivery partic-ipants each provided a median (range) of 57 (1-60) daily diaryentries (N 5 7612) once daily from date of discharge throughday 60 after surgery. Most participants in each surgicalpopulation (97% of TJA and 75% of CD patients) had 7 or fewerdays with missing entries over the 2-month period after surgery(Fig. 2).
The burden on support personnel and method of diary entrydiffered significantly by surgical population. For the CD group,over 90% of participants entered daily diary information throughSMS texting to study personnel. Up to 50 subjects were providingdaily diary information per day at the time of peak enrollment,requiring a minimum of 2 hours per day of study personnel time inreceiving and responding to text messages. A few subjectselected to use paper and pencil, but none returned the forms. Theremainder used a daily online survey with email remindersgenerated by REDCap electronic data capture tool hosted atWake Forest School of Medicine through theWake Forest Clinicaland Translational Science Institute (UL1 TR001420; PI: McClain)8
with more missing data than those using SMS texting.
Table 1
Demographic characteristics.
Lower extremity totalmajor joint arthroplasty(TJA) cohort (n 5 31)
Cesarean delivery (CD)cohort (n 5 155)
Age, y, mean (SD) 61.1 (10.6) 30.2 (7.0)
Sex, n (%)
Male 15 (48.4)
Female 16 (51.6) 155 (100)
Surgery type, n (%)
Knee 21 (67.7)
Hip 10 (32.3)
Race, n (%)
African American 5 (16.1) 47 (31)
White 26 (83.9) 98 (63)
Hispanic 0 (0) 8 (5)
Other 0 (0) 2 (1)
CESD total, mean (SD) 14.5 (10.9)
PROMIS depression total,
mean (SD)
11.22 (4.1)
PROMIS, Promise Health Organization Emotional Distress-Depression Short Form 8b (range [8-40]); CESD,
Center for Epidemiological Studies Scale of Depression Scale (range [0-60]).
Figure 1. Flow chart of participant disposition for both orthopedic and cesarean section cohorts.
November 2017·Volume 158·Number 11 www.painjournalonline.com 2149
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.29

