is cost benefit analysis making us sick?
TRANSCRIPT

Is cost-benefit analysis making us sick? Issues in evaluation of active transport projects and
transport investment health impacts
Dr. Cameron GordonAdjunct Associate Professor (Transport Economics)
Centre for Research and Action in Public Health (CeRAPH)Health Research Institute
University of Canberra (Australia)
Visiting ScholarTRANSyT Centre
Polytechnic University of Madrid
Principal InvestigatorCity University of New York
Social Policy Simulation Center

One economist´s research agenda
Active transport
Health
Evaluation methods
Specific adjustments to CBA to more accurately account for
health, active mode choice
Broader co-benefits of
transit investments
´Rapid Review´ and other policy
analysis modes
Re-think and reconceptualise
health and active transport
evaluation methods and
ideas
Presentation motivation and overview
1. Premise: Existing CBA project evaluations are biased when it comes to active transport and transport and health projects
2. Task: interrogate the first principles of transport project economic evaluation
3. A brief review of the assumptions of welfare economics Transport economics Cost-benefit analysis (CBA) 4 step model and generalised cost
4. ‘Complications´- Health: morbidity and mortality- Active transport: non-neutral mode choice/shift5. Modifications and augmentations of CBA6. To CBA or not to CBA: An analytical decision tree 7. A methodological ´ecosystem´?
Welfare Economics assumptions
• Welfare economics: 'optimal' allocation of scarce resources
• Assume: atomistic, disembodied, rational, maximising agents each with individual utility functions. Utility=satisfaction= ´welfare´
• Basic task of each agent: Max U s.t. budget constraint (scarcity)
• Market mechanism: individuals consuming, producing and transacting to achieve maximum valued output through the price mechanism (P=MC is the optimum condition)
• The market thus delivers maximum welfare given scarce resources (measured by consumer and producer surplus i.e. total net utility)
• Or in marginal terms: P=MC=MU

Transport economics • Introduce: physical space and ´friction´of need
to travel (transport) across that space• Travel is a ´bad´(cost) to be minimised by whatever
means possible (e.g. location, mode etc).• Minimise generalised costs:• G = p + u(w), where p is monetary costs of travel,
u(w) is utility costs of travel, w being level of service of the transport network.
• In the simplest world u(w) = travel time.• Agents now make choices to minimise g while
maximising u. • Much effort goes into modelling these choices
(choice modelling)

The 4-step modelBecause travel is a 'derived demand', demand for travel must be estimated indirectly. A typical approach begins with specification of spatial travel zones with (generally) households producing trips, employers attracting trips and together creating initial travel demand overlaid with a transport network that represents travel supply. Final travel demand is predicted using these 4 steps:
– (1) trip generation (each zone generates trips by purpose)
– (2) trip distribution (a potential flow of trips across the given network is estimated given the relative ´attractiveness´ of each zone)
– (3) mode choice (traveller choose their desired travel mode to minimise their generalised costs)
– (4) trip assignment (actual paths taken across the network are generated).

Transport cost-benefit analysis • Cost-benefit analysis (CBA) is an application of welfare
economics while transport CBA adds transport economics principles including (typically) the 4 step model.
• Given market imperfections (e.g. public goods) there may be a need for nonmarket interventions (CBA refers to these as ´projects´).
• A procedure is needed to determine whether ´projects´improve or decrease net ´welfare´.
• This is what CBA is. It measures all ´benefits´ (U +) against all ´costs´(U -) to determine the net gain/loss of U due to the project.
• U – projects are rejected, U + projects provisionally accepted.
• Societal welfare (utility) without project (´before´condition or ´baseline´)
• Societal welfare (utility) with project (´after´condition)
U without projectU with project
U WITHOUTU WITH minus
U NET GAIN/LOSS
equals

Consumer Sovereignty• Welfare economics and CBA put individual
consumer satisfaction in pride of place.• The ethical ground of CBA is utilitarian
individualism which rests on individual subjective experience and its ethical standard for judging intervention outcomes is consumer sovereignty.
• This is an ethics based on extrinsic outcomes not intrinsic standards.
• This flows straight from the measure of social welfare as being the sum of total individual utility (satisfaction) maximisation.
Note on ´household production´
• Current approaches to transport economics are heavily influenced by the ´household production´ models of Mincer and Becker.
• In this world utility maximising agents have a ´time budget´ and a set of activities they wish to pursue, each of which takes time and must fit into this budget.
• Activity based travel models use this as their basis, with travel as one of the activities that the household time-budget must accomodate.
• Conceptually, though, this approach also is derived from transport economics which is drawn from welfare economics and has the same basic assumptions about human behaviour and ethical ground of utility maximisation.

