it’s good to talk: engaging with our stakeholders
TRANSCRIPT

It’s good to talk: Engaging with our stakeholdersLinda TerryBioanalysis, Immunogenicity and Biomarkers (GSK, Stevenage site)
EBF Focus meeting September 2019: Context of use

Disclaimer and COI
– I am a GSK employee and shareholder– Any views expressed in these slides are my personal thoughts and do not necessarily
represent those of GSK or the industry– All animal studies were ethically reviewed and carried out in accordance with Animals
(Scientific Procedures) Act 1986 and the GSK Policy on the Care, Welfare and Treatment of Animals.”

– How we discuss CoU at GSK– How it drives our fit-for-purpose method development and validation– A case study: The expectations, assumptions, challenges, results, the way forward, how it
changed our way of thinking and talking to our stakeholders
Supporting project teams for drug development: Minimising risk where we can
Context of Use for biomarker assessment in practice
EBF 2019 3
We are moving away from the 3-tiered approach
Using CoU to determine development and validation strategy
EBF 2019 4
– Has been useful in many cases
– Recent experience is leading us away from this approach and into a different paradigm
– Assay development is more complicated than the three broad buckets

Tailored NOT tiered
Using CoU to determine development/validation strategy
EBF 201916x9 core template 5
Why?• Because broad buckets do not tend to work for us in the
translational and early development space (one size does not fit all)
• Hinders the scientific process of decision making and accountability and inadvertently disengages the scientist’s brain
• Exploratory is a catch all for biomarkers whatever their purpose, from as broad as potentially useful development support with no clear decisions to making clear internal decisions including dose decisions.

– A: Type of Biomarker (Target engagement, distal/proximal pharmacodynamics, safety, disease, patient selection etc) and stage of development
– B: How data will be used and who will be using it. (making dose decisions, exploring potential treatment effects, support for hypothesis driven questions, regulatory submission)
– C: What type of data is expected (mass units, change from baseline, percent control, cut-off assessment, large/small delta etc)
– D: Basic assay challenges (normal/disease levels, matrix, endogenous available, assay available etc)
Considerations for CoU: getting into the weeds
The GSK evolving approach
EBF 2019 6
How much risk is the programme team willing to take?

– Typically in early development: Preclinical to FTIH– Internal decisions (often described as exploratory)
– Essential data to drive programme progression (candidate selection)– Data used to make dose decisions/recommendations– Actual mass units used to develop models – May be used to make dose escalation decisions– Needs to be sufficiently robust to give relatively accurate measurements that are consistent through
preclinical and dose escalation (FTIH) in humans
The Case Study:Biomarkers to demonstrate Target Engagement
EBF 2019 7
Expectations all the same? Cookie cutter approach? Translational? Tier 2?

Levels of CoU– A: Target engagement in a Preclinical PK/PD study to be used for candidate
selection
– B: Visualisation only (not to be used for modelling), no expectations of pair wise comparisons. Not discussed with modeller (user of data). (Error alert)
– C: Relative accuracy preferred (molar concentrations standard)
Case study ctd
EBF 2019 8
TE assay for a mAb therapeutic targeting a soluble analyte X:

– D: Basic assay Challenges: The assumptions
– Assumption 1: Levels of the soluble target analyte will accumulate as apparent half life of the analyte takes on half life of the drug
– Assumption 2: Unable to measure baseline levels, assume low pg/ml that will accumulate to low ng/ml
Case Study: Development of a TE assay for translational purpose
EBF-2019 9

– Analyte accumulates to ng/ml quantities from BLQ at baseline
– Dose response– Molar units reported– Data used to model, make
recommendations for dose at next stage
A typical response post Ab administrationEquivalent PK/PD study to case study
EBF 2019 10
01 6 8
3 3 65 0 4
6 7 28 4 0
0
5 0 0 0
1 0 0 0 0
1 5 0 0 0
2 0 0 0 0
2 5 0 0 0
A n a ly te Y T o ta l
T im e (H rs p o s t a d m in )
co
nc
(p
g/m
l)
low
m id
h ig h

Potential Assay Formats for case study
EBF 2019 11
Challenge 1: Levels not detectable at baselineChallenge 2: No available in house or commercial assay suitable for the speciesChallenge 3: Reagent scarcity. Challenge 4: Endogenous analyte not available from relevant speciesChallenge 5: Not much time (4 months before start of study)
Development strategy based on what was available at the time and not true CoU

