janemschmaltzportfolio.files.wordpress.com viewrefining the education provided to patients suffering...
TRANSCRIPT

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 1
Refining the Education Provided to Patients Suffering from a Cerebrovascular Accident in the
Acute Care Setting
Jenni McRoy
Kim Nicholls
Jane Schmaltz
University of Mary

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 2
Acknowledgements
This University of Mary Stroke Project team would like to acknowledge the following
people for their efforts making this project possible. First, this project team would like to thank
Claudia Dietrich, faculty Project Advisor, who has been and continues to be a mentor for all
members of this group and helped guide the creative process for this evidence-based project
(EBP). The University of Mary has provided this Stroke team the opportunity to create an
evidence-based project that enhances the quality of patient care and education they receive at
Research Medical Center and other healthcare facilities alike. Without this opportunity, the
members of the University of Mary Stroke Project team would not have had the opportunity to
work and grow together to create the framework for this project. Sherry Bahr, APRN, CNRN,
Stroke Program Coordinator, has been a fundamental resource helping guide this project in the
direction that upholds the healthcare organization’s mission and values by refining the education
patients receive during an acute hospitalization. Through her consistent dedication to this
project, she has expelled an excitement within the executive leadership team, ancillary staff
member's, interdisciplinary team members, and most of all patients and family members at
Research Medical Center that would not have occurred without her support. Research Medical
Center has graciously allowed University of Mary’s Stroke Project team the opportunity to
become cohesive partners enhancing current processes to improve patient outcomes for stroke
patients. Jenni McRoy, the project lead for the University of Mary’s Stroke Project team, has
communicated the vision of Research Medical Center to all members of University of Mary’s
Stroke Project team. Her attention and dedication to the success of this project has been vital
helping guide the direction of the team. Without her efforts, this project would not have been
possible. Kim Nicholls and Jane Schmaltz have dedicated countless hours to the external

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 3
literature review, paper, and the Power Point presentation. Their dedication, support, and
effective communication have helped guide the direction for this project. The front-line core
staff members for their flexibility and constant acceptance to the implementation of change
ensuring the patient’s educational plan of care is top priority.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 4
Table of Contents
Acknowledgements…………………………………………………………………………….….2
Executive Summary……………………………………………………………………………….9
Problem Statement…………………………………………………………………………….....12
Significance of Clinical Problem at the Organizational Level………………………………......14
PICO(T) Question………………...……………………………………………….………….….15
Purpose Statement…………………………………………………………………………….….16
Review of Literature………………………………………………………………………….….17
Literature Search…………………………………………………………………………17
Synthesis of Current Literature……………………………………………………….….33
Organizational Recommendations……………………………………………...………..39
Project Problem Identification…………………………………………………………………...40
Internal Evidence………………………………………………………………………...40
External Evidence………………………………………………………………………..41
Project Recommendations……………………………………………………………………….44
Project Implementation Plan…………………………………………………………….……….47
Change Theory………………………………………………………….……………......47
Key Stakeholders…………………………………………………………………….…..50

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 5
Barriers and Facilitators/ Drivers and Resistors to Change……………………………...53
Business Impact…………………………………………………………….……………55
Organization Planning Process……………………………………………………...…...56
Implementation Plan……………………………………………………………………………..57
Project Measurement Plan……………………………………………………………………….63
Human Subject Protection Statement……………………………………………………………66
Implementation and Measurement…………………………………………………………….…68
Implementation…………………………………………………………………………..68
Measurement……………………………………………………………………………..70
Handoff…………………………………………………………………………………..77
Conclusion...………………………………………………………………………………..........78
References……………………………………………………………………………………......81
Appendix…………………………………………………………………………….……...…....85

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 6
List of Tables
Table 1: External Data: Importance of the Nurse Role in Patient Education……………………18
Table 2: External Data: Importance of the Nurse Role in Patient Education/Level of
Evidence……………………………………………………………………………………….....19
Table 3: External Data: Stroke patient perception of educational needs………………………...23
Table 4: External Data: Stroke Patient Perception of Educational Needs/Level of Evidence…….
……………………………………………………………………………………24
Table 5: External Data: Benefits & Effectiveness of Education………………………....…....…27
Table 6: External Data: Benefits & Effectiveness of Education/Level of Evidence…………….28
Table 7: Internal Data Needs…………………………………………………………………….40
Table 8: Attendance vs. Stroke Census for Weeks 1-10…………………………………………71
Table 9: Pre and Post Survey Questionnaire Results…………………………………………….72

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 7
List of Figures
Figure 1: The Johns Hopkins Nursing Evidence-Based Practice Model………………………49

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 8
List of Appendices
Appendix A: Permission Granting the Use of Johns Hopkins Nursing Evidence-Based Practice
Model……………………………………………………...……………………………………..85
Appendix B: Flyer for Huddle…………………………………………………………………...86
Appendix C: Pre-Education Informative Questionnaire for Patients………………………..…..87
Appendix D: Post-Education Informative Questionnaire for Patients…………………...………88
Appendix E: Stroke Education Course Flyer…………………………………………………….89
Appendix F: Nurse Education Feedback…………………………………………………….…..90
Appendix G: Institutional Review Board (IRB) Application…………..………...……….……..91
Appendix H: IRB Approval……………………………………………………………………...99

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 9
Executive Summary
This University of Mary's Stroke Project team has worked in collaboration with Research
Medical Center (RMC) in Kansas City, Missouri, to implement evidence-based practice (EBP)
interventions, such as a structured stroke support and educational class and enhanced nurse
education regarding the teach-back method, to improve patient understanding of their stroke risk
factors. RMC identified an organizational problem as needing to enhance the educational
understanding of stroke patients and their families through the utilization of a hospital initiated
stroke support and educational program, as evidenced by recurrent admissions and a verbalized
lack of understanding from previous patients and their families.
The purpose of this EBP project was to evaluate and refine the educational process at
RMC in order to enhance the educational understanding stroke patients receive regarding their
individualized specific type of stroke, risk factors, and care. Guided by this information, the
University of Mary's Stroke Project team performed an extensive literature search to assist
RMC's Stroke Program in the refinement of their educational offerings through the most current
and successful evidence-based practices. The themes that were used to complete the literature
review were the importance of the nurse role in patient education, the patient's perspective of
educational needs, and the benefits and effectiveness of education. As the external data provided
supportive documentation, the internal data from RMC supported the recurring themes noted
during the external literature review; as well as provided an exclusive insight suggesting a great
need for refining education provided to patients during an acute hospitalization.
The University of Mary's Stroke Project team proposed their recommendations for a
formalized structured classroom setting; where a weekly education class dedicated to providing
stroke education to patients and their families in order to reduce the patient’s risk of suffering

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 10
from an subsequent stroke. In addition, the proposed recommendation was to review the stroke
booklet in detail with front line staff and all new orientees with a member of the University of
Mary's Stroke Project team, the Stroke Program Coordinator, the Stroke educators, or the Stroke
Registered Nurse Navigators.
The Stroke Team’s Nurse Navigators initiated the required weekly staff re-education of
stroke patient education to all nursing staff delivering direct care to stroke patients. The
education occurred during morning and evening huddles on each unit that house stroke patients
ensuring all front-line staff attend this education can attend. The front-line staff was re-educated
on the stroke booklet that all patients receive at the time of admission when diagnosed with a
stroke.
Through collaborative efforts, a weekly stroke support and educational class was
designed and implemented. The project lead referred to the stroke booklet during a PowerPoint
presentation, expanding on the written content. Alternative methods to promote attendance and
compliance to the stroke support and education class were discussed and implemented. These
included announcing every Thursday during bed huddle the time and location of the stroke
support and education class, along with overhead paging a reminder one hour prior to the class
start time. Overall, the two superior strengths after implementation included the enhanced
understanding the patient and family members have verbalized, and the self-confidence and
empowerment nurses have verbalized. Incorporating the baseline metrics revealed through the
internal data review, project measurements were identified utilizing the mnemonic acronym
S.M.A.R.T. Pre and post-education questionnaires were administered and tracked using an excel
spreadsheet. During the introduction of each class a questionnaire was completed to evaluate
their understanding of strokes, risk factors, and signs and symptoms. After the presentation, a

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 11
questionnaire was completed asking the same initial six questions along with asking for an
explanation of what benefits they received from this intimate disease-specific education, as well
as what could be improved on the class.
To measure the efficacy of this training of the education that was provided to nursing
staff, a routine post education survey was distributed which resulted in 100% of nurses feeling
like the nurse patient education and teach-back method were an imperative aspect to evaluating
patient understanding. The nurses expressed feelings of empowerment and self-confidence
through the education and use of the nurse-patient teach-back tool. This aspect continues to be
crucial for nurse retention and loyalty for any healthcare organization.
Implementing an educational opportunity in a safe environment that provides a
personalized approach to the patients and their family members has promoted a cohesive
learning environment. This opportunity enhanced the knowledge level of the patient and family,
and promoted and encouraged healthier lifestyle choices potentially extending the longevity of
their life. Implementing these interventions helped make patients more knowledgeable about
their disease process so they are less likely to experience negative outcomes and less uncertainty
related to their stroke diagnosis. A handoff plan was developed so RMC could continue on with
the implementation of these interventions that will continue to improve the lives of individuals
and their family members suffering from this devastating, life-altering diagnosis.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 12
Refining the education provided to patients suffering from a Cerebrovascular Accident in the
Acute Care setting
In the United States, approximately 800,000 people suffer from cerebrovascular accidents
(CVA) a year (American Stroke Association, 2016). As a result of this, CVA’s, also known as
stroke or transient ischemic attack (TIA), are the 5th leading cause of death in the United States
and are also the number one cause of long term disability (ASA, 2016). Evidence-based research
suggests that when a patient is able to speak to their current status, know their personal risk
factors and how to prevent future strokes, they are less likely to experience future CVA’s while
improving their disability from current deficits. Due to the substantial need for understanding,
the focus of this University of Mary’s Stroke Project team has been directed towards reducing
future strokes in patients that have already suffered from a CVA by improving their knowledge
level regarding their specific risk factors affecting their personal disease process.
The following will identify common themes that were found while conducting a review
of literature for improving education for patients that have recently experienced a stroke. This
University of Mary’s Stroke Project team has worked in collaboration with Research Medical
Center to implement evidence-based practice (EBP) interventions, such as an organized and
structured stroke support and educational class and enhanced nurse education regarding the
teach-back method, to improve patient understanding of their risk factors. By understanding
these risk factors, patients can incorporate preventative techniques into their lifestyle to reduce
the likelihood of the patient experiencing additional CVA’s in their lifetime.
Problem Statement
From a global perspective, strokes do not discriminate against who they affect. Patients

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 13
are affected by CVA’s everywhere around the world; proving an imperative need for enhanced
educational opportunities and a comprehensive understanding of this particular disease process.
The more patients and their families understand about personal stroke risk factors, signs and
symptoms, and care, the more likely they are at implementing an interventional strategic plan to
help reduce their risk for recurrent strokes or recurrent hospital admissions.
When a stroke occurs, patients and their families are often in shock and only retain a
portion, if any, of what the healthcare professionals are explaining to them. Leaving a hospital
after suffering a stroke can be frightening and quite possibly overwhelming. Having a plan in
place to assist patients and their families with thorough education personally geared towards
their specific type of stroke, will help facilitate an understanding of what to look for and what to
expect.
Problem statements encompass the concerns or problems that are acknowledged in a EBP
project. Sherry Bahr, APRN, CNRN, Stroke Program Coordinator, along with Research Medical
Center’s executive leadership team have identified the organizational problem as needing to
enhance the educational understanding of stroke patients and their families through the
utilization of a hospital initiated stroke support and educational program, as evidenced by
recurrent admissions of stroke patients and a verbalized lack of understanding from previous
patients and their families. Guided by this information, The University of Mary’s Stroke Project
team performed an extensive literature search to assist Research Medical Center’s Stroke
Program in the refinement of their educational offerings through the most current and successful
evidence-based practices.
A coordinated educational process dedicated to chronic disease education such as this
should be a priority; not only for the organization this project is benefitting, instead a national or