For the TJA group, all participants recorded daily diaryinformation through paper and pencil. Up to 19 subjects wereproviding daily diary information per day at the time of peakenrollment.
3.2. Model forms
Examination of the candidate model forms yielded 2 modelsthat best described the systematic changes in pain over timethat occurs after surgery. The first model predicted that painreports decreased as a function of the log of time (log(time))model. When estimated in these samples, the predictions fromthis model were monotonic in that the individual modelpredictions steadily decreased over time in the vast majorityof individuals (94% TJA and 100% CD) but in a few casesincreased over time (6% TJA and 0% CD). The second modelused a cubic polynomial function that predicted that painreports decreased as a function of the time, time2, and time3
(ie, cubic model). When estimated in these samples, thepredictions from this model reflected 2 inflection points inthe rate of recovery in direction of pain reporting (ie, changes inthe rate of change). Despite the fact that the cubic model usesmore parameters (ie, more information) to describe painreports, it was superior to the log(time) model in fitting thedata from the CD (22,278 (log(time)) vs 21,415 [cubic])patients, but not those undergoing TJA (BIC: 3417 (log(time))vs 4022 [cubic]). The residuals (ie, the lack of fit) from bothmodels were scrutinized and compared. We chose the log(time) form to model change in pain based on its simplicity (1change parameter vs 3), nearly identical fit with the morecomplicated cubic model, better expected performance at theextremes of the observation period, and ease of interpretationfor evaluating external influences on change in pain over time.
The individual model fits are presented in Figure 3A with theresiduals from these fits in Figure 3B. The model parameters forthe 2 samples were
TJA : Pain ¼ 7:73442 1:6013 ðlogðtimeÞÞ
CD : Pain ¼ 7:30232 1:8432 ðlogðtimeÞÞ
The random effects components (variance components)revealed that there is a substantial variation (SE) in intercepts(ie, discharge pain scores) across participants in both samples:TJA (s2 5 13.5 [3.7]), P , 0.001 and CD (s2 5 8.3 [1.0]), P ,0.001. These estimates reflect that participants report a range ofpain experiences after surgery. Furthermore, there is a substantialvariation in slopes (ie, change in pain) across participantsindicating that apparent change in pain rates vary widely acrossparticipants. Finally, there is a substantial association betweenintercepts and slopes in both samples: TJA (23.2 [1.0]), P 50.002 and CD (21.9 [0.3]), P, 0.001, indicating that higher painscores at discharge are associated with more rapid reductionsin pain.
3.3. Day-to-day pain experience during recovery
The log(time) model was themost parsimonious representation ofthe recovery process. However, further examination of how thismodel fit the observed data provides a wealth of informationabout the nature of the recovery process. We examined each ofthe residual series, the variance in pain scores after applying thelog(time) recovery model, for patterns that would reflect eithera lack of fit of the model or suggest some other underlyingprocess not encapsulated by the model. In so doing, we wereable to identify several issues with the model and to identifyseveral change patterns that are not well accounted for by themodel.
The residuals from the log(time) model contained substantialamounts of autocorrelation (Fig. 3C). When the current error (ie,residual) of a prediction is correlated with past values or pastpredictions, a pattern exists in the residuals that can bias theestimates of change. For example, Figure 4 displays individualexamples of several different patterns of change that all introducepatterns (autocorrelation) into the residuals. For ease ofcommunication we named the patterns, and close examinationcan identify where the errors become correlated. In the “fast”reduction in pain, the recovery model underestimates thereduction while attempting to accommodate the many “0” painreports later in the diary. In this case, the intercepts of the model(ie, pain at day 0) are biased low making the model predictions atfirst systematically low and then systematically high for the rest ofthe recovery period. In the pain “flare” pattern, for a short duration,pain intensity is strikingly enhanced, but then returns to itsprevious trajectory. In such cases, the model describes thereduction in pain very well for most of the recovery period, butsubstantially underestimates pain during the pain flare-up. In pain“state” change pattern, the recovery model describes the overallreduction in pain quite well, but close examination indicates thatthe pain reports are consistent from day-to-day but exhibita change in state from higher to lower only after several dayswithin the state (eg, a pain of “4” is experienced for 5 days, butthen resolves to a “3” for 4 days). In the final example, a “delayed”reduction in pain is observed when the pain remains stubbornlyhigh but quickly resolves at a later time. The log(time) model againprimarily underestimates the reduction in pain (especially mid-way through recovery) such that pain reports are predicted to belower than actual for much of the recovery process, but then
Figure 2. Distribution of days with missing data over the 60 days period afterhospital discharge in the 2 surgical populations (TJA in red 5 lower extremitytotal major joint arthroplasty; CD in blue5 cesarean delivery). Of note that thefrequency of diary entry differed between the groups, with 60 days with dataentry for the CD population and 32 days for the TJA population.
2150 T.T. Houle et al.·158 (2017) 2147–2154 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.30

