issues in comprehensive pediatric nursing the …backoffice.neonatologia.it/upload/988_bs_neonatal...
TRANSCRIPT

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [EBSCOHost EJS Content Distribution]On: 13 November 2008Access details: Access Details: [subscription number 902156990]Publisher Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Issues in Comprehensive Pediatric NursingPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713630242
The Neonatal Skin Risk Assessment Scale for Predicting Skin Breakdown inNeonatesBarbara Huffines a; M Cynthia Logsdon a
a School of Nursing and Health Sciences, Spalding University, Louisville, Kentucky, USA
Online Publication Date: 01 April 1997
To cite this Article Huffines, Barbara and Logsdon, M Cynthia(1997)'The Neonatal Skin Risk Assessment Scale for Predicting SkinBreakdown in Neonates',Issues in Comprehensive Pediatric Nursing,20:2,103 — 114
To link to this Article: DOI: 10.3109/01460869709026881
URL: http://dx.doi.org/10.3109/01460869709026881
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

THE NEONATAL SKIN RISK ASSESSMENT SCALE FOR PREDICTING SKIN BREIAKDOWN Rv NEONATES
BARBARA HUFFINES, RN, MSN, ARNP-C, FNP M. CYNTHIA LOGSDON, DNS, RN School of Nursing and Health Sciences, Spalding Universiy, Louisville, Kentucky, USA
An instrument was developed to assess neonates at risk for skin breakdown, based on the Braden Scale for Predicting Pressure Sore Risk in adults. Using such an instru- ment to predict, and thus prevent, skin breakdown could decrease costs associated with prolonged hospital stays in neonates. The Neonatal Skin Risk Assessment Scale (NSRAS) was piloted with 32 neonates. Reliability was high for the subscales of general physical condition, activity, and nutrition, but low in the other three sub- scales. For predictive validity, sensitivity was 83% and specificity was 81%. The NSRAS appears to be useful in predicting days most likely for skin breakdown to occur.
In neonatology, the skin is used to assess maturity and neonatal vitality and acts as a defense against assault from the external environment. The skin is a major organ of the neonate, making up 13% of the neonate’s body weight as compared with 3% of an adult’s body weight. Today’s survival rates of smaller and more immature neonates-and increased technology involving the use of new, and potentially invasive, equipment on neonates with fragile skin-demands research to provide a scientific database to reduce skin breakdown.
Nursing care practices that affect the fragile, underdeveloped skin of the neonate present major dilemmas for health care providers. Significant morbidity and mortality of neonates can be attributed to practices that cause trauma to skin or alterations in normal skin function.
Although assessment tools have been used for prediction of skin im- pairment risk in adults (Bergstrom, Demuth, & Braden, 1987), such pre- diction could also be useful in neonatal populations. An effective instru- ment should identify neonates who are at risk for skin impairment and, when they are at risk, assist nurses in early problem identification, with particular vigilance possible on days of greatest risk. Prevention of skin
Address correspondence to M. Cynthia Logsdon, 7514 Chestnut Hill Drive, Prospect, KY 40054, USA. E-mail: mclogs0l~ulkyvm.louisville.edu
Issues in Comprehensive Pediab-ic Nursing, 20: 103-1 14, 1997 Copyright 0 1997 Taylor & Francis
0146-0862/97 $12.00 + .OO I03
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

104 B. Huffnes and M C. Logsdon
breakdown could result in decreased hospital stays and thus reduce costs of neonatal care, a goal worthy of pursuit.
BACKGROUND
Human skin is composed of three anatomically distinct layers: the epider- mis, the dermis, and the subcutaneous tissue. The horny outer layers of the epidermis, the stratum corneum, which are composed mostly of closely packed dead cells, are the skin’s main barrier to protection and are con- tinually being sloughed off by clothing and bathing. These cells take approximately 26 days to migrate up to the stratum comeurn. In a study of fetal skin development, Hosimoto (1966) found that the keratinized stratum corneum begins to develop in the 6th or 7th month of fetal life.