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 14
worldwide focus to help combat CVA’s being one of the highest leading causes of death and
long-term disability. With extensive education programs, this will help to consistently provide
the knowledge necessary to facilitate an understanding of strokes and stroke care. Furthermore,
this educational understanding will help to reduce future readmissions or potentially help prevent
future strokes.
Significance of Clinical Problem at the Organizational Level
Research Medical Center of Kansas City has identified an increased admission rate for
recurrent stroke victims for individuals suffering from a CVA. During daily rounding and
conversations with these individuals and their family members, a lack of understanding
regarding personal specific risk factors and necessary interventional implementations for
improved health wellness have been identified by the executive and direct leadership teams.
Lack of education and a comprehensive understanding of personal risk factors are interrelated
and are measured through a verbalized lack of ability to restate personal specific risk factors
leading to their primary stroke. Along with an inability to verbalize personal risk factors is an
inability to state an optimal personalized interventional implementation plan to improve upon
current risk factors reducing their chance of suffering from a secondary CVA.
On an organizational level, these interrelated factors are measured through an increased
readmission rate for secondary strokes leading to potential financial organizational burden and
increased individual mortality and morbidity rates. In fact, 1 out of 4 individuals suffering from
a primary diagnosis of a stroke will suffer from another stroke in their lifetime (Furie, 2011).
Recently designated as a Comprehensive Stroke Center places an imminent organizational need
to refine educational processes enhancing patient knowledge. This enhanced knowledge level
will assist and lead the patient and their family to an improved health status post discharge.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 15
Improving the quality of care provided in health care organizations is of key significance.
Reimbursement methods are based off a multitude of key factors including readmissions rates
and patient satisfaction scores. Identified patient and family dissatisfiers include lack of
education and an increased fear of not being prepared to provide necessary cares post-discharge.
This fear, as noted from verbal conversations with patients and family members, is based off an
undesirable lack of confidence in understanding personal specific risk factors and how to
implement lifestyle changes. Therefore, refining the education and enhancing educational
opportunities for patients and families suffering from a primary or secondary diagnosis of a CVA
can provide the individual and their family the crucial information to make a more informed
interventional strategy improving their overall health wellness by decreasing their risk for
disease induced mortality and morbidity.
PICO(T) Question
For the purpose of this EBP project, the PICO(T) question format was utilized to
formulate a well-rounded researchable question. The EBP project clinical question follows
wording that includes (P) the population or patients, (I) the intervention or influence, (C)
comparison, and (O) the outcomes (Polit & Beck, 2017). Often times the utilization of (T) time is
added to the question to indicate the timeframe representing in the question.
The University of Mary’s Stroke Project team has identified the need to enhance the
educational understanding for patients that were recently diagnosed with a stroke for this project.
In order to ensure the group met the needs of the organization, a PICOT question was developed.
The question written for this EBP project is “How are recent stroke patients (P) who complete a
coordinated educational process in a formal organized hospital stroke program (I), compared to
the current practice of no formal organized hospital stroke program (C), impact understanding

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 16
(O) within the first 6 weeks(T)?”
Purpose Statement
The purpose of this EBP project was to evaluate and refine the educational process at
Research Medical Center, a comprehensive designated Stroke Center and Level One Trauma
hospital in Kansas City, Missouri, in order to enhance the educational understanding stroke
patients receive regarding their individualized specific type of stroke, risk factors, and care. This
evaluation of current processes and offered educational opportunities Research Medical Center is
presently practicing would include personalized specific health and wellness interventions,
comprehensive understanding of medication compliance, therapy treatments, and utilization of
organized support systems and local community resources.
The EBP project has initiated a more comprehensive educational process for patients
suffering from a CVA beginning upon admission. The goal was to identify the health care needs
that include education to the patient and family regarding their specific risk factors, the type of
stroke they suffered, the location of the stroke, and how it will affect their life moving forward.
This EBP project was intended to improve the patient's comprehensive understanding of their
personal specific risk factors, medication compliance, therapy treatments necessary for
improving their personal outcomes, lifestyle modifications, and utilization of organized support
and educational systems, and local community resources. Educational opportunities for current
and newly hired staff members were also been identified as an area of opportunity; along with a
more in-depth process necessary to educate patients and families suffering from a stroke.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 17
Review of Literature
Literature Search
Nurses are one of many members of the multidisciplinary team that assist in providing
patient education. As the literature review was completed by the University of Mary’s Stroke
Project team, a common recurring theme was the importance of patient education by nurses and
all interdisciplinary members of the team. The goal of this education is to provide the patient
with the tools they need to successfully understand their personal diagnosis and how to better
themselves. The themes that were used to complete the literature review were the importance of
the nurse role in patient education, the patient’s perspective of educational needs, and the
benefits and effectiveness of education.
A literature review was conducted to find adequate data to support the need for this
project. The search engines that were used for this review were The Cumulative Index to
Nursing and Allied Health Literature (CINAHL), Cochrane Database, and MEDLINE. The key
search words that were used to capture the needs of this project and the results of those searches
in each database are listed in tables 1-6 below. A filter was placed to capture data between 2010
and 2017 to ensure the most up to date data was collected. Another filter was added to only
include full text articles. It was found that the abstract of an article provides a summary of the
article that is being reviewed, but without the data within the research articles it is difficult to
find supporting evidence for this project.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 18
Table 1
External Data: Importance of the Nurse Role in Patient Education
CINAHL MEDLINE Cochrane
Nurse education 1,328 498 315
Patient education 5,979 9,097 4,705
Nurse empowerment 51 13 7
Stakeholders and stroke
45 61 0
Nurse empowerment and education
19 5 1

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 19
Table 2
External Data: Importance of the Nurse Role in Patient Education/Level of Evidence
Full APA Citation Research Purpose
Study Design
Sample (Setting)
Data Collection/
Measures
Analysis/
Outcomes
Strengths/
Limitations
Joanna Briggs Level of Evidence
Study Quality
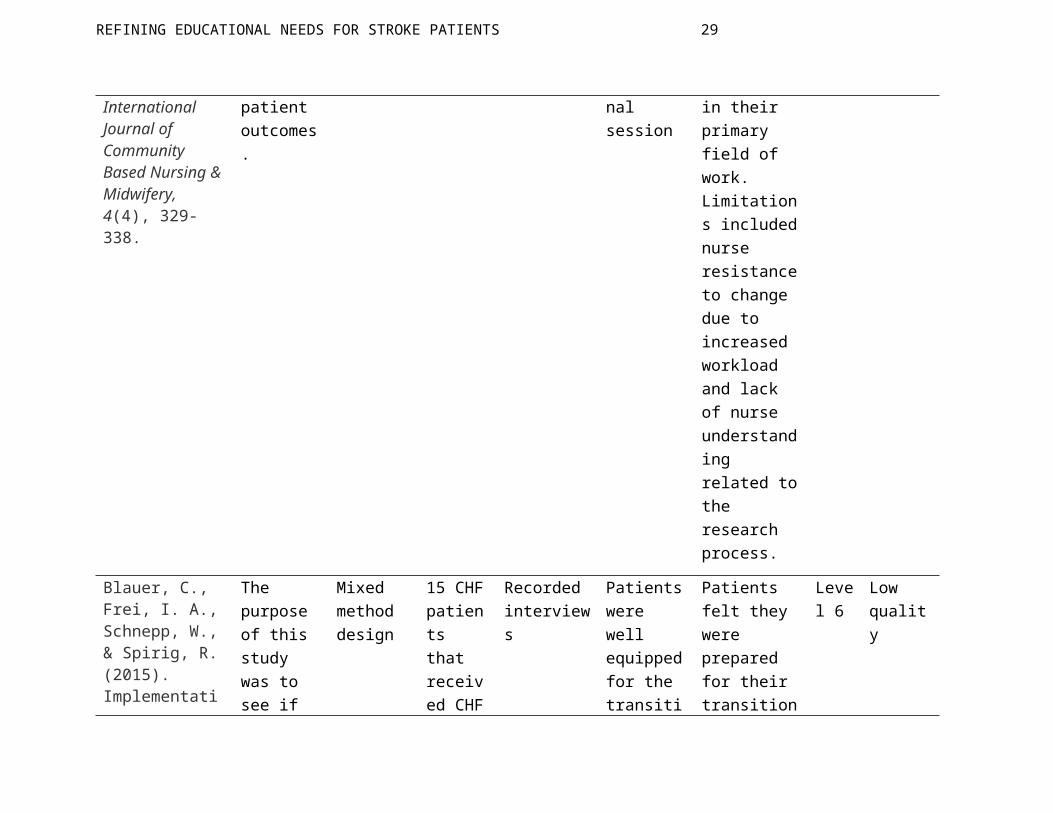
Aslani, Z., Alimohammadi, N., Taleghani, F., & Khorasani, P. (2016). Nurses’ empowerment in self-care education to stroke patients: An action research study. International Journal of Community Based Nursing & Midwifery, 4(4), 329-338.
The purpose of this study was to evaluate if there was a link between the level of nurse empowerment and patient outcomes.
Action research design
23 nurses who volunteered from an inpatient neurology unit.
Semi-structured group and individual interviews were conducted until data was saturated.
Nurses felt they were better prepared to answer questions with concise answered after the educational session
Based on the results of this research, the study was able to support the importance of providing additional education for nurses in their primary field of work. Limitations included nurse resistance to change due to increased workload and lack of nurse
Level 6
Low quality

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 20
understanding related to the research process.
Blauer, C., Frei, I. A., Schnepp, W., & Spirig, R. (2015). Implementation of a nurse-led education programme for chronic heart failure patients during hospitalisation and strategies supporting their self-management at home: A practice development project in the context of the Swiss healthcare system. International Practice Development Journal, 5(1).
The purpose of this study was to see if creating nurse led education programs could meet the need of patients.
Mixed method design
15 CHF patients that received CHF education from nurses at the time of discharge.
Recorded interviews
Patients were well equipped for the transition home, but the patients individual living situations were not accounted for and were unprepared to deal with those challenges.
Patients felt they were prepared for their transition home. Some limitations to this study was the sample size was limited and the education did not anticipate challenges patients experienced in their home environment.
Level 6
Low quality
Håkanson, C., Sahlberg-Blom,
To find a relationship
Evaluative research
51 patients
Two self-assessment
Statistical analysis
Positive outcomes were
Level Low

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 21
E., Ternestedt, B., & Nyhlin, H. (2011). Learning to live with irritable bowel syndrome. The influence of a group-based patient education programme on peoples' ability to manage illness in everyday life. Scandinavian Journal Of Caring Sciences, 25(3), 491-498.
between group based education and management of a chronic disease.
design with irritable bowel syndrome that participated in the group visits
questionnaires were used to gather data. The first one was prior to group education and the second was sent out about 2-3 months following the education.
with software.
reported via patient survey. Limitations were noted as not having a controlled group and there was a high dropout rate from the first survey to the second.
6 quality
Sherman, J.R. (2016). An initiative to improve patient education by clinical nurses. MEDSURG Nursing, 25(5), 297-333.
The purpose of this study was to review simulations about patient education to see if nurses developed a better understanding of
Cross-sectional design.
66 RN’s that were going through annual training.
Utilized pre-and-post tests to identify areas of improvement.
Pre-and-posttest that were evaluated by statistical analysis.
Reviewers collected 66 pre-and-posttests from RN’s. The simulations found statistically significant improvements to nurses’ knowledge regarding
Level 6
Low quality

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 22
performing patient education.
teaching patient education and identify proper teach-back technique.
Limitations that were identified were a small sample size and the statistical significance of tools were not determined to be reliable.
REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 23
Table 3
External Data: Stroke patient perception of educational needs
CINAHL MEDLINE Cochrane
Stoke education 346 793 13
Patient needs 15,180 10,064 8
Patient perception 4,771 2,984 3
Stroke awareness 176 505 2
1&2 11 5 23
1&3 2 1 92
1&4 51 77 28
2&3 434 41 22
2&4 4 18,306 19
3&4 4 1 24

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 24
Table 4
External Data: Stroke Patient Perception of Educational Needs/Level of Evidence
Full APA Citation Research Purpose
Study Design
Sample (Setting)
Data Collection/
Measures
Analysis/
Outcomes
Strengths/
Limitations
Joanna Briggs Level of Evidence
Study Quality
Sowtali, S. N., & Harith, S. (2014). Educational Needs among Stroke Patients Admitted to Hospital Universiti Sains Malaysia: Preliminary Findings. Jurnal Sains Kesihatan
The purpose of this study was to gather basic information about the types of educational needs among
A cross-sectional survey in the format of a preliminary descriptive correlation study design.
41 stroke patients diagnosed and confirmed with CT scan were chosen from the Universiti Sains Malaysia Hospital’s Medical and
A questionnaire consisting of five domains related to stroke; each domain contains questions that reflect a topic related to stroke was
The results showed a perceived need from the patients for more education needed on general information about stroke, and on prevention and causes of strokes; needs on the risk factor management of stroke; needs on treatment of stroke from medicine, surgery and traditional medicine
Strengths included were the study’s highlighted points that stroke patients were more interested to know about prevention, causes and risk factors of stroke. The limitations to this study were the difference of
Level 3
Moderate quality was determined based on content validity and internal consistency for questionnaire using Cronbach’s alpha.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 25
Malaysia, 12(1), 67-73. doi:10.17576/jskm-1201-2014-09
stroke patients admitted to Hospital Universiti Sains Malaysia, in order to get preliminary information to help design further educational interventions.
Surgical floor between September to December 2012.
given to the patients prior to discharge.
aspects; need to know for all listed post-stroke problems, including the post-stroke diet management. Data obtained were analyzed using SPSS 20.0 descriptively. Ethical clearance was obtained from HUSM Human Ethical Committee prior to study.
medical history background might impact the degree of educational needs; only one stroke patient had no previous medical disease prior to stroke; and there is still an uncertainty whether single morbidity or multiple morbidities had impact on the stroke education needs.
Yonaty, S., & Kitchie, S. (2012). The Educational Needs of Newly Diagnosed Stroke Patients. Journal of Neuroscience Nursing, 44(5),
To determine if there is a change in the perceptions of what individuals
Descriptive correlational study design.
71 newly diagnosed, first-time stroke patients from two metropoli
A questionnaire with eight domain related to stroke; each domain contains
Analysis through descriptive statistics, t tests, and repeated measures ANOVA.
Satisfaction levels were below level 4 on Likert’s scale; making the overall perception of education not
Level 3
High quality was determined based on content validity,

