jas-world aids day ppt
TRANSCRIPT
HIV/AIDS

WORKSHOP ON WORLD AIDS DAY

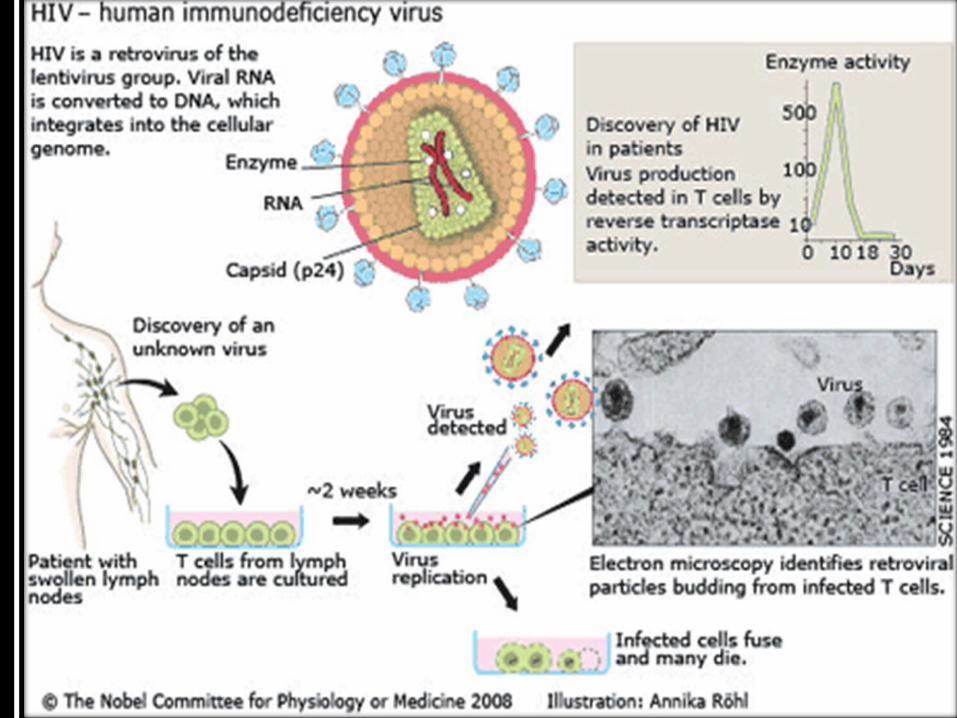
H Human
I Immunodeficiency
V Virus

A Acquired
I Immuno
D Deficiency
S Syndrome

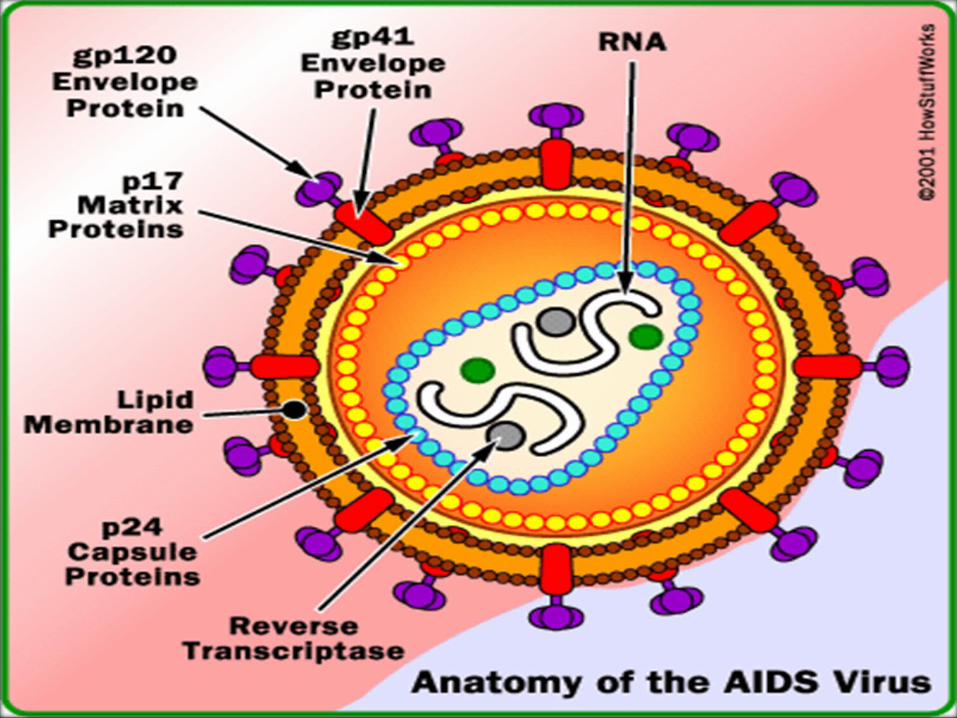
HIV - virusHIV - virusHIV - virusHIV - virus
membrane:derived from the host cell membrane
two kinds of glycoproteins: gp160 gp120 and gp41
gp41 is a transmembrane protein, and gp120 is an external protein, noncovalently associated with membrane.

