journal of dental research … · j dent res 2013 92: 773 originally published online 10 july 2013...
TRANSCRIPT

http://jdr.sagepub.com/Journal of Dental Research
http://jdr.sagepub.com/content/92/9/773The online version of this article can be found at:
DOI: 10.1177/0022034513496428
2013 92: 773 originally published online 10 July 2013J DENT RESC. Stoecklin-Wasmer, A.W.S. Rutjes, B.R. da Costa, G.E. Salvi, P. Jüni and A. Sculean
Absorbable Collagen Membranes for Periodontal Regeneration: A Systematic Review
Published by:
http://www.sagepublications.com
On behalf of:
International and American Associations for Dental Research
can be found at:Journal of Dental ResearchAdditional services and information for
http://jdr.sagepub.com/cgi/alertsEmail Alerts:
http://jdr.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Jul 10, 2013OnlineFirst Version of Record
- Aug 15, 2013Version of Record >>
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research
at Universitaetsbibliothek Bern on November 7, 2013 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
© International & American Associations for Dental Research

773
C. Stoecklin-Wasmer1†, A.W.S. Rutjes2,3†, B.R. da Costa2,4, G.E. Salvi1, P. Jüni2,4, and A. Sculean1*
1Department of Periodontology, University of Bern, Freiburgstrasse 7, 3010 Bern, Switzerland; 2Institute of Social and Preventive Medicine, University of Bern, Finkenhubelweg 11, 3012 Bern, Switzerland; 3Centre for Aging Sciences (Ce.S.I.), G. d’Annunzio University Foundation, Palazzina SEBI 3° livello, Campus Universitario Chieti Scalo, 66100 Chieti Scalo, Italia; 4CTU Bern, Department of Clinical Research, University of Bern, Finkenhubelweg 11, 3012 Bern, Switzerland; †authors contributed equally as co-first authors; *corresponding author, [email protected]
ABSTRACTGuided tissue regeneration (GTR) with bioabsorb-able collagen membranes (CM) is commonly used for the treatment of periodontal defects. The objective of this systematic review of randomized clinical trials was to assess the clinical efficacy of GTR procedures with CM, with or without bone substitutes, in peri-odontal infrabony defects compared with that of open flap debridement (OFD) alone. Primary outcomes were tooth loss and gain in clinical attachment level (CAL). Screening of records, data extraction, and risk-of-bias assessments were performed by two reviewers. Weighted mean differences were esti-mated by random effects meta-analysis. We included 21 reports on 17 trials. Risk of bias was generally high. No data were available for the primary outcome tooth loss. The summary treatment effect for change in CAL for GTR with CM compared with OFD was 1.58 mm (95% CI, 1.27 to 1.88). Despite large between-trial heterogeneity (I2 = 75%, p < .001), all trials favored GTR over OFD. No differences in treat-ment effects were detected between trials of GTR with CM alone and trials of GTR with CM in combi-nation with bone substitutes (p for interaction, .31). GTR with CM, with or without substitutes, may result in improved clinical outcomes compared with those achieved with OFD alone. Our findings support GTR with CM for the treatment of infrabony peri-odontal defects.
KEY WORDS: periodontal disease(s)/periodontitis, surgery, meta-analysis, biomaterial(s), guided tissue regeneration, clinical studies/trials.
DOI: 10.1177/0022034513496428
Received April 30, 2013; Last revision June 6, 2013; Accepted June 9, 2013
A supplemental appendix to this article is published elec-tronically only at http://jdr.sagepub.com/supplemental.
© International & American Associations for Dental Research
CLINICAL REVIEW
INTRODUCTION
Infrabony periodontal osseous defects represent a frequent sequela of peri-odontitis (Papapanou and Tonetti, 2000). Guided tissue regeneration (GTR)
regenerates connective tissue attachment (i.e., forming cementum by inserting collagen fibers and periodontal ligament) and alveolar bone in periodontal defects. A mechanical barrier prevents or retards the apical migration of the gingival epithelium and allows periodontal ligament and bone tissue to selec-tively repopulate the root surface during healing (Nyman et al., 1982; Gottlow et al., 1986; Stahl et al., 1990).
A systematic review that evaluated the effects of GTR with both non- bioabsorbable and bioabsorbable membranes showed that GTR improved attachment gain, reduced pocket depth, and resulted in less gingival recession and more hard-tissue fill than did open flap debridement (OFD) alone (Needleman et al., 2006). The different barrier types [expanded polytetrafluoroethylene (ePTFE) barrier, collagen-derived or polymeric bioabsorbable barrier type] exhibited no significant differences in results (Murphy and Gunsolley, 2003).
However, a second surgical procedure is necessary to remove non- bioabsorbable membranes, and this increases the risk that newly formed tis-sues will be compromised. Moreover, flap elevation for membrane removal may result in crestal bone resorption (Pihlstrom et al., 1983) and decrease coverage of the newly formed tissue, thus interrupting the healing process (Tonetti et al., 1993, 1996). The use of non-bioabsorbable membranes increases risk of membrane exposure and bacterial colonization and thus may inhibit healing (Nowzari et al., 1995). Bioabsorbable membranes, including collagen membranes (CM), have been developed for, and used in, GTR to prevent these problems.
Human histological studies have provided evidence that treatment of infrabony defects, with CM with or without the addition of bone substitutes, improves periodontal regeneration (Parodi et al., 1997; Camelo et al., 1998; Sculean et al., 2004). Combining CM with bone substitutes may prevent the barrier from collapsing, especially in non-contained infrabony defects, and may thus ensure space maintenance (Bunyaratavej and Wang, 2001).
The goal of this systematic review was to assess the clinical, radiographic, and safety outcomes of GTR with absorbable CM, alone or in association with bone substitutes, as compared with those achieved with OFD alone. We also aimed at assessing whether the variations between trials could be explained by characteristics of the procedure or by biases affecting individual trials.
Absorbable Collagen Membranes for Periodontal Regeneration: A Systematic Review
JDR92910.1177/0022034513496428research-article2013
J Dent Res 92(9):773-781, 2013

774 Stoecklin-Wasmer et al. J Dent Res 92(9) 2013
METHODS
We followed a standard protocol for all review steps. We included randomized or quasi-randomized controlled trials (RCTs) with patients who displayed infrabony periodontal defects around sin-gle- or multi-rooted teeth. We excluded studies that addressed only furcation defects. We considered trials that compared GTR with bioabsorbable CM, with or without the application of bone substi-tutes and other bio-active materials, with OFD alone. Primary out-comes were tooth loss and change in clinical attachment level (CAL). Secondary outcomes were change in probing pocket depth (PPD), change in gingival recession (REC), radiographic hard-tis-sue fill, clinical hard-tissue fill (bone sounding, re-entry surgeries), and post-operative complications (membrane exposure, infection).
Literature Search
We searched electronic databases, without language restrictions: Cochrane Central Register of Controlled Trials, MEDLINE, and EMBASE through Ovid (from inception to January 8, 2013) (see Appendix Tables 1 and 2 for search algorithms). This was complemented by a hand search of the Journal of Periodontology, Journal of Clinical Periodontology, and Journal of Periodontal Research up to January 2013 and reviews of bibliographies of all relevant systematic review articles and included trial reports. In addition, we contacted GTR experts with the request to indi-cate any report we had not captured in our online and hand searches. We did not seek unpublished data.
Trial Selection, Data Collection, and Risk-of-Bias Assessment
Titles and abstracts of the search results were screened indepen-dently in duplicate (CS, GES). We considered only reports with available full text, and those were independently assessed by two review authors (CS, GES), who determined their eligibility. Disagreements were resolved by consensus or discussion with a third reviewer (AS). If several reports described the same trial, we chose the most recent report or most complete report as the main report. Remaining reports were checked for complemen-tary data on clinical outcomes, descriptions of study partici-pants, or design characteristics.
Data were extracted independently by two reviewers (CS, AR) and entered into a Web-based extraction form. We collected the following information: patient characteristics (sex, average age, periodontal diagnosis, smoking status); tooth-related characteris-tics (infrabony defect configuration); type of bioabsorbable CM used; type of bone substitute material applied, if applicable; surgi-cal flap design; post-operative care provided (including post-operative systemic antibiotics); enrollment in supportive periodontal treatment (SPT); clinical outcome variables at baseline and longest follow-up observation (tooth retention, CAL, PPD, REC, x-ray hard-tissue level, clinical hard-tissue level); post-operative complications (membrane exposure, infection); trial size, trial design, trial duration (defined as time from surgical intervention until end of follow-up); and number of study centers (single vs. multicenter). We considered concealment of allocation, blinding of patients, surgeons, and those performing outcome assessment, according to current guidelines of the Cochrane
Handbook (Higgins et al., 2011). We determined if analyses were conducted according to the intention-to-treat principle, and if we could detect selective outcome reporting or other biases.
We considered allocation concealment to be adequate if the investigators responsible for patient selection were unable to pre-dict which treatment was next before allocation. Central random-ization and sequentially numbered, sealed, opaque envelopes were considered adequate methods. Concealment was judged to be associated with high risk of bias (ROB) if evidence of inade-quate sequence generation was found. We decided that there was low risk of performance bias (Juni et al., 2001) if the treatment allocation was revealed to the surgeon only after mucoperiosteal flap elevation and defect debridement were completed. However, for split-mouth studies, both test and control sites would need to be prepared simultaneously to be considered at low risk of perfor-mance bias. If an attempt to blind patients was reported, we con-sidered blinding of patients to be associated with low risk of bias. Blinding of outcome assessment was judged to result in low risk of bias if the investigators who performed the outcome assess-ment were explicitly reported to be blind.
Statistical analyses were considered adequate if all random-ized patients were included in the analysis according to the intention-to-treat principle (Rutjes et al., 2012). Trials were con-sidered to have a high risk of selective reporting bias if we identi-fied 1 or more outcome measures in published reports for which results were not reported. We used a cut-off of 25 patients per group in case of parallel designs and 25 patients overall in case of split-mouth designs, to distinguish between small and moderate-to-large trials. This sample size yields a power of 80% to detect a biologically large difference between groups of 0.8 standard deviations, with a two-sided alpha of 0.05. We also examined how defects were ascertained as another source of bias. If multiple sites were measured, but only the deepest defect at baseline was considered in the analysis, we judged this to result in low risk of bias. If whole-tooth means were used, we judged this to be associ-ated with high risk of bias, since this resulted in a dilution of potential effects and a bias toward the null.
Data Synthesis and Analysis
We used results from intention-to-treat analyses at the longest follow-up, whenever reported. We calculated weighted mean differences (WMDs) in changes from baseline between experi-mental and control groups for clinical outcomes. Effect sizes were used if at least 1 trial expressed change values in percent-ages, when other trial(s) expressed results in millimeters. Here, the differences in mean change from baseline across treatment groups were divided by the pooled standard deviation. An effect size of -0.20 standard deviation units was considered a small difference between experimental and control groups, an effect size of -0.50 was a moderate difference, and an effect size of -0.80 a large difference (Cohen, 1988). If differences in mean changes were unavailable, we used the reported baseline and follow-up values to approximate them. If some of the required data were unavailable, we used the approximations previously described (Reichenbach et al., 2007). We expressed binary out-comes as risk ratios (RR) and excluded comparisons with zero events in both groups in the analyses (Sweeting et al., 2004). In studies that used a split-mouth design in which more than 1