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 26
E1-E9. doi:10.1097/jnn.0b013e31826663f2
newly diagnosed with stroke perceive as important to learn about stroke during different times of their stroke recovery.
tan hospitals in the Northeast.
questions that reflect a topic related to stroke. Initial questionnaire given within 24-72 hours of admission, again upon discharge, and 2 weeks post discharge.
The outcomes determined the medical knowledge and medication treatment were rated the most important to learn; however, treatments with herbal or alternative medicine and dietary habits were the least important to learn about.
satisfactory. Limitations of the primary researcher being the only one involved in selection of patient participation, some patients unable to complete second questionnaire due to early discharge, only two designated stroke centers, the study was self-reporting, and the number of patients could have been larger.
internal consistency for questionnaire using Cronbach’s alpha, no assumptions were violated, reading level was at a grade 6, eligibility and sampling procedures followed.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 27
Table 5
External Data: Benefits & Effectiveness of Education
CINAHL MEDLINE Cochrane
Stoke education 782 435 13
Patient education 69,386 26,282 122
Benefits of education 2,672 1,287 5
Effectiveness of education 2,637 2,039 35
1&2 225 67 85
1&3 16 3 100
1&4 22 17 117
2&3 539 210 4
2&4 605 448 17
3&4 67 40 1

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 28
Table 6
External Data: Benefits & Effectiveness of Education/Level of Evidence
Full APA Citation
Research Purpose
Study Design
Sample (Setting)
Data Collection/
Measures
Analysis/
Outcomes
Strengths/
Limitations
Joanna Briggs Level of Evidence
Study Quality
Ing, M. M., Linton, K. F., Vento, M. A., & Nakagawa, K. (2015). Investigation of stroke needs (INVISION) study: Stroke awareness and education. Hawai’i Journal of Medicine & Public Health,
The purpose of this study was to assess the overall understanding and effectiveness of current inpatient stroke
A qualitative study design.
21 participants consisting of 10 patients who were recently hospitalized with intracerebral hemorrhage and their caregiver
Data was collected by two trained research staff members conducted face-to-face, semi-structured interviews with caregivers and patients
The voice-recorded interview data was transcribed and content analysis was performed. The content was placed into codes that grouped the data into recurrent and prominent themes across participants. The researchers developed a codebook to display the broad themes that were apparent;
Strengths of the study show that the qualitative methods that were utilized to capture the complexity of stroke education and awareness experienced by specific individual patients and their caregivers. Limitations for this study
Level 6
Low quality
REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 29
74(4), 141-145. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4407457/
education practices.
s (11 participants) during the follow-up visits were interviewed at the Queen's Medical Center; which is located on Oahu, the largest hospital in Hawaii.
utilizing scripted questions developed by the research team. The scripted questions consisted of open-ended questions with a focus on nine major subjects related to strokes.
based on the frequency, emotion, and extensiveness of the narrative. The two authors then discussed and created the final analysis codebook. The analysis codebook revealed three themes presented as concerns; lack of stroke knowledge or awareness, need for stroke education, and fear of stroke recurrence due to inefficient education while hospitalized. This study suggests a need for increased continuity and communication with health-care providers to address the evolving educational and practical needs of
include the small number of participants limits the generalization of the results, limiting the participation selection due to geographic locations of the Hawaiian Islands made it difficult to expand to other areas within the Hawaiian Islands, limitations of participants due to language barriers due to the caregivers and patients being required to speak English in order to participate in this study, which could

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 30
stroke patients and their caregivers after hospital discharge.
have possibly overlooked certain populations due to the narrative properties of the qualitative study.
Sanders, K., Schnepel, L., Smotherman, C., Livingood, W., Dodani, S., Antonios, N., ... Silliman, S. (2014). Assessing the impact of health literacy on education retention of stroke patients. Preventing Chronic Disease, 11, 1-10. http://dx.doi.o
The purpose of this study was to assess the relationship of patient’s health literacy to stroke education outcomes, following stroke education in an acute stroke unit at a hospital
A prospective cross-sectional qualitative study.
The sample consisted of 100 patients who were admitted to the hospital stroke unit with a diagnosis of acute ischemic stroke at the University of Florida Health in Jacksonville Florida. Participants were
Health literacy levels were measured by using the short form of Test of Functional Health Literacy in Adults (S-TOFHLA). Standard Joint Commission patient education protocols were utilized to provide patients with appropriate standardized
Statistical analyses and modeling were conducted using SAS version 9.3. Continuous variables were described by using means, standard deviations (SDs), and medians. Category variables were analyzed using Pearson χ or Fisher Exact tests, when appropriate. Univariate and multivariable analyses were used to identify factors independently associated with Stroke Patient Education Retention (SPER) score. For
Strengths for this study was the link formed between heath literacy and educational retention for stroke patients. Thus determining the need for education based on literacy levels. The limitations to this study was the lack of evidence validating the stroke patient educational outcomes, such as long-term retention and patient adherence or compliance to medical
Level 6
Low quality

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 31
rg/10.5888/pcd11.130259
in Jacksonville, Florida. A secondary intention of the study was to assess the relationship between patient demographics and other characteristics associated with the patient’s levels of health literacy and to explore their relationship to education
identified and recruited by the treating neurologist or a stroke unit nurse manager.
stroke education. The post stroke care educational outcomes and knowledge retention was assessed for each participant upon discharge through the utilization of a questionnaire that consisted of a series of 5 questions that were derived from the Joint Commission’s stroke performance measures on stroke education. The effect of health
univariate analysis, the differences in the SPER scores among the 3 S-TOFHLA groups were assessed using the nonparametric Kruskal–Wallis. For multivariate analysis, analysis of covariance (ANCOVA) was used to model the data and estimate the least squared means. Even after receiving the Joint Commission standardized recommended education, only 12% of the patients could identify all 5 warning signs for a stroke, 43% could name all of their personal risk factors, and fewer than half could identify the type of stroke they suffered. The study showed ineffective education of patients; all of which can be influenced by health
treatments. The other limitations the authors recognized was the small sample size for such a large population, to be able to detect the effect of many demographic factors on stroke occurrence.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 32
al outcomes in ischemic stroke patients at the time of their hospital discharge.
literacy on the Stroke Patient Education Retention scores was assessed by using univariate and multivariate analyses.
literacy and knowledge retention, which was the focus of the study. The patients’ inadequate health literacy had a significantly lower stroke education retention rate than patients with marginal or adequate literacy. The analysis displayed an overwhelming connection between health literacy and stroke education outcomes.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 33
Synthesis of Current Literature
After completing the review of literature, three major themes were found in the data.
These themes were elevating the nurse’s role in patient education, understanding the patient’s
perception of education needs in stroke patients, and the benefits and effectiveness of patient
education. The following sections will expand on the external data that was found to support
these major themes.
Elevating the Nurse’s Role in Patient Education. There have been major shifts in the
way patient education is managed during a hospital stay over the past 10 years and changes will
continue to occur. Since change is happening at a rapid rate, it is important for nursing staff to
understand their role and how it relates to patient outcomes. The literature review revealed that
nurses are not adequately prepared to provide patient education during hospitalization.
In order for nurses to provide adequate education to patients, they must feel empowered
to do so. The feeling of empowerment allows nurses to have the impression that they have
benefitted the patient while also feeling a sense of accomplishment (Aslani, Alimohammadi,
Taleghani, and Khorasani, 2016). In order for the organization to support this, the nurses must
have the resources and skills to provide sufficient patient education. If the nurses feel there are
barriers hindering their ability to provide education, the nurses can become frustrated and may
not support the initiative (Melnyk & Fineout-Overholt, 2015).
Another way for an organization to better support the empowerment of nurses is to
provide sufficient knowledge regarding patient education topics. The lack of knowledge by
nurses in understanding and providing patient education was also a common theme recognized
during the external literature review. In nursing school, nurses are prepared to manage patients
at all levels of care throughout the spectrum of life. Due to this, it is difficult to educate nurses

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 34
on the intricate details of specialty units. One study found that patients had better outcomes
when nurses had several training sessions related to disease specific education (Blauer, Frei,
Schnepp, & Spirig, 2015).
One challenge for nurses in becoming proficient at administering patient education is that
there is no one way to provide patient education because there are so many factors to consider
such as patient’s health literacy and resources (Sherman, 2016). Even within a single
organization, it can be difficult to find continuity among the different units. Based on a study by
Sherman (2015), it was found that nurses felt more confident when a consistent method of
providing patient education was used. The author recommended staff provide education using
the teach-back method while using similar patient education tools as it allows the nursing staff to
gain insight into the patient’s understanding of the education (Sherman, 2015). The teach-back
method allows the patient to explain to the educator the information that was just reviewed
(Tamura-Lis, 2013). By allowing the patient to explain the education to the nurse or other
member of the multidisciplinary team, the team member will know whether the patient fully
understands the teaching. These skills can also instill confidence in the nurse’s abilities.
When nurses feel they have confidence in their ability to teach, they can share their
knowledge with patients in larger group settings such as group visits. This concept has gained
traction in recent years and is now being offered more consistently across the healthcare
spectrum. In a study conducted by Håkanson, Sahlberg-Blom, Ternestedt, and Nyhlin (2011), it
found that patient’s “experience of the illness is most certainly influenced by his or her level of
knowledge about the disease” (p. 496). Developing a safe group setting allows patients the
confidence to discuss their experiences and knowledge which can be beneficial for all members
of the group while also having a healthcare professional guide the discussion. Another key

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 35
factor identified was the use of a multidisciplinary team approach to provide patient education
assisting in improving the patient’s ability to cope with their illness; while also improving their
understanding of symptom severity (Håkanson, et. al., 2011). Nurses can use these platforms as
a way to provide education to several patients allowing patients to teach and learn from one
another with the guidance of nurses and other multidisciplinary team members.
Stroke Patient Perception of Educational Needs. The stroke patient’s perception of
their personal educational needs becomes vitally important in their willingness to learn and retain
the material being taught to them. There are many different topics to teach stroke patients and
their caregivers in order to help increase their level of educational understanding of their disease
process. The subjects that pique the interest of different patients at different intervals of their
recovery are the subjects or information that the staff need to pay particularly close attention to.
These areas typically hold an element of fear due to the unknown; these areas of focused learning
will help ease their fears and enhance their learning.
The overall findings from the external data indicate that education for stroke patients is
nothing short of lacking. Patients relay their dissatisfaction with the education they received and
deemed many specific topics as being very important to know and understand about their stroke
diagnosis. “Stroke patients often express a lack of understanding about the nature of their illness,
treatment, and recovery, and they perceive information from healthcare professionals to be
inadequate and too complicated” (Choi-Kwon, Lee, Park, Kwon, Ahn, & Kim, 2005, p. 86). This
lack of understanding regarding their disease process leads to many thought provoking questions.
Gaining the “answers to such questions and educating newly diagnosed stroke patients about
stroke-related information that is presumed to be important to them to learn is vital in the
prevention of further illness and complications after a stroke as well as in the recovery phase”

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 36
(Yonaty & Kitchie, 2012, p. E1).
Choi-Kwon, et. al., (2005) developed a questionnaire that has been utilized in many
studies to determine what stroke patients want to learn about or what they find as an important
topic to learn about and understand. Two of the studies that cited the utilization of this
questionnaire, incorporated several of the domains listed on the original questionnaire. These
domains included but not limited to: medical knowledge, risk factors, treatments with
medication, treatment with surgery, treatment with herbal or alternative medicine, rehabilitation,
dietary habits, and other topics such as ability to think, talk, work, drive, and understand (Yonaty
& Kitchie, 2012). These domains were listed in congruence with several subcategories listed
under each domain. The domains were then worked into the two studies to determine what
patients thought were the most important domains to learn about for them personally. In the
Yonaty & Kitchie, (2012) study, medical knowledge and medication treatment were rated the
most important to learn; dietary needs and treatments with herbal or alternative medicine were
considered the least important to learn. In the study by Sowtali & Harith, (2014), educational
needs highlighted that stroke patients were more interested to know about prevention, causes and
risk factors of strokes, than any other domains listed on the questionnaire. The essential need for
further education continues to be of the utmost importance stroke patients and their families.
Educational needs and enhanced understanding of strokes and stroke care, can be deemed a
necessity as evidenced by the external supportive data for further education.
Benefits & Effectiveness of Education. In a world where the hospital length of stay
seems to be getting shorter by the day, educating patients beginning upon their admission
becomes a necessity. The elements of knowledge and understanding are essential for patients to
feel comfortable and confident recovering at home. There are many fundamentals of education

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 37
that benefit the patients, especially those patients with a recent stroke diagnosis.
The benefits to stroke education can be life changing if the education given is effective
and memorable. In order for stroke education to be beneficial or effective, there must be a great
deal of attention placed on individualizing the approach necessary to help each patient
individually. There must be consideration taken towards comprehension through the patient's’
health literacy, as well as any residual deficits that could inhibit understanding and retention of
materials being taught. The health care professionals must pay close attention to the efficacy of
their teaching styles and if the patient is benefiting from the educational sessions. Often times an
alternative method of teaching would need to be utilized in order to ensure the patient and their
caregiver is receiving effective education providing the fundamental foundation assisting in their
post-discharge care.
There are multiple barriers to the benefits and effectiveness of educating a patient and
their families; health literacy positions itself at the top of the list. Health literacy is a major
barrier that hampers the ability of stroke patients to reduce their risk of strokes by the inability
“to obtain, process, and understand health information and services needed to promote better
health” (Sanders, Schnepel, Smotherman, Livingood, Dodani, Antonios, Silliman, 2014, p.2). In
patients with a lower health literacy understanding, they are less likely to understand their
medical condition, comply with recommended treatments, or reduce the modifiable risk factors
associated with stroke recurrence, thus making their stroke education ineffective and not
extremely beneficial.
Ineffective educational experiences need an approach that would modify the material in
order to accommodate differences in literacy and understanding. “Developing approaches to
education that adjust to the individual circumstance of each patient are likely to be needed, given