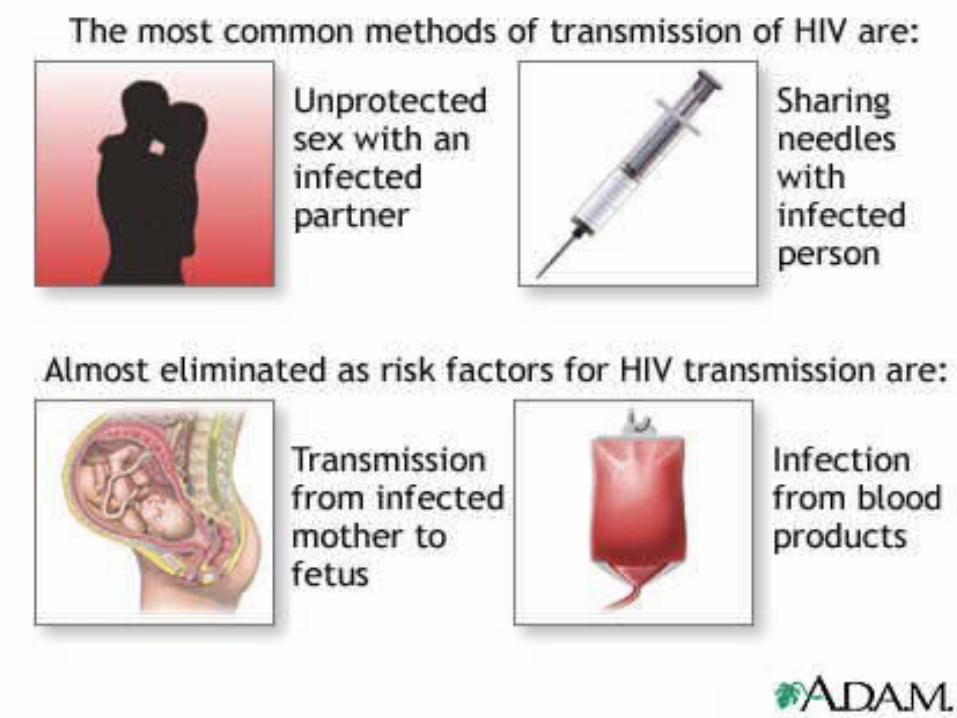
HIV Transmission
• Common fluids that are a means of transmission:
– Blood
– Semen
– Vaginal Secretions
– Breast Milk

epidemiology 、 prevention and cure
major group at risk : homosexual 、 drug abusers、
infected blood or blood products
spread manner : sexual contact 、 blood 、 mother-to-
child transmission
HIV Transmission
• HIV enters the bloodstream through:
– Open Cuts
– Breaks in the skin
– Mucous membranes
– Direct injection