J Dent Res 92(9) 2013 Absorbable Collagen Membranes for Periodontal Regeneration 775
tooth contributed to a single treatment arm, we adjusted the standard errors as follows:
If a report provided clinical outcome data for more than 1 site, we pooled the estimates of treatment effects within the trial to pre-vent it from being too heavily weighted in the overall analyses.
We used a standard inverse-variance random-effects model to summarize the estimates of treatment effects across trials to account fully for between-study variance. We quantified between-study variance using the I2 statistic (Higgins et al., 2003), which describes the percentage of variation across trials attributable to heterogeneity rather than chance, and the corresponding Chi2 test. I2 values of 25%, 50%, and 75% were interpreted as low, moder-ate, and high between-trial heterogeneity, although the precision of trials included in the meta-analysis must be considered for interpretation of I2 values (Rücker et al., 2008).
For the primary outcome, the association between trial size and treatment effects was investigated in funnel plots. We plot-ted WMDs on the vertical axis against their standard errors on the horizontal axis. We assessed asymmetry by the asymmetry coefficient. We used the difference in size of WMDs per unit increase in standard error (Sterne and Egger, 2001), which is mainly a surrogate for sample size.
In all analyses, we differentiated between the 2 kinds of GTR: CM with and without bone substitutes. For the outcome CAL gain, we performed stratified analyses by risk-of-bias items: concealment of allocation; blinding of patients, surgeons, and outcome assessors; analysis in accordance with the intention-to-treat principle; selective outcome reporting; and other bias. We also evaluated the following trial characteristics: type of CM (cross-linked vs. native CM), protocol-mandated use of antibiot-ics, percentage of smokers at baseline, and percentage of defects with three-wall involvement. We used uni-variable random-effects meta-regression models to determine if these factors were associated with estimates of treatment effect (Thompson and Sharp, 1999). All statistical analyses were done in STATA version 12.1 (StataCorp, College Station, TX, USA). All p val-ues are two-sided.
RESULTS
Description of Studies
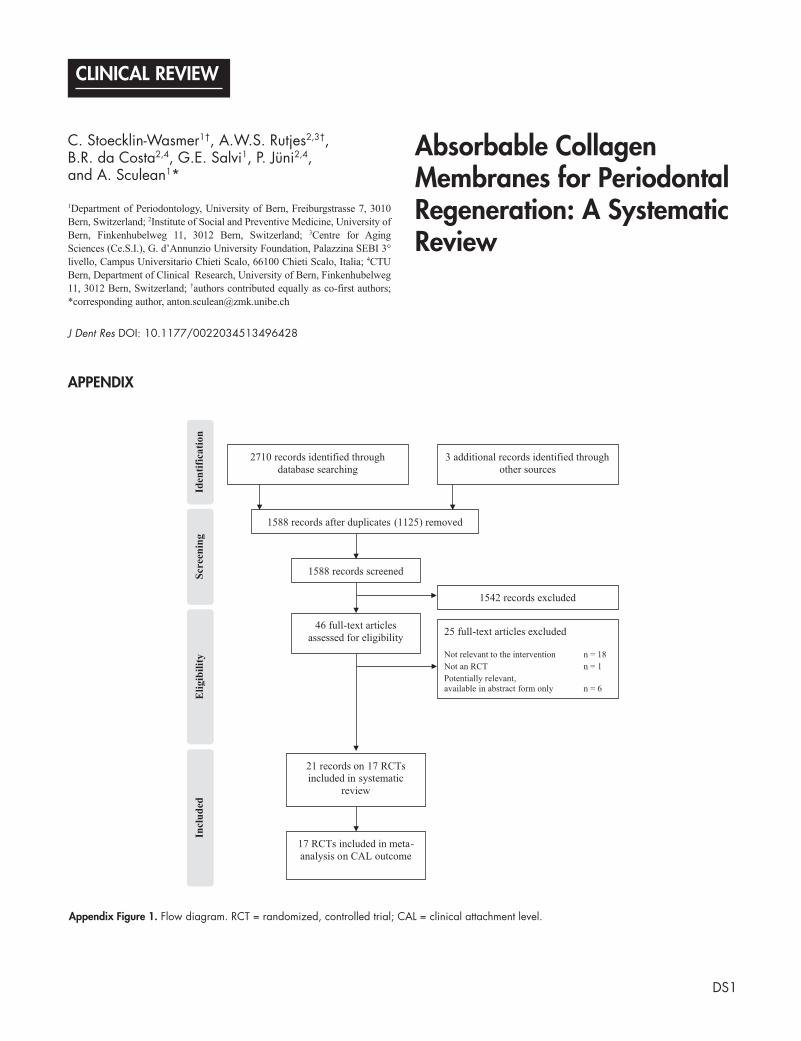
We identified 2,713 references, of which 46 were potentially eligible. Of the 46, 25 reports did not meet our inclusion criteria (see flow diagram in Appendix Fig. 1 and excluded reports in Appendix Table 3). The remaining 21 eligible reports described 17 trials with 35 arms and 507 patients (Blumenthal and Steinberg, 1990; Chung et al., 1990; Quteish and Dolby, 1992; al-Arrayed et al., 1995; Camargo et al., 2000, 2005; Lekovic et al., 2001; Sculean et al., 2003, 2005, 2007; Tonetti et al., 2004; Vouros et al., 2004; Heitz-Mayfield et al., 2006; Linares et al., 2006; Paolantonio et al., 2008, 2010; Boynuegri et al., 2009; Sowmya et al., 2010; Trombelli et al., 2010; Singh et al., 2012a,b). The mean ages of patients ranged from 41 to 51 yrs, and the average percentage of women, if reported, ranged from
29% to 70%. The number of patients randomized per trial ranged from 10 to 124. Smokers were explicitly included in 5 studies, were excluded in 7 studies and were not reported in 5 of the remaining studies. Six trials explicitly included patients with chronic periodontitis only. Ten trials reported morphology of
standard errornumber of teeth
number of patients.•
Figure 1. Methodological characteristics of included trials. (+) low risk of bias, (?) unclear, and (–) high risk of bias on a specific item.

776 Stoecklin-Wasmer et al. J Dent Res 92(9) 2013
infrabony defects: 1 trial considered three-wall defects only, and in 1 trial most infrabony lesions showed a three-wall configura-tion; in 8 trials, the majority of infrabony lesions represented two-wall defects. Two trials explicitly reported that some infrabony defects displayed the concomitant presence of furca-tion lesions. Initial furcation involvement (degree I) was present in 4 out of 38 defects in the trial by al-Arrayed et al. (1995) and in 4 out of 52 defects in Quteish and Dolby (1992), with equal distribution of furcation-involved defects in both trial arms. Nine trials used a parallel group design, and the remaining trials used a split-mouth design. Eight trials had follow-up durations of 6 mos, 1 trial had a follow-up period of 9 mos, 7 trials had a follow-up period of one yr, and 1 trial reported outcomes up to 60 mos. All studies were conducted in a single-center university setting except for 1 trial, which was multi-centric, conducted at a university and in private practices.
Six trials tested OFD against CM alone, 10 trials tested OFD against CM and bone substitutes, and 1 trial tested OFD against CM with and without bone substitutes. Porcine-derived CM were used in 7 trials, human CM were tested in 4 trials, and 4 trials evaluated non-porcine-derived xenogen CM. Two trials did not declare the origin of membranes used. Thirteen trials used sulcular incisions on the mucoperiosteal flap to access the infrabony defect, 3 applied papilla preservation techniques, and 1 trial did not report on flap design. Appendix Tables 4 and 5 list further clinical trial characteristics.
Fig. 1 and Appendix Table 6 present the methodological characteristics of trials. In none of the trials was the conceal-ment of allocation described in sufficient detail to allow for any
judgment on the potential risk of bias. Only 2 trials stated that randomization envelopes were used, but the trialists did not describe whether these were opaque and consecutively numbered (Tonetti et al., 2004; Vouros et al., 2004). One trial reported blinding of patients, 2 trials reported adequate blinding of surgeons (i.e., revealing treatment code only after the preparation of mucoperiosteal flaps and defect debridement), and 8 out of 17 trials reported blinding of outcome asses-sors. Thirteen trials had analyzed all patients according to the intention-to-treat principle, and 2 trials had sample sizes considered sufficiently large for clinically important treatment effects of 0.8 standard deviation units to be detected. Eight trials addressed all out-comes mentioned in the methods section in either the results or discussion section, but in the remaining 9 trials, selective outcome reporting was found for 1 or more outcomes.
Effects of Interventions
Tooth loss
None of the trials explicitly assessed tooth loss as an outcome. One trial incidentally reported 2 lost teeth, both in the OFD trial arm: 1 was extracted on request by the patient due to lack of improvement in tooth mobility, the other due to an accident (Tonetti et al., 2004).
Gain in clinical attachment level (CAL)
All included trials reported on change in attachment level. The overall analysis (Fig. 2) shows that GTR with bioabsorbable CM had a greater mean CAL gain compared with OFD, as indi-cated by a mean difference of 1.58 mm (95% CI, 1.27 to 1.88). An I2 of 71.9% indicated a high degree of between-trial hetero-geneity (p for heterogeneity < .001; Fig. 2), and an inspection of the funnel plot suggested a lack of non-significant results from small trials in the white area (Appendix Fig. 2). Subgroup analysis of trials reporting on CM alone showed a WMD in gain in CAL of 1.39 mm (95% CI, 0.99 to 1.78), whereas the combi-nation of CM and bone substitutes yielded a WMD of 1.71 mm (95% CI, 1.26 to 2.15) when compared with OFD only. Differences between the two subgroups were not statistically significant (p for interaction, .31).
Fig. 3 shows results from stratified analyses. Estimates varied to some extent, according to types of different charac-teristics, but CIs overlapped considerably between strata, and p values for interaction were all negative. Thirteen trials con-tributed to the analysis of a linear association between the percentage of smokers and gain in CAL, and 11 trials contrib-uted to the analysis on an association between the percentage of three-wall involvement and gain in CAL. We found little
NOTE: Weights are from random effects analysis
Overall (I2 = 71.9%, p < .001)
Author / Year
1.58 (1.27, 1.88)
Favors CM +/- boneFavors control0-3 -2.5 -2 -1.5 -1 -.5 0 .5 1 1.5 2 2.5 3
Mean differencein mm (95% CI)
Paolantonio 2008
Subtotal (I2 = 64.6%, p = .010)
Chung 1990
Paolantonio 2010
Blumenthal 1990al-Arrayed 1995
Quteish 1992
Boynuegri 2009
1.60 (1.19, 2.01)
1.39 (0.99, 1.78)
1.27 (0.61, 1.93)
1.60 (1.17, 2.03)
0.42 (-0.12, 0.96)1.22 (-0.79, 3.23)
1.70 (0.91, 2.49)
1.80 (1.19, 2.41)
GTR with collagen membrane
Lekovic 2001
Tonetti 2004
Sculean 2007
Subtotal (I2 = 75.0%, p < .001)
Trombelli 2010
Camargo 2000Camargo 2005
Sculean 2005
Singh 2012a
Blumenthal 1990
Sowmya 2010
Vouros 2004
2.33 (1.73, 2.92)
0.80 (0.24, 1.36)
2.30 (1.46, 3.14)
1.71 (1.26, 2.15)
0.30 (-1.35, 1.95)
1.51 (1.03, 1.98)2.96 (2.29, 3.63)
2.20 (1.50, 2.90)
1.00 (0.06, 1.94)
1.26 (0.72, 1.80)
1.50 (0.50, 2.50)
1.96 (0.64, 3.28)
GTR with collagen membrane and bone substitute
Weighted mean difference
Gain in clinical attachment level (mm)
Figure 2. Forest plot of weighted mean differences in gain in clinical attachment level expressed in mm in 18 comparisons from 17 trials.