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 38
the variation in patient being served” (Sanders et al., 2014, p.5). In order to improve the efficacy
and understanding to all ranges of health literacy, the external data shows a need for
modifications in the educational delivery that focus on the patient's overall understanding on a
personalized level.
Educational materials that are difficult to understand or that are not very effective can
create a communication barrier between the patients, caregivers, and their healthcare providers.
Despite providing the stroke education materials to the patients and caregivers, these materials
are often not actually utilized by the patients if there is not comprehensive information regarding
care for their current state, as well as care that will be needed throughout their recovery. “While
presenting information just prior to discharge may be a practical time for stroke care providers to
educate caregivers and patients, there are studies that demonstrate patients need information
pertaining to care after discharge” (Ing, Linton, Vento, & Nakagawa, 2015). The lack of
comprehensive education can lead to anxiety, unanswered questions, and ineffective education to
the patients and their families.
Similar to other areas of chronic illnesses, educational needs change over time during the
illnesses, and the optimal timing and mechanism of effective delivery of stroke education needs
to be further considered; especially since occasionally stroke patients cannot remember the
hospitalization or education at all (Ing, Linton, Vento, & Nakagawa, 2015). In order to facilitate
beneficial and effective education, the patient’s education must begin upon their admission, and
often times there is a need for repeating the material throughout their hospital stay to ensure
understanding. The external data shows that the efficacy of the education provided to stroke
patients and their family’s needs to be refined. Healthcare organizations and stroke teams have a
great need to perfect their educational materials and delivery methods, in order to capture this

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 39
powerful moment to provide an all-inclusive education to their patients and caregivers.
Organizational Recommendations
As the external data provides supportive documentation, the internal data from Research
Medical Center provides an exclusive insight suggesting a great need for refining education
provided to patients during an acute hospitalization (see table 7). Moreso, the preparation for
home beyond the hospital, after a life-altering experience, is proving to be inadequate. Thus
stating, patients and families are ill prepared to provide care for themselves, or a loved one, once
they are discharged from the acute care facility.
For Research Medical Center, this had become visibly evident with an increase of
hospital readmissions, and a verbalized discomfort from patients in regards to their provided
education. Therefore, the University of Mary’s Stroke Project team in collaboration with the
Stroke Program at Research Medical Center recommended to refinement of the education
provided to patients suffering from a stroke diagnosis, starting with the design and
implementation of a formal structured stroke support and weekly educational class for all
inpatients. The next recommendation was to provide the nursing staff, along with
multidisciplinary team members, the skills and tools necessary to provide adequate education for
this vulnerable population through a re-education of cerebrovascular disease and the associated
risk factors during morning and evening huddle times. Refined education utilizing the already
implemented stroke booklet was also provided to the front-line nursing staff that incorporated an
organizational verbal teach-back method in order to evaluate patient and/or family understanding
of their specific disease process and personal risk factors.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 40
Project Problem Identification
Internal Evidence
Table 7
Internal Data Needs
Data Need Special Considerations Source
Improved Stroke Education Patients diagnosed with cerebrovascular accident (CVA) or TIA
The Joint Commission guidelines for Comprehensive Stroke Designated Centers as identified from the Joint Commission, American Heart Association, & American Stroke Association; identified need from patient and family expert opinion.
Improved understanding of personal risk factors
Patients, as well as family members opinions affected by the diagnosis of CVA
Patient and family verbalized lack of understanding; staff recognition of improved educational materials and classes to better prepare for a more focused to chronic disease education.
Compliance with National Guidelines for Organizations Designated Comprehensive Stroke Centers
Certification for Excellence in stroke education and treatments.
The Joint Commission Guidelines; The American Heart Association; The American Stroke Association; Get with the Guidelines
Patient Satisfaction with quality and service of measures.
Analytical measurements of patient sensitive measures via patient satisfaction surveys.
Organizational patient survey report; quality department

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 41
External Evidence
A comprehensive literature review was conducted to evaluate the importance and
necessity for improved discharge education with attention to individuals suffering from a stroke.
As described throughout this paper, the evidence was consistently repeated. A common theme
throughout the comprehensive literature review revealed nurses associated a lack of
empowerment to their inability to provide appropriate and detailed education to patients. First,
providing nurses with the resources, tools, education, and skills fostering a culture of
empowerment is positively associated with organizational respect and nurse satisfaction.
Second, as change occurs rapidly, accessibility to essential resources and additional educational
materials specific to the specialty unit they are working, are vital to the personal and professional
success of the nurse (Blauer, Frei, Schnepp, & Spirig, 2015). Third, enhancing the nurses’
knowledge base empowers their ability to educate patients, elevating their ability to effectively
communicate. Providing individual patient education is only one-way nurses can provide
education. Group settings allow for patients and their families to participate in group
discussions. This form of education has the ability to enhance the patient’s coping mechanisms
and their understanding of their disease process (Håkanson, et. al., 2011). This is especially vital
for individuals suffering from the life-altering diagnosis of a stroke. There is life after stroke,
and initially this devastating diagnosis can intimidate the healing process and coping skills
necessary to participate in progressive and preventative treatments. However, during group
therapies, education, and discussion patients can converse with others affected by the same
diagnosis, and, in turn, create a supportive, safe environment assisting their healing and learning
processes. This type of environment also aids patients and family members with information for
therapies, coping skills, regimens for medication or exercise, etc. that have personally helped

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 42
themselves or others during this time.
This comprehensive literature review also revealed patient dissatisfaction with the
education and materials provided at discharge stating “the information provided was inadequate,
too complicated, and difficult to understand” (Choi-Kwon, et. al., 2005, p. 86). First, a
diagnosis, such as a stroke, is shocking to the patient and their family promoting extreme
anxiety, fear, and inability to retain provided education and information. Therefore, addressing
education must be done gently with finesse. Second, education must be repetitive to be receptive
and retained. Third, education must be provided in an atmosphere conducive to learning, and at
their health literacy level. Providing front line nursing staff, and multidisciplinary team
members, the accessibility to resources enabling their ability to provide sufficient and
exceptional education to patients and their family members fosters a positive, safe, and satisfying
atmosphere.
Internal evidence supported the recurring themes noted during the external literature
review. Nurses revealed their dissatisfaction with their accessibility to sufficient educational
resources to provide patients and their families. Time constraints were also a recurrent
verbalized dissatisfier for the front line multidisciplinary team members, as they are
overwhelmed with their task duties limiting their available time at the bedside. Further internal
evidence revealed a disruptive educational experience affecting patients and their family
members. Patient satisfaction surveys divulged an expressed dissatisfaction with their level of
comfort in providing home care once discharged directly related to their lack of education during
hospitalization. Given the organization has recently received Comprehensive Stroke designation,
refining the discharge educational process is vital to the organization’s ability to not only meet
the initial 8 stroke core measures (STK) for a primary stroke center; however, the additional 8

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 43
comprehensive stroke core measures (CSTK) as mandated by the Joint Commission (American
Heart Association, 2015). These additional 8 stroke core measures elevate the performance of
the organization illuminating the organization’s ability to provide extensive, yet exceptional care
to individuals suffering from a complex stroke diagnosis at any time. Serving as a guideline for
provisionary care for individuals suffering from the potential life-altering diagnosis of a stroke,
the additional set of 8 CSTK measures were “developed for the management of both ischemic
and hemorrhagic stroke patients in hospitals equipped with the clinical expertise, infrastructure,
and specialized neuro interventional and imaging services needed to provide the next level of
stroke care” (The Joint Commission, 2017). In essence, the 16 CSTK provide a foundational
guideline to the exceptional care provisions necessary to implement and enhance the care and
outcomes for individuals suffering from a stroke diagnosis utilizing organizational clinical
expertise and exclusive neuro interventional techniques.
Receiving the prestigious nationally recognized certification for elite status in providing
exceptional care for the most complex stroke patients is no easy feat. Therefore, on an
organizational level maintaining this elite nationally recognized certification is vital to the
organization’s success. Stroke education provided to patients and their family members is
crucial to their ability to enhance their own health wellness through essential therapies,
medication regimens, and ability to prevent recurrence. The hospital is experiencing a decrease
in satisfaction from both patients and family members, as well as nurses expressing their
unhappiness with their ability to sufficiently educate. The organization, although lower than the
national standard for preventable readmission within 30 days (Litchman, Leifheit-Limson, Jones,
Wang, & Goldstein, 2013), is also experiencing an increase in readmissions for recurrence of
stroke signs and symptoms directly relating to expressed lack of education and understanding of

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 44
their personal risk factors and disease process. Enhancing the discharge process for patients
suffering from a stroke is vital to elevate nursing and patient satisfaction scores. Therefore,
implementing a weekly stroke support and educational class for suffering patients and their
family members will decrease the potential financial impact the organization could experience by
maintaining current certification, retaining current nursing staff, and increasing patient and nurse
satisfaction.
Implementing process improvements is organizational development. However, this is not
always an easily implemented task. Although, addressing multiple avenues to enhance the
discharge process for stroke patients have been attempted, both the internal and external data
collection prove an imperative need to implement a more structured form to deliver vital patient
education and ensure patient or family understanding. The following section will detail project
recommendations developed from the internal and external data collection.
Project Recommendations
Through an expressed desire and need to enhance and refine educational opportunities
provided to patients diagnosed with an ischemic or hemorrhagic CVA, or TIA the University of
Mary’s Stroke Project team identified formalized structured classroom setting to be a principal
recommendation. A recent designation to hold the title Comprehensive Stroke Center, Research
Medical Center, along with all other Comprehensive Stroke Centers, have made the
“commitment to treat stroke patients effectively and efficiently with the goal of improving care
and outcomes” (The Joint Commission, 2014, para 2). Accomplishing comprehensive stroke
designation requires hours of dedication to ensure the organization’s stroke program is equipped
with the skills, tools, and educational materials necessary to provide care to individuals suffering
from the most complex stroke diagnosis at any time. Therefore, along with all other

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 45
organizations holding this certification, establishing a culture of enhanced quality and safety
warranting a specialized personal focus to all individuals suffering from a stroke as directed
through their guidelines meeting all specialized criteria, provide the organization foundational
basis to remain an elite designated Certified Comprehensive Stroke Center. This University of
Mary’s Stroke Project team has experienced complete support from all interdisciplinary team
members and executive leadership to initiate and implement a structured formalized educational
weekly classroom teaching.
Organizational frontline nursing staff members, for specialized stroke units, had
expressed a lack of knowledge in providing educational materials personalized to the patient and
their specific risk factors. Individuals suffering from a stroke diagnosis, also affecting their
family members, had verbalized a desire to have a more personalized approach to their health
wellness plan of care. A desire to understand their specific risk factors and ways to implement
positive healthier choices was a verbalized top priority for patients and their families. The
requests verbalized from organizational members and patients identified with a diagnosis of
CVA have influenced the University of Mary’s Stroke Project team to divulge this information to
the executive leadership team, enlisting their assistance and advice for opportunities to enhance
educational opportunities offered to both staff members and patients.
Educating Front-Line Nursing Staff. Through the review of literature there was a
significant amount of support to provide detailed education for front-line nursing staff (Blauer,
Frei, Schnepp, & Spirig, 2015). The proposed recommendation was to review the stroke booklet,
that all stroke patients receive, in detail with front line staff with a member of the University of
Mary’s Stroke Project team, the Stroke Program Coordinator, the Stroke educators, or the Stroke
Registered Nurse Navigators. This time allowed nurses the ability to ask questions that may

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 46
have arose and also provided a detailed explanation of the education and why it is important for
nursing staff to have thorough knowledge in this area. This education has also been incorporated
in orientation for all new staff members starting on the stroke units at Research Medical Center
to ensure they have detailed knowledge and understanding of stroke patient education.
The second part of the nursing education that the University of Mary’s Stroke Project
team is proposed is education related to the teach-back method. This teaching method allows
the patient to explain, in their words, the education that was just provided. This teaching method
allows the nurse to assess the comprehension and health literacy levels of the patient and re-
explain or reiterate areas the patient may not have understood (Sherman, 2015).
Structured formal weekly patient and family education. The recommendation for this
project to incorporate a structured formal weekly education dedicated to providing stroke
education to patients and their families has provided a foundation that has enhanced their overall
knowledge level. This dedicated avenue of personalized information has enable their ability to
make a more informed decision regarding personalized healthier lifestyle choices and
compliance with their current health wellness plan. Evidence identifies and supports the need for
established education for patients, a personalized approach to health wellness plans, improved
educational opportunities for specially trained stroke nurses, and an interdisciplinary team
approach for stroke victims and their families. After all, excellence in provided stroke care is
comprehensive and team based.
Throughout this literature review, evidence has proven that an enhanced avenue
providing specific education dedicated to stroke patients is imperative to their ability to make
informed health wellness decisions. Incorporating their family members into the teaching and
education provides an opportunity for enhanced retention and learning. Guided from the Joint