substantially overestimates the pain after it has resolved. In eachof these examples, the pattern of change deviates from therelationship specified by a log(time) model. Thus, to properlyaccommodate the nature of change, we explored an additionalstrategy to improve fit.
3.4. Change-point models
A change-point model assumes that the nature of change (eg,either the level or slope of change) itself changes during theobservation period. Change-point models are often applied intime-series analyses when a model form abruptly changesbecause of any external reason. We applied these methods, asthey appear to be an intuitive fit for the nature of change aftersurgery or injury. In the recovery process, it is assumed that painresolves fully for most individuals, and that at some point anindividual experiences no pain due to the original injury. In suchcases, the point of complete recovery can be thought of asa change point in that the pain reports afterward are far differentthan that before recovery.
We allowed each participant to have from zero to 3 changepoints in their pain series, and fit a unique model optimizing thenumber and location of the change points. Figure 5 displays thebest fitting locations with the posterior probability of the changepoint occurring at a particular point in time (ie, the probability thatthe change process has changed at that point). Nearly allindividuals in both surgery types exhibited a change pattern,where a change-point fit the data better than assuming a singlemodel form. The location of the change point varied substantiallyacross individuals, but generally followed a normal distribution
with most individuals exhibiting a change point between day 10and 21 after surgery. Figure 3A (bottom panel) shows thepredicted values from a log(time) model with a change point.Figure 3B displays the superior fit of the change-point models tothe data (ie, the residuals are more condensed) and Figure 3Cdemonstrates that by incorporating a change point into themodel, the degree of autocorrelation in the residuals is sub-stantially reduced.
4. Discussion
In this study, we pursued several distinct aims. We observed thatdaily diary data collection procedures are feasible in patientsrecovering from surgery. In addition, we identified a simple modeldescribing the resolution of pain after surgery (ie, a log(time)model). When this model is used as a pain resolution model (orrecovery after surgery model), we can gain insight into a “typical”pain experience for a typical person. Finally, we explored whenthis model did not fit the data well and described several patternsof change that might lead to biased estimates of the resolutionprocess. To accommodate the unique process of pain resolution,we devised a strategy using change points that allow the modelform to change over time in response to complete resolution orsome new pain state.
4.1. Feasibility
Those previous reports of pain after surgery have not used dailymeasures for several weeks suggest that investigators recognizethe barriers to this approach. We examined feasibility in 2
Figure 3. Themodeled pain trajectories over time (A), the residuals (ie, error) around these predictions (B) and the first-order autocorrelation of the residuals (ie, howrelated errors are over subsequent time points) (C). The gray represents the total major joint arthroplasty participants and the black the cesarean deliveryparticipants. The top row represents the log(time) models that appear to represent the change in pain over time, but the use of a change-point model (bottom row)fit the data even better while reducing the correlation in the errors.
November 2017·Volume 158·Number 11 www.painjournalonline.com 2151
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.31

populations: (1) elderly patients undergoing major surgery whoexhibit a high incidence of postoperative cognitive dysfunctionand who are often uncomfortable or unfamiliar interacting withnovel electronic devices and (2) young women undergoingsurgery for childbirth who go home to a stressful althoughtypically viewed as positive experience with a new baby, who areat low risk for postoperative cognitive dysfunction, and who are
comfortable and familiar with digital technology. The TJA patientsoverwhelmingly preferred pencil and paper reporting, a methodwhich suffers from the lack of a time stamp to confirm real-timereporting rather than reliance on memory of previous pain. Ina subsequent study in the TJA population (NCT02685735), weare using tablet-based digital entry to a secure REDCap site withgood success (data not shown).
In contrast to the TJA population, CD patients overwhelminglypreferred digital entry, usually through SMS or REDCap surveymethods. These methods allowed study personnel daily toassess compliance on a daily basis and to provide reminders. Itshould be noted that these methods require dedicated researchpersonnel to assess compliance and respond to hardware andsoftware problems 7 days per week.
Regardless of the method used to acquire data, missing dataare inevitable in this setting and missing observations complicatedata analysis using traditional repeated measures analysis ofvariance designs. If the data are missing at random, and factorsthat predict missingness can be included in the model, then thechange estimates are unbiased.6 If data are not missing atrandom (eg, patients with higher pain aremore likely to drop out ofthe study early), then the estimates of change will be biased andfurther efforts must be made to reduce this bias.
4.2. Frequent assessments provide unique perspectives
These data and analyses add meaningfully to our understandingof recovery from pain after surgery in 2 important ways. First, theyextend the period of frequent observations from 5 to 6 days whilepatients are in hospital1,4,14 to a 2months period. Interpretation ofpatterns of pain intensity scores in hospitalized patients isobscured by the analgesic interventions of varying efficacyapplied, the titration of these interventions to pain intensityscores, and the ongoing trend to reduce the period ofhospitalization after surgery. Extending these observations to 2
Figure 4. Examples of change processes that induce a pattern of errors into the residuals. In each example, the distance from the prediction line to the observedpoint contains a temporal pattern such that points nearby can be used to predict the error of subsequent points. This can be the case because of many “0” painscores in a sequence (“fast”) because a small group of points are very aberrant (“flare”), because the change process is not typical of a log(timemodel) (delayed), orbecause the pain scores follow a state-like pattern where the only change levels occasionally.
Figure 5. The location of the change point (x-axis) for each individualparticipant (each row on the y-axis). The size of the circle reflects the probabilitythat there is a change point at that time for that participant.
2152 T.T. Houle et al.·158 (2017) 2147–2154 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.32