Several factors, including increased permeability that favors transcuta- neous absorption of chemicals and drugs, heat dissipation, and an in- crease in cutaneous insensible water loss, demonstrate that the underde- veloped stratum corneum of the preterm neonate’s skin interferes with the natural barrier functions of the skin (Harpin & Rutter, 1983; Rutter, 1987). In a review of the maturation process of neonatal skin, researchers have concluded that the barrier properties of the neonate’s skin are dependent on both gestational and chronological ages (Harper & Rutter, 1983; Holbrook, 1982; Kuller, 1984; Rasmussen, 1987). A significant nursing challenge is the ability to predict which neonates will develop skin breakdown and to protect their immature skin until maturation occurs.
Stressors such as nutritional status (LeFrak, 1984), therapeutics such as use of paralytic agents that increase permeability (Jackson & Suther- land, 1981; Kuller, Lund, & Tobin, 1983; West, Worobec, & Solomon, 1981), use of technology (Lund, Kuller, Tobin, LeFrak, & Franck, 1986; McManus, 1 9Sl), and characteristics of the physical environment (Doyle & Sinclair, 1982; O’Leary, 1983) are also thought to influence skin in- tegrity. Protecting neonates from these threats is time consuming and demands specialized nursing practices.
Some researchers (Huffines & Logsdon, 1995; Larson, 1986) have described the usefulness of assessment tools to predict and prevent pa- tient problems. An ability to predict threatening conditions, such as skin breakdown, potentially saves patient discomfort as well as costly resources in nursing time, procedures, equipment, and length of hospital stay. Braden and her associates (Braden & Bergstrom, 1994; Bergstrom, Demuth, & Braden, 1987) developed and tested an instrument, the Braden Scale for Predicting Pressure Sore Risk, to predict development of pressure sores in a nursing home population. Other researchers have successfully used the instrument at large acute-care facilities (Barnes & Payton, 1994; Gawron,
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

Predicting Skin Breakdown in Neonates 105
1994) and long-term care facilities (Xakellis, Frantz, Arteaga, Njuyen, & Lewis, 1992).
The Braden Scale for Predicting Pressure Sore Risk is composed of six subscales: Mobility, Activity, Sensory Perception, Skin Moisture, Nutri- tional Status, and Friction and Shear. The scale is based on the theoretical premise that pressure sores develop as a result of both pressure (amount and duration) and the tolerance of the tissue for pressure. Subscale scores are rated on a scale ranging from 1 to 4, except for friction, which is rated on a scale ranging from 1 to 3. Higher scores indicate higher levels of functioning and thus lower levels of risk. The critical cut-off point at which patients are considered at risk to develop pressure sores, deter- mined in a clinical trial, is 16 out of a maximum of 23 points. The sensitivity of the instrument has been established; all participants who developed pressure sores had scores of 16 or less. The scale is also re- ported to be 64%-90% specific, meaning that the majority of patients assessed to be at risk developed pressure sores (Bergstrom et al., 1987). Thus, the Braden scale is an excellent criterion on which to base an instrument for neonates. Although another instrument developed for a pediatric population and based on Braden’s scale has been reported in the literature, no reliability or predictive validity data are reported (Quigley & Curley, 1996). Thus, there is a need for the present study.
RESEARCH METHOD AND DESIGN
Research Design
We designed this descriptive pilot study to test the reliability and predic- tive validity of the Neonatal Skin Risk Assessment Scale (NSRAS).
Participants
A neonatal intensive care unit in a southern, tertiary-care hospital was the setting of the study. During the 3-month data collection period, a conve- nience sample of 32 neonates in the neonatal intensive care unit partici- pated in the study after written consent was obtained from the parent. Participants were eligible for inclusion in the study if they did not have any existing breaks or lacerations on their skin and were excluded if they had any genetic dermatological conditions.