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 47
Commission, the American Heart Association, the American Stroke Association, and the Brain
Attack Coalition measures have been implemented for all Comprehensive Stroke Centers as a
roadmap to enhance the effectiveness, quality, and efficacy of stroke treatments. In addition to
those measures, a structured formal weekly educational opportunity has enhanced the patient’s
ability to recognize specific signs and symptoms, verbalize their personal risk factors, enhance
their overall health status through the implementation of interventional methods and
recommendations, and help create their personalized plan of care.
Project Implementation Plan
Change Theory
Change, while inevitable, is a process that must be handled with finesse and strategic
implementation to achieve the desired long-term goals of the organization. The concept of
change theory intimately relates to project implementation plans providing a road map necessary
for successful integration of obligatory changes. For this project, a comprehensive
understanding of change theory was imperative to ensure successful project implementation.
The John Hopkins Nursing Evidence-Based Practice (JHNEBP) model is a powerful tool
assisting health-care professionals in clinical decision making (The Johns Hopkins Hospital/The
Johns Hopkins University, n.d.). This model was chosen due to its simplicity and easy to follow
three step process empowering bedside nurses to safely and quickly implement processes
enhancing patient care while providing the most current evidence-based practices. Utilizing their
three-step process more commonly known as PET (practice question, evidence, and translation)
(The Johns Hopkins Hospital/The Johns Hopkins University, n.d.) the JHNEBP model helps
“bedside nurses translate evidence to clinical, administrative, and educational nursing practice”

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 48
(Melnyk & Fineout-Overholt, 2015, p. 302).
The first step of this three-step process is the collaboration from organizational team
members to identify a process or question needing further investigation. The organizational team
members describe and refine the practice in question in order to define the scope for the process
or question identifying key stakeholders (The Johns Hopkins Hospital/The Johns Hopkins
University, n.d.). Through this initial step the project leader(s) are identified and a timeline for
project implementation is developed, along with a scheduled meeting plan.
The second step entails the collection of data, both external and internal proving the need
for an improved or newly implemented process. Many factors have the ability to affect the
collection, evaluation, and integration of best evidence practices; therefore, proving to be the
most crucial step in this process, the collection of data is an integral key component to the
identification, integration, and implementation of the highest quality evidence into daily
practices enhancing patient care (Figure 1). Throughout this step, the evidence is evaluated,
depicted, and appraised detailing the strength and quality ensuring the most updated strong
evidence is utilized for process improvement. In this model, the pyramid of three steps have also
identified external and internal factors potentially affecting the implementation and integration of
process improvement (The Johns Hopkins Hospital/The John Hopkins University, n.d.).
Permission was granted to use The Johns Hopkins Nursing Evidence-Based Practice Model and
tools (Appendix A).

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 49
Figure 1. The Johns Hopkins Nursing Evidence-Based Practice Model
©The Johns Hopkins Hospital/The Johns Hopkins University.
The third and final step of this model involves translation and an organizational action
plan for implementation (Brooks-Staub, 2005). In order to translate the need for enhanced
process improvement, an organizational support system consisting of executive and primary
direct leadership team members, as well as supportive multidisciplinary team members must be
present. Ensuring the appropriate and correct interdisciplinary team members dedicated to the
refinement of the educational materials offered to stroke patients and frontline nursing staff,
consist of the Stroke Program Coordinator, Stroke Registered Nurse Navigators, direct
leadership members for the stroke units, and multidisciplinary team members to be present
empowering the change process paving the way for organizational success. Another important
aspect for this final step is to ensure the necessary resources are gathered and available. This
will ensure the action plan can be implemented according to the project designated time line.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 50
One of the most imperative elements is project outcome measurement. This key step evaluates
the implemented project allowing for an in-depth examination of the process and allows for
restructuring, if desired, to improve or alter the projects process. The project findings are then
reported to the key stakeholders allowing for further determination if the improved or newly
initiated process provided will promote the best evidence-based practices enhancing provided
services and cares to patients.
Key stakeholders
Achieving excellence in the culture leads to excellence in service, and excellence in
service saves lives. Recently, achieving Comprehensive Stroke Designation, along with multiple
American Heart Association and American Stroke Association awards, Research Medical Center
is dedicated to augment upon the education stroke patients receive. Their mission is “above all
else we are dedicated to the care and improvement of human life” (Research Medical Center,
2017). This organization developed the stroke program devoted to maintaining and enhancing
stroke survivor’s health and wellness. Education is the key strategic element. Knowledge begets
power, and one who holds the knowledge holds the power to achieve greatness.
A multitude of essential stakeholders have been identified through this project. The
program coordinator, Sherry Bahr APRN, CNRN, remains a key stakeholder in this project. Her
support, dedication, and excitement uphold the organization’s mission and value statements;
therefore, her support brings top level organizational support. Sherry’s ability to determine the
needs of the organization provides a foundational guideline and direction for patients and staff
members. Her advanced knowledge and education for stroke patients help guide strategic
interventional methods dedicated to enhancing the education and care patients and family
members receive.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 51
The support of Nisha Mills, MBA, Director of Neurophysiology, is crucial for her
guidance and support for funding and budget implementation. The Assistant Chief Nursing
Officer (ACNO) and Chief Nursing Officer (CNO) are imperative team members as they guide
and promote changes within the nursing practice. The Chief Executive Officer (CEO) also plays
a vital role in the promotion and advancement of the stroke program. Her top-level support and
dedication to the enhancement of the Stroke Program is essential for the implementation loyal to
the stroke population within the organization and community. The front-line staff members are
an absolute essential aspect as they promote the education, answer questions, and guide patients
and family members to the Stroke team for further education. Nursing staff providing daily
bedside care also help ensure patients receive essential therapies, medications, and treatments
necessary to maintain, enhance, and progress upon their health wellness. The certified nursing
aides (CNA’s), essential front-line staff members, are another important stakeholder as they will
be helping transport patients to the proposed weekly education.
The Neurologists are a vital key stakeholder as they guide the treatment for individuals
suffering from a stroke to ensure timely administration of life saving medications, procedures,
and testing are in correlation with The Joint Commission and Centers for Medicaid and Medicare
(CMS) guidelines. The team of neurologists ensure that the most current evidence-based
practices are promoted within the organization remaining on the cutting edge of treatment
therapies for the stroke population. They promote educational opportunities for organizational
members ensuring everyone has the ability to remain informed; while also guiding educational
information provided to patients and their family members.
The Director of Research Medical Center’s quality department provides necessary matrix
and data information regarding the stroke patients. Along with her, the quality department is

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 52
vital to the overall success and stability of the program by ensuring all essential and vital
concepts are provided the attention to detail necessary for overall program success. Their
department also provide assistance with chart audits and nursing quality compliance. This data
will help support whether the interventions that were implemented were effective in improving
patient understanding of their diagnosis and expected outcomes.
Physical, occupational, and speech therapies ensure a personalized comprehensive
evaluation is completed and their recommendations guide treatments dedicated to the safety of
the patient. Their therapy programs are imperative to build patient strength and mobility
enhancing their quality of life. These therapies also provide education to the patient and their
family regarding any new physical deficits and how to work with or overcome the loss of these
essential functions.
The educators for units housing acutely ill patients suffering from a stroke are vital to the
success of this project. They will help deliver pertinent educational information to nursing staff,
as well as ensuring a comprehensive understanding of essential tasks to be completed. These
educators will also provide one-on-one assistance for any staff member needing guidance in
performing the National Institute of Health Stroke Scale (NIHSS), or ensuring care plans are
completed properly and discharge information is completed and documented meeting the
standards guided by The Joint Commission and Centers for Medicaid and Medicare accordingly.
Patients and their families will remain the key stakeholders in this project. Ensuring they
possess a comprehensive understanding specific to their stroke, their risk factors, and their plan
of care post discharge is the ultimate goal. The patient and/or their family members play a vital
role in their personalized post-discharge treatment and care plan. A strategic planning process
along with interventional methods specific to the patient and their lifestyle is imperative to their

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 53
overall success. A complete comprehensive understanding and ability to verbally teach back
specific risk factors and how to implement lifestyle changes is crucial to a patient’s compliance.
Encouraging family participation with education, therapies, medication regimens, post discharge
planning, and support groups, etc. is essential for the patient to implement the changes and
remain dedicated to the change in order to enhance their health and wellness.
Barriers and Facilitators/ Drivers and Resistors to Change
Barriers are directly related to the internal and external factors associated with The Johns
Hopkins Hospital/The Johns Hopkins University change theory model. A multitude of barriers
exist when implementing changes in process, policies, or any aspect of life. Change, while
innately inevitable, produces a fear within individuals constructing an invisible barrier.
Therefore, understanding the factors which foster an environment that is acceptable and
conducive to change is indispensable. Inadvertently, examined traditional barriers are often
directly the source for an undesired effect for change implementation.
Barriers to change related to this project, are illuminated through The Johns Hopkins
Hospital/Johns Hopkins University change model noted by internal and external barriers (The
Johns Hopkins University/John Hopkins University, n.d.). Internal barriers for front-line staff
members include a decreased confidence in providing education to patients regarding specific
disease processes. Potential additional barriers include the nurse’s inability to appropriately
evaluate the level of understanding for the patient and their families, and an inability to locate
appropriate written educational materials dedicated to the patient’s level of understanding.
These were expressed by verbal opinion during weekly rounds for tenured employees and during
orientation classes for newly hired employees. Consistent verbal agreement was noted during a
monthly leadership meeting, as well as during administrative and stakeholder meetings for this

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 54
project.
Barriers represented through patient expression remain explicitly important, as they are
the key stakeholder for this project. Fear of the unknown and the unexpected riddle patients who
have been diagnosed with this life-altering disease process, while also affecting their family
members’ lives. An assortment of barriers are present from the beginning including the initial
mind blowing detrimental diagnosis of a CVA to the degree of resulting deficits. Patient
determination and current overall health wellness are vital barriers potentially affecting their
ability to remain compliant with their personalized plan of care post discharge.
Barriers identified during internal investigation illuminate aspects impeding successful
implementation. Organizational cultural acceptance, fear of the unknown, and potential loss or
failure are fundamental aspects needing pertinent attention. For this project, one extremely
imperative organizational barrier includes acceptance from a multitude of physician teams who
play an important part of the patient’s personalized health wellness plan of care. These teams
include Neurology, Neurosurgery, Pharmacy, Hospitalists, Internal Medicine Residents, Family
Practice Physicians, and teams of Nurse Practitioners. Constructing a timeline conducive for all
team members, including patients and their family members is essential to achieving attendance.
Acquiring a meeting room sized to incorporate an estimated group of individuals is imperative to
produce a comfortable learning environment. The resolution of said barriers has been an aspect
with direct attention from the initiation of the project. This group enlisted the aid of Sherry
Bahr, APRN, CNRN, Stroke Program Coordinator as an influential leader and mentor. The
mentorship and aid she has provided throughout the beginning phases of this project have been
exceptional. An additional behind the scenes influential leader and mentor has been the interim
Director for the acute inpatient Oncology Unit, Deborah Wooten, RN, BSN, MBA-HA. The

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 55
help she has provided to the team has been educational and exceptional. These two mentors
have been exemplary facilitators in assisting the forward movement of the team. Additionally,
many organizational leaders, including the CEO, CNO, ACNO, Director of Medical Services,
the Neurology team, Rehabilitation therapy member's, primary unit educators, and the Director’s
for the primary care units providing essential care for stroke patients have become an
indispensable asset to this project.
Reducing the resistance met from internal and external factors is crucial for organizations
as they implement change process. For this project, the driving forces of external factors include
standards to maintain Comprehensive Stroke designation from The Joint Commission. This
organization must continually evaluate opportunities for improvement and excellence when
providing stroke education to patients and family members. Additional external factors
associated with this project include utilization of current resources as a measure to reduce out-of-
pocket costs, maintain a standard of excellence in quality, and improve the facilitation of quality
metrics, core measures, and fundamental standards from front-line staff members. Improving
their ability to include the vital information delineated for quality metrics remains imperative to
not only meeting standardized guidelines, but surpassing them striving for excellence. The
Stroke team with a combined effort from the leadership team and essential interdisciplinary team
members continue to reduce and eliminate both internal and external barriers influencing the
enhancement of imperative educational opportunities for this patient population and their family
members.
Business Impact
By improving the quality of patient care through an enhanced educational program that
increases the patient's understanding regarding their individual stroke and stroke care, Research

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 56
Medical Center will help to improve patient outcomes and enhance patient satisfaction; which, in
turn, can improve the financial successes of the facility. Enhancing the quality of care provided
to the patients through an improved educational understanding can reduce hospital readmissions
and unreimbursed costs, and improve patient outcomes by providing the organization with return
customers and increased funding. By the organization linking funding and expenditure, closely
following the American Heart Association and The Joint Commission guidelines, to the quality
of the care provided, this helps in improving financial gains along with patient satisfaction.
With increased patient satisfaction scores, the organization could utilize internal and
external marketing to increase the community awareness of the advances in education that have
led to increased patient satisfaction. An institution that increases the satisfaction of its patients,
will increase the number of referrals through a word-of-mouth reputation. “Research has shown
that good service quality leads to the retention of existing customers and the attraction of new
ones, reduced costs, an enhanced corporate image, positive word-of-mouth recommendation,
and, ultimately, enhanced profitability” (Alrubaiee & Alkaa’ida, 2011, p.103). This
organization's willingness to focus on enhancing the quality of educational understanding with
their stroke patients will help the organization increase their patient satisfaction scores, moreover
enhancing the business impact through the implementation of this project.
Organization Planning Process
The implementation plan of this project upholds the standards set by the mission, vision,
and values of Research Medical Center. Research Medical Center’s mission is “above all else,
we are committed to the care and improvement of human life” (Research Medical Center, 2017).
The goal of this project is to reduce the morbidity and mortality of patients suffering from a
stroke diagnosis by better preparing nurses to meet the needs of patients and also enhance the

