joelho / knee - mr
DESCRIPTION
Protocolos; Anatomia; Checklist; Meniscos: Roturas e Degeneração; Ligamentos Cruzados: Roturas; Cartilagem / Condromalácia. Ligamentos Colaterais: Estiramentos e Roturas; Complexo Ligamentar Patelofemoral;TRANSCRIPT
JOELHO - RM
Dr. Emanuel R. Dantas
Médico Radiologista
Membro Titular do Colégio Brasileiro de Radiologia
Fonte: Stoller
Emanuel R. Dantas

IMAGING PROTOCOLS FOR THE KNEE
FS PD FSE is a fluid-, articular cartilage-, and marrow-sensitive sequence (TR ≥3,000 msec and TE 40–50 msec) that should be performed in the coronal, sagittal, and axial planes.
Sagittal T2* GRE images are helpful for identifying meniscal degeneration, patellar tendinosis, and chondrocalcinosis.
Incorporate a T1-weighted image in at least one imaging plane to obtain an accurate assessment of marrow fat signal intensity changes in sclerosis or edema in cases of trauma, infection, and neoplasia.
Trochlear groove chondral lesions are best evaluated with sagittal images, whereas patellar facet chondromalacia is best assessed on axial images.
An acquisition matrix (number of phase encodings) of 256 or higher, a field of view of 12 to 14 cm, and 1 to 2 number of excitations (NEX) are routinely used.
Emanuel R. Dantas

IMAGING PROTOCOLS FOR THE KNEE
Observações:
If FS PD FSE images are not acquired, conventional
or non-FS FSE T2-weighted images are usually
supplemented with a short inversion time (TI)
inversion recovery (STIR) sagittal acquisition to
improve visualization of osseous contusions and
muscle trauma.
Emanuel R. Dantas

Emanuel R. Dantas
Emanuel R. Dantas
IMAGING PROTOCOLS FOR THE KNEE
• Observações:
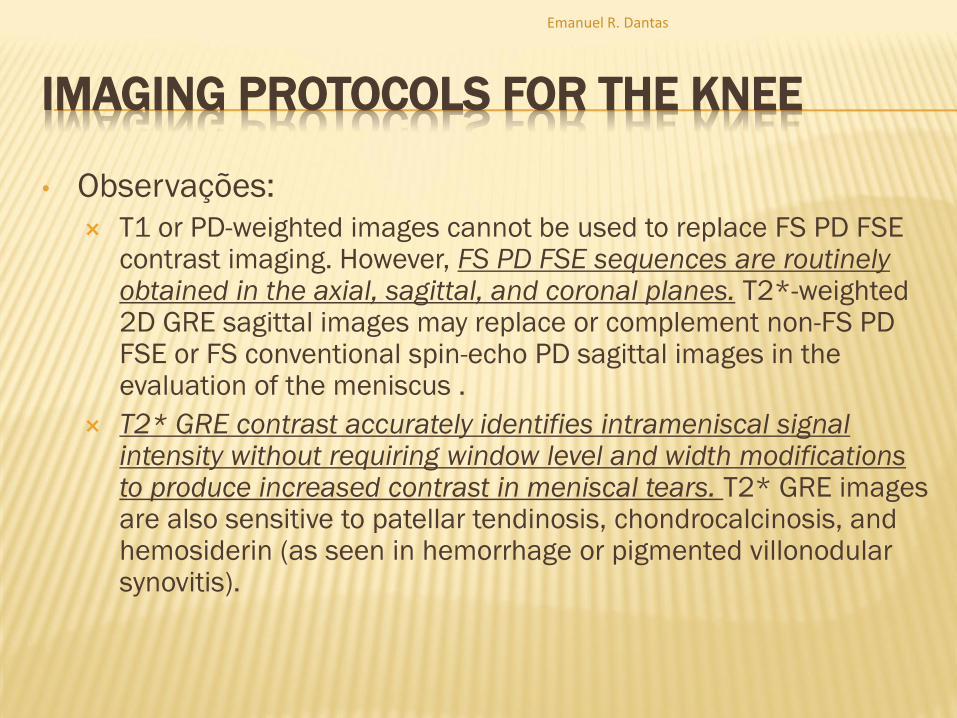
T1 or PD-weighted images cannot be used to replace FS PD FSE contrast imaging. However, FS PD FSE sequences are routinely obtained in the axial, sagittal, and coronal planes. T2*-weighted 2D GRE sagittal images may replace or complement non-FS PD FSE or FS conventional spin-echo PD sagittal images in the evaluation of the meniscus .
T2* GRE contrast accurately identifies intrameniscal signal intensity without requiring window level and width modifications to produce increased contrast in meniscal tears. T2* GRE images are also sensitive to patellar tendinosis, chondrocalcinosis, and hemosiderin (as seen in hemorrhage or pigmented villonodular synovitis).
Emanuel R. Dantas
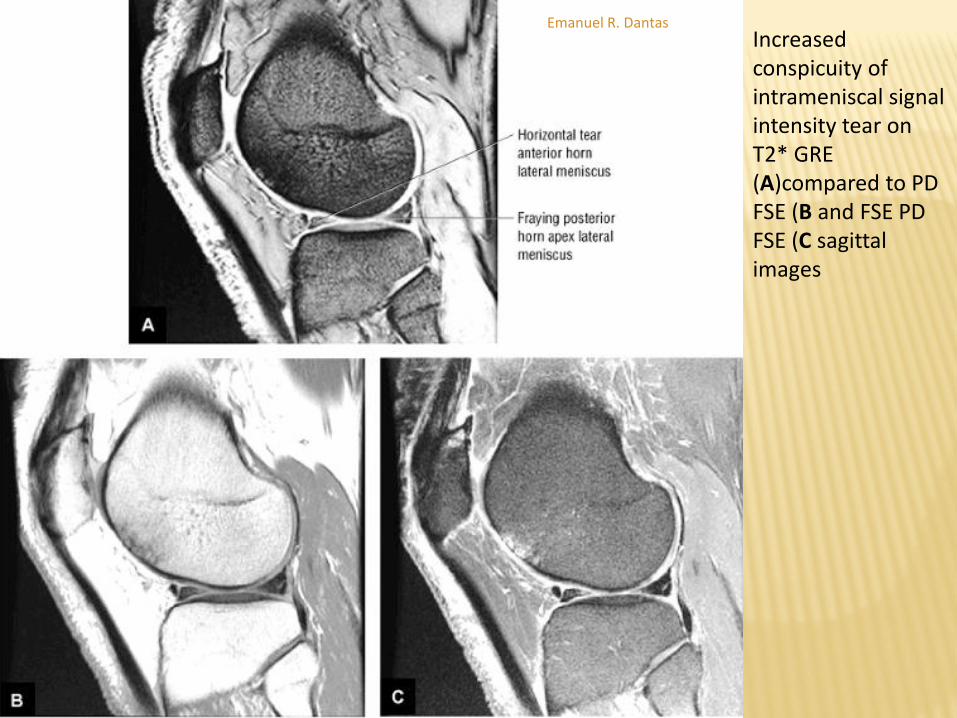
Increased conspicuity of intrameniscal signal intensity tear on T2* GRE (A)compared to PD FSE (B and FSE PD FSE (C sagittal images
Emanuel R. Dantas
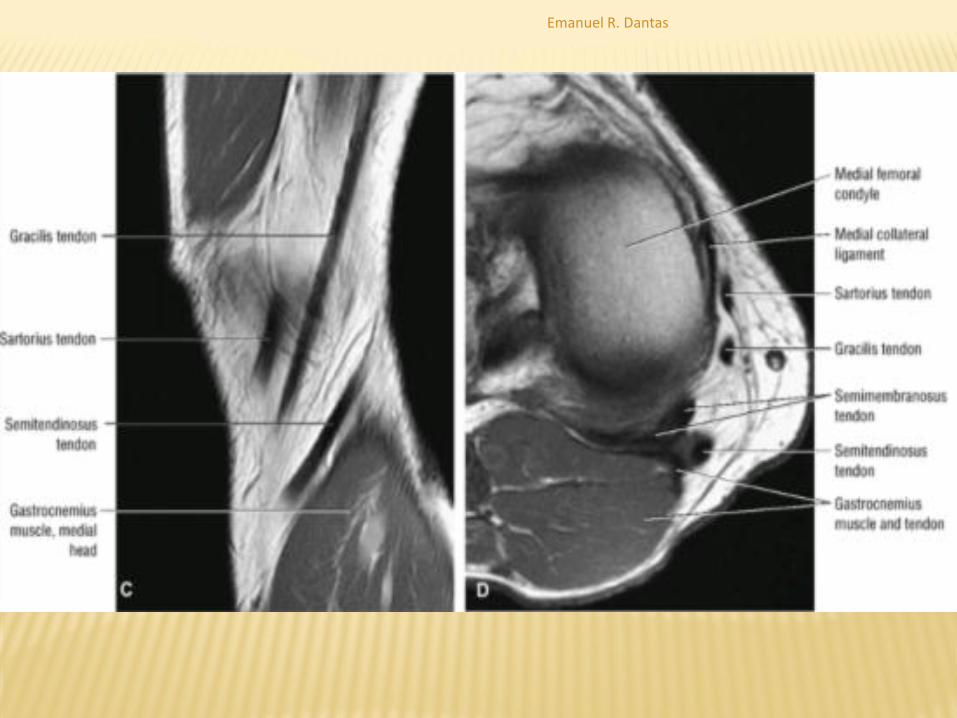
SAGITTAL IMAGES – ANATOMY
Sagittal plane dissection displays the components of the medial and lateral collateral ligaments and the adjacent capsule:
Superficial medial dissection displays the conjoined pes anserinus tendons (semitendinosus, gracilis, and sartorius) as they course along the posteromedial aspect of the knee.
The pes anserinus runs superficial to the distal MCL and inserts into the anteromedial tibial crest distal to the joint line.
Emanuel R. Dantas

Emanuel R. Dantas
Emanuel R. Dantas

SAGITTAL IMAGES – ANATOMY
On the lateral aspect of the knee, the LCL and
the more posteriorly located fabellofibular
ligament (structures of the posterolateral
corner of the knee) can be seen.
Emanuel R. Dantas

Lateral retinaculum and related structures and attachment of the iliotibial band, also referred to as the iliotibial tract, to Gerdy's tubercle. The thickened fascia lata forms a longitudinal fiber band referred to as the iliotibial tract. The iliotibial tract and tensor fasciae latae originate from the anterior superior iliac spine
Emanuel R. Dantas
SAGITTAL IMAGES – ANATOMY
The ACL and PCL are best displayed on sagittal images.
The LCL, or fibular collateral ligament, and the biceps
femoris tendon also may be seen on peripheral sagittal
sections.
Images in the sagittal plane are key in evaluating meniscal
anatomy for both degenerations and tears.
The MCL is usually partially defined in the sagittal plane on
peripheral medial sagittal images. Complex meniscal and
bucket-handle tears may require coronal images to identify
displaced meniscal tissue or fragments
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - CORONAL
PLANE CHECKLIST
In the coronal plane, the primary checklist
structures are:
(1) the collateral ligaments.
Additional structures to be examined include:
(2) the cruciate ligaments,
(3) the menisci,
(4) articular cartilage,
(5) osseous structures,
(6) the iliotibial tract.
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - CORONAL
PLANE CHECKLIST
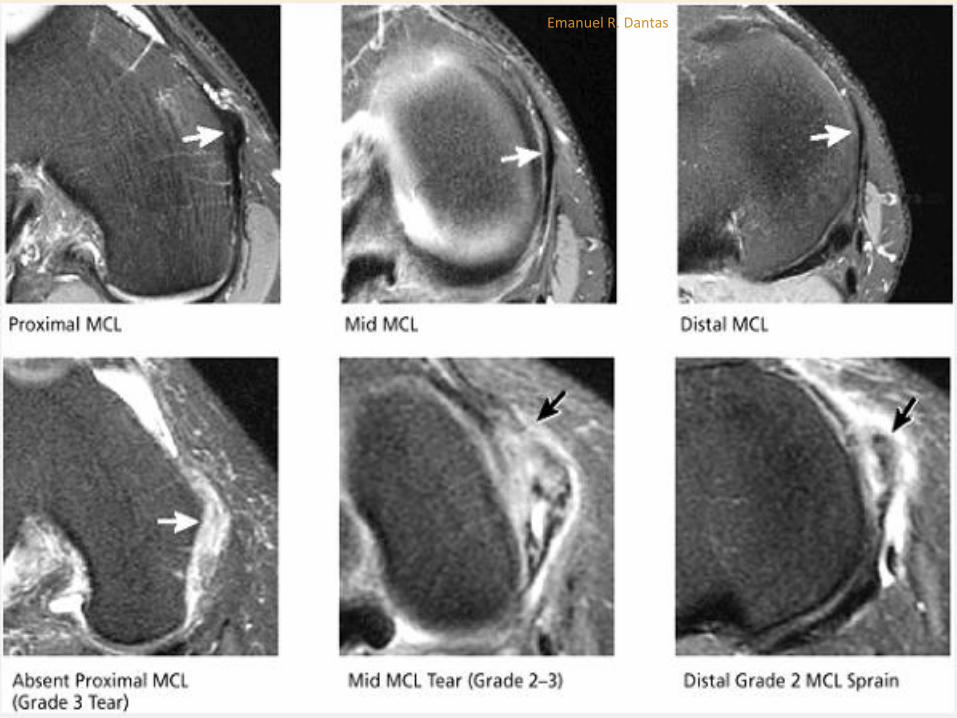
Medial Collateral Ligament:
The MCL is initially located on the image that demonstrates fusion of the medial and lateral femoral condyles.
On this image, the posterior aspect of the MCL is seen as a hypointense band of fibers extending along the peripheral aspect of the medial femoral condyle and medial tibial plateau.
Proceeding in an anterior direction, the entire posterior-to-anterior extent of the MCL is demonstrated over the next one or two images.
A coronal image through the intact posterior fibers of the MCL may not demonstrate a partial-thickness tear, since these injuries preferentially involve the anterior fibers.
It is important to examine the entire course of the MCL from its origin on the medial femoral condyle to its distal insertion on the proximal tibial metaphysis, as tears can occur anywhere along this course.
Emanuel R. Dantas
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - CORONAL
PLANE CHECKLIST
Lateral Collateral Ligament :
Identification of the LCL also starts with the image on which
the femoral condyles fuse.
The origin of the LCL from the lateral femoral condyle is
visualized on either this image or one image posterior to it.
Unlike the MCL, which has a nearly straight vertical course,
the LCL runs posteriorly in an oblique inferior direction.
Proceeding in a posterior direction, it is demonstrated in its
entire course, to the attachment of the LCL at the tip of the
fibular head, over two images.
Emanuel R. Dantas

Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - CORONAL
PLANE CHECKLIST
Anterior Cruciate Ligament:
Identification of the LCA again starts with the image that demonstrates the femoral condyles fusing.
Proceeding for two or three images in a posterior direction, the origin of the LCA is identified along the medial margin of the lateral femoral condyle.
From this image location, proceeding in an anterior direction, the entire posterior-to-anterior course of the LCA is demonstrated over the next five or six images. The LCA follows an inferior oblique course to its insertion on the anterior tibia.
Emanuel R. Dantas

Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - CORONAL
PLANE CHECKLIST
Posterior Cruciate Ligament:
The origin of the PCL, at the anterior lateral aspect of
the medial femoral condyle, can be identified on or
near the same image as the distal insertion of the LCA.
On coronal images, proximal PCL fibers are seen in
cross-section.
Progressing in a posterior direction for four or five
images, the PCL fibers can be seen to gradually turn
90° and course vertically downward to their insertion
on the posterior tibia.
Emanuel R. Dantas

Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - CORONAL
PLANE CHECKLIST
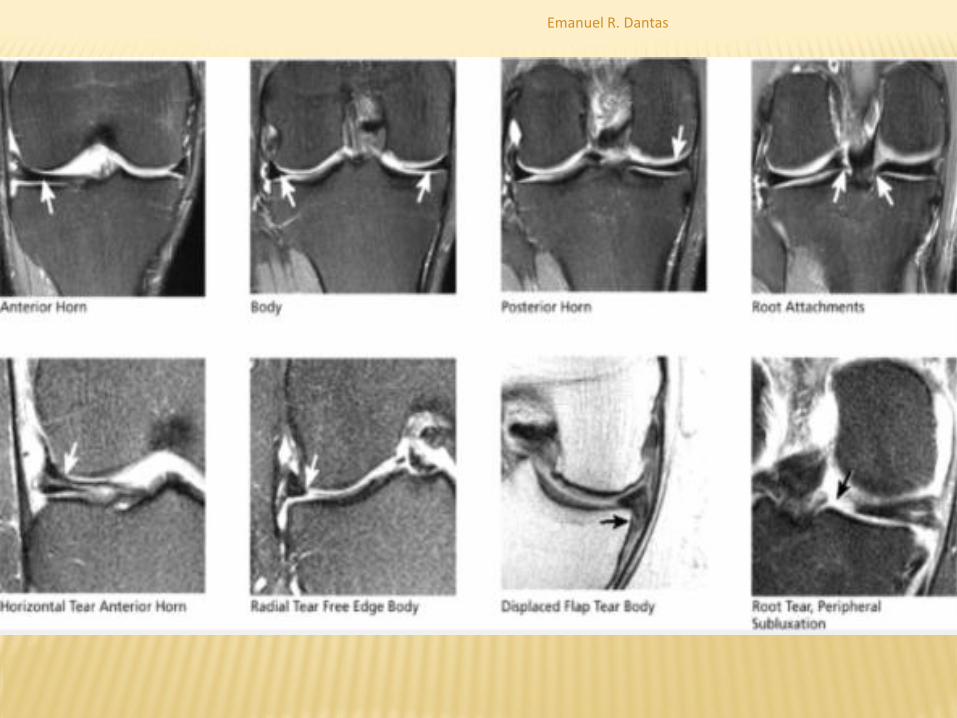
Menisci:
The posterior horns of the menisci are first identified on the coronal image on which the fibula first comes into view.
The meniscal root ligaments are seen as thin, short, hypointense fibrous bands that extend from the inner margins of the posterior horns to where they attach centrally near the tibial spines.
The root is a frequent location for radial tears that disrupt the root attachment and undermine the meniscal hoop containment fibers, which keep the meniscus from extruding peripherally with joint loading.
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - CORONAL
PLANE CHECKLIST
Menisci:
The body segments of the menisci are demonstrated on coronal images anterior to the level of the fibula.
Continuing in an anterior direction, the anterior horns can be seen at the margins of the anterior edge of the tibia.
Normal anterior horn and body segments appear on coronal images as black triangles with sharp tips, which represent the inner free edge. There is no increased signal interrupting either the superior or inferior articular surface of the meniscus.
Emanuel R. Dantas
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - CORONAL
PLANE CHECKLIST
Articular Cartilage :
Cartilage can be seen covering the medial and lateral tibial plateau and
distal femur.
On coronal images, the anterior horns of the menisci are the landmarks for
demarcating cartilage compartments.
At and posterior to the anterior horns, cartilage covers the femoral condyle
and tibial plateau, and is classified as medial or lateral compartment
cartilage.
The underlying subchondral bone is also examined to identify reactive bone
marrow edema or cystic change subjacent to areas of chondral erosion.
On coronal images, loose bodies are often identified along the posterior joint
line posterior to the PCL and menisci, along the anterior joint line anterior to
the LCA, and within the patellofemoral recesses between the patella and
distal femur.
Emanuel R. Dantas

Emanuel R. Dantas

Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
In the sagittal plane, the primary checklist structures are:
(1) the medial and lateral menisci;
(2) the chondral surfaces of the medial and lateral compartment;
(3) the trochlear groove cartilage;
(4) the anterior and posterior cruciate ligaments.;
Other structures observed in the sagittal plane include:
(5) the posteromedial and posterolateral corners;
(6) the patellar and quadriceps tendons,
(7) subchondral bone and marrow,
(8) joint fluid/effusion,
(9) Hoffa's fat pad and plicae
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
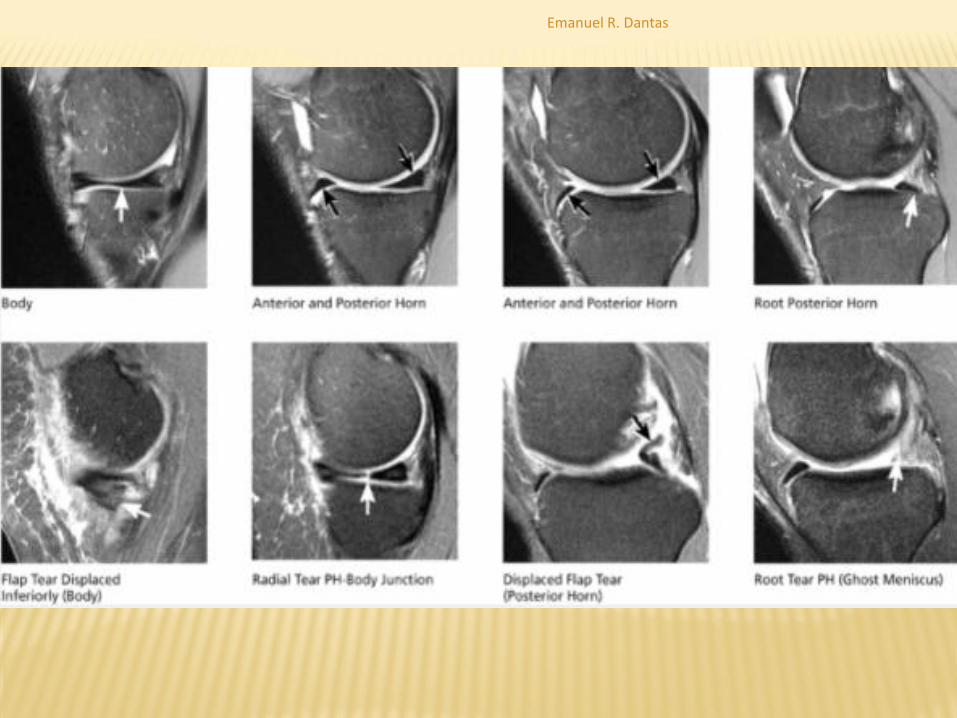
Medial and Lateral Menisci:
The anterior and posterior horns of the meniscus appear as black triangles with a sharp inner free edge.
The root of the posterior horn can be identified in the peripheral aspect of the medial or lateral compartment, approaching the intercondylar notch.
A radial tear through the root of the posterior horn appears as a “ghost meniscus,” with absence of meniscal signal in the expected location of the posterior horn root.
The “ghost meniscus” appearance is due to localization of the sagittal image in a plane directly through the gap in the posterior horn meniscal tissue caused by the radial tear.
Emanuel R. Dantas
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
Medial and Lateral Compartment Articular Cartilage:
Cartilage covers the medial and lateral femoral condyles from anterior to posterior.
The anterior meniscal horn demarcates the division between the trochlear groove cartilage (located anterior to the anterior horn), and the femoral condyle cartilage (located at and posterior to the anterior horn).
Covering the mid-weight-bearing surfaces of the femoral condyles, the cartilage extends posteriorly past the level of the posterior horn of the meniscus and posterosuperiorly to cover the extreme posterior aspect of the femoral condyle subjacent to the gastrocnemius tendon origins.
Emanuel R. Dantas

Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
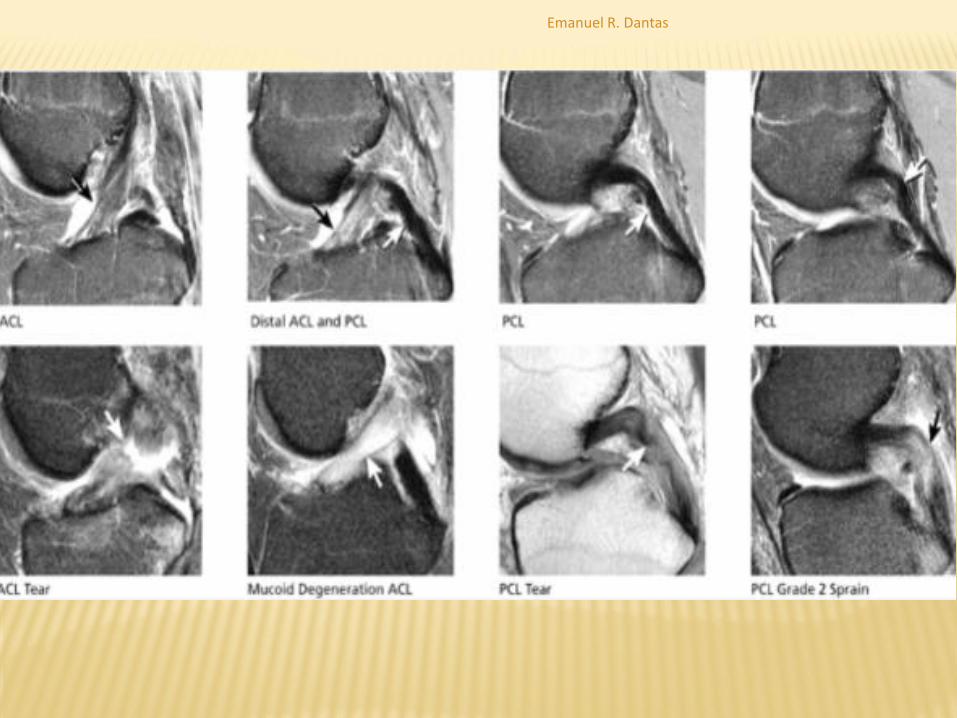
Anterior and Posterior Cruciate Ligaments:
The entire course of the LCA and PCL can be seen on two or three
midline sagittal images.
Complete acute tears are characterized with respect to
involvement of the origin, proximal third, middle third, or distal
attachment.
Full-thickness tears present as complete discontinuity of LCA or
PCL fibers, whereas sprains are characterized by continuous
fibers traversing the entire length of the notch, although
individual fibers display laxity, increased signal intensity, or loss
of definition.
In the case of LCA scarring, fibers also appear lax or indistinct.
Emanuel R. Dantas
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
Posteromedial and Posterolateral Corners:
A secondary role for sagittal imaging is to assess the structures of
the posteromedial corner, including all tendons, ligaments, and
capsular structures that traverse the posterior medial quadrant of
the knee.
Individual tendons are not always depicted on each MR image. The
MCL is seen on the most peripheral sagittal image.
Subsequent images depict the distal sartorius, gracilis, and
semitendinosus tendons coursing obliquely posteromedial to the
tibia.
The origin of the semimembranosus can be seen at the
posteromedial margin of the medial tibial plateau.
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
Posteromedial and Posterolateral Corners:
The origin of the medial head of the gastrocnemius is seen at the posteromedial margin of the medial femoral condyle metaphysis.
The meniscotibial and meniscofemoral ligaments (also known as the meniscocapsular ligaments) are seen along the entire course of the posteromedial corner, fanning out and away from the posterior edge of the posterior horn of the medial meniscus.
The meniscocapsular ligaments also can be seen extending along the anteromedial quadrant to form a full arc around the entire course of the meniscus.
Emanuel R. Dantas

Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
Posteromedial and Posterolateral Corners:
The most peripheral image through the posterolateral corner demonstrates the V-shaped convergence of the fibular collateral ligament (anterior limb of the “V”) and the distal biceps femoris tendon (posterior limb of the “V”) inserting on the proximal fibula.
On the next, deeper, image the origin of the popliteus tendon along the posterolateral aspect of the lateral femoral condyle is displayed.
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
Posteromedial and Posterolateral Corners:
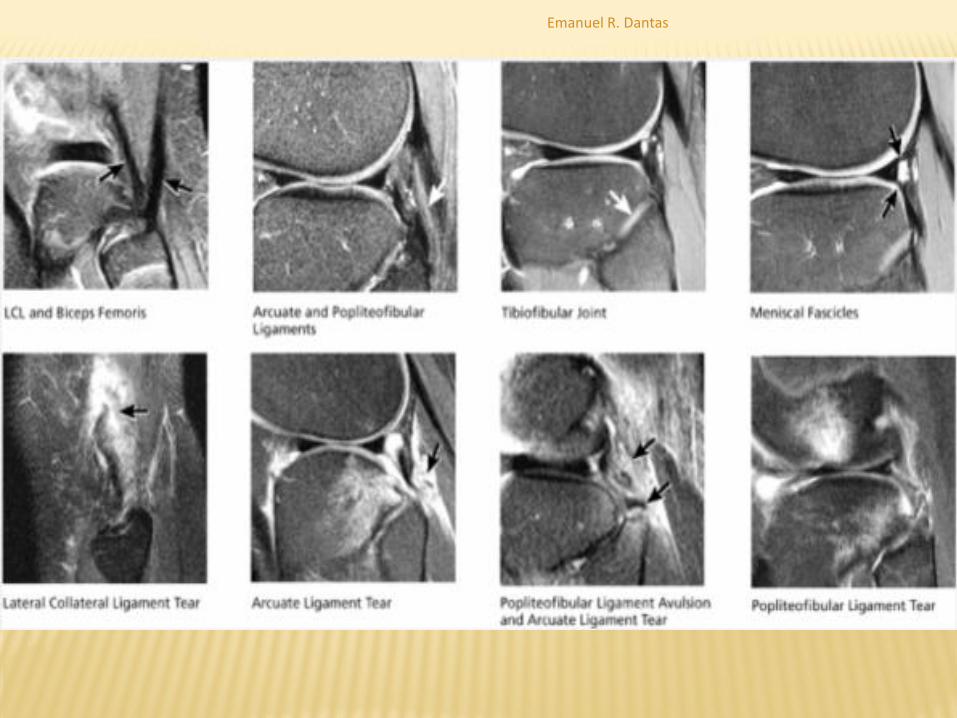
Occasionally, the popliteofibular ligament is also displayed on this
same image and is seen as a dark band of fibers extending from
the origin of the popliteus tendon to the superior tip of the fibula.
The course of the popliteus tendon, as it sweeps posterolateral to
the posterior horn of the lateral meniscus, can be followed over the
next four or five images.
The arcuate ligament is a thin dark band occasionally visualized
posterior to the popliteus tendon on sagittal images. Severe edema
posterior to the popliteus tendon, with joint fluid in the space
beyond the normal posteromedial capsular structures, is a clue to
the presence of an arcuate ligament tear.
Emanuel R. Dantas
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST
Patellar and Quadriceps Tendons:
The distal quadriceps tendon and the entire course of the patellar tendon can be seen on five or six consecutive sagittal images through the patella.
All sagittal images displaying tendon tissue should be examined carefully, since partial tears and tendinosis occasionally involve only the peripheral margin of the tendons.
Distal quadriceps tendinosis is characterized by thickening and increased signal intensity at the distal quadriceps insertion on the superior pole of the patella.
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - SAGITTAL
PLANE CHECKLIST Patellar and Quadriceps Tendons:
Patellar tendinosis commonly occurs at the proximal origin of the patellar tendon on the inferior pole of the patella.
Patellar tendon inflammation associated with Osgood-Schlatter disease is displayed on sagittal images at the distal insertion of the patellar tendon on the tibial tubercle.
Patella baja and patella alta are also diagnosed on sagittal images based on the relative position of the patella (and length of the patellar tendon) with respect to the femur
Emanuel R. Dantas

Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - AXIAL
PLANE CHECKLIST
In the axial plane, the primary checklist structure to evaluate is (1) the cartilage covering the articular surfaces of the patella (patellofemoral compartment).
Additional structures to be evaluated include:
(2) the intercondylar notch,
(3) the menisci,
(4) collateral ligaments, and
(5) joint fluid/effusion.
Axial images are used to confirm pathology in ligaments, tendons, and muscles that are oriented nearly 90° to the axial plane (including the collateral ligaments and patellar tendon).
Joint effusions and popliteal cysts can be quantified and characterized on axial plane images.
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - AXIAL
PLANE CHECKLIST
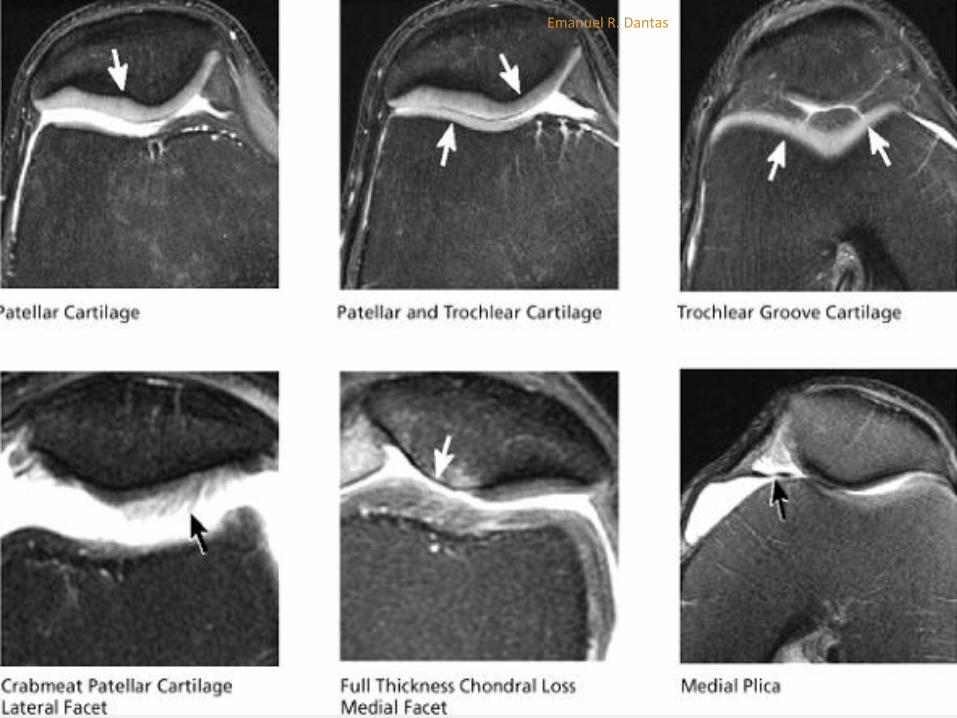
Patellofemoral Compartment
The primary structures reviewed on axial images are in the patellofemoral compartment.
The medial patellar facet, median ridge, and lateral patellar facet cartilages are clearly demonstrated.
The full cranial-caudal extent of the patellar cartilage is demonstrated on consecutive axial images.
The medial plica, extending from the medial capsule toward the medial patellar facet, may also be seen on axial plane images, with fluid visualized both anterior and posterior to the plica.
Emanuel R. Dantas
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - AXIAL
PLANE CHECKLIST
Patellofemoral Compartment The patellar and quadriceps tendons are evaluated
by examining consecutive cranial-to-caudal images above and below the patella. The patellar and quadriceps tendon fibers are oriented nearly 90° to the axial plane.
On superior axial images above the level of the patella, the tendons for the vastus medialis and lateralis are seen just medial and lateral to the distal quadriceps tendon.
Emanuel R. Dantas

Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - AXIAL
PLANE CHECKLIST
Patellofemoral Compartment
As the superior aspect of the patella comes into view, the medial and lateral retinacula are depicted, originating on the medial and lateral aspect of the patella and extending peripherally to insert on the medial and lateral femoral condyles, respectively.
In transient lateral subluxation of the patella, tears of the medial retinaculum are often identified at either the patellar origin or the medial femoral condyle insertion. If transient lateral subluxation is recognized, a careful search for osteochondral defects and associated loose bodies should be performed.
Emanuel R. Dantas

Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - AXIAL
PLANE CHECKLIST
Intercondylar Notch
On superior images through the femoral condyles, the posterior
intercondylar notch is shown as a U-shaped, wide, concave groove
between the posterior medial and lateral femoral condyles.
The origin of the LCA is seen as a thin, obliquely oriented band of
fibers lying along the anterolateral aspect of the “U” formed by the
posterior intercondylar notch.
It is important to identify a normal LCA origin in the axial plane,
since tears commonly occur at or near the LCA origin.
Tears are seen as ill-defined high-intensity signal that replaces the
normal thin hypointense band of LCA origin fibers
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE - AXIAL
PLANE CHECKLIST
Intercondylar Notch
Moving in an inferior direction through the notch, as
the intercondylar notch opens anteriorly,
consecutive axial images depict the LCA origin
fanning out into multiple distinct dark LCA fibers
that course medially and inferiorly through the
intercondylar notch.
The LCA ends distally as a foot-shaped insertion
upon the anterolateral tibia.
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE - AXIAL
PLANE CHECKLIST
Intercondylar Notch
The PCL origin can be seen two images inferior to the axial image displaying the LCA origin.
The PCL origin is depicted as a broad band of fibers occupying the medial half of the “U” formed by the posterior intercondylar notch.
Proceeding in an inferior direction from the origin, the PCL can be seen to make a 90° turn on the next one or two images.
At this point it becomes perpendicular to the axial plane and descends in the mid-posterior notch to insert on the posterior tibia.
Emanuel R. Dantas

Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE
Collateral Ligaments
The MCL and fibular collateral ligament are oriented at a 90° angle to
the axial plane.
At the medial margin of the medial femoral condyle, the origin of the MCL
can be seen as a thin short band of fibers that course along the medial
joint line to insert on the proximal tibia, anterior to the pes anserinus
tendons.
The LCL is depicted at the lateral margin of the lateral femoral condyle,
and courses inferiorly to insert on the lateral tip of the fibula.
Complete rupture of the collateral ligaments is seen as a “ghost
ligament,” caused by the absence of ligament fibers on the axial image
directly through the level of the tear, and is most often accompanied by
prominent surrounding edema and synovitis.
Emanuel R. Dantas
IMAGING CHECKLIST FOR THE KNEE
Collateral Ligaments
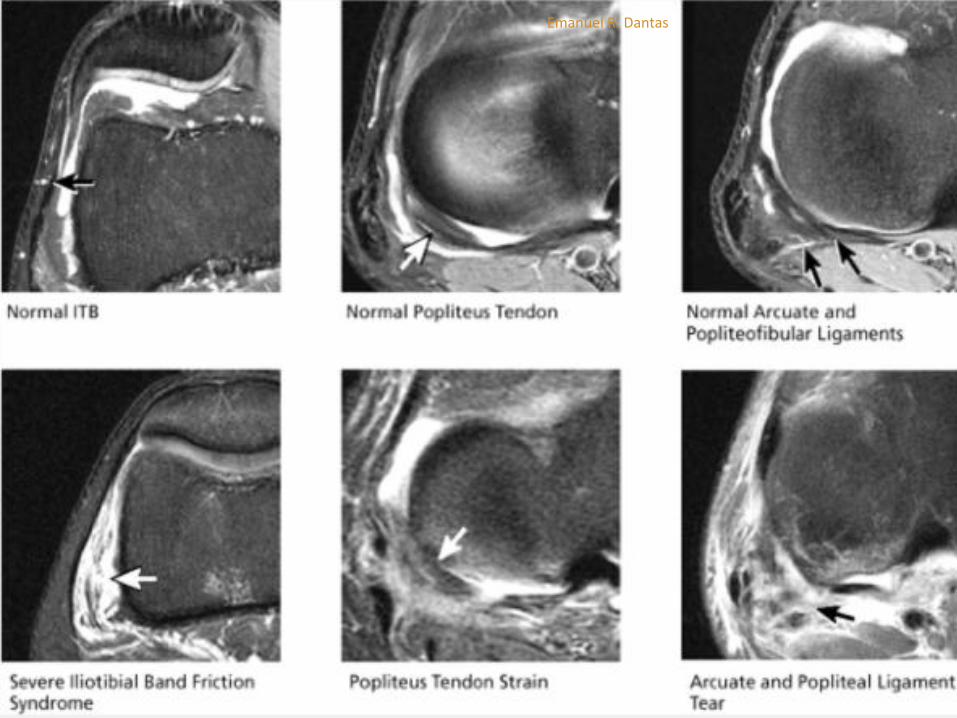
The posterolateral corner structures adjacent to the LCL are
also identified on axial images.
The popliteus tendon origin is seen just posterior and deep
to the LCL origin along the lateral femoral condyle.
On more inferior images, the popliteus tendon swings
medially to course posterior to the posterior lateral tibial
plateau.
The arcuate ligament and popliteofibular ligament are seen
posterior to the popliteus tendon on images above the level
of the fibula.
Emanuel R. Dantas
Emanuel R. Dantas

Emanuel R. Dantas
Emanuel R. Dantas

IMAGING CHECKLIST FOR THE KNEE
Joint Fluid/Effusion
Joint effusions are evaluated on axial images to determine the size of the effusion and the character of its contents.
In chondromalacia or osteochondral lesions, a careful search should be made for loose bodies within the effusion.
The loose bodies may be osseous, chondral, or osteochondral in nature.
Common locations for loose bodies include the medial and lateral patellofemoral recesses, the suprapatellar bursa, the popliteus tendon sheath, the posterior intercondylar notch, and within popliteal cysts.
Popliteal cysts may also be found between the semimembranosus tendon and the tendon for the medial head of the gastrocnemius.
Bursitis in multiple locations, including prepatellar bursitis, pes anserinus bursitis, and tibial collateral ligament bursitis, may also be depicted.
Emanuel R. Dantas

Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pearls and Pitfalls
Grade 1 and grade 2 signal intensity represent intrasubstance
degeneration and not fibrocartilaginous tearing.
Grade 3 signal intensity represents a meniscal tear. (The term
“tear” should not be used in conjunction with grade 1 or grade 2
signal.)
A closed meniscal tear is characterized by grade 3 signal intensity
that weakens or attenuates as it approaches an articular surface
of the meniscus.
The articular surface of the meniscus is defined as an inferior or
superior surface or the free edge apex of the meniscal
fibrocartilage.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pearls and Pitfalls
Degenerative changes and tears results in local increases in the freedom of
trapped water molecules, causing an increase in T2 times and allowing
detection of increased signal intensity on short-TE sequences.
As a result, the increased intrameniscal signal intensity seen in
degeneration and tears is best visualized on short-TE images using T1,
intermediate-weighted (PD), or GRE sequences. Increased signal intensity in
synovial fluid gaps has been confirmed in surgically induced tears in animal
models.
In the absence of a joint effusion, meniscal degenerations and tears may
actually decrease in signal intensity on T2-weighted images. On T2*-
weighted GRE images, however, intrasubstance degeneration and tears
generate increased signal intensities. Therefore, GRE sequences are
extremely sensitive to the spectrum of meniscal degenerations and tears.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pearls and Pitfalls FSE sequences are not as useful in the evaluation of
intrasubstance meniscal signal intensity and tears, even when performed with an ETL (number of echoes per TR) of 4 or less.29 FSE images may underestimate the extent or grades of MR signal intensity and thus mask the presence of a tear.
Rubin et al.29 have attributed this blurring, which limits the usefulness of FSE images, to a ghosting artifact or an increase in magnetization transfer. Blurring is more pronounced with the use of a shorter effective TE, a longer echo train, and a smaller acquisition matrix.
Short effective TE-related blurring occurs secondary to attenuation by T2 decay of later echoes (high spatial-frequency data) at the edges of k-space.
Emanuel R. Dantas

(A) Collagen network representing the radial tie fibers oriented from the circumferential peripheral zone. (B) Gross meniscal sections identify the location of the middle perforating collagen bundle and the site of preferential horizontal mucinous degeneration (arrowheads).
Emanuel R. Dantas

C) Grade 2 signal intensity (arrow) is seen in the posterior horn of the medial meniscus on a T2*-weighted image. (D) Grade 2 signal seen in C is not apparent on the corresponding FS T2-weighted FSE image
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
To understand the significance of increased signal
intensity in meniscal abnormalities, an MR grading
system has been developed and correlated with a
pathologic (i.e., histologic) model.
Areas of degeneration demonstrate increased signal
intensity in a spectrum of patterns or grades that are
based on the signal distribution (morphology) relative
to an articular meniscal surface or meniscal apex,
exclusive of the peripheral capsular margin of the
meniscus, which is considered nonarticular.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
The articular meniscal surfaces refer to the superior and inferior aspects of the meniscus opposite the distal femoral and proximal tibial articular cartilage surfaces, respectively.
Signal intensity changes include the following:
In MR grade 1, a nonarticular focal or globular intrasubstance increased signal intensity is seen.
Histologically, grade 1 signal intensity correlates with foci of early mucinous degeneration and chondrocyte-deficient or hypocellular regions that are pale-staining on hematoxylin and eosin preparations. The terms “mucinous,” “myxoid,” and “hyaline” degeneration can be used interchangeably to describe the accumulation of increased production of mucopolysaccharide ground substance in stressed or strained areas of the meniscal fibrocartilage.
These changes usually occur in response to mechanical loading and degeneration.
Grade 1 signal intensity may be observed in asymptomatic athletes and normal volunteers and is not clinically significant.
Emanuel R. Dantas

(A) Focal or globular intrameniscal degeneration (yellow) within the central shear plane of the middle collagen fibers. (B) Corresponding grade 1 signal intensity within the posterior horn of the medial meniscus on an FS PD FSE sagittal image. (C) On a cut gross section, a focus of meniscal degeneration (arrow) can be seen. (D) The corresponding photomicrograph shows hypocellularity, with decreased numbers of chondrocytes (black arrow) in pale-staining areas (white arrow). (Hematoxylin and eosin stain)
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
In MR grade 2, a horizontal, linear intrasubstance increased signal intensity
usually extends from the capsular periphery of the meniscus without
involving an articular meniscal surface.
Areas and bands of mucinous degeneration are more extensive in MR
grade 2 than in MR grade 1.
Patients with images of grade 2 signal intensity are usually asymptomatic.
Although the posterior horn of the medial meniscus is the most common
location of grade 2 signal intensity, the finding of grade 2 signal intensity
cannot be used as a prognostic indicator for development of grade 3 signal
intensity.
Although it is has been suggested that grade 2 meniscal signal intensity is a
risk factor for the development of symptomatic meniscal tears, this theory
has not been confirmed
Emanuel R. Dantas

(A) Linear orientation of grade 2 intrasubstance degeneration (yellow) in the middle layer of the meniscal fibrocartilage. (B) Corresponding linear grade 2 signal intensity located in the central shear plane of the meniscus between the superior and inferior leaves of the meniscal fibrocartilage
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
A meniscus is considered MR grade 3 when the area of increased signal intensity communicates or extends to at least one articular surface.
A meniscus may contain multiple areas of grade 3 signal intensity or the entire meniscal segment (horn) may be involved, with irregular morphology.
Grade 3 signal intensity is most frequent in the posterior horn of the medial meniscus, a finding supported by the observations of increased stress and strain generated on the undersurface of the medial meniscus with femoral tibial rotations.
Emanuel R. Dantas

(A) Continuity of meniscal tear with intrasubstance degeneration (yellow) as an area of structural weakening of the meniscal fibrocartilage. (B) Flap tear inferior surface extension and continuity with peripheral directed meniscal hyperintensity. There are both horizontal (H) and vertical (V) components to this obliquely oriented tear.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Fibrocartilaginous separation or tears can be found in all menisci with grade 3 signal intensity. In less than 5%, these disruptions represent what has been referred to in the orthopaedic literature as confined intrasubstance cleavage or closed tears
Diagnosis of closed meniscal tears requires surgical probing during arthroscopy and might be missed altogether on a routine arthroscopic examination if surface extension is not identified.
Attenuation of grade 3 meniscal signal intensity as it approaches an articular surface is characteristic of closed tears.
Closed tears may also represent some of the false-positive interpretations of grade 3 signal intensity when correlated with arthroscopy. Meniscal tears frequently occur adjacent to areas of intrasubstance degeneration.
Emanuel R. Dantas

Attenuated grade 3 signal intensity that weakens toward the inferior articular surface of the meniscus in a closed tear (sagittal perspective).
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Classification of Meniscal Tears - Pearls and Pitfalls
Based on MR sagittal sections:
Vertical
Horizontal (includes the pure horizontal cleavage type)
Based on circumferential or surface anatomy:
Longitudinal (vertical or horizontal on corresponding meniscal sections)
Flap (vertical or horizontal)
Radial (vertical)
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Classification of Meniscal Tears - Pearls and Pitfalls
Longitudinal and flap tears can have either a primary vertical or horizontal tear pattern on corresponding sagittal images.
Confusion exists because longitudinal and flap tears have been previously classified only as vertical tear types.
Radial tears, including classic radial tears and root tears, are vertical tears.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Horizontal Tears - Pearls and Pitfalls
A pure horizontal cleavage tear extends to the apex of the meniscus and results from excessive shear stress.
Longitudinal and flap tears may have a relative (not pure) horizontal orientation as viewed in the sagittal plane. However, these tear patterns occur only in association with superior or inferior leaf extension.
Horizontal cleavage tears are less common than flap tears.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Horizontal Tears - Pearls and Pitfalls
The term “horizontal tear” is used to describe a horizontal cleavage tear that extends to the free edge of the meniscus in the plane of the middle collagen fibers with peripheral signal degeneration that may extend to the capsular periphery.
In other words, horizontal tears occur in the horizontal plane and dissect circumferential collagen fibers, resulting in two separate shelves or leaves of the meniscal fibrocartilage.
Although flap tears and longitudinal tears may have a relative horizontal tear vector or may demonstrate obliquely oriented grade 3 signal intensity on cross-section of the meniscus in the sagittal plane, these tears should not be classified as horizontal or pure cleavage tears.
Emanuel R. Dantas
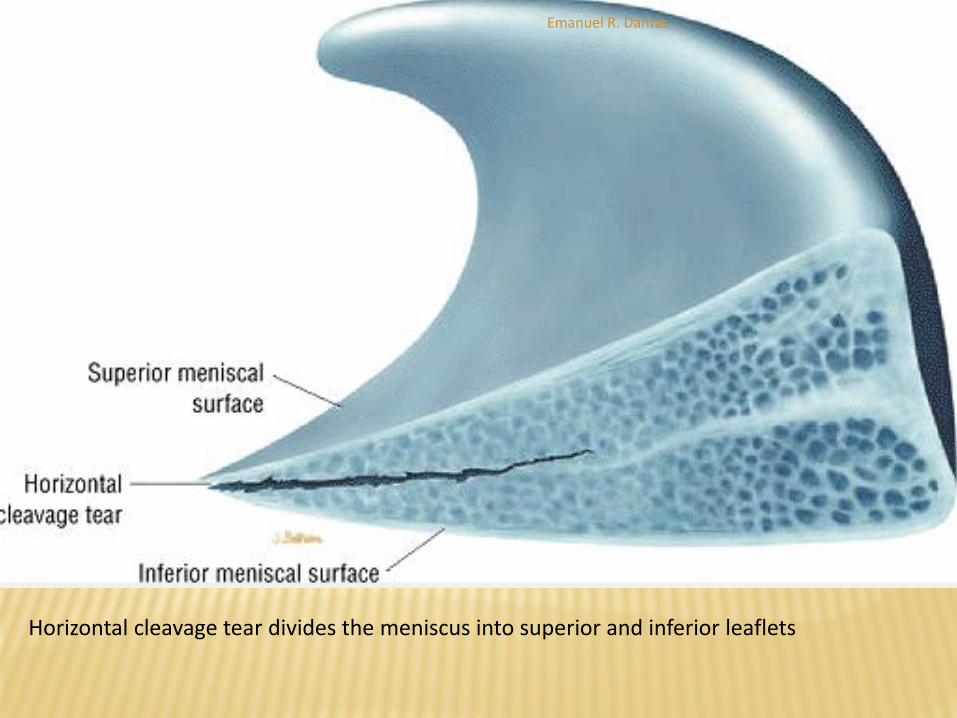
Horizontal cleavage tear divides the meniscus into superior and inferior leaflets
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Horizontal Tears
Meniscal cyst formation is commonly associated with horizontal tears.
In the presence of meniscal degeneration, tears may occur after minimal trauma.
A flap tear results when there is superior or inferior extension resulting in a change of direction (into a non-horizontal plane) of the meniscal tear pattern.
Flap tears may also develop from a radial tear with a secondary longitudinal component.
Emanuel R. Dantas

Coexistence of horizontal and flap tear patterns in the posterior horn of the medial meniscus on FS PD FSE coronal (A) and sagittal (B) images. The blunting of the inferior of the meniscus with articular surface extension represents flap tear morphology. The peripheral mensical tear pattern is primarily horizontal or vertical tear patterns on corresponding sagittal images.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Bucket-Handle Tears - Pearls and Pitfalls
Common tear in young patients with trauma
Associated with ACL injury
An unstable meniscal fragment locks into the intercondylar notch and involves at least two thirds of the meniscal circumference.
Diagnosis of a bucket-handle tear requires identification of displaced meniscal tissue from posterior to a relative anterior coronal location. If displaced meniscal tissue is restricted to posterior coronal images, consider a displaced flap tear pattern.
A double delta sign and/or a double PCL sign are sagittal MR findings of a displaced bucket-handle tear.
A displaced longitudinal tear of the meniscus, usually the medial meniscus, is called a bucket-handle tear because the separated central fragment resembles the handle of a bucket
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Medial meniscus bucket-handle tears
Medial meniscus bucket-handle tears are three times more frequent than bucket-handle tears involving the lateral meniscus.
The central fragment of a bucket-handle tear may be completely displaced into the intercondylar notch or, as may occur with a shorter tear of the posterior meniscus, may be only partially displaced.
A bucket-handle tear effectively reduces the width of the meniscus, and peripheral sagittal images fail to demonstrate the normal bowtie configuration of the body of the meniscus
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Medial meniscus bucket-handle tears
On coronal images, a displaced meniscal fragment can
frequently be identified within the intercondylar notch.
On sagittal images (provided the fragment displaces into
the intercondylar notch), the displaced fragment of a
bucket-handle tear is seen as a low-signal-intensity band
parallel and anterior to the PCL.
In simple and complex bucket-handle tears, axial images
show the relation of the displaced tear to the remaining
meniscus in a single section.
Emanuel R. Dantas
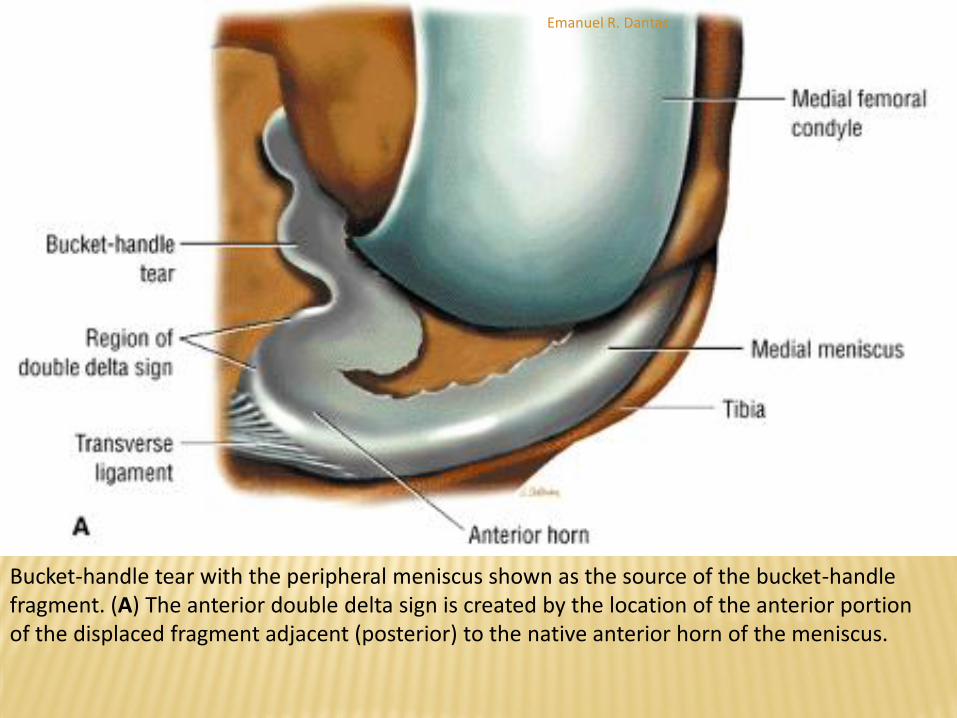
Bucket-handle tear with the peripheral meniscus shown as the source of the bucket-handle fragment. (A) The anterior double delta sign is created by the location of the anterior portion of the displaced fragment adjacent (posterior) to the native anterior horn of the meniscus.
Emanuel R. Dantas

(B) Sagittal PD FSE image showing the anterior double delta sign of a medial meniscus bucket-handle tear. Note the foreshortened posterior horn on this sagittal image. (C) An axial FS PD FSE image of the bucket-handle tear.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Medial meniscus bucket-handle tears
The double PCL sign refers to visualization of the displaced
meniscal fragment anterior to the PCL in the intercondylar notch.
The double delta sign refers to visualization of flipped inner
meniscal fragments adjacent (posterior) to the anterior horn of
the donor site.
The double delta sign is produced by two triangular structures
adjacent to each other anteriorly. The free edge of the native
anterior horn is deformed (blunted) at the anterior tear site of the
bucket-handle tear, whereas the displaced meniscal tissue has a
well-defined free edge and may be mistaken for the native
anterior horn meniscus.
Emanuel R. Dantas

Double delta and double PCL signs. (A) Axial perspective color illustration showing the displaced fragment in proximity and posterior to the anterior horn segment. The central portion of the bucket fragment is responsible for the double PCL sign. (B) Corresponding sagittal section with double delta and double PCL fragments.
Emanuel R. Dantas

(C) Effectively reduced width of the body of the meniscus serving as the donor site for the bucket-handle fragment. Native anterior horn of the medial meniscus is characteristically anterior to the displaced notch fragment on direct axial image. (D) Double PCL, double delta, and transverse ligament all on one single sagittal image.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Medial meniscus bucket-handle tears
Therefore, the presence of a third structure (separate from the ACL and PCL) within the intercondylar notch must be documented on more than a single posterior coronal image to fulfill the criteria of a bucket-handle tear.
A less common occurrence is the finding of bucket-handle tears in both the medial and lateral compartments.
In this situation four meniscal fragments can be seen in the coronal plane.
Three separate meniscal fragments can be seen anterior to the PCL on sagittal plane images when the anterior tear site of the bucket-handle tear and the displaced notch fragments are co-linear.
Emanuel R. Dantas
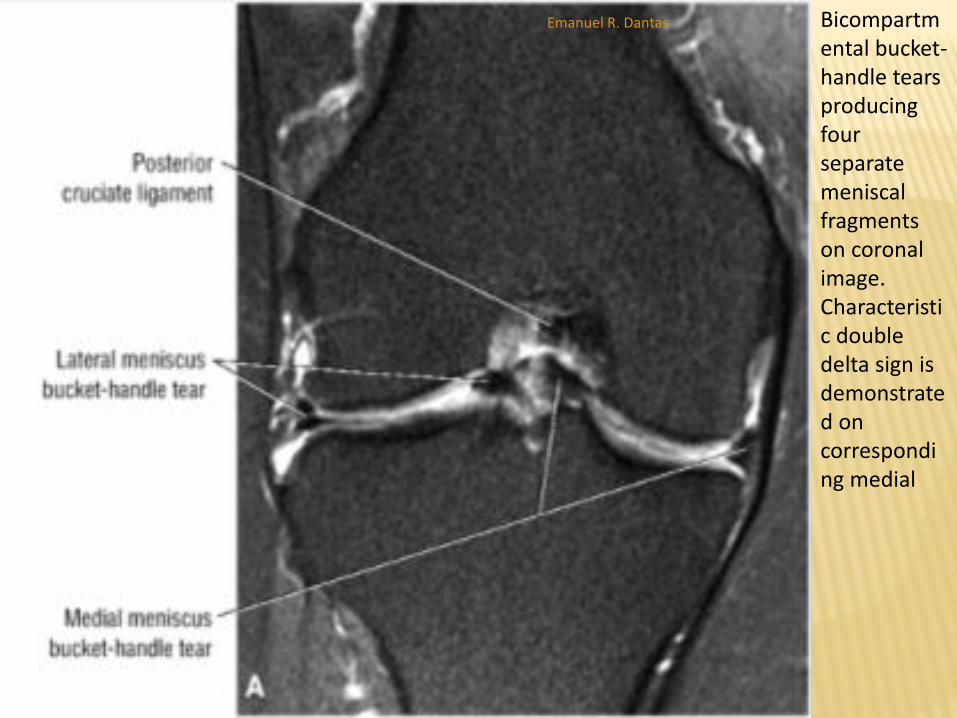
Bicompartmental bucket-handle tears producing four separate meniscal fragments on coronal image. Characteristic double delta sign is demonstrated on corresponding medial
Emanuel R. Dantas

