it's not my job....or is it? the role of the rt in the patient centered medical home by...
TRANSCRIPT

IT’S NOT MY JOBOR IS IT?
THE ROLE OF AN RT IN A PCMH
RESPIRATORY CARE SYMPOSIUMJUNE 26TH, 2015
CANDACE RAMOS, MHA, RRT
www.cmpcn.org
Objectives for presentation
At the end of the session, learners will be able to:1. Define the Patient-Centered Medical Home
model2. Discuss previous education models within the
health care system.3. Describe the role of the Respiratory Therapist
in the Patient-Centered Medical Home model.
www.cmpcn.org
History of PCMH
1967: Concept first introduced by the American Academy of Pediatrics (AAP)
2001: The IOM’s Crossing the Quality Chasm: A New Health System for the 21st Century states that “the system of care should revolve around the patient
2007: Joint Principles of the Patient-Centered Medical Home is put forth by the AAP, AAFP, ACP, and AOA
www.cmpcn.org
What is a Medical Home?
• An approach (not a place) providing care that involves a partnership with the child, family, primary care practice as the “home” where the family and child feel recognized and supported. ( Children’s Hospital and Clinics of Minnesota)
• Team based health care delivery system, physician led, providing comprehensive and continuous care maximizing health outcomes.
www.cmpcn.org
Medical Home News definition