Complication #1: human health
• Welfare economics implicitly assumes immortal agents in disembodied form (or at least irrelevancy of individual mortality).
• When we relax these assumptions we come to the need to account for human mortality (life expectancy, and reductions and increases in that life expectancy) and human morbidity (the occurrence of disease).
•

Energy expenditure, transport, and health
• Because human beings have a specific form, physiology now becomes an important thing to study.
• “Physical activity” is a broad term that refers to any form of muscular movement that produces energy expenditure.
• It is the energy expenditure that yields the health benefit generally (i.e. reduced mortality and morbidity).
• The traditional CBA/welfare economics/transport economics paradigm does not account for this and it is important because now the basic rule of more activity = more energy expenditure = less mortality/morbidity (within some limit of course) and to the extent transport involves energy expenditure it is not a uniform 'bad'.

Non-neutral travel mode and travel choice
• Because of this link between human health and energy expenditure, two things formerly 'neutral' in all but an economic sense are now no longer so:
• Choice to travel or not• Choice of mode of travel• CBA can add health impacts as
individual 'benefits' but theoretically this is actually ad hoc.
Consumers no longer fully sovereign
• Another aspect that health introduces into CBA is the notion of individual choice.
• It is well known that built environment and the existing transport network heavily affect travel and mode choice decisions. In other words, choice is not fully 'free' in an individual sense.
• This may not be too much of an issue if economics is the only concern since so long as travel costs are minimised then consumption and utility are maximised.
• But with health this issue is no longer so simple since minimum travel time modes may reduce health and hence utility even the environment may be driving consumers towards suboptimal choices.
• This can be treated as an 'externality' but this seems to be more of a tension in the consumer choice model used.

'Objective' v 'subjective' risk• Epidemiologists focus on ´relative risk´ which is
the ratio of the probability of an event occurring in an exposed group (e.g. being injured) to the probability of the event occurring in a non-exposed group (a control group) which ideally is identical in all respects except for the exposure (which could be a treatment or intervention).
• However CBA puts subjective experience in a central position because this is what drives utility.
• What happens when the two clash, as they often do? Risk generally is something that is usually not treated very carefully and often not this empirically in most CBAs.
Ethical conundrums• CBA has an implicit ethical standard of
utilitarianism and all its valuation standards derive from this. It is fundamentally extrinsic in nature.
• Medical and health ethics stand in contrast to this. No one standard is used but clearly at least some of the relevant standards used are intrinsic in nature recognising a fundamental value of life and a fundamental right to care.
• CBA does not inherently recognise this and it must be introduced, not always easily.

Complication (2): ´active´ transport• Directly following from the reality of human form and
health is ´active´ transport, i.e. cycling and walking (and other modes, generally insignificant, such as rollerblading).
• Transport economics compares mode choice simply along relative generalised costs. Otherwise mode choice is ´neutral´.
• ´Active´transport has implications for mortality and morbidity and is are not neutral with respect to inactive modes. In other words, the form of mode does matter.
• It raises the question of whether and how CBA may need to be adjusted to account for this (and whether the obvious eonomist´s answer of putting those impacts into the generalised cost function is sufficient).

Transport may be a ´good´ A more subtle issue related to
form is whether travel is always a ´bad´ (i.e. utility reducing) as opposed to sometimes a ´good´ (i.e. utility increasing).
In other words, travel may possibly at times be an end in itself or, if used for a particular purpose, some forms may be more desirable from a utility point of view. (This discussion can apply to automobile and other ´inactive´ transport as well but the greater mode choice implications appear to be present for active modes.)
Source: https://vimeo.com/74324675

More travel time is better than less● This fact upends, at least in part, the
fundamental primacy of VTTS (Value of Travel Time Saved) as a core benefit, especially for active transport investments.
● Since subjective experience is the core valuation standard of CBA what are we to make of the possibility that some cyclists and walkers prefer more time spent in those modes rather than less, at least at times?
● “Average” values will no longer wash since for some users in some instances the sign will be wrong, i.e. travel time having a positive rather than negative utility value.