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 57
knowledge and understanding of the stroke disease process for patients that have recently
experienced a stroke. As Research Medical Center has continued to strive for excellence in their
ability to provide exceptional stroke care, they have received the prestigious honor of becoming
a Certified Comprehensive Stroke Center. By striving for excellence in stroke patient care,
guided by the specific guidelines dictated from the American Heart Association, the facility is
working towards their vision of the health system which is “together, we will be the premier
healthcare destination for all we serve” (Research Medical Center, 2017). This is accomplished
through integrity, compassion, respect, and excellence by all members of the multidisciplinary
team which are the values that help guide the care that is provided on a daily basis.
Implementation Plan
Guided by Research Medical Centers executive leadership team, the focus of the
University of Mary’s Stroke Project team was to focus on patient education in the stroke unit(s)
of Research Medical Center in Kansas City, Missouri which had recently achieved
Comprehensive Stroke Center Certification. The specified stroke unit is a 34-bed unit that
houses the less-critical patients suffering from a current stroke diagnosis. Research Medical
Center also has critical care units, the Intensive Care Unit (ICU) and Progressive Care Unit
(PCU), that provide care to the more critically ill patients suffering from a more extensive or
traumatic stroke, or have recently received thrombolytics. Therefore, having patients potentially
housed in multiple units, a direct need for specialized and specific disease education remained an
imperative concept. When creating the implementation plan, the University of Mary Stroke
Project team kept the PICO(T) question at the forefront guiding the discussion. The PICO(T)
question was designed to identify whether patients had enhanced knowledge of their stroke
diagnosis after receiving specialized disease specific education. The educational

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 58
recommendations to Research Medical Center has been presented in a group setting designed to
enhance the understanding of the stroke disease process. In order to make these educational
opportunities possible, the University of Mary’s Stroke Project team had earned the support of
key stakeholders within Research Medical Center.
Gaining support of key stakeholders. In order for the University of Mary’s Stroke
Project team to gain support, the project lead for the University of Mary’s Stroke Project team
openly communicated, built relationships with the front-line staff and the key stakeholders not
directly involved in the educational process. Utilizing transformational and servant leadership
skills, the project lead promoted these initiatives with passion, engagement, and strong
communication skills. The skills associated with these leadership styles assisted the project lead
in listening, empathizing, and supporting patients and nursing staff while also showing how the
importance of their actions today can shape future outcomes (Melnyk & Fineout-Overholt,
2015). These leadership styles have assisted the project lead to “develop teams, to better
collaborate, and to work cohesively” with all members of the multidisciplinary team (Roussel,
Thomas, & Harris, 2016, p. 101). Implementing these leadership styles has proved beneficial for
both the patients and team members involved in this process.
In collaboration with Sherry Bahr, APRN, CNRN, Stroke Program Coordinator, the
project lead worked diligently to gain the support of key stakeholders throughout the facility. A
main focus for meeting with the executive leadership team and key stakeholders was to promote
this phenomenal opportunity to refine the educational opportunities for patients suffering from a
stroke or presenting with signs and symptoms securing their support and expertise. The
meetings were successful as team members exuded excitement to implement a program where all
multidisciplinary team members will be educated the same way promoting a consistent

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 59
educational process for patients and their family members plagued with a stroke diagnosis. This
educational opportunity has been successful for enhancing patient education and understanding
in regards to stroke; therefore, additional opportunities for refined education for chronic diseases
would prove beneficial for the organization.
Educating Front-Line Nursing Staff. Research Medical Center has identified patient
education as an area of opportunity within the stroke program. In order to refine this process, the
Stroke Team Nurse Navigators, which is comprised of the project lead Jenni McRoy, RN, BSN,
Amy Goodson, RN, Sherri Bahr, APRN, CNRN, the team of Neurologists, and the unit stroke
educators, initiated the required weekly staff re-education of stroke patient education during the
second week of September. The second week of September was selected to help meet the needs
of Research Medical Center but also work in conjunction with the requirements of the academic
semester. Research Medical Center granted the request to require all nursing staff delivering
direct care to stroke patients to attend this education and have highly encouraged other members
of the multidisciplinary team to attend as well.
Seven days before the re-education of front-line staff, a flyer regarding the staff education
was passed through report to inform them of this elite educational opportunity (Appendix B).
The education did occur during morning and evening huddle times on each unit that house stroke
patients to ensure all front-line staff attending this education had the opportunity to attend.
During the staff education, the project lead, Sherri Bahr, APRN, CNRN, and stroke
educators have re-educated front-line staff on the stroke booklet that all patients receive at the
time of admission when diagnosed with a CVA or neurological deficits potentiating a stroke
workup. The teach-back method was used during the re-education process. By using this
teaching method, it allowed the project lead, Sherri Bahr, APRN, CNRN, and the stroke

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 60
educators to verify that the front-line staff understood the materials reviewed. The teach-back
method was also taught to members of the front-line staff so they were aware and able to use this
teaching method to improve patient knowledge and understanding of education. As time
allowed, the front-line nursing staff received the opportunity to practice using the teach-back
method on each other to improve confidence in their ability to provide specific disease
education. The project lead, Sherri Bahr, APRN, CNRN, and the stroke educators were available
to answer questions for front-line staff throughout the education and were able to answer
questions regarding the education materials.
The knowledge gained through reviewing the stroke booklet and the delivery method for
patient education was a change compared to RMC’s previous patient education process.
Previously, front-line staff were taught by other front-line staff during orientation. This resulted
in decreased staff and patient understanding as not all front-line staff are proficient at teaching
other members of the multidisciplinary team to deliver patient education or they lack the
understanding of the educational material to provide quality education. Providing this
opportunity and ensuring all new front-line staff attend this educational session in the future will
build a strong foundation and help create a more confident multidisciplinary team that will be
more adept to answer unpredictable patient questions. Additionally, executive leadership have
supported the need to incorporate this disease-specific education into the orientation for newly
hired licensed professionals on the stroke units. As support from the executive leadership team
is elevated, the chance for sustaining this beneficial education is guaranteed, especially due to the
positive outcomes from this refined educational opportunity.
Implementing a Stroke Support and Educational Class. Research Medical Center had
expressed interest to start an inpatient stroke support and educational class for patients that have

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 61
been diagnosed with a stroke or neurological deficit potentiating a stroke workup and evaluation.
Due to this, the University of Mary’s Stroke Project team worked in conjunction with Research
Medical Center’s Stroke team to design and implement a stroke support and educational class.
Patients and their families that are hospitalized at the time of the group visit will be highly
encouraged to attend by front-line staff members, and members of the multidisciplinary team.
All members of the multidisciplinary team, including all therapy groups, agreed to assist with
transporting patients to and from the stroke support and educational class. This class is held
weekly on Thursdays in the rehabilitation education and dining room on the rehab unit at 1500.
This class is led by the University of Mary’s Stroke Project team project lead and Research
Medical Center’s Stroke team.
As the stroke support and educational class began, a safe, secure environment free from
judgement, prejudice, and ridicule was established by Research Medical Center’s Stroke team
and the project lead for the University of Mary’s Stroke Project team allowed for patients and
their family members to freely express their personal experiences, opinions, and ask questions.
Once the environment was created, the project lead referred to the stroke booklet during a
PowerPoint presentation, which expanded on the written content provided to patients and family
members. The booklet addresses stroke risk factors, common side effects for stroke patients, and
also lifestyle changes that reduce the elevated risk of patients experiencing additional strokes in
the future. The stroke support and educational class was taught using the teach-back method and
encouraged patient and family participation in the visit. This allowed the organization’s Stroke
team to evaluate the effectiveness of the education. Questions that had been asked throughout
the stroke support and educational class were collected to ensure the information is incorporated
into future stroke support and educational classes.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 62
Another factor incorporated was having stroke survivors, that participate in the already
implemented outpatient stroke support group, attend the inpatient stroke support and educational
class. This allowed the stroke survivor to expand on their daily struggles sharing their
experience of living life after a stroke. The hope was that the patients and families would
develop a connection with the stroke survivor and find benefit in attending the inpatient class
which increased the likelihood of patients attending the monthly outpatient stroke support group
meeting. Patients did find value in this group session and RMC was able to see positive results
related to this education; therefore, the likelihood of sustaining this group education was high.
Implementing additional education for front-line staff and the stroke support and
educational class assisted Research Medical Center to meet some of the stroke core measures set
by the Joint Commission. These core measures have been established to help guide the care for
patients hospitalized for a stroke or neurological deficit potentiating a stroke workup. Two of the
core measures this EBP project has assisted Research Medical Center to reach included
education addressing risk factors for stroke along with education that addressed the warning
signs and symptoms of stroke (The Joint Commission, 2017). In these measures set forth by the
Joint Commission no specific benchmark has been established. The goal is to continue to see
growth and organizational improvement in these areas along with the rest of the core stroke
measures.
Financial Insight. A majority of this project is focused on education; therefore, the fiscal
impact to RMC is very minimal. Resources that will need to be included is cost for nursing staff
to attend, and the cost of the Stroke Teams Nurse Navigators and Sherri Bahr, APRN, CNRN, to
provide the education. Stroke booklets are already being produced in large quantities as they are
handed out to all patients diagnosed with a stroke. Patients are encouraged to bring their stroke

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 63
booklet, personalized with their specific information, to be reviewed during the stroke support
and education class. Additionally, the PowerPoint presentation slides, based off the stroke
booklet, are printed off and provided to each patient and family attending to provide for
additional space for note taking and questions. This particular handout also provides the patient
and/or family with a more in-depth disease specific education, while also proactively answering
questions and stating facts that might otherwise be overlooked.
Project Measurement Plan
Refining processes enhancing the care provided to patients is not only important;
however, vital to their morbidity and mortality. Discharge education is crucial to patient
preparation for home beyond the hospital. Empowering the patient with all necessary education
and materials promote an ability to make well educated, informed decisions regarding their
health wellness. Incorporating the baseline metrics revealed through the internal data review,
project measurements were identified utilizing the mnemonic acronym S.M.A.R.T (specific,
measurable, attainable, realistic, and time-limited). Researching, designing, and implementing
an organizational wide one-hour weekly education program providing essential stroke
information for patients, family members, and caregivers to better prepare them for life after a
stroke has been implemented within Research Medical Center. This weekly class supports
Research Medical Center’s mission, vision, and values statements of “above all else we are
committed to the care and improvement of human life” (RMC, 2017). Research Medical
Center’s vision “together, we will be the premier healthcare destination for all we serve” was
illuminated through increased education provided to the stroke population (RMC, 2017).
Measuring the Efficacy of the Stroke Support and Educational Class. A pre-
education and post-education formative questionnaire (Appendix C & Appendix D) was

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 64
completed which evaluated the level of understanding for patients, families, and caregivers
regarding patient personal risk factors, signs and symptoms of stroke, and types of strokes for
patients and family members who attended the weekly structured formalized educational class.
In doing so, RMC’s Stroke RN Navigators evaluated the effectiveness and efficacy of education
provided during the stroke support and educational class. These surveys were completed at the
beginning and end of each stroke support and educational class. The pre-educational survey and
post-educational formative questionnaire were collected at the end of each weekly class and
evaluated by the Stroke team. The data results were reported to the Stroke Program Coordinator
for an intricate overview for necessary changes and potential restructuring of the education
provided during the weekly sessions. Research Medical Center’s Stroke team was solely
responsible for the collection of data. For the purpose of the academic semester, the data from
these surveys was gathered for ten weeks.
The weekly structured and formalized stroke support and education class was held in the
rehabilitation unit on Thursdays at 1500. This set time accommodated the patient’s daily
therapies, treatments, and medication regimens while positively accommodating the Stroke
Program Coordinator’s schedule, the Stroke RN Navigator’s schedule, and the rehabilitation
unit’s free time. The rehabilitation unit’s dining room houses approximately 35 individuals
which allowed for sufficient room for the estimated amount of 5-25 individuals weekly. Flyers
were posted promoting the weekly class to all staff members, providers, family members, and
patients (Appendix E). Physician providers were educated during their monthly meetings with
the Medical Director, as well as through the hospital organization email system. Incorporating
Social Workers and Case Managers assistance, support, and guidance through the discharge
process for patients and families suffering from a stroke is imperative to their recovery process.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 65
As described in an earlier section, the University of Mary’s Stroke Project team gained the
unconditional support of Research Medical Center’s executive and nursing leadership team
members.
This class has helped provide relevant, realistic, and essential stroke education for
patients suffering from a stroke diagnosis with personalized information guided by their specific
diagnosis. This class has enhanced Research Medical Center’s culture of service commitment,
through a refined educational opportunity for stroke patients. Providing essential information
necessary to reduce the morbidity and mortality enhancing the health wellness of the stroke
population. The goal for this class was to ensure that patients, families, and caregivers have a
comprehensive understanding of their specific type of stroke, personal risk factors, and how to
implement healthier lifestyles.
The time frame suitable for implementation of this structured class was the second week
of September 2017. This allowed for the educational materials to be built and perfected before
initiation. This date also allowed for a sufficient amount of time to ensure all staff members,
including the primary physicians managing care for the stroke patient, were educated regarding
this educational opportunity. Flyers were prepared for promotion of this newly structured
formalized stroke support and education class that were strategically placed within waiting
rooms and acute inpatient units so that family members and patients can read them during their
visits (Appendix E). Building upon this designated time frame provided the Stroke Program
Coordinator the ability to promote this educational opportunity to members of the Stroke Support
Group so they had the opportunity to attend not only the ribbon cutting open house; however, to
also attend the first class which helped to provide a safe, supportive environment for newly
diagnosed stroke patients and their family members.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 66
Measuring the Efficacy of Front-Line Nursing Staff Education. The education that
was provided to nursing staff and other members of the multidisciplinary team was vital to the
success of this EBP intervention. The method that was selected to measure the efficacy of this
training was through a routine post education survey (Appendix F). The questions in this survey
are open ended to encourage members of the team to provide feedback, whether it is positive or
it identifies an area of opportunity. This feedback allowed the group to evaluate the success of
the education and the method of teaching. With this feedback, the University of Mary’s Stroke
Project team and Research Medical Centers Stroke Program team were able to make changes
based on the feedback from the multidisciplinary team to refine the education and make it more
effective for the team.
Measuring the Efficacy of Patient Education. Through routine post-discharge calls, the
effectiveness and efficacy of the education provided to the patient and family members during
this weekly stroke support and educational class has been evaluated. Research Medical Centers
Stroke team have developed a post-call evaluation and satisfaction tool utilized during an already
implemented process of routine discharge calls. An additional metric measurement has included
the addition of supplementary questions on the previously mailed out post-hospitalization patient
satisfaction surveys. These added questions do include specific information regarding the
patient’s hospitalization and the reason for admission, i.e. stroke. If they mark yes, they are
prompted to answer an extra three to five questions illuminating their satisfaction on provided
care, treatments, and education.
Human Subject Protection Statement
The purpose for this EBP project presented by the University of Mary’s Stroke Project
Team was to refine the education provided to patients, during hospitalization, suffering from a