(B) and lateral (C) compartment sagittal images.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND
TEARS
Lateral meniscus bucket-handle tears
The lateral meniscus may also be the site of bucket-handle tears in
which the body of the lateral meniscus is displaced into the intercondylar
notch.
In lateral meniscus tears there may be greater anterior displacement of
posterior horn tissue than is seen in medial bucket-handle tears.
As with medial meniscus bucket-handle tears, the native anterior horn
fragments usually have a blunted free edge, whereas the more
posteriorly located (relative to the anterior horn) flipped or displaced
fragment may be mistaken for the normal anterior horn segment.
The proximity of a lateral meniscus fragment to the ACL should be
carefully evaluated on both coronal and sagittal planes to avoid
underdiagnosis.
Emanuel R. Dantas
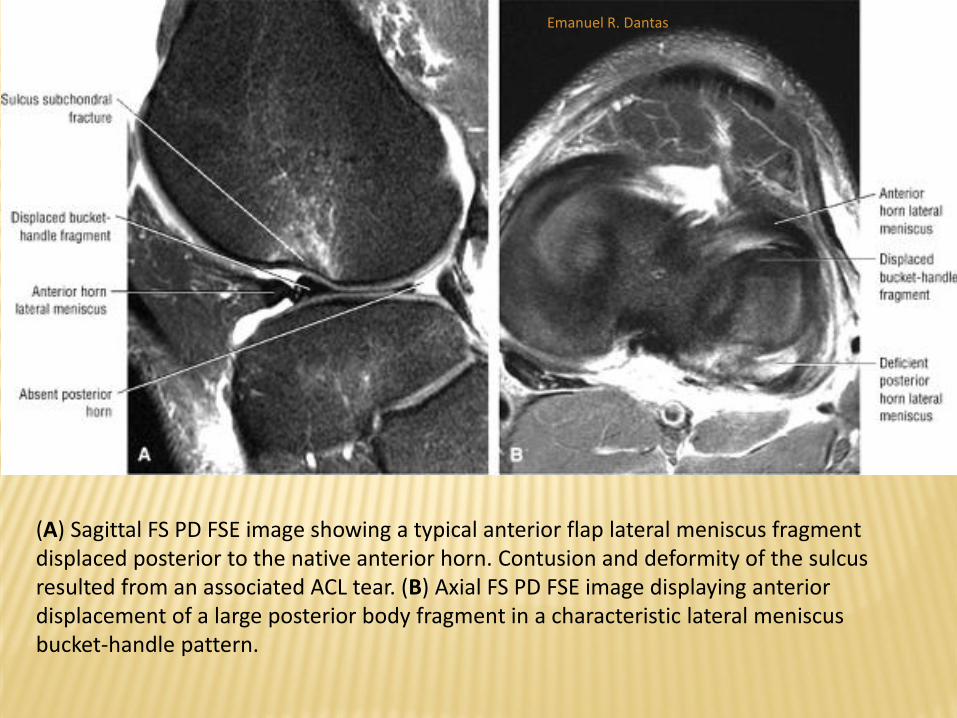
(A) Sagittal FS PD FSE image showing a typical anterior flap lateral meniscus fragment displaced posterior to the native anterior horn. Contusion and deformity of the sulcus resulted from an associated ACL tear. (B) Axial FS PD FSE image displaying anterior displacement of a large posterior body fragment in a characteristic lateral meniscus bucket-handle pattern.
Emanuel R. Dantas
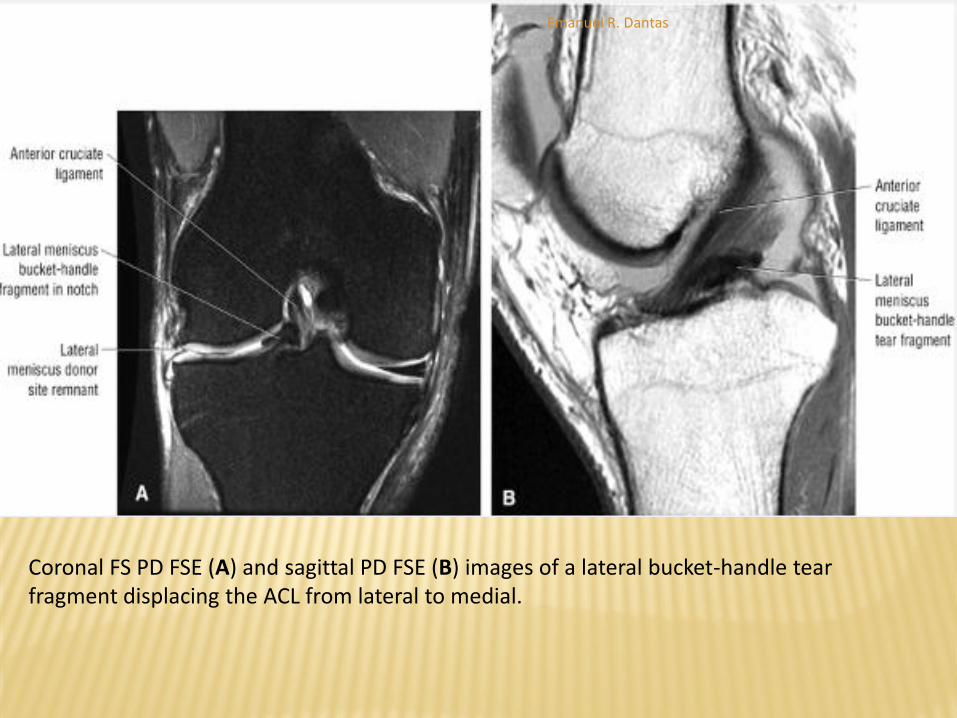
Coronal FS PD FSE (A) and sagittal PD FSE (B) images of a lateral bucket-handle tear fragment displacing the ACL from lateral to medial.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Radial or Transverse Tears - Pearls and Pitfalls
There are three subtypes of classic radial tears (more common in lateral meniscus):
Anterior horn-body junction
Body
Posterior horn-body junction
Root tears are more common in the posterior horn of the medial meniscus.
Classic radial tears are commonly associated with horizontal tears in the lateral meniscus and flap tears in the medial meniscus.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Radial or Transverse Tears
MR findings in classic radial tears include:
(1) a blunted anterior horn and elongated posterior horn body
segment;
(2) a blunted posterior horn in association with an elongated anterior
horn body segment; or
(3) free edge increased signal intensity or blunting restricted to the
middle third of the meniscus that does not involve blunting of the
anterior or posterior horns or elongation of body segment.
Root tears are defined by abrupt loss or blunting of posterior
horn meniscal tissue on posterior coronal images adjacent to
the root meniscal insertion.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Radial or Transverse Tears
Radial or transverse tears are defined as vertical tears perpendicular to the free edge of the meniscus and are subdivided into classic radial tears and root tears.
Classic radial tears are further subdivided by location within the lateral meniscus.
Both classic and root tears may involve either the medial or lateral meniscus.
Classic radial tears, however, are more common in the lateral meniscus.
Root tears are more frequently observed involving the posterior horn or the medial meniscus.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Classic radial tears
There are three recognized locations of classic radial tears.
The most common classic radial tear involves the anterior horn-body junction of the free edge of the lateral meniscus.
Less commonly, classic radial tears present along the middle third of the meniscus (appearing as free edge blunting) or at the posterior horn-body junction of the meniscus.
Emanuel R. Dantas

(A) Free edge radial tear at the junction of the anterior horn and body of the lateral meniscus. (B) Corresponding sagittal section produces the characteristic blunted foreshortened anterior horn and elongated components of the meniscal body and posterior horn.
Emanuel R. Dantas
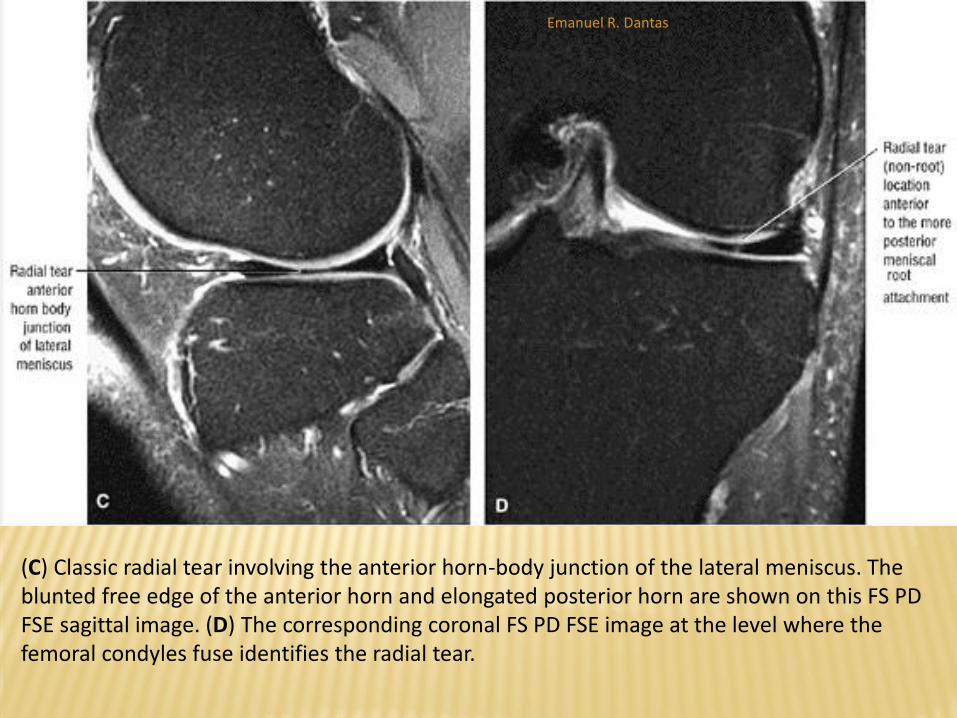
(C) Classic radial tear involving the anterior horn-body junction of the lateral meniscus. The blunted free edge of the anterior horn and elongated posterior horn are shown on this FS PD FSE sagittal image. (D) The corresponding coronal FS PD FSE image at the level where the femoral condyles fuse identifies the radial tear.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Classic radial tears Because the sagittal plane sections the meniscus perpendicular to the free
edge orientation of the tear, the only evidence of a radial tear on sagittal images may be increased signal intensity (focal grade 3) on one or two peripheral sections.
On these images, the classic or common radial tear is characterized by blunting of both the anterior horn-body junction and blunting and elongation of the posterior horn body segment.
Because the tear plane is in the anterior third of the meniscus, the posterior horn body segment is seen as exaggerated or elongated, a finding characteristic of radial tears.
The more closely the plane of section approximates the free edge of the meniscus, the more prominent the blunted anterior horn segment.
On sagittal images of a radial tear located at the junction of the posterior horn and body, the anterior horn body segment is elongated or exaggerated in anterior to posterior length.
Emanuel R. Dantas
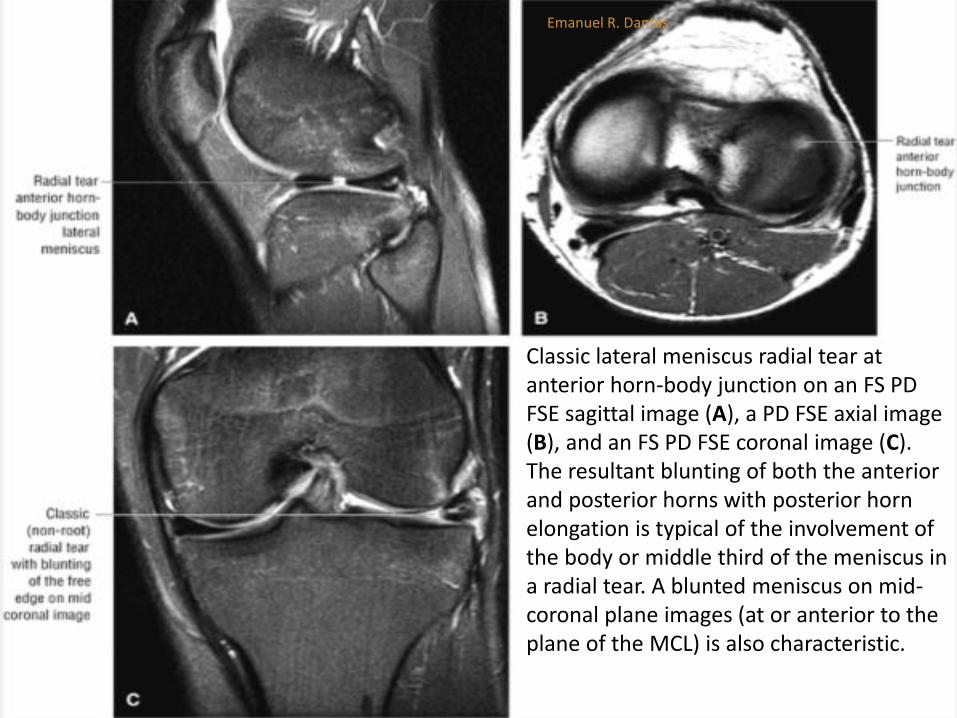
Classic lateral meniscus radial tear at anterior horn-body junction on an FS PD FSE sagittal image (A), a PD FSE axial image (B), and an FS PD FSE coronal image (C). The resultant blunting of both the anterior and posterior horns with posterior horn elongation is typical of the involvement of the body or middle third of the meniscus in a radial tear. A blunted meniscus on mid-coronal plane images (at or anterior to the plane of the MCL) is also characteristic.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Root tears
The root tear subtype of radial tear can occur in either the medial or lateral meniscus, although it is more common in the medial meniscus, where it is thought to represent a degenerative tear.
The meniscotibial attachment of the posterior horn is a typical location for this tear type, as is the junction of the meniscus-root interface .
Displacement of the root tear produces a relative absence of posterior horn meniscal fibrocartilage on sagittal images.
Emanuel R. Dantas

(A) Medial meniscal root tear avulsion occurring directly from the osseous tibial attachment site. (B) Arthroscopic view of medial meniscus root avulsion.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
• Root tears
Diffuse increased signal intensity seen on one or two sagittal images of these displaced root type radial tears represents the so-called ghost meniscus.
Corresponding posterior coronal images demonstrate abrupt blunting of the normal meniscotibial attachment and foreshortening of the meniscus toward the posterior aspect of the intercondylar notch.
As with bucket-handle tears, lateral meniscus root tears are associated with ACL tears.
Displacement of these root tears may result in flipping of meniscal fragments into the posterior aspect of the intercondylar notch. These flipped meniscal fragments are best appreciated on posterior coronal images.
Large radial tears (>50% of the meniscal width) or root tears are also associated with significant (>3 mm) meniscal extrusion relative to the tibial plateau.
Emanuel R. Dantas

Displaced posterior horn root tear of the medial meniscus on axial illustration (A) and FS PD FSE axial images (B). Corresponding “ghost” meniscus is demonstrated on a sagittal illustration
Emanuel R. Dantas

C) and FS PD FSE sagittal image (D) through fluid-filled tear gap. Note residual meniscal tissue still attached to the meniscotibial attachment on coronal FS PD FSE image (E).
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Flap Tears - Pearls and Pitfalls
Flap tears usually result from extensions of radial or horizontal
cleavage tears and represent the most common clinical tear type.
Vertical grade 3 signal intensity in the inner one third to one half
of the meniscus and relative deficiency of the inferior surface of
the meniscus are the most common findings in flap tears.
Flap tears may demonstrate meniscal extrusion into the coronary
recess of a meniscotibial ligament on coronal images.
Reactive tibial plateau marrow edema is associated with these
extrusions.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Flap Tears - Pearls and Pitfalls
Oblique meniscal signal intensity on sagittal images
does not necessarily equate with flap tear
morphology (see criteria for for flap tear diagnosis).
Flap tears, large radial tears (including root tears),
and complex tears are associated with major (>3
mm) meniscal extrusion.
Displaced flap tears of the posterior horn of the
lateral meniscus are associated with tears.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Flap Tears A flap tear, which represents a composite of a
longitudinal and a radial tear, starts on the free edge of the meniscus and curves obliquely into the meniscal fibrocartilage .
These tears may also be referred to as oblique tears.
Flap tears represent the most common meniscal tear type and are frequently associated with oblique signal intensity on sagittal plane meniscal cross-section (e.g., grade 3 signal intensity commonly extending to the inferior surface of the posterior horn of the medial meniscus).
Emanuel R. Dantas

(A) Illustration depicting a flap tear at arthroscopy. (B) Vertical inner-third tearing produces an anteriorly displaced meniscal fragment, creating the flap identified at arthroscopy. (C) Blunting of the free edge of the meniscus is shown on a sagittal FS PD FSE image. Corresponding coronal plane diagnosis of a flap tear usually requires evidence of meniscal displacement into the meniscofemoral or meniscotibial recess.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND
TEARS
Flap Tears Flap tears may display either a primary vertical or horizontal tear
pattern.
Identification of obliquely oriented grade 3 meniscal signal on sagittal images does not necessarily indicate the presence of a flap or oblique tear, since longitudinal tears may also appear as an oblique course of grade 3 signal intensity extending to the meniscal surface.
Unlike longitudinal tears, flap tears involve the inner one third to one half of the meniscus, with superior or inferior leaf extension creating the mobile limb or flap of fibrocartilage.
In contrast, longitudinal tears are more likely to involve the peripheral third of the meniscus, where there is a greater concentration of circumferential fibers.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Flap Tears
The criteria for diagnosis of a flap tear based on sagittal images include:
A vertical tear encompassing the inner third of the meniscus, either coapted or non-coapted
Relative deficiency of the inner third of the inferior meniscal surface with associated blunting of the remaining inferior leaf
A blunted free edge of the meniscus with displaced meniscal tissue inferior to the periphery of the meniscus
A change in the slope of the superior surface of the meniscus, indicating a change in the direction of the tear that creates the flap.
Emanuel R. Dantas

Coapted flap tear with vertical tear morphology involving the inner third of the medial meniscus as seen on a sagittal color illustration with superior and cross-sectional view of the meniscus and flap tear (A) and a sagittal FS PD FSE image (B).
Emanuel R. Dantas

Coapted or nondisplaced flap tears of the posterior horn medial meniscus. (A) Inner margin vertical grade 3 signal intensity is identified in the sagittal plane. (B) Direct visualization of flap morphology is demonstrated on this axial image.
Emanuel R. Dantas
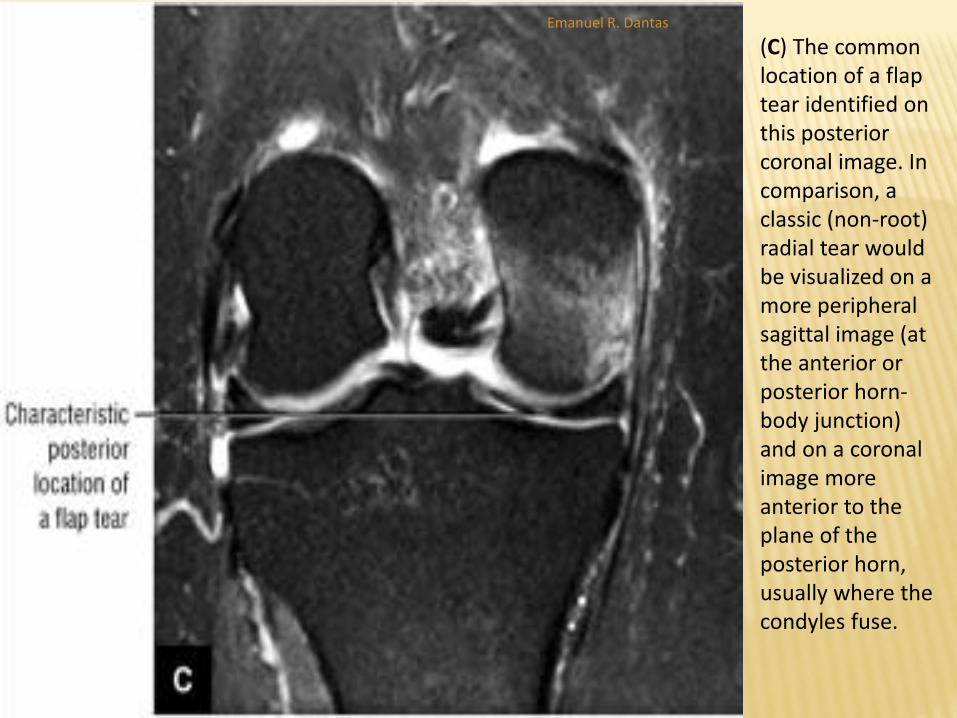
(C) The common location of a flap tear identified on this posterior coronal image. In comparison, a classic (non-root) radial tear would be visualized on a more peripheral sagittal image (at the anterior or posterior horn-body junction) and on a coronal image more anterior to the plane of the posterior horn, usually where the condyles fuse.
Emanuel R. Dantas
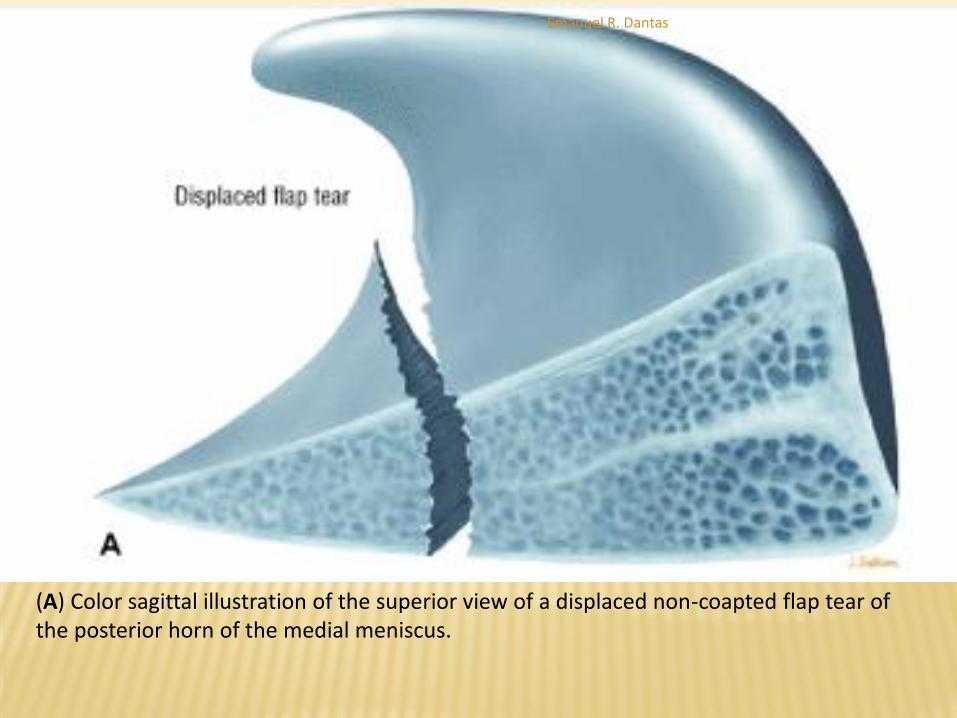
(A) Color sagittal illustration of the superior view of a displaced non-coapted flap tear of the posterior horn of the medial meniscus.
Emanuel R. Dantas
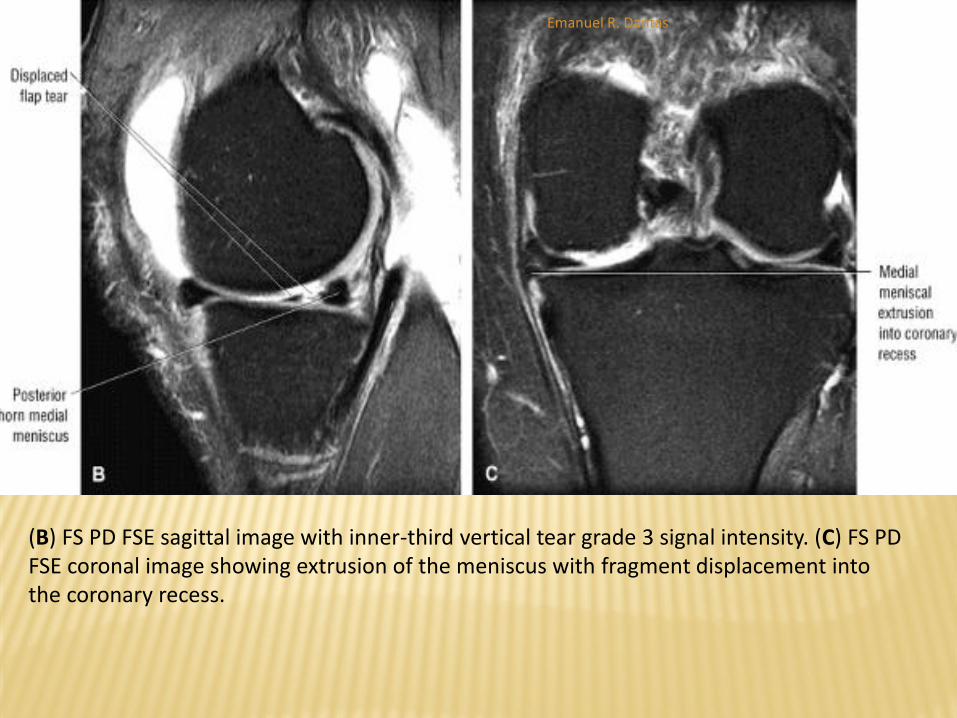
(B) FS PD FSE sagittal image with inner-third vertical tear grade 3 signal intensity. (C) FS PD FSE coronal image showing extrusion of the meniscus with fragment displacement into the coronary recess.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Flap Tears
In addition, extrusion of a portion of the meniscus
into the coronary recess below the joint line is seen
on coronal images.
The displaced flap in the coronary recess is also
visualized on peripheral sagittal images with
hypointense meniscal tissue below the level of the
joint line or tibial plateau deep to the MCL on
peripheral medial images.
Emanuel R. Dantas

Separation of displaced medial meniscus flap fragment with inferior displacement into coronary recess.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Flap Tears
Although flap tears most commonly involve the posterior horn of the medial meniscus, they may also be seen in the lateral meniscus.
As the mobile flap rotates it may produce either double-decker or stacked leaflet meniscal morphology, or it may extend into the meniscofemoral or meniscotibial recess.
When associated with ACL injuries, complex flap tears may displace posteriorly into the intercondylar notch.
Complex flap displacement and rotation of the posterior horn of the lateral meniscus may be mistaken for ACL ligamentous tissue (double ACL sign).
Emanuel R. Dantas
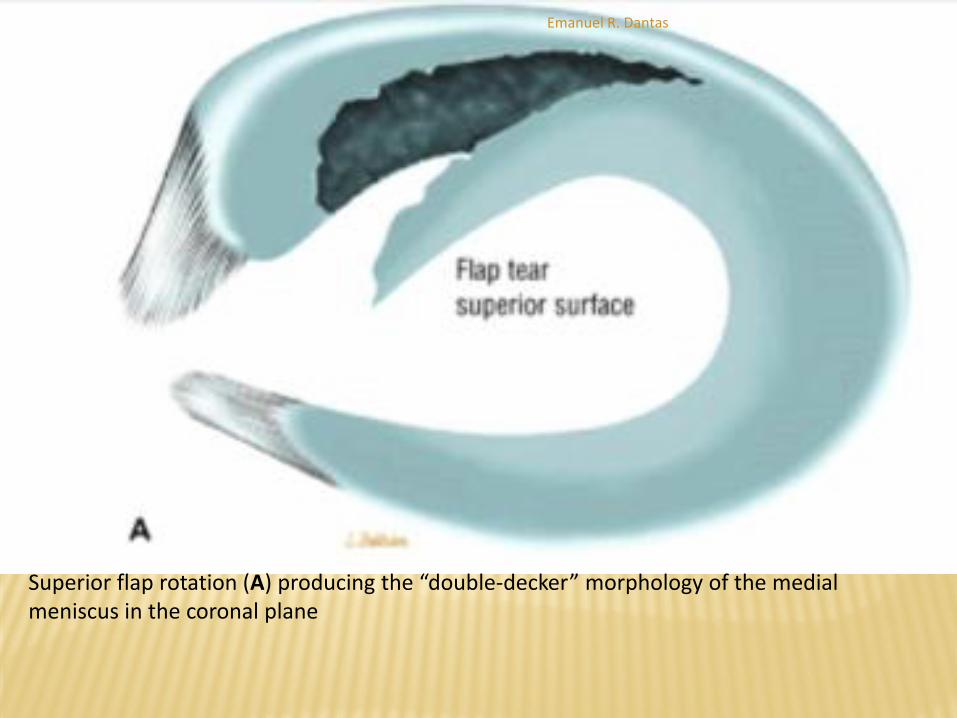
Superior flap rotation (A) producing the “double-decker” morphology of the medial meniscus in the coronal plane
Emanuel R. Dantas
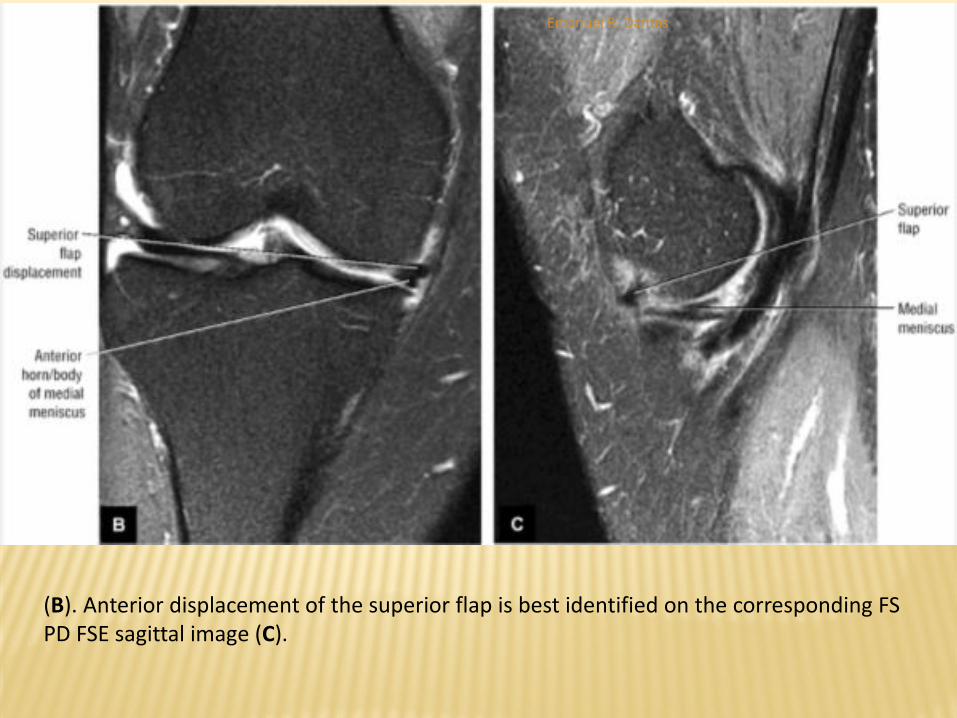
(B). Anterior displacement of the superior flap is best identified on the corresponding FS PD FSE sagittal image (C).
Emanuel R. Dantas
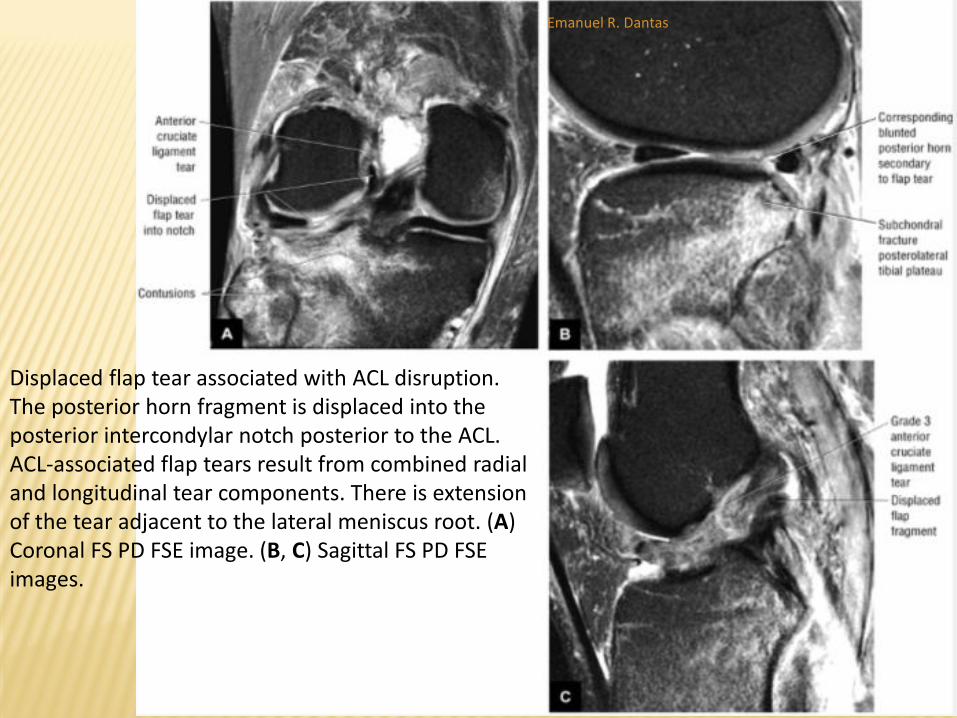
Displaced flap tear associated with ACL disruption. The posterior horn fragment is displaced into the posterior intercondylar notch posterior to the ACL. ACL-associated flap tears result from combined radial and longitudinal tear components. There is extension of the tear adjacent to the lateral meniscus root. (A) Coronal FS PD FSE image. (B, C) Sagittal FS PD FSE images.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Discoid Meniscus - Pearls and Pitfalls
Incomplete discoid menisci can be differentiated from
complete discoid types by the degree of discoid morphology.
No anterior or posterior horn equivalents are identified in the
complete discoid meniscus (type A).
Prominent or cavitary grade 2 signal intensity in a discoid
meniscus may be associated with positive clinical signs and
symptoms related to the lateral compartment.
The popping or snapping knee syndrome is associated with
the Wrisberg variant (absence of the posterior coronary
ligament).
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Discoid Meniscus
A discoid meniscus is a dysplastic meniscus that has lost its normal or semilunar shape and has a broad disc-like configuration.
Lateral discoid menisci are more common than medial discoid menisci, and the degree of enlargement varies from mild hypertrophy to a bulky slab of fibrocartilage
The incidence of discoid menisci is reported to be 1.4% to 15.5%.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Discoid Meniscus
Watanabe's classification groups discoid menisci into
incomplete, complete, and Wrisberg-ligament type (Wrisberg
variant).
Complete and incomplete refer to the degree or extent to
which the meniscus demonstrates discoid morphology with
an intact posterolateral meniscotibial ligament.
A complete discoid meniscus extends to the intercondylar
notch.
Discoid menisci are considered congenital deformities and
are frequently bilateral.
Emanuel R. Dantas