Mixing up the four steps• Active transport may also 'mix up' our traditional four
step model.● This model assumes independence of (1) trip
generation (each zone generates trips by purpose) from (3) mode choice (traveler choose their desired travel mode to minimise their generalised costs).
● But with active modes, mode choice is no longer neutral from either a health or a utility perspective and so (1) and (3) are jointly decided.
● If this is so then (2) trip distribution (a potential flow of trips across the given network is estimated given the relative ´attractiveness´ of each zone) and (4) trip assignment (actual paths taken across the network are generated) are no longer purely discrete either.
● And, in fact, these two may have interdependency with subjective utility driven by subjective experience.

What to do (analytically)?• We now come to a point where one has to ask: should
transport project evaluations change to properly:• (1) account for health impacts of transport• (2) assess active versus inactive transport modes• If so, how? • Conceptually I argue that we must ask ourselves a
number of ´first principle´questions in terms of method choice and application.
• It should not be assumed that CBA can accomodate these dimensions under all circumstances. In many cases they may need to be modified, sometimes fundamentally.
• In other cases we may have to discard CBA altogether.

• Adjust existing benefit and cost categories for health/active transport factors (e.g. adjust generalised cost parameters)
• Add new benefit and cost categories specific to health and active transport
• Do customised/specialised results report (applies to either above)
CBA adjustments in order of deviation from neoclassical paradigm (on-
model)

CBA 'On-model' adjustments continued
• Do detailed separate analyses for health, epidemiological impacts etc.
• Modify the CBA assumptions, e.g. modified utility maximisation according to behavioural economics
• Don´t monetise benefits and costs – provide only impacts.
• Incorporate more inductive measures into the CBA costs and benefits, especially epidemiology findings
'Off-model' adjustments
• Alter 4-step analysis (especially for mode choice step) – e.g. use finer grain zones (e.g. PAZ etc).
• Collect better data• Use alternative travel demand models,
e.g. modified activity based models (this is suggested by Challis et. al. And NCHRP 2006)

Reasons to reconsider the neoclassical paradigm• Economists will say that existing CBA and neoclassical
concepts, can incorporate all health dimensions and thus CBA, however modified, should be used for any project evaluation.
• However these significant and unresolved philosophical tensions between health and transport and a purely economic approach may in some cases be too great.
• Subjective versus objective/relative risk – utility maximisation holds that subjective risk is most important but public health often dictates the use of objective relative risk. It is not entirely clear that this can be handled by ´simple´tweaks to parameters.
• Complexity of health as a phenomenon, both subjectively and objectively – in some cases the health cause-effect of interventions and subjective experiences of health impacts that drive the pure consumer surplus/gain concept may not mesh.
• Ethical grounding – CBA is implicitly utilitarian in its ethics (a fact often ignored). Therefore only ´use´ value is important. But health may not sit well in this framework. Indeed, many of the debates about ´value of life´ effectively revolve around this tension. (And recall the Hippocratic Oath which is more a Kantian than a utilitarian imperative)
• Valuation difficulties – CBA requires an economic price to arrive at an economic valuation. This may be problematic for some health impacts.
• Non-neutrality of modes and shifts from ´goods´ to ´bads´and back: Relatively poorly understood is the relationship between modes of travel and travel as a good versus a bad, i.e. desirable in and of itself. It is possible that this is a fundamental contradiction that mere parameter adjustment may not deal with adequately.

A decision tree of analytical alternatives:Here is a framework of method choice in the
presence of health impacts and/or active transport
Use a Unified
approach
Use neoclassical
welfare paradigm
Use CBA
Add health/active transport benefit and
cost categories
Yes Yes
Do auxiliary analyses
e.g. entity financial, equity, HIA etc.
Use modified economic paradigm
(e.g. behavioural economics)
Use noneconomic
paradigm (e.g. inductive
framework, epidemiologic
al etc.)
No
No
Do conceptually separate analyses for separate dimensions and do not
´allow´ comparisons across types (e.g. economic
impacts to health impacts)
Do customised
results reporting or
more ´meaningful
´ metrics
Could add…
Could add…
Adjust 4-step model and generalised
costs

Choice 1: stick with neoclassical economics and CBA
Use a Unified
approach
Use neoclassical
welfare paradigm
Use CBA
Add health/active
transport benefit and
cost categoriesYes Yes
Do auxiliary analyses
e.g. entity financial, equity, HIA etc.
Use modified economic paradigm
(e.g. behavioural economics)
Do customised
results reporting or
more ´meaningful
´ metrics
Adjust 4-step model
and generalised
costs
• The most common current response of analysts when confronted with health impacts is to stick with the CBA and its attendant neoclassical welfare economics assumptions and just modify it accordingly.
• This is where most of the academic effort and policy attention is focused currently, probably because CBA is so widely accepted and often required for government programs.