Participants ranged from 26 to 40 weeks’ gestation ( M = 33.03, SD = 3.99), were nearly equally divided between boys (47%) and girls (53%), and were predominantly Caucasian (84%). The most frequently occurring diagnoses were respiratory distress syndrome, prematurity, and sepsis (see Table 1).
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

I06 B. Husfines and M. C. Logsdon
Table 1. Characteristics of skin breakdown positive (SB+) and skin breakdown negative (SB-) subjects
Characteristic SB+
( n = 6) SB-
(n = 26)
Age (weeks) M i SD 29.42 f 2.66 33.90 f 3.80 Range 27-34 24-40
Weight (grams) M f SD 1,448 f 528.98 2,030 f 703.64 Range 937-2,390 825-3,565
Gender
Female Male
Caucasian Black
Diagnosis Prematurity RDS Sepsis CA Fetal distress IUGR
Race
~~~
n YO n YO
2 33 15 58 4 67 1 1 42
6 100 21 81 0 0 5 19
4 67 8 31 2 33 12 46 0 0 3 12 0 0 1 4 0 0 1 4 0 0 1 4
Note. RDS = respiratory distress syndrome; CA = congenital anomaly; IUGR = intrauterine growth retardation.
Procedure
Bergstrom et al. (1987) described the procedure for conducting a clinical trial to test the predictive validity of an assessment tool. It is necessary to have a clear definition of the outcome to be measured and two people conducting assessments who are blind to each other’s scores. We fol- lowed this procedure in the present study.
Barbara Huffines and the nurse providing primary care to the neonate separately rated each neonate by means of the NSRAS within 24 hr post- delivery. Approximately 30 neonatal nurses received inservice education on the use of the instrument from Huffines before study participation. The rating scales completed by the neonatal nurses were placed in sealed envelopes and given to Huffines, who remained blind to the score as- signed by the neonatal nurse and the identity of the individual nurse to
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

Predicting Skin Breakdown in Neonates 107
prevent bias. Skin assessments were performed at the beginning of the study and every day for 7 days, then weekly for 2 months or until dis- charge or skin breakdown.
Instruments
We used two instruments to collect data in this study: a demographic data sheet and the NSRAS. The demographic data tool recorded charac- teristics that may influence the results of the study, such as the gesta- tional age at birth, weight at birth, sex, and diagnosis.
The NSRAS is a population-specific numerical scale developed to pro- vide nurses with an objective and quick estimate of immature skin integ- rity. The NSRAS is based on the Braden Scale for Predicting Pressure Sore Risk (Braden & Bergstrom, 1994) and is composed of six subscales: General Physical Condition, Mental State, Mobility, Activity, Nutrition, and Moisture. All subscales are rated on a scale ranging from 1 to 4, and each rating is operationalized by criteria for rating. Potential scores range from 6 to 24, with higher scores indicating lower levels of risk. During development of the scale, no level was specified at which neonates were deemed at risk of skin breakdown. The scale was used in addition to regular standards of care provided each neonate in the neonatal intensive care unit.
Content validity of the instrument was assessed by input from staff neonatal nurses, clinical nurse specialists, enterostomal nurses, nurse re- searchers, neonatal nurse practitioners, dermatologists, and neonatologists. The purpose of the NSRAS is to lend objectivity to the bedside nurses’ assessment in identifying neonates at high risk for skin breakdown.
Interrater Reliability
We calculated interrater reliability coefficients on each pair of ratings, for each subscale, and for each day until Day 21 (see Table 2). This date was chosen because of the small number of participants after Day 14, no skin breakdown after Day 14, and the maturation of neonate’s skin after 21 days.