• PCMH model of primary care is designed to strengthen the patient-clinic relationship, replace episodic care with effective care coordination and improve health outcomes.
• Medical homes offer:enhanced accessshared decision makingactive participation in their own care
Medical Home News, Volume 7, Number 6 June 2015
www.cmpcn.org
IHI*Triple Aim Supports PCMH
• Improve the Health of Populations• Improve the Patient Experience of Care• Reduce the per capita Costs of Care of
HealthcareInspires Quality of CareEngaging Patient RelationshipsSavings through access and delivery of care options
*IHI- Institutes of Healthcare Improvement
www.cmpcn.org
WHY create a Medical Home?Value
Improve clinical outcomes= QUALITY
Decrease ER visits Decrease hospital admissions Increase preventative screenings, quality
measures
Improve reimbursement and reduce COSTS
Higher satisfaction for patient, providers and staff IMPROVED OPERATIONAL EFFECTIVENESS
AND EFFICIENCY
www.cmpcn.org
HEALTHCARE REFORM
www.cmpcn.org
The ANSWER
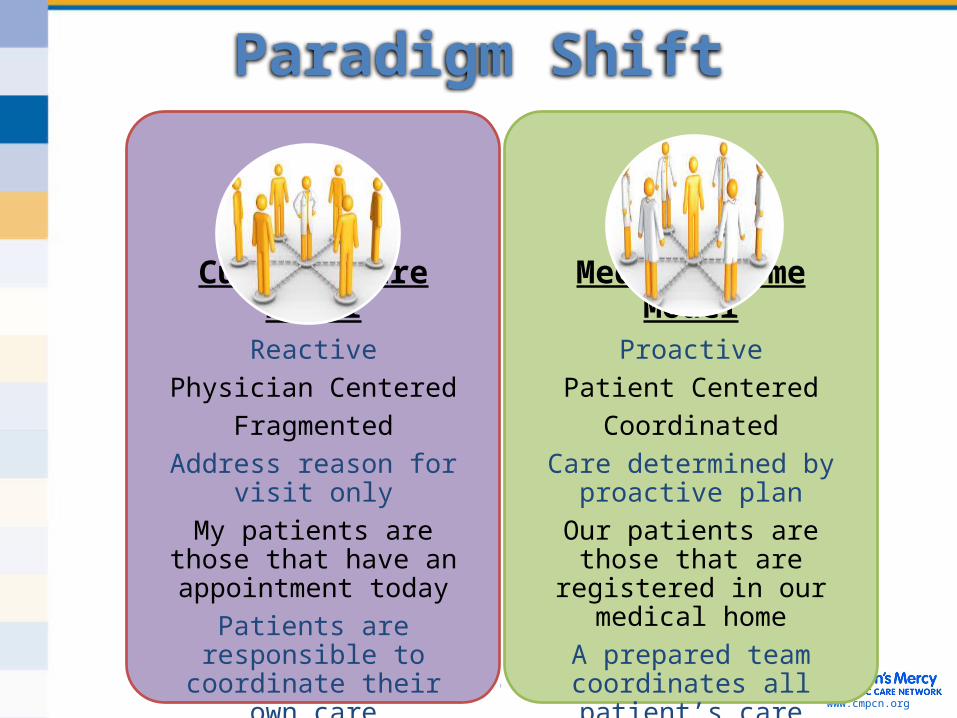
Current Care ModelReactive
Physician CenteredFragmented
Address reason for visit onlyMy patients are those that have an appointment todayPatients are responsible to coordinate their own care
Medical Home ModelProactive
Patient CenteredCoordinated
Care determined by proactive plan
Our patients are those that are registered in our medical
homeA prepared team coordinates
all patient’s care
Paradigm Shift
www.cmpcn.org