12
Analyte X Complex Assay Validation Summary
Parameter ResultAssay range 200,000 – 400 pg/mL
MRD 1 in 2: parallelism not tested due to lack of availability of samples: RISK!
Precision (%CV) Intra assay: ≤30.8% CVInter assay: ≤31.2% CV
Accuracy (%RE) Intra assay: ≤±23.5% REInter assay: ≤±16.4% RE
Selectivity ~30% of individuals are high responders in absence of drug. RISK
Specificity Confirmed
Stability No endogenous, not tested. RISK
Interfering substances Not done. RISK
RISKS identified but assay seemed fit for purpose based on assumptions
EBF 2019 13
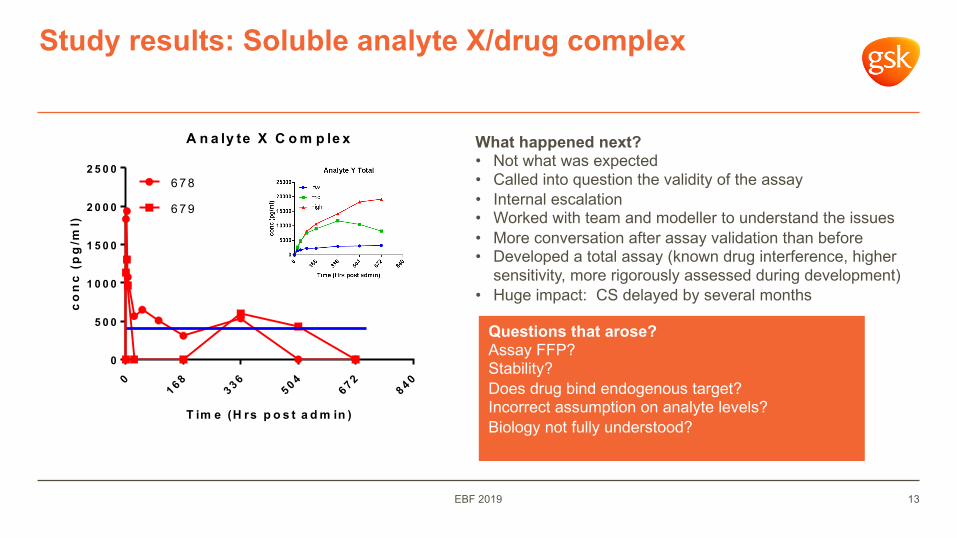
Study results: Soluble analyte X/drug complex
01 6 8
3 3 65 0 4
6 7 28 4 0
0
5 0 0
1 0 0 0
1 5 0 0
2 0 0 0
2 5 0 0
A n a ly te X C o m p le x
T im e (H rs p o s t a d m in )
co
nc
(p
g/m
l)
678
679
What happened next?• Not what was expected• Called into question the validity of the assay• Internal escalation • Worked with team and modeller to understand the issues• More conversation after assay validation than before• Developed a total assay (known drug interference, higher
sensitivity, more rigorously assessed during development)• Huge impact: CS delayed by several months
Questions that arose?Assay FFP?Stability?Does drug bind endogenous target?Incorrect assumption on analyte levels?Biology not fully understood?

14
Several months later: Analyte X Total Redevelopment and Validation Summary
Parameter Result
Assay range 3.9 – 15000 pg/mL
Parallelism (lysate) Acceptable neat through to 1/8 (human not cyno; RISK!)
Standard Curve Precision (%CV)
≤12% CV
Standard Curve Accuracy (%RE)
≤15% RE
VC Precision (%CV) ≤14% CV
VC Accuracy (%RE) ≤±21% RE
EQC Precision (%CV) using cell lysate
≤21% CV
Total Error ≤30%
Stability (of lysate) F/T stable through x3 cycles. RISK of unknown sample stability
Drug Interference High drug interference observed with both recombinant and EQCs. Managed by adding drug into curve. HIGH RISK mitigated
• Higher sensitivity (400 to 4 pg/ml). • Most risks mitigated. • Biology team and modeller highly
engaged throughout process• Sample analysis approved by the project
team

EBF 2019 15
Study results: Soluble Total analyte
Answered question about validity of the first assay
• TE confirmed
• Levels only reached ~70 pg/ml (<400 pg/ml)
• The profile was as expected but concentrations 2 logs lower
• Team agreed that due to level of validation this was likely a true reflection of actual levels
• Likely explanation: Analyte Biology!01 6 8
3 3 65 0 4
6 7 28 4 0
0
2 0
4 0
6 0
8 0
A n a ly te X T o ta l
T im e (H rs p o s t a d m in )
co
nc
(p
g/m
l)
677
678
679

EBF 2019 16
And the final word
– Case study steering us towards a CoU driven approach and greater stakeholder involvement prior to development
– A great learning experience
– Rewarding interactions with the biologists and the modeller: More satisfactory understanding of data, encouraging a no blame culture and be true scientists
– Still evolving dev/validation strategies
– Sometimes the unexpected happens
– Thanks to all the analysts: Mike Naughton, Julie Egerton and Teresa Heslop (all GSK/UK), for keeping their heads while many were losing theirs