Incomplete discoid lateral meniscus illustrated on superior view (A) and shown on corresponding axial
Emanuel R. Dantas
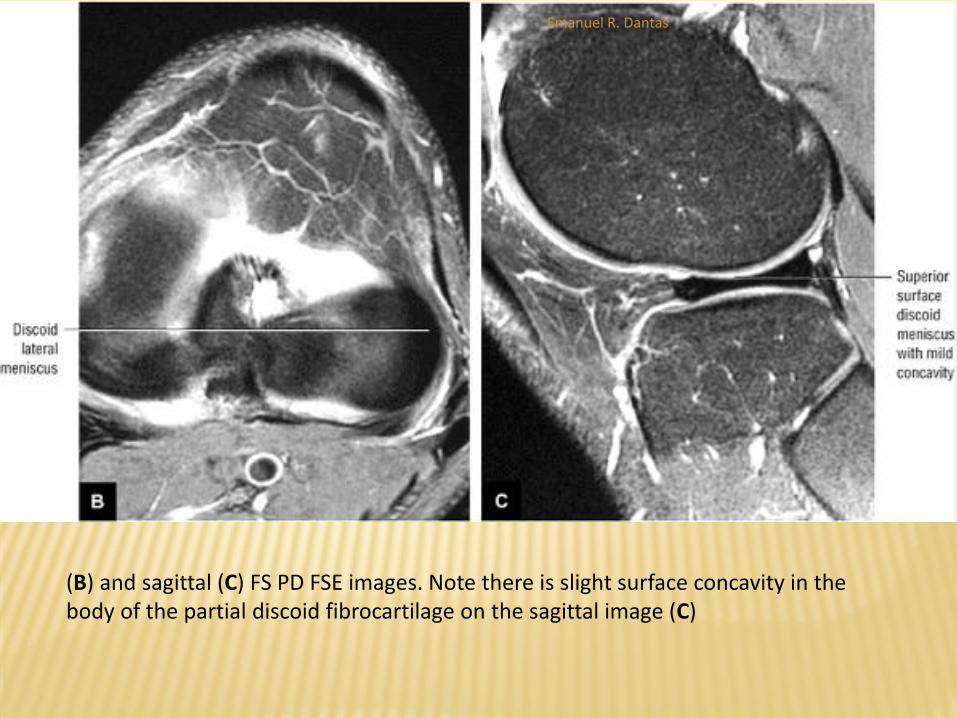
(B) and sagittal (C) FS PD FSE images. Note there is slight surface concavity in the body of the partial discoid fibrocartilage on the sagittal image (C)
Emanuel R. Dantas
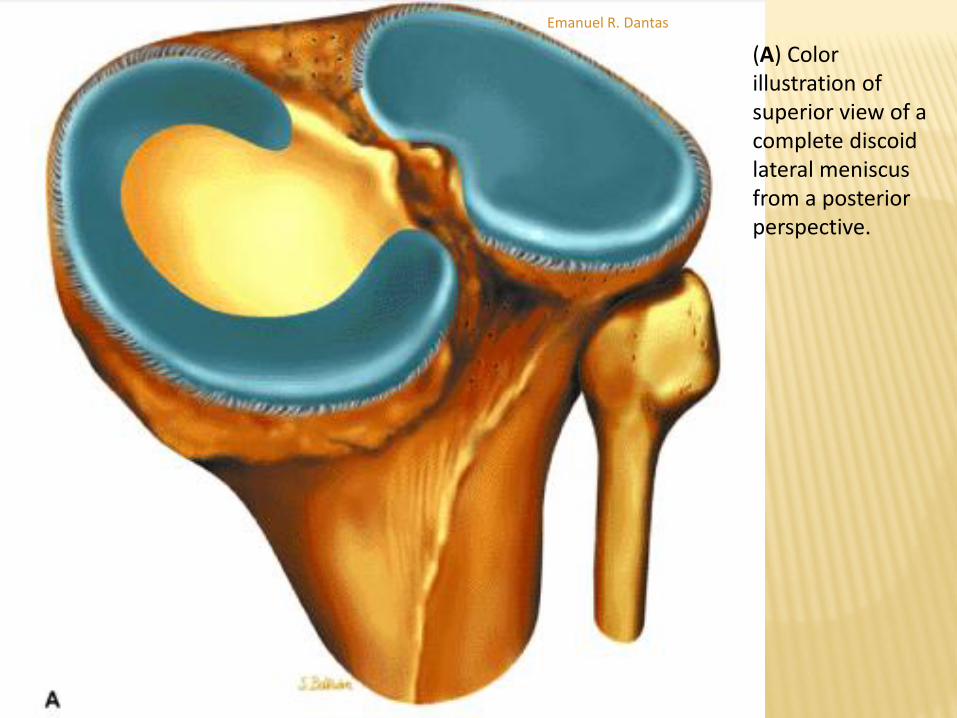
(A) Color illustration of superior view of a complete discoid lateral meniscus from a posterior perspective.
Emanuel R. Dantas
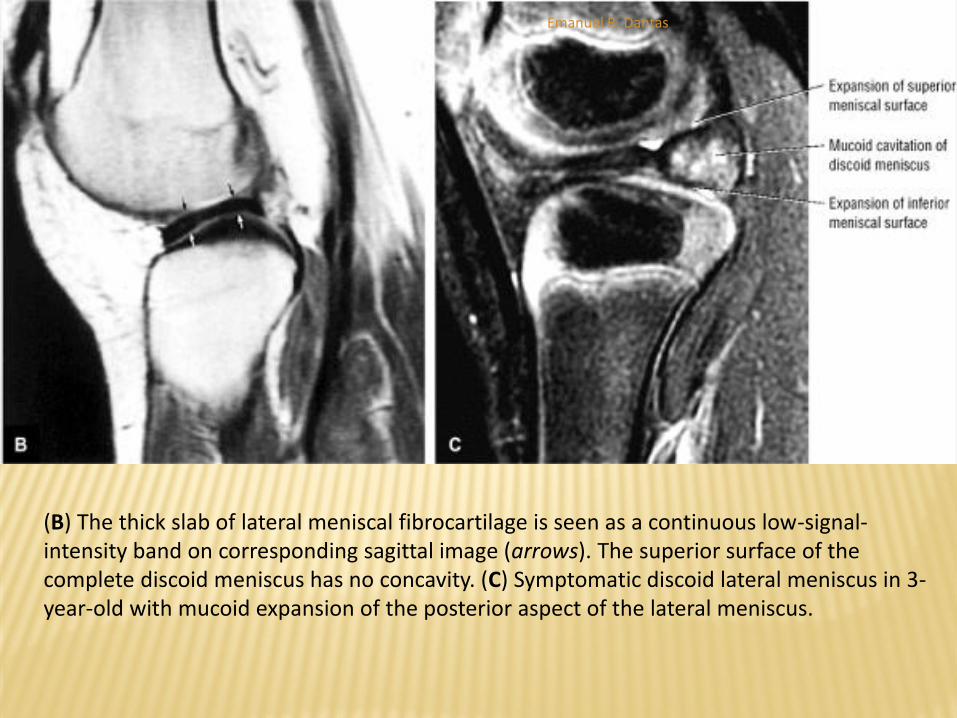
(B) The thick slab of lateral meniscal fibrocartilage is seen as a continuous low-signal-intensity band on corresponding sagittal image (arrows). The superior surface of the complete discoid meniscus has no concavity. (C) Symptomatic discoid lateral meniscus in 3-year-old with mucoid expansion of the posterior aspect of the lateral meniscus.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Discoid Meniscus
The differential diagnosis of a discoid meniscus includes any condition that presents as a “snapping knee” on physical examination (a snapping sound during knee flexion and extension).
The following conditions are included in the differential: Patellofemoral joint subluxation or dislocation
Meniscal cysts
Congenital subluxation of the tibiofemoral joint
Subluxation or dislocation, or both, of the proximal tibiofibular joint
Snapping of the tendons about the knee on an osteophyte or roughened surface
A displaced flap tear or bucket-handle tear
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Discoid Meniscus
Imaging findings in the evaluation of discoid menisci include the following:
Plain-film radiographs (although usually of limited value) may show widening of the involved compartment (lateral joint space), a hypoplastic lateral femoral condyle, a high fibular head, chondromalacia, cupping of the lateral tibial plateau, and a squared-off lateral femoral condyle.
Arthrography demonstrates an elongated and enlarged meniscus that extends toward the intercondylar notch.
On sagittal MR images, using a 4-mm slice thickness, a discoid meniscus exhibits a continuous or bowtie appearance on three or more consecutive images.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Discoid Meniscus
Imaging findings in the evaluation of discoid menisci include the following:
The increased inferior-to-superior dimensions of the meniscus can be appreciated on both coronal and sagittal images. A discoid meniscus may be as much as 2 mm higher than the opposite meniscus.112
Coronal images show the extension of the discoid meniscus apex toward or into the intercondylar notch.
In a complete discoid meniscus, meniscal fibrocartilage without distinct anterior and posterior horns is usually interposed between the femoral condyle and the tibial plateau on every sagittal image through the involved compartment.
In the more common incomplete discoid type of meniscus, the meniscus does not extend into the intercondylar notch on coronal images.
Emanuel R. Dantas

A complete discoid meniscus (small arrows) interposed between the lateral femoral condyle and tibial plateau extending to the intercondylar notch on FS PD-weighted FSE coronal images. An intact meniscotibial ligament (A, curved arrow) and Wrisberg-ligament (B, W) are shown
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Discoid Meniscus
Imaging findings in the evaluation of discoid menisci include the following:
In the presence of an effusion, the enlarged meniscus is outlined with high-signal-intensity fluid on FS PD FSE, T2*-, or STIR-weighted images.
Axial images demonstrate the circumferential morphology of both incomplete and complete discoid menisci. Grade 2 signal intensity and discoid menisci may correlate with intrameniscal cavitations or cysts, and many orthopaedic surgeons recommend meniscectomy for a symptomatic discoid meniscus, even without grade 3 signal intensity. These menisci usually demonstrate a prominent and thickened grade 2 signal intensity that may correlate with an intrasubstance cleavage tear.
Emanuel R. Dantas
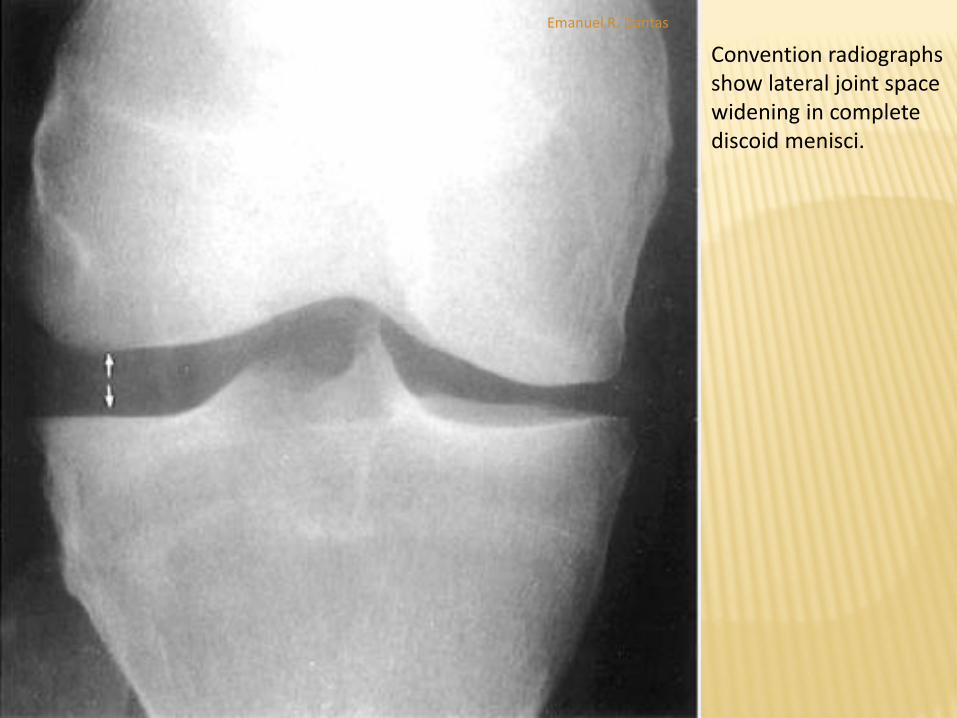
Convention radiographs show lateral joint space widening in complete discoid menisci.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings -
Pearls and Pitfalls
Attenuation of grade 3 signal intensity extension to an
articular surface is associated with a closed meniscal tear.
External rotation of the knee may accentuate the course of
the meniscofemoral ligaments. The ligament of Wrisberg is
often mistaken for a peripheral tear of the posterior horn of
the lateral meniscus.
Meniscal flounce does not indicate the existence of or
increased association with a meniscal tear.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings - Transverse
Ligament
The transverse ligament of the knee, which connects the anterior horns
of the medial and lateral meniscus, can simulate an oblique tear
adjacent to the anterior horn of the lateral meniscus.
On sagittal or axial images, the transverse ligament can be identified
coursing between the tibial attachment of the ACL and Hoffa's
infrapatellar fat pad to its insertion on the anterior superior aspect of the
anterior horn of the medial meniscus.
In the presence of a joint effusion, increased signal intensity may be
present in the interface between the transverse ligament and the
anterior horn of the lateral meniscus on FS PD FSE images.
Emanuel R. Dantas
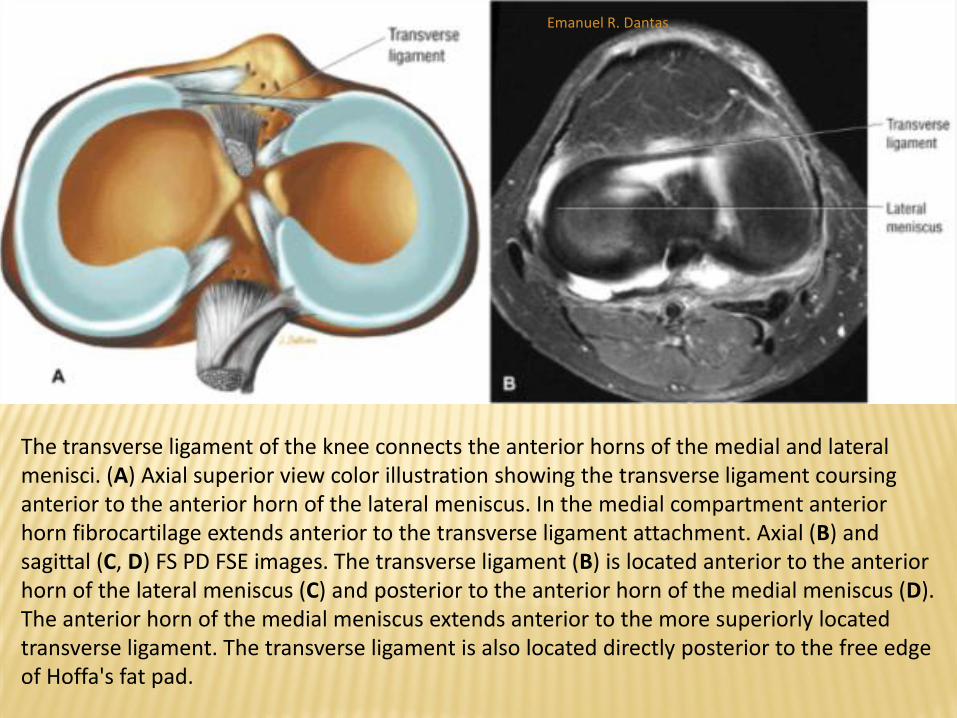
The transverse ligament of the knee connects the anterior horns of the medial and lateral menisci. (A) Axial superior view color illustration showing the transverse ligament coursing anterior to the anterior horn of the lateral meniscus. In the medial compartment anterior horn fibrocartilage extends anterior to the transverse ligament attachment. Axial (B) and sagittal (C, D) FS PD FSE images. The transverse ligament (B) is located anterior to the anterior horn of the lateral meniscus (C) and posterior to the anterior horn of the medial meniscus (D). The anterior horn of the medial meniscus extends anterior to the more superiorly located transverse ligament. The transverse ligament is also located directly posterior to the free edge of Hoffa's fat pad.
Emanuel R. Dantas

The transverse ligament of the knee connects the anterior horns of the medial and lateral menisci. (A) Axial superior view color illustration showing the transverse ligament coursing anterior to the anterior horn of the lateral meniscus. In the medial compartment anterior horn fibrocartilage extends anterior to the transverse ligament attachment. Axial (B) and sagittal (C, D) FS PD FSE images. The transverse ligament (B) is located anterior to the anterior horn of the lateral meniscus (C) and posterior to the anterior horn of the medial meniscus (D). The anterior horn of the medial meniscus extends anterior to the more superiorly located transverse ligament. The transverse ligament is also located directly posterior to the free edge of Hoffa's fat pad
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings -
Transverse Ligament
Axial images demonstrate the course of the transverse
ligament as a low-signal-intensity band traversing Hoffa's
infrapatellar fat pad.
On serial sagittal images, the round transverse ligament may
be traced from the anterior horn of the lateral meniscus to
the anterior horn of the medial meniscus.
The central attachment of the anterior horn of the medial
meniscus is located anterior to the transverse ligament when
viewed in the sagittal plane
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings - Anterior Horn of the Lateral Meniscus
Isolated tears of the anterior horn of the lateral meniscus can be easily differentiated from transverse ligament pseudo-tears and are relatively uncommon compared to other meniscal tear locations.
The central anterior ligamentous attachment of the anterior horn of the lateral meniscus itself may be mistaken for a meniscal tear. This attachment, which is rhomboid, is normally directed obliquely upward on sagittal images and frequently contains increased internal signal intensity.
In this location the increased signal intensity is sometimes referred to as “speckled.” It may be visualized on one or two sagittal images adjacent to the intercondylar notch and occurs near the origin of the transverse ligament.
Emanuel R. Dantas

(A) Sagittal FS PD FSE image shows the speckled pattern of the normal central rhomboid attachment of the anterior horn of the lateral meniscus. (B) T1-weighted axial image of the central rhomboid attachment (small arrows) of the anterior horn (AH) of the lateral meniscus.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings - Fibrillation
Fibrillation or fraying of the concave free edge of the meniscus facing the
intercondylar notch is seen as increased signal intensity restricted to the
apex of the meniscus in the presence of normal meniscal morphology.
If, however, there is abnormal morphology (truncation or foreshortening
of the meniscus), a meniscal tear (radial or flap tear) is likely.
FS PD-weighted FSE images are useful in defining the meniscal outline or
morphology but are less sensitive to the detection of intrameniscal signal
intensity.
It is sometimes difficult to differentiate between the MR characteristics of
fraying and tearing of the meniscus.
Emanuel R. Dantas
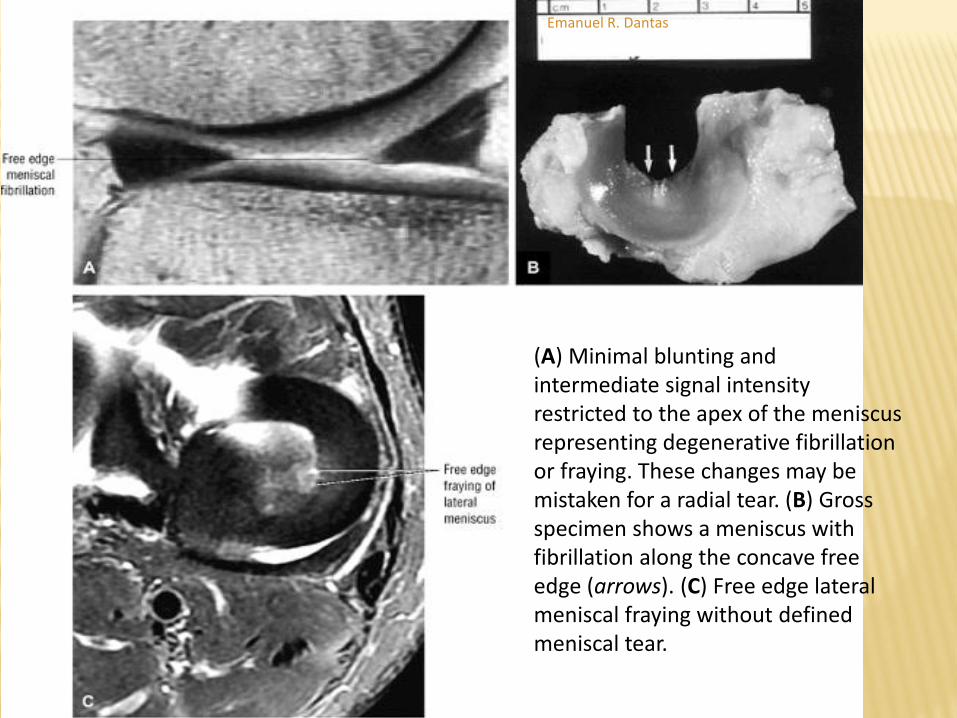
(A) Minimal blunting and intermediate signal intensity restricted to the apex of the meniscus representing degenerative fibrillation or fraying. These changes may be mistaken for a radial tear. (B) Gross specimen shows a meniscus with fibrillation along the concave free edge (arrows). (C) Free edge lateral meniscal fraying without defined meniscal tear.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings - Popliteus Tendon
In the posterior horn of the lateral meniscus, the popliteus tendon sheath may be mistaken for grade 3 signal intensity and can be falsely interpreted as a tear.
The popliteus tendon sheath is intermediate in signal intensity on T1- and FS PD- or T2-weighted images and courses in an oblique, anterosuperior-to-posteroinferior direction, anterior to the low-signal-intensity popliteus tendon.
In the presence of a joint effusion, fluid in the popliteus sheath demonstrates bright signal intensity on T2- or T2*-weighted images.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings -
Popliteus Tendon
In addition, the superior and inferior fascicles of the posterior
horn of the lateral meniscus are best displayed on T2-weighted
images (including FS PD-weighted FSE or T2*-weighted
sequences) in the presence of a joint effusion.
A fascicle tear should not be confused with the normal superior
and inferior meniscocapsular defects, which allow passage of the
popliteus tendon through the popliteus hiatus.
In the sagittal plane, the most lateral image through the popliteus
tendon displays the anatomy of the inferior fascicle, with normal
deficiency of the superior fascicle.
Emanuel R. Dantas

Coronal (A) and sagittal (B) images at the level of the superior popliteomeniscal ligament or fascicle deficiency on a lateral peripheral image. (C) Both inferior and superior fascicles are visualized between the lateral and medial sagittal sections through the hiatus. (D) A more medial section through the hiatus showing the normal inferior popliteomeniscal ligament (fascicle) deficiency.
Emanuel R. Dantas

Coronal (A) and sagittal (B) images at the level of the superior popliteomeniscal ligament or fascicle deficiency on a lateral peripheral image. (C) Both inferior and superior fascicles are visualized between the lateral and medial sagittal sections through the hiatus. (D) A more medial section through the hiatus showing the normal inferior popliteomeniscal ligament (fascicle) deficiency.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings - Meniscofemoral Ligaments
Laterally, the meniscofemoral ligament consists of the ligament of Humphrey, which extends anterior to the PCL, and a posterior branch of the ligament of Wrisberg, seen posterior to the PCL.
The meniscofemoral ligament most commonly has direct attachment to the lateral meniscus and is obliquely oriented to its insertion on the medial femoral condyle. The posterior branch of the meniscofemoral ligament, the ligament of Wrisberg, is the larger of the two branches and may appear to be half the cross-sectional diameter of the PCL.
Emanuel R. Dantas

The ligaments of Humphrey and Wrisberg attach the lateral meniscal posterior horn to the medial femoral condyle. Partial insertion of the popliteus tendon into the posterolateral aspect of the lateral meniscus occurs through the superior and inferior fasciculus forming the popliteal hiatus.
Emanuel R. Dantas
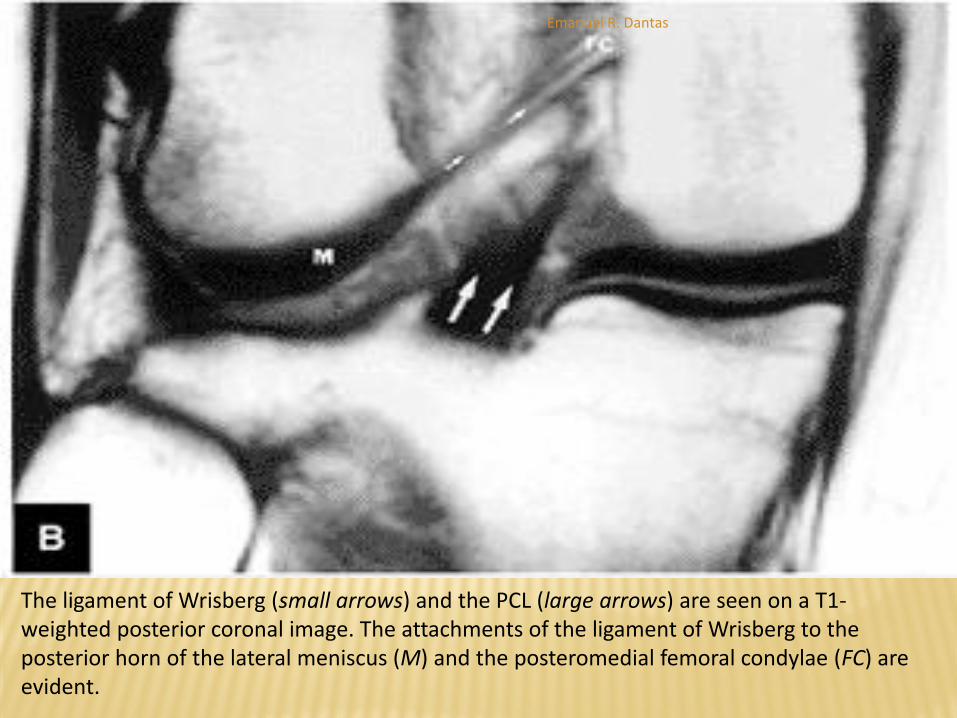
The ligament of Wrisberg (small arrows) and the PCL (large arrows) are seen on a T1-weighted posterior coronal image. The attachments of the ligament of Wrisberg to the posterior horn of the lateral meniscus (M) and the posteromedial femoral condylae (FC) are evident.
Emanuel R. Dantas

MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings -
Meniscofemoral Ligaments
The ligament of Humphrey can be best seen on sagittal images,
whereas the ligament of Wrisberg is best shown on posterior coronal
images. The ligament of Humphrey can, however, be identified on
coronal images.
Meniscal insertion of the meniscofemoral ligament may mimic the
appearance of a vertical tear in the posterior horn of the lateral
meniscus.
This pseudo-tear, the result of fat and or fluid interposed between the
meniscus attachment and the meniscofemoral ligament, can be seen
extending obliquely from the superior meniscal surface and is directed
posteriorly and inferiorly toward the inferior meniscal surface
Emanuel R. Dantas
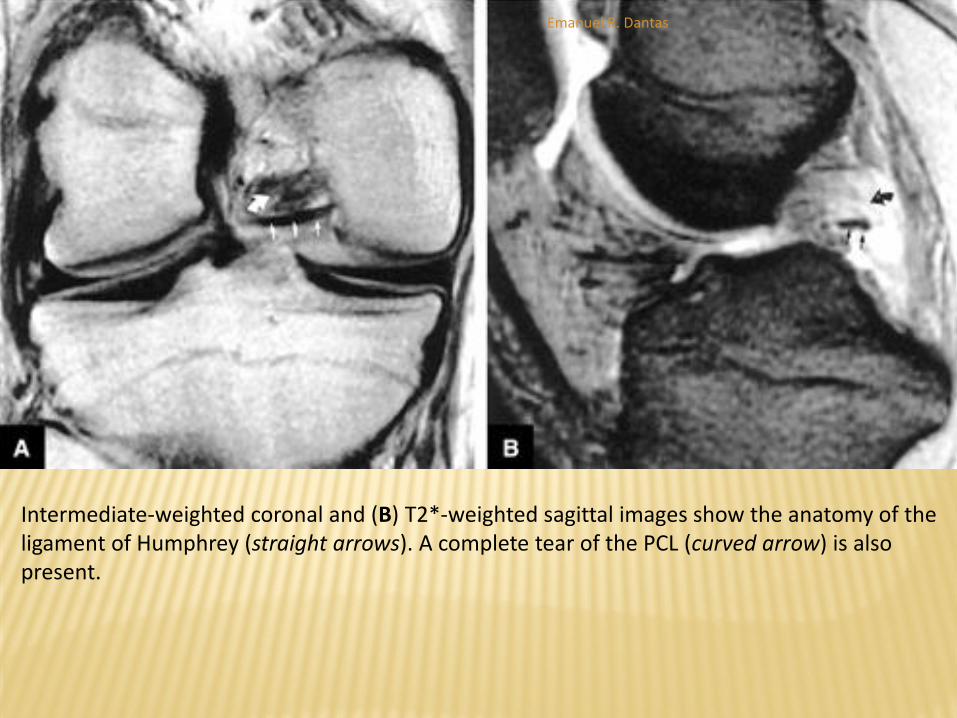
Intermediate-weighted coronal and (B) T2*-weighted sagittal images show the anatomy of the ligament of Humphrey (straight arrows). A complete tear of the PCL (curved arrow) is also present.
Emanuel R. Dantas