J Dent Res 92(9) 2013 Absorbable Collagen Membranes for Periodontal Regeneration 777
evidence for a linear association between these characteristics and treatment effect (p from meta-regression, .43 and .81, respectively).
Probing pocket depth (PPD) reduction
Sixteen studies reported on changes in probing pocket depths. The analysis (Fig. 4) suggested that GTR with bioabsorbable CM had a greater mean reduction in PPD than did OFD, with a WMD of 1.52 mm (95% CI, 1.18 to 1.86). Subgroup analysis of studies showed that GTR with CM alone reduced PPD 1.66 mm more than did OFD (95% CI, 0.99 to 2.33) on average, while the combination of GTR with bone substitutes reduced PPD by 1.44 mm (95% CI, 1.04 to 1.85, p for interaction, .56).
Gingival recession (Rec)
Twelve studies assessed gingival recession as an outcome. The pooled estimate revealed no statistically significant difference between GTR (with or without the application of bone substi-tutes) and OFD (Fig. 5). The overall WMD was -0.06 (95% CI, -0.18 to 0.06). Treatment effects appeared more pronounced
with GTR and bone substitution than with GTR alone, with a borderline p for interaction of .056.
Clinical and radiographic hard-tissue fill (HTF)
Fig. 6A shows results from meta-analyses of all the 8 studies that contributed outcomes for clinical hard-tissue fill. The results dem-onstrated that GTR improved clinical HTF over OFD, with a WMD of 2.22 mm (95% CI, 1.54 to 2.90). The combination of GTR and bone substitutes was associated with larger treatment effects than with GTR alone (p for interaction, .004). Radiographic hard-tissue fill was assessed in 4 trials, with an overall effect size of 2.35 standard deviation units (95% CI, 1.68 to 3.03). No differ-ences were detected between GTR with CM alone and GTR with CM in combination with bone substitutes, when compared with OFD (p for interaction, .70) (Fig. 6B).
Post-operative complications: wound infection and membrane exposure
Thirteen trials reported that no wound infections had occurred, neither in experimental groups (216 teeth in 192 patients) nor in
62/62
I2
All trials
Type of GTRCollagen membraneCollagen membrane and bone
Flap designPapilla preservationSulcular incisions
Type of membraneCross-linkedNatural form
Protocol-mandatedantibiotics useYesNo
Ascertainment of defectAt deepest defectUsing whole-tooth mean
Type of designParallelSplit-mouth
SettingSingle-center or unclearMulti-center
Blinding of patientsLow ROBHigh or unclear ROB
Blinding of surgeonsLow ROBHigh or unclear ROB
Blinding of outcome assessorsLow ROBHigh or unclear ROB
Intention-to-treatLow ROBHigh or unclear ROB
Selective outcome reportingLow ROBHigh or unclear ROB
Trial sizeModerate to largeSmall
18
711
315
411
135
108
99
171
117
315
810
144
810
216
322/319
106/106216/213
88/88234/231
67/67220/217
239/23683/83
217/214105/105
159/156163/163
260/257
12/12310/307
88/86234/233
144/142178/177
274/27248/47
170/170152/149
90/90232/229
1.58 (1.27, 1.88)
1.39 (0.99, 1.78)1.71 (1.26, 2.15)
1.09 (0.38, 1.81)1.67 (1.34, 2.01)
1.34 (0.87, 1.81)1.79 (1.42, 2.15)
1.60 (1.23, 1.96)1.56 (1.02, 2.10)
1.78 (1.30, 2.26)1.34 (1.01, 1.68)
1.57 (1.23, 1.92)1.59 (1.07, 2.11)
1.63 (1.33, 1.94)0.80 (0.24, 1.36)
0.30 (-1.35, 1.95)1.61 (1.30, 1.91)
1.00 (0.22, 1.77)1.66 (1.34, 1.97)
1.84 (1.41, 2.26)1.40 (1.00, 1.79)
1.60 (1.25, 1.94)1.50 (0.87, 2.12)
1.54 (1.18, 1.90)1.64 (1.12, 2.15)
1.87 (-0.24, 3.98)1.54 (1.27, 1.81)
72%
65%75%
68%72%
0%71%
78%37%
76%58%
55%81%
70%n/a
36%72%
n/a73%
67%69%
77%41%
66%78%
96%59%
.31
.16
.22
.82
.15
.94
.18
.20
.17
.15
.81
.73
.55
-
-
Favors control Favors cm +/- bone
0-3 -2.5 -2 -1.5 -1 -.5 0 .5 1 1.5 2 2.5 3
Characteristic Trials, nSites in the experimental group / control group, n/N
p for interaction
Mean differencein mm (95% CI)
Gain in clinical attachment level (mm)
Figure 3. Results of stratified analyses of the gain in clinical attachment level. Note: n/a = not applicable.

778 Stoecklin-Wasmer et al. J Dent Res 92(9) 2013
control groups (216 teeth in 193 patients). Membrane exposure was reported in 3 trials of CM alone and occurred in a median of 24% of patients (range, 0% to 29%), and in 9 trials of CM with bone substitute, with a median percentage of patients with
membrane exposure of 11% (range, 0% to 43%) (Appendix Fig. 3).
DISCUSSION
The present meta-analysis showed that, in infrabony defects, GTR with bioab-sorbable CM barriers, either alone or in association with bone substitutes, yielded more beneficial effects than OFD for our primary outcome CAL gain. The overall weighted mean differ-ence was 1.58 mm. However, there were no data available for the other primary outcome, “tooth loss”. Analysis of sec-ondary outcomes demonstrated that reduction of PPD was greater in GTR with CM compared with OFD (WMD of 1.52 mm), as was the increase in clinical and radiographic defect fill, which showed WMDs of 2.22 mm and 2.35 mm, respectively. We did not detect differ-ences between experimental and control interventions for gingival recession change. In addition, we stratified the analysis by the use of bone substitutes in the experimental group (trials of GTR with CM alone vs. trials of GTR with CM and bone substitutes). Even though the effects of CM were larger in trials with, as compared with trials without bone substitutes, the non-significant p value for interaction indicated that this difference could be a chance finding. This information may bear clinical rele-vance, since it indicates that GTR with the combination of CM and bone substi-tutes may not additionally improve the outcomes compared with the use of CM alone and is in agreement with findings from previous systematic reviews (Murphy and Gunsolley, 2003). Nonetheless, caution is indicated, since the majority of the defects in our meta-analysis were self-contained (e.g., they displayed a two- to three-wall configura-tion), thus possibly preventing mem-brane collapse and diminishing the need for space-maintaining bone substitutes. Although our meta-regression analysis did not show any association between morphology and treatment outcomes, such an association cannot be ruled out. Previous studies have suggested that non-contained (e.g., displaying one-wall
configuration) infrabony defects may yield better clinical out-comes with the combination of CM and bone substitutes (Paolantonio, 2002; Cortellini and Tonetti, 2005). Regarding adverse healing outcomes, no study observed wound infections
NOTE: Weights are from random effects analysisOverall (I2 = 73.6%, p < .001)
GTR with collagen membrane and bone substitute
Subtotal (I2 = 68.8%, p < .001)Vouros 2004
Sculean 2007
Paolantonio 2010
Blumenthal 1990Camargo 2000
Boynuegri 2009
Lekovic 2001
al-Arrayed 1995
Singh 2012a
Subtotal (I2 = 82.4%, p < .001)
Tonetti 2004
Paolantonio 2008
Trombelli 2010
Quteish 1992
Camargo 2005
Sowmya 2010
Blumenthal 1990
Sculean 2005
GTR with collagen membrane
Author / Year
1.52 (1.18, 1.86)
1.44 (1.04, 1.85)2.58 (1.51, 3.65)
1.50 (0.14, 2.86)
2.30 (1.66, 2.94)
1.22 (0.68, 1.76)1.37 (0.38, 2.36)
1.40 (0.52, 2.28)
1.95 (1.43, 2.48)
1.43 (0.77, 2.09)
1.11 (0.22, 2.00)
1.66 (0.99, 2.33)
0.50 (-0.08, 1.08)
2.40 (1.75, 3.05)
0.00 (-1.60, 1.60)
2.00 (1.12, 2.88)
2.16 (1.66, 2.67)
1.10 (0.46, 1.74)
0.48 (-0.06, 1.02)
1.80 (1.03, 2.57)
--
-
Favors control Favors CM +/- bone0-2 -1.5 -1 -.5 0 .5 1 1.5 2
Weighted mean difference
Probing pocket depth reduction in mm
2.5 3 3.5 4
Mean differencein mm (95% CI)
Figure 4. Forest plot of weighted mean differences in probing pocket depth reduction expressed in mm in 17 comparisons from 16 trials.
NOTE: Weights are from random effects analysis
Overall (I2 = 67.1%, p < .001)
Blumenthal 1990
Sculean 2005
Trombelli 2010
Paolantonio 2010
Subtotal (I2 = 65.0%, p = .002)
Tonetti 2004
Camargo 2005
Subtotal (I2 = 73.1%, p = .024)
Author / Year
Camargo 2000
Sowmya 2010
Blumenthal 1990
Paolantonio 2008
Lekovic 2001
Sculean 2007Singh 2012a
-0.06 (-0.18, 0.06)
-0.28 ( 0.82, 0.26)
-0.30 (-0.96, 0.36)
-0.40 (-1.31, 0.51)
0.60 (-0.03, 1.23)
-0.10 (-0.21, 0.02)
-0.40 (-0.77, 0.03)
0.04 (0.01, 0.08)
0.33 (-0.30, 0.96)
-0.25 (-0.54, 0.05)
0.10 (-0.77, 0.97)
-0.33 (-0.87, 0.21)
0.70 (0.16, 1.24)
-0.07 (-0.13, -0.01)
-0.90 (-1.83, 0.03)0.11 (-0.43, 0.65)
-
- -
-
- -- -
- - -
- -
Favors CM +/- bone Favors control0-1.5 -1 -.5 0 .5 1 1.5
Weighted mean difference
Mean differencein mm (95% CI)
GTR with collagen membrane
GTR with collagen membrane and bone substitute
Gingival recession in mm
Figure 5. Forest plot of weighted mean differences in gingival recession expressed in mm in 13 comparisons from 12 trials.