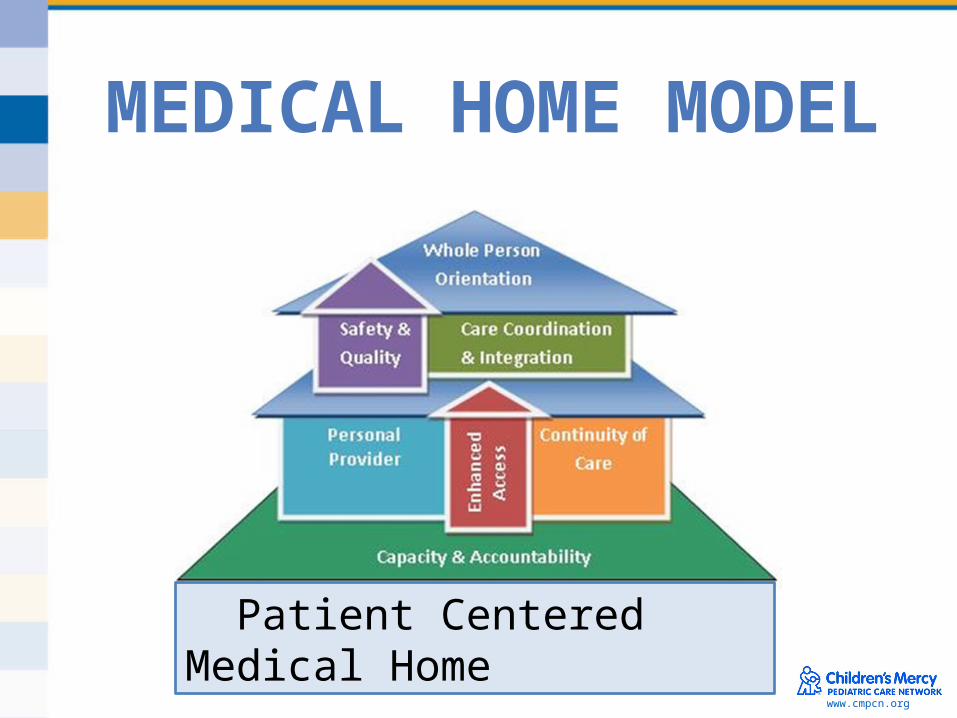
Patient Centered Medical Home
MEDICAL HOME MODEL
12www.cmpcn.org
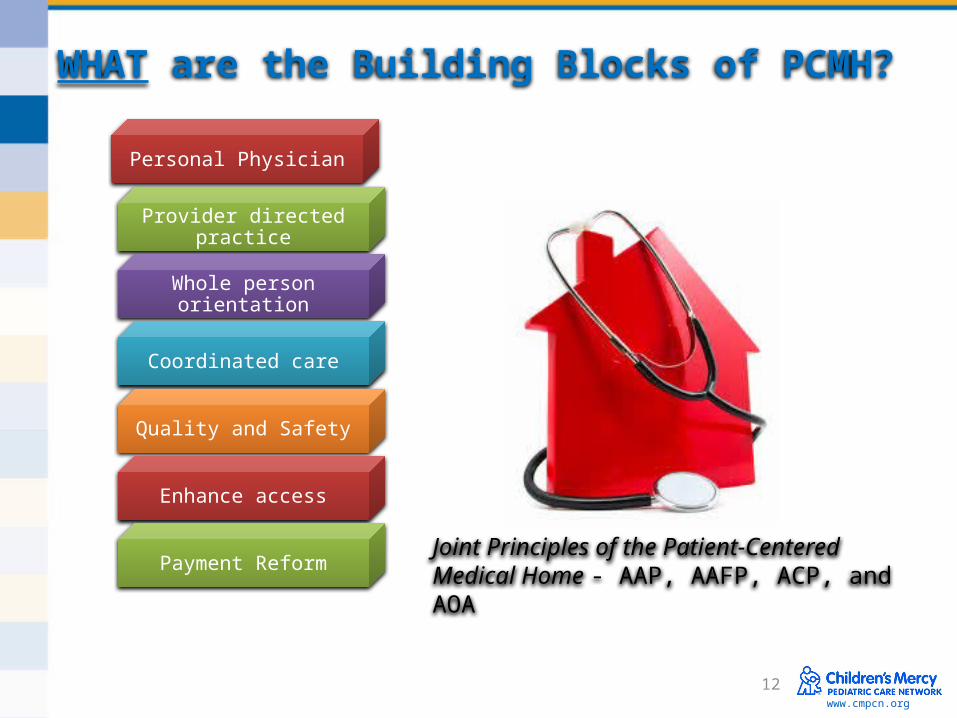
WHAT are the Building Blocks of PCMH?
Personal Physician
Provider directed practice
Whole person orientation
Coordinated care
Quality and Safety
Enhance access
Payment ReformJoint Principles of the Patient-Centered Medical Home - AAP, AAFP, ACP, and AOA
13www.cmpcn.org
WHAT are the Building Blocks of PCMH?
•each patient has an ongoing relationship with a personal physician trained to provide first contact, continuous and comprehensive care
Personal Physician
Provider directed practice
Whole person orientation
Coordinated care
Quality and Safety
Enhance access
Payment Reform
14www.cmpcn.org
WHAT are the Building Blocks of PCMH?
Personal Physician
•the personal provider leads a team of individuals at the practice level who collectively take responsibility for the ongoing care of patients.
Provider directed practice
Whole person orientation
Coordinated care
Quality and Safety
Enhance access
Payment Reform
15www.cmpcn.org
WHAT are the Building Blocks of PCMH?
Personal Physician
Provider directed practice
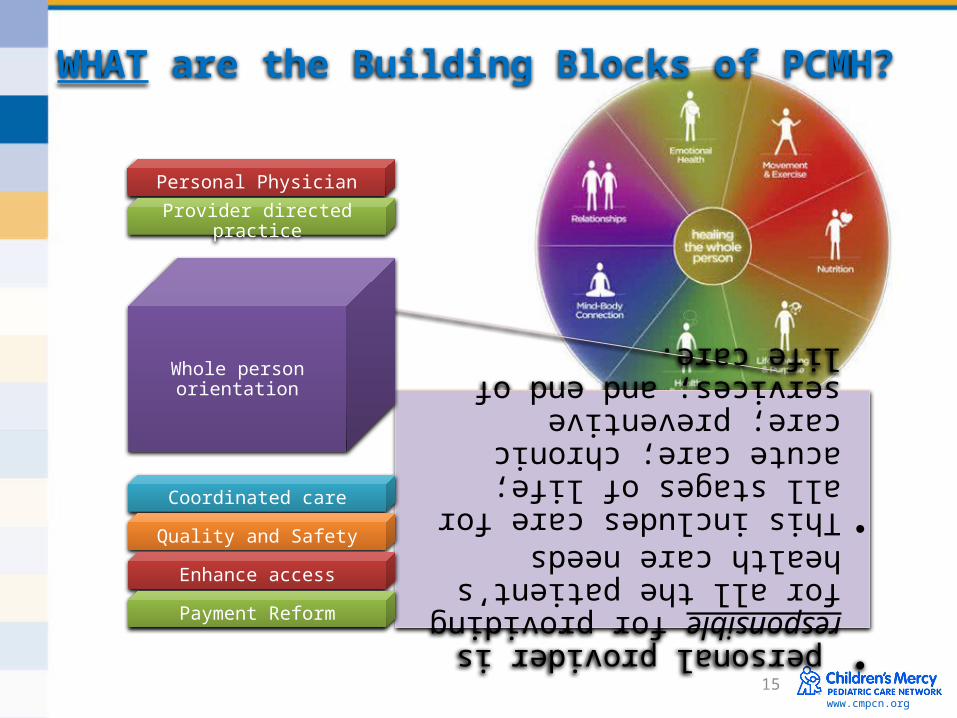
• personal provider is responsible for providing for all the patient’s health care needs
•This includes care for all stages of life; acute care; chronic care; preventive services; and end of life care.
