irritable bowel syndrome dr john hamlin phd mrcp consultant gastroenterologist leeds general...
Post on 19-Dec-2015
222 views
TRANSCRIPT

Irritable Bowel Irritable Bowel SyndromeSyndrome
Dr John Hamlin PhD MRCPDr John Hamlin PhD MRCP
Consultant Consultant GastroenterologistGastroenterologist
Leeds General InfirmaryLeeds General Infirmary


Areas to cover:Areas to cover:
What is IBS?What is IBS? What are the typical symptoms?What are the typical symptoms? Taking a good historyTaking a good history What examination should the GP do?What examination should the GP do? What investigations should the GP do?What investigations should the GP do? Can it be diagnosed by the GP without a Ba Can it be diagnosed by the GP without a Ba
enema or without referral ie. On clinical enema or without referral ie. On clinical history?history?
Treatments – what are they / the evidence / Treatments – what are they / the evidence / what about probiotics and yoghurt type drinks?what about probiotics and yoghurt type drinks?

EpidemiologyEpidemiology
Diagnosis of exclusion vs. disease Diagnosis of exclusion vs. disease entityentity
Affects 10-25% of the population.Affects 10-25% of the population. 75% don’t seek medical care75% don’t seek medical care 50% of GI consults50% of GI consults 1/3 diarrhoea 1/3 constipation 1/3 1/3 diarrhoea 1/3 constipation 1/3
pain predominant symptompain predominant symptom 2:1 F:M (4:1 in secondary care)2:1 F:M (4:1 in secondary care) Oscillating courseOscillating course

Great effect on QOLGreat effect on QOL
Large drain on healthcare and Large drain on healthcare and economyeconomy
Accounts for 20% self certificationAccounts for 20% self certification
Av 14.8 sick days vs. 8.7 averageAv 14.8 sick days vs. 8.7 average
Illness seeking behaviour: 3-4 times Illness seeking behaviour: 3-4 times chance of abdominal surgerychance of abdominal surgery

Aetiology??Aetiology??
Visceral hypersensitivity. Decrease Visceral hypersensitivity. Decrease balloon distension thresholds on the colonballoon distension thresholds on the colon
(Ritchie GUT 1973) (Ritchie GUT 1973) Normal somatic pain thresholdsNormal somatic pain thresholds Not seen in non medical seeking IBSNot seen in non medical seeking IBS Altered motility (inconsistent results)Altered motility (inconsistent results) Psychological factors/central processingPsychological factors/central processing Post infectious (30% cases)Post infectious (30% cases) Food intolerancesFood intolerances

Visceral hyperalgesia Evidence of visceral hyperalgesia (increased
sensitivity to noxious stimuli in the gut) includes perception of pain from distention of a rectal balloon at smaller volumes than in normal patients
Post-infectious or post-antibiotic Onset of IBS after an episodes of enteritis or
antibiotics have been described. A meta-analysis found the prevalence of IBS to 9.8% after enteritis as compared to 1.2% in controls.
Food allergies and sensitivities

Bacterial overgrowthBacterial overgrowth
StressStress
HormonesHormones The role of hormones in IBS is not yet fully The role of hormones in IBS is not yet fully
understood. Menstruation frequently understood. Menstruation frequently triggers or exacerbates IBS symptoms, triggers or exacerbates IBS symptoms, while pregnancy and menopause can either while pregnancy and menopause can either worsen or improve symptoms. worsen or improve symptoms.

Defining the diseaseDefining the disease
No biological markersNo biological markers Reliant on grouping of symptom patternsReliant on grouping of symptom patterns Manning Criteria 1978Manning Criteria 1978 Rome Criteria 1988Rome Criteria 1988 Rome II 2000Rome II 2000 Study by Vanner et al. showed 100% Study by Vanner et al. showed 100%
PPV in a retrospective study and 98% in PPV in a retrospective study and 98% in a prospective study (Am J Gastro 1999)a prospective study (Am J Gastro 1999)

Areas to cover:Areas to cover:
What is IBS?What is IBS? What are the typical symptoms?What are the typical symptoms? Taking a good historyTaking a good history What examination should the GP do?What examination should the GP do? What investigations should the GP do?What investigations should the GP do? Can it be diagnosed by the GP without a Ba Can it be diagnosed by the GP without a Ba
enema or without referral ie. On clinical enema or without referral ie. On clinical history?history?
Treatments – what are they / the evidence / Treatments – what are they / the evidence / what about probiotics and yoghurt type drinks?what about probiotics and yoghurt type drinks?
Rome Criteria (1)Rome Criteria (1)
3 months of continuous or recurring 3 months of continuous or recurring symptoms of abdo pain or irritation that:symptoms of abdo pain or irritation that:
May be relieved with a bowel movementMay be relieved with a bowel movement
May be coupled with changed frequencyMay be coupled with changed frequency
May be coupled with changed May be coupled with changed consistencyconsistency
(2 out of 3 features) and……………(2 out of 3 features) and……………