J Dent Res 92(9) 2013 Absorbable Collagen Membranes for Periodontal Regeneration 779
in the post-surgical phase in either treat-ment groups. In contrast, of the 11 trials that reported on membrane exposure, 7 observed this kind of untoward event. Taken together, these findings indicate that, despite the fact that treatment of infrabony periodontal defects by means of GTR with CM (with or without bone substitutes) resulted in superior clinical outcomes compared with those achieved with OFD alone, we still cannot ascertain whether this regenerative approach may indeed prevent tooth loss.
Factors that have been repeatedly suggested to have a potential influence on wound-healing are membrane expo-sure and subsequent bacterial coloniza-tion (Selvig et al., 1992; Nowzari et al., 1995; Ling et al., 2003). However, in the present study, it was not feasible to ana-lyze the effect of membrane exposure on clinical outcomes, because subgroup outcome data were not available in the trials. However, the present findings are in agreement with those from a previous systematic review (Needleman et al., 2006), which failed to demonstrate an effect of barrier exposure on healing, despite frequently reported exposure.
There are several other limitations. The included trials were generally of poor methodological quality and report-ing. None of the included trials reported on the number of patients screened for inclusion. Most studies failed to report on the time point of communicating treatment allocation to surgeons. Only 3 studies of parallel design reported this. Therefore, we are uncertain about per-formance bias causing an overestimation of treatment effects if surgeons con-sciously or unconsciously performed better at flap preparation and defect debridement in experimental groups than in control groups. We generally found a high degree of heterogeneity, which we were unable to explain. This means that the true magnitude of treatment effects remains unclear. Inspection of the funnel plot suggested a selective lack of non-significant results for small trials with large standard errors. This is likely to have introduced bias due to small study effects, even though the fun-nel plot did not satisfy the conventional criteria for asymmetry.
It is unfortunate that none of the included trials reported on our primary outcome, “tooth loss”. Only 1 of the included trials would have a sufficiently long follow-up of 5 yrs to allow for the clinically meaningful interpretation of effects of different treatments on tooth loss. All other trials were limited to a
follow-up of 6 to 12 mos. When follow-up time is limited in clinical trials, surrogate endpoints, such as clinical attachment loss, are substitutes for true, patient-relevant clinical endpoints, such as tooth loss (Hujoel, 2004). However, unless additional long-term trials ascertain this outcome, it remains difficult in our view to understand whether CM indeed enhance tooth reten-tion. Conversely, the inclusion of 5-year results from the trial by Sculean et al. (2007) could have biased results for the other primary outcome, CAL gain, toward the null, since changes in
NOTE: Weights are from random effects analysis
Overall (I2 = 95.3%, p < .001)
Blumenthal 1990
Subtotal (I2 = 0.0%, p = .471)
Paolantonio 2010
Camargo 2005
Subtotal (I2 = 83.5%, p < .001)
Blumenthal 1990
Camargo 2000
Author / Year
Chung 1990
Sowmya 2010
Lekovic 2001
Paolantonio 2008
2.22 (1.54, 2.90)
1.49 (0.95, 2.03)
1.47 (1.16, 1.79)
0.90 (-0.20, 2.00)
3.42 (3.38, 3.46)
2.99 (2.50, 3.48)
3.37 (3.03, 3.71)
2.60 (1.37, 3.83)
1.16 (0.40, 1.92)
2.10 (1.55, 2.65)
3.06 (1.76, 4.35)
1.70 (1.21, 2.19)
Favors control Favors CM +/- bone0-2 -1.5 -1 -.5 0 1.5 1.5 2
Weighted mean difference
GTR with collagen membrane
GTR with collagen membrane and bone substitute
Hard-tissue fill, clinical (in mm)
Mean differencein mm (95% CI)
3 3.52.5
A
NOTE: Weights are from random effects analysis
Overall (I2 = 48.8%, p = .119)
Boynuegri 2009
Subtotal (I2 = 17.3%, p = .298)
Author / Year
Singh 2012a
Subtotal
Sowmya 2010
Vouros 2004
2.35 (1.68, 3.03)
3.35 (2.11, 4.59)
2.10 (1.54, 2.66)
ES (95% CI)
2.34 (1.29, 3.38)
3.35 (2.11, 4.59)
2.50 (1.62, 3.37)
1.62 (0.84, 2.40)
ES (95% CI)
Favors control Favors CM +/- bone0-2 -1.5 -1 -.5 0 .5 1 1.5 2 2.5 3 3.5 4 4.5
Effect size
GTR with collagen membrane
GTR with collagen membrane and bone substitute
Hard-tissue fill, radiographic in standard deviation units
B
Figure 6. Forest plot of weighted mean differences in hard-tissue fill. Panel A: clinical, expressed in mm in 9 comparisons from 8 trials. Panel B: radiographic, expressed in standard deviation units in 4 trials.

780 Stoecklin-Wasmer et al. J Dent Res 92(9) 2013
CAL beyond 1 yr could be mainly a function of SPT rather than of the allocated interventions. A post hoc sensitivity analysis based on 1-year data from this trial showed much the same results, however (data available on request).
We were unable to satisfactorily address 2 clinically relevant questions: whether defect configuration (Tonetti et al., 1993) and whether smoking (Cortellini and Tonetti, 2004) affect regenera-tive treatment effects. Our preliminary results of aggregate level data do not point toward an association of treatment effects with these characteristics. However, we could have missed associa-tions because of the ecological fallacy (Piantadosi et al., 1988). To address these issues properly, a meta-analysis of individual patient data, infeasible given the resource constraints, would be required to perform proper subgroup analyses in smokers and non-smokers and across different defect configurations.
This is the first systematic review to analyze the outcomes of GTR with CM as compared with OFD, without considering any other types of barrier membranes. Combining trials of different barrier membranes, Needleman et al. (2006) reported a weighted mean difference of 1.22 mm for our primary outcome of CAL gain (95% CI 0.80 to 1.64), favoring GTR procedures with membranes over OFD. Murphy and Gunsolley (2003) reported mean differences in CAL gain in a subgroup of trials with CM compared with OFD to be around 0.95 mm. Our estimate tends to be slightly more beneficial, but confidence intervals from our and previous meta-analyses overlap, which indicates that our results are compatible with those reported in previous publications.
In conclusion, GTR with CM, with or without bone substitutes, may lead to improved clinical outcomes compared with those achieved with OFD alone. Our meta-analysis lends support to this concept in the treatment of infrabony periodontal defects.
ACKNOWLEDGMENTS
This work was funded by the authors’ own institution. The authors declare no conflict of interest with respect to the author-ship and/or publication of this article.
REFERENCESal-Arrayed F, Adam S, Moran J, Dowell P (1995). Clinical trial of cross-
linked human type I collagen as a barrier material in surgical periodon-tal treatment. J Clin Periodontol 22:371-379.
Blumenthal N, Steinberg J (1990). The use of collagen membrane barriers in conjunction with combined demineralized bone-collagen gel implants in human infrabony defects. J Periodontol 61:319-327.
Boynuegri D, Ozcan G, Senel S, Uc D, Uraz A, Ogus E, et al. (2009). Clinical and radiographic evaluations of chitosan gel in periodontal intraosseous defects: a pilot study. J Biomed Mater Res B Appl Biomater 90:461-466.
Bunyaratavej P, Wang HL (2001). Collagen membranes: a review. J Periodontol 72:215-229.
Camargo PM, Lekovic V, Weinlaender M, Nedic M, Vasilic N, Wolinsky LE, et al. (2000). A controlled re-entry study on the effectiveness of bovine porous bone mineral used in combination with a collagen mem-brane of porcine origin in the treatment of intrabony defects in humans. J Clin Periodontol 27:889-896.
Camargo PM, Lekovic V, Weinlaender M, Vasilic N, Madzarevic M, Kenney EB (2005). A reentry study on the use of bovine porous bone mineral, GTR, and platelet-rich plasma in the regenerative treatment of intrabony defects in humans. Int J Periodontics Restorative Dent 25:49-59.
Camelo M, Nevins ML, Schenk RK, Simion M, Rasperini G, Lynch SE, et al. (1998). Clinical, radiographic, and histologic evaluation of human periodontal defects treated with Bio-Oss and Bio-Gide. Int J Periodontics Restorative Dent 18:321-331.
Chung KM, Salkin LM, Stein MD, Freedman AL (1990). Clinical evaluation of a biodegradable collagen membrane in guided tissue regeneration. J Periodontol 61:732-736.
Cohen J (1988). Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum.
Cortellini P, Tonetti MS (2004). Long-term tooth survival following regen-erative treatment of intrabony defects. J Periodontol 75:672-678.
Cortellini P, Tonetti MS (2005). Clinical performance of a regenerative strategy for intrabony defects: scientific evidence and clinical experi-ence. J Periodontol 76:341-350.
Gottlow J, Nyman S, Lindhe J, Karring T, Wennstrom J (1986). New attach-ment formation in the human periodontium by guided tissue regenera-tion. Case reports. J Clin Periodontol 13:604-616.
Heitz-Mayfield L, Tonetti MS, Cortellini P, Lang NP (2006). Microbial colonization patterns predict the outcomes of surgical treatment of intrabony defects. J Clin Periodontol 33:62-68.
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003). Measuring incon-sistency in meta-analyses. BMJ 327:557-560.
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343:d5928.
Hujoel PP (2004). Endpoints in periodontal trials: the need for an evidence-based research approach. Periodontology 2000 36:196-204.
Juni P, Altman DG, Egger M (2001). Systematic reviews in health care: assessing the quality of controlled clinical trials. BMJ 323:42-46.
Lekovic V, Camargo PM, Weinlaender M, Kenney EB, Vasilic N (2001). Combination use of bovine porous bone mineral, enamel matrix pro-teins, and a bioabsorbable membrane in intrabony periodontal defects in humans. J Periodontol 72:583-589.
Linares A, Cortellini P, Lang NP, Suvan J, Tonetti MS (2006). Guided tissue regeneration/deproteinized bovine bone mineral or papilla preservation flaps alone for treatment of intrabony defects. II: Radiographic predic-tors and outcomes. J Clin Periodontol 33:351-358.
Ling LJ, Hung SL, Lee CF, Chen YT, Wu KM (2003). The influence of membrane exposure on the outcomes of guided tissue regeneration: clinical and microbiological aspects. J Periodontal Res 38:57-63.
Murphy KG, Gunsolley JC (2003). Guided tissue regeneration for the treat-ment of periodontal intrabony and furcation defects. A systematic review. Ann Periodontol 8:266-302.
Needleman IG, Worthington HV, Giedrys-Leeper E, Tucker RJ (2006). Guided tissue regeneration for periodontal infra-bony defects. Cochrane Database Syst Rev 2:CD001724.
Nowzari H, Matian F, Slots J (1995). Periodontal pathogens on polytetra-fluoroethylene membrane for guided tissue regeneration inhibit heal-ing. J Clin Periodontol 22:469-474.
Nyman S, Lindhe J, Karring T, Rylander H (1982). New attachment follow-ing surgical treatment of human periodontal disease. J Clin Periodontol 9:290-296.
Paolantonio M (2002). Combined periodontal regenerative technique in human intrabony defects by collagen membranes and anorganic bovine bone. A controlled clinical study. J Periodontol 73:158-166.
Paolantonio M, Perinetti G, Dolci M, Perfetti G, Tete S, Sammartino G, et al. (2008). Surgical treatment of periodontal intrabony defects with calcium sulfate implant and barrier versus collagen barrier or open flap debridement alone: a 12-month randomized controlled clinical trial. J Periodontol 79:1886-1893.
Paolantonio M, Femminella B, Coppolino E, Sammartino G, D’Arcangelo C, Perfetti G, et al. (2010). Autogenous periosteal barrier membranes and bone grafts in the treatment of periodontal intrabony defects of single-rooted teeth: a 12-month reentry randomized controlled clinical trial. J Periodontol 81:1587-1595.
Papapanou PN, Tonetti MS (2000). Diagnosis and epidemiology of peri-odontal osseous lesions. Periodontol 2000 22:8-21.
Parodi R, Carusi G, Santarelli G, Nanni F, Pingitore R, Brunel G (1997). Guided tissue regeneration employing a collagen membrane in a human periodontal bone defect: a histologic evaluation. Int J Periodontics Restorative Dent 17:282-291.