A hierarchy of analytic choices
Use a Unified
approach
Use neoclassical welfare paradigm
Use CBA
Add health/active
transport benefit and
cost categoriesYes Yes
Do auxiliary analyses
e.g. entity financial, equity, HIA etc.
Use modified economic paradigm
(e.g. behavioural economics)
Do customised
results reporting or
more ´meaningful
´ metrics
Adjust 4-step model
and generalised
costs
Adjustments to CBA can be ´on model´ and ´off model´. In other words one can adjust the CBA directly and/or one can adjust the detailed inputs into the model through modifications in other models such as the 4-step travel demand model.Adjustments can also stick very closely to the neoclassical economics/transport paradigm or stray from it a bit while remaining reliant on its basic assumptions.

Choice 2: stick with a unified approach but discard the neoclassical paradigm
Use a Unified
approach
Use neoclassical
welfare paradigm
Yes
Use noneconomic
paradigm (e.g.
inductive framework,
epidemiological etc.)
No
Do customised results
reporting or more
´meaningful´ metrics
Could add…
• Another alternative is to discard the neoclassical paradigm altogether.
• A ´radical´ possibility is to put health, or at least physical impacts, first analytically, and focus on those exclusively or primarily.
• Some environmentalists have argued for this in that domain.
• This sort of approach is more inductive and ethically sits in a different realm than the neoclassical paradigm, using intrinsic value rather than consumer use value.
• This obviously sits at odds with current practice and has the disadvantage that impacts of different sorts cannot be added up and compared with one another as is possible with CBA.
Use a Unified
approach
No
Do conceptually separate analyses for separate dimensions and do not
´allow´ comparisons across types (e.g. economic
impacts to health impacts)
Do customised results
reporting or more
´meaningful´ metrics
Could add…
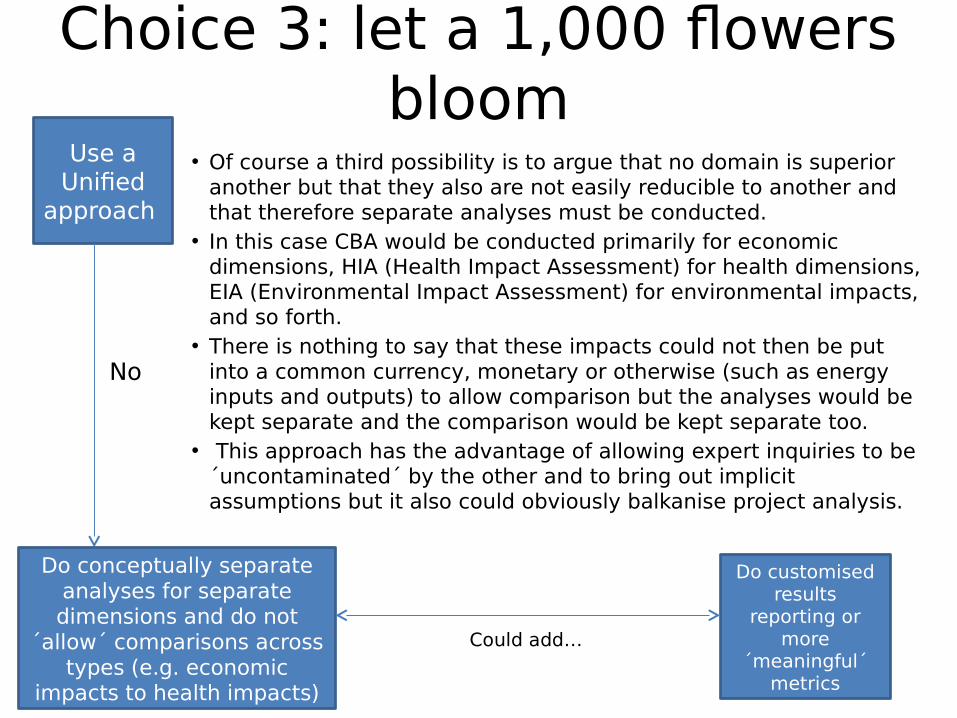
Choice 3: let a 1,000 flowers bloom
• Of course a third possibility is to argue that no domain is superior another but that they also are not easily reducible to another and that therefore separate analyses must be conducted.
• In this case CBA would be conducted primarily for economic dimensions, HIA (Health Impact Assessment) for health dimensions, EIA (Environmental Impact Assessment) for environmental impacts, and so forth.
• There is nothing to say that these impacts could not then be put into a common currency, monetary or otherwise (such as energy inputs and outputs) to allow comparison but the analyses would be kept separate and the comparison would be kept separate too.
• This approach has the advantage of allowing expert inquiries to be ´uncontaminated´ by the other and to bring out implicit assumptions but it also could obviously balkanise project analysis.