HIV in Body Fluids
Semen11,000 Vaginal
Fluid7,000
Blood18,000
Amniotic Fluid4,000 Saliva
1
Average number of HIV particles in 1 ml of these body fluids
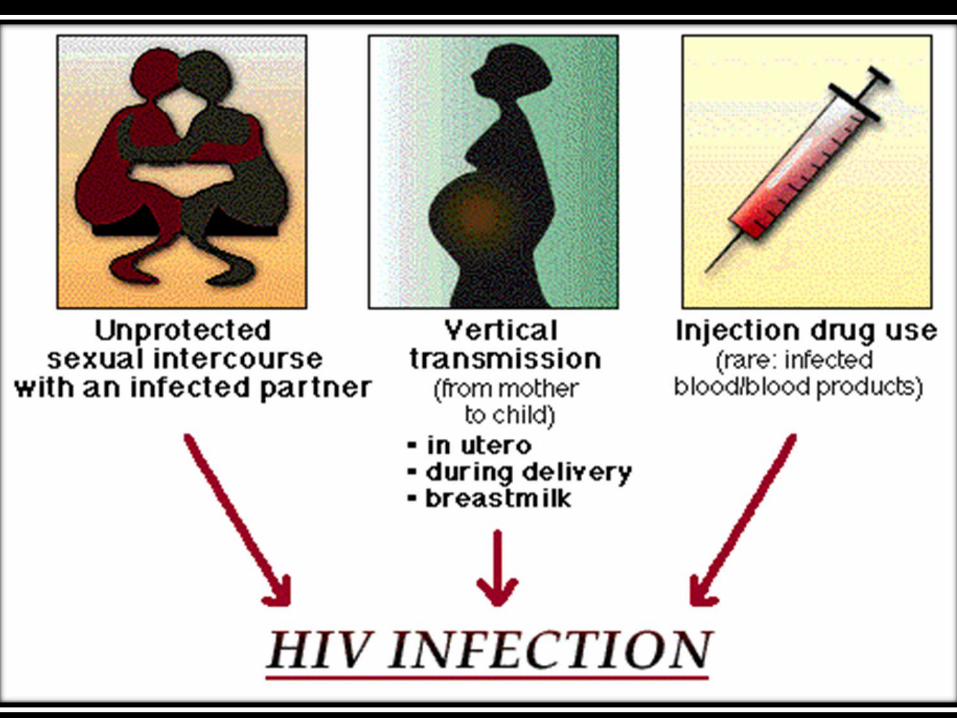
Routes of Transmission of HIV
Sexual Contact: Male-to-maleMale-to-female or vice versaFemale-to-female
Blood Exposure: Injecting drug use/needle sharing Occupational exposure Transfusion of blood products
Perinatal: Transmission from mom to babyBreastfeeding

HIV - life cycleHIV - life cycleHIV - life cycleHIV - life cycle
enter into cell
CD4+T cell is the major target cell
human HeLa cells
human HeLa cells transfected with
CD4 antigen
without infection infection

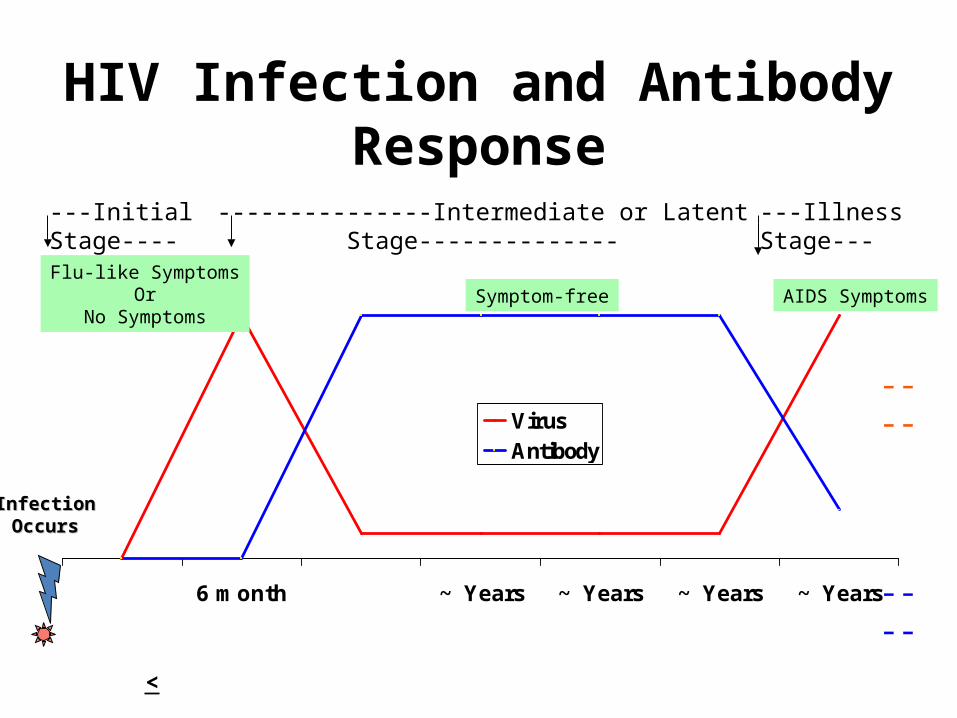
HIV Infection and Antibody Response
6 month ~ Years ~ Years ~ Years ~ Years
VirusAntibody
InfectionInfectionOccursOccurs
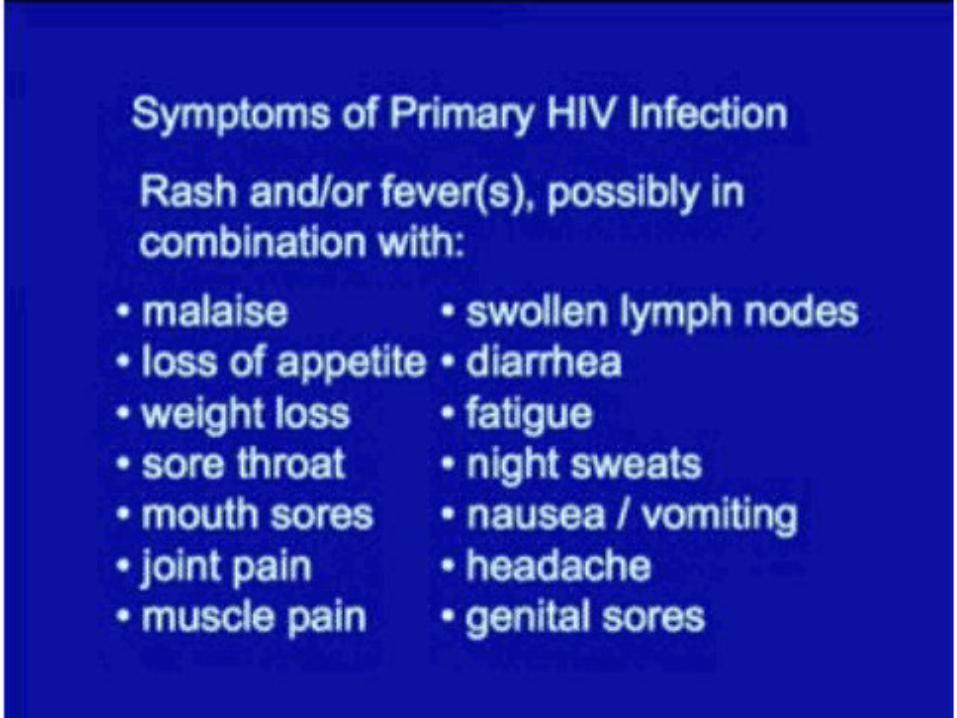
AIDS Symptoms
---Initial Stage---- ---------------Intermediate or Latent Stage-------------- ---Illness Stage---
Flu-like SymptomsOr
No SymptomsSymptom-free
<
----
----