J Dent Res 92(9) 2013 Absorbable Collagen Membranes for Periodontal Regeneration 781
Piantadosi S, Byar DP, Green SB (1988). The ecological fallacy. Am J Epidemiol 127:893-904.
Pihlstrom BL, McHugh RB, Oliphant TH, Ortiz-Campos C (1983). Comparison of surgical and nonsurgical treatment of periodontal dis-ease. A review of current studies and additional results after 61/2 years. J Clin Periodontol 10:524-541.
Quteish D, Dolby AE (1992). The use of irradiated-crosslinked human col-lagen membrane in guided tissue regeneration. J Clin Periodontol 19:476-484.
Reichenbach S, Sterchi R, Scherer M, Trelle S, Burgi E, Burgi U, et al. (2007). Meta-analysis: chondroitin for osteoarthritis of the knee or hip. Ann Intern Med 146:580-590.
Rücker G, Schwarzer G, Carpenter JR, Schumacher M (2008). Undue reli-ance on I(2) in assessing heterogeneity may mislead. BMC Med Res Methodol 8:79.
Rutjes AW, Juni P, da Costa BR, Trelle S, Nuesch E, Reichenbach S (2012). Viscosupplementation for osteoarthritis of the knee: a systematic review and meta-analysis. Ann Intern Med 157:180-191.
Sculean A, Berakdar M, Chiantella GC, Donos N, Arweiler NB, Brecx M (2003). Healing of intrabony defects following treatment with a bovine-derived xenograft and collagen membrane. A controlled clinical study. J Clin Periodontol 30:73-80.
Sculean A, Stavropoulos A, Windisch P, Keglevich T, Karring T, Gera I (2004). Healing of human intrabony defects following regenerative periodontal therapy with a bovine-derived xenograft and guided tissue regeneration. Clin Oral Investig 8:70-74.
Sculean A, Chiantella GC, Windisch P, Arweiler NB, Brecx M, Gera I (2005). Healing of intra-bony defects following treatment with a com-posite bovine-derived xenograft (Bio-Oss Collagen) in combination with a collagen membrane (Bio-Gide PERIO). J Clin Periodontol 32:720-724.
Sculean A, Schwarz F, Chiantella GC, Donos N, Arweiler NB, Brecx M, et al. (2007). Five-year results of a prospective, randomized, controlled study evaluating treatment of intra-bony defects with a natural bone mineral and GTR. J Clin Periodontol 34:72-77.
Selvig KA, Kersten BG, Chamberlain AD, Wikesjö UM, Nilvéus RE (1992). Regenerative surgery of intrabony periodontal defects using ePTFE barrier membranes: scanning electron microscopic evaluation of retrieved membranes versus clinical healing. J Periodontol 63:974-978.
Singh VP, Nayak DG, Uppoor AS, Shah D (2012a). Nano-crystalline hydroxyapatite bone graft combined with bioresorbable collagen
membrane in the treatment of periodontal intrabony defects: a random-ized controlled clinical trial. J Indian Soc Periodontol 16:562-568.
Singh VP, Nayak DG, Uppoor AS, Shah D (2012b). Clinical and radiographic evaluation of nano-crystalline hydroxyapatite bone graft (Sybograf) in combination with bioresorbable collagen membrane (Periocol) in peri-odontal intrabony defects. Dent Res J (Isfahan) 9:60-67.
Sowmya NK, Tarun Kumar AB, Mehta DS (2010). Clinical evaluation of regenerative potential of type I collagen membrane along with xeno-genic bone graft in the treatment of periodontal intrabony defects assessed with surgical re-entry and radiographic linear and densitomet-ric analysis. J Indian Soc Periodontol 14:23-29.
Stahl SS, Froum S, Tarnow D (1990). Human histologic responses to guided tissue regenerative techniques in intrabony lesions. Case reports on 9 sites. J Clin Periodontol 17:191-198.
Sterne JA, Egger M (2001). Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J Clin Epidemiol 54:1046-1055.
Sweeting MJ, Sutton AJ, Lambert PC (2004). What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data. Stat Med 23:1351-1375.
Thompson SG, Sharp SJ (1999). Explaining heterogeneity in meta-analysis: a comparison of methods. Stat Med 18:2693-2708.
Tonetti MS, Pini-Prato G, Cortellini P (1993). Periodontal regeneration of human intrabony defects. IV. Determinants of healing response. J Periodontol 64:934-940.
Tonetti MS, Prato GP, Cortellini P (1996). Factors affecting the healing response of intrabony defects following guided tissue regeneration and access flap surgery. J Clin Periodontol 23:548-556.
Tonetti MS, Cortellini P, Lang NP, Suvan JE, Adriaens P, Dubravec D, et al. (2004). Clinical outcomes following treatment of human intrabony defects with GTR/bone replacement material or access flap alone. A multicenter randomized controlled clinical trial. J Clin Periodontol 31:770-776.
Trombelli L, Simonelli A, Pramstraller M, Wikesjö UM, Farina R (2010). Single flap approach with and without guided tissue regeneration and a hydroxyapatite biomaterial in the management of intraosseous peri-odontal defects. J Periodontol 81:1256-1263.
Vouros I, Aristodimou E, Konstantinidis A (2004). Guided tissue regenera-tion in intrabony periodontal defects following treatment with two bioabsorbable membranes in combination with bovine bone mineral graft. A clinical and radiographic study. J Clin Periodontol 31:908-917.
DS1
C. Stoecklin-Wasmer1†, A.W.S. Rutjes2,3†, B.R. da Costa2,4, G.E. Salvi1, P. Jüni2,4, and A. Sculean1*
1Department of Periodontology, University of Bern, Freiburgstrasse 7, 3010 Bern, Switzerland; 2Institute of Social and Preventive Medicine, University of Bern, Finkenhubelweg 11, 3012 Bern, Switzerland; 3Centre for Aging Sciences (Ce.S.I.), G. d’Annunzio University Foundation, Palazzina SEBI 3° livello, Campus Universitario Chieti Scalo, 66100 Chieti Scalo, Italia; 4CTU Bern, Department of Clinical Research, University of Bern, Finkenhubelweg 11, 3012 Bern, Switzerland; †authors contributed equally as co-first authors; *corresponding author, [email protected]
J Dent Res DOI: 10.1177/0022034513496428
Absorbable Collagen Membranes for Periodontal Regeneration: A Systematic Review
APPENDIX
CLINICAL REVIEW
RCT = randomized,controlled trial; CAL = clinical attachment level tr to legend and add .
2710 records identified through database searching
3 additional records identified through other sources
1588 records after duplicates (1125) removed
1588 records screened
1542 records excluded
46 full-text articles assessed for eligibility
21 records on 17 RCTsincluded in systematic
review
25 full-text articles excluded
Not relevant to the intervention n = 18Not an RCT n = 1Potentially relevant, available in abstract form only n = 6
17 RCTs included in meta-analysis on CAL outcome
Identification
Screening
Eligibility
Included
Appendix Figure 1. Flow diagram. RCT = randomized, controlled trial; CAL = clinical attachment level.

DS2 Stoecklin-Wasmer et al. J Dent Res
NOTE: Weights are from random effects analysis
Overall (I2 = 0.0%, p = .749)
Sculean 2007
Lekovic 2001*
Singh 2012a
Paolantonio 2008
Trombelli 2010*
Blumenthal 1990*
Blumenthal 1990*
Subtotal (I2 = 0.0%, p = .501)
Trial / Year
Subtotal (I2 = 0.0%, p = .751)
GTR with collagen membrane and bone substitute
Sowmya 2010*
GTR with collagen membrane
Sculean 2005
Camargo 2000
Paolantonio 2010
Vouros 2004
3 / 14
0 / 18
1 / 9
4 / 17
No. of teeth / total
0 / 12
0 / 15
0 / 15
0 / 10
4 / 16
6 / 22
4 / 14
6 / 14
0.25 (0.17, 0.33)
0.21 (-0.00, 0.43)
0.11 (-0.12, 0.34)
0.24 (0.03, 0.44)
0.25 (0.15, 0.35)
Incidence (95% CI)
0.26 (0.10, 0.41)
0.25 (0.04, 0.46)
0.27 (0.09, 0.46)
0.29 (0.05, 0.52)
0.43 (0.17, 0.69)
0.25 (0.17, 0.33)
0.21 (-0.00, 0.43)
0.11 (-0.12, 0.34)
0.24 (0.03, 0.44)
0.25 (0.15, 0.35)
0.26 (0.10, 0.41)
0.25 (0.04, 0.46)
0.27 (0.09, 0.46)
0.29 (0.05, 0.52)
0.43 (0.17, 0.69)
Incidence of membrane exposure (%) 0 0 .1 .2 .3 .4 .5 .6 .7 .8 .9 1
Appendix Figure 3. Incidence of membrane exposure. Note: *Comparisons with 0 events in both trial arms did not contribute to the analysis.
0
.2
.4
.6
.8
-3 -2 -1 0 1 2 3Weighted mean difference
Sta
ndar
d er
ror o
f wei
ghte
d m
ean
diffe
renc
e
Gain in clinical attachment level (mm)
Appendix Figure 2. Contour-enhanced funnel plot for effects on the gain of clinical attachment level. Contour areas display areas of sig-nificance at p ≤ .05 (gray) and non-significance (white).