Whole person orientation
Coordinated care
Quality and Safety
Enhance access
Payment Reform
www.cmpcn.org
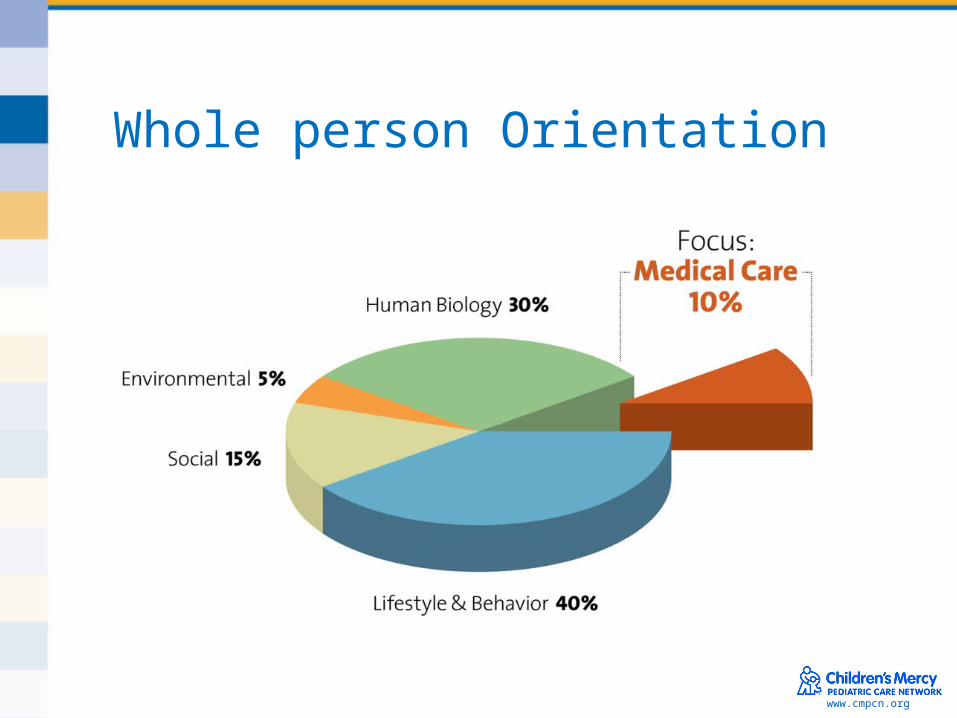
Whole person Orientation
17www.cmpcn.org
WHAT are the Building Blocks of PCMH?
Personal Physician
Physician directed practice
Whole person orientation
Coordinated care
Enhance access
Payment Reform
www.cmpcn.org
What is Care Coordination?
Care that is coordinated across the health care system and the patient’s communityPromotes:• Peer to peer communication• Tools and information that promote best practices and guidelines• Opportunities to connect with specialists and services-
Transitions of care
18
www.cmpcn.org
What are team-based relationships?