Sagittal FS PD FSE images of the normal meniscofemoral ligaments without a meniscal tear. (A) The ligaments of Humphrey and Wrisberg can be seen posterior to the posterior horn of the lateral meniscus. (B) On next medial sequential image through the lateral compartment, the ligament of Wrisberg courses superiorly to pass posterior to the PCL within the intercondylar notch. The hyperintense interface between the lateral meniscus and meniscofemoral ligament is normal, even though a fracture of the posterior lateral tibial plateau can be seen on this image.
Emanuel R. Dantas
MR OF MENISCAL DEGENERATIONS AND TEARS
Pitfalls in Interpretation of Meniscal Tear Findings -
Pseudohypertrophy of the Anterior Horn (Anterior Flipped
Meniscus)
Complex meniscal tears may present with a unique MR appearance. In
the lateral meniscus, the posterior horn may be absent or truncated, or it
may be displaced or flipped anteriorly, occupying the space adjacent to
the anterior horn, creating pseudohypertrophy of the anterior horn
fibrocartilage.
This pattern is commonly seen in bucket-handle tears of the lateral
meniscus.
The two meniscal horns are separated by an interface of fluid.
The flipped posterior horn tissue is posterior to the anterior horn.
Emanuel R. Dantas
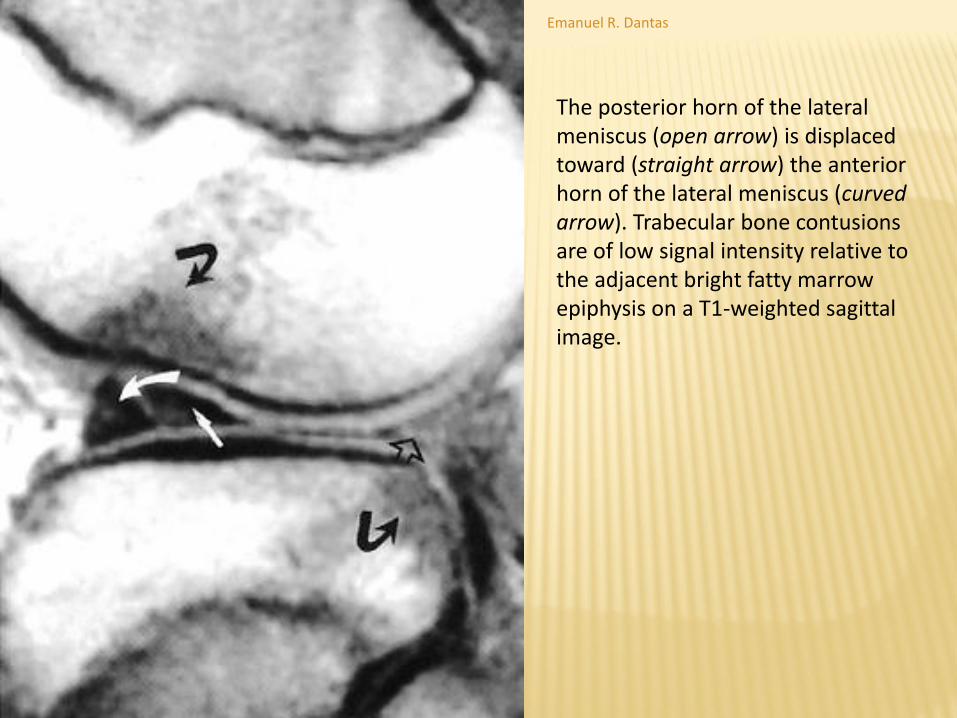
The posterior horn of the lateral meniscus (open arrow) is displaced toward (straight arrow) the anterior horn of the lateral meniscus (curved arrow). Trabecular bone contusions are of low signal intensity relative to the adjacent bright fatty marrow epiphysis on a T1-weighted sagittal image.
Emanuel R. Dantas

MISCELLANEOUS MENISCAL PATHOLOGY
Meniscocapsular Separations - Pearls and Pitfalls:
The meniscocapsular ligaments consist of meniscofemoral and
meniscotibial ligaments and are defined in layer 3 of the knee joint
capsule.
Tears of the proximal MCL are associated with meniscofemoral ligament
injuries.
Fluid interposed between the meniscus and capsular periphery
posterolateral to the superficial MCL and deep MCL represents a form of
meniscocapsular tearing and may be associated with a posterior medial
meniscal corner tear in acute ACL injuries.
Meniscal avulsions involving the meniscotibial attachment occur in both
the medial and lateral meniscus.
Emanuel R. Dantas

MISCELLANEOUS MENISCAL PATHOLOGY
Meniscocapsular Separations
Meniscocapsular separations or tears usually involve
the less mobile medial meniscus.115 The thick medial
third of the joint capsule or medial capsular ligament is
divided into meniscofemoral and meniscotibial
components.
Anteriorly these fibers are separated from the
superficial fibers of the MCL by an interposed bursa
and can best be seen on routine FS PD FSE radial
images through the medial compartment of the knee.
Emanuel R. Dantas

Coronal FS PD FSE image showing the medial meniscofemoral and meniscotibial ligaments proximal and distal, respectively, to the lateral joint line.
Emanuel R. Dantas

Sagittal PD FSE image showing complete meniscocapsular separation at the interface of the posterior horn of the medial meniscus and the peripheral capsular tissue. Hypointense thick capsular tissue should not be mistaken for meniscal fibrocartilage
Emanuel R. Dantas
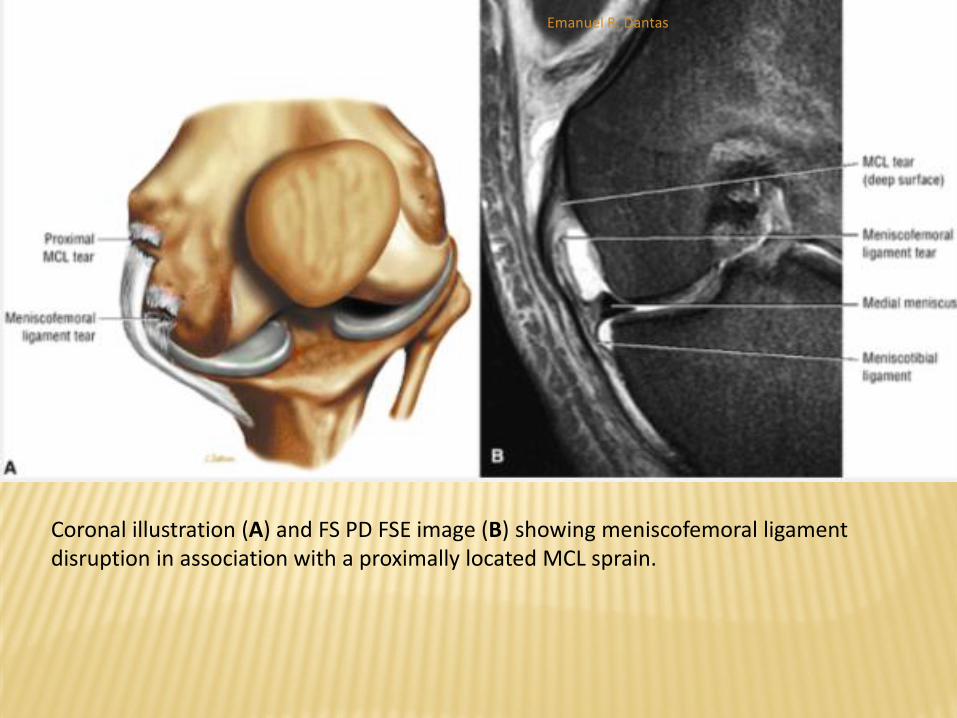
Coronal illustration (A) and FS PD FSE image (B) showing meniscofemoral ligament disruption in association with a proximally located MCL sprain.
Emanuel R. Dantas

MISCELLANEOUS MENISCAL PATHOLOGY
Meniscal Cysts - Pearls and Pitfalls
Meniscal cysts are related to either microscopic or
macroscopic tears in meniscal fibrocartilage.
Horizontal cleavage tears or complex meniscal
tears with a horizontal component are associated
with the development of meniscal cysts.
Loculations, septations, and dissection of the cyst
from the site of origin are common findings.
Emanuel R. Dantas

MISCELLANEOUS MENISCAL PATHOLOGY
Meniscal Cysts
They are classified into three types: intrameniscal,
parameniscal, and synovial cysts:
Intrameniscal cysts are uncommon and represent
intrameniscal fluid collections in continuity with meniscal tears.
Parameniscal cysts are more common and most frequently
present as loculated or simple fluid collections located at the
periphery of the meniscus, often with a horizontal cleavage
tear pattern on cross-section.
Synovial cysts are rare and are not associated with meniscal
tears. They represent cystic outpouching of the joint capsule.26
Emanuel R. Dantas
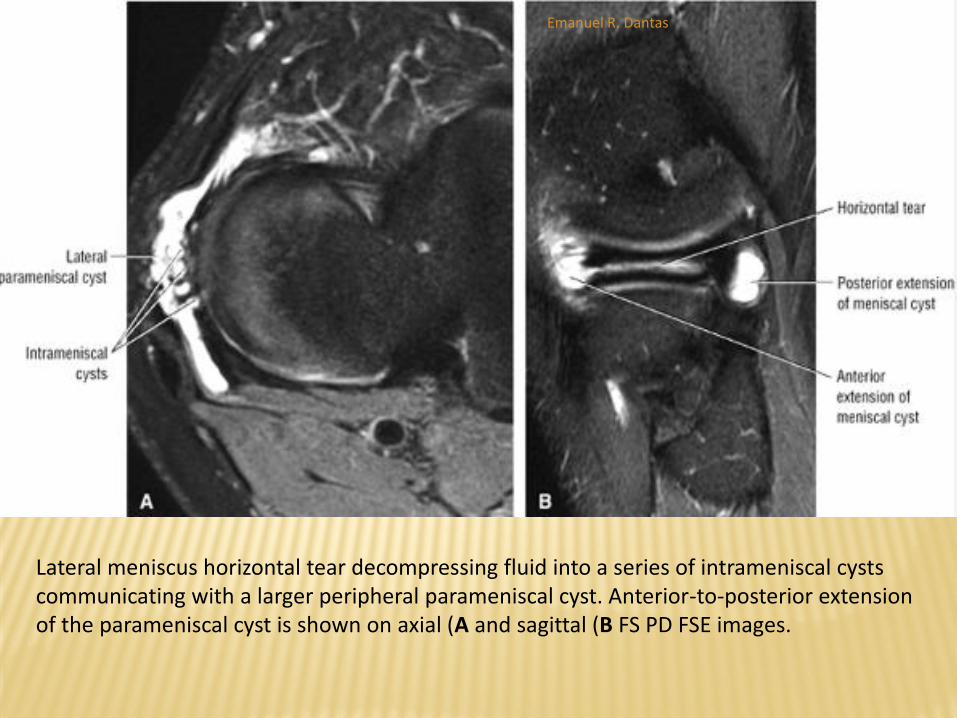
Lateral meniscus horizontal tear decompressing fluid into a series of intrameniscal cysts communicating with a larger peripheral parameniscal cyst. Anterior-to-posterior extension of the parameniscal cyst is shown on axial (A and sagittal (B FS PD FSE images.
Emanuel R. Dantas

MISCELLANEOUS MENISCAL PATHOLOGY
Meniscal Cysts
Parameniscal cysts usually present at the level of the joint line, either as a focal mass or a swelling. They may develop in response to trauma or degeneration and are associated with meniscectomy.
Lateral parameniscal cysts are three to seven times more common than medial cysts, and they often present at the medial third of the peripheral margin of the meniscus.
The difference in the prevalence of lateral and medial meniscal cysts may be exaggerated because of underreporting of medial cysts, which are less likely to cause symptoms.
Emanuel R. Dantas

MISCELLANEOUS MENISCAL PATHOLOGY
Meniscal Cysts
Medial meniscal cysts may dissect through soft tissue
(i.e., joint capsule and MCL) and often present in a
different location than the meniscus tear origin.
They are frequently found deep to the MCL or in the
posteromedial corner, deep to the posterior oblique
ligament.
Pericruciate meniscal cysts may arise from tears of the
posterior horn of the medial meniscus and may be
mistaken for a posterior cruciate ganglion cyst
Emanuel R. Dantas

Peripheral meniscal cyst formation in continuity with horizontal tear. (A) Sagittal cross-section with parameniscal cyst in yellow.
Emanuel R. Dantas

(B) Coronal PD FSE image. (C) Coronal FS PD FSE image.
Emanuel R. Dantas

MISCELLANEOUS MENISCAL PATHOLOGY
Meniscal Cysts
Medial meniscal cysts can been seen extending from the posterior horn and dissecting peripherally to present in a more anterior location. A thin stalk in continuity with the meniscus can usually be identified in these cases.
In 90% of cases, lateral meniscal cysts are also associated with a horizontal flap tear, a horizontal cleavage tear, or a complex tear with horizontal and radial components. Lateral meniscal cysts are usually located anterior to the LCL or between the LCL and popliteus tendon.
Meniscal cysts are uniformly low in signal intensity on T1-weighted images and increase in signal intensity on FS PD-weighted FSE images, T2* GRE images, or STIR images.
Because cysts may also contain bloody or gelatinous fluid with an increased protein content, there may be some variation in their signal-intensity properties on T2-type sequences relative to the appearance and imaging characteristics of free synovial fluid.
Loculations or septations may be seen, especially in complex meniscal cysts, usually in those cysts removed in distance from their site of origin (meniscal tear).
Erosion of the adjacent tibial condyle may occur with large, untreated lateral meniscal cysts.
Emanuel R. Dantas

A large septated and multilobulated lateral parameniscal cyst dissecting freely into Hoffa's fat pad as seen on sagittal PD FSE (A), sagittal FS PD FSE (B), and axial FS PD FSE images.
Emanuel R. Dantas

CRUCIATE LIGAMENTS
Anterior Cruciate Ligament - Pearls and Pitfalls
The ACL is a two-bundle ligament with a small anteromedial and a larger posterolateral (tight in extension) bundle. Functional ACL fiber recruitment, however, is more complicated than assignment to one of two fiber bundles.
The ACL is the primary restraint to anterior tibial displacement, with the posterolateral bundle providing the principal resistance to hyperextension forces.
Emanuel R. Dantas

CRUCIATE LIGAMENTS
Anterior Cruciate Ligament
The cruciate ligaments are intracapsular and extrasynovial.
The ACL and PCL are enveloped by a fold of synovium that takes origin from the posterior intercondylar area of the knee.
Proximally, the ACL is attached to a fossa on the posteromedial aspect of the lateral femoral condyle.
Distally the ACL extends inferior and medial to the anterior tibial intercondylar area and attaches to a fossa anterior and lateral to the anterior tibial spine, between the anterior attachments of the menisci.
The tibial attachment of the ACL (broader or larger than the femoral attachment) passes deep to the transverse ligament of the knee.
It begins as the ACL starts to fan out in its proximal third. Ligamentous branches of the middle geniculate artery form a vascular plexus that supplies both the ACL and PCL
Emanuel R. Dantas

(A) Tibial insertion sites for the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). Insertions are also indicated for the meniscal fibrocartilage. The ACL inserts between the anterior attachments of the menisci. The PCL attaches to the posterior intercondylar area and posterior tibial surface.
Emanuel R. Dantas

(B) Corresponding axial MR image demonstrating hypointense cruciate ligament insertions. (C) Anterior tibial insertion sites of the ACL and menisci on anterior coronal perspective.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - Mechanism of Injury - Pearls and Pitfalls
Pivot Shift Injury
Non-contact injury in skiers or American football players
Valgus load, flexion and external rotation of the tibia or internal rotation of the femur
ACL rupture and lateral compartment contusions
Dashboard Injury (Impacto anterior)
Applied force to anterior proximal tibia with knee in flexion
Associated with anterior tibial and posterior patellar edema with rupture of the PCL and posterior joint capsule
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - Mechanism of Injury - Pearls and Pitfalls
Hyperextension Injury
Direct force applied to the anterior tibia with a planted foot
Direct injury secondary to car bumper impacting on the anterior tibia of a pedestrian
Indirect force as caused by a forceful kicking motion
Kissing contusions of anterior femoral condyle and anterior tibial plateau (hyperextension with an applied valgus force shifts the kissing or opposing bone contusions medially)
Associated soft tissue injuries include ACL or PCL and a meniscal injury.
Knee dislocation with at-risk structures including ACL, PCL, popliteal neurovasular structures and posterolateral complex injuries
Clip Injury
Contact injury secondary to pure valgus stress to a partially flexed (10° to °30) knee
Seen in American football players
Ossesous contusion of lateral femoral condyle from a direct blow with medial femoral epicondylar edema related to MCL avulsion stress
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament
With varus or valgus stress, the ACL is injured after collateral ligament failure.
Forced valgus in external rotation is the most common mechanism of injury and causes disruption of the MCL and medial supporting structures.
Most ACL injuries are caused by a direct or contact mechanism of injury versus an indirect mechanism.
O'Donoghue's triad of ACL, MCL, and medial meniscus injuries is associated with valgus stress in external rotation, also known as a clip injury
Emanuel R. Dantas
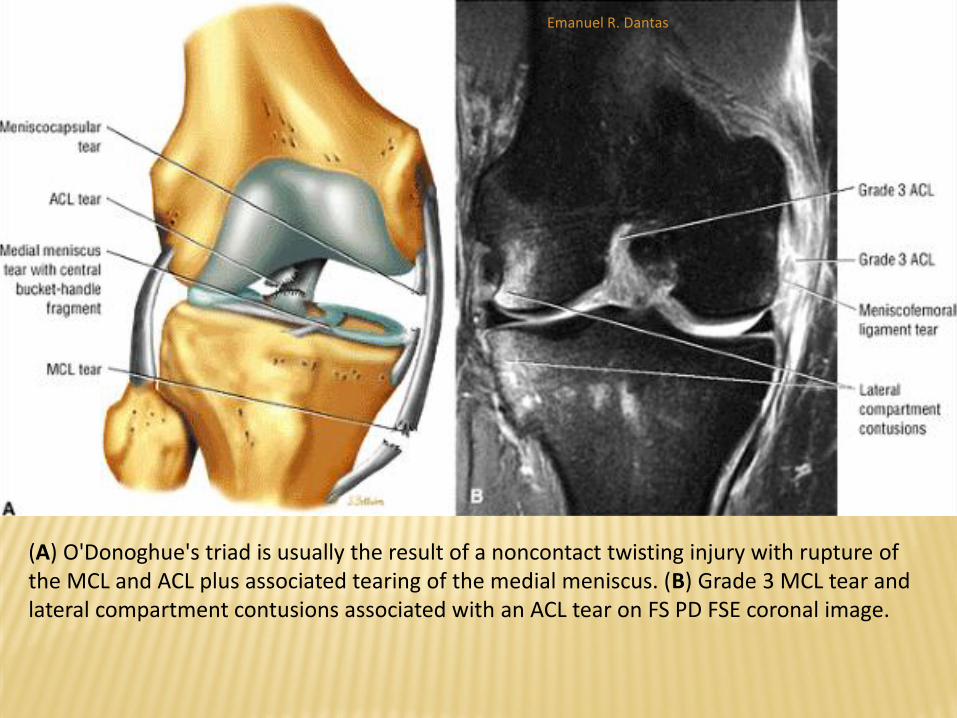
(A) O'Donoghue's triad is usually the result of a noncontact twisting injury with rupture of the MCL and ACL plus associated tearing of the medial meniscus. (B) Grade 3 MCL tear and lateral compartment contusions associated with an ACL tear on FS PD FSE coronal image.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT Anterior Cruciate Ligament
The second most common mechanism of injury (occurring in 30% of patients) is hyperextension associated with a meniscus tear. A direct blow to the flexed knee with the ankle flexed, as seen in turf injuries, represents the third most common pattern of injury to the ACL.
The PCL and posterior capsule may also be damaged in severe contact hyperextension injuries. Posterolateral instability may be associated with disruption of the posterolateral complex.
Isolated ACL injuries are less common but can occur with pivoting during deceleration, which causes forced internal rotation of the femur. The classic knee injury in skiing is a forward fall catching the inside edge of the ski, placing the knee in external rotation in valgus stress
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - Associated Intra-
articular Pathology
Patients with acute ACL injuries are found to have a
higher incidence of lateral meniscal tears (including
displacement of flap fragments into the
intercondylar notch), whereas medial meniscal
tears are more common in patients with chronic
ACL injuries
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - MR Appearance of ACL Tears
Primary Signs
Abnormal ligament course (abnormal Blumensaat angle)
Abnormal ligament signal intensity (coronal images should be used in conjunction with sagittal images to compensate for segmental visualization in the sagittal plane)
Ligament discontinuity
Secondary Signs
Lateral compartment ossesous contusions (posterolateral tibial plateau is most specific)
Posteromedial tibial plateau contusion or fracture
Anterior tibial displacement (assessed in the lateral aspect of the lateral compartment)
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - MR Appearance of ACL Tears
Secondary Signs
Uncovered posterior horn lateral meniscus
Posterior cruciate line and angle
Coronal T1- and PD FSE images identify increased signal intensity within an ACL sprain or complete tear.
An intact ligament remains hypointense and maintains ligamentous continuity on corresponding FS PD FSE coronal images on at least one image posterior to and including the plane of the MCL.
Chronic ACL tears demonstrate resolution of the ossesous contusions, effusions, synovitis, and ligamentous hyperintensity that are characteristic of acute injuries unless seen in the setting of an acute injury.
Mucoid degeneration and ACL or intercondylar notch cysts may be symptomatic with associated restricted range of motion without direct evidence of an ACL sprain or partial tear.
Emanuel R. Dantas
CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - MR Appearance of ACL Tears
The discontinuity of the ACL, especially as assessed in the sagittal and
axial planes, and failure of ACL fascicles to parallel the Blumensaat line,
creating an abnormal Blumensaat angle, are considered primary and
accurate signs of a ligament tear.
The Blumensaat line courses parallel to the roof of the intercondylar
notch (the posterior surface of the femur).
The Blumensaat angle is formed by the Blumensaat line and a line along
the margin (including the distal portion) of the ACL.
A negative (normal) Blumensaat angle occurs when the apex of the angle
is directed superiorly, and a positive (abnormal) Blumensaat angle occurs
when the apex of the angle is directly inferior.
Emanuel R. Dantas
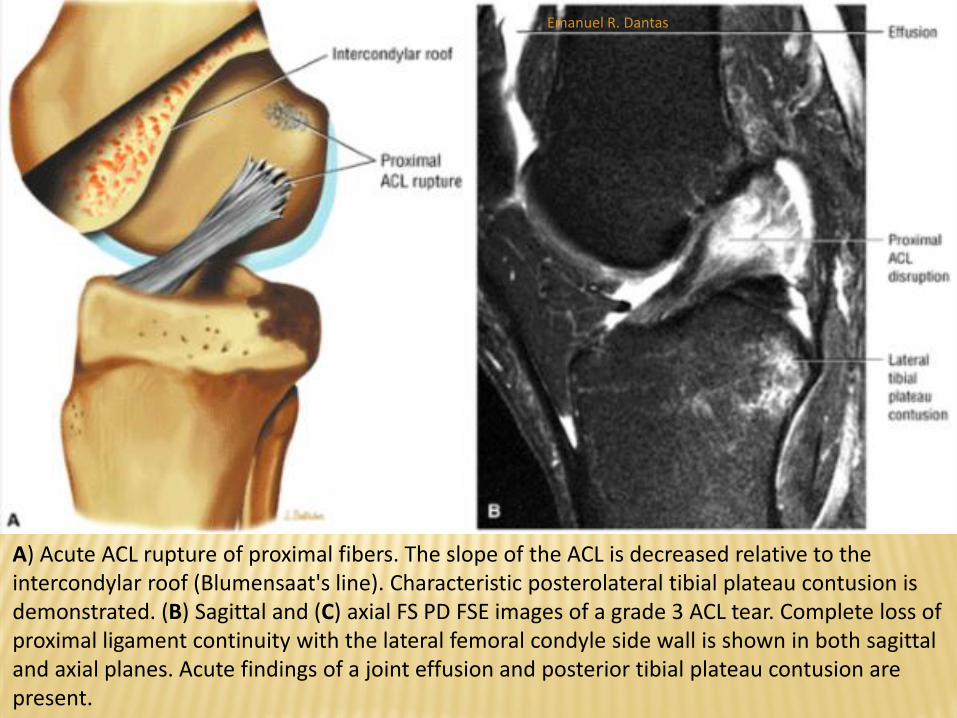
A) Acute ACL rupture of proximal fibers. The slope of the ACL is decreased relative to the intercondylar roof (Blumensaat's line). Characteristic posterolateral tibial plateau contusion is demonstrated. (B) Sagittal and (C) axial FS PD FSE images of a grade 3 ACL tear. Complete loss of proximal ligament continuity with the lateral femoral condyle side wall is shown in both sagittal and axial planes. Acute findings of a joint effusion and posterior tibial plateau contusion are present.
Emanuel R. Dantas
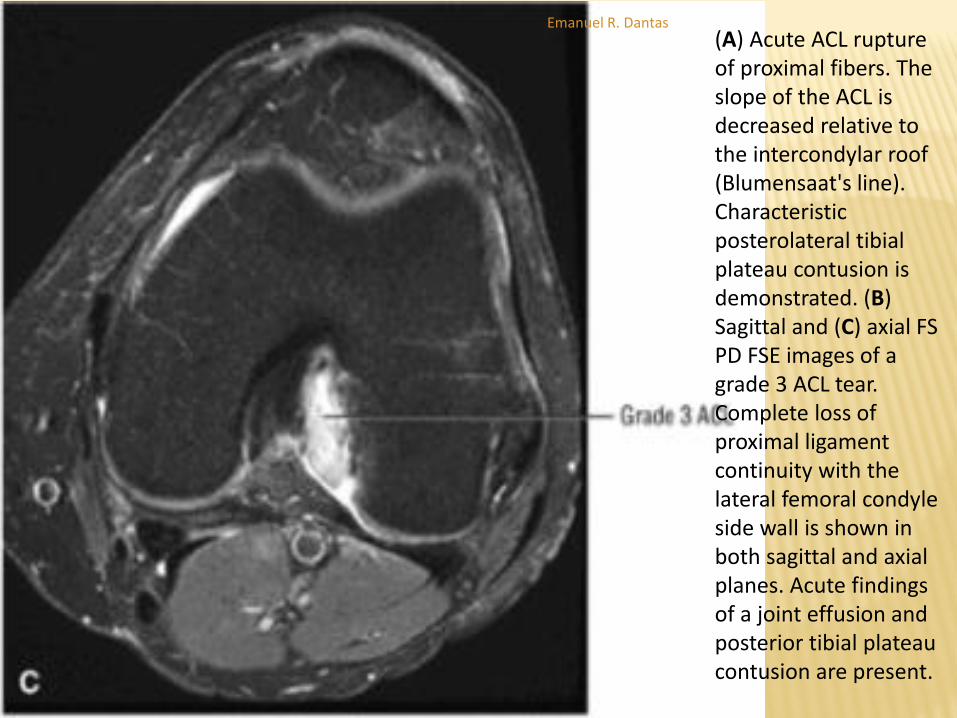
(A) Acute ACL rupture of proximal fibers. The slope of the ACL is decreased relative to the intercondylar roof (Blumensaat's line). Characteristic posterolateral tibial plateau contusion is demonstrated. (B) Sagittal and (C) axial FS PD FSE images of a grade 3 ACL tear. Complete loss of proximal ligament continuity with the lateral femoral condyle side wall is shown in both sagittal and axial planes. Acute findings of a joint effusion and posterior tibial plateau contusion are present.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - MR Appearance of ACL Tears
In an acute ACL tear, there is loss of ligament continuity associated with a wavy or lax contour (including posterior bowing or concavity of the anterior margin of the ACL).
The ruptured ligament has a more horizontal orientation, as demonstrated on sagittal images.
The ACL itself usually demonstrates increased signal intensity on T2-, FS PD FSE, or T2*-weighted images.
Changes in signal intensity may be less pronounced with FSE or FS FSE techniques
Emanuel R. Dantas

