jacob h rand, md department of pathology and laboratory ... · department of pathology and...
TRANSCRIPT

UNDERSTANDINGaPLA
JacobHRand,MDDepartmentofPathologyandLaboratoryMedicine
WeillCornellMedicalCollege
DISCLOSURESTATEMENTSpeaker:JacobHRand,MD
IncompliancewithACCMEpolicy:Employment:NothingtodiscloseConsultancy:NothingtodiscloseEquityOwnership:NothingtodiscloseResearchFunding:NothingtodiscloseHonoraria:NothingtodisclosePatents&Royalties:InventorofUSPatents#6,284,475and7,252,959
assignedtoMountSinaiSchoolofMedicineSpeakersBureau:NothingtodiscloseMembershipinadvisoryboards:NothingtodiscloseOther:Nothingtodisclose

• To review where we are now and how we got here
• To describe the aPLA conundrum
• Doing the best with the current empirically-derived lab tests
• A path forward?
Planforthispresentation:

APS:clinicalmanifestationsandlaboratorytests
ClinicalDVT,PE,ATE,
stroke,pregnancyloss,placental
infarction,IUGR,oligohydramnios,preeclampsia
LaboratoryaCLIgG,IgM
aß2GPIIgG,IgM
LA:aPTT,dRVVT,others(aPTT,dPT,KCT,hexagonalphase…)

A“Classic”Case
30 year old woman referred for 4 spontaneous pregnancy losses • Prior History: DVT and pulmonary embolism; imaging studies of
brain showed an old cerebral infarct • Initial labs: Markedly abnormal antiphospholipid tests • Diagnosis: APS Treatment: heparin and aspirin • Course: At 18 wks gestation developed thrombotic microangiopathy
(catastrophic APS) with fetal loss Treated with plasmapheresis, anticoagulation and IV-IgG Subsequently developed recurrent lower extremity DVTs refractory to oral anticoagulant therapy and requires long term LMW-heparin

EmpiricOriginsoftheCurrentAntiphospholipidAssays
1906 Syphilis testing
1940 Isolation of cardiolipin
1950’s BFP
syphilis
1980’s Anticardiolipin antibody
assay; First description of syndrome
1990’s - present Recognition that
cofactors are targets: aß2GPI
antibodies
1950’s PTT inhibitor
1960’s Lupus Anticoagulant;
Association with thrombosis
1980’s Lupus
anticoagulants; aPTT, DRVVT, etc; Association with
APS)

• Negative: Lower than the 95th percentile cutoff (generally <22 GPL units for IgG)
• Low-positive/indeterminate: 95th-99th percentiles
• Medium/moderate-positive: usually 60-80 GPL units
• High-positive = >80 GPL units (Lakos et al, Arthritis & Rheumatism 2012)
InternationalConsensusGuidelinesonInterpretationofaCLantibodyassays

• Complementcontrol/shortconsensusrepeatsuperfamily
• BindsphospholipidviadomainVasmonomer,thenagglomeratesintoclusters
• Deficiencyisnotassociatedwithobviousdiseasephenotype
• Mayplayroleinclearingapoptoticcellsandmembraneparticles
• MayplayaroleinscavengingLPS
• Anti-ß2GPIIgGpromotethrombosisinanimalmodels
Gamsjaeger et al Biochem J (2005) 389:665
ß2GPI(apo-H)isamajortargetantigenforaPLA


Some aPLA Cofactors
• prothrombin • factor V • factor VII/VIIa • protein C • protein S • annexin A2 • annexin A5 • ox-LDL • high and low molecular weight kininogens • heparin plasmin • vimentin • sulfatides (acidic glycosphingolipids) and more ….
SomeadditionalaPLAcofactors

MultiplemechanismshavebeenproposedforAPS
• Disruption of the annexin A5 antithrombotic shield • Disruption of the annexin A2-mediated fibrinolysis • Interferences with protein C and S pathway • Inhibition of TFPI activity • Effects of autoantibodies against: annexins, protein Z, plasmin • Inhibition of ß2GPI-mediated dampening of vWF-platelet interaction • Increase of plasminogen activator inhibitor-1 • Induction of receptors for cell adhesion molecules on endothelium • Induction of tissue factor expression on endothelial cells and on monocytes • Stimulation of platelet activation • Direct injury to endothelium • Induction of apoptosis in vascular cells • Release of membrane-bound microparticles • Complement-mediated injury to trophoblast/endothelium • Antibody-mediated alteration of eicosanoid synthesis • Increase of endothelin-1 • Ab-mediated concentration of prothrombin on phospholipid membranes • Ab binding to intracellular membranes