J Dent Res Absorbable Collagen Membranes for Periodontal Regeneration DS3
Appendix Table 1. Search Terms for MEDLINE and EMBASE
MEDLINE* EMBASE*
Search terms related to periodontitis 1. in*ra*bon* defect*.mp.2. in*ra-bon* defect*.mp.3. intra-osseous.mp.4. intraosseous.mp.5. (angular adj1 defect*).mp.6. (vertical adj1 defect*).mp.7. exp periodontitis/8. exp periodontal disease/Search terms related to guided tissue regeneration 9. exp tissue regeneration/10. guided tissue regeneration.mp.11. gtr.mp.12. barrier* membrane*.mp.13. (resorbable adj10 membrane*).mp.14. (bioabsorb$ adj10 membrane*).mp.15. (periodontal adj5 regeneration).mp.16. exp xenograft/17. (collagen adj1 membrane*).mp.18. collagen barrier*.mp.19. xenograft$.mp.20. graft*.ti,ab.21. bon* substitut*.mp.22. exp Bone Substitutes/23. exp Biocompatible Materials/24. biomaterial*.mp.
Search terms related to design 25. randomized controlled trial.pt.26. controlled clinical trial.pt.27. randomized.ab.28. placebo.ab.29. drug therapy.fs.30. randomly.ab.31. trial.ab.32. groups.ab.
Search terms related to periodontitis1. exp periodontitis/ or exp periodontal disease/2. in*ra*bon* defect*.mp.3. in*ra-bon* defect*.mp.4. intra-osseous.mp.5. intraosseous.mp.6. (angular adj1 defect*).mp.7. (vertical adj1 defect*).mp.Search terms related to guided tissue regeneration 8. exp tissue regeneration/ 9. guided tissue regeneration.mp.10. gtr.mp.11. resorbable membrane*.mp.12. (resorbable adj10 membrane*).mp.13. (periodontal adj5 regeneration).mp.14. exp xenograft/15. (collagen adj1 membrane*).mp.16. collagen barrier*.mp.17. xenograft$.mp.18. (bioabsorb$ adj10 membrane*).mp.19. (bioabsorb$ adj10 barrier*).mp.20. barrier membrane*.mp.21. exp bone graft/22. graft$.ti,ab.23. bon* substitut*.mp.24. exp biomaterial/25. biomaterial*.mp.Search terms related to design26. random$.tw.27. factorial$.tw.28. (crossover$ or cross-over$).tw.29. placebo$.tw.30. (doubl$ adj blind$).tw.31. (singl$ adj blind$).tw.32. assign$.tw.33. allocat$.tw.34. volunteer$.tw.35. Crossover Procedure.sh.36. Double-blind Procedure.sh.37. Randomized Controlled Trial.sh.38. Single-blind Procedure.sh.
Combining terms33. or/1-834. or/9-2435. or/27-3436. and/25-26,3737. exp animals/ not humans.sh.38. 36 not 3739. limit 38 to yr=“1982 -Current”
Combining terms39. or/1-740. or/8-2541. or/26-3842. and/26-27,4543. animal/44. animal/ and human/45. 43 not 4446. 42 not 4447. limit 46 to yr=“1982 -Current”
* MEDLINE and EMBASE searched through the OVID platform on January 8, 2013.

DS4 Stoecklin-Wasmer et al. J Dent Res
Appendix Table 2. Search Terms for the Cochrane Databases
Cochranea
Search terms related to periodontitis#1 MeSH descriptor: [Periodontitis] explode all trees#2 MeSH descriptor: [Periodontal Diseases] explode all trees#3 vertical near/1 defect*:ti,ab,kw (Word variations have been searched)#4 angular near/1 defect*:ti,ab,kw (Word variations have been searched)#5 intraosseous:ti,ab,kw (Word variations have been searched)#6 “intra osseous”:ti,ab,kw (Word variations have been searched)#7 in*ra bon* defect*:ti,ab,kw (Word variations have been searched)#8 in*ra*bon* defect*:ti,ab,kw (Word variations have been searched)#9 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8Search terms related to guided tissue regeneration#10 MeSH descriptor: [Guided Tissue Regeneration] explode all trees#11 guided tissue regeneration:ti,ab,kw (Word variations have been searched)#12 gtr:ti,ab,kw (Word variations have been searched)#13 barrier* membrane*:ti,ab,kw (Word variations have been searched)#14 resorbable near/5 membrane*:ti,ab,kw (Word variations have been searched)#15 periodontal near/5 regeneration:ti,ab,kw (Word variations have been searched)#16 bioabsorb* near/5 membrane*:ti,ab,kw (Word variations have been searched)#17 collagen near/1 membrane*:ti,ab,kw (Word variations have been searched)#18 collagen barrier*:ti,ab,kw (Word variations have been searched)#19 “graft”:ti,ab,kw (Word variations have been searched)#20 bon* substitut*:ti,ab,kw (Word variations have been searched)#21 biomaterial*:ti,ab,kw (Word variations have been searched)#22 MeSH descriptor: [Bone Substitutes] explode all trees#23 MeSH descriptor: [Biocompatible Materials] explode all trees#24 MeSH descriptor: [Transplantation, Heterologous] explode all treesCombining terms#25 #10 or #11 or #12 or #13 or #14#26 #15 or #16 or #17 or #18 or #19 or #20 or #21#27 #22 or #23 or #24#28 #25 or #26 or #27#29 #9 and #28
aSearches in all databases embedded in Cochrane, including the Central Register of Controlled Trials, DARE, and Cochrane reviews search, performed on January 9, 2013.

J Dent Res Absorbable Collagen Membranes for Periodontal Regeneration DS5
Appendix Table 3. List of Excluded Reports
Report Reason for Exclusion
Aimetti et al. (2005) Intervention does not fitBatista et al. (1999) Intervention does not fitBratthall et al. (1996) No full text availableCamargo et al. (2001) No full text availableCamargo et al. (2009) Intervention does not fitChristgau et al. (1996) No full text availableChristgau et al. (1997) No full text availableChristgau et al. (2003) Intervention does not fitCortellini et al. (1996a) Study design does not fitCortellini et al. (1996b) Intervention does not fitCortellini et al. (1998) Intervention does not fitJoly et al. (2000) No full text availableJoly et al. (2002) Intervention does not fitKeles et al. (2006) Intervention does not fitKim et al. (1996) Intervention does not fitKuru et al. (2004) Intervention does not fitLekovic et al. (2000) No full text availableLoos et al. (2002) Intervention does not fitProestakis et al. (1992) Intervention does not fitSculean et al. (2001) Intervention does not fitSculean et al. (2004) Intervention does not fitSculean et al. (2008) Intervention does not fitStavropoulos et al. (2003) Intervention does not fitTonetti et al. (1996) Intervention does not fitTonetti et al. (1998) Intervention does not fit
Appendix Table 3. References to Reports Excluded in This Review
Aimetti M, Romano F, Pigella E, Pranzini F, Debernardi C (2005). Treatment of wide, shallow, and predominantly 1-wall intrabony defects with a bioabsorbable membrane: a randomized controlled clinical trial. J Periodontol 76:1354-1361.
Batista EL Jr, Novaes AB Jr, Simonpietri JJ, Batista FC (1999). Use of bovine-derived anorganic bone associated with guided tissue regenera-tion in intrabony defects. Six-month evaluation at re-entry. J Periodontol 70:1000-1007.
Camargo PM, Lekovic V, Weinlaender M, Divnic-Resnik T, Pavlovic M, Kenney EB (2009). A surgical reentry study on the influence of platelet-rich plasma in enhancing the regenerative effects of bovine porous bone mineral and guided tissue regeneration in the treatment of intrabony defects in humans. J Periodontol 80:915-923.
Christgau M, Aslanidis C, Felden A, Hiller KA, Schmitz G, Schmalz G (2003). Influence of interleukin-1 gene polymorphism on periodontal regeneration in intrabony defects. J Periodontal Res 38:20-27.
Cortellini P, Paolo G, Prato P, Tonetti MS (1996a). Long-term stability of clinical attachment following guided tissue regeneration and conven-tional therapy. J Clin Periodontol 23:106-111.
Cortellini P, Pini Prato G, Tonetti MS (1996b). Periodontal regeneration of human intrabony defects with bioresorbable membranes. A controlled clinical trial. J Periodontol 67:217-223.
Cortellini P, Carnevale G, Sanz M, Tonetti MS (1998). Treatment of deep and shallow intrabony defects. A multicenter randomized controlled clinical trial. J Clin Periodontol 25:981-987.
Joly JC, Palioto DB, de Lima AF, Mota LF, Caffesse R (2002). Clinical and radiographic evaluation of periodontal intrabony defects treated with guided tissue regeneration. A pilot study. J Periodontol 73:353-359.
Keles GC, Cetinkaya BO, Isildak I, Koprulu H, Acikgoz G (2006). Levels of platelet activating factor in gingival crevice fluid following peri-odontal surgical therapy. J Periodontal Res 41:513-518.
Kim CK, Choi EJ, Cho KS, Chai JK, Wikesjo UM (1996). Periodontal repair in intrabony defects treated with a calcium carbonate implant and guided tissue regeneration. J Periodontol 67:1301-1306.
Kuru L, Griffiths GS, Petrie A, Olsen I (2004). Changes in transforming growth factor-beta1 in gingival crevicular fluid following periodontal surgery. J Clin Periodontol 31:527-533.
Loos BG, Louwerse PH, Van Winkelhoff AJ, Burger W, Gilijamse M, Hart AA, et al. (2002). Use of barrier membranes and systemic antibiotics in the treatment of intraosseous defects. J Clin Periodontol 29:910-921.
Proestakis G, Bratthall G, Söderholm G, Kullendorff B, Grondahl K, Rohlin M, et al. (1992). Guided tissue regeneration in the treatment of infrabony defects on maxillary premolars. A pilot study. J Clin Periodontol 19:766-773.
Sculean A, Windisch P, Chiantella GC, Donos N, Brecx M, Reich E (2001). Treatment of intrabony defects with enamel matrix proteins and guided tissue regeneration. A prospective controlled clinical study. J Clin Periodontol 28:397-403.
Sculean A, Donos N, Schwarz F, Becker J, Brecx M, Arweiler NB (2004). Five-year results following treatment of intrabony defects with enamel matrix proteins and guided tissue regeneration. J Clin Periodontol 31:545-549.
Sculean A, Kiss A, Miliauskaite A, Schwarz F, Arweiler NB, Hannig M (2008). Ten-year results following treatment of intra-bony defects with enamel matrix proteins and guided tissue regeneration. J Clin Periodontol 35:817-824.
Stavropoulos A, Karring ES, Kostopoulos L, Karring T (2003). Deproteinized bovine bone and gentamicin as an adjunct to GTR in the treatment of intrabony defects: a randomized controlled clinical study. J Clin Periodontol 30:486-495.
Tonetti MS, Prato GP, Cortellini P (1996). Factors affecting the healing response of intrabony defects following guided tissue regeneration and access flap surgery. J Clin Periodontol 23:548-556.
Tonetti MS, Cortellini P, Suvan JE, Adriaens P, Baldi C, Dubravec D, et al. (1998). Generalizability of the added benefits of guided tissue regen-eration in the treatment of deep intrabony defects. Evaluation in a multi-center randomized controlled clinical trial. J Periodontol 69:1183-1192.