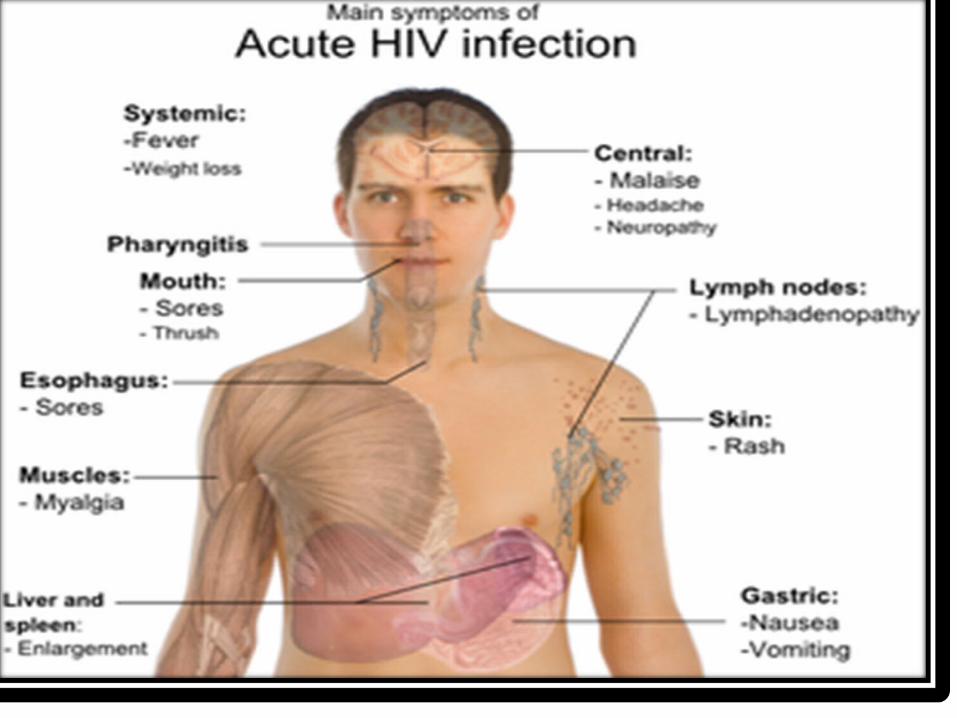
Clinical features
Latent period : 6 month—4 year
Infection phase: influenza-like symptom 、 infectious
Abs production : 3-20 weeks
symptom : AIDS related complex ARC
( 1) opportunistic infections
( 2) malignant tumors : Kaposi’s sarcoma 、malignant , lymphoma
( 3) abnormal of the central nervous system



