journal club: percutaneous coronary intervention versus coronary-artery bypass grafting for severe...
TRANSCRIPT
Journal Club:Percutaneous Coronary Intervention
versus Coronary-Artery Bypass Grafting for Severe Coronary Artery
Disease
Tiffany Sun, MDMay 19, 2009

Background
• Cardiovascular disease remains the #1 cause of death in the US.
• 650,000 + deaths due to cardiovascular disease in 2007 (CDC).

Coronary-Artery Bypass Grafting (CABG)
• Introduced in 1968• 253,000 CABG surgeries were
performed in the United States in 2006 .
• Overall 3-4% mortality rate• 5-10% incidence of perioperative MI• 1-2% incidence of CVA• 5% of patients require re-
exploration 24 hrs after surgery for bleeding
• Best performed in patients with multiple blockages in multiple locations, or when blockages are located in certain arterial segments which are not well-suited for PCI.
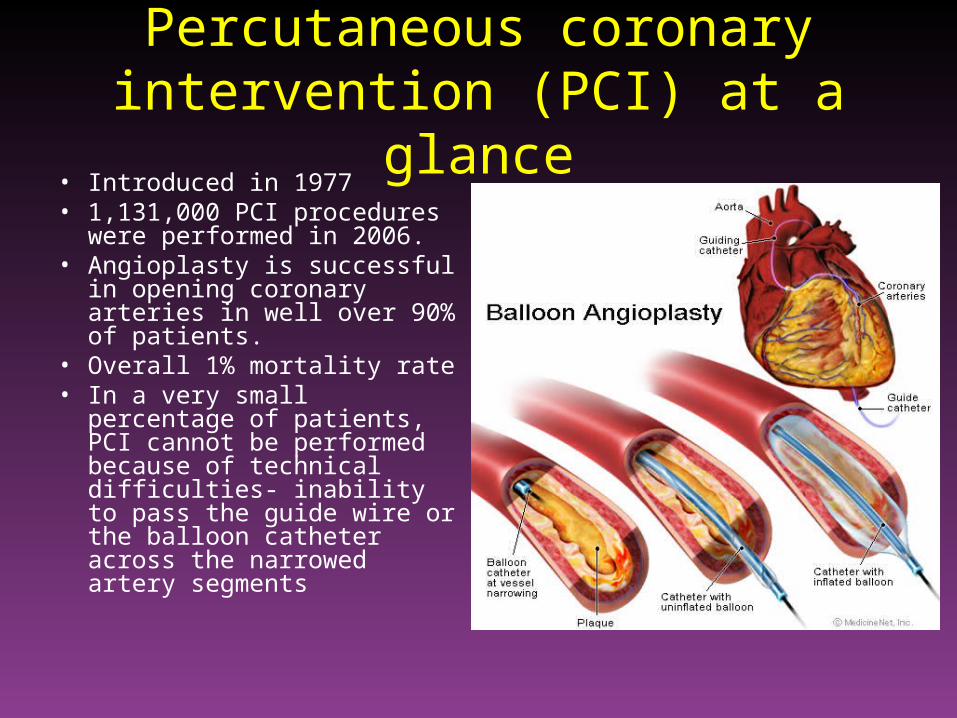
Percutaneous coronary intervention (PCI) at a glance
• Introduced in 1977• 1,131,000 PCI procedures
were performed in 2006.• Angioplasty is successful in
opening coronary arteries in well over 90% of patients.
• Overall 1% mortality rate• In a very small percentage of
patients, PCI cannot be performed because of technical difficulties- inability to pass the guide wire or the balloon catheter across the narrowed artery segments

Study Background
• Several trials comparing PCI involving bare-metal stents with CABG in patients with multivessel disease showed similar survival rates but higher revascularization rates among patients with bare-metal stents at 5 years.
• However, studies comparing PCI involving drug-eluting stents with CABG have generally been smaller and nonrandomized with inconsistent results.