Rome criteria (2)Rome criteria (2)
Two or more of the following are present Two or more of the following are present at least 25% of the time:at least 25% of the time:
1.1. A change in stool frequency (>3 day A change in stool frequency (>3 day <3 week <3 week
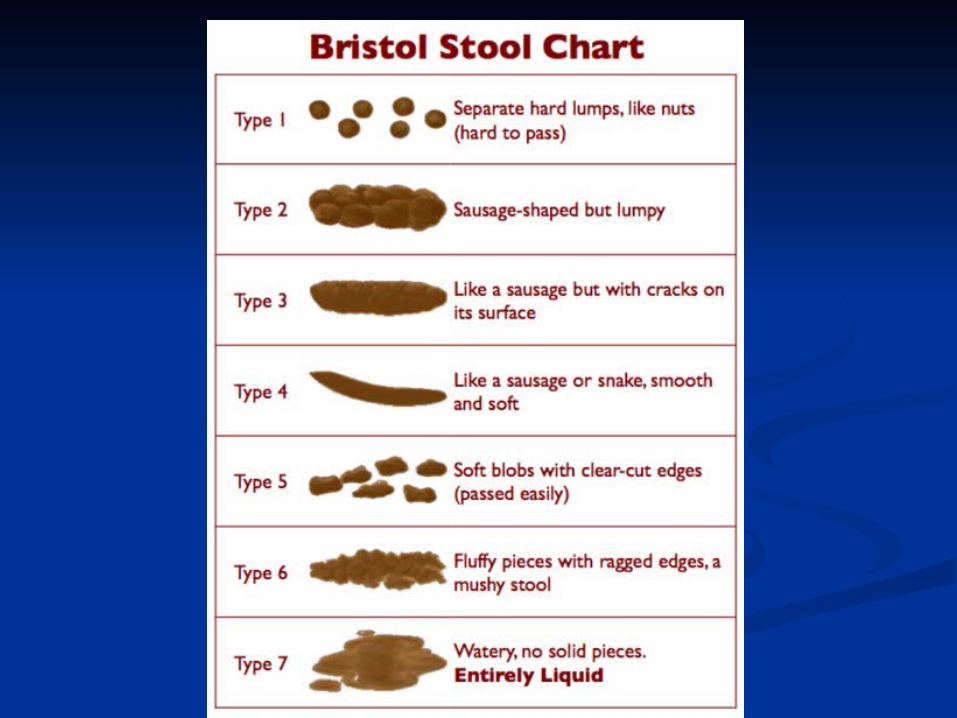
2.2. Noticeable difference in stool formNoticeable difference in stool form
3.3. Passage of mucous in stoolsPassage of mucous in stools
4.4. Bloating or feeling of abdo distensionBloating or feeling of abdo distension
5.5. Altered stool passage (tenesmus, Altered stool passage (tenesmus, straining)straining)

Supportive symptoms of Supportive symptoms of IBS:IBS:
A) Fewer than three bowel movements a week A) Fewer than three bowel movements a week B) More than three bowel movements a day B) More than three bowel movements a day C) Hard or lumpy stools C) Hard or lumpy stools D) Loose (mushy) or watery stools D) Loose (mushy) or watery stools E) Straining during a bowel movement E) Straining during a bowel movement F) Urgency (having to rush to have a bowel movement) F) Urgency (having to rush to have a bowel movement) G) Feeling of incomplete bowel movement G) Feeling of incomplete bowel movement H) Passing mucus (white material) during a bowel H) Passing mucus (white material) during a bowel
movement movement I) Abdominal fullness, bloating, or swellingI) Abdominal fullness, bloating, or swelling
Diarrhoea-predominantDiarrhoea-predominant: At least 1 of B, D, F and none of : At least 1 of B, D, F and none of A, C, E; or at least 2 of B, D, F and one of A or E.A, C, E; or at least 2 of B, D, F and one of A or E.
Constipation-predominantConstipation-predominant: At least 1 of A, C, E and : At least 1 of A, C, E and none of B, D, F; or at least 2 of A, C, E and one of B, D, Fnone of B, D, F; or at least 2 of A, C, E and one of B, D, F