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 67
CVA. The University of Mary’s Stroke Project Team had the opportunity to work in
collaboration with RMC leaders to implement EBP interventions such as a formal, organized,
and structured stroke support and educational class, as well as nurse led teach-back patient
education. By understanding risk factors, disease process, and alternative implementation
methods, it is hoped that patients incorporate preventative techniques into their lifestyle to reduce
their likelihood of experiencing additional CVAs in their lifetime.
When implementing an EBP project, the individuals involved in the implementation
process can become highly involved in the presentation and outcomes. This can make it difficult
for members of the team to remain objective which could compromise the rights and care of the
patient inadvertently (Polit & Beck, 2012). In order to protect patient rights during these times,
many organizations have created an Institutional Review Board (IRB).
“The duty of the IRB is to ensure that the proposed plans meet federal requirements for
ethical research” (Polit & Beck, 2012, p. 166). The IRB process has a purpose of ensuring that in
fact an EBP project has a purpose for involving human participants in their data collection;
effectively ensuring that the project will gain some form of scientific data that is deemed
valuable. The IRB approval method essentially lets the writers know if they have violated any
rights, regulations, or laws in the process of initiating this research paper or evidence-based
project. Protection of the patients is the ultimate goal of the IRB approval process.
In order to protect the rights of the participants during the implementation phase of this
project, an IRB application was submitted and approved through the University of Mary’s IRB
approval process (Appendix G). Research Medical Center did not require this project to submit
an application to the facilities IRB since this is an EBP project. Ultimately, the University of
Mary’s IRB approval helped to detect any unintentional circumstances that may have been

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 68
missed in regards to the protection of the patients.
Implementation and Measurement
Implementation
During the second week of September Research Medical Center’s stroke team initiated
the nurse education regarding the teach-back method for all units housing patients suffering from
a Stroke diagnosis or neurological deficit potentiating a stroke workup. Over the next week, the
Stroke RN navigators along with the Stroke educators and Stroke program coordinator, attended
morning and evening huddles to provide intimate education for the nurse performing the teach
back method. Additionally, nurses were evaluated during their performance utilizing this key
tool with the patient and family members. Constructive feedback was performed after each
evaluation providing nurses an ability to ask questions to enhance their ability to provide explicit
education and resources personalized for the patient’s specific situation. During this time, the
Medical Director for the Neurosciences department educated the primary care teams providing
comprehensive care for the acute hospitalized patients with a stroke diagnosis or stroke workup.
This education was provided through email, direct conversation, and daily and monthly
conference meetings.
After the nurse education had been provided, the implementation of the stroke support
and education class began. A PowerPoint presentation was designed and developed to present
specific information regarding what a stroke is, the different types of strokes, implementation
measures, risk factors that can and cannot be modified, and what to expect after a stroke
physically, emotionally, and mentally. Additionally, our expert Clinical Rehab Specialist
attended the weekly class to provide information on the different types of rehabilitation available

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 69
post the acute diagnosis. Upon arrival to the class, patients and family members attending were
asked to complete a pre-survey in order to gain insight on their knowledge prior of strokes
(Appendix C). Once this is completed, the PowerPoint presentation begins. Patient’s and family
members are encouraged to ask questions or present self-stories during any part of the
presentation. After the presentation was given, all questions are answered, and stories were
shared, the post-education informative questionnaire was given evaluating the effectiveness of
the class and education provided. Additionally, an area for comments regarding their thoughts of
the class, the education provided, and what can be done to better improve the class was provided.
Responses help restructure and reformat the education provided to ensure a comprehensive
approach was provided for this disease specific stroke information.
Initially, the Stroke RN navigators were ensuring that all patients, charge nurses, and
primary nurses were rounded on each Thursday as an additional measure to promote class
attendance. As this promoted compliance and attendance, it soon proved difficult to get to all the
primary nurses on the day of the class due to increased census and different obligations, and as
such, attendance began to suffer. Alternative methods to promote attendance and compliance for
this crucial information provided in the weekly offered stroke support and education class were
discussed and implemented. These included announcing every Thursday at the morning bed
huddle meeting which charge nurses, managers, and directors attend that the class was being held
that day with the time and location, along with an overhead page from the operators one hour
prior to the class start time. Additionally, a professional and educational email was sent to all
managers, directors, and leadership executives stressing the importance of this class as a part of
the patient’s treatment plan to highlight our recent Comprehensive Stroke designation. The class
following these alternative implementation methods drastically improved for patient, family

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 70
member, and staff attendance. As such, these additional measures have become a permanent
addition to the promotion and success for this class.
Initially, the educating for new hires and orientees was to be completed during their
orientation period on their designated unit. However, once this was discussed and thought about
it became evident there was a better way to ensure all new hires are educated with this vital
information. Therefore, an additional measure the Stroke team has incorporated includes
attending bi-weekly orientation groups and educating the new hires on the importance of
utilizing the teach-back method when providing disease specific education. During this time,
education for the newly implemented stroke support and education class is provided stressing the
importance for attendance as part of the patient’s treatment plan diagnosed with stroke or stroke
workup. Moreso, this opportunity allowed for direct questions from newly onboarded staff
members.
Measurement
Prior to the implementation of this class, there was not a measurable method in place to
evaluate patient satisfaction for provided education. However, it was estimated, from routine
post-discharge calls and patient and family rounding, that approximately 90% were dissatisfied
with the disease specific education received. In fact, their dissatisfaction ranked so high, it
potentiated a comprehensive dissatisfaction for their entire stay. The patient's verbalized phrases
such as “I was not prepared to care for myself when I got home” and “I had so many questions
and was scared to even come home”. When asked about their ability to re-state the meaning for
the acronym F.A.S.T. they were not able to; therefore, additional education was provided over
the phone to ensure a basic understanding. Therefore, in order to keep track of attendance and
results from the pre and post-education questionnaires, an excel spreadsheet was created and

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 71
specifically designed to house the information collected weekly.
Initially, the first week of attendance brought two patients and three family members.
This correlated with the patient’s ability to attend and sit through the hour-long class and family
member presence during hospitalization. Table 8 below presents realistic attendance the
subsequent weeks:
Table 8: Attendance vs Stroke Census for weeks 1-10
During the initial meet and greet for each class, patients, family members, and caregivers were
asked to complete a pre-survey questionnaire to evaluate their understanding of strokes, risk
factors, and signs and symptoms. They were all encouraged to answer each of the six questions
to the best of their ability, as there is no right or wrong answer. Once this was completed, the
questionnaires were gathered and placed in a folder to be evaluated after the class. At this time,
the PowerPoint presentation began, during which it was paused for questions and concerns.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 72
After the presentation, a post class questionnaire was completed asking the same initial six
questions along with asking for an explanation of what benefits they received from this intimate
disease specific education, as well as what can be improved on the class. Table 9 below
represents the statistical graph proving that this formalized and structured classroom experience
provided an intimate atmosphere for further understanding regarding stroke disease specifics;
while enhancing the patient, family, and caregiver’s ability to make a more informed decision
regarding their post-discharge care.
Table 9: Pre and Post survey questionnaire results
Additionally, patients have expressed gratitude, a deeper and enhanced knowledge base, a sense
of community, and excitement for the educational materials and insight provided through written
comments and verbal conversations.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 73
During the week prior to the implementation of the class, nurse, staff, and physician
education was implemented and successful. Physician education was done through the
organizational email system, one-on-one conversations, and daily and weekly physician
conferences. Although, there have been some minor slip-up’s, the education has proved
beneficial overall. Both physician admission and discharge orders are being completed to reflect
a stroke admission workup or a stroke discharge. As each patient admitted for a neurological
deficit or stroke workup is followed by RMC’s Stroke team until either ruled out with the
definitive MRI or physician documentation stating the patient no longer requires a stroke
workup, necessary continued education was provided when a potential fall-out has been noticed
during chart audits. This allowed for real-time education and reflection, while also revising the
inconsistent documentation. In fact, physicians were much more aware of successful
documentation than ever before, and have reached out to our Stroke Program Coordinator,
Sherry Bahr, APRN, CNRN, as well as, both the Stroke RN Navigators for assistance and
clarification. This allowed for an enhanced collaborative working environment.
The nurse education was extremely successful. After review of the nurse education
survey, it was noted that 100% of nurses felt the education provided regarding the nurse-patient
teach-back method and tool was an imperative aspect to evaluate patient and family member
understanding of the provided education. Moreso, it allowed for nurses and therapeutic
disciplines to devise alternative methods for educational opportunities based off patient and
family needs. In essence, the teach-back education tool provided verbalized opportunities to
format a more personalized plan of care, disease specific education, and post-discharge teaching
catered to expressed patient needs and desires. This specifically has created an atmosphere
where nurses “feel” they are helping the patient. Additionally, the nurses have expressed

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 74
feelings of empowerment and self-confidence through the use of and education for the nurse-
patient teach-back tool. One of the comments by a bedside stroke nurse was the fact they now
have a face-to-face method to evaluate patient understanding, and; therefore, can provide
additional education, contact the physician or other disciplines for assistance in providing the
education the patient needs to enhance their overall health wellness and transition to post-
discharge therapies and treatment. Providing the knowledge, tools, and skill set to the bedside
nurses and multidisciplinary team members have proved successful through an increase in
patient satisfaction scores and a verbalized desire to remain at RMC while continuing to grow
professionally.
Through the implementation of the stroke support and education class, as well as the
nurse, staff, and physician education, there was a multitude of exposed positive factors. As
expected, there has also been a few minor alterations to the original implementation plan. Due to
an increased census, additional job requirements, and an inability to physically round on each
patient and nurse, the University of Mary Stroke Project team’s lead and clinical liaison added
minute additions. These additions included seeking approval for an overhead announcement to
be made each Thursday at 14:00 to remind staff, patients, and family members the class would
be beginning in one hour and to make their way to the 5th floor Rehab West dining room. This
approval was granted and takes place each week. Through verbalized feedback, directors,
managers, and staff members are grateful for this overhead reminder, as they can become tied up
with other tasks and lose track of time. Another measure was to announce every Thursday
during the bed huddle meetings that the class would be taking place that day, time, and place.
Through verbalized feedback, this too has proved to remind managers, directors, and charge
nurses that it is Thursday and they need to remind their direct patient care staff providing care for

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 75
the stroke patients of such. Additionally, a flyer (Appendix E) has now permanently been placed
in the stroke booklets provided to each patient at admission. This new implementation has
recently taken place and currently there has not been any staff feedback. However, the RMC
Stroke team foresees this as an additional opportunity to promote the stroke support and
education class, while minimizing the potential for the Stroke RN Navigators to formally request
the patient and family’s attendance at the class. As the patient is admitted and provided a
complimentary stroke booklet, the primary nurse educates and provides the strategically placed
flyer to the patient and family.
As with any change process, strengths and weakness are illuminated and potential
obstacles that need to be overcome are identified in order to promote a successful change.
Identified through the implementation of the stroke support and education class, as well as,
refining the educational materials provided to the patient and family, many strengths are
highlighted. The two superior strengths include the enhanced understanding the patient and
family members have verbalized, and the self-confidence and empowerment nurses have
verbalized. These two strengths alone create an atmosphere of positivity, self-confidence,
happiness, and empowerment where nurses know they are providing excellent, beneficial care,
and education to the patient ultimately enhancing the patient’s overall health wellness and
success once discharged home. This aspect is crucial for nurse retention and loyalty for any
healthcare organization.
As with the strengths, weaknesses too are illuminated. The weaknesses with the
implementation of this University of Mary graduate EBP project have been easily overcome with
additional reminders put in place, as well as, assurance that someone from RMC’s stroke team is
always accessible for questions or concerns. Moreso, the weaknesses have been strongly