As there were low reliability coefficients on the Mental State, Mobil- ity, and Moisture subscales, they were deleted for this pilot study. The remaining subscales, General Physical Condition, Activity, and Nutrition, were tested for interrater reliability and internal consistency. An analysis of variance for the General Physical Condition, Activity, and Nutrition subscales indicated that they were not significantly different across scales, F(2,14) = 0.439, p = .653, and across Days 1-7, F(7,14) = 2.028, p = .123 The interrater reliability for the three subscales and two examiners across 14 days was very high (r = .97).
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

I08 B. Htifines and M. C. Logsdon
Table 2. Interrater reliability coefficients scale
Subscale I 2 3 4 5 6 7 14 21
Genpc .91* .91* .88* .96* .89* .93* .95* .94* .95*
Mobil .09 .I8 .20 .30 -.04 .08 -.I9 .31 1.00 Act .SO* .93* 1.00* .91* 1.00* 1.00* .90* 1.00* 1.00* Nutr .77 .96* .99* .95* .93* .97* .93* .89* .86*
Ment .40 . I 1 .43 .57 .I6 .04 -. 14 .02
Moist .I1 -.I2 - - -.I6 - -.27 - -.05
n 31 32 32 32 32 31 32 23 1 1
Note. Genpc = General Physical Condition; Ment = Mental State; Mobii = Mobility; Act =
*p .05. Activity; Nutr = Nutrition; Moist = Moisture.
RESULTS
Six (1 9%) of the 32 neonates developed skin breakdown during the ob- servation period. There were no differences between gender, race, and diagnosis in those who did and those who did not develop skin break- down. However, age and weight did show a difference between those who did and those who did not develop skin breakdown. The mean ges- tational age at birth of those developing skin breakdown was 29.4 weeks (SO = 2.6 weeks) versus 33.9 weeks (SD = 3.8 weeks) for those not developing skin breakdown. The body weight of neonates with skin break- down was lower ( M = 1,448 g, SD = 529 g) than the weight of neonates without skin breakdown (M= 2,030 g, SD = 704 g).
Although results of a multivariate analysis of variance indicated that the NSRAS was significantly different across Days 1-7,1;(6,186) = 23.65, p = .OOO, the post hoc Tukey tests did not reveal any differences between the ratings (critical differences = .17). We chose the post hoc Tukey test because it allowed comparisons among all possible combinations of the subscales and maintained an error rate at 5%. This led to an attempt to determine if a particular day of life was associated with increased risk of skin break down in the neonate.
The participants were divided into those who developed skin break- down and those who did not, and the means were calculated from the NSRAS scores for Days 1-7 and Day 14. There were significant differ- ences by T tests in the NSRAS scores of participants who developed skin breakdown and those who did not for Days 1 and 2. Differences in scores for Day 14 were marginally significant (see Table 3).
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

Predicting Skin Breakdown in Neonates 109
Table 3. Neonatal Skin Risk Assessment Scale scores by skin breakdown
Score
N I 2 3 4 5 6 7 8
No breakdown 26 6.27 7.12 7.31 7.69 8.08 6.27 8.50 9.53 Skin breakdown 6 4.69 4.50 5.83 6.83 7.00 7.00 7.33 6.75 t value 3.37 4.22 1.15 .76 .97 1.13 1.10 3.58 Two-tailed p .004* .0001* ,291 .469 .362 .291 ,305 .010
n 32 32 32 32 32 32 32 23
Note. On Day 14, the n for no was 19 and the n for yes was 4. Using Bonferroni correction, a p value of .006 was used to claim significance.
We calculated sensitivity, specificity, percentage of predictive value of positive scores, and percentage of predictive value of negative scores for each possible score on the NSRAS. These terms are explained in the following paragraphs.