months is important, as the presence and intensity of persistentpain at this time period is a high risk factor (odds ratio 18.4) forpain lasting years.18 Second, the current data include a consid-erably larger number of observations than that has beenpreviously acquired (Fig. 6). As noted in Figure 6, the smallnumber of time points has largely restricted analysis to simplemodels (linear and quadratic), and the only study using morecomplex modeling in a large number of subjects was restricted toonly a few days in hospitalized patients.10
4.3. Application of growth curve modeling
In retrospect, it is intuitively obvious that pain experience may notfollow a simple form during recovery from injury. In most cases,pain completely resolves, in which case any model must betruncated, but in many cases pain may fluctuate around zero forseveral days, complicating the decision of when to truncate themodel. In other cases, pain may initially change (either decreaseor increase4) after a pattern that can be well fit, but then changesto a different pattern. Analysis of autocorrelations in the log(time)model in the current study suggested that this shift from 1 patternto another occurs frequently in the postoperative population,leading to our application of a Bayesian change-point model. Wenote that the first (and often only) change point occursapproximately 10 to 21 days after surgery, a time of the mostrapid return toward normal sensory processing leading. This mayalso be the time when processes which foster slow resolution ofpain (eg, the so-called transition to chronic pain) become
manifest. Regardless of this interpretation, the enhancedgranularity of understanding shifting time courses of recoveryfrom pain provided by this time-change model approach may beuseful in assessing efficacy of interventions aimed at speedingrecovery in entire surgical populations or reducing the incidenceof chronic postsurgical pain.
The current data suggest that there is a typical experience ofpain resolution after surgery, but that meaningful subpopulationsof experience may exist. Individuals reported a wide variety ofday-to-day experiences after surgery ranging from very fastresolution of pain (ie, 6 days) to much slower courses (.40 days).Interestingly, the differences in pain resolution varied as muchwithin surgery type as across surgeries, suggesting that individualdifferences play as large a role as surgical insult. Although thedefining trend was pain resolution, there were patterns ofexperience that could be identified (eg, “flare-ups”) that aredifficult to model using only 1 model form.
In addition, identifying latent classes of subjects with initialrecovery patterns or patterns after the first change point couldsubstantially impact our appreciation for the experience of painafter surgery. Some individuals with fast resolution are oftenignored by the chronic pain research community, whereas otherindividuals may initially seem to follow a trajectory toward chronicpain, only to have a rapid resolution later during the 6months aftersurgery. An important question might be how these 2 types ofindividuals differ and how best to predict which individuals are inwhich category.
4.4. Limitations
This is an exploratory analysis that uses 2 disparate surgicalpopulations, but it is difficult to generalize these results beyondthese surgical procedures. The best fitting pain resolutionmodels were remarkably similar between these 2 groups ofpatients, but the extent to which other surgeries might followthe same trajectories is unclear. Different procedures indifferent patient populations will result in different initial painseverity and time of resolution and that it is conceivable that insome cases the form could differ by procedure. However,variability in initial severity or time to resolution could also beconsidered a strength in this attempt to define the general formof recovery.
We considered a wide range of models in selecting the “best”pain resolution model, but other candidates may fit better oraccount for the variety of experiences in a more flexible way. Weattempted to posit a simple model (eg, log(time)) in the context ofa change point and perhaps this model could serve as a startingplace for which to compare other more complex forms of change.For example, there may well be 2 forms of change in the recoveryprocess: an initial recovery model and maintenance phases. Weobserved that many participants experienced pain even after“resolution” (ie, experienced occasional pain after pain reached“0” for the first time), but the extent to which a model thatassumed an inflection of change (eg, a knot or state-changemodel) fits better than our simple approach should be evaluatedin a novel data set.
Our approach to characterizing the day-to-day experienceof pain was ultimately qualitative, despite the fact that webased our characterizations on patterns in the autocorrelationfunction. Data-driven procedures have been developed tooptimize latent classes of models, but our modest sample sizeprecluded the use of these procedures (eg, latent class growthcurve models). Future work should use such procedures asprudent.
Figure 6. Summary of previous studies of recovery after surgery1,3,4,7,11,13–16
or with serial time sampling in medical patients,5,10 showing number ofsamples obtained per patient and the modeling period. Each symbolrepresents a single study, unless otherwise noted, in when no formal model(red) or linear (black), quadratic (green), or complex (orange) models were fit tothe data.
November 2017·Volume 158·Number 11 www.painjournalonline.com 2153
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.33