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 76
overpowered by the strengths of this EBP project. This project has enlightened, enhanced, and
rejuvenated RMC’s core nursing team that despite one’s job title, all disciplines are there to
elevate the patient experience while providing the necessary needs for the patient with the same
common goal in place: the enhanced overall health wellness of our patient. Additionally,
through the refinement of educational materials for this life-altering disease process, stroke
readmissions have decreased by 2%. In fact, through routine rounding for patients suffering a
stroke diagnosis within the last 30 days, their readmission has been related to additional
comorbidities and disease process other than stroke.
Through the implementation of this EBP project, considerations for additional refined
disease specific education have been discussed. Moreso, through the review and outstanding
success for this EBP project, RMC is discussing additional positions for disease specific
education, i.e. STEMI RN Navigator, Infectious Disease RN Navigator, etc. Additionally, the
implementation of this EBP project have increased patient and nurse satisfaction scores, along
with an enhanced community reputation. Individuals seeking care at RMC have posted positive
feedback on national social media websites. Moreso, patients and family members are being
discharged with an enhanced knowledge base for how to implement interventions conducive to
improving their overall health wellness, as well as a sense of community. They are also
discharged with the confidence to recognize signs and symptoms of a stroke, when to call 9-1-1,
the realization they can provide care for themselves, and that there is hope and life after a stroke.
Patients and family members are being provided with the phone numbers of the Stroke RN
Navigators so that any question does not go unanswered. The sense of community, or that they
are not alone, is something that cannot be taught or educated, only felt. Therefore, the fact
patients and family members are verbalizing these once concerns they are no longer riddled by

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 77
prove the imperativeness, effectiveness, and efficacy for refined and enhanced disease specific
educational materials provided during acute hospitalization.
Handoff
The handoff of a project to the organization where it is implemented is a very important
stage in the projects future operational success. A well organized, efficient, and effective handoff
of information, practices, changes, and successes will help ensure the success and sustainability
of the project's future. At Research Medical Center, this project will be handed over to the
Stroke RN Navigator, Amy Ludwig and the Stroke Program Coordinator, Sherry Bahr, APRN,
CNRN.
The Stroke RN Navigator is working with the University of Mary’s Stroke Project team
project liaison to facilitate a smooth transition. The Stroke RN Navigator will be taking over the
very essence of the project by learning the educational material, reviewing the PowerPoint
presentation and educational notes, and visiting the classes to become more acquainted with the
teaching information. There will be a review of the project's current data, introductions to key
stakeholders of the project, and discussions on what did and did not work well with the project
implementation project. There will be a three-week transition and orientation period for the new
Stroke RN Navigator in order to facilitate a successful transition. The Stroke RN Navigator will
ultimately begin teaching the classes with the University of Mary’s Stroke Project team member
as their preceptor and eventually taking over the class and the project in its entirety. The
University of Mary’s Stroke Project team will remain available to the Research Medical Center
and the Stroke RN Navigator for any future questions or concerns.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 78
Conclusion
In conclusion, designing and implementing a structured and formalized educational class
providing information on a specific disease process requires commitment from the organization
at all positions and managerial hierarchy. Executive leadership members must find merit in the
program in order to provide their direct support. Acute direct supervisors and leadership
members need to find value in the educational program ensuring adequate resources are
available, as well as individual and team mentoring ensuring all front-line team members possess
a comprehensive understanding of the programs exclusive goal and intent. The Stroke Program’s
team members must also find merit and value in the program to bestow their supportive
measures. Stroke leaders, while lending their support, must assist in providing an excitement
within their co-workers about the program and the exceptional opportunity it provides patients
and family members.
Beginning at admission, the Stroke booklets will continue to be provided to the patient
and their family member(s). The admission nurse will provide education regarding the details of
the workbook and ask the patient, if able, and family member(s) to familiarize themselves
directing them to write down any questions or concerns in the allotted section. This booklet will
contain a flyer, inside the left pocket, inviting the patient and family to the stroke support and
education class offered every Thursday at 1500. Primary nurses providing daily care to the
patient will assist the patient and family to enter their pertinent lab values, vital signs, current and
home medications, as well as patient centered goals, and answer any questions. Promoting the
weekly class will also be done through all multidisciplinary team members, including the Stroke
team. As close to admission as possible, the Stroke RN Navigators will visit the patient
answering any questions or concerns providing personalized education. The Stroke RN

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 79
Navigators will educate the patient and family about the stroke support and education class held
weekly encouraging their attendance.
Conversely, CVA’s affect thousands of patients per year in the United States and
worldwide. Strokes, unfortunately, will continue to be the number one cause of disability each
year unless patients become more knowledgeable about their personal risk factors and ways to
implement changes. The external evidence-based literature review, along with the internal
organizational need, suggests an innovative form of quality education that is both beneficial and
will effectively address patient’s personal and specific needs. The group project presented,
throughout this paper, displays an intriguing detailed plan implementing preventative technique
to reduce the ineffective education patients were receiving, by providing improved educational
opportunities that enhanced the patient’s understanding of their personal disease process.
A diagnosis of a stroke is not only a shocking, but frightening experience for patients and
their families; therefore, providing educational information that assists patients, family members,
and their caregivers in enhancing their understanding regarding their personal risks, needs, and
care will help to alleviate those feelings of uncertainty and fear. Implementing an educational
opportunity in a safe environment that provides a personalized approach to the patients and their
family members has promoted a cohesive learning environment. This presented opportunity has
not only enhanced the knowledge level of the patient and family; it has promoted and
encouraged healthier lifestyle choices potentially extending the longevity of their life.
Often times it is difficult to know the individual needs of patients; however, when nurses
are adequately prepared to provide quality patient education they are able to individualize and
personalize educational materials meeting the needs of the patients. The utilization of group
support and educational classes can be implemented to assist patients in boosting knowledge of

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 80
their disease process through group discussions. This setting allows patients to learn from
multidisciplinary team members while also providing an opportunity for patients to share their
personal experiences learning from each other. Group support and educational classes foster an
environment of comfort and safety for patients, family members, and caregivers knowing that
they are not the only one experiencing tragedy in relation to a stroke disease process.
Implementing these interventions provided by the University of Mary’s Stroke Project
team, has made patients more knowledgeable about their disease process so they are less likely to
experience negative outcomes and less uncertainty related to their stroke diagnosis. The
University of Mary’s Stroke Project team has developed a handoff plan so RMC can continue on
with the implementation of these interventions with excitement and positivity in the fact this
project will improve the lives of individuals and their family members suffering from this
devastating, life-altering diagnosis.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 81
References
Alrubaiee, L., & Alkaa'ida, F. (2011). The mediating effect of patient satisfaction in the
patients' perceptions of healthcare quality – Patient trust relationship. International
Journal of Marketing Studies, 3(1). doi:10.5539/ijms.v3n1p103
American Stroke Association (ASA). (2016). Impact of Stroke. Retrieved from
http://www.strokeassociation.org/STROKEORG/AboutStroke/Impact-of-Stroke-Stroke-
statistics_UCM_310728_Article.jsp#.WUZ_JuTXtet.
American Stroke Association (ASA). (2015). Stroke fact sheet. Retrieved from
https://www.heart.org/idc/groups/heartpublic/@wcm/@gwtg/documents/downloadable/
ucm_451247.pdf.
Aslani, Z., Alimohammadi, N., Taleghani, F., & Khorasani, P. (2016). Nurses’ empowerment in
self-care education to stroke patients: An action research study. International Journal of
Community Based Nursing & Midwifery, 4(4), 329-338.
Blauer, C., Frei, I. A., Schnepp, W., & Spirig, R. (2015). Implementation of a nurse-led
education programme for chronic heart failure patients during hospitalisation and
strategies supporting their self-management at home: A practice development project in
the context of the Swiss healthcare system. International Practice Development Journal,
5(1).
Brooks-Staub, K. (2005). The evidence is in. Johns Hopkins Nursing. Retrieved from
http://magazine.nursing.jhu.edu/2005/12/the-evidence-is-in/.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 82
Choi-Kwon, S., Lee, S. K., Park, H. A., Kwon, S. U., Ahn, J. S., & Kim, J. S. (2005). What
stroke patients want to know and what medical professionals think they should know
about strokes: Korean perspectives. Patient Education and Counseling, 56(1), 85-92.
http://dx.doi.org/10.1016/j.pec.2003.12.011.
Furie, K. L., et al. (2011). Guidelines for Prevention of Stroke in Patients With Ischemic
Stroke or Transient Ischemic Attack. Stroke, 42: 227-276.
Håkanson, C., Sahlberg-Blom, E., Ternestedt, B., & Nyhlin, H. (2011). Learning to live with
irritable bowel syndrome. The influence of a group-based patient education programme
on peoples' ability to manage illness in everyday life. Scandinavian Journal Of Caring
Sciences, 25(3), 491-498.
Ing, M. M., Linton, K. F., Vento, M. A., & Nakagawa, K. (2015). Investigation of stroke needs
(INVISION) study: Stroke awareness and education. Hawai’i Journal of Medicine &
Public Health, 74(4), 141-145. Retrieved from
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4407457/.
The Johns Hopkins University. (2017). [Image of the Johns Hopkins Nursing
Evidence-Based Practice model]. Johns Hopkins Nursing Evidence-Based Practice
model retrieved from
http://www.hopkinsmedicine.org/evidence-based-practice/jhn_ebp.html.
The Joint Commission. (2014). Why choose comprehensive stroke center certification?
Retrieved from

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 83
https://www.jointcommission.org/certification_for_comprehensive_stroke_centers/.
The Joint Commission. (2017). Comprehensive Stroke Certification:Standardized Performance
Measures. Retrieved from
https://www.jointcommission.org/
performance_measures_for_comprehensive_stroke_centers .
Litchman, J.H., Leifheit-Limson, E.C., Jones, S.B., Wang, Y., & Goldstein, L.B. (2013).
Preventable readmissions within 30 days of ischemic stroke among Medicare
beneficiaries. Stroke, 44, 3429-3435. DOI: 10.1161/STROKEAHA.113.003165
Melnyk, B. M. & Fineout-Overholt, E. (2015). Evidence-based practice in nursing &
healthcare: A guide to best practice. (3rd ed.). Philadelphia: Lippincott Williams &
Wilkins.
Polit, D. F., & Beck, C. T. (2017). Evidence-based nursing: Translating research evidence into
practice. In Nursing research: Generating and assessing evidence for nursing practice
(10th ed.). Philadelphia, PA: Wolters Kluwer.
Polit, D. F., & Beck, C. T. (2012). Nursing research: Generating and assessing evidence for
nursing practice (9th ed.). Philadelphia: Wolters Kluwer/Lippincott Williams &
Wilkins.
Research Medical Center. (2017). About us. http://researchmedicalcenter.com/about/index.dot.
Roussel, L, Thomas, P. L., & Harris, J. L. (2016). Management and leadership for nurse

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 84
administrators. (7th ed.). Burlington, MA: Jones & Bartlett Learning.
Sanders, K., Schnepel, L., Smotherman, C., Livingood, W., Dodani, S., Antonios, N., ...
Silliman, S. (2014). Assessing the impact of health literacy on education retention of
stroke patients. Preventing Chronic Disease, 11, 1-10.
http://dx.doi.org/10.5888/pcd11.130259.
Sherman, J.R. (2016). An initiative to improve patient education by clinical nurses.
MEDSURG
Nursing, 25(5), 297-333.
Sowtali, S. N., & Harith, S. (2014). Educational needs among stroke patients admitted to
Hospital Universiti Sains Malaysia: Preliminary findings. Jurnal Sains Kesihatan
Malaysia, 12(1), 67-73. http://dx.doi.org/10.17576/jskm-1201-2014-09.
Tamura-Lis, W. (2013). Teach-back for quality education and patient safety. Urologic
Nursing,
33(6), 267-298.
Yonaty, S., & Kitchie, S. (2012). The Educational Needs of Newly Diagnosed Stroke Patients.
Journal of Neuroscience Nursing, 44(5), E1-E9. doi:10.1097/jnn.0b013e31826663f2

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 85
Appendix A
Permission Granting the Use of Johns Hopkins Nursing Evidence-Based Practice Model
“We are happy to give you permission to use the model and tools as you described. The zipped
file of the tools are located here -
http://www.hopkinsmedicine.org/institute_nursing/_docs/Model_and_Tools_2013.zip
If you choose to use the Johns Hopkins Nursing Evidence-Based Practice Model and Tools in
any other way, please submit another request for that specific use. You may not modify the
model or the tools. All reference to source forms should include “©The Johns Hopkins
Hospital/The Johns Hopkins University.” Please note, this permission does not include any
commercial use.”
Kim Bissett
Evidence-Based Practice Coordinator
Institute for Johns Hopkins Nursing

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 86
Appendix B
Flyer for Huddle
Great Educational Opportunity!● Who: All nursing staff and members of the
multidisciplinary teams● What: Education on stroke booklet and how to
provide patient education using the teach-back method
● Where: Unit huddle locations● When: Unit huddle times● Why: So, nursing staff and members of the
multidisciplinary team can gain more confidence in their abilities to understand and educate on the stroke booklet and learn how to provide patient education using the teach-back method.

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 87
Appendix C
Pre-Education Informative Questionnaire for Patients, Families, & Caregivers

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 88
Appendix D
Post-Education Informative Questionnaire for Patients, Families, & Caregivers

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 89
Appendix E
Stroke Education Course Flyer

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 90
Appendix F
Education Feedback
Nurse Education Feedback
1. Was this educational opportunity helpful?Yes______ No______
2. What did you learn that you felt was beneficial?__________________________________________________________________________________________________________________________________________________________________________________________________________________ 3. What area of education could be improved?__________________________________________________________________________________________________________________________________________________________________________________________________________________
Appendix G

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 91
Institutional Review Board (IRB) Application

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 92

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 93

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 94

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 95

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 96

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 97

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 98

REFINING EDUCATIONAL NEEDS FOR STROKE PATIENTS 99
Appendix H
IRB Approval