Red flag symptoms which Red flag symptoms which are are notnot typical of IBS: typical of IBS:
Pain that awakens/interferes with Pain that awakens/interferes with sleep sleep
Diarrhoea that awakens/interferes Diarrhoea that awakens/interferes with sleep with sleep
Blood in the stool (visible or occult) Blood in the stool (visible or occult) Weight loss Weight loss Fever Fever Abnormal physical examination Abnormal physical examination

Areas to cover:Areas to cover:
What is IBS?What is IBS? What are the typical symptoms?What are the typical symptoms? Taking a good historyTaking a good history What examination should the GP do?What examination should the GP do? What investigations should the GP do?What investigations should the GP do? Can it be diagnosed by the GP without a Ba Can it be diagnosed by the GP without a Ba
enema or without referral ie. On clinical enema or without referral ie. On clinical history?history?
Treatments – what are they / the evidence / Treatments – what are they / the evidence / what about probiotics and yoghurt type drinks?what about probiotics and yoghurt type drinks?

Examination findingsExamination findings
NilNil

Areas to cover:Areas to cover:
What is IBS?What is IBS? What are the typical symptoms?What are the typical symptoms? Taking a good historyTaking a good history What examination should the GP do?What examination should the GP do? What investigations should the GP do?What investigations should the GP do? Can it be diagnosed by the GP without a Ba Can it be diagnosed by the GP without a Ba
enema or without referral ie. On clinical enema or without referral ie. On clinical history?history?
Treatments – what are they / the evidence / Treatments – what are they / the evidence / what about probiotics and yoghurt type drinks?what about probiotics and yoghurt type drinks?
InvestigationInvestigation
Do we over investigate and over Do we over investigate and over ‘medicalise’ the patient‘medicalise’ the patient
Systematic review: ‘the utility of Systematic review: ‘the utility of diagnostic tests in IBS’ Cash diagnostic tests in IBS’ Cash et alet al. . Am J Gastro 2002Am J Gastro 2002
Chances of organic disease in Chances of organic disease in patients meeting the symptom based patients meeting the symptom based criteria in IBS as normal population criteria in IBS as normal population

Pretest probability of organic GI Pretest probability of organic GI disease in patients meeting disease in patients meeting
symptom based criteria for IBSsymptom based criteria for IBSOrganic GI Organic GI diseasedisease
IBS patients IBS patients %%
(pre test (pre test prob.)prob.)
Prevelance inPrevelance in
General pop. General pop. %%
Colitis/IBDColitis/IBD 0.51-0.980.51-0.98 0.3-1.20.3-1.2
Colorectal CaColorectal Ca 0-0.510-0.51 4-64-6
CoeliacCoeliac 4.674.67 0.25-0.50.25-0.5
GI infectionGI infection 0-1.70-1.7 NANA
Thyroid abn.Thyroid abn. 66 5-95-9
Lactose Lactose malabsmalabs
22-2622-26 2525

Investigation cont.Investigation cont.
<1% pickup of IBD/CCA<1% pickup of IBD/CCA 10 times incidence of coeliac10 times incidence of coeliac Colonic imaging <1% chance of picking Colonic imaging <1% chance of picking
up significant pathology overallup significant pathology overall Routine biochem/coeliac serology Routine biochem/coeliac serology
probably usefulprobably useful BSG Blood screen and flexi in BSG Blood screen and flexi in
secondary caresecondary care Value of reassurance not assessedValue of reassurance not assessed

BSG Guidelines 2000

Areas to cover:Areas to cover:
What is IBS?What is IBS? What are the typical symptoms?What are the typical symptoms? Taking a good historyTaking a good history What examination should the GP do?What examination should the GP do? What investigations should the GP do?What investigations should the GP do? Can it be diagnosed by the GP without a Ba Can it be diagnosed by the GP without a Ba
enema or without referral ie. On clinical enema or without referral ie. On clinical history?history?
Treatments – what are they / the evidence / Treatments – what are they / the evidence / what about probiotics and yoghurt type drinks?what about probiotics and yoghurt type drinks?

