james b. hale, phd, med, abpdn, absnp - masp.mb.ca · reduced activation in right orbitofrontal...
TRANSCRIPT

School Neuropsychology of Behaviourand Psychopathology
James B Hale PhD MEd ABPdN ABSNPProfessor of Education and Medicine
University of Calgary
halejbucalgaryca
Kelly Ryan Hicks MScRegistered Psychologist
School Psychologist Calgary Board of Education
Manitoba Association of School Psychologists14-15 November 2013
bull Phineas Gage was a railroad foreman who
had a tamping pole blown through his
orbital and dorsolateral prefrontal regions
bull He was walking and talking a few minutes
after the injury but vomited sending more
brain tissue to the floor with swelling
leading to coma
bull Recovery was slow mood was variable
and he was disinhibited contentious and
socially inept so ldquono longer Gagerdquo
bull Frontal lobes and limbic system ldquoSeat of
Personalityrdquo and psychopathology (not far
off)
The Strange Case of Phineas Gage
Physiological Basis of Psychopathology
bull Eysenck (1967) Theory of Autonomic Arousal Internalizing and externalizing dimensions
Internalizers have cortical overarousal Cope by limiting environmental stimuli
Externalizers have cortical underarousal Cope by seeking environmental stimuli
Hemispheric Functions and Psychopathology
bull Sackheim (1982) review of hemispheric functions and psychopathology
Left hemisphere lesionsanesthetization and catastrophicdepressive reactions
Right hemisphere lesionsanesthetization and euphoricindifferent reactions
bull Davidsonrsquos (2000) work in brain functioning in typical populations
Left hemisphere activation = Positive affect The ldquoapproachrdquo hemisphere
Right hemisphere activation = Negative affect The ldquoavoidantrdquo hemisphere
bull Implications for discordant-divergent (new relationships) and concordant-convergent (known relationships) thought
Cortical-Subcortical Circuits and the Third Axis
Oculo-motor
Motor
BasalGanglia
Thalamus
Cingulate
Cerebellum
Working memory memoryencoding amp retrieval
Attention concentrationactivity and impulse control
Plan organize strategize implement monitor evaluate modify and amp change behaviour
Anterior Cingulate Circuit and Psychopathology
bull Cognitive Functions ndash arousal motivation performance monitoring switching behavioral initiation posterior-anterior communication online data processing manager (like RAM)
bull Dysfunction Psychopathologies ndash depression bipolar ADHD schizophrenia autism
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Apathy or poor motivation
Poor response control and shiftingswitching behavior
Difficulty with decision-making
Lack of enjoyment ndash anhedonia
Poor response to reinforcement
Slow processing speed
Limited idea generation and creativity
Dorsolateral Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash planning organizing strategizing monitoring evaluating shifting and changing behavior working memory memory encoding and retrieval strategy generation and hypothesis testing
bull Dysfunction Psychopathologies ndash depression schizophrenia ADHD autism
bull Associated Neuropsychological Deficits ndash External task-oriented executive skills
Difficulty with hypothesis generation and problem solving
Limited or excessive interest in environment
Poor sustained attention
Mental inflexibility
Decreased verbal and design fluency
Encoding andor retrieval from long-term memory deficits
Poor planning organization and checking behavior
Orbital Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash indirect influence on tasks emotional and behavioral self-regulation inhibition empathy social control integrating emotions into contextually relevant behavior
bull Dysfunction Psychopathologies ndash obsessive compulsive disorder anxiety disorder bipolar disorder conduct disorder
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Perseveration or disinhibition
Tactlessness
Irritability
Sexual deviance (extreme interest or disinterest)
Antisocial or asocial behaviors
Inappropriate feelings (eg sadness or euphoria)
Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