4.5. Conclusions
These data demonstrate the feasibility of acquiring daily painassessments for 2 months after surgery in young as well as olderpatients undergoing major surgery, although the burden on studypersonnel is large and missing data are frequent. Despite theseproblems, this approach yields an adequate number of obser-vations for growth curvemodeling, something that heretofore hasnot been possible at this level of detail in this 2-month time period.The Bayesian change-point model that best fit these data isbiologically plausible, suggests a time period in which transitionsto persistent pain or healing occurs, and applies in this modestsample size to disparate surgical procedures. Its application toa broader surgical population and replication will lay thefoundation for its use as a novel outcome measure.
Conflict of interest statement
J. C. Eisenach consults to Adynxx (San Francisco, CA, USA) andTEVA Pharmaceutical Industries (North Wales, PA, USA) re-garding preclinical and clinical analgesic development of analge-sics. Adynxx is developing agents to speed recovery fromsurgery, but does not use the methods described in thismanuscript and did not participate in this work or the manuscript.The remaining authors have no conflict of interest to declare.
Supported in part by grant P01 GM113852 to J. C. Eisenach(PI) and to S. Miller, J. E. Lang, T. T. Houle, R. S. Curry andC. A. Aschenbrenner from the National Institutes of Health,Bethesda, MD, USA.
Article history:Received 19 May 2017Received in revised form 30 June 2017Accepted 5 July 2017Available online 11 July 2017
References
[1] Althaus A, Arranz BO, Neugebauer E. Distinguishing between painintensity and pain resolution: using acute post-surgical pain trajectories topredict chronic post-surgical pain. EurJ Pain 2014;18:513–21.
[2] Brantley PJ, Waggoner CD, Jones GN, Rappaport NB. A daily stressinventory: development, reliability, and validity. J Behav Med 1987;10:61–74.
[3] Chapman CR, Davis J, Donaldson GW, Naylor J, Winchester D.Postoperative pain trajectories in chronic pain patients undergoingsurgery: the effects of chronic opioid pharmacotherapy on acute pain.J Pain 2011;12:1240–6.
[4] Chapman CR, Donaldson GW, Davis JJ, Bradshaw DH. Improvingindividual measurement of postoperative pain: the pain trajectory. J Pain2011;12:257–62.
[5] Downie AS, Hancock MJ, Rzewuska M, Williams CM, Lin CWC, MaherCG. Trajectories of acute low back pain: a latent class growth analysis.PAIN 2016;157:225–34.
[6] Enders CK. Missing not at random models for latent growth curveanalyses. Psychol Methods 2011;16:1–16.
[7] Gaudilliere B, Fragiadakis GK, Bruggner RV, NicolauM, Finck R, TingleM,Silva J, Ganio EA, Yeh CG, Maloney WJ, Huddleston JI, Goodman SB,Davis MM, Bendall SC, Fantl WJ, Angst MS, Nolan GP. Clinical recoveryfrom surgery correlates with single-cell immune signatures. Sci TranslMed 2014;6:255ra131.
[8] Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Researchelectronic data capture (REDCap)–a metadata-driven methodology andworkflow process for providing translational research informatics support.J Biomed Inform 2009;42:377–81.
[9] Johansen A, Romundstad L, Nielsen CS, Schirmer H, Stubhaug A.Persistent postsurgical pain in a general population: prevalence andpredictors in the Tromso study. PAIN 2012;153:1390–6.
[10] Kannampallil T, Galanter WL, Falck S, Gaunt MJ, Gibbons RD, McNutt R,Odwazny R, Schiff G, Vaida AJ,Wilkie DJ, Lambert BL. Characterizing thepain score trajectories of hospitalized adult medical and surgical patients:a retrospective cohort study. PAIN 2016;157:2739–46.
[11] Lenguerrand E, Whitehouse MR, Wylde V, Gooberman-Hill R, Blom AW.Pain and function recovery trajectories following revision hip arthroplasty:short-term changes and comparison with primary hip arthroplasty in theADAPT cohort study. PLoS One 2016;11:e0164839.
[12] Melzack R. The short-form McGill pain questionnaire. PAIN 1987;30:191–7.
[13] Miaskowski C, Cooper B, Paul SM, West C, Langford D, Levine JD,Abrams G, Hamolsky D, Dunn L, DoddM, Neuhaus J, Baggott C, DhruvaA, Schmidt B, Cataldo J, Merriman J, Aouizerat BE. Identification ofpatient subgroups and risk factors for persistent breast pain followingbreast cancer surgery. J Pain 2012;13:1172–87.
[14] Page MG, Katz J, Curtis K, Lutzky-Cohen N, Escobar EM, Clarke HA.Acute pain trajectories and the persistence of post-surgical pain:a longitudinal study after total hip arthroplasty. J Anesth 2016;30:568–77.
[15] Page MG, Katz J, Romero Escobar EM, Lutzky-Cohen N, Curtis K, FussS, Clarke HA. Distinguishing problematic from nonproblematicpostsurgical pain: a pain trajectory analysis after total knee arthroplasty.PAIN 2015;156:460–8.
[16] Rabbitts JA, Zhou C, Groenewald CB, Durkin L, Palermo TM. Trajectoriesof postsurgical pain in children: risk factors and impact of late painrecovery on long-term health outcomes after major surgery. PAIN 2015;156:2383–9.
[17] Rappaport BA, Cerny I, Sanhai WR. ACTION on the prevention of chronicpain after surgery: public-private partnerships, the future of analgesicdrug development. Anesthesiology 2010;112:509–10.
[18] Romundstad L, Breivik H, Roald H, Skolleborg K, Romundstad PR,Stubhaug A. Chronic pain and sensory changes after augmentationmammoplasty: long term effects of preincisional administration ofmethylprednisolone. PAIN 2006;124:92–9.
[19] Wallenstein S, Brem H. Statistical analysis of wound-healing rates forpressure ulcers. Am J Surg 2004;188(1A suppl):73–8.
2154 T.T. Houle et al.·158 (2017) 2147–2154 PAIN®
Copyright � 2017 by the International Association for the Study of Pain. Unauthorized reproduction of this article is prohibited.34