Diagnostic Criteria Clinical• VascularthrombosisForhistopathologicdiagnosis,thereshouldbeno
evidenceofinflamma9oninthevesselwall
• Pregnancymorbidi9esa=ributabletoplacentalinsufficiency,including:a)threeormoreotherwiseunexplainedrecurrentspontaneousmiscarriages,before10weeksofgesta9on,b)oneormorefetallossesaEerthe10thweekofgesta9on,c)s9llbirth,andd)episodeofpreeclampsia,pretermlabor,placentalabrup9on,intrauterinegrowthrestric9onoroligohydramniosthatareotherwiseunexplained
Laboratory• Mediumorhigh9teraCLoran9-β2GPIIgGand/orIgMan9bodypresenton
twoormoreoccasions,atleast12weeksapart,measuredbystandardELISAs
• Lupusan9coagulantinplasma,ontwoormoreoccasions,atleast12weeksapart
DiagnosticCriteriaforAPS(investigational)

TheAPSConundrum
ClinicalThrombosis
andPregnancyComplications
L a bTestsaCL IgG/IgM,a n t i - β 2GP IIgG/IgM;LA
aPLposesauniquepuzzlebecause:§ Asofyet,thereisno“goldstandard”§ TheclinicalmanifestationsareneitherrarenorspecificforAPS§ Thelaboratorytestsoftendonotcorrelatewitheachother§ Patientswhotestpositivebuthavenothadanarelabeledas“falsepositives”whensomemaynotyethadaclinicalmanifestationbuthaveincreasedrisk

• To review where we are now and how we got here
• To describe the aPLA conundrum
• Doing the best with the current empirically-derived lab tests
• A path forward?
Planforthissegment:

Probability of developing a first VTE correlates with the number of positive aPL antibody tests
Modified from Pengo et al Blood 2011

Cumulative incidence of TE events in triple positives for aPL tests
Pengo et al Blood 2011

PROMISSE (Predictors of pRegnancy Outcome: bioMarkers In Antiphospholipid antibody Syndrome and Systemic lupus Erythematosus
Lockshin MD et al, Arthritis Rheum 2012 64:2311
%Adv
erseClin
icalEvents
%Adv
erseClin
icalEvents
Fig1

• To review where we are now and how we got here
• To describe the aPLA conundrum
• Doing the best with the current empirically-derived lab tests
• A path forward?
Planforthissegment:

PrincipleofLAAssay
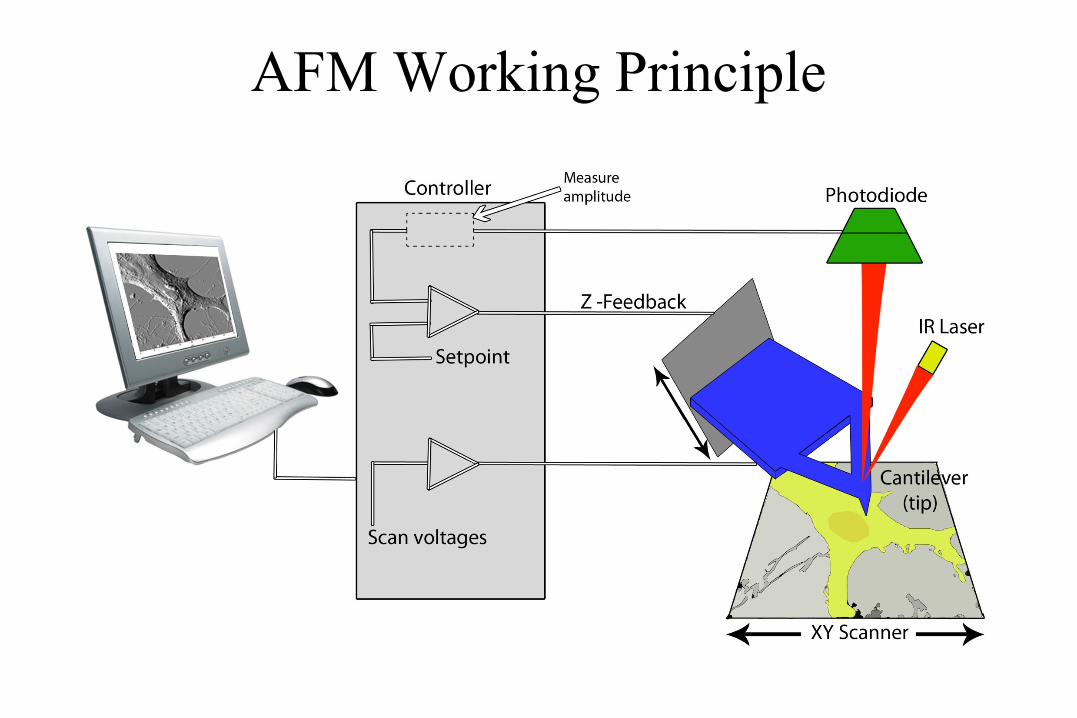
AFM Working Principle