bull Phineas Gage was a railroad foreman who
had a tamping pole blown through his
orbital and dorsolateral prefrontal regions
bull He was walking and talking a few minutes
after the injury but vomited sending more
brain tissue to the floor with swelling
leading to coma
bull Recovery was slow mood was variable
and he was disinhibited contentious and
socially inept so ldquono longer Gagerdquo
bull Frontal lobes and limbic system ldquoSeat of
Personalityrdquo and psychopathology (not far
off)
The Strange Case of Phineas Gage
Physiological Basis of Psychopathology
bull Eysenck (1967) Theory of Autonomic Arousal Internalizing and externalizing dimensions
Internalizers have cortical overarousal Cope by limiting environmental stimuli
Externalizers have cortical underarousal Cope by seeking environmental stimuli
Hemispheric Functions and Psychopathology
bull Sackheim (1982) review of hemispheric functions and psychopathology
Left hemisphere lesionsanesthetization and catastrophicdepressive reactions
Right hemisphere lesionsanesthetization and euphoricindifferent reactions
bull Davidsonrsquos (2000) work in brain functioning in typical populations
Left hemisphere activation = Positive affect The ldquoapproachrdquo hemisphere
Right hemisphere activation = Negative affect The ldquoavoidantrdquo hemisphere
bull Implications for discordant-divergent (new relationships) and concordant-convergent (known relationships) thought
Cortical-Subcortical Circuits and the Third Axis
Oculo-motor
Motor
BasalGanglia
Thalamus
Cingulate
Cerebellum
Working memory memoryencoding amp retrieval
Attention concentrationactivity and impulse control
Plan organize strategize implement monitor evaluate modify and amp change behaviour
Anterior Cingulate Circuit and Psychopathology
bull Cognitive Functions ndash arousal motivation performance monitoring switching behavioral initiation posterior-anterior communication online data processing manager (like RAM)
bull Dysfunction Psychopathologies ndash depression bipolar ADHD schizophrenia autism
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Apathy or poor motivation
Poor response control and shiftingswitching behavior
Difficulty with decision-making
Lack of enjoyment ndash anhedonia
Poor response to reinforcement
Slow processing speed
Limited idea generation and creativity
Dorsolateral Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash planning organizing strategizing monitoring evaluating shifting and changing behavior working memory memory encoding and retrieval strategy generation and hypothesis testing
bull Dysfunction Psychopathologies ndash depression schizophrenia ADHD autism
bull Associated Neuropsychological Deficits ndash External task-oriented executive skills
Difficulty with hypothesis generation and problem solving
Limited or excessive interest in environment
Poor sustained attention
Mental inflexibility
Decreased verbal and design fluency
Encoding andor retrieval from long-term memory deficits
Poor planning organization and checking behavior
Orbital Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash indirect influence on tasks emotional and behavioral self-regulation inhibition empathy social control integrating emotions into contextually relevant behavior
bull Dysfunction Psychopathologies ndash obsessive compulsive disorder anxiety disorder bipolar disorder conduct disorder
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Perseveration or disinhibition
Tactlessness
Irritability
Sexual deviance (extreme interest or disinterest)
Antisocial or asocial behaviors
Inappropriate feelings (eg sadness or euphoria)
Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Physiological Basis of Psychopathology
bull Eysenck (1967) Theory of Autonomic Arousal Internalizing and externalizing dimensions
Internalizers have cortical overarousal Cope by limiting environmental stimuli
Externalizers have cortical underarousal Cope by seeking environmental stimuli
Hemispheric Functions and Psychopathology
bull Sackheim (1982) review of hemispheric functions and psychopathology
Left hemisphere lesionsanesthetization and catastrophicdepressive reactions
Right hemisphere lesionsanesthetization and euphoricindifferent reactions
bull Davidsonrsquos (2000) work in brain functioning in typical populations
Left hemisphere activation = Positive affect The ldquoapproachrdquo hemisphere
Right hemisphere activation = Negative affect The ldquoavoidantrdquo hemisphere
bull Implications for discordant-divergent (new relationships) and concordant-convergent (known relationships) thought
Cortical-Subcortical Circuits and the Third Axis
Oculo-motor
Motor
BasalGanglia
Thalamus
Cingulate
Cerebellum
Working memory memoryencoding amp retrieval
Attention concentrationactivity and impulse control
Plan organize strategize implement monitor evaluate modify and amp change behaviour
Anterior Cingulate Circuit and Psychopathology
bull Cognitive Functions ndash arousal motivation performance monitoring switching behavioral initiation posterior-anterior communication online data processing manager (like RAM)
bull Dysfunction Psychopathologies ndash depression bipolar ADHD schizophrenia autism
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Apathy or poor motivation
Poor response control and shiftingswitching behavior
Difficulty with decision-making
Lack of enjoyment ndash anhedonia
Poor response to reinforcement
Slow processing speed
Limited idea generation and creativity
Dorsolateral Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash planning organizing strategizing monitoring evaluating shifting and changing behavior working memory memory encoding and retrieval strategy generation and hypothesis testing
bull Dysfunction Psychopathologies ndash depression schizophrenia ADHD autism
bull Associated Neuropsychological Deficits ndash External task-oriented executive skills
Difficulty with hypothesis generation and problem solving
Limited or excessive interest in environment
Poor sustained attention
Mental inflexibility
Decreased verbal and design fluency
Encoding andor retrieval from long-term memory deficits
Poor planning organization and checking behavior
Orbital Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash indirect influence on tasks emotional and behavioral self-regulation inhibition empathy social control integrating emotions into contextually relevant behavior
bull Dysfunction Psychopathologies ndash obsessive compulsive disorder anxiety disorder bipolar disorder conduct disorder
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Perseveration or disinhibition
Tactlessness
Irritability
Sexual deviance (extreme interest or disinterest)
Antisocial or asocial behaviors
Inappropriate feelings (eg sadness or euphoria)
Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Hemispheric Functions and Psychopathology
bull Sackheim (1982) review of hemispheric functions and psychopathology
Left hemisphere lesionsanesthetization and catastrophicdepressive reactions
Right hemisphere lesionsanesthetization and euphoricindifferent reactions
bull Davidsonrsquos (2000) work in brain functioning in typical populations
Left hemisphere activation = Positive affect The ldquoapproachrdquo hemisphere
Right hemisphere activation = Negative affect The ldquoavoidantrdquo hemisphere
bull Implications for discordant-divergent (new relationships) and concordant-convergent (known relationships) thought
Cortical-Subcortical Circuits and the Third Axis
Oculo-motor
Motor
BasalGanglia
Thalamus
Cingulate
Cerebellum
Working memory memoryencoding amp retrieval
Attention concentrationactivity and impulse control
Plan organize strategize implement monitor evaluate modify and amp change behaviour
Anterior Cingulate Circuit and Psychopathology
bull Cognitive Functions ndash arousal motivation performance monitoring switching behavioral initiation posterior-anterior communication online data processing manager (like RAM)
bull Dysfunction Psychopathologies ndash depression bipolar ADHD schizophrenia autism
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Apathy or poor motivation
Poor response control and shiftingswitching behavior
Difficulty with decision-making
Lack of enjoyment ndash anhedonia
Poor response to reinforcement
Slow processing speed
Limited idea generation and creativity
Dorsolateral Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash planning organizing strategizing monitoring evaluating shifting and changing behavior working memory memory encoding and retrieval strategy generation and hypothesis testing
bull Dysfunction Psychopathologies ndash depression schizophrenia ADHD autism
bull Associated Neuropsychological Deficits ndash External task-oriented executive skills
Difficulty with hypothesis generation and problem solving
Limited or excessive interest in environment
Poor sustained attention
Mental inflexibility
Decreased verbal and design fluency
Encoding andor retrieval from long-term memory deficits
Poor planning organization and checking behavior
Orbital Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash indirect influence on tasks emotional and behavioral self-regulation inhibition empathy social control integrating emotions into contextually relevant behavior
bull Dysfunction Psychopathologies ndash obsessive compulsive disorder anxiety disorder bipolar disorder conduct disorder
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Perseveration or disinhibition
Tactlessness
Irritability
Sexual deviance (extreme interest or disinterest)
Antisocial or asocial behaviors
Inappropriate feelings (eg sadness or euphoria)
Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
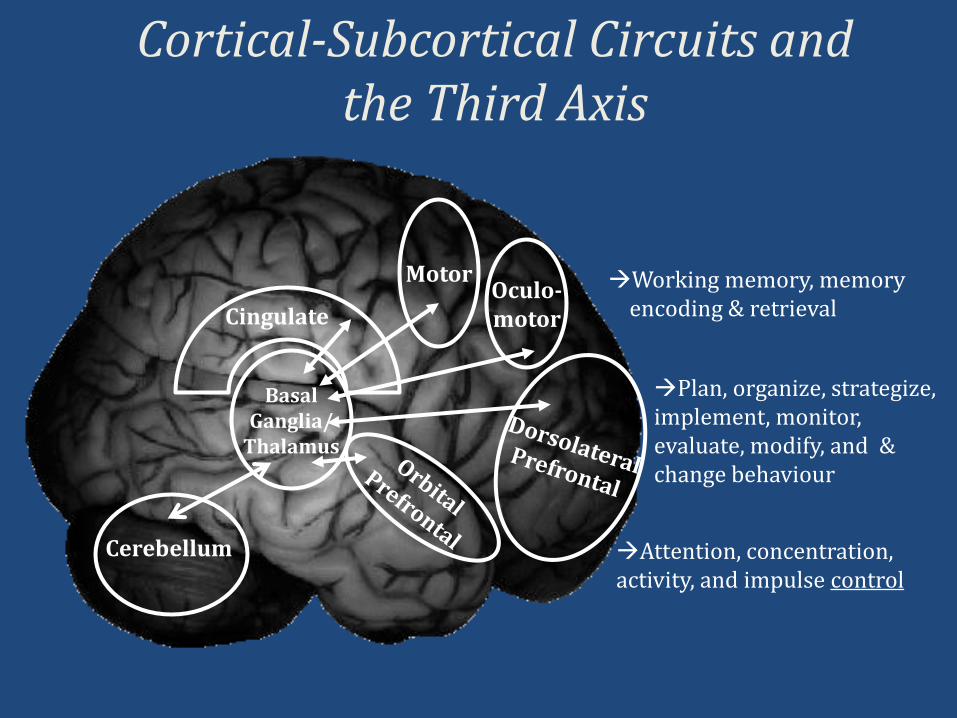
Cortical-Subcortical Circuits and the Third Axis
Oculo-motor
Motor
BasalGanglia
Thalamus
Cingulate
Cerebellum
Working memory memoryencoding amp retrieval
Attention concentrationactivity and impulse control
Plan organize strategize implement monitor evaluate modify and amp change behaviour
Anterior Cingulate Circuit and Psychopathology
bull Cognitive Functions ndash arousal motivation performance monitoring switching behavioral initiation posterior-anterior communication online data processing manager (like RAM)
bull Dysfunction Psychopathologies ndash depression bipolar ADHD schizophrenia autism
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Apathy or poor motivation
Poor response control and shiftingswitching behavior
Difficulty with decision-making
Lack of enjoyment ndash anhedonia
Poor response to reinforcement
Slow processing speed
Limited idea generation and creativity
Dorsolateral Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash planning organizing strategizing monitoring evaluating shifting and changing behavior working memory memory encoding and retrieval strategy generation and hypothesis testing
bull Dysfunction Psychopathologies ndash depression schizophrenia ADHD autism
bull Associated Neuropsychological Deficits ndash External task-oriented executive skills
Difficulty with hypothesis generation and problem solving
Limited or excessive interest in environment
Poor sustained attention
Mental inflexibility
Decreased verbal and design fluency
Encoding andor retrieval from long-term memory deficits
Poor planning organization and checking behavior
Orbital Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash indirect influence on tasks emotional and behavioral self-regulation inhibition empathy social control integrating emotions into contextually relevant behavior
bull Dysfunction Psychopathologies ndash obsessive compulsive disorder anxiety disorder bipolar disorder conduct disorder
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Perseveration or disinhibition
Tactlessness
Irritability
Sexual deviance (extreme interest or disinterest)
Antisocial or asocial behaviors
Inappropriate feelings (eg sadness or euphoria)
Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Anterior Cingulate Circuit and Psychopathology
bull Cognitive Functions ndash arousal motivation performance monitoring switching behavioral initiation posterior-anterior communication online data processing manager (like RAM)
bull Dysfunction Psychopathologies ndash depression bipolar ADHD schizophrenia autism
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Apathy or poor motivation
Poor response control and shiftingswitching behavior
Difficulty with decision-making
Lack of enjoyment ndash anhedonia
Poor response to reinforcement
Slow processing speed
Limited idea generation and creativity
Dorsolateral Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash planning organizing strategizing monitoring evaluating shifting and changing behavior working memory memory encoding and retrieval strategy generation and hypothesis testing
bull Dysfunction Psychopathologies ndash depression schizophrenia ADHD autism
bull Associated Neuropsychological Deficits ndash External task-oriented executive skills
Difficulty with hypothesis generation and problem solving
Limited or excessive interest in environment
Poor sustained attention
Mental inflexibility
Decreased verbal and design fluency
Encoding andor retrieval from long-term memory deficits
Poor planning organization and checking behavior
Orbital Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash indirect influence on tasks emotional and behavioral self-regulation inhibition empathy social control integrating emotions into contextually relevant behavior
bull Dysfunction Psychopathologies ndash obsessive compulsive disorder anxiety disorder bipolar disorder conduct disorder
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Perseveration or disinhibition
Tactlessness
Irritability
Sexual deviance (extreme interest or disinterest)
Antisocial or asocial behaviors
Inappropriate feelings (eg sadness or euphoria)
Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Dorsolateral Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash planning organizing strategizing monitoring evaluating shifting and changing behavior working memory memory encoding and retrieval strategy generation and hypothesis testing
bull Dysfunction Psychopathologies ndash depression schizophrenia ADHD autism
bull Associated Neuropsychological Deficits ndash External task-oriented executive skills
Difficulty with hypothesis generation and problem solving
Limited or excessive interest in environment
Poor sustained attention
Mental inflexibility
Decreased verbal and design fluency
Encoding andor retrieval from long-term memory deficits
Poor planning organization and checking behavior
Orbital Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash indirect influence on tasks emotional and behavioral self-regulation inhibition empathy social control integrating emotions into contextually relevant behavior
bull Dysfunction Psychopathologies ndash obsessive compulsive disorder anxiety disorder bipolar disorder conduct disorder
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Perseveration or disinhibition
Tactlessness
Irritability
Sexual deviance (extreme interest or disinterest)
Antisocial or asocial behaviors
Inappropriate feelings (eg sadness or euphoria)
Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Orbital Prefrontal Circuit and Psychopathology
bull Cognitive Functions ndash indirect influence on tasks emotional and behavioral self-regulation inhibition empathy social control integrating emotions into contextually relevant behavior
bull Dysfunction Psychopathologies ndash obsessive compulsive disorder anxiety disorder bipolar disorder conduct disorder
bull Associated Neuropsychological Deficits ndash Internal state executive skills
Perseveration or disinhibition
Tactlessness
Irritability
Sexual deviance (extreme interest or disinterest)
Antisocial or asocial behaviors
Inappropriate feelings (eg sadness or euphoria)
Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Orbital Prefrontal Circuit and Theory of Mind
bull Theory of Mind ndash the ability to take the perspective of others or feel empathy
bull Does empathy only require perception or does it also require Action
bull Posterior systems linked to affect perception
Parietal lobe and ldquomirrorrdquo neurons
Temporal lobe and face recognition
bull Why then is theory of mind linked to the frontal systems
Pars opercularis and imitation
Medial orbital cortex and theory of mind
bull Are posterior systems related to affect perception while anterior systems related to empathy
The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