DS6
App
endi
x Ta
ble
4. T
rial D
escr
iptio
ns
Tria
lD
esig
n
No.
of
Tria
l A
rms
No.
of
Stud
y C
ente
rsN
o. o
f Pat
ient
s Ra
ndom
ized
No.
of
Teet
h In
volv
edFo
llow
-up
Dur
atio
nFr
actio
n of
Fe
mal
es (%
)M
ean
Age
(y
rs)
Frac
tion
of
Smok
ers
(%)
Type
of
Perio
dont
itis
32
1C
ombi
natio
nO
utco
mes
Incl
uded
al-A
rray
ed e
t al
., 19
95sp
lit-m
outh
21
14nr
67/
14 (5
0%)
44nr
Oth
er18
/38
16/3
84/
38n/
aC
AL;
PPD
Blum
enth
al a
nd
Stei
nber
g,
1990
split
-mou
th5
110
7112
4/10
(40%
)nr
nrO
ther
19/7
125
/71
3/71
24/7
1C
AL;
PPD
; REC
; HTF
clin
; M
embr
ane
exp;
In
fect
ion
Boyn
uegr
i et a
l.,
2009
para
llel
41
20nr
69/
20 (4
5%)
nr0/
20 (0
%)
Chr
onic
nrnr
nrnr
CA
L; P
PD; H
TF R
x
Cam
argo
et a
l.,
2000
split
-mou
th2
nr22
446
nr43
14/2
2 (6
4%)
nr11
/44
33/4
40/
44n/
aC
AL;
PPD
; REC
; HTF
clin
; M
embr
ane
exp;
In
fect
ion
Cam
argo
et a
l.,
2005
split
-mou
th2
128
566
12/2
8 (4
3%)
4112
/28
(43%
)O
ther
21/5
635
/56
0/56
n/a
CA
L; P
PD; R
EC; H
TF c
lin
; Inf
ectio
nC
hung
et a
l.,
1990
split
-mou
th2
115
3012
8/15
(53%
)nr
nrnr
nrnr
nrnr
CA
L; P
PD; H
TF c
lin
Leko
vic
et a
l.,
2001
split
-mou
th2
118
366
8/18
(44%
)42
12/1
8 (6
7%)
Oth
er11
/36
25/3
60/
36n/
aC
AL;
PPD
; REC
; HTF
clin
; M
embr
ane
exp;
In
fect
ion
Paol
anto
nio
et
al.,
20
08pa
ralle
l3
151
5112
29/5
1 (5
7%)
460/
51 (0
%)
Chr
onic
nrnr
nrnr
CA
L; P
PD; R
EC; H
TF c
lin;
Mem
bran
e ex
p;
Infe
ctio
nPa
olan
toni
o
et a
l.,
2010
para
llel
31
4242
1222
/42
(52%
)48
0/42
(0%
)C
hron
icnr
nrnr
nrC
AL;
PPD
; REC
; HTF
clin
; M
embr
ane
exp;
In
fect
ion
Qut
eish
and
D
olby
, 199
2sp
lit-m
outh
21
1952
6nr
nrnr
Oth
ernr
nrnr
nrC
AL;
PPD
; Inf
ectio
n
Scul
ean
et a
l.,
2005
para
llel
21
3232
1217
/32
(53%
)nr
0/32
(0%
)nr
5/32
18/3
29/
32n/
aC
AL;
PPD
; REC
; HTF
clin
; M
embr
ane
exp;
In
fect
ion
Scul
ean
et a
l.,
2007
para
llel
21
2828
6015
/28
(54%
)nr
5/28
(18%
)C
hron
ic4/
2815
/28
9/28
n/a
CA
L; P
PD; R
EC; H
TF c
lin;
Mem
bran
e ex
p;
Infe
ctio
nSi
ngh
et a
l.,
2012
apa
ralle
l2
116
206
7/16
(44%
)nr
0/16
(0%
)nr
0/18
12/1
80/
186/
18C
AL;
PPD
; REC
; HTF
Rx;
M
embr
ane
exp;
In
fect
ion
Sow
mya
et a
l.,
2010
split
-mou
th2
110
209
7/10
(70%
)46
0/10
(0%
)nr
20/2
00/
200/
200/
20C
AL;
PPD
; REC
; HTF
clin
; H
TF R
x; M
embr
ane
exp;
Infe
ctio
nTo
netti
et a
l.,
2004
para
llel
210
124
124
12nr
/124
(62%
)50
nrC
hron
icnr
nrnr
n/a
CA
L; P
PD; R
EC; H
TF c
lin
Trom
belli
et a
l.,
2010
para
llel
21
2424
67/
24 (2
9%)
512/
24 (8
%)
nr6/
2411
/24
7/24
n/a
CA
L; P
PD; R
EC;
Mem
bran
e ex
p;
Infe
ctio
nVo
uros
et a
l.,
2004
para
llel
31
3440
1223
/34
(68)
nr0/
34 (0
%)
Chr
onic
nrnr
nrn/
aC
AL;
PPD
; HTF
clin
; HTF
Rx
; Mem
bran
e ex
p
nr =
not
rep
orte
d; n
/a =
not
app
licab
le;
CA
L =
clin
ical
atta
chm
ent l
evel
; PP
D =
pro
bing
poc
ket d
epth
; RE
C =
gin
giva
l rec
essi
on;
HTF
clin
= h
ard-
tissu
e fil
l, cl
inic
al;
HTF
Rx
= ha
rd-ti
ssue
fill,
ra
diog
raph
ic; M
embr
ane
exp
= m
embr
ane
expo
sure
Mor
phol
ogy
(wal
ls)

DS7
App
endi
x Ta
ble
5. D
escr
iptio
n of
Tria
l Arm
s an
d In
terv
entio
ns
Tria
lIn
clud
ed T
rial A
rms
Flap
Des
ign
Col
lage
n M
embr
ane
(CM
)Bo
ne G
raft
Cro
ss-li
nked
M
embr
ane
Prot
ocol
-m
anda
ted
Ant
ibio
tic U
se
Post-
surg
ical
C
are
Prov
ided
Supp
ortiv
e Pe
riodo
ntal
Th
erap
y Pr
ovid
edA
scer
tain
men
t of D
efec
t
al-A
rray
ed e
t al.,
19
95O
FD v
s. G
TR C
MSu
lcul
ar
inci
sion
sFr
eeze
-drie
d cr
oss-l
inke
d hu
man
type
I C
Mn/
aye
sno
yes
yes
Unc
lear
if m
easu
rem
ents
of th
e 6
site
s w
ere
aver
aged
, or
if th
e de
epes
t def
ect w
as u
sed
Blum
enth
al a
nd
Stei
nber
g,
1990
OFD
vs.
GTR
CM
vs
. GTR
CM
+
bone
Sulc
ular
in
cisi
ons
CM
(sou
rce
/ br
and
not
repo
rted)
auto
lyze
d an
tigen
-ext
ract
ed
allo
gene
ic fr
eeze
-drie
d bo
ne
- col
lage
n ge
l im
plan
t
nrye
sye
sye
s≥
1 to
oth
per
quad
rant
per
pat
ient
was
in
clud
ed in
the
anal
yses
for
each
trea
tmen
t m
odal
ity; r
esul
ts w
ere
aver
aged
Boyn
uegr
i et a
l.,
2009
OFD
vs.
GTR
CM
Sulc
ular
in
cisi
ons
CM
(sou
rce
/ br
and
not
repo
rted)
soa
ked
in
chito
san
gel 1
%
n/a
nrye
snr
nrN
o re
port
on n
umbe
r of
teet
h in
clud
ed p
er
patie
nt, o
r if
mea
sure
men
ts w
ere
aver
aged
, or
if o
nly
the
deep
est d
efec
ts at
bas
elin
e w
ere
cons
ider
edC
amar
go e
t al.,
20
00O
FD v
s. G
TR
CM
+ b
one
Sulc
ular
in
cisi
ons
Porc
ine
CM
(Bio
-Gid
e)C
ance
llous
bov
ine
poro
us
bone
min
eral
(BPB
M)
gran
ules
(0.2
5-1.
0 m
m) (
Bio-
Oss
)
noye
sye
sye
sA
dequ
ate
Cam
argo
et a
l.,
2005
OFD
vs.
GTR
C
M +
bon
eSu
lcul
ar
inci
sion
sPo
rcin
e C
M (B
io-G
ide)
Can
cello
us B
PBM
gra
nule
s (0
.25-
1.00
mm
) (Bi
o-O
ss)
and
coag
ulat
ed p
late
let-r
ich
plas
ma
noye
sye
sye
sA
dequ
ate
Chu
ng e
t al.,
1990
OFD
vs.
GTR
CM
Sulc
ular
in
cisi
ons
Bovi
ne c
ross
-link
ed C
M (P
erio
-Ba
rrie
r)n/
aye
sno
yes
yes
Out
com
es w
ere
mea
sure
d at
6 p
robi
ng s
ites
per
toot
h; w
hole
-toot
h m
eans
wer
e us
ed fo
r an
alys
isLe
kovi
c et
al.,
20
01O
FD v
s. G
TR
CM
+ b
one
Sulc
ular
in
cisi
ons
Bovi
ne c
olla
gen/
PLA
m
embr
ane
(Bio
-Gid
e C
ompo
site
)
BPBM
gra
nule
s (B
io-O
ss) a
nd
enam
el m
atrix
pro
tein
s (E
mdo
gain
)
noye
sye
sye
sA
dequ
ate
Paol
anto
nio
et
al.,
20
08O
FD v
s. G
TR C
MSu
lcul
ar
inci
sion
sLy
ophi
lized
hum
an
peric
ardi
um C
M (T
utop
last
Peric
ardi
um)
n/a
noye
sye
sye
sU
ncle
ar if
mea
sure
men
ts of
the
6 si
tes
wer
e av
erag
ed, o
r if
the
deep
est d
efec
t was
use
d
Paol
anto
nio
et
al.,
20
10O
FD v
s. G
TR C
MPa
pilla
pr
eser
vatio
nLy
ophi
lized
hum
an
peric
ardi
um C
M (T
utop
last
Peric
ardi
um)
n/a
noye
sye
sye
sU
ncle
ar if
mea
sure
men
ts of
the
6 si
tes
wer
e av
erag
ed, o
r if
the
deep
est d
efec
t was
use
d
Qut
eish
and
D
olby
, 199
2O
FD v
s. G
TR C
MSu
lcul
ar
inci
sion
sIrr
adia
ted,
glu
tara
ldeh
yde-
cros
slink
ed h
uman
pla
cent
a C
M (t
ype
I)
n/a
yes
nonr
nrA
dequ
ate
Scul
ean
et a
l.,
2005
OFD
vs.
GTR
C
M +
bon
eSu
lcul
ar
inci
sion
sPo
rcin
e C
M (B
io-G
ide
Perio
)Bo
vine
-der
ived
xen
ogra
ft (B
io-
Oss
Col
lage
n)no
noye
sye
sA
dequ
ate
Scul
ean
et a
l.,
2007
OFD
vs.
GTR
C
M +
bon
eSu
lcul
ar
inci
sion
sPo
rcin
e C
M (B
ioG
ide
Perio
)BP
BM g
ranu
les
(0.2
5-1.
0 m
m)
(Bio
-Oss
)no
yes
yes
yes
Ade
quat
e
Sing
h et
al.,
2012
aO
FD v
s. G
TR
CM
+ b
one
nrFi
sh C
M (P
erio
Col
)N
ano-
crys
talli
ne
Hyd
roxy
apat
ite (H
A) b
one
repl
acem
ent g
raft
(Syb
ogra
f)
noye
sye
sye
sA
dequ
ate
Sow
mya
et a
l.,
2010
OFD
vs.
GTR
C
M +
bon
eSu
lcul
ar
inci
sion
sXe
noge
n C
M (H
ealig
uide
)Xe
noge
n D
MBM
type
I co
llage
n (O
sseo
graf
t)no
yes
nono
Unc
lear
if m
easu
rem
ents
of th
e 6
site
s w
ere
aver
aged
, or
if th
e de
epes
t def
ect w
as u
sed
Tone
tti e
t al.,
2004
OFD
vs.
GTR
C
M +
bon
ePa
pilla
pr
eser
vatio
nPo
rcin
e C
M (B
io-G
ide)
.BP
BM g
ranu
les
(Bio
-Oss
)no
yes
yes
yes
Ade
quat
e
Trom
belli
et a
l.,
2010
OFD
vs.
GTR
C
M +
bon
ePa
pilla
pr
eser
vatio
nEq
uine
cro
ss-li
nked
CM
(P
arog
uide
)H
A-b
ased
bio
mat
eria
l (Bi
ostit
e)ye
sno
yes
yes
Ade
quat
e
Vour
os e
t al.,
2004
OFD
vs.
GTR
C
M +
bon
eSu
lcul
ar
inci
sion
sPo
rcin
e C
M (B
ioG
ide)
BPBM
gra
nule
s (B
io-O
ss
spon
gios
a)no
yes
yes
yes
Ade
quat
e
OFD
= o
pen
flap
debr
idem
ent;
GTR
= g
uide
d tis
sue
rege
nera
tion;
CM
= c
olla
gen
mem
bran
e; b
one
= bo
ne s
ubsti
tute
; nr
= no
t rep
orte
d; n
/a =
not
app
licab
le.