35

36

37

38

39

40

41

_________________________________________________________________________________________________________________________
© Copyright 2018 International Association for the Study of Pain. All rights reserved.
IASP brings together scientists, clinicians, health-care providers, and policymakers to stimulate and support the study of pain and translate that knowledge into improved pain relief worldwide.
FACT SHEET No. 1
The Gap Between Knowledge and Practice Persistent pain affects millions of people worldwide across the lifespan and is a global cause of disability in the developed and developing world alike (1). Unfortunately, neither policymakers, nor caregivers, nor system administrators, nor the public understand pain and its impact. Poorly managed pain is costly not only for the affected individuals and their families but also for governments and taxpayers.
The U.S. National Institutes of Health estimates the annual costs of persistent pain from $560 billion to $635 billion. This exceeds the economic costs of the six most costly major health problems: cardiovascular diseases ($309 billion); neoplasms ($243 billion); injury and poisoning ($205 billion); endocrine, nutritional, and metabolic diseases ($127 billion); digestive system diseases ($112 billion); and respiratory system diseases ($112 billion) (2).
In 2010, the IASP Declaration of Montreal stated, “All people have the right to have access to appropriate assessment and treatment of pain by adequately trained health-care professionals.” However, there continues to be a gap between what is known about effective pain management and the actual delivery of appropriate patient care. Professional education about acute, persistent (chronic), and/or cancer pain management has been repeatedly documented as inadequate worldwide. As a result, people continue to deal on their own with the consequences and social stigma associated with their pain and to be limited by their lack of awareness of available treatment options.
Ineffective pain management in the very young to the very old is linked to inadequate pain education. These failures are exacerbated by their potential to be self-perpetuating. Pain education targeting professionals, governments, people with pain and their families, and the public is an important strategy to remedy ineffective pain management practices. The international community can do so much more to improve pain education so that people may have access to appropriate pain treatments.
42