Diagnostic accuracy for IBS is over Diagnostic accuracy for IBS is over 95% when Rome II criteria are met, 95% when Rome II criteria are met, history and physical exam do not history and physical exam do not suggest any other cause, and initial suggest any other cause, and initial laboratory testing is negative.laboratory testing is negative.
Areas to cover:Areas to cover:
What is IBS?What is IBS? What are the typical symptoms?What are the typical symptoms? Taking a good historyTaking a good history What examination should the GP do?What examination should the GP do? What investigations should the GP do?What investigations should the GP do? Can it be diagnosed by the GP without a Ba Can it be diagnosed by the GP without a Ba
enema or without referral ie. On clinical enema or without referral ie. On clinical history?history?
Treatments – what are they / the evidence / Treatments – what are they / the evidence / what about probiotics and yoghurt type drinks?what about probiotics and yoghurt type drinks?

TreatmentTreatment
ReassuranceReassurance Lifestyle changesLifestyle changes Dietary interventionDietary intervention Psychological interventionPsychological intervention Drug interventionDrug intervention

Dietary interventionDietary intervention
No conclusive/consistent evidenceNo conclusive/consistent evidence Food intolerances: ‘challenge studies’ in Food intolerances: ‘challenge studies’ in
IBS pts suggest intolerance in 6-50%IBS pts suggest intolerance in 6-50% Exclusion diets or elimination diets usedExclusion diets or elimination diets used 6/8 trials showed no improvement with 6/8 trials showed no improvement with
fibre increasefibre increase High sorbitol/fructose rich diets eg. High sorbitol/fructose rich diets eg.
slimmingslimming Caffeine although little evidence in Caffeine although little evidence in
literatureliterature

DietDiet Dietary changes may prevent the overreaction of the Dietary changes may prevent the overreaction of the
gastrocolic reflex and lessen pain, discomfort, and gastrocolic reflex and lessen pain, discomfort, and bowel dysfunction.bowel dysfunction.
Having soluble fibre foods and supplements, Having soluble fibre foods and supplements, substituting soy or rice products for milk products, substituting soy or rice products for milk products, being careful with fresh fruits and vegetables that are being careful with fresh fruits and vegetables that are high in insoluble fibre, and eating frequent meals of high in insoluble fibre, and eating frequent meals of small amounts of food, can all help to lessen the small amounts of food, can all help to lessen the symptoms of IBS. symptoms of IBS.
Foods and beverages to be avoided or minimized Foods and beverages to be avoided or minimized include red meat, oily or fatty and fried products, milk include red meat, oily or fatty and fried products, milk products (even when there is no lactose intolerance), products (even when there is no lactose intolerance), solid chocolate, coffee (regular and decaffeinated), solid chocolate, coffee (regular and decaffeinated), alcohol, carbonated beverages (especially those also alcohol, carbonated beverages (especially those also containing sorbitol), and artificial sweeteners. containing sorbitol), and artificial sweeteners.

Definitive determination of dietary issues can Definitive determination of dietary issues can be accomplished by testing for the be accomplished by testing for the physiological effects of specific foods.physiological effects of specific foods.
The The ELISAELISA food allergy panel can identify food allergy panel can identify specific foods to which a patient has a specific foods to which a patient has a reaction. Other testing can determine if there reaction. Other testing can determine if there are nutritional deficiencies secondary to diet are nutritional deficiencies secondary to diet that may also play a role.that may also play a role.
Removal of foods causing IgG immune Removal of foods causing IgG immune response as measured using the ELISA food response as measured using the ELISA food panel has been shown to substantially panel has been shown to substantially decrease symptoms of IBS in several studies.decrease symptoms of IBS in several studies.

There is no evidence that digestion of food or There is no evidence that digestion of food or absorption of nutrients is problematic for absorption of nutrients is problematic for those with IBS at rates different from those those with IBS at rates different from those without IBS.without IBS.
However, the very act of eating or drinking However, the very act of eating or drinking can provoke an overreaction of the can provoke an overreaction of the gastrocolicgastrocolic response response in some patients with in some patients with IBS due to their heightened visceral IBS due to their heightened visceral sensitivity, and this can lead to abdominal sensitivity, and this can lead to abdominal pain, diarrhoea, and/or constipation.pain, diarrhoea, and/or constipation.