Sensitivity of a test is the extent to which a true characteristic is clas- sified correctly, thus identifying the majority of individuals with the char- acteristic, or the rate of “true positives” (Larson, 1986). In testing the NSRAS, sensitivity referred to those with skin breakdown whose scores were equal to or less than cut-off. SpecificiQ of a test is the extent to which the absence of a characteristic is correctly classified, thus correctly identifjling individuals who are free of a given characteristic, or the rate of “true negatives” (Larson, 1986). In testing the NSRAS, specificity was those without skin breakdown whose scores were greater than the cut-off. Together, sensitivity and specificity were used to measure the validity of a test. However, one must remember that because sensitivity and speci- ficity are inversely related, increasing the sensitivity of a test by lowering the point at which a test is considered positive (the cut-off point) de- creases the specificity of the test, and vice versa. In determining where to set a cut-off point for any test, one must consider the effects, both emo- tional and financial, of a false positive result; prevalence of the condition; and the implications of missing a diagnosis.
The predictive value of a positive test is the probability that when a test is positive, the characteristic is truly present (Larson, 1986). In test- ing the NSRAS, predictive value of a positive test was those scores equal to, or less than, the cut-off in which the neonate has skin breakdown. The predictive value of a negative test is the probability that when the test is negative, the characteristic is truly absent (Larson, 1986). In testing the NSRAS, predictive value of a negative test was those with scores higher
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

110 B. Huffnes and M. C. Logsdon
Table 4. Test of validity of Neonatal Skin Risk Assessment Scale for each possible score: Day 2
~~
YO Predictive % Predictive Score Sensitivity Specificity value of + value of -
3 4 5" 6 7 8 9
10 1 1
. I7
.50
.83 1 .oo 1 .oo 1 .oo I .oo 1 .oo 1 .oo
.88
.85
.81
.61
.42
.35
.I5
.04
.oo
.25
.43
.50
.38
.29
.26
.2 1
.I9
.I9
.82
.88 35"
1 .oo I .oo 1 .oo 1 .oo 1 .oo I .oo
Tritical cut-off point for this clinical study.
than the cut-off in which the neonate does not have skin breakdown. Therefore, predictive value as well as sensitivity and specificity must be considered when evaluating the clinical usefulness of a test. A critical cut-off score of 5 on the NSRAS was determined to indicate risk of skin breakdown. At a score of 5, the instrument was 83% sensitive and 81% specific, with 50% predictive value of positive scores and 95% predictive value of negative scores (see Table 4).
The NSRAS is composed of six subscales that reflect the critical determi- nants of skin breakdown. These six subscales reflect factors that identify the amount and duration of skin pressure (mental state, activity, and mobil- ity) and the tolerance of skin and its supporting structures for skin break- down (general physical condition, moisture, and nutrition). The Braden scale, on which the NSRAS is based, also has six subscales to predict pressure sores in the adult population. However, these two scales are different owing to their specific populations and the need to include levels of skin development in the neonate.
Together, three of the six subscales on the NSRAS were found to have high specificity and sensitivity in predicting skin breakdown in hospital- ized neonates: General Physical Condition, Activity, and Nutrition. Low reliability coefficients resulted in the deletion of the Mental State, Mobil- ity, and Moisture subscales. These three deleted subscales reflect factors considered by experts to be essential components in determining the po- tential for skin breakdown in the neonate, as they assess the neonate's
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

Predicting Skin Breakdown in Neonates 111
ability to move and respond and the fiequency of being moist. Therefore, continued use of the total instrument is recommended.
The three deleted subscales need further clarification in the operational definitions corresponding to each number on the scale. This process should increase interrater reliability in future studies.
Further work with the NSRAS with other populations needs to include the deleted subscales. The relevant role of friction may also be con- sidered. In addition, data collected in further studies should include therapies and devices that make positioning changes difficult Extracorpo- real Membrane Oxygenation (ECMO), ventilators, total parenteral nutri- tion, and number of probes and monitors attached to the skin.
In conclusion, accurate prediction of risk for skin breakdown allows at-risk neonates to benefit from nursing interventions and equipment while decreasing costs of nursing time and equipment charges to those who are less vulnerable. In an age of decreasing health care dollars and earlier discharges of hospitalized neonates, prevention measures and using less money are appealing.