An interstitial tear. (A) An ACL interstitial tear pattern with diffuse hyperintensity (arrows) along the entire course of the ligament on a T2*-weighted sagittal image. (B) A thickened and posteriorly bowed ACL (arrows) is visualized with decreased signal intensity on a corresponding FS PD-weighted FSE sagittal image. The GRE image thus overestimates the degree of ligamentous tearing and should only be used in conjunction with a more specific FS PD or T2-weighted FSE sequence for this application.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - Associated Posterolateral Corner The posterolateral corner is also referred to as the posterolateral or arcuate complex.
It includes the following structures: Lateral collateral ligament
Popliteus muscle and tendon
Arcuate ligament
Medial limb—courses over the popliteus muscle and tendon and joins the oblique popliteal ligament
Lateral limb—blends with the capsule near the condylar insertion of the lateral head of the gastrocnemius muscle Popliteofibular ligament
Popliteomeniscal fascicles
Fabellofibular ligament
Lateral head of gastrocnemius muscle
The biceps femoris tendon and iliotibial band, although not usually listed as components of the posterolateral complex, contribute to the stability of the lateral and
posterolateral knee.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Anterior Cruciate Ligament - Associated
Posterolateral Corner
Injuries to the posterolateral corner (also referred to
as the posterolateral or arcuate complex) are
frequently associated with acute ACL (also PCL)
tears.
It is uncommon for the posterolateral corner to be
involved as an isolated injury
Emanuel R. Dantas
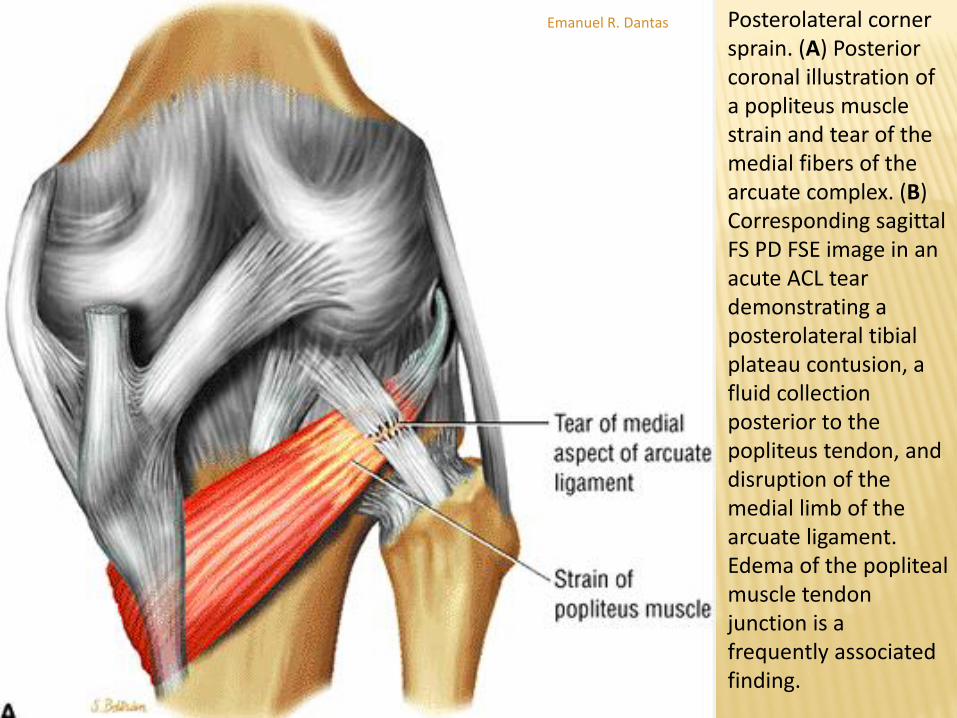
Posterolateral corner sprain. (A) Posterior coronal illustration of a popliteus muscle strain and tear of the medial fibers of the arcuate complex. (B) Corresponding sagittal FS PD FSE image in an acute ACL tear demonstrating a posterolateral tibial plateau contusion, a fluid collection posterior to the popliteus tendon, and disruption of the medial limb of the arcuate ligament. Edema of the popliteal muscle tendon junction is a frequently associated finding.
Emanuel R. Dantas
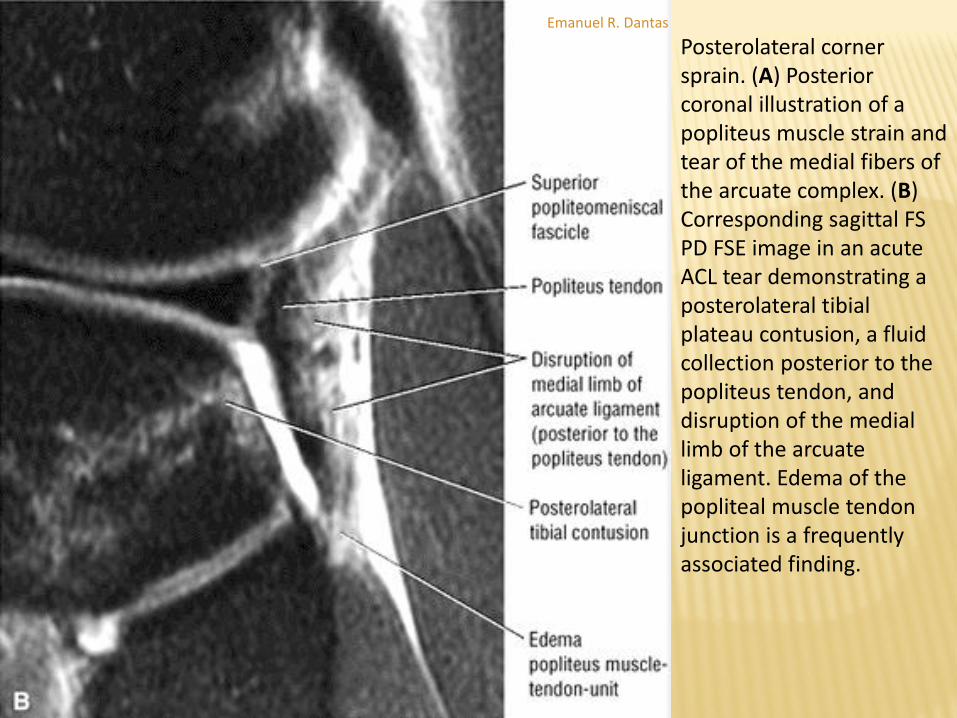
Posterolateral corner sprain. (A) Posterior coronal illustration of a popliteus muscle strain and tear of the medial fibers of the arcuate complex. (B) Corresponding sagittal FS PD FSE image in an acute ACL tear demonstrating a posterolateral tibial plateau contusion, a fluid collection posterior to the popliteus tendon, and disruption of the medial limb of the arcuate ligament. Edema of the popliteal muscle tendon junction is a frequently associated finding.
Emanuel R. Dantas
CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Osseous Injuries - Pearls and Pitfalls
Posteromedial tibial plateau contusions or fractures represent contre-coup injuries associated with lateral compartment osseous impaction with ACL ruptures.
Posterior peripheral medial meniscus tears and meniscocapsular separations occur in conjunction with posteromedial tibial plateau injuries.
The Segond fracture is visualized on anterior coronal images at the location of the lateral compartment of the meniscotibial ligament.
It is associated with avulsion forces directed by the posterior fibers of the iliotibial tract.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Osseous Injuries
Avulsion fractures of the fibular head are associated with
PCL tears.
Several osseous injuries are associated with tears of the ACL.
The most commonly seen are lateral compartment bone
contusions involving the weight-bearing portion of the lateral
femoral condyle and the posterolateral tibial plateau.
Murphy et al. have found posterolateral tibial plateau (94%)
and lateral femoral condyle (91%) subchondral bone
impactions to be relatively specific signs of an acute ACL tear
Emanuel R. Dantas

Nondisplaced posterolateral tibial plateau fracture secondary to ACL disruption on a sagittal FS PD image.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Osseous Injuries
The Segond fracture, previously thought to represent a bony ligamentous
avulsion of the meniscotibial portion of the middle third of the lateral
capsular ligament, is currently attributed to an avulsion injury of the
posterior fibers of the iliotibial tract or anterior oblique band of the LCL .
It is associated with rupture of the ACL in 75% to 100% of cases.
On MR scans a small vertical avulsion of the LCL insertion in the lateral
aspect of the proximal tibia can be identified.
The elliptical fracture fragment may be seen at the fracture site on
coronal images.
In acute or subacute injuries, the fracture fragment demonstrates low
signal intensity on T1- or PD-weighted images and hyperintensity on FS
T2-weighted FSE or STIR images.
Emanuel R. Dantas
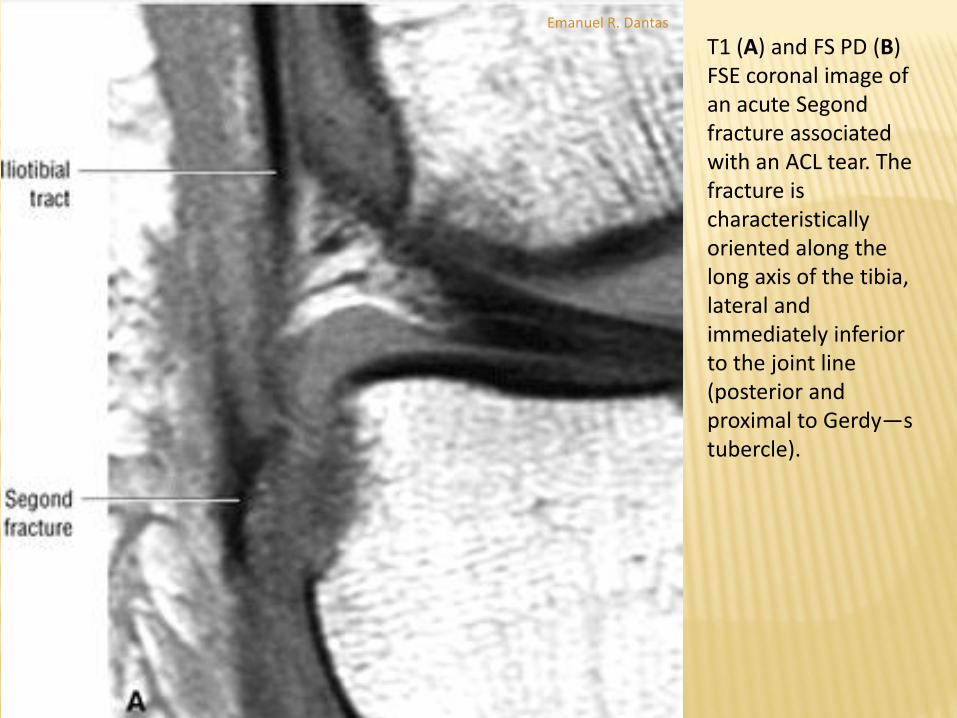
T1 (A) and FS PD (B) FSE coronal image of an acute Segond fracture associated with an ACL tear. The fracture is characteristically oriented along the long axis of the tibia, lateral and immediately inferior to the joint line (posterior and proximal to Gerdy—s tubercle).
Emanuel R. Dantas

T1 (A) and FS PD (B) FSE coronal image of an acute Segond fracture associated with an ACL tear. The fracture is characteristically oriented along the long axis of the tibia, lateral and immediately inferior to the joint line (posterior and proximal to Gerdy—s tubercle).
Emanuel R. Dantas

CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Osseous Injuries
A tibial spine avulsion is an uncommon but specific finding for ACL
injury.
Distal ACL injuries are frequently associated with avulsion injuries
because the distal ACL fibers are relatively stronger than adjacent bone.
Avulsion tears represent only 5% of ACL injuries in adults, however, and
ACL injuries that are thought to be primarily avulsion injuries more likely
are either intraligamentous or complete tears of the ACL.
Kaplan et al. correctly correlated bone contusions of the posterior lip of
the medial tibial plateau (with or without involvement of the medial
femoral condyle) with a contre-coup injury, which occurs as the tibia
reduces after an ACL rupture
Emanuel R. Dantas
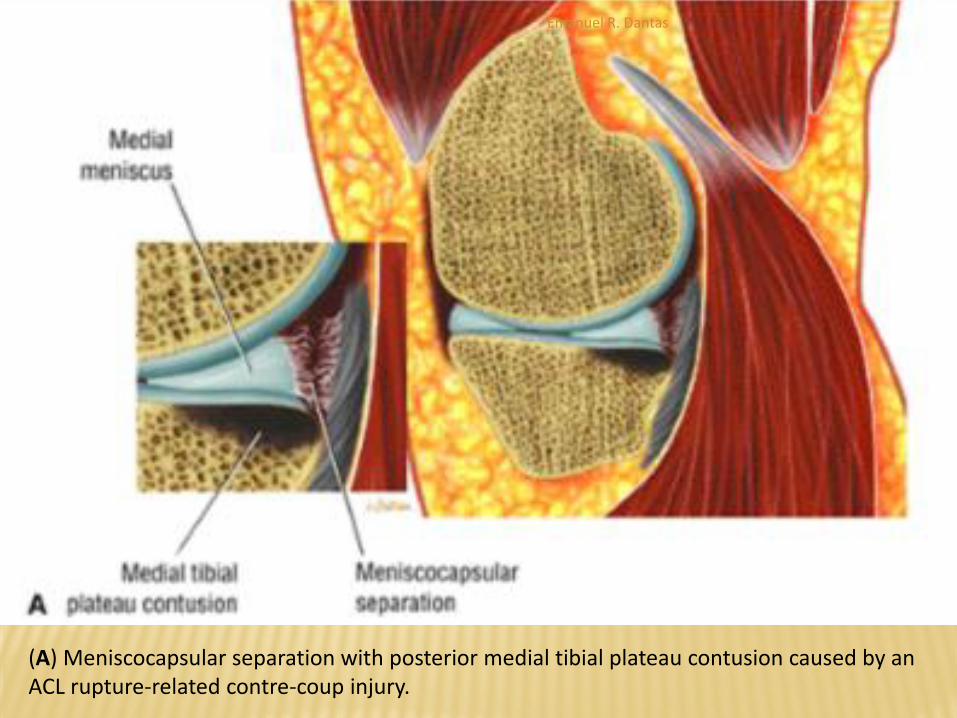
(A) Meniscocapsular separation with posterior medial tibial plateau contusion caused by an ACL rupture-related contre-coup injury.
Emanuel R. Dantas

(B) Corresponding sagittal image displaying a hyperintense meniscocapsular separation and a medial tibial plateau contusion. Lateral compartment contusions (C) and the grade 3 ACL tear (D) are demonstrated. (B), (C), and (D) are sagittal FS PD FSE images.
Emanuel R. Dantas
CRUCIATE LIGAMENTS - ANTERIOR CRUCIATE
LIGAMENT
Osseous Injuries
An avulsion fracture of the head of the fibula known as the arcuate sign is associated with injuries to the PCL and posterolateral ligaments .
The fractured elliptical fragment of the fibular styloid process serves as the attachment for the popliteofibular, arcuate, and fabellofibular ligaments.
The LCL and the tendon of the biceps femoris, in contrast, attach to the lateral margin of the fibular head and not the styloid or apex of the fibular head. Avulsions of the LCL and biceps femoris are less common.
Emanuel R. Dantas

Acute ACL-related arcuate ligament injury with an avulsion fracture of the head at the attachment sites of the popliteofibular and arcuate ligaments. (A) Coronal FS PD FSE image showing the medial displacement of the popliteofibular ligament. (B) Sagittal FS PD FSE image showing arcuate ligament disruption. (C) Axial FS PD FSE image displaying the posterior involvement of the fibular head, corresponding to the attachments of the popliteofibular and arcuate ligaments.
Emanuel R. Dantas
CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
Pearls and Pitfalls
PCL injuries include reverse Segond fractures, an
arcuate sign, and anterior compartment osseous
contusions.
MR findings of partial or interstitial tears of the PCL
are more common than complete ligament
ruptures.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
Functional Anatomy
The PCL originates in the lateral aspect of the medial
femoral condyle, crosses the ACL, and attaches to the
posterior intercondyloid fossa of the tibia.
The PCL, similar to the ACL, is intra-articular but is
extrasynovial and enveloped by a fold of synovium
reflected from the posterior capsule.
The PCL is composed of an anterolateral and
posteromedial band that tightens on flexion and
extension respectively
Emanuel R. Dantas
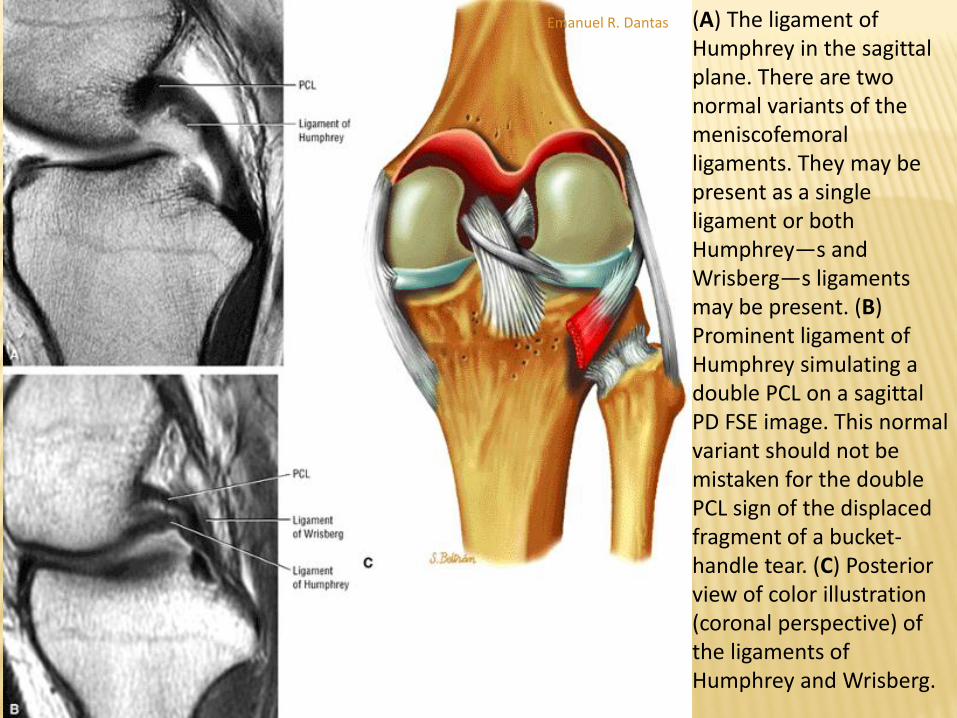
(A) The ligament of Humphrey in the sagittal plane. There are two normal variants of the meniscofemoral ligaments. They may be present as a single ligament or both Humphrey—s and Wrisberg—s ligaments may be present. (B) Prominent ligament of Humphrey simulating a double PCL on a sagittal PD FSE image. This normal variant should not be mistaken for the double PCL sign of the displaced fragment of a bucket-handle tear. (C) Posterior view of color illustration (coronal perspective) of the ligaments of Humphrey and Wrisberg.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
Location and Mechanism of Injury
The PCL is twice as strong as the ACL, with a larger cross-sectional
area and higher tensile strength. These features account for a
lower incidence of rupture of the PCL
Tears of the PCL are most common in the midportion (76%),
followed by avulsions from the femur (36% to 55%) and the tibia
(22% to 42%).
Rupture may be caused by excessive rotation, hyperextension,
dislocation, or direct trauma while the knee is flexed.
Motor vehicle accidents (dashboard injuries) and injuries
sustained in contact sports such as football are the most common
causes of damage to the PCL.
Emanuel R. Dantas

PCL injury with hyperextension and valgus mechanism results in contusions of the anterior compartment of the knee. Forced hyperextension of the knee may tear the ACL, PCL, and posterior capsule. (A) Sagittal color illustration with anterior tibial hyperextension contusions. (B) Sagittal FS PD FSE image showing PCL sprain with anterior tibial contusion and posteromedial fiber bundle involvement. (C) Lateral sagittal FS PD FSE image with anterior lateral compartment contusions.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
Location and Mechanism of Injury
Injuries to the PCL are usually associated with tears
of the ACL, the meniscus, collateral ligaments, or
posterolateral structures (Fig. 4.254).246,254 When
there is a lateral shift of the normal center of the
axis of rotation of the joint, PCL insufficiency may
lead to articular cartilage degeneration in the
medial compartment of the knee.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
MR Imaging
The normal PCL is seen as a uniform low-signal-intensity band.
The morphology and signal intensity of the PCL are routinely
evaluated on axial, coronal, and sagittal images.
In the sagittal plane, the PCL has an arcuate shape with the knee
positioned in neutral or minimal flexion and is visualized in its
entire length on one or two consecutive sagittal images.
In the posterior coronal plane, the PCL demonstrates a more
vertical orientation as it is sectioned in the downward slope of its
curved arc.
Mid- and anterior-coronal images display the more circular cross-
section of the ligament.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
MR Imaging
Axial images can be used to follow the sectioning of the ligament from the posterior tibia to its broad anterior medial femoral condyle attachment.
Findings of increased signal intensity with normal PCL morphology on T1- or PD-weighted images require the addition of conventional T2-, T2*-, or FS T2-weighted FSE images to identify the sites of ligamentous pathology.
Hemorrhage and edema, seen in acute injuries, are bright on T2-(including FSE)
Emanuel R. Dantas
CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
MR Imaging
Any increase in PCL signal intensity on T1-, PD-, T2-, T2*-, or FS PD-weighted FSE images is abnormal.
In an interstitial tear, the entire ligament or long segment may be difficult to identify because of diffuse widening and increased signal intensity.
A long segment of interstitial tear may produce a division of the PCL into separated fiber bundles.
In complete tears, there is amorphous high signal intensity without definable ligamentous fibers.
Alternatively, focal discontinuity or a gap may be seen at the site
Emanuel R. Dantas

As the PCL tightens with flexion, forced hyperflexion produces excessive strain on the anterolateral bundle of the PCL. This type of sprain may lead to interstitial failure of the PCL. (A) Coronal FS PD FSE image. (B) Sagittal FS PD FSE image.
Emanuel R. Dantas
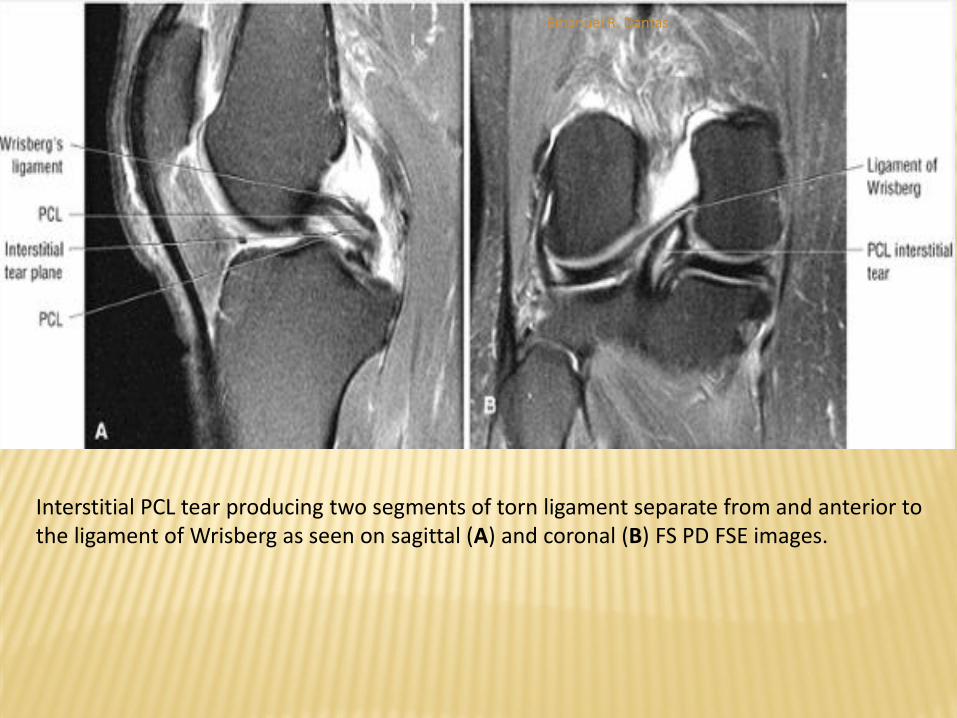
Interstitial PCL tear producing two segments of torn ligament separate from and anterior to the ligament of Wrisberg as seen on sagittal (A) and coronal (B) FS PD FSE images.
Emanuel R. Dantas
CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
MR Imaging
Partial tears display increased signal intensity, with discernible fibers identified along the course of the ligament.
A chronic partial tear may be difficult to identify on MR, even in the presence of a clinically positive posterior sag sign.
It is easier to assess ligament morphology on FS PD-weighted FSE images than on GRE images, which tend to display a greater degree of hyperintensity in regions of edema and hemorrhage.
Emanuel R. Dantas
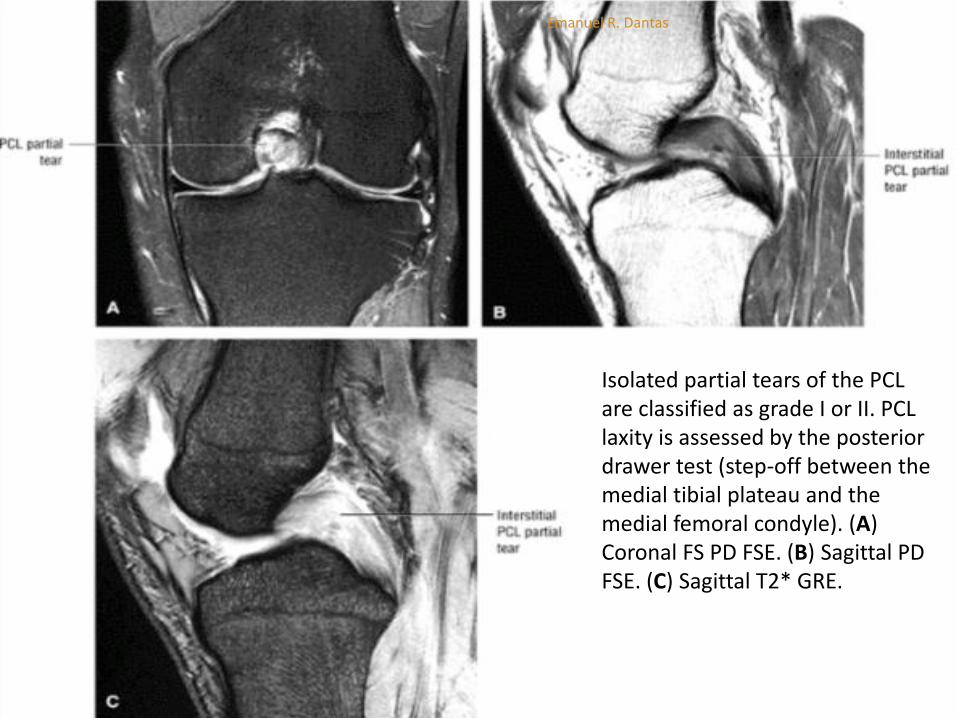
Isolated partial tears of the PCL are classified as grade I or II. PCL laxity is assessed by the posterior drawer test (step-off between the medial tibial plateau and the medial femoral condyle). (A) Coronal FS PD FSE. (B) Sagittal PD FSE. (C) Sagittal T2* GRE.
Emanuel R. Dantas

CRUCIATE LIGAMENTS - POSTERIOR CRUCIATE
LIGAMENT (PCL)
MR Imaging
Bone contusions in the anterolateral tibia and posterior lateral femoral condyle are consistent with a forced posterior displacement of the tibia in a flexed knee.
Hyperextension injuries may demonstrate contusions of the anterotibial articular surface and the anterior aspect of the femoral condyle. There may be an associated ACL rupture.
An avulsion tear off the tibial plateau may be associated with high-signal-intensity ligamentous hemorrhage and a bone fragment containing marrow.
Subchondral marrow edema and hemorrhage between the avulsed fragment and tibia are frequently seen on FS PD-weighted FSE and STIR images.
Emanuel R. Dantas
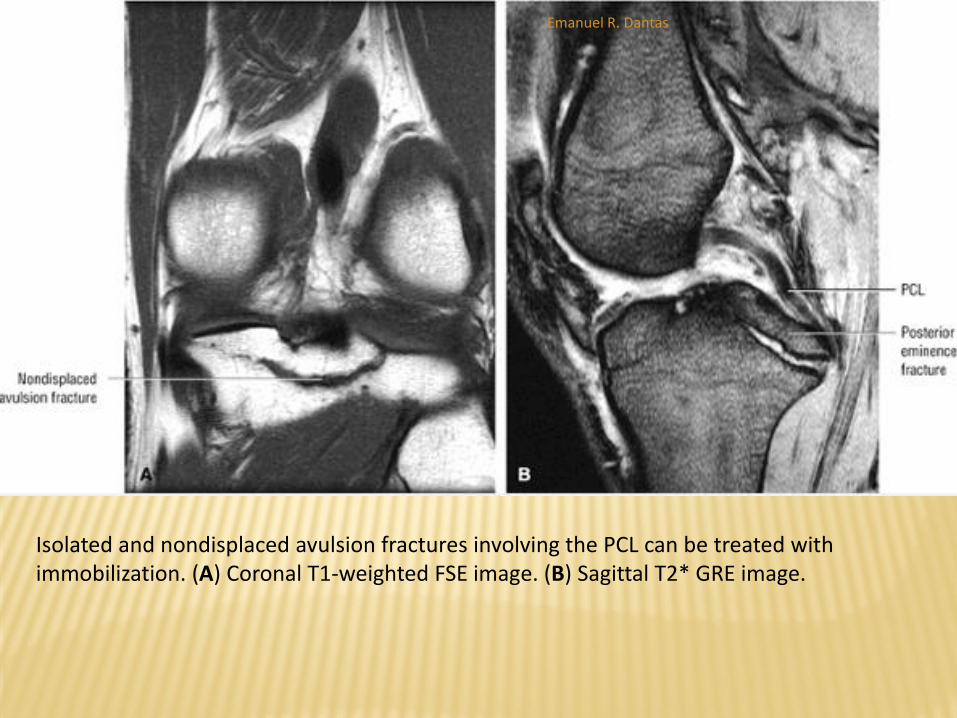
Isolated and nondisplaced avulsion fractures involving the PCL can be treated with immobilization. (A) Coronal T1-weighted FSE image. (B) Sagittal T2* GRE image.
Emanuel R. Dantas
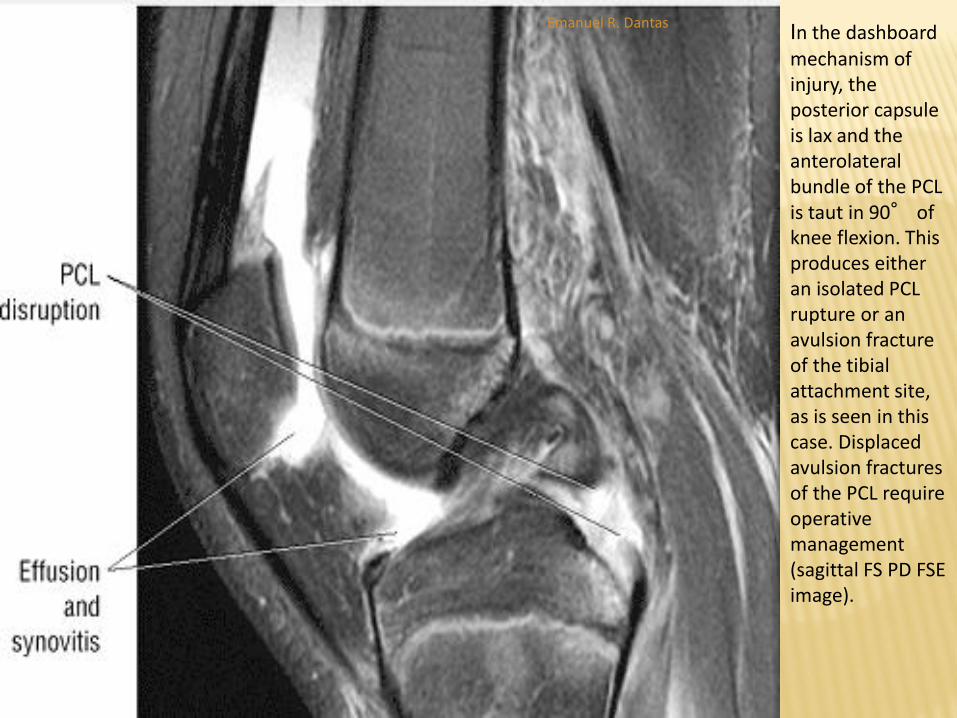
In the dashboard mechanism of injury, the posterior capsule is lax and the anterolateral bundle of the PCL is taut in 90° of knee flexion. This produces either an isolated PCL rupture or an avulsion fracture of the tibial attachment site, as is seen in this case. Displaced avulsion fractures of the PCL require operative management (sagittal FS PD FSE image).
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
Pearls and Pitfalls
The superficial MCL represents layer 2 of the medial supporting structures.
Layer 3 is formed by the deep MCL (meniscofemoral and meniscotibial attachments), found deep to the superficial MCL.
Laxity of the MCL is associated with distal MCL tears.
The MCL heals with scar formation, which is visualized as a thickened hypointense structure.
Medial meniscal injuries may be associated with MCL tears and should be carefully looked for.
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
Functional Anatomy
The MCL, or tibial collateral ligament, is 8 to 11 cm long and extends from its medial epicondylar origin to attach 5 to 7 cm inferior to the tibial plateau and posterior to the pes anserinus insertion.
The insertion of the MCL on the tibia is covered by the muscle group of the pes anserinus.
The MCL is considered to be composed of two layers:
(1) deep fibers, corresponding to layer 3, that attach to the capsule and medial meniscus peripherally and
(2) more superficial fibers, corresponding to layer 2
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
Functional Anatomy
The posteromedial corner of the knee is an
important and anatomically complex region
frequently injured in association with other medial
supporting structures and the medial meniscus.
The posteromedial corner receives an important
contribution from the semimembranosus tendon
Emanuel R. Dantas