PATHOGENESIS
• Hallmark of HIV disease is a profound immunodeficiency resulting primarily from a progressive quantitative & qualitative deficiency of the subset of T lymphocytes referred to as helper T cells or inducer T cells.

HIV-Infected T-Cell
HIVVirus
T-CellHIV Infected
T-Cell
New HIVVirus
Window Period
• This is the period of time after becoming infected when an HIV test is negative
• 90 percent of cases test positive within three months of exposure
• 10 percent of cases test positive within three to six months of exposure


WHO Case Definitions
• Case definition for HIV/AIDS is fulfilled in the presence of at least 2 major signs and at least 1 minor sign:– Major signs (weight loss, chronic diarrhea,
prolonged fever)– Minor signs (persistent cough, herpes
zoster, oropharyngeal candidiasis, etc.)
Where HIV testing is not available, patients can be diagnosed clinically based on major and minor signs and symptoms

WHO Case Definitions
Where HIV testing is available• The case definition for HIV/AIDS is fulfilled if
an HIV test is positive and one or more of the following conditions is present:
• HIV encephalopathy• Esophageal candidiasis• Life threatening or recurrent
pneumonia• Invasive cervical cancer

WHO Case Definitions
Where HIV testing is available• The case definition for HIV/AIDS is fulfilled if
an HIV test is positive and one or more of the following conditions is present:
• Weight loss • Cryptococcal meningitis• Tuberculosis• Kaposi’s sarcoma
• HIV encephalopathy• Esophageal candidiasis• Life threatening or recurrent
pneumonia• Invasive cervical cancer
WHO Clinical Staging System
• The WHO clinical staging system includes: – a clinical classification system– a laboratory classification to categorize the
immunosuppression of adults by their total lymphocyte counts
• This staging system has proven reliable for predicting morbidity and mortality in infected adults
• The WHO Clinical Staging System is based on clinical markers believed to have prognostic significance resulting in four categories

WHO Clinical Staging SystemClinical Stage 1
1. Asymptomatic infection
2. Persistent generalized lymphadenopathy (PGL)
3. Acute retroviral infection
Clinical Stage 2
4. Unintentional weight loss, < 10%
5. Minor mucocutaneous manifestations
6. Herpes zoster, within previous 5 years
7. Recurrent upper respiratory tract infections