• Care determined by proactive plan-AAP• Meet patients needs• Address chronic disease at every visit• Staff work flow-– Pre-visit Planning/Huddles
• Working at the top of licenseEducation/Assessment/Treatment Plan
20www.cmpcn.org
Personal Physician
Physician directed practice
Whole person orientation
Coordinated care
Quality and Safety
Enhance access
Payment Reform
WHAT are the Building Blocks of PCMH?
In quality and safety all of the pieces come together in the right way, at the right time and in the right place.
www.cmpcn.org
What is Organized, Evidence-based Care?
• Clinical Practice Guidelines (CPG’s) for clinically important conditions– Asthma – Diabetes– Immunization schedules
• Educating providers-everyone on the same page – Consistent message for patients– Standardized workflow can create more
satisfaction for staff-– Performance monitoring– Improved outcomes
www.cmpcn.org
Moving from Traditional Care to Population Health
Chronic disease self management- • empower patients to take an active role• Regardless of chronic condition, people have
similar challenges with self management( Asthma/CF/COPD)
• Partnership with primary care and population health
• Prevention and Chronic Care management• Training and population health support
22
23www.cmpcn.org
WHAT are the Building Blocks of PCMH?
Personal Physician
Physician directed practice
Whole person orientation
Coordinated care
Quality and Safety
Enhance access
Payment Reform
24www.cmpcn.org
Personal Physician
Provider directed practice
Whole person orientation
Coordinated care
Quality and Safety
Enhance access
Payment Reform
WHAT are the Building Blocks of PCMH?
www.cmpcn.org
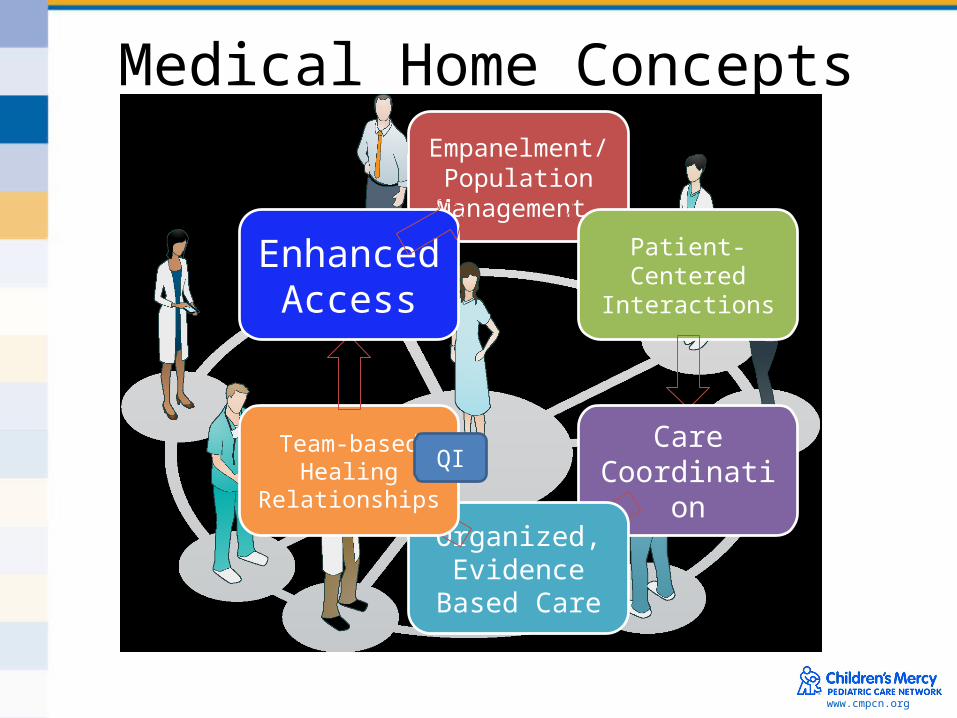
Medical Home ConceptsEmpanelment/