An ´ecosystem´ of approaches?
• Of course these branches need not be mutually exclusive for all domains.
• Indeed, it is probably true that traditional CBA works well for some projects in some domains (e.g. road expansions) which can be adapted with relative ease to account for noneconomic impacts with relative ease but that alternatives are needed for other projects in other domains.
• Health and active transport would seem to be one of those domains.
• Some more ´biodiversity´in the project evaluation world is likely in order. (This is what Challis et. al. argue for)
• And perhaps one should not assume CBA to be the best alternative for active transport projects. It may be, but one should not assume it to be.

ReferencesAlberini, A., Cropper, M., Krupnick, A., & Simon, N. B. (2004). Does the value of a statistical life vary with age and health status? Evidence from the US and Canada. Journal of Environmental Economics and Management, 48(1), 769-792.Berrigan, D., Pickle, L. W., & Dill, J. (2010). Associations between street connectivity and active transportation. Int J Health Geogr, 9(1).Blomquist, G. C. (2004). Self-protection and averting behavior, values of statistical lives, and benefit cost analysis of environmental policy. Review of Economics of the Household, 2(1), 89-110.Bom, P. R., & Ligthart, J. E. (2009). What have we learned from three decades of research on the productivity of public capital?. Journal of Economic Surveys, 28(5), 889-916.Button, K. (2010, October). Transportation economics: Some developments over the past 30 years. In Journal of the Transportation Research Forum (Vol. 45, No. 2).Cavill, N., Kahlmeier, S., Rutter, H., Racioppi, F., & Oja, P. (2008). Economic analyses of transport infrastructure and policies including health effects related to cycling and walking: a systematic review. Transport policy, 15(5), 291-304.De Blaeij, A., Florax, R. J., Rietveld, P., & Verhoef, E. (2003). The value of statistical life in road safety: a meta-analysis. Accident Analysis & Prevention, 35(6), 973-986.Ellison, R., & Greaves, S. (2011). Travel time competitiveness of cycling in Sydney, Australia. Transportation Research Record: Journal of the Transportation Research Board, (2247), 99-108.Elvik, R. (2000). Which are the relevant costs and benefits of road safety measures designed for pedestrians and cyclists?. Accident Analysis & Prevention, 32(1), 37-45.European Commission: SafetyNet (2009). Cost-benefit analysis. http://ec.europa.eu/transport/road_safety/specialist/knowledge/pdf/cost_benefit_analysis.pdf retrieved 18 June 2015.Frank, L. D., Sallis, J. F., Conway, T. L., Chapman, J. E., Saelens, B. E., & Bachman, W. (2006). Many pathways from land use to health: associations between neighborhood walkability and active transportation, body mass index, and air quality. Journal of the American Planning Association, 72(1), 75-87.Giles-Corti, B., Foster, S., Shilton, T., & Falconer, R. (2010). The co-benefits for health of investing in active transportation. New South Wales public health bulletin, 21(6), 122-127.Gordon, C. (2015). Behavioural approaches to corporate governance. London: Routledge.Götschi, T., & Hintermann, B. (2014). Valuation of public investment to support bicycling. Swiss Society of Economics and Statistics 150 (4) 297-329. Graham, J. D., & Vaupel, J. W. (1981). The Value of a Life: What Difference Does It Make?. In Risk/Benefit Analysis in Water Resources Planning and Management (pp. 233-243). Springer US.Krag, T. (2005). Cost benefit analysis of cycling–Denmark. CBA of Cycling, Nordic Council of Ministers, Stockholm, Norway.Krizec, K. J. (2007). Estimating the economic benefits of bicycling and bicycle facilities: An interpretive review and proposed methods. In Essays on transport economics (pp. 219-248). Physica-Verlag HD.Litman, T. (1994). Bicycling and Transportation Demand Management. Transportation Research Record 1441, Transportation Research Board, 134-140.Litman, T. (2004). Economic value of