Posteromedial structures above the joint line on (A) a color axial cross-section and (B) an axial T1-weighted MR arthrogram.
Emanuel R. Dantas

Posteromedial structures above the joint line on (A) a color axial cross-section and (B) an axial T1-weighted MR arthrogram.
Emanuel R. Dantas

(A) Ruptured gracilis and semitendinosus tendons on a sagittal PD FSE image. (B) Medial view of normal pes tendons for comparison on a color illustration from the sagittal perspective.
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
MR Appearance - Tears and Sprains
MR evaluation of these injuries is best accomplished with coronal images that demonstrate the low-signal MCL and its attachment points, where it merges with low-signal-intensity cortical bone.
Separation of the deep and superficial layers can be distinguished on FS PD FSE-weighted images.
A thin band of intermediate signal intensity, originally thought to be fat, is actually an intraligamentous bursa between layers 2 and 3 and is often seen between the anterior portion of the MCL and the deep medial capsular ligament complex.
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
MR Appearance - Tears and Sprains
Edema and hemorrhage, which extend into subcutaneous fat, are identified parallel to the superficial MCL and may occur in acute grade I sprains (entorse).
The MCL is of normal thickness and is closely applied to the underlying cortical bone.
Partial tears or grade II sprains of the MCL demonstrate displacement of ligament fibers from adjacent cortical bone with varying degrees of edema and hemorrhage
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
MR Appearance - Tears and Sprains
FS PD FSE and STIR images demonstrate high-signal-intensity
edema, hemorrhage, or both around low-signal-intensity
ligamentous fibers, which are superficial and deep to the MCL.
Usually there is some degree of ligamentous attenuation or areas
of fluid separating partially torn fibers in grade II injuries.
Contusions of either the medial femoral condyle or lateral tibial
plateau may be associated with grade II or III sprains.
Intraligamentous hyperintensity and thickening is appreciated on
coronal and axial images.
Segmental or focal ligamentous thickening can be seen in grade II
sprains
Emanuel R. Dantas
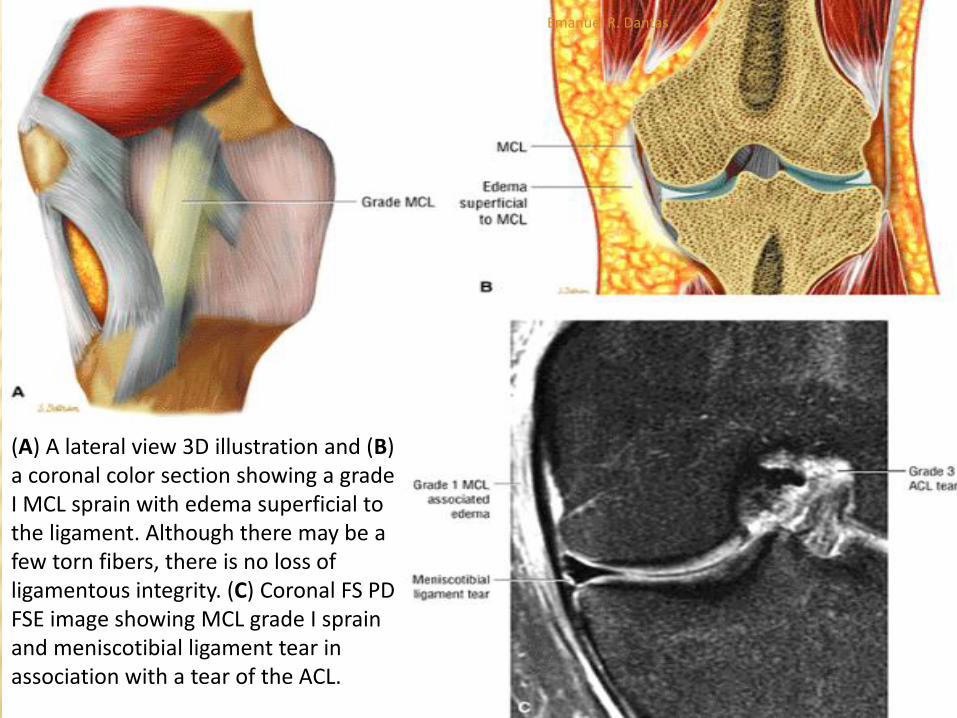
(A) A lateral view 3D illustration and (B) a coronal color section showing a grade I MCL sprain with edema superficial to the ligament. Although there may be a few torn fibers, there is no loss of ligamentous integrity. (C) Coronal FS PD FSE image showing MCL grade I sprain and meniscotibial ligament tear in association with a tear of the ACL.
Emanuel R. Dantas

Grade 1 MCL sprain with fluid (arrow) superficial to the MCL is hypointense on a T1-weighted coronal image (A) and hyperintense on a FS PD-weighted FSE coronal image (B). There is no displacement or thickening of the low-signal-intensity ligament. A grade 1 tear is primarily a periligamentous injury with associated microscopic tearing of ligament fibers.
Emanuel R. Dantas

Grade 2 MCL sprain with intraligamentous thickening and degeneration in association with fluid and/or edema superficial and deep to the ligament. Grade 2 injuries are moderate sprains or incomplete tears without pathologic laxity. The MCL fibers are apposed, allowing for ligamentous healing. (A) Lateral 3D color illustration. (B) Coronal color section. (C) Coronal FS PD FSE image.
Emanuel R. Dantas

Grade 2 MCL sprain with intraligamentous thickening and degeneration in association with fluid and/or edema superficial and deep to the ligament. Grade 2 injuries are moderate sprains or incomplete tears without pathologic laxity. The MCL fibers are apposed, allowing for ligamentous healing. (A) Lateral 3D color illustration. (B) Coronal color section. (C) Coronal FS PD FSE image.
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
MR Appearance - Tears and Sprains
In grade III lesions or tears, there is complete loss of continuity of the ligamentous fibers with or without extension into the capsular layer.
It may be difficult to distinguish between high-grade partial tears and complete tears of the MCL, however.
Complete biomechanical failure of the MCL is associated with disruption of the medial capsular layer or ligament.
A tear of the distal or tibial attachment of the MCL may be associated with a wavy or serpiginous ligamentous contour as a reflection of ligamentous laxity.
A retracted distal MCL tear may have a more serpiginous morphology and requires surgical repair.
Distal MCL tears may be associated with pes tendon sprains. A pes tendon rupture can occur, however, without tear of the MCL
Emanuel R. Dantas

A) A lateral 3D color illustration and (B) a coronal color section showing a grade III proximal sprain or tear with loss of ligament integrity. Swelling and ecchymosis are common, and there is associated pathologic laxity. Grade 3 tears may have no end-point to abduction stress.
Emanuel R. Dantas
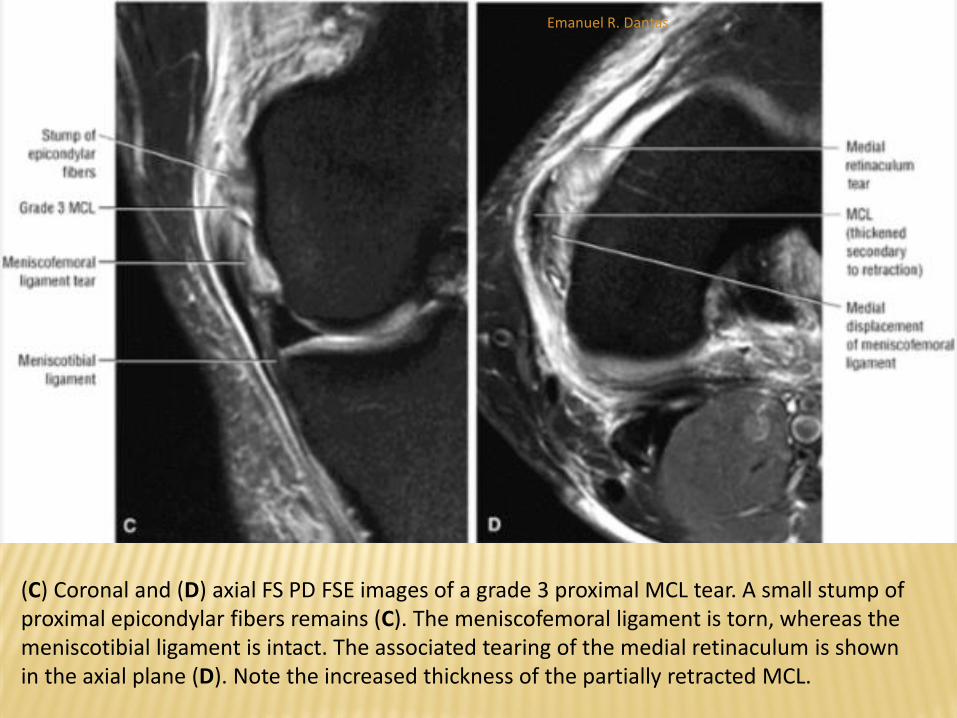
(C) Coronal and (D) axial FS PD FSE images of a grade 3 proximal MCL tear. A small stump of proximal epicondylar fibers remains (C). The meniscofemoral ligament is torn, whereas the meniscotibial ligament is intact. The associated tearing of the medial retinaculum is shown in the axial plane (D). Note the increased thickness of the partially retracted MCL.
Emanuel R. Dantas
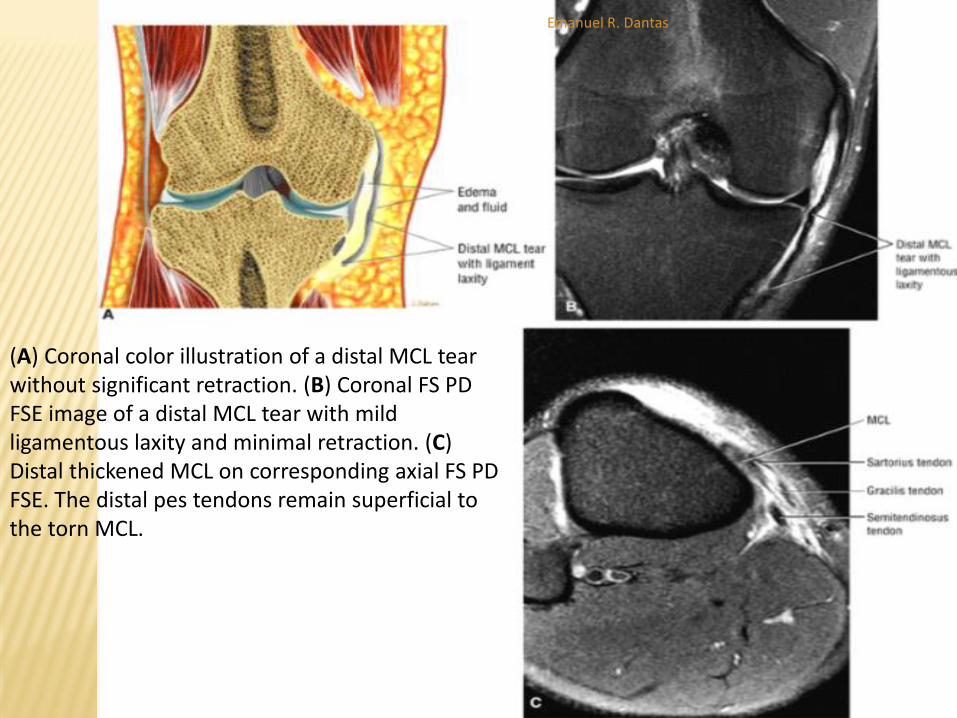
(A) Coronal color illustration of a distal MCL tear without significant retraction. (B) Coronal FS PD FSE image of a distal MCL tear with mild ligamentous laxity and minimal retraction. (C) Distal thickened MCL on corresponding axial FS PD FSE. The distal pes tendons remain superficial to the torn MCL.
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
MR Appearance - Tears and Sprains
Ossification of the femoral epicondylar or proximal
attachment of the MCL is thought to be the result
of chronic trauma and is referred to as Pellegrini-
Stieda disease.
Areas of ossification in Pellegrini-Stieda disease
may demonstrate marrow fat signal intensity or may
be hypointense if sclerotic.
Emanuel R. Dantas

Pellegrini-Stieda syndrome with ossification of the femoral attachment of the MCL. The ossification is directed along the long axis.
Emanuel R. Dantas

COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
MCL (Tibial Collateral Ligament) and Pes
Anserinus Bursitis
Bursitis can be demonstrated on MR images in
patients presenting with medial joint pain.
Involvement of Voshell's bursa is seen as
hyperintense signal located between layer 2
(superficial MCL) and layer 3 (medial capsular
ligament) on T2- or FSE PD-weighted scans.
Emanuel R. Dantas
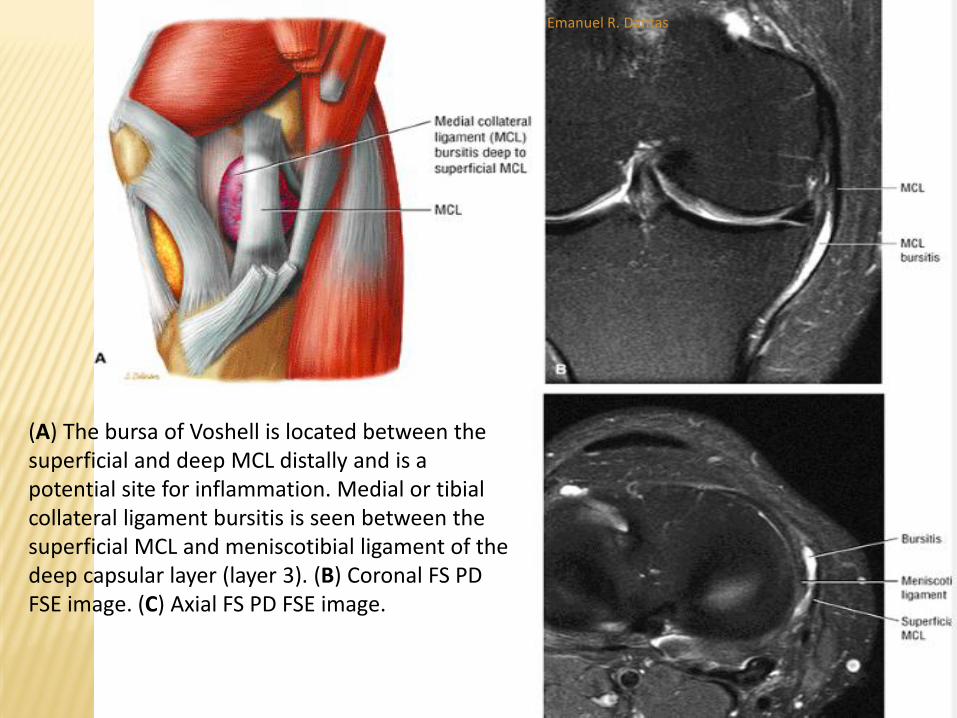
(A) The bursa of Voshell is located between the superficial and deep MCL distally and is a potential site for inflammation. Medial or tibial collateral ligament bursitis is seen between the superficial MCL and meniscotibial ligament of the deep capsular layer (layer 3). (B) Coronal FS PD FSE image. (C) Axial FS PD FSE image.
Emanuel R. Dantas
COLLATERAL LIGAMENTS
MEDIAL COLLATERAL LIGAMENT
MCL (Tibial Collateral Ligament) and Pes Anserinus Bursitis
Pes anserinus bursitis is characterized by fluid anterior to the conjoined tendons of the sartorius, semitendinosus, and gracilis tendons that demonstrates low signal intensity on T1-weighted images and hyperintensity on FS PD FSE images.
There may be a septation or hemorrhage within the bursa.
The pes bursa overlies the pes tendons and is located distal to Voshell's bursa.
Pes bursitis may be associated with athletic activity or degenerative
Emanuel R. Dantas
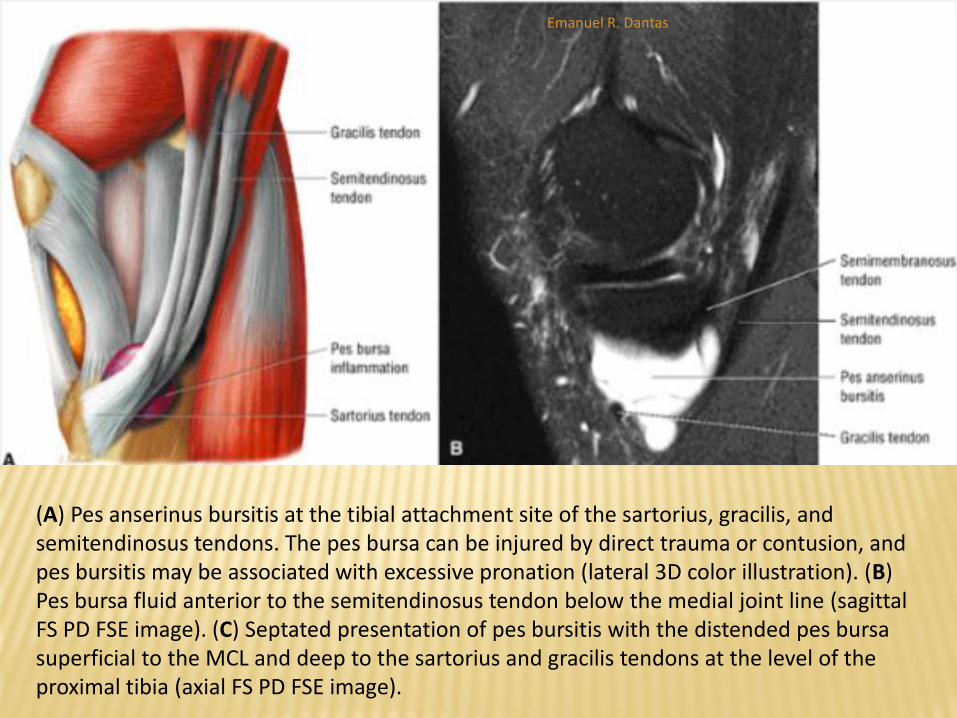
(A) Pes anserinus bursitis at the tibial attachment site of the sartorius, gracilis, and semitendinosus tendons. The pes bursa can be injured by direct trauma or contusion, and pes bursitis may be associated with excessive pronation (lateral 3D color illustration). (B) Pes bursa fluid anterior to the semitendinosus tendon below the medial joint line (sagittal FS PD FSE image). (C) Septated presentation of pes bursitis with the distended pes bursa superficial to the MCL and deep to the sartorius and gracilis tendons at the level of the proximal tibia (axial FS PD FSE image).
Emanuel R. Dantas
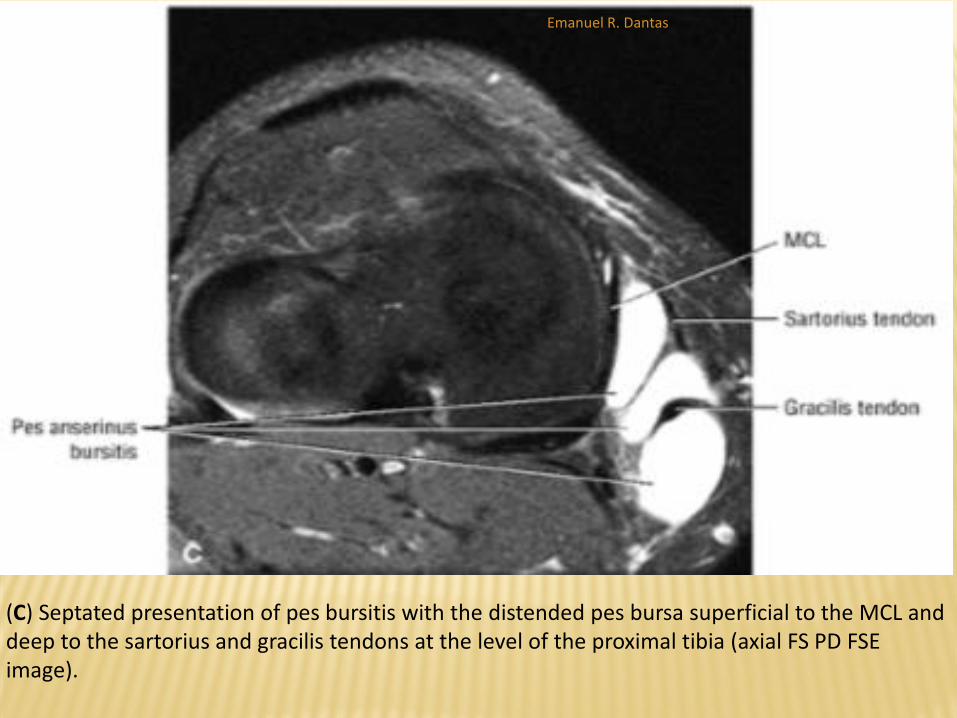
(C) Septated presentation of pes bursitis with the distended pes bursa superficial to the MCL and deep to the sartorius and gracilis tendons at the level of the proximal tibia (axial FS PD FSE image).
Emanuel R. Dantas

LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
Pearls and Pitfalls
LCL tears are associated with injury to other posterolateral
structures.
Popliteus muscle or myotendinous unit strains represent
extra-articular injuries. Intra-articular popliteus tears, which
are less common, involve the hiatus or popliteus femoral
attachment at the fossa.
The LCL and biceps femoris attach to the lateral margin of
the fibular head and not the styloid, accounting for a reduced
likelihood of avulsion injury compared to the popliteofibular,
fabellofibular, and arcuate ligaments.
Emanuel R. Dantas

LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
The lateral aspect of the knee is divided into three structural
layers:
Layer 1 is the most superficial layer and consists of the iliotibial tract with
its anterior expansion and the superficial portion of the biceps femoris
with its posterior expansion.
Layer 2 consists of the quadriceps retinaculum anteriorly and two
patellofemoral ligaments or retinacula posteriorly. Layers 1 and 2 merge at
the lateral aspect of the patella.
Layer 3 is the deepest layer and consists of the lateral joint capsule,
including attachments to the lateral meniscus, and the lateral capsular
ligament with its meniscofemoral and meniscotibial components. The LCL
is located posteriorly between the superficial and deep divisions of layer 3.
The ligament itself is considered a layer 2 structure.
Emanuel R. Dantas

Superficial lateral structures of the knee on peripheral sagittal image.
Emanuel R. Dantas
LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
Axial plane anatomy demonstrates the relationships of the LCL and biceps femoris and popliteus tendons at the level of the lateral femoral condyle and joint line.
The popliteus tendon is a useful landmark at the level of the lateral meniscus as it is located just medial to the LCL.
The posterolateral (arcuate) complex includes the LCL, the popliteus tendon, the lateral head of the gastrocnemius muscle, and the arcuate ligament
Emanuel R. Dantas

Superior axial cross-section of the lateral compartment at the level of the lateral meniscus on (A) a 3D color illustration and (B) an axial T1-weighted MR arthrogram.
Emanuel R. Dantas
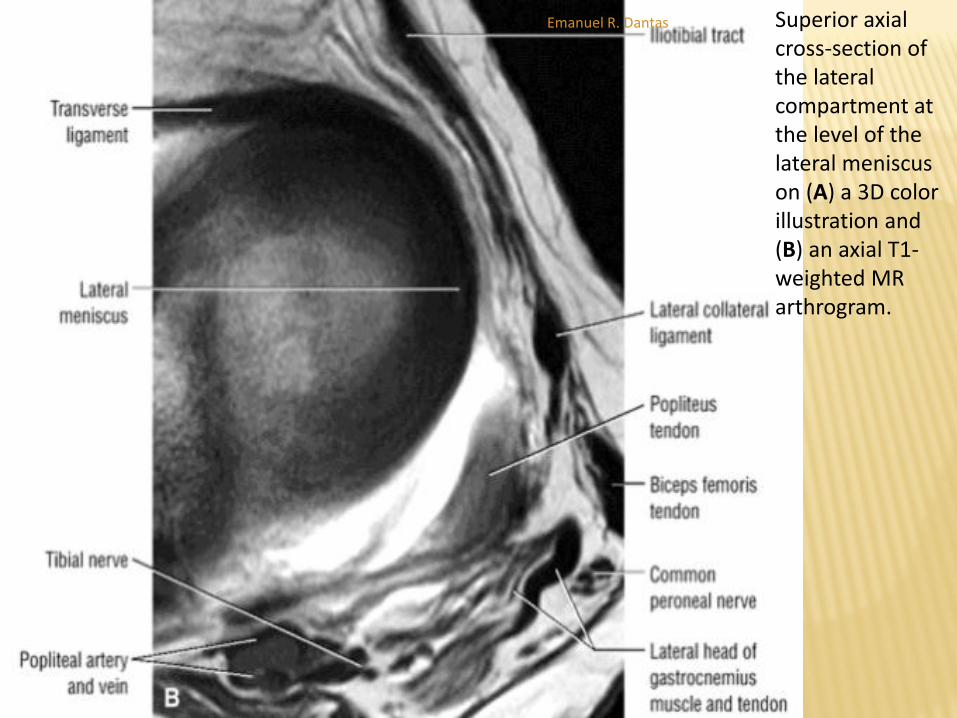
Superior axial cross-section of the lateral compartment at the level of the lateral meniscus on (A) a 3D color illustration and (B) an axial T1-weighted MR arthrogram.
Emanuel R. Dantas

LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
The insertion of the popliteus tendon onto the
popliteus fossa of the lateral femoral condyle is
distal and anterior to the proximal LCL (the
popliteus tendon crosses deep to the LCL).
The posterolateral complex also includes the
popliteofibular and fabellofibular ligaments.
Emanuel R. Dantas
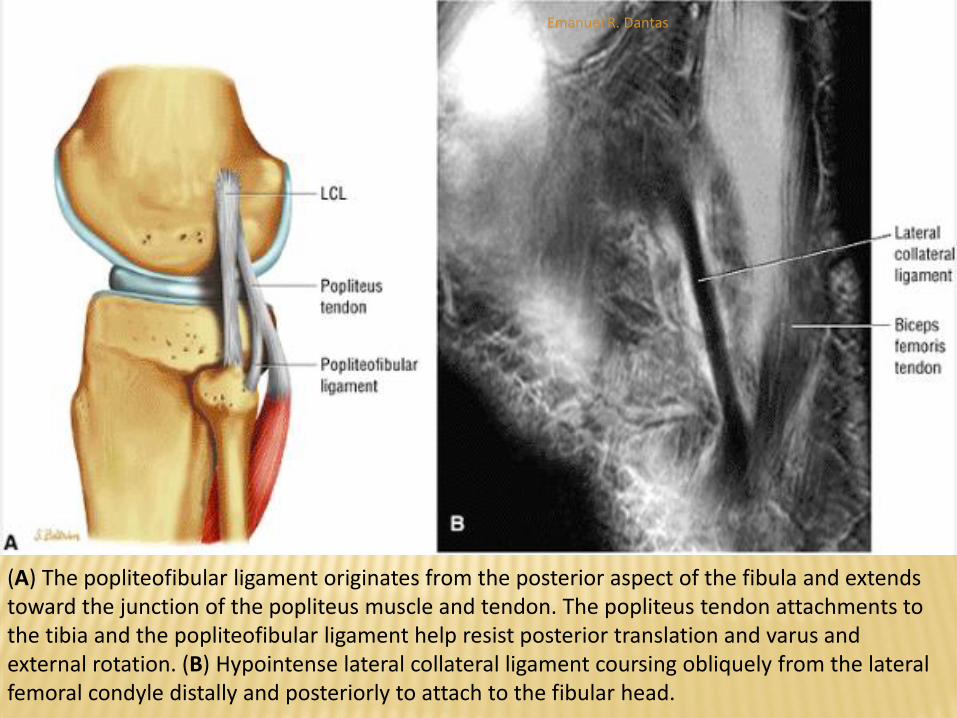
(A) The popliteofibular ligament originates from the posterior aspect of the fibula and extends toward the junction of the popliteus muscle and tendon. The popliteus tendon attachments to the tibia and the popliteofibular ligament help resist posterior translation and varus and external rotation. (B) Hypointense lateral collateral ligament coursing obliquely from the lateral femoral condyle distally and posteriorly to attach to the fibular head.
Emanuel R. Dantas
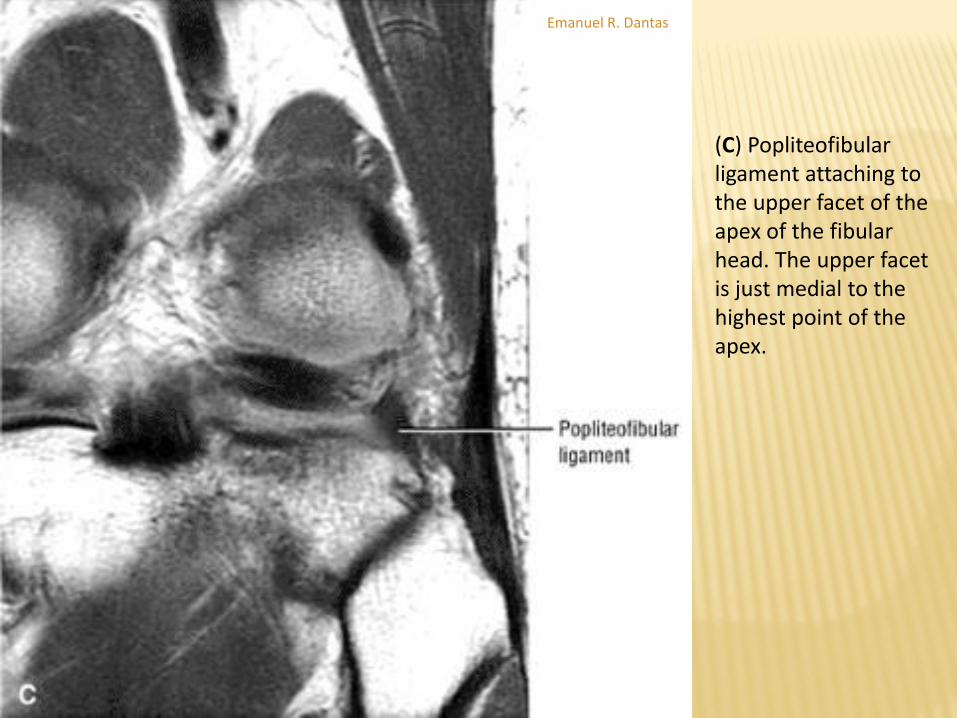
(C) Popliteofibular ligament attaching to the upper facet of the apex of the fibular head. The upper facet is just medial to the highest point of the apex.
Emanuel R. Dantas

LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
Functional Anatomy
The LCL, or fibular collateral ligament, is 5 to 7 cm long.
It is extracapsular and free from meniscal attachment in its course from the lateral femoral epicondyle to its conjoined insertion with the biceps femoris tendon on the fibular head.
The intracapsular popliteus tendon passes medial to the LCL, and the posterior fibers of the LCL blend with the deep capsule, which contributes to the arcuate ligament
Emanuel R. Dantas
LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
Location and Mechanism of Injury of the LCL and Posterolateral
Structures
The arcuate ligament and complex stabilize the posterolateral aspect of
the knee against varus and external rotation.
With the leg in internal rotation, an applied varus force can cause injury
to the LCL and capsule.
Injury or disruption of the LCL is significantly less common than injury to
the MCL.
Injury to the posterolateral corner can result from direct or noncontact
forces that cause knee hyperextension or hyperextension and external
rotation
MR imaging may reveal widening of the joint space, a fracture of the
fibular head, and a Segond fracture, in association with ACL injuries
Emanuel R. Dantas

Acute Segond fracture with osseous avulsion secondary to the pull of the posterior fibers of the ITB on (A) coronal FS PD FSE and (B) axial FS PD FSE images.
Emanuel R. Dantas
LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
MR Appearance
Edema and hemorrhage, although less frequent in this location, are seen as ligamentous thickening with increased signal intensity on T2- or FSE PD-weighted images (with FS).
Edema and hemorrhage may also be confirmed on peripheral sagittal images.
Signal intensity is not as high in LCL injuries as in MCL disruptions, perhaps because the normal capsular separation of the LCL excludes accumulation of extravasated joint fluid.
In complete disruptions, the LCL demonstrates a wavy or serpiginous contour and loss of ligamentous continuity.
There may be proximal migration of the avulsed ligament from its fibular attachment
Emanuel R. Dantas
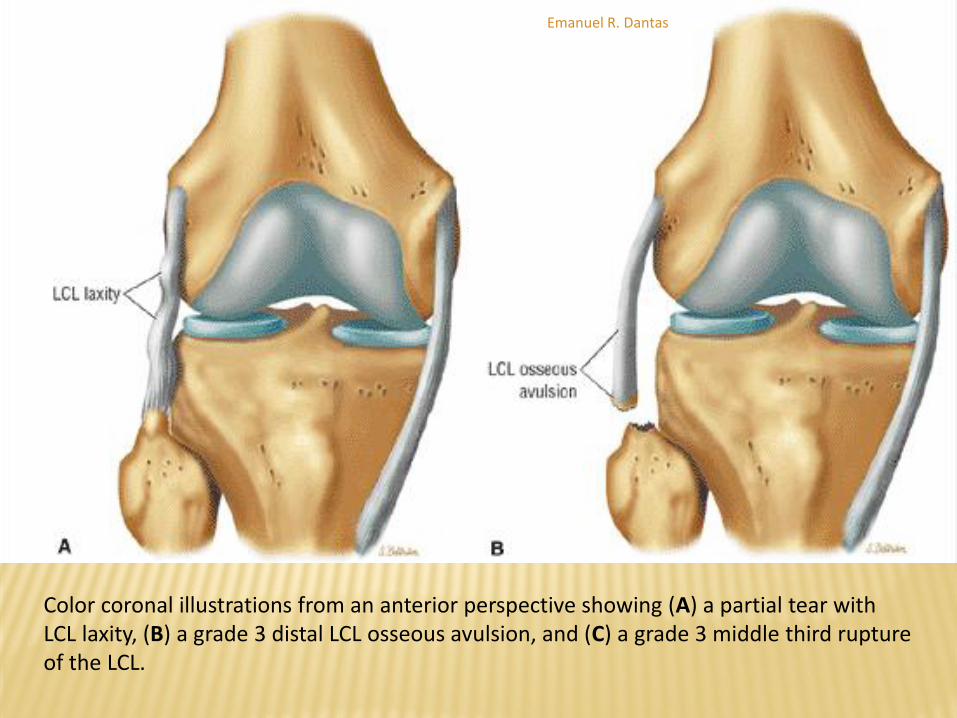
Color coronal illustrations from an anterior perspective showing (A) a partial tear with LCL laxity, (B) a grade 3 distal LCL osseous avulsion, and (C) a grade 3 middle third rupture of the LCL.
Emanuel R. Dantas

Color coronal illustrations from an anterior perspective showing (A) a partial tear with LCL laxity, (B) a grade 3 distal LCL osseous avulsion, and (C) a grade 3 middle third rupture of the LCL.
Emanuel R. Dantas

LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
MR Appearance
Biceps femoris and LCL injuries may be associated and
can be evaluated on coronal or sagittal images.
Popliteofibular ligament or combined popliteofibular,
fabellofibular, and arcuate ligament avulsions are more
commonly associated with fibular avulsion fractures
(styloid) compared to the more lateral LCL avulsions.
FS PD FSE axial images are also important in
diagnosing ligament tears when the course of the entire
LCL cannot be visualized on coronal images.
Emanuel R. Dantas

A distal avulsion of the lateral collateral ligament and biceps femoris tendon associated with a grade 3 proximal PCL tear as seen on (A) coronal PD FSE, (B) axial FS PD FSE, and (C) sagittal FS PD FSE images.
Emanuel R. Dantas
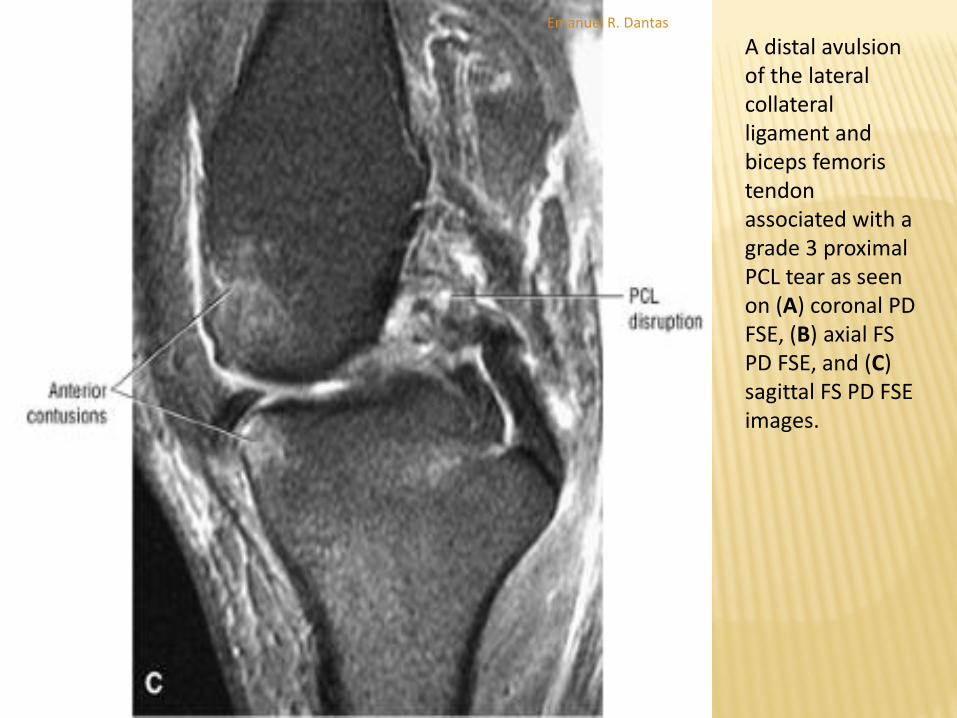
A distal avulsion of the lateral collateral ligament and biceps femoris tendon associated with a grade 3 proximal PCL tear as seen on (A) coronal PD FSE, (B) axial FS PD FSE, and (C) sagittal FS PD FSE images.
Emanuel R. Dantas

The popliteofibular ligament attaches to the upper facet of the apex of the fibular head medial to the insertions of the fabellofibular and arcuate ligaments. The lateral collateral ligaments and the direct arm of the long head of the biceps femoris tendon are attached more peripherally to the lateral margin of the fibular head.
Emanuel R. Dantas

Popliteofibular and arcuate ligament avulsion at the fibular apex with lateral collateral ligament and biceps femoris avulsion at the lateral margin of the fibular head. (A) Coronal PD FSE image. (B) Sagittal FS FSE image. (C) Coronal FS PD FSE image. (D) Axial FS PD FSE image.
Emanuel R. Dantas
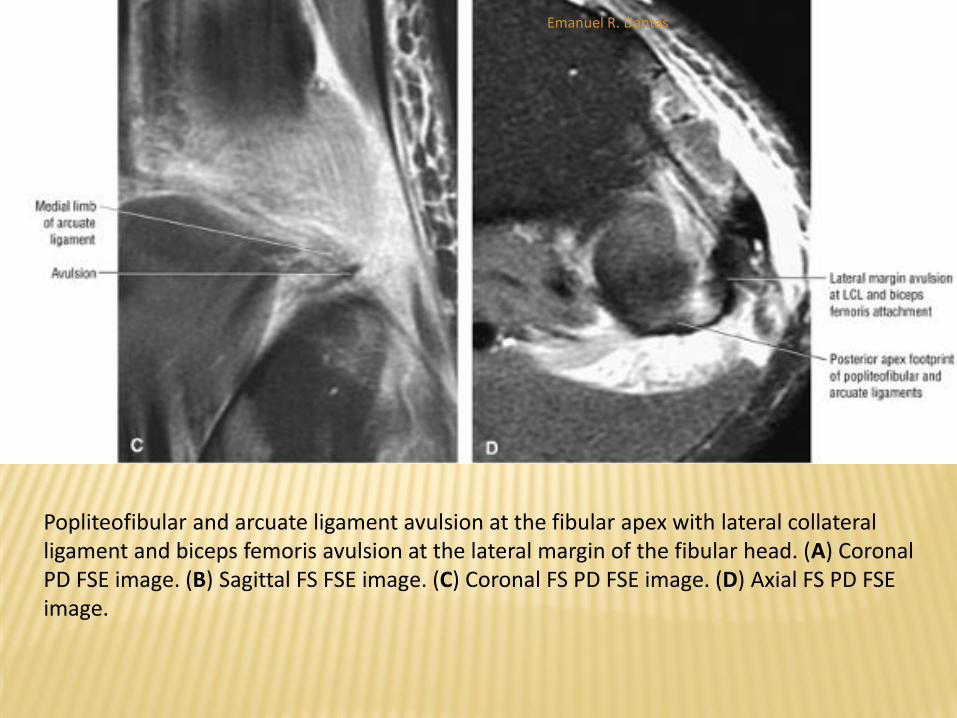
Popliteofibular and arcuate ligament avulsion at the fibular apex with lateral collateral ligament and biceps femoris avulsion at the lateral margin of the fibular head. (A) Coronal PD FSE image. (B) Sagittal FS FSE image. (C) Coronal FS PD FSE image. (D) Axial FS PD FSE image.
Emanuel R. Dantas
LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
MR Appearance
Tears of the ITB may also be associated with LCL
disruptions.
There is an association among LCL tears, popliteus tendon
ruptures (at the fossa), and iliotibial tract disruptions.
Inclusion of the ITB on anterior coronal images is important
if this structure is to be used to reconstruct the LCL.
The ITB, which provides lateral compartment support, is
seen as a thin band of low signal intensity, parallel to the
femur, with an anterolateral tibial insertion on Gerdy's
tubercle.
Emanuel R. Dantas

Proximal disruption of the lateral collateral ligament and popliteus tendon associated with distal iliotibial tract tear. A biceps femoris muscle sprain is shown proximally. (A) Coronal PD FSE image. (B) Axial FS PD FSE image. (C) Sagittal FS PD FSE image. (D) Coronal FS PD FSE image.
Emanuel R. Dantas

Proximal disruption of the lateral collateral ligament and popliteus tendon associated with distal iliotibial tract tear. A biceps femoris muscle sprain is shown proximally. (A) Coronal PD FSE image. (B) Axial FS PD FSE image. (C) Sagittal FS PD FSE image. (D) Coronal FS PD FSE image.
Emanuel R. Dantas

LATERAL COLLATERAL LIGAMENT AND
POSTEROLATERAL CORNER
MR Appearance
Popliteus and related posterolateral injuries are best displayed on FS PD-weighted FSE or STIR sagittal and axial images.
Areas of muscle edema and hemorrhage can be evaluated in these planes.
Focal enlargement of the popliteus muscle may be secondary to hemorrhage or tearing of muscle fibers.
Areas of increased signal intensity can be visualized at the muscle–tendon junction on sagittal images in conjunction with ACL and posterolateral corner injuries.
The popliteus muscle and tendon are associated with concomitant injuries to the posterolateral complex. Although rare, there are reports of isolated popliteus tendon rupture
Emanuel R. Dantas

Isolated proximal popliteus tendon tear on a coronal FS PD FSE image.
Emanuel R. Dantas
PATELLOFEMORAL JOINT AND THE EXTENSOR
MECHANISM
Pearls and Pitfalls
The medial patellar facet has a convex articular surface,
whereas the lateral patellar facet has a concave
articular surface.
The medial facet of the patella is divided into a medial
odd facet and a lateral middle facet. The middle facet is
thus located between the lateral and odd patellar facets.
The excessive lateral pressure syndrome is associated
with lateral patellar facet chondromalacia and edema of
the proximal lateral aspect of Hoffa's fat pad.
Emanuel R. Dantas
PATELLOFEMORAL JOINT AND THE EXTENSOR
MECHANISM
Patellar Anatomy
The patella is a sesamoid bone contained within the
quadriceps tendon.
It functions both to protect the femoral articular surface as
well as to increase the efficiency of the quadriceps
mechanism by virtue of the fulcrum effect.
The articular surface of the patella is roughly oval and is
divided into medial and lateral facets by a vertical ridge that
is oriented in the long axis of the patella.
The facets may be of equal size, although predominance of
the lateral facet is more common.
Emanuel R. Dantas

PATELLOFEMORAL JOINT AND THE EXTENSOR
MECHANISM
Patellar Anatomy
The medial facet demonstrates considerable anatomic variation.
It is subdivided by a small vertical ridge (the secondary ridge) into the
medial facet proper and a smaller odd facet along its medial border.
The secondary ridge runs in a longitudinal oblique direction and is closer
to the midline proximally than distally.
The odd facet, which is concave or flat, may be in the same plane as the
medial facet or may be oriented at as much as a 60° angle to it.
The medial facet is usually flat or convex, with articular cartilage of
varying thickness.
The lateral facet is both longer and wider than the medial facet and is
concave in both vertical and transverse planes.
Emanuel R. Dantas

PATELLOFEMORAL JOINT AND THE EXTENSOR
MECHANISM
Patellar Anatomy
Wiberg291 proposed a three-part classification scheme to describe the majority of patellar facet configurations.
The system was based upon the configuration of the subchondral bone of the facets as depicted on tangential conventional radiographs:
In the Wiberg type 1 configuration, both facets are gently concave, symmetrical, and nearly equal in size.
In the type 2 configuration, the medial facet is smaller than the lateral, which remains concave. The medial facet is flat or convex. Type 2 is the most common configuration, accounting for up to 65% of patellae. The differences between type 1 and type 2 patellae represent a continuum and may be subtle.
In the type 3 configuration, the medial facet is distinctly smaller, and there is marked lateral predominance. This configuration accounts for approximately 25% of patellae.
Emanuel R. Dantas
PATELLOFEMORAL JOINT AND THE EXTENSOR
MECHANISM
Patella Alta and Patella Baja
Patellar height is considered to be normal when the inferior pole of the patella is positioned in the superior aspect of the femoral trochlear groove.
Patella alta, an abnormally high position of the patella, is diagnosed when the inferior pole of the patella is positioned above the superior aspect of the femoral trochlear groove with the joint extended.
It is associated with various patellofemoral problems, including patellofemoral joint instability, patellar dislocation, and chondromalacia patellae, and is found more often in women than in men.
Patella baja, an abnormally low position of the patella, is diagnosed when the entire patella is positioned in or below the femoral trochlear groove with the joint extended.
It is often seen in young adult athletes in conjunction with Osgood-Schlatter disease297 (a traumatic disturbance in the development of the tibial tuberosity in adolescents).
Emanuel R. Dantas

CHONDROMALACIA
Pearls and Pitfalls
Chondromalacia is commonly associated with patellofemoral overload or malalignment.
FS PD FSE images identify basal, intrasubstance, and surface chondral defects.
The patellar facets are evaluated on axial images, whereas trochlear groove articular cartilage is assessed on sagittal images. Patellar subchondral sclerosis is associated with chronic chondral injuries.
Emanuel R. Dantas

CHONDROMALACIA
Chondromalacia patellae is characterized by patellofemoral (i.e., retropatellar) joint pain, accentuated during knee flexion, and associated crepitus.
Softening of the articular cartilage with associated degenerative changes is responsible for the spectrum of changes seen.
Chondromalacia most often affects adolescents and young adults and may be primary and idiopathic or occur subsequent to patellar trauma.
Emanuel R. Dantas
CHONDROMALACIA
MR Appearance of Chondromalacia
Outerbridge311,312 has classified chondromalacia into five arthroscopic grades:
In grade 0 chondromalacia, the articular cartilage is normal.
In grade 1 chondromalacia, there is discoloration of the articular cartilage, sometimes accompanied by blistering, usually without fragmentation or fissuring. Blistering represents separation of the superficial layer of articular cartilage. Localized softening, swelling, and fibrillation are limited to an area of 0.5 cm or less in diameter.
In grade 2 disease, fissuring and fibrillation within soft areas of the articular cartilage may extend to a depth of 1 to 2 mm and to an area of 1.3 cm or less in diameter.
Emanuel R. Dantas

CHONDROMALACIA
MR Appearance of Chondromalacia
Outerbridge311,312 has classified chondromalacia into five arthroscopic grades:
In grade 3 chondromalacia, fissuring and fibrillation may involve more than half of the depth of the articular cartilage thickness and an area greater than 1.3 cm in diameter. The articular cartilage surface resembles crabmeat, with fasciculation of multiple cartilaginous fragments attached to the underlying subchondral bone. There is no involvement of subchondral bone, however.
In grade 4 (i.e., end-stage) chondromalacia, complete loss or erosion of the articular cartilage surface results in exposed subchondral bone.
Emanuel R. Dantas
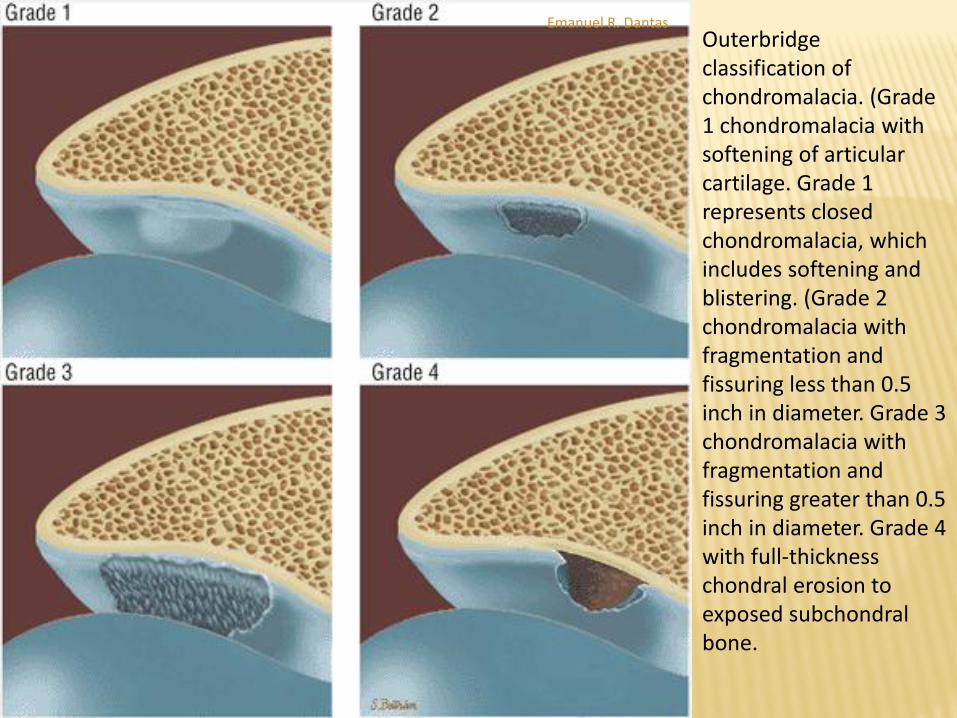
Outerbridge classification of chondromalacia. (Grade 1 chondromalacia with softening of articular cartilage. Grade 1 represents closed chondromalacia, which includes softening and blistering. (Grade 2 chondromalacia with fragmentation and fissuring less than 0.5 inch in diameter. Grade 3 chondromalacia with fragmentation and fissuring greater than 0.5 inch in diameter. Grade 4 with full-thickness chondral erosion to exposed subchondral bone.
Emanuel R. Dantas

CHONDROMALACIA
Cartilage Changes in Chrondromalacia Grade 1
In arthroscopic grade 1 chondromalacia, T1-weighted images show focal areas of decreased signal intensity without cartilage surface or subchondral bone extension.
FS PD-weighted FSE images display focal areas of hyperintensity in the absence of any discontinuity in the smooth superficial cartilage contour.
Early-stage blister formation with focal chondral convexity may also be observed.
We consider the blister lesion as part of cartilage softening and swelling in grade 1.
On FS PD-weighted FSE images, small irregularities (<1 mm) in the articular cartilage surface may be seen.
These irregularities represent the earliest changes of softening and swelling of articular cartilage.
Emanuel R. Dantas
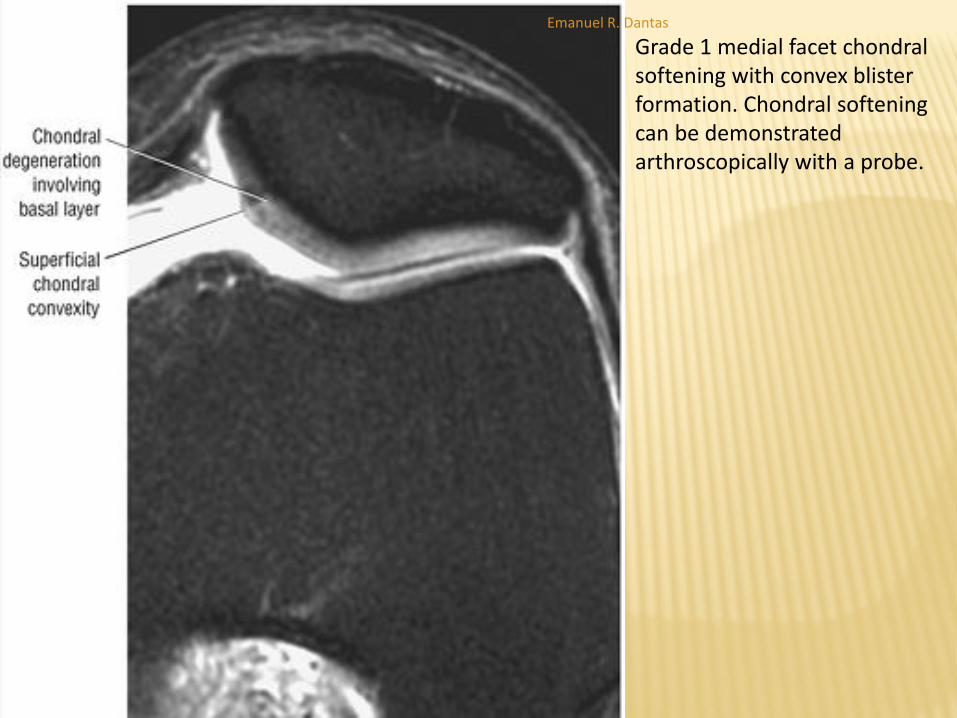
Grade 1 medial facet chondral softening with convex blister formation. Chondral softening can be demonstrated arthroscopically with a probe.
Emanuel R. Dantas
CHONDROMALACIA
Cartilage Changes in Chrondromalacia
Grade 2
In grade 2 chondromalacia, in addition to blister-like
swelling, there may be fissuring and fragmentation
confined to a small area (usually <1.3 cm).
FS PD-weighted FSE images demonstrate hyperintense
superficial or deep fissures.
Intracartilaginous hyperintensity may also be seen with
superficial and focal surface irregularity.
Emanuel R. Dantas

Superficial fissure of the medial aspect of the lateral patellar facet in grade 2 chondromalacia. This fissure produces a small flap because its orientation is parallel or tangential to the articular cartilage surface.
Emanuel R. Dantas

(A) Deep lateral patellar facet fissure on transverse color illustration. (B, C) Deep fissuring of the medial aspects of the lateral facets and lateral aspects of the medial facet. In its most frequent location chondromalacia traverses the central area (ridge) of the patella with sparing of the superior and inferior thirds of the articular surface. Deep fissures extending to subchondral bone can be seen in grade 2 chondromalacia in both the Outerbridge and Insall classifications. (B) Axial T1-weighted FSE image. (C) FS PD FSE image.
Emanuel R. Dantas

(A) Deep lateral patellar facet fissure on transverse color illustration. (B, C) Deep fissuring of the medial aspects of the lateral facets and lateral aspects of the medial facet. In its most frequent location chondromalacia traverses the central area (ridge) of the patella with sparing of the superior and inferior thirds of the articular surface. Deep fissures extending to subchondral bone can be seen in grade 2 chondromalacia in both the Outerbridge and Insall classifications. (B) Axial T1-weighted FSE image. (C) FS PD FSE image.
Emanuel R. Dantas
CHONDROMALACIA
Cartilage Changes in Chrondromalacia
Grade 3
On T1-weighted images, the surface irregularity and attenuation seen in arthroscopic grade 3 lesions directly correlate with focal areas of decreased signal intensity associated with loss of the sharp articular margin between the patellar and trochlear surfaces.
On FS PD-weighted FSE images the imbibed fluid in surface articular cartilage defects is seen as high-signal-intensity sites.
Axial or sagittal FS PD FSE scans are also helpful in identification of focal ulcerations and resolution of “crabmeat” lesions .
Basal degeneration may be seen in association with surface fibrillation in grade 3.
A spectrum of grades of chondral loss may be seen in the same patella.
Emanuel R. Dantas

“Crabmeat” erosion centered on the patellar ridge. The fragmentation and fissuring in grade 3 is also referred to as fibrillation. (A) Axial FS PD FSE image. (B) Sagittal FS PD FSE image.
Emanuel R. Dantas

CHONDROMALACIA
Cartilage Changes in Chrondromalacia
Grade 4
Ulceration and exposure of subchondral bone seen in arthroscopic grade 4 are represented on MR images by frank articular cartilage defects, exposed subchondral bone, and underlying fluid.
On T1-weighted images there are low-signal-intensity changes in the subchondral bone of the medial and lateral patellar facets.
These areas may be hyperintense on FS PD-weighted FSE or STIR images.
The precise depth of articular cartilage fissures or ulceration is best determined on FS PD-weighted FSE images.
MR sagittal images often demonstrate reciprocal subchondral bone changes in the femoral trochlear groove and patellar facet .
Trochlear groove involvement may also present with minimal patellar facet changes.
Emanuel R. Dantas

Lateral patellar facet full-thickness chondral erosion with increasing age. Erosion to subchondral bone is more commonly seen in the lateral patellar facet. (A) Axial FS PD FSE image. (B) Sagittal FS PD FSE image.
Emanuel R. Dantas
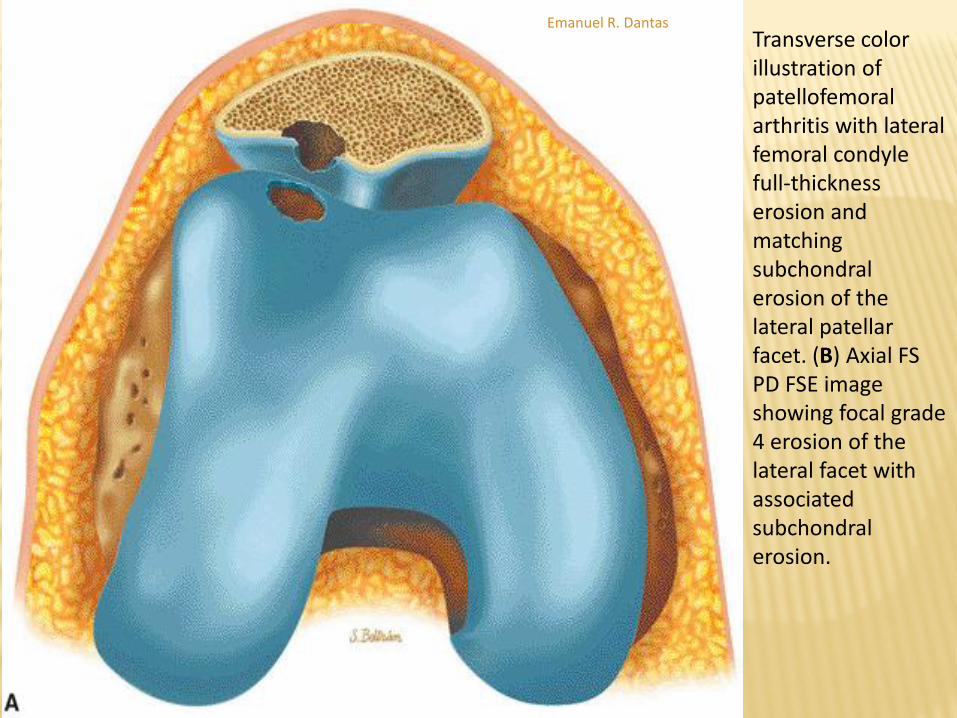
Transverse color illustration of patellofemoral arthritis with lateral femoral condyle full-thickness erosion and matching subchondral erosion of the lateral patellar facet. (B) Axial FS PD FSE image showing focal grade 4 erosion of the lateral facet with associated subchondral erosion.
Emanuel R. Dantas

Transverse color illustration of patellofemoral arthritis with lateral femoral condyle full-thickness erosion and matching subchondral erosion of the lateral patellar facet. (B) Axial FS PD FSE image showing focal grade 4 erosion of the lateral facet with associated subchondral erosion.
Emanuel R. Dantas