REFERENCES
Barnes, D., & Payton, R. G. (1994). Clinical application of the Braden Scale in the acute-care setting. Dermatology Nursing, 5(5), 386-388.
Bergstrom, N., Demuth, P., & Braden, B. (1987). A clinical trial of the Braden Scale for Predicting Pressure Sore Risk. Nursing Clinics of North America, 22(2), 417-428.
Braden, B., & Bergstrom, N. (1994). Predictive validity of the Braden Scale for pressure sore risk in a nursing home population. Research in Nursing and Health, I7(6), 459- 470.
Doyle, L., & Sinclair, J. C. (1982). Insensible water loss in newborn infants. Clinics in Perinatology, 9(3), 453-482.
Gawron, C. L. (1994). Risk factors for and prevalence of pressure ulcers among hospi- talized patients. Journal of Wound-Ostomy-Continence Nursing, 21(6), 232-240.
Harpin, V. A., & Rutter, N. (1983). Barrier properties of the newborn’s skin. Journal of Pediatrics, 102(3), 419-425.
Holbrook, K. A. (1982). A histological comparison of infant and adult skin. In H. Maiback & E. Boisitis (Eds.), Neonatal skin: Structure and function (pp. 3-3 I) . New York: Marcel Decker.
Hosimoto, K. (1966). The ultrastructure of skin of human embryos, IV. The epidermis. Journal of Investigative Dermatology, 47, 3 17.
Huffines, B., & Logsdon, M. C. (1995). The elements associated with skin impairment of the hospitalized neonate. DOINGS, 20, 7-9.
Jackson, H., & Sutherland, R. (1981). Effect of providone-iodine on neonatal thyroid function. The Lancet, 2, 992.
Kuller, J. (1984). Part I: Skin development and function. Neonatal Network, 3(3), 18-23. Kuller, J., Lund, C., & Tobin, C. (1983). Improved skin care for premature infants.
Maternal Child Nursing, 8, 200-203.
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

I 12 B. Hufines and M. C. Logsdon
Larson, E. (1986). Evaluating validity of screening tests. Nursing Research, 35, 186-
LeFrak, L. (1984). Nutrition and its effects on the skin. Neonatal Network, 3(3), 3 6 3 9 . Lund, C., Kuller, J., Tobin, C., LeFrak, L., & Franck, L. (1986). Evaluation of a pectin-
based barrier under tape to protect neonatal skin. Journal of Obstetric. Gynecological and Neonatal Nursing, IS(]), 39-44.
McManus, J. (1981). Skin care in the intensive care nursery. Neonatal Network, I(]), 2- 5.
O’Leary, M. J. (1983). Nutrition and fluid administration. In W. A. Hodson & W. E. Truog (Eds.), Critical care of the newborn (p. 32). Philadelphia: W . B. Saunders.
Quigley, S. M., & Curley, M. A. Q. (1996). Skin integrity in the pediatric population: Preventing and managing pressure ulcers. Journal of the Society of Pediatric Nurses,
Rasmussen, J. (1987). The skin: Structure, function, and percutaneous absorption. In V. C. Kelley (Ed.), Practice of pediatrics (pp. 1-6). Philadelphia: Harper & Row.
Rutter, N. (1987). Percutaneous drug absorption in the newborn: Hazards and uses. Clinics in Perinatology, 14(4), 91 1-930.
West, D., Worobec, S., & Solomon, L. (1981). Pharmacology toxicology of infant skin. The Journal of Investigative Dermatology, 76, 147-1 50.
Xakellis, G . C., Frantz, R. A,, Arteaga, M., Njuyen, M., & Lewis, A. (1992). A com- parison of patient risk for pressure ulcer development with nursing use of preventive interventions. Journal of the American Geriatric Society, 40( 12), 1250-1254.
188.
I, 7-18.