Methods• Prospective, clinical trial conducted in 85 sites in 17
countries in Europe and the US.• Eligible patients were those with previously untreated
three-vessel disease and those with left main coronary artery disease (alone or with co-existing one-, two-, or three-vessel disease)
• A local interventional cardiologist and cardiac surgeon evaluated eligible patients to determine if equivalent anatomical revascularization could be achieved with either CABG or PCI.
• Patients for whom only one treatment option was suitable were entered into parallel, nested registries.

Randomization

Revascularization and Pharmacologic Treatment
• Intent was to achieve complete revascularization of all vessels at least 1.5 mm in diameter with stenosis of 50% or more
• Each patient was assigned a SYNTAX score, which reflects a comprehensive anatomical assessment, with higher scores indicating more complex coronary artery disease.
• Surgical techniques for CABG, the approaches for stent implantation, and the postprocedural medication regimen were “chosen according to local clinical practice.”

Statistical Analysis• Primary analysis- noninferiority comparison of
the two treatments for the primary end point• Primary endpoint- composite of major adverse
cardiac and cerebrovascular events (i.e., death from any cause, stroke, myocardial infarction, or repeat revascularization) throughout the 12-month period after randomization
• If the one-sided 95% upper confidence limit for the difference was less than the prespecified delta value of 6.6%, PCI would be considered noninferior to CABG (based on historical data).

What is a Noninferiority Trial?• Randomized clinical trial in which a new test
treatment is compared with a standard active treatment rather than a placebo/control group.
• Intended to show that the effect of a new treatment is not worse than that of an active control by more than a specified margin.
• Inherent weaknesses include no internal demonstration of assay sensitivity, no single conservative analysis approach, lack of protection from bias by blinding, and difficulty in specifying the noninferiority margin.

Baseline Characteristics of the Patients
Characteristic PCI (N=903) CABG (N=897) P Value
BP ≥ 130/85 mmHg (%) 68.9 64 0.03
Triglycerides ≥ 150 mg/dl (%) 32.3 38.7 0.007
HDL cholesterol <40 mg/dl for men or <50 mg/dl for women (%)
46.2 52.5 0.01
SYNTAX score 28.4 ± 11.5 29.1 ± 11.4 0.19
Time to procedure (days) 6.9 ± 13.0 17.4 ± 28.0 <0.001
Procedure duration (hr) 1.7 ± 0.9 3.4 ± 1.1 <0.001
Postprocedural hospital stay (days)
3.4 + 4.5 9.5 ± 8.0 <0.001
Complete revascularization (%) 56.7 63.2 0.005Plus-minus values are means ± SD.SYNTAX score reflects a comprehensive anatomical assessment, with scores ranging from 0 to 83 and higher scores indicating more complex coronary disease

Treatment
• On average, 4.4 lesions treated in CABG group and 4.3 lesions in PCI group.
• In the CABG group, off-pump surgery was performed in 15% of patients and 97.3% of patients received one or more arterial grafts.
• In the PCI group, 14.1% of patients underwent staged procedures, 63.1% had at least one bifurcation or trifurcation treated, and 33% of patients had placement of stents with total length >100 mm.