WHO Clinical Staging System
8. Unintentional weight loss, >10%
9. Chronic diarrhea
10.Prolonged fever
11.Oral candidiasis
12.Oral hairy leukoplakia
13.Pulmonary tuberculosis
14.Severe bacterial infections
15.Vulvovaginal candidiasis
Clinical Stage 3
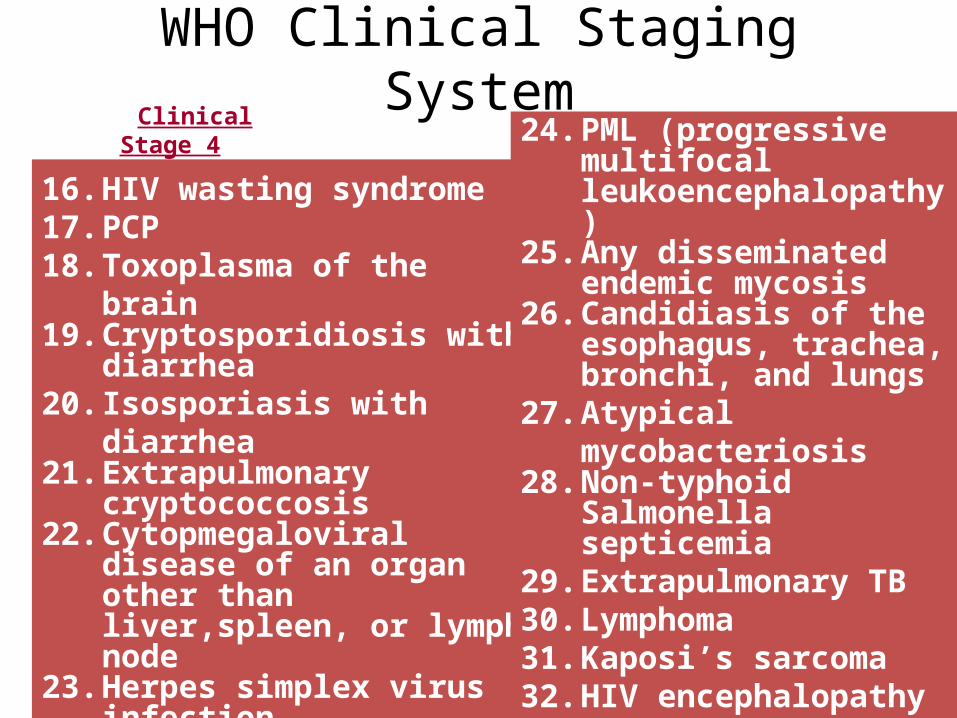
WHO Clinical Staging SystemClinical
Stage 4
16. HIV wasting syndrome17. PCP18. Toxoplasma of the brain19. Cryptosporidiosis with
diarrhea20. Isosporiasis with diarrhea21. Extrapulmonary
cryptococcosis22. Cytopmegaloviral disease
of an organ other than liver,spleen, or lymph node
23. Herpes simplex virus infection
24. PML (progressive multifocal leukoencephalopathy)
25. Any disseminated endemic mycosis
26. Candidiasis of the esophagus, trachea, bronchi, and lungs
27. Atypical mycobacteriosis
28. Non-typhoid Salmonella septicemia
29. Extrapulmonary TB30. Lymphoma31. Kaposi’s sarcoma32. HIV encephalopathy
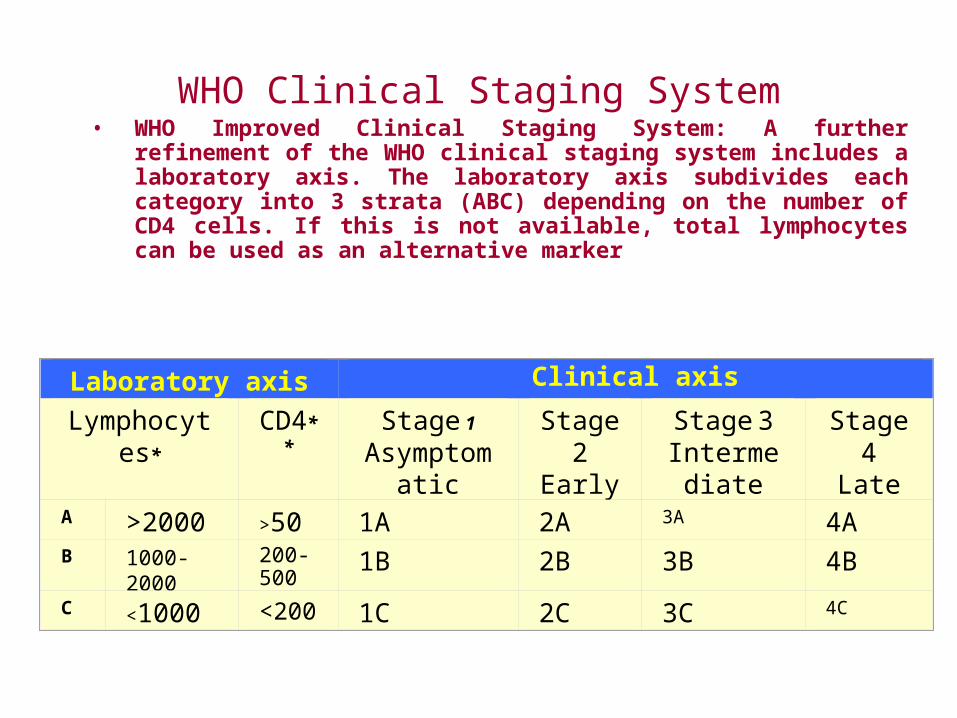
WHO Clinical Staging System• WHO Improved Clinical Staging System: A further refinement of
the WHO clinical staging system includes a laboratory axis. The laboratory axis subdivides each category into 3 strata (ABC) depending on the number of CD4 cells. If this is not available, total lymphocytes can be used as an alternative marker
Laboratory axis Clinical axis
Lymphocytes* CD4** Stage 1
AsymptomaticPGL
Stage 2Early
HIV
Stage 3Intermediate
(ARC)***
Stage 4Late
AIDSA >2000 >500 1A 2A 3A 4AB 1000- 2000 200-
5001B 2B 3B 4B
C <1000 <200 1C 2C 3C 4C
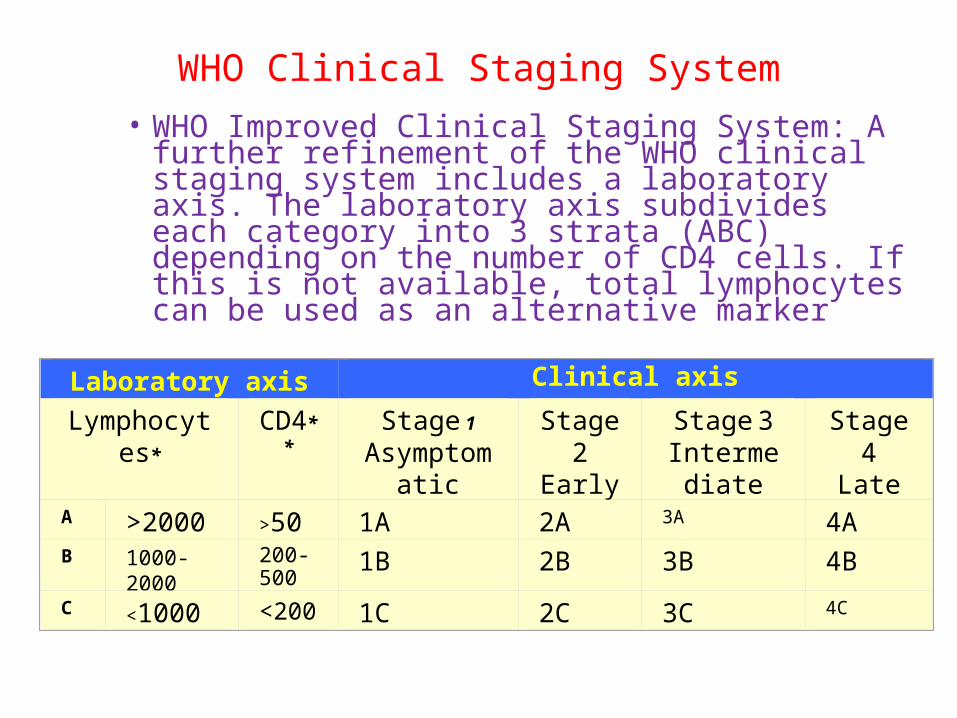
WHO Clinical Staging System• WHO Improved Clinical Staging System: A further
refinement of the WHO clinical staging system includes a laboratory axis. The laboratory axis subdivides each category into 3 strata (ABC) depending on the number of CD4 cells. If this is not available, total lymphocytes can be used as an alternative marker
Laboratory axis Clinical axis
Lymphocytes* CD4** Stage 1
AsymptomaticPGL
Stage 2Early
HIV
Stage 3Intermediate
(ARC)***
Stage 4Late
AIDSA >2000 >500 1A 2A 3A 4AB 1000- 2000 200-
5001B 2B 3B 4B
C <1000 <200 1C 2C 3C 4C