DS8
App
endi
x Ta
ble
6. M
etho
dolo
gica
l Cha
ract
eris
tics
of T
rials
Aut
hor/
Ye
ar
Gen
erat
ion
of
Allo
catio
n Se
quen
ceD
escr
iptio
n of
Allo
catio
n G
ener
atio
n
Con
ceal
men
t of
Allo
catio
n M
etho
dD
escr
iptio
n of
Con
ceal
men
tBl
indi
ng o
f the
Sur
geon
Blin
ding
of O
utco
me
Ass
esso
rs
Con
trol G
roup
ITT:
nu
mbe
rs a
naly
zed
/ nu
mbe
rs
rand
omiz
ed
Expe
rimen
tal
Gro
up IT
T:
num
bers
ana
lyze
d /
num
bers
ra
ndom
ized
al-A
rray
ed
et a
l.,
1995
uncl
ear
Allo
catio
n of
mat
ched
bila
tera
l les
ions
w
as “
deci
ded
by r
ando
m d
esig
n an
d w
hen
appr
opria
te”.
Ran
dom
izat
ion
met
hod
not r
epor
ted.
uncl
ear
nrTh
e su
rgeo
n w
as b
linde
d un
til a
fter
debr
idem
ent a
t th
e fir
st de
fect
. At t
he
seco
nd d
efec
t, th
e su
rgeo
n w
as n
ot b
linde
d (s
plit-
mou
th d
esig
n).
Ass
esso
r w
as n
ot th
e su
rgeo
n an
d w
as b
lind
to th
e si
tes.
19 /
nr
anal
yzed
19 /
nr
anal
yzed
Blum
enth
al
and
Stei
nber
g,
1990
uncl
ear
Rand
omiz
atio
n se
emed
per
qu
adra
nt,
allo
catin
g ea
ch o
f the
4 q
uadr
ants
to
1 of
the
4 ex
perim
enta
l gro
ups.
A
lloca
tion
of th
e co
ntro
l tee
th
rem
aine
d un
clea
r.
uncl
ear
nrnr
nr15
/15
ana
lyze
dC
M: 1
5 /
15
anal
yzed
; CM
+
bone
: 15
/ 15
ana
lyze
d
Boyn
uegr
i et
al.,
200
9un
clea
rN
ot m
entio
ned
if a
rand
omiz
atio
n m
etho
d w
as u
sed.
uncl
ear
nrnr
nr5
/ 5
anal
yzed
5 /
5 an
alyz
ed
Cam
argo
et
al.,
200
0co
in-to
ssin
gTw
o in
terp
roxi
mal
site
s w
ere
rand
omly
as
sign
ed to
the
expe
rimen
tal o
r co
ntro
l gro
ups.
uncl
ear
nrnr
Ass
esso
rs w
ere
not t
he s
urge
ons
and
wer
e bl
ind
to th
e si
tes.
22 /
22
anal
yzed
22 /
22
anal
yzed
Cam
argo
et
al.,
20
05
coin
-toss
ing
Two
inte
rpro
xim
al s
ites
wer
e ra
ndom
ly
assi
gned
to th
e ex
perim
enta
l or
cont
rol g
roup
s.
uncl
ear
nrnr
Ass
esso
r w
as n
ot th
e su
rgeo
n an
d w
as b
lind
to th
e si
tes.
28 /
28
anal
yzed
28 /
28
anal
yzed
Chu
ng e
t al.,
19
90un
clea
rEx
perim
enta
l site
s w
ere
rand
omly
se
lect
ed fo
r te
st tre
atm
ent;
mat
chin
g co
ntra
late
ral s
ite s
erve
d as
a c
ontro
l w
ithin
the
sam
e pa
tient
.
uncl
ear
nrnr
nr10
/ 1
5 an
alyz
ed10
/ 1
5 an
alyz
ed
Leko
vic
et a
l.,
2001
coin
-toss
ing
Two
inte
rpro
xim
al s
ites
wer
e ra
ndom
ly
assi
gned
to th
e ex
perim
enta
l or
cont
rol g
roup
s.
uncl
ear
nrnr
Ass
esso
r w
as n
ot th
e su
rgeo
n an
d w
as b
lind
to th
e si
tes.
18 /
18
anal
yzed
18 /
18
anal
yzed
Paol
anto
nio
et
al.,
20
08
com
pute
r-ge
nera
ted
“com
pute
r-gen
erat
ed ta
ble”
uncl
ear
nrnr
Ass
esso
r w
as b
lind
to th
e si
tes.
17 /
17
anal
yzed
17 /
17
anal
yzed
Paol
anto
nio
et
al.,
20
10
com
pute
r-ge
nera
ted
“com
pute
r-gen
erat
ed ta
ble”
uncl
ear
nrnr
Ass
esso
r w
as b
lind
to th
e si
tes.
14 /
14
anal
yzed
14 /
14
anal
yzed
Qut
eish
and
D
olby
, 19
92
uncl
ear
Rand
omiz
atio
n m
etho
d no
t rep
orte
d.un
clea
rnr
nrnr
26 /
26
anal
yzed
26 /
26
anal
yzed
Scul
ean
et a
l.,
2005
uncl
ear
Def
ects
wer
e ra
ndom
ly a
ssig
ned
befo
re
surg
ery
to th
e tw
o tre
atm
ent g
roup
s w
ith th
e ra
ndom
ized
blo
ck a
ppro
ach.
uncl
ear
nrnr
Ass
esso
r w
as n
ot a
war
e of
su
rgic
al p
roce
dure
to b
e pe
rform
ed (b
linde
d at
ba
selin
e). U
ncle
ar b
lindi
ng a
t fo
llow
-up
asse
ssm
ent.
16 /
16
anal
yzed
16 /
16
anal
yzed
Scul
ean
et a
l.,
2007
uncl
ear
Def
ects
wer
e ra
ndom
ly a
ssig
ned
befo
re
surg
ery
to th
e tw
o tre
atm
ent g
roup
s w
ith th
e ra
ndom
ized
blo
ck a
ppro
ach.
uncl
ear
nrnr
Ass
esso
r w
as n
ot th
e su
rgeo
n.
Blin
ding
unc
lear
.9
/ 14
ana
lyze
d10
/ 1
4 an
alyz
ed
Sing
h et
al.,
20
12a
coin
-toss
ing
“coi
n fli
p” m
etho
dun
clea
rnr
nr
nr9
/ 10
ana
lyze
d9
/ 10
ana
lyze
d
Sow
mya
et
al.,
201
0un
clea
rRa
ndom
izat
ion
met
hod
not r
epor
ted.
“T
he s
ites
wer
e di
vide
d ra
ndom
ly.”
uncl
ear
nrnr
nr10
/ 1
0 an
alyz
ed10
/ 1
0 an
alyz
ed
Tone
tti e
t al.,
20
04co
mpu
ter-
gene
rate
dA
ssig
nmen
t was
per
form
ed b
y a
cent
ral
study
reg
istra
r us
ing
a cu
stom
-mad
e pr
ogra
m b
ased
on
bala
nced
ran
dom
pe
rmut
ed b
lock
s
enve
lope
sU
se o
f a c
entra
l reg
istra
r an
d se
aled
env
elop
es, n
ot
repo
rted
if la
tter
wer
e op
aque
or
cons
ecut
ivel
y nu
mbe
red.
The
surg
eon
was
blin
ded
until
afte
r de
brid
emen
tA
sses
sor
and
surg
eon
wer
e id
entic
al. N
o bl
indi
ng.
59 /
62
anal
yzed
61 /
62
anal
yzed
Trom
belli
et
al.,
201
0co
mpu
ter-
gene
rate
d“c
ompu
ter-g
ener
ated
ran
dom
izat
ion
list”
uncl
ear
nrTh
e su
rgeo
n w
as b
linde
d un
til a
fter
debr
idem
ent.
Ass
esso
r w
as b
lind
to th
e si
tes.
12 /
12
anal
yzed
12 /
12
anal
yzed
Vour
os e
t al.,
20
04co
mpu
ter-
gene
rate
dC
ompu
ter
rand
omiz
atio
n pr
ogra
m.
Rand
omiz
atio
n se
ems
to b
e at
the
toot
h le
vel.
enve
lope
sSe
aled
env
elop
es, n
ot
repo
rted
if th
ese
wer
e op
aque
or
cons
ecut
ivel
y nu
mbe
red.
The
surg
eon
was
blin
ded
until
afte
r de
brid
emen
tA
sses
sor
was
not
the
surg
eon
and
was
blin
d to
the
site
s.12
/ 1
2 an
alyz
ed14
/ 1
4 an
alyz
ed
ITT
= in
tent
ion-
to-tr
eat;
nr =
not
rep
orte
d.