_________________________________________________________________________________________________________________________
© Copyright 2018 International Association for the Study of Pain. All rights reserved.
IASP brings together scientists, clinicians, health-care providers, and policymakers to stimulate and support the study of pain and translate that knowledge into improved pain relief worldwide.
Now is the time to put pain education into the spotlight and help bridge the gap between knowledge and practice.
Overall areas of concern worldwide include the lack of understanding about the sheer magnitude of the public health issues surrounding pain. Professional health and medical education often does not recognize pain content as essential or a high priority. Moreover, the burgeoning opioid crisis, primarily in North America, has led to greater emphasis on recognizing and managing addiction while deprioritizing pain assessment and treatment generally (3). As a result, alarming deficits continue to be documented in the provision of undergraduate pain education, and progress and improvement of postgraduate education remain unacceptably slow. In addition, education for specialized pain management is only sporadically available. The resulting lack of transfer of current research and clinical evidence impedes the dissemination of optimal pain management practices.
Gaps and shortfalls in specific pain-related areas include the following:
Pain content in prelicensure curricula for health-care professionals remains inadequate. Licensure qualifications rarely require competency in appropriate pain assessment and management, particularly the safe and effective use of opioids. Pain-related competencies to ensure graduates are sufficiently educated so they can provide appropriate pain management are underutilized. Post-licensure continuing professional development opportunities for specialized expertise in pain management are lacking. Contemporary evidence is not being transferred to pain management practices in optimal fashion. Voices of individuals and their families are not sufficiently considered in pain management planning and monitoring. Outcome evaluations of pain education are not routinely captured and tend to focus on knowledge rather than competence and improved patient outcomes. The public health impact and related population-health consequences of pain are not well understood. People with persistent pain often lack access to or are unaware of available resources and treatment options.
The Global Year for Excellence in Pain Education strives to address the above gaps by focusing on the following four key areas.
1. Public and Government Education 2. Patient Education 3. Professional Education 4. Pain Education Research
43
_________________________________________________________________________________________________________________________
© Copyright 2018 International Association for the Study of Pain. All rights reserved.
IASP brings together scientists, clinicians, health-care providers, and policymakers to stimulate and support the study of pain and translate that knowledge into improved pain relief worldwide.
To help members with a call to action by organizations, including universities and governments, we have developed prospectuses to promote Public and Government Education, Professional Education, and Self-Management Education (http://s3.amazonaws.com/rdcms-iasp/files/production/public/globalyear/2018%20Global%20Year%20for%20Excellence%20in%20Pain%20Education%20Brand%20Prospectus%201.17.18.pdf). REFERENCES
1. Rice A., Smith B, Blyth F. Pain and the global burden of disease. Pain 2016;157(4): 791-796. 2. Darrell J., Richard P. The Economic Costs of Pain in the United States. J Pain 2012; 13(8): 715-724 3. National Academies of Sciences, Engineering, and Medicine. Pain Management and the Opioid Epidemic: Balancing Societal and Individual Benefits and Risks of Prescription Opioid Use. Washington, D.C.: National Ac ademies Press; 2017. https://www.nationalacademies.org/opioidstudy
AUTHORS
Paul Wilkinson, MB, BS, B.Med.Sci, M.Clin.Ed., MRCGP, FRCA, FFPMRCA Chair, Global Year Task Force Chair, IASP SIG Education Consultant in Pain Medicine Newcastle Pain Management Unit Royal Victoria Infirmary Newcastle upon Tyne, UK Judy Watt-Watson, RN, MSc, PhD Professor Emeritus Lawrence S. Bloomberg Faculty of Nursing Senior Fellow, Massey College University of Toronto Toronto, Ontario, Canada REVIEWERS Daniel B. Carr, MD, DABPM, FFPMANZCA (Hon) Professor of Public Health and Community Medicine (primary appointment) Professor of Anesthesiology and Medicine (secondary appointments) Founding Director, Tufts Program on Pain Research, Education and Policy Public Health Program Tufts University School of Medicine Boston, Mass., USA Andreas Kopf, dr. Med. Dept. of Anaesthesiology and Intensive Care Campus Benjamin Franklin Charité - Medical University Berlin Berlin, Germany
44