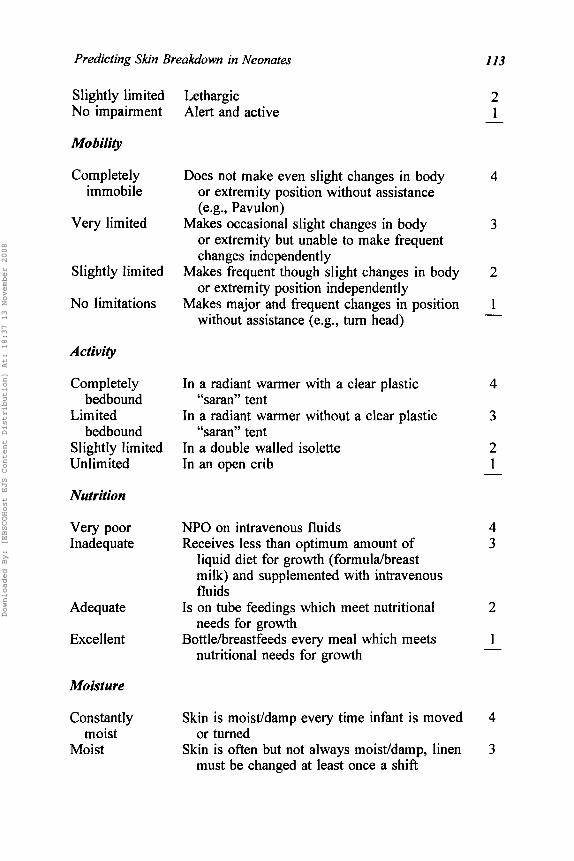
Appendix A Neonatal Skin Risk Assessment Scale (NSRAS)
CLINICAL CONDITION PARAMETERS
General Physical Condition
Very poor Gestational age I 2 8 weeks 4 Gestational age > 28 weeks but 5 33 weeks Gestational age > 33 weeks but I 3 8 weeks
3 2 1 - Gestational age > 38 weeks to postterm
Mental State
Completely Unresponsive (does not flinch, grasp, moan, 4 limited increase blood pressure, or heart rate) to
painful stimuli due to diminished level of consciousness or sedation
moans, increased blood pressure, or heart rate) Very limited Responds only to painful stimuli (flinches, grasps, 3
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008
Predicting Skin Breakdown in Neonates 113
Slightly limited No impairment
MobiIity
Completely immobile
Very limited
Slightly limited
No limitations
Activity
Completely bedbound
Limited bedbound
Slightly limited Unlimited
Nutrition
Very poor Inadequate
Adequate
Excellent
Moisture
Constantly moist
Moist
Lethargic Alert and active
Does not make even slight changes in body or extremity position without assistance (e.g., Pavulon)
or extremity but unable to make frequent changes independently
Makes frequent though slight changes in body or extremity position independently
Makes major and frequent changes in position without assistance (e.g., turn head)
Makes occasional slight changes in body
In a radiant warmer with a clear plastic “saran” tent
In a radiant warmer without a clear plastic “saran” tent
In a double walled isolette In an open crib
NPO on intravenous fluids Receives less than optimum amount of
liquid diet for growth (formulahreast milk) and supplemented with intravenous fluids
needs for growth
nutritional needs for growth
Is on tube feedings which meet nutritional
Bottlehreastfeeds every meal which meets
Skin is moistldamp every time infant is moved
Skin is often but not always moisddamp, linen or turned
must be changed at least once a shift
2 1 -
4
3
2
1
4
3
2 1
4 3
2
1
4
3
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008

114 B. Huffines and M. C. Logsdon
Occasionally Skin is occasionally moist/damp, requiring 2 moist an extra linen change approximately once
a day Skin is usually dry, linen requires changing
only every 24 hours 1 - Rarely moist
TOTAL -
DIRECTIONS
Under each clinical condition parameter, circle the numerical value that best describes your infant.
Downloaded By: [EBSCOHost EJS Content Distribution] At: 18:37 13 November 2008