Population Management
Patient-Centered
Interactions
Care Coordination
Organized, Evidence
Based Care
Team-based Healing
Relationships
Enhanced Access
QI
www.cmpcn.org
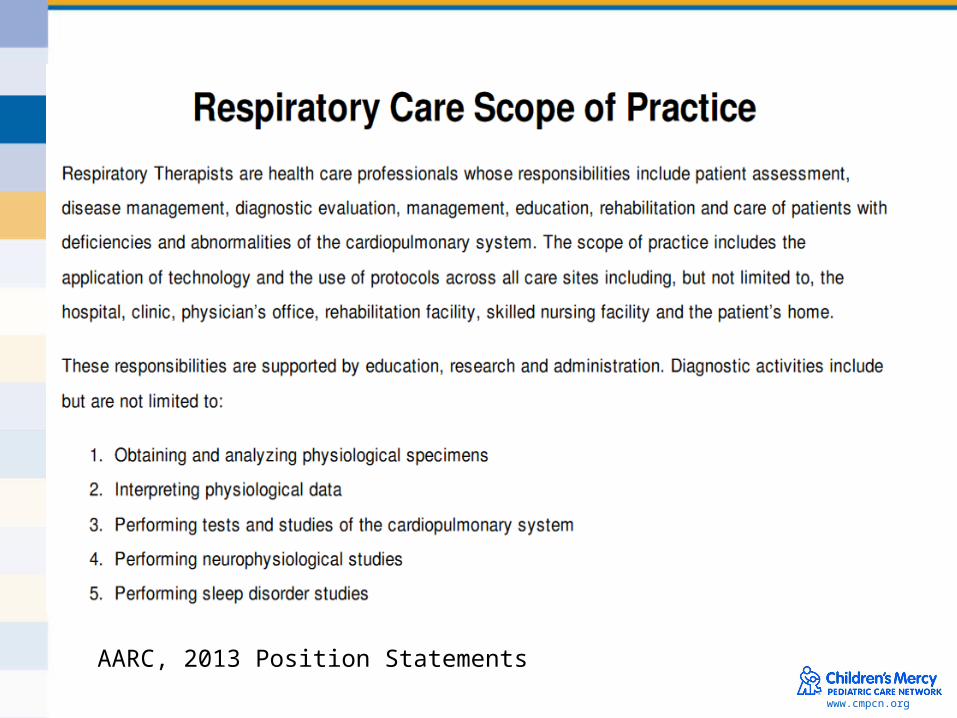
A
AARC, 2013 Position Statements
www.cmpcn.org
New Strategic Plan for RT
1) Refine and expand the scope of practice….2) Support research and scientific inquiry to
strengthen the scientific foundation and promote best practice for patient care.
3) Advocate for federal and state health care policies that enhance patient care, patients access to care, and professional practice.
4) Advance knowledge base…to ensure competent care and foster patient safety…
AARC- New Strategic Plans, Full implementation by 2020
www.cmpcn.org
RT Scope of Practice
• What’s my job?Treatment Plan Empowerment of Self ManagementChronic DiseasesDisease Specific EducationPatient Education
Access, Where is care delivered? PCP
www.cmpcn.org
Example of RT in the PCMH
• Asthma RegistriesReview AAP at every visitPFT’s completed before provider enters
• ER visits- Reinforce PCP engagement• Primary Care Appt’s- Call the patient if they
don’t come in PROACTIVE vs REACTIVE Care
www.cmpcn.org
Traditional Disease Management to Medical Home
Disease Management Disease focused Disease managers Change patients & physicians
PCMH Office practice focused Multidisciplinary teams Change physicians &
patients
SHS©
www.cmpcn.org
ROLES
TRANSITIONS
Where to begin?
www.cmpcn.org
www.cmpcn.org
CHALLENGE
1. Call a PCP to solicit input into the Plan of Care/Discharge Plan
2. Discuss importance of follow up with PCP
3. Review Treatment Plan with Patient and providers
www.cmpcn.org
HEALTHCARE REFORM
www.cmpcn.org
Future of the RT
IT IS MY JOB!!