Rates of Outcomes among the Study Patients
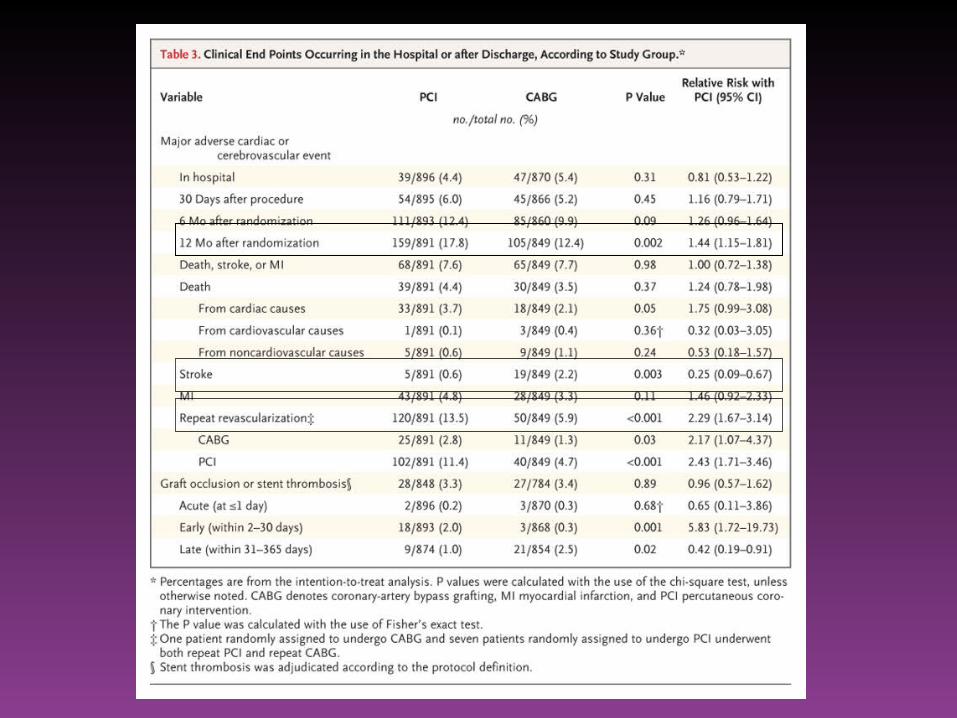

• Patients with low or intermediate SYNTAX scores in both groups had similar rates of major adverse cardiac or cerebrovascular events whereas patients with high scores had a significantly higher event rate in the PCI group.

Conclusion
• For the primary composite end point (death from any cause, stroke, MI, or repeat revascularization throughout the 12 month follow up period), the noninferiority of PCI as compared with CABG was not demonstrated. Thus, CABG proved to be superior.

Strengths
1. Prospective, randomized, multi-center trial2. Large sample size, high enrollment rate (71%)3. Intention-to-treat analysis4. Congruence between cardiac surgeon and
interventional cardiologist on which procedure should be offered to each patient.
5. Newest technology used- arterial grafts (>90%), drug-eluting stents

Weaknesses
1. Short follow-up period (12 months)2. Postprocedure medication regimens were chosen
“according to local clinical practice.” Patients in the CABG group were less likely to receive optimal medical therapy (i.e., aspirin, statins, ACEIs).
3. Increased risk of stroke in CABG group- related to the procedure or due to differences between the two groups in the occurrence of atrial fibrillation and/or discrepancy between use of antiplatelet agents?
4. 78% of participants were men- are these results applicable to women?

Take-home Points• CABG is associated with a lower rate of major adverse cardiac or
cerebrovascular events at 1 year among patients with three-vessel or left main coronary artery disease when compared to PCI.
• SYNTAX scores may be helpful in delineating which patients have complex coronary anatomy and thus have an increased risk of suboptimal outcome with PCI.
• Patients benefit from a thorough review of all pertinent data. A “heart team” should make a decision regarding the best treatment for the patient and actively involve the patient in making this decision.
• 40% of patients will clearly benefit from one procedure vs. the other (e.g., those unable to take antiplatelets, difficult anatomy).
• The risk of PCI and repeat revascularization needs to be balanced against the invasiveness of CABG and the risk of stroke.

References• Hannan EL, Wu C, Walford G, et al. Drug-eluting stents vs. coronary-artery
bypass grafting in multivessel coronary disease. N Engl J Med 2008;358:331-41.• Bravata DM, Gienger Al, McDonald KM, et al. Systematic review: the
comparative effectiveness of percutaneous coronary interventions and coronary artery bypass graft surgery. Ann Intern Med 2007;147:703-16.
• Sianos G, Morel MA, Kappetein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. Euro Interv 2005;1:219-27.
• Pocock, SJ. The pros and cons of noninferiority trials. Fund Clin Pharm 2003;17:483-90.
• Hwang IK, Morikawa T. Design issues in noninferiority/equivalence trials. Drug Information J. 1999;33:1205–1218.
• Snapinn, SM. Noninferiority Trials. Curr Control Trials Cardiovasc Med. 2000; 1(1): 19–21.