The Often Neglected Cerebellum Motor Functioning or The Mini Brain
bull Cerebellum is ldquomini-brainrdquo involved in most cognition
bull Ipsilateral ldquocheck and balancerdquo for cortical functions
bull Important for fine motor and gross motor control
bull Higher level functions include timing precision learning coordination amplification of mental activity or ldquoscriptsrdquo
bull Cerbellar vermis and frontal-subcorticalinterpretative axis damage leads to ldquocognitive-affective syndromerdquo
bull Koziol Budding and Hale (2013) argue cerebellar automaticity functions could play into routinized psychopathology (eg personality disorders)
The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

The Third Axis Regulating Brain Function
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Emotion and Behavior Cortical-Subcortical Interactions
Prefrontal cortex
Limbic system
bull Limbic system for emotion registration and awareness
bull Right hemisphere and emotion processing perception of facial affect prosody and mirror neurons
bull Orbital prefrontal for emotion regulation and theory of mind for empathy
bull Should cortical disorders be treated with cognitive behavior therapy but subcortical disorders be treated with behaviouraltherapy Cerebellum
The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

The Three Axes InterpretationLeft Hemisphere-RoutinizedDetailedLocal-ConvergentConcordant-Crystallized Abilities
Right Hemisphere-NovelGlobalCoarse-DivergentDiscordant-Fluid Abilities
AnteriorSuperior-Executive Regulationand Supervision-Motor Output
Posterior-Sensory Input-Comprehension
Inferior-Executive Efficiency-Precision of action
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
Executive functions are essential for all academics and adaptive behavior
Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Differential Diagnosis of Childhood Psychopathologies
Halersquos Balance Theory
Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Frontal-Subcortical Circuits and Psychopathology Regions of Interest
DLPFC = Dorsolateral Prefrontal Cortex OFC = Orbital Frontal Cortex SMA = Supplementary Motor Area FEF = frontal eye fields ACG = Anterior Cingulate Gyrus CB = Cerbellum CC = Corpus Callosum Basal Ganglia CN = Caudate Nucleus PU = Putamen GP = Globus Pallidus (from Roth amp Saykin 2004)
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
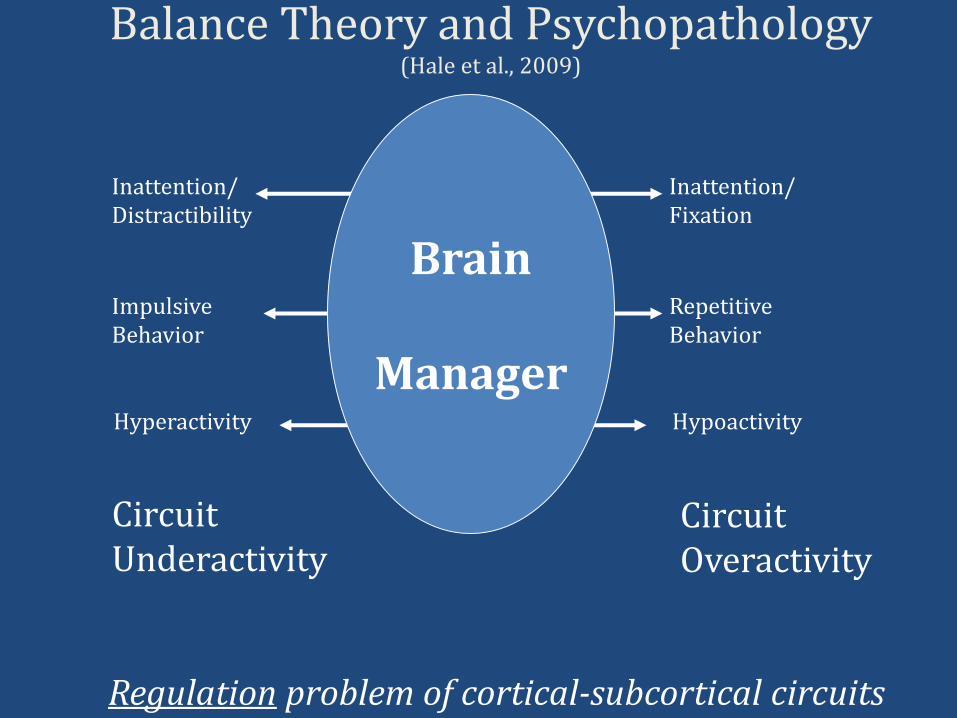
Balance Theory and Psychopathology(Hale et al 2009)
InattentionDistractibility
ImpulsiveBehavior
Hyperactivity
InattentionFixation
RepetitiveBehavior
Hypoactivity
Brain
Manager
CircuitUnderactivity
CircuitOveractivity
Regulation problem of cortical-subcortical circuits
Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Rubia (2002) fMRI ADHD vs Schizophrenia Hypoactive and Hyperactive in Response
Significant differences in MR signal response between ADHD Schizophrenia and Controls Yellow = increased MR signal in controls Blue = increased MR signal in schizophrenia
Rubia (2002) The dynamic approach to neurodevelopmental psychiatric disorders use of fMRI combined with neuropsychology to elucidate the dynamics of psychiatric disorders exemplified in ADHD and schizophrenia Behavioral Brain Research 130 47-56
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
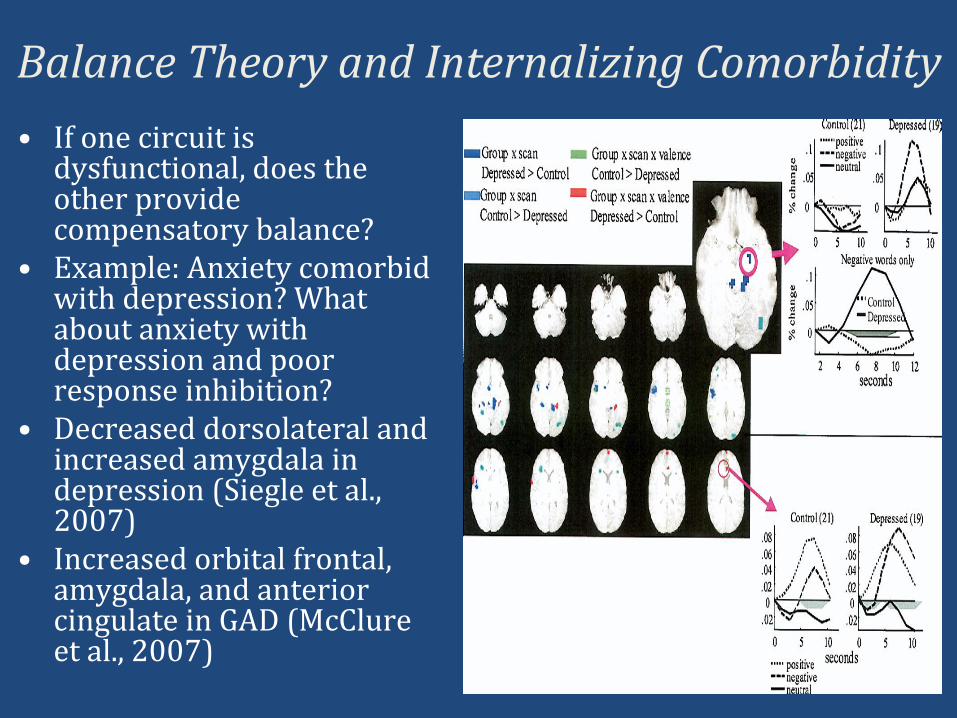
Balance Theory and Internalizing Comorbidity
bull If one circuit is dysfunctional does the other provide compensatory balance
bull Example Anxiety comorbidwith depression What about anxiety with depression and poor response inhibition
bull Decreased dorsolateral and increased amygdala in depression (Siegle et al 2007)
bull Increased orbital frontal amygdala and anterior cingulate in GAD (McClure et al 2007)
Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Yoursquoll like Mr Woolford he has an Attention-Deficit Disorder
So what IS ADHD
The question is WHAT TYPE of attention-deficit disorder
Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Using Neuroimaging Techniques to Examine Psychopathology in Children
Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Anxiety Disorder Neuroimaging FindingsStudy Sample Characteristics Clinical Group Circuit Findings
Krain et al 2008 Generalized anxiety disorder social phobia and control groups
Increased frontal-limbic region activation that reported higher intolerance of uncertainty
McClure et al 2007 Generalized anxiety disorder amp control groups
Increased activation in ventral prefrontal anterior cingulate and amygdala
Monk et al 2006 Generalized anxiety
disorder and control
groups
Increased activation in right ventrolateral prefrtonal
assocaited in response to angry faces and attention bias
away but reduced anxiety compensatory response
Anxiety Disorder
Obsessive Compulsive Disorder
Study Sample Characteristics Clinical Group Circuit FindingsSzeszesko et al 2004 Children with OCD and
controlsIncreased cingulate gray matter volume
Viard et al 2005 Adolescents with OCD amp control group
Abnormal activation in parietal temporal amp precuneus regions hyperactivity in anterior cingulate amp left parietal subregions
Woolley et al 2008 Adolescent males with OCD amp control group
Reduced activation in right orbitofrontal cortex thalamus cingulate amp basal ganglia during response inhibition
Yucel et al 2007 Adolescents with OCD and controls
Hyperactivation of medial frontal cortex compensatory for reduced dorsal anterior cingulated
Nakao et al 2005 Patients with OCD pre and post-treatment
Hyperactivity in orbital frontal and cingulatereduced with SSRI medication treatment
Rosenberg amp Keshavan 1998
Children with OCD and controls
Increased ventral prefrontal
Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Mood Disorder Neuroimaging Findings
Study Sample Characteristics Clnical Group Circuit Findings
Forbes et al 2006 Youth with MDD anxiety disorder amp control group
Decreased amygdala and orbital frontal cortex in response to reward inconsistent with anxiety group
Grimm et al 2008 MDD (unmedicated) amp control group
Hypoactivity in left dorsolateral hyperactivity in right dorsolateral prefrontal correlated with depression severity
Steingard et al 2002 Adolescents with MDD amp control group
Decreased white matterincreased gray matter in frontal lobe
Wagner et al 2005 MDD (unmedicated) amp control group
Hyperactivity in rostral anterior cingulate gyrus amp left dorsolateral prefrontal cortex in during Interference phase
Major Depressive Disorder
Bipolar Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Adler et al 2005 Children with Bipolar Disorder with and without ADHD
Children with comorbid ADHD showed decreased ventrolateral and cingulated activity
Blumberg et al 2003 Adolescents with Bipolar Disorder amp control group
Increased left putamen amp thalamus depressive symptoms and ventral striatum positively correlated
Adler et al 2005 Youth with BD + ADHD amp BD groups
Decreased activation of ventrolateral prefrontal cortex amp anterior cingulated (BD + ADHD group)
Chang et al 2004 Youth with Bipolar Disorder and controls
Increased activation in anterior cingulated left dorsolateral prefrontal right inferior and right insula
Gruber et al 2003 Bipolar Disorder and Controls
Increased dorsolateral and decreased cingulated
Nelson et al 2007 Adolescents with Bipolar Disorder and controls
Increased left dorsolateral prefrontal and premotor activity interfere with flexibility
Rich et al 2006 Adolescents with Bipolar Disorder and controls
Greater putamen accumbens amygdala and ventral prefrontal with emotional face processing
Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Effected Systems in ADHD Cingulate and SuperiorLongitudinal Fasiculus White Matter Deficiency
Makris et al (2008) Attention and Executive Systems Abnormalities in Adults with Childhood ADHD A DT-MRI Study of Connections Cerebral Cortex 18 1210-1220
Diffusion Tensor Imaging ADHD lt Controls in fractional anisotropy (white matter integrity) findings for anterior cingulate and superior longitudinal fasciculus R more deficient than L
Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Dickstein et al (2006) The neural correlates of attention deficit hyperactivity disorder An ALE meta-analysis Journal of Child Psychology and Psychiatry 47 1051-1062
Dickstein et al (2006) Activation Likelihood Estimation (ALE) Meta-Analysis
bull ADHD lt controls in right dorsolateral inferior frontalorbital cingulate striatum thalamus and parietal regions
bull For response inhibition inferior frontalorbital anterior cingulate and precentral gyrus underactive in ADHD
bull Overactivation in several regions (left insula occipital middle frontal gyrus right precentral gyrus) may reflect compensatory strategy to overcome underactive regions