Advantages of AFM • Minimal specimen preparation • Able to image sample unfixed in fluid medium • Resolution for biological samples in nm range
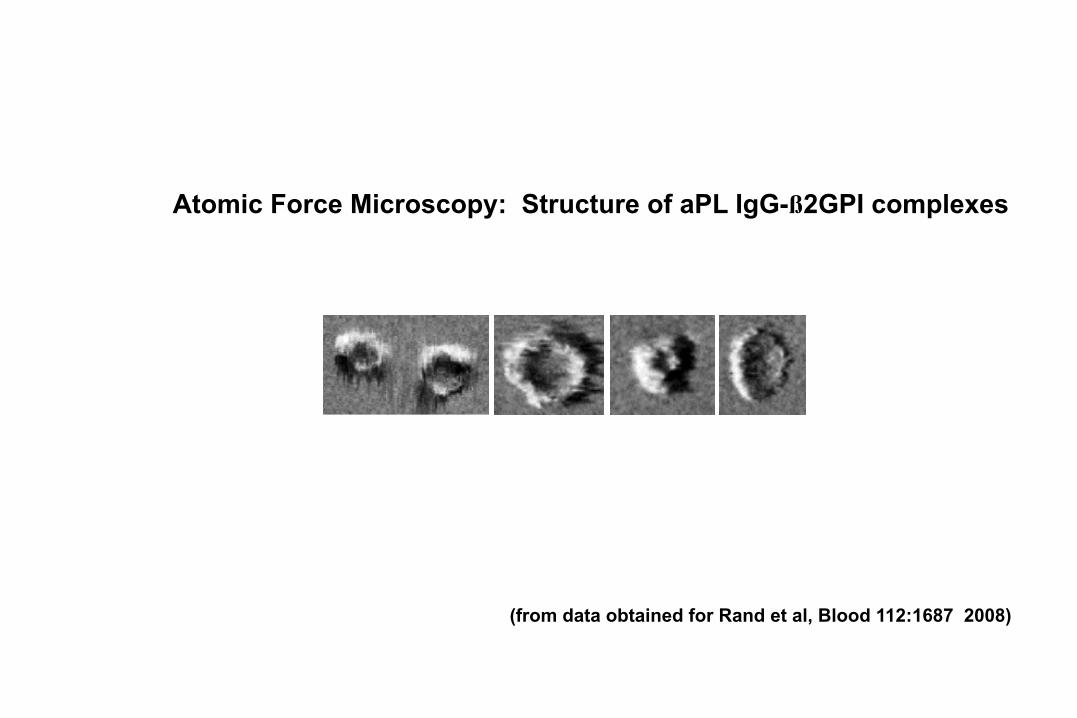
(from data obtained for Rand et al, Blood 112:1687 2008)
Atomic Force Microscopy: Structure of aPL IgG-ß2GPI complexes

Formation of aPL mAb-β2GPI Immune Complexes on Phospholipid Bilayers Visualized
by ImmunoAFM

Time (min)0 2 4 6 8 10 12 14 16 18 20 22 24 26
Bou
nd P
rote
in (µ
g/cm
2 )
0.0
0.1
0.2
0.3
0.4
0.5
0.6 APS IgG + fl2GPI
Control IgG + fl2GPI
Add IgG & fl2GPI ↓
Rapid adsorption of APS immune complexes to phospholipid bilayer

• aPLAlabtestsareempiricallyderivedandcurrentdiagnosticcriteriaareinvestigationalmeanttoidentify“definite”APSpatientsforclinicalinvestigations
• TheLAandmultipositivityappeartobethestrongestpredictorsofadverseclinicaloutcomes
• AFMandSEMimagingdemonstrateformationofaPLAmacro-immunecomplexesonphospholipidmembranes
• Thesearecomposedofimmunoglobulinsandmultipleplasma-derivedcofactors
• Hypothesis:ThecoreabnormalityAPSistheformationofpolyclonalmultivalentmacro-immunecomplexesonvulnerablecellmembranesandvesiclesthattriggermultiplepathogeniceffects
Sometakehomepoints

Weill Cornell and Montefiore-Einstein Collaborators
Pathology Xiao-Xuan Wu Lucy Wolgast Ljiljana Vasovic Mojgan Raoufi Yanhua Wang Jessica Niakan Ervis Bezati Julissa Pena-Medina Mayra Almonte Laura Santambrogio
Pediatric Rheumatology Dawn Wahezi Norman Ilowite Einstein Biochemistry Steve Almo Ron Seidel, III Mark Girvin

Outside Collaborators
UVM - AFM Facility Douglas Taatjes Anthony Quinn Maastricht University Bas de Laat Saartje Bloemen NYU- Ob-Gyn Alan Arslan Seth Guller

Ques9ons?