Importance of Early Testing and Diagnosis
• Allows for early treatment to maintain and stabilize the immune system response
• Decreases risk of HIV transmission from mother to newborn baby
• Allows for risk reduction education to reduce or eliminate high-risk behavior

HIV Testing
• Requires a blood or oral fluid sample
• HIV test detects the body’s antibody response to HIV infection
• The test does NOT detect the HIV virus

HIV testing policy
• No mandatory testing.• HIV testing should not be imposed as a precondition
for employment /providing health care facilities.• Voluntary HIV testing should be done with pretest and
post test counseling.• Strict confidentiality of result should be maintained .

HIV testing policy conttt….
• Person should be encouraged to share the information with hi s family members.
• In case of marriage (If one partner insists on marriage ) the test should be done by
• The contracting party to the satisfaction of the person cocerned.
LABORATORY DIAGNOSIS
• IMMUNOLOGICAL TEST.• SPECIFIC TEST.

• (1) ELISA plate is coated with a capture antibody; • (2) Sample is added, and the respective antigen
present binds to capture antibody;• (3) Biotin-conjugated secondary detection
antibody is added, and binds to the antigen captured by the first antibody;
(4) Streptavidin-HRP is added and binds to the biotin conjugated detection antibody;
(5) Colored product is formed in proportion to the amount of antigen present in the sample; The reaction is terminated by addition of acid and absorbance is measured at 450 nm;

EIA/ELISATest
PositiveNegative
Run IFAConfirmation
RepeatPositive
Positive
End Testing
Repeat ELISAEvery 3 months
for 1 year
Negative
PositiveNegativeIndeterminate
Repeat at 2-4 months
Repeat at 3 weeks
HIV Testing
No HIV ExposureLow Risk
HIV ExposureHigh Risk
NegativeHIV
+
Repeat every 6 months for continued
High risk behavior


PRESENTED BY:-GAGAN DEEP KAUR


PREVENTION OF AIDS
• Avoiding AIDS as easy as...• A bstain• B e faithful• C ondomise

PREVENTION OF AIDS
• Don't share needles.• Limit your number of sexual partners. • Know that not all types of birth control will
protect you from HIV. • Don't use nonoxynol-9. .• Get screened for STIs. • Talk with your partner. • Don't douche.
• Once a person is infected they are always
infected
• Medications are available to prolong life but they do not cure the disease
• Those who are infected are capable of infecting others without having symptoms or knowing of the infection
HIV AIDS

HIV Risk Reduction
• Avoid unprotected sexual contact
• Use barriers such as condoms and dental dams
• Limit multiple partners by maintaining a long-term relationship with one person
• Talk to your partner about being tested before you begin a sexual relationship
HIV Risk Reduction
• Avoid drug and alcohol use to maintain good judgment
• Don’t share needles used by others for:Drugs
Tattoos Body piercing
• Avoid exposure to blood products

Condoms
Using condoms is not 100 percent effective in preventing transmission of sexually transmitted infections including HIV
Condoms = Safer sex
Condoms ≠ Safe sex

People Infected with HIV
• Can look healthy• Can be unaware of their infection• Can live long productive lives when
their HIV infection is managed• Can infect people when they engage in
high-risk behavior

HIV Exposure and Infection
• Some people have had multiple exposures without becoming infected
• Some people have been exposed one time and become infected

•COLOUR CODING TO PREVENT INFECTION



HIV and Sexually Transmitted Diseases

HIV and Sexually Transmitted Diseases
STDs increase infectivity of HIV
– A person co-infected with an STD and HIV may be more likely to transmit HIV due to an increase in HIV viral shedding
– More white blood cells, some carrying HIV, may be present in the mucosa of the genital area due to a sexually transmitted infection
HIV and Sexually Transmitted Diseases
• STDs increase the susceptibility to HIV– Ulcerative and inflammatory STDs compromise
the mucosal or cutaneous surfaces of the genital tract that normally act as a barrier against HIV
– Ulcerative STDs include: syphilis, chancroid, and genital herpes
– Inflammatory STDs include: chlamydia, gonorrhea, and trichomoniasis

HIV and Sexually Transmitted Diseases
• The effect of HIV infection on the immune system increases the the risk of STDs
A suppressed immune response due to HIV can:
• Increase the reactivation of genital ulcers• Increase the rate of abnormal cell growth • Increase the difficulty in curing reactivated or
newly acquired genital ulcers• Increase the risk of becoming infected with
additional STDs
HIV Post Exposure Prophylaxis

HIV Occupational Exposure
• Review facility policy and report the incident• Medical follow-up is necessary to determine
the exposure risk and course of treatment• Baseline and follow-up HIV testing• Four week course of medication initiated one to
two hours after exposure • Liver function tests to monitor medication
tolerance• Exposure precautions practiced
HIV Non-Occupational Exposure
• No data exists on the efficacy of antiretroviral medication after non-occupational exposures
• The health care provider and patient may decide to use antiretroviral therapy after weighing the risks and benefits
• Antiretrovirals should not be used for those with low-risk transmissions or exposures occurring more than 72 hours after exposure
PREVENTION --- FIRSTPREVENTION --- FIRST

HIV Non-Occupational Exposure
• Provider Considerations:
– Evaluate HIV status of patient and risk history of source patient
– Provide necessary medical care and counseling– Evaluate risk event and factors for exposure– Determine elapsed time from exposure– Evaluate potential for continuous HIV exposure– Obtain informed consent for testing and treatment– Evaluate pregnancy status of females– Monitor for drug toxicity and acute infection