walkability. World Transport Policy & Practice 10 (1)Mokhtarian, P., Salomon, I., Lothlorien, S (2001). Understanding the Demand for Travel: It's Not Purely 'Derived'. Innovation: The European Journal of Social Science Research 14 (4). McDonald, N. C. (2008). Critical factors for active transportation to school among low-income and minority students: evidence from the 2001 National Household Travel Survey. American journal of preventive medicine, 34(4), 341-344.McNally, M. (2007). The Four Step Model. Chapter 3, Handbook of Transport Modeling, Hensher, D., and Button. K, eds.. 2nd edition. (New York: Pergamon Press).Ministry of infrastructure and environment (Netherlands) (2012). Social costs and benefits of cycling – Summary. Prepared by Decisio.National Cooperative Highway Research Program (NCHRP) (1998). Travel estimation techniques for urban planning. NCHRP Report 365. Washington, DC: Transportation Research BoardNational Cooperative Highway Research Program (NCHRP) (2006). Guidelines for analysis of investments in bicycle facilities. NCHRP Report 552. Washington, DC: Transportation Research Board.National Cooperative Highway Research Program (NCHRP) (2014). Estimating bicycling and walking for planning and project development: a guidebook. NCHRP Report 770. Washington, DC: Transportation Research BoardOlds, Tim (2014). Australia vying to be world champion of inactivity. The Conversation. 21 September 2014. Reynolds, C. C., Harris, M. A., Teschke, K., Cripton, P. A., & Winters, M. (2009). The impact of transportation infrastructure on bicycling injuries and crashes: a review of the literature. Environmental Health, 8(47).Roads and Traffic Authority of NSW and the Department of Environment and Climate Change (2009). Evaluation of the costs and benefits to the community of financial investment in cycling programs and projects in New South Wales: Final Report. http://www.pcal.nsw.gov.au/__data/assets/pdf_file/0008/90899/Evaluation_of_NSW_cycling_study.pdf Sælensminde, K. (2004). Cost–benefit analyses of walking and cycling track networks taking into account insecurity, health effects and external costs of motorized traffic. Transportation Research Part A: Policy and Practice, 38(8), 593-606.Sallis, J. F., Frank, L. D., Saelens, B. E., & Kraft, M. K. (2004). Active transportation and physical activity: opportunities for collaboration on transportation and public health research. Transportation Research Part A: Policy and Practice, 38(4), 249-268.Scheepers, C. E., Wendel-Vos, G. C. W., den Broeder, J. M., van Kempen, E. E. M. M., van Wesemael, P. J. V., & Schuit, A. J. (2014). Shifting from car to active transport: A systematic review of the effectiveness of interventions. Transportation research part A: policy and practice, 70, 264-280.Stromberg, J (2014). Bike lanes have actually sped up car traffic in New York City. September 8, 2014. Vox.Viscusi, W. K., & Aldy, J. E. (2003). The value of a statistical life: a critical review of market estimates throughout the world. Journal of risk and uncertainty, 27(1), 5-76.Wang, G., Macera, C. A., Scudder-Soucie, B., Schmid, T., Pratt, M., & Buchner, D. (2004). Cost effectiveness of a bicycle/pedestrian trail development in health promotion. Preventive Medicine, 38(2), 237-242.Winters, M., Ries, F., & Gouge, B. (2010). Active transportation in urban areas: exploring health benefits and risks. National Collaborating Centre for Environmental Health.Yi, M., Feeney, K., Adams, D., Garcia, C. and Chandra, P. (2011). Valuing cycling – Evaluating the economic benefits of providing dedicated cycle ways at a strategic network level. Australasian Transport Research Forum 2011 Proceedings 28 - 30 September 2011, Adelaide, Australia. Publication website: http://www.patrec.org/atrf.aspxYounger, M., Morrow-Almeida, H. R., Vindigni, S. M., & Dannenberg, A. L. (2008). The built environment, climate change, and health: opportunities for co-benefits. American journal of preventive medicine, 35(5), 517-526.