Diet -FibreDiet -Fibre In patients who do In patients who do notnot have diarrhoea have diarrhoea
predominant irritable bowel, soluble fibre at predominant irritable bowel, soluble fibre at doses of 20 grams per day can reduce overall doses of 20 grams per day can reduce overall symptoms but will not reduce pain. symptoms but will not reduce pain.
The research supporting dietary fibre The research supporting dietary fibre contains conflicting, small studies that are contains conflicting, small studies that are complicated by the heterogeneity of types of complicated by the heterogeneity of types of fibre and doses used . fibre and doses used .
The one The one meta-analysismeta-analysis that controlled for that controlled for solubility found that only soluble fibre solubility found that only soluble fibre improved global symptoms of irritable bowel improved global symptoms of irritable bowel and neither type of fibre reduced pain. and neither type of fibre reduced pain.
Positive studies have used 20-30 grams per Positive studies have used 20-30 grams per day of day of psylliumpsyllium seed ( seed (also called also called ispaghulaispaghula husk husk). ).

Drug interventionDrug intervention
High placebo response 30-70%. High placebo response 30-70%. Difficult to assess.Difficult to assess.
Laxatives: No RCTs, Limited benefitLaxatives: No RCTs, Limited benefit Antidiarrhoeals: eg loperamide.Antidiarrhoeals: eg loperamide.
4 RCTs show some effect on 4 RCTs show some effect on decreasing abdo pain but no effect decreasing abdo pain but no effect on global symptoms or bloating on global symptoms or bloating

Drug intervention cont.Drug intervention cont. Antispasmodics: 3 RCTs. Questionable Antispasmodics: 3 RCTs. Questionable
benefit. Only short term trials. A meta-benefit. Only short term trials. A meta-analysis by the Cochrane Collaboration analysis by the Cochrane Collaboration suggest NNT = 6. suggest NNT = 6.
Antidepressants: TCADs: Meta analysis in Antidepressants: TCADs: Meta analysis in 2000 Am J Gastro showed significant effect 2000 Am J Gastro showed significant effect over placebo NNT 3 (best for D-IBS).over placebo NNT 3 (best for D-IBS).
SSRIs: Citalopram (Tack SSRIs: Citalopram (Tack et alet al., Gut 2006) ., Gut 2006) improved pain, bloaring and QOL. Better for improved pain, bloaring and QOL. Better for C-IBS?C-IBS?

Drugs affecting serotonin (5-Drugs affecting serotonin (5-HT)HT)
Serotonin stimulates the gut motility and so agonists can help Serotonin stimulates the gut motility and so agonists can help constipation predominate irritable bowel while antagonists can help constipation predominate irritable bowel while antagonists can help diarrhea predominant irritable bowel:diarrhea predominant irritable bowel:
AgonistsAgonists TegaserodTegaserod, a selective 5-HT4 agonist for IBS-C, is available for relieving , a selective 5-HT4 agonist for IBS-C, is available for relieving
IBS constipation in women and chronic idiopathic constipation in men IBS constipation in women and chronic idiopathic constipation in men and women. A meta-analysis by the Cochrane Collaboration (NNT = 17) and women. A meta-analysis by the Cochrane Collaboration (NNT = 17)
Selective serotonin reuptake inhibitorSelective serotonin reuptake inhibitor anti-depressantsanti-depressants (SSRIs), (SSRIs), because of their serotonergic effect, would seem to help IBS, especially because of their serotonergic effect, would seem to help IBS, especially patients who are constipation predominant. Initial crossover studies patients who are constipation predominant. Initial crossover studies and randomized controlled trials support this role. and randomized controlled trials support this role.
AntagonistsAntagonists AlosetronAlosetron, a selective 5-HT3 antagonist for IBS-D, which is only , a selective 5-HT3 antagonist for IBS-D, which is only
available for women in the United States under a restricted access available for women in the United States under a restricted access program, due to severe risks of side-effects if taken mistakenly by IBS-A program, due to severe risks of side-effects if taken mistakenly by IBS-A or IBS-C sufferers. or IBS-C sufferers.
CilansetronCilansetron, also a selective 5-HT3 antagonist, is undergoing further , also a selective 5-HT3 antagonist, is undergoing further clinical studies in Europe for IBS-D sufferers. In 2005, Solvay clinical studies in Europe for IBS-D sufferers. In 2005, Solvay Pharmaceuticals withdrew Cilansetron from the United States Pharmaceuticals withdrew Cilansetron from the United States regulatory approval process after receiving a "not approvable" action regulatory approval process after receiving a "not approvable" action letter from the FDA requesting additional clinical trials. letter from the FDA requesting additional clinical trials.