bull ADHD is not just right frontal-striatal hypoactivity but hyperactivity of compensatory regions as well
bull Result suggest balance of dysfunction and compensatory activity
Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Are Oppositional Defiant DisorderConduct Disorder Findings Different from ADHD
bull De Brito et al (2009) ndash increased grey matter in conduct disorder in several areas (ratio of white-grey matter important)
bull Sterzer et al (2005) ndash hypoactivation in response to negative pictures in the dorsal anterior cingulate and left amygdala in CD
bull Rubia et al (2008) ndash ldquoPurerdquo ADHD had reduced ventrolateral and increased cerebellum in sustained attention while ldquopurerdquo CD showed decreased anterior cingulate insula and hippocampus reward condition they showed right orbital frontal hypoactivity
bull ADHD is ventral-lateral and cerebellar while CD is orbital-paralimbic
Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Externalizing Disorders Neuroimaging FindingsAttention-DeficitHyperactivity Disorder
Study Sample Characteristics Clinical Group Circuit Findings
Booth et al 2005 Children with ADHD amp control group
Decreased activation in inferior middle superior amp medial fronto-striatal regions caudate nucleus amp globus pallidus
Cao et al 2008 Adolescent males amp control group
Decreased activation in frontal (middle amp superior frontal gyrus) putamen amp inferior parietal lobe
Durston et al 2003 Children with ADHD and controls
ADHD underactivated ventrolateral prefrontal anterior cingulate and caudate during response inhibition
Pliszka et al 2006 ADHD treatment naiumlve amp previously medicated groups amp control group
ADHD treatment naiumlve less cingulate and left ventrolateral activation during impulsive responding than controls
Rubia et al 2005 ADHD adolescents amp matched controls
ADHD less right inferior frontal activation during inhibition
Scheres et al 2007 ADHD adolescents and matched controls
Reduced ventral striatum activity during reward anticipation
Schultz et al 2004 Male adolescents with ADHD amp control group
Increased left amp right ventrolateral inferior frontal gyrus left amp right frontopolar regions of the middle frontal gyrus right dorsolateral middle frontal gyrus left anterior cingulate gyrus amp left medial frontal gyrus
Tamm et al 2004 Children with ADHD and controls
Hypoactivation of anterior cingulated and hyperactivation temporal compensatory regions
Vaidya et al 1998 Children with ADHD and controls
Frontal activity possible compensation for striatalhypoactivity normalized with stimulant treatment
Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Autism Neuroimaging Findingsbull Koshino et al (2005) ndash autism use right parietal but
controls use left parietal for verbal working memory task and (2008) autism less left frontal and right temporal for face working memory plus processing faces as objects suggesting asocial face processing style
bull Luna et al (2002) ndash autism showed lower dorsolateral and posterior cingulate functioning during spatial working memory task suggesting poor executive control and communication across hemispheres rather than ldquopurerdquo spatial deficit
bull Pierce et al (2001) ndash autism face processing outside the fusiform region including the primary occipital region and prefrontal cortex suggesting they process faces as objects or parts of objects not as faces
bull Dapretto et al (2005) ndash autism showed less activity in pars opercularis (mirror neurons area) important for imitation and empathy (theory of the mind)
bull Allen amp Courchesne (2003) significantly more motor activation (neocerebellum) and less attention activation (vermis) in cerebellum
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
Is Asperger Syndrome on the ldquoSpectrumrdquo
bull In 1944 Hans Asperger described ldquoautistic psychopathyrdquo cases with ldquonormalrdquo intelligence with peculiar social skills pedantic speech and preference for routinized activities
bull Myklebust (1975) ndash Social judgment and reciprocity impaired due to misperception of external cues and internal experiences
bull Denckla (1983) ndash Right hemisphere developmental learning disability Affects cognition academic and psychosocial functions
bull Rourke (1989) ndash Nonverbal learning disabilities due to white matter syndrome poor visual-spatial-motor and novel problem solving both internalizing and externalizing psychopathology
Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Is Asperger Syndrome on the ldquoSpectrumrdquobull OrsquoNeill (1999) describes Aspergerrsquos as ldquolittle
professors who canrsquot understand social cuesrdquo donrsquot understand gist of social discourse
bull Klin et al (1996) compared neuropsychological profiles and found Asperger gt autism on verbal measures reverse was true for nonverbal (visuospatial visuomotor and visual memory) concluding profile in Aspergerrsquos was similar to NVLD and distinct from high functioning autism
bull Volkmar et al (2000) describe ldquoRobertrdquo good reader but eccentric and clumsy high anxiety levels and poor social and adaptive functioning found right hemisphere white matter lesion
bull Bryan amp Hale (2001) ndash DiscordantDivergent processes affect nonverbal (spatial-holistic) and verbal (implicit language) functioning
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
Specific Learning Disabilitiesand Psychopathology
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
Psychopathology in SpecificLearning Disabilities
bull Byron Rourkersquos ldquononverbalrdquo SLD right hemisphere dysfunction and the ldquoWhite Matter Modelrdquo of psychopathologyProsody implicit language neglect of self and environment limited recognition of facessocial cues integration of complex stimuli poorResults in both internalizing and externalizing psychopathology (under socialized delinquency) no distinction of anteriorposterior
bull VerbalLeft Hemisphere DysfunctionRourke says no but early childhood internalizing problems and delinquents show LEFT hemisphere dysfunction (Moffit 1993 Forrest 2004)
Could shift from internalizing to externalizing reflect environmental causes (eg socialized delinquency)
Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Differentiating Right Hemisphere Functions
bull Attention to Environment
bull Attention to Self (Body Awareness)
bull SpatialHolistic Processing
bull Left Hand Sensory Feedback
bull Object Recognition
bull Facial Perception
bull Affect Recognition
bull Contextual Comprehension
bull Implicit Comprehension
bull Discordant Comprehension
bull Receptive Prosody
bull Social Comprehension
Right Posterior Region
bull Sustained Attention
bull Planning
bull Strategizing
bull Evaluating
bull FlexibilityShifting
bull Immediate Learning
bull Working Memory
bull Memory Retrieval
bull Novel Problem Solving
bull Divergent Thought
bull Implicit Expression
bull Expressive Prosody
bull Social Adaptability
Right Anterior Region
ADHD-Inattentive TypeAsperger Syndrome
ADHD-Combined Type
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
bull 155 children age 6 to 16 (M = 1086 SD = 280) with SLD by school district and Concordance-Discordance Model criteria
bull 42 excluded for not meeting processing asset and deficit (eg Hale et al 2006)
bull WISC-IV BASC-2 TRS and achievement scores in average range with mild impairments but heterogeneity masked significant profile differences
bull Average linkage within groups variant of the unweighted pair-group method arithmetic average (UPGMA) revealed six neurocognitive SLD subtypes
VisualSpatial (VS) (n = 14) Fluid Reasoning (FR) (n = 10) CrystallizedLanguage (CL) (n = 15)Processing Speed (PS) (n = 30)ExecutiveWorking Memory (EWM) (n = 19)High FunctioningInattentive (HFI) (n = 25)
SLD Psychopathology StudyHain Hale amp Glass-Kendorski (2010)
Participants
Results
Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Preliminary Study of SLD Subtypes and Psychopathology
bull Participants and Methods
bull 124 students ages 6-11
bull All underwent comprehensive evaluations in two Canadian school districts
bull Students were divided into three groups based on concordance-discordance methods (CDM) to determine significant patterns of processing strengths and weaknesses
bull C-DM identified three specific subtype groups Working Memory (n = 24) Processing Speed (n = 32) and No SLD Disability (n = 32) subtypes
bull Specific LD subtype domains were examined further comparing subtype groups to specific cognitive academic and psychosocial domains
CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

CDM-Determined SLD WISC-IV Cognitive Results
CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

CDM-Determined LD Psychosocial DimensionsEternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
ExternalizingM
SD59001427
5629 1113
5872 1150
25 784
HyperactivityM
SD59931536
6082 1401
5933 1221
05 950
AggressionM
SD60931738
5459 1136
5850 1095
93 401
Conduct ProblemsM
SD54271053
5206837
5667 1296
79 460
CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

CDMndashDetermined SLD Psychosocial DimensionsInternalizing Behaviors
No LDn = 15
WMIn = 17
PSIn = 18
F P
InternalizingM
SD5847 1167
5547 1136
6417 1634
189 162
AnxietyM
SD5587 1177
5718 1282
5944 1447
32 730
DepressionM
SD6180 1461
5971 1426
6917 1963
159 215
SomatizationM
SD5227 1093
6917 1963
5517 1633
207 138
WithdrawalM
SD5713 1229
5718 1106
6861ab
1343498 011
Note a Greater than No LD group b Greater than WMI group
CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

CDM-Determined SLD Psychosocial DimensionsAdaptive Skills
No LDn = 15
WMIn = 17
PSIn = 18
F P
Overall Adaptive SkillsMSD
4367 814
4153 710
3622a
429568 006
Adaptability MSD
4520 1273
4524 1126
3789ab
890258 087
Social SkillsMSD
4613 990
4447 852
3856a
634394 026
LeadershipMSD
4593 689
4263 552
4089a
413345 040
Functional CommunicationMSD
4387 714
3881 638
3694a
854368 033
Note a Greater than No LD group b Greater than WMI group
Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Relevance of School Neuropsychological Assessment for Intervention
Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Recognizing Brain Functioning in the ClassroomBrain Area Possible Effects of Left
Hemisphere DamagePossible Effects of Right Hemisphere Damage
Occipital Lobe Slow reading poor spelling with letter substitutions difficulty with visual discrimination of details
Limited comprehension and writing when visual imagery required object recognition limited
Dorsal Stream Poor leftright orientation sound-symbol association (ie alphabetic principle) and letter reversals
Poor handwriting and math from spatial deficits poor awareness of self and environment during social
Ventral Stream Difficulty recognizing sight words poor reading fluency object naming limited
Difficulty with sight words and perception of affect and faces
LateralMedialTemporal Lobe
Canrsquot remember facts and words due to difficulty with long-term memory poor categorization
Limited understanding of context metaphor multiple word meanings and humor
Superior Temporal Lobe
Frequent requests for repetition poor word reading poor auditory and phonological processing
Poor perception of rate and pitch or prosody difficulty with complex sentence processing
Anterior Parietal Lobe
Poor right hand grasping writing too light or dark complains after writing that ldquohand hurtsrdquo
Poor left hand grasping and limited bimanual coordination skills
BOLDED Items reflect processes that could lead to psychosocial concerns
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
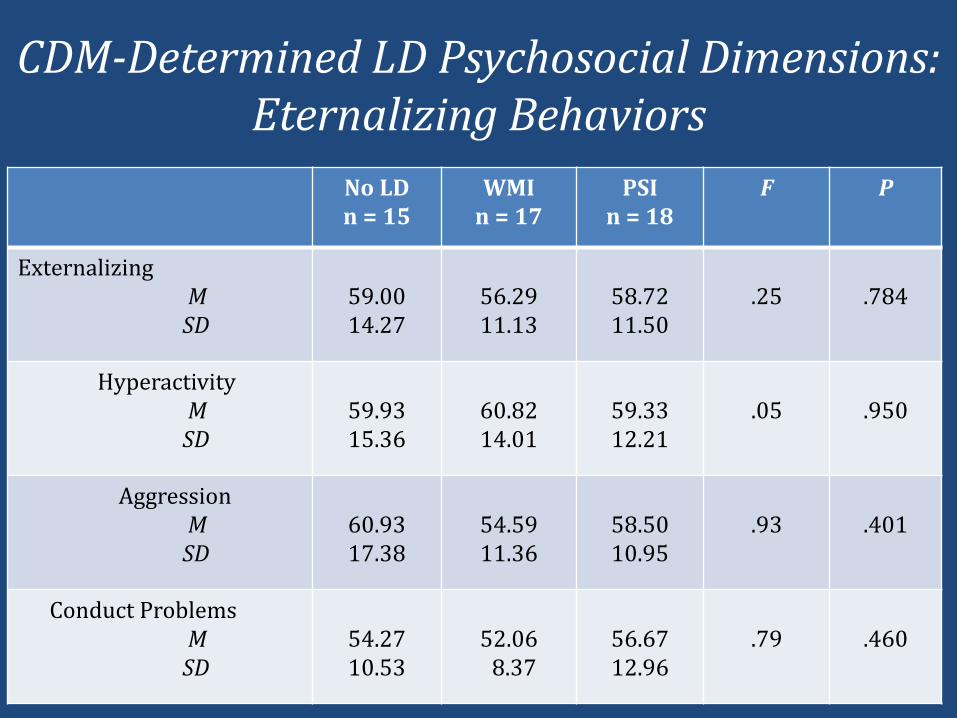
Recognizing Brain Functioning in the Classroom
Brain Area Possible Effects of LeftHemisphere Damage
Possible Effects of Right Hemisphere Damage
Occipital-temporal-parietal crossroads and WernickersquosArea
Difficulty connecting sounds (phonemes) with symbols (graphemes) difficulty connecting numbers with quantity and math algorithms limited comprehension of explicit language
Poor math problem solving and comprehension of implicit language complex language poetry difficulty with new learning and integrating different types of information poor understanding of humor
Posterior Frontal Lobe
Difficulty with dressing drawing and handwriting limited or no motor skill automaticity
Difficulty with learning new motorskills and sports requiring fine motor difficulty with using both hand simultaneously
Brocarsquos Area Halting speech with little output and difficulty with articulation and syntax even impulse control
Poor verbal prosody and word substitutions verbose but limited pragmatics
Dorsolateral-DorsalCingulate
Poor encoding for storage limited decision making rigid and inflexible thinking difficultywith concordant and convergent thought
Poor retrieval from long term memory sustained attention and novel problem solving difficulty with discordantdivergent thought
Orbital-VentralCingulate
Depressive symptoms and avoidancewithdrawal excessive emotional control
Disinhibition and indifference aggression and or conduct problems
The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

The Cognitive Hypothesis Testing Model
Source Hale J B amp Fiorello C A (2004) School Neuropsychology A Practitionerrsquos Handbook New York NY Guilford Press
Theory
Hypothesis
Data Collection
Interpretation
1 Presenting Problem
2IntellectualCognitive Problem
3 AdministerScore Intelligence Test
4 Interpret IQ or Demands Analysis
5 Cognitive StrengthsWeaknesses
6 Choose Related Construct Test
7 AdministerScore Related Construct Test
8 Interpret ConstructsCompare
9 Intervention Consultation
10 Choose Plausible Intervention
11 Collect Objective Intervention Data
12 Determine Intervention Efficacy
13 ContinueTerminateModify
Comprehensive Evaluation for Disability Determination and Service Delivery
Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Choosing Tier 3 Interventions for ADHD and Other Psychopathologies Affecting Attention
bull Determine whether a what problem (cortical-cognitive behaviour therapy metacognitive strategies) a whenproblem (basal ganglia-social skills role playing) or a how problem (cerebellar-behavioural intervention) GOAL Move from subcortical to cortical
bull Medication likely for cortical andor subcortical problems consider agonist vs antagonist issues and cortical hyperactivityhypoactivity
bull Adaptive strategies (self-monitoring metacognitive strategies problem-solving conflict resolution social skills planners organizers routines response inhibition flexible brainstorming empathy instruction working memory computer games)
bull Importance of monitoring treatment response
Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Instructional Strategies for Children with Psychopathology
ndash Keeping lesson objectives clear
ndash Deliver the lesson at a brisk pace
ndash Encourage collaboration among students
ndash Use meaningful materials and manipulatives
ndash Prompt student answers after five seconds of wait time
ndash Vary the tone of your voice and model enthusiasm
ndash Break up long assignments by chunking content
ndash Encourage regular student responding
ndash Reduce amount of work on assignments for good performance
ndash Provide extended time on assignments and exams
ndash Ensure success in responding assignments and exams
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Executive Deficits Metacognition and Learning Strategies ldquolsquoThe individuals own awareness and consideration of hisor her cognitive processes and strategiesrdquo (Flavell 1979)
bull Learning strategiesPaired Associates Rehearsal Mnemonics Visualization Notetaking Self-Talk Brainstorming Checking Scaffolding Outlining
bull Ask metacognitive questions during the day (thinking about your thinking)
bull Give kids models to help them evaluate their workbull Teach a problem-solving procedurebull Give assignments that require evaluative skillsbull Demonstrate ldquothinking aloudrdquo during lessonsbull Working memory training (eg CogMed)bull Attention training
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Working Memory Training and Improved Cognitive Functioning
Takeuchi et al 2010
bull N-Back task
bull Increased working memory performance
bull Changes in regions near intraparietal sulcus amp anterior corpus callosum
bull Amount of training correlated with increased fractional anisotropy (changes in white matter)
CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

CogMed Working Memory Training(Brehmer et al 2011)
bull Working Memory training and adults
bull Improved working memory performance with CogMed training
bull Decreased activity in frontal and parietal areas
bull Increased activity in subcortical regions (thalamas amp caudate)
bull Suggests more efficient working memory and cortical-subcortical circuit functions
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
Coping with ADHD Behavior Problems Proactive or Reactive
Scheduling
ldquoOn taskrdquo behaviors decrease during day more academic instruction mornings
and more non-academic afternoon activities
Productive Physical Movement
Allow opportunities for movement (eg office trip sharpen pencil stand at desk
assist with class duties movement in assignments)
Choice Making
Provide student with menu of potential tasks to choose
Alter Environment
Provide control through preferential seating or teacher proximity
Task Duration
Brief assignments and immediate feedback long assignments broken down into
smaller parts
Prompt Appropriate Classroom Behavior
Visual auditory verbal or physical cues
Specific Rules and Reminders
Barkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Changes in Brain Functioning withPsychological and Medication Interventions
bull Cognitive Behavioral Therapy for Obsessive-Compulsive Disorder (Freyer et al 2011 OrsquoNeill et al 2011)
ndash Decreased activation in orbitofrontal cortex and right putamen
ndash Metabolic changes in anterior cingulate and thalamus
bull Social Skills Therapy for Autism (Bolte et al 2006)ndash Increased activation in parietal and occipital lobe
ndash Suggests a compensatory mechanism for emotion recognition
bull Medication Treatment for Attention-DeficitHyperactivity Disorder (Pliszka et al 2006 Hale et al 2011)
ndash Normalized cingulate functioning following medication treatment even without medication
ndash Only children with ADHD and executive dysfunction show stimulant response best dose for cognitive functioning lower than best dose for behaviour
Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Coping with ADHD Behavior Problems Proactive or Reactive
Differential Reinforcement
DRO ndash Other behavior
DRA ndash Alternative behavior
DRI ndash Incompatible behavior
Time Out
Time out from learning extinction of negative attention
Duration is equivalent to studentrsquos age
Do not remove student or allow other reinforcing activities
Token EconomyContingency Contracting
Students earn tokens or points for meeting behavioral expectations and lose points
for poor behavior
Points can be exchanged for privileges
Effective at home and school
Tokens- chips class money stickers
Self Management
Requires students to monitor andor evaluate their own behavior over time
Teacher identifies target behaviors expected provides scale with criteria for self-
ratings and teaches student to chart behaviorBarkley 2006 DuPaul amp Stoner 2004 Majewicz-Hefley amp Carlson 2007 Toplak et al 2008 Barkley Edwards Laneri Fletcher amp Metevia 2001 Klingberg amp Forssberg 2002 Lonigan Elbert amp Johnson 1998
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
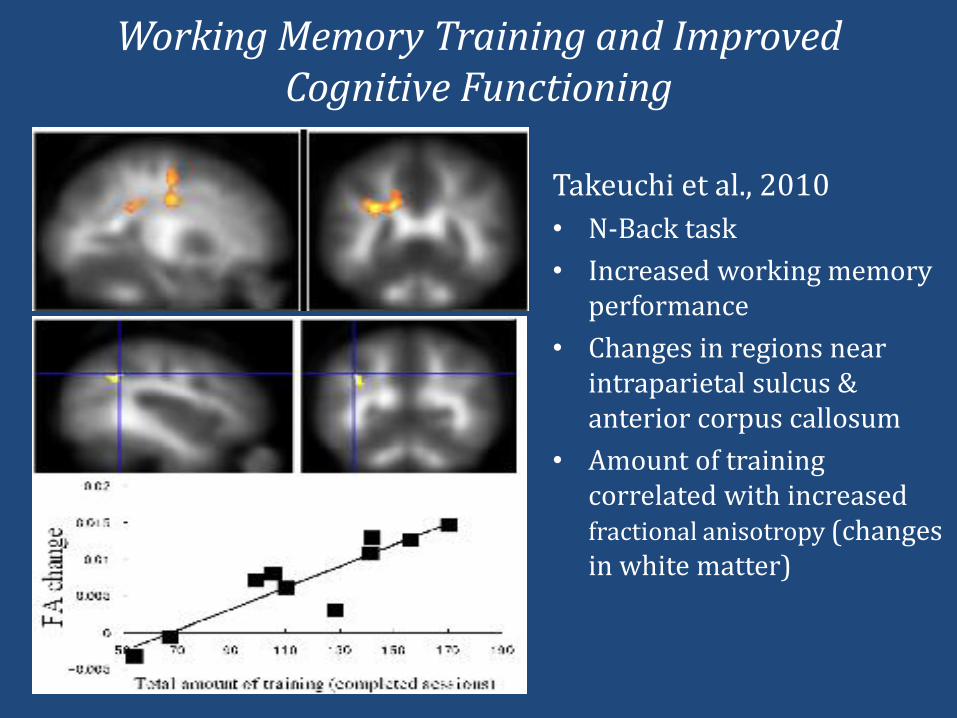
Choosing Therapeutic Interventions Based on Neuropsychological Functioning
Inferior
Superior
-Executive Efficiency-Precision in Motor and Language Action
-Executive Regulation and Supervision
Automatized Behaviors(eg operant conditioning
desensitization)
Executive Problem(eg Cognitive Behavior
Therapy Learning Strategy Instruction)
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
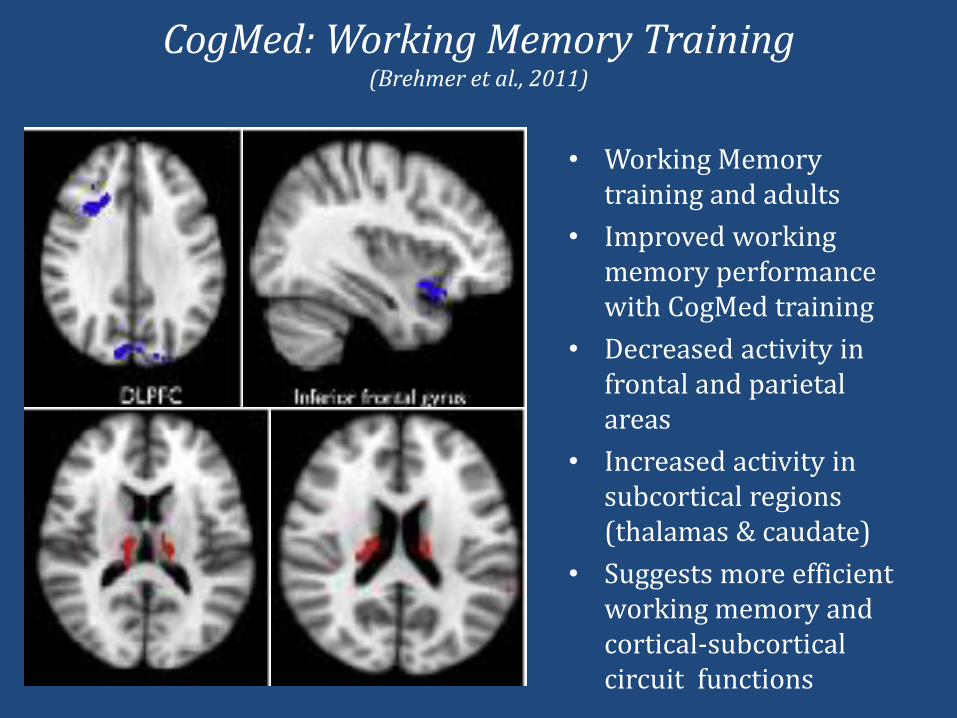
Get Parents Involved
bull Home based reinforcement program
bull Allows child to earn privileges at home based on positive school behaviour
bull Home-school report card - accomplished through notes between teacher and parent
bull Contingency contract specifies academic performance and classroom behavior expected and privileges that can be earned
bull Most effective if earned daily rather than weekly
bull Start with criteria that is easy to accomplish and slowly build to more challenging goals
Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Conducting Executive Function Interventions
Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Relevance of School Neuropsychological Assessment for Intervention
Hale et al (2011) ADHD Study
Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Executive Impairment Determines ADHD Medication Response Implications for
Academic AchievementJames B Hale Linda Reddy Margaret Semrud-Clikeman Lisa A Hain James Whitaker Jessica Morley Kyle
Lawrence Alex Smith and Nicole Jones
AbstractMethylphenidate (MPH) often ameliorates attention-deficithyperactivity disorder (ADHD) behavioral dysfunction
according to indirect informant reports and rating scales The standard of care behavioral MPH titration
approach seldom includes direct neuropsychological or academic assessment data to determine treatment
efficacy Documenting ldquocoolrdquo executive-working memory (EWM) and ldquohotrdquo self-regulation (SR)
neuropsychological impairments could aid in differential diagnosis of ADHD subtypes and determining cognitive
and academic MPH response In this study children aged 6 to 16 with ADHD inattentive type (IT n = 19) and
combined type (n = 33)hyperactive-impulsive type (n = 4) (CT) participated in a double-blind placebo-controlled
MPH trials with baseline and randomized placebo low MPH dose and high MPH dose conditions EWMSR
measures and behavior ratingsclassroom observations were rank ordered separately across conditions with
nonparametric randomization tests conducted to determine individual MPH response Participants were
subsequently grouped according to their level of cool EWM and hot SR circuit dysfunction Robust cognitive and
behavioral MPH response was achieved for children with significant baseline EWMSR impairment yet
response was poor for those with adequate EWMSR baseline performance Even for strong MPH responders
the best dose for neuropsychological functioning was typically lower than the best dose for behavior Findings
offer one possible explanation for why long-term academic MPH treatment gains in ADHD have not been
realized Implications for academic achievement and medication titration practices for children with behaviorally
diagnosed ADHD will be discussed
copy Hammill Institute on Disabilities 2010
httpjournaloflearningdisabilitiessagepubcom
Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Medication Treatment and ADHD
bull Approximately 2000000 treated with stimulants
bull Medication effective in 70 to 90
bull Medication wakes the ldquobrain managerrdquo (ie reduces frontal-striatal hypoactivity)
bull Dopamine agonists (eg stimulants) affect striatum
bull Norepinephrine agonists (eg Strattera) affect prefrontal cortex
bull Improves classroom behavior performance and interactions
bull Few serious side effects (appetite sleep irritability and headache ndash not common and typically decrease)
bull Best dose for behavior may be higher than best dose for cognition
bull Behavioral diagnosis and titration limit treatment efficacy
Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Double-Blind Placebo Protocol(Hoeppner et al 1997 Hale et al 1998 2005 2007 in press)
bull Children diagnosed and referred by physician diagnosis independently confirmed by psychologist
bull Weekly neuropsychological testing parent and teacher behavior ratings and classroom observation for 4 weeks
bull Baseline then randomized placebo low and high dose conditions
bull Child parent teacher and graduate research assistant blind
bull Physician psychologist and pharmacist not blind (safety)
bull Data rank ordered across conditions
bull Nonparametric randomization tests determine separate cognitive and behavioral response
bull Results graphically depicted and reported to referring physicians for subsequent clinical decision-making
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
Hale-DencklaCancellationTask X
XX X
XX
X XX
X XX X
X XX X
XX
X XX
X XX
XX X
X X
Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Trail-MakingTestPart B
StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

StroopColor-WordTest
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoBluerdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoRedrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoGreenrdquo
ldquoBluerdquoldquoRedrdquo
ldquoBluerdquo
Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Drug Trial Example Lisabull Lisa was a 6 year 10 month-old friendly and outgoing girl who
thrived on adult attention
bull Academic and social concerns in the first grade included
Inattentive easily distracted fidgety and frequently off task
Attentional difficulties during whole-group instruction and independent work
Poor writing skills including difficulties with grammar and illegible handwriting
Noncompliant behavior with teacher
Limited social skills and frequent conflicts with peers
bull Recurrent discussions and removal of privileges did not help
bull Comprehensive neuropsychological evaluation revealed cognitive neuropsychological academic and behavioral data consistent with ADHD
bull Following consultation with parents pediatrician referred Lisa for double-blind placebo controlled trial of methylphenidate
Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Neuropsychological Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
Go-No Go 17 (4) 21 (3) 27 (1) 26 (2)
SRTM Word Storage 41 (35) 41 (35) 53 (1) 48 (2)
Stroop Errors 4 (3) 4 (3) 2 (1) 4 (3)
Stroop Color Word Correct 14 (4) 17 (1) 15 (3) 16 (2)
SRTM Consistent Retrieval 24(3) 21 (4) 43 (1) 36 (2)
TOMAL Digits Backward 10 (4) 12 (3) 20 (1) 14 (2)
Hale-Denckla Cancellation Correct 13 (4) 18 (3) 26 (15) 26 (15)
Hale-Denckla Cancellation Time 172 (2) 199 (4) 163 (1) 191 (3)
Trails B Errors 6 (4) 3 (3) 1 (1) 2 (2)
Trails B Time 534 (4) 56 (2) 44 (1) 60 (3)
Connersrsquo CPT-II Omissions 65 (4) 62 (3) 55 (1) 60 (2)
Connersrsquo CPT-II Commissions 60 (3) 64 (4) 43 (2) 34 (1)
Connersrsquo CPT-II RT Block Change 57 (3) 61 (4) 44 (2) 41 (1)
Connersrsquo CPT-II RT ISI Interval 57 (3) 69 (4) 51 (2) 42 (1)
MEAN RANK 343 303 143 210
Auditory-VerbalMotorMeasures
Visual-MotorMeasures
1Order =Baseline10mg MPHPlacebo5mg MPH
Connersrsquo CPT-II Reaction Time 41 (3) 47 (1) 54 (2) 63 (4)
Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Behavioural Medication Trial Results for LisaBaseline Placebo 5 mg MPH 10 mg MPH1
CPRS-RL Cognitive Problems 89 (4) 81 (2) 72 (1) 87 (3)
CPRS-RL Hyperactivity Index 87 (4) 84 (3) 80 (2) 70 (1)
HSQ-R Mean Score 74 (35) 75 (35) 74 (2) 69 (1)
SERS Parent 0 3 0 21
CPRS-RL DSM-IV Hyperactive-Impulsive 83 (2) 90 (4) 89 (3) 75 (1)
CPRS-RL DSM-IV Inattentive 90 (4) 80 (2) 74 (1) 84 (3)
CTRS-RL Cognitive Problems 89 (35) 81 (2) 76 (1) 89 (35)
CTRS-RL Hyperactivity Index 77 (4) 74 (3) 71 (2) 70 (1)CTRS-RL DSM-IV Inattentive 82 (4) 72 (2) 66 (1) 74 (3)
CTRS-RL DSM-IV Hyperactive-Impulsive 73 (2) 80 (4) 79 (3) 65 (1)
SSQ-R Mean Severity 65 (4) 60 (2) 63 (3) 46 (1)
APRS Learning 18 (25) 18 (25) 16 (4) 22 (1)APRS Impulse Control 15 (3) 15 (3) 15 (3) 18 (1)APRS Academic Performance 22 (2) 21 (3) 18 (4) 28 (1)
SERS Teacher 7 11 12 18
MEAN RANK 319 276 226 179
Parent Ratings
Teacher Ratings
Classroom Observations
RAT Off-Task 28 (2) 35 (4) 10 (1) 33 (3)
RAT Plays with Objects 20 (3) 25 (4) 5 (1) 10 (2)RAT Fidgeting 33 (3) 38 (4) 28 (2) 15 (1)
RAT Out of Seat 3 (2) 5 (3) 10 (4) 0 (1)RAT Vocalizes 13 (35) 10 (2) 13 (35) 3 (1)
CTRS-RL Oppositional 65 (35) 58 (1) 63 (2) 65 (35)
CPRS-RL Oppositional 60 (35) 52 (1) 56 (2) 60 (35)
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
Lisarsquos Response to Stimulant Medication
40
30
20
00
10
Baseline Placebo 5mg MPH 10mg MPH
Note Lower Ranks = Better Performance and BehaviorOrder of Conditions = Baseline 10mg MPH Placebo 5mg MPH
Cognitive Response
Behavioural Response
Mean
Ran
k
0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

0
2
4
6
8
10
12
14
None (+1 SD or more) Low (+99 to 0) Moderate (0 to -99) High (-1 SD or less)
Inattentive Type
Combined Type
Frontal-Subcortical Impairment and Diagnosis
of
Pa
rtic
ipa
nts
Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Medication Response for No Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (NS)
Behavioural Response (BgtPLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Medication Response for Low Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH LgtH)
Behavioural Response (BgtPLH PLgtH)
25
20
15
10
5
0
35M
ean
Ran
k
Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Medication Response for Moderate Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BgtPLH PgtLH)
25
20
15
10
5
0
35M
ea
n R
an
k
Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Medication Response for High Impairment Group
30
Baseline Placebo Low Dose High Dose
Note Lower Ranks = Better Performance and Behaviour
Cognitive Response (BPgtLH)
Behavioural Response (BPgtLH)
25
20
15
10
5
0
35
0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

0
2
4
6
8
10
No MPH Response
Cog or Beh MPH Response
Cog and Beh MPH Response
Medication Response by Subtype and Impairment Group
Inattentive Type ADHD
Combined Type ADHD
Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

Solution Should We Put Ritalin in the Water Supply
Question is not WHETHER medication should be used for ADHD but rather WHOM do we use it for HOW do we monitor it and WHAT dose should we use (in conjunction with other interventions)hellip
SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab

SNAP-FIT (Student Neuropsychological Assessment Profiles for Innovative
Teaching) Kai Case Study
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
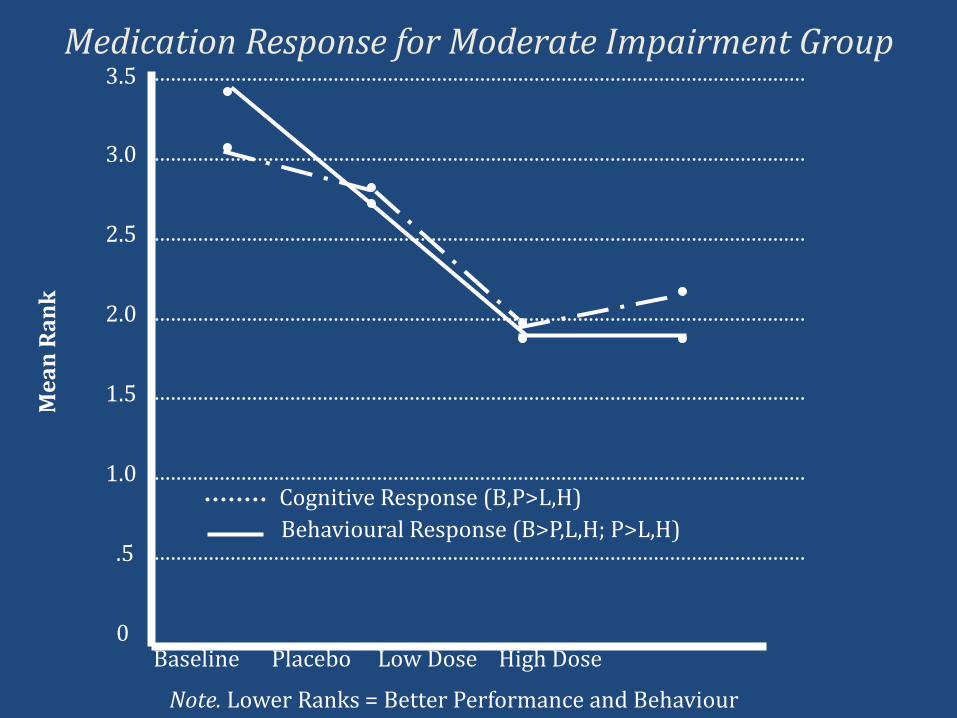
ldquoOpen exploration of multiple viewpoints breathes life into disciplinealternatively ignoring or minimizing that discourse only suffocates itrdquo (Hale 2007)
Together we can help all children learn and behave
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab
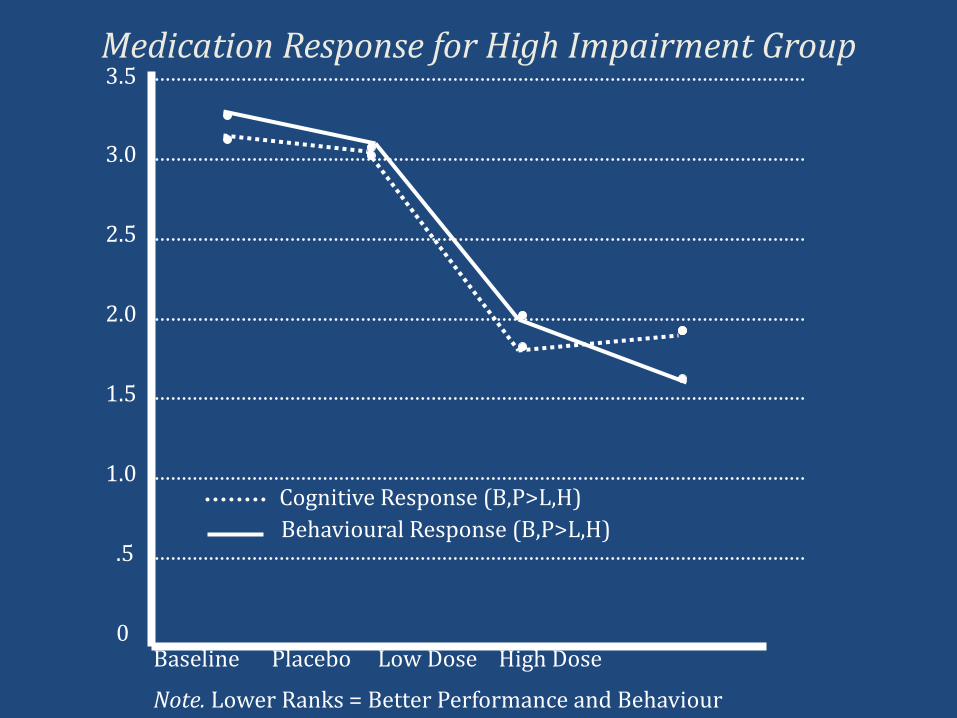
THANK YOU QUESTIONS COMMENTS
Find us online wwweducucalgarycabraingainFollow us on Twitter braingainlab
Like us on Facebook wwwfacebookcombraingainlab