New drugsNew drugs
Aloesetron (GSK) 5HT3 antagonistAloesetron (GSK) 5HT3 antagonist FDA approved 2000FDA approved 2000 Withdrawn 2000 Ischaemic colitis Withdrawn 2000 Ischaemic colitis
(1:1000)(1:1000) A few deaths attributed to itA few deaths attributed to it Reintroduced 2002Reintroduced 2002 Reduced doseReduced dose Severe restrictions (counselling, Severe restrictions (counselling,
consent)consent)

AloesetronAloesetron
Slows colonic transit timesSlows colonic transit times 5 RCTs 5 RCTs Significant benefit over mebeverineSignificant benefit over mebeverine Consistent modest improvement in Consistent modest improvement in
global symptoms in diarrhoea global symptoms in diarrhoea predom. femalespredom. females
No application for license in the UK No application for license in the UK or Europeor Europe

TegaserodTegaserod
5HT4 agonist5HT4 agonist Increase GI motility in healthy Increase GI motility in healthy
subjects and IBS patients.subjects and IBS patients. Possible visceral analgesic property: Possible visceral analgesic property:
Reduced sensitivity to rectal stimuli in Reduced sensitivity to rectal stimuli in healthy volunteers (Coffin healthy volunteers (Coffin et al.et al. Aliment Pharmacol Ther 2003)Aliment Pharmacol Ther 2003)
Applying for European license (exp Applying for European license (exp 2005)2005)

TegaserodTegaserod
6 RCTs show modest but statistically 6 RCTs show modest but statistically significant improvement in global significant improvement in global symptoms in constipation symptoms in constipation predominant IBSpredominant IBS
3 month trial of 1519 pts with 3 month trial of 1519 pts with constipation predom. IBS showed constipation predom. IBS showed therapeutic gain of 15% at 1/12 but therapeutic gain of 15% at 1/12 but only 5% at 3/12 in global symptoms.only 5% at 3/12 in global symptoms.
Side effects Diarrhoea, headacheSide effects Diarrhoea, headache

Future therapiesFuture therapies
Abdo pain: Muscarinic antagonists, Abdo pain: Muscarinic antagonists, Beta 3 agonists vs spasm. Kappa Beta 3 agonists vs spasm. Kappa opioid agonists for analgesia eg. opioid agonists for analgesia eg. FedozotineFedozotine
Constipation: Other 5HT4 agonists, Constipation: Other 5HT4 agonists, 5HT3 agonists, CCK antagonists, 5HT3 agonists, CCK antagonists, opioid antagonistsopioid antagonists
Diarrhoea: Other 5HT3 agonists, Diarrhoea: Other 5HT3 agonists, 5HT4 agonists, alpha 2 agonists5HT4 agonists, alpha 2 agonists
Recent studies have suggested that Recent studies have suggested that rifaximinrifaximin, a non-, a non-absorbable antibiotic, can be used as an effective treatment absorbable antibiotic, can be used as an effective treatment for abdominal bloating and flatulence, giving more for abdominal bloating and flatulence, giving more credibility to the potential role of bacterial overgrowth in credibility to the potential role of bacterial overgrowth in some patients with IBS.some patients with IBS.
A double-blind, randomized, placebo-controlled trial A double-blind, randomized, placebo-controlled trial compared the multi-herbal extract Iberogast versus placebo compared the multi-herbal extract Iberogast versus placebo in the treatment of all three forms of irritable bowel in the treatment of all three forms of irritable bowel syndrome. This multi-target phytopharmaceutical was found syndrome. This multi-target phytopharmaceutical was found to be significantly superior to placebo via both an abdominal to be significantly superior to placebo via both an abdominal pain scale (p value = 0.0009) and an IBS symptom score (p pain scale (p value = 0.0009) and an IBS symptom score (p value = 0.001) after four weeks of treatment.value = 0.001) after four weeks of treatment.
Enteric coated Enteric coated peppermintpeppermint oil capsules has been advocated oil capsules has been advocated for IBS symptoms in adults and children; however, results for IBS symptoms in adults and children; however, results from trials have been inconsistent. Peppermint may from trials have been inconsistent. Peppermint may exacerbate exacerbate gastroesophagealgastroesophageal reflux disease reflux disease..
Alternative treatmentsAlternative treatments

Psychotherapy and Psychotherapy and hypnotherapyhypnotherapy
There is a strong brain-gut component to IBS, There is a strong brain-gut component to IBS, and and cognitive therapycognitive therapy may improve symptoms in may improve symptoms in a proportion of patients in conjunction with a proportion of patients in conjunction with antidepressantsantidepressants. In a . In a randomized controlled trialrandomized controlled trial of referred patients, of referred patients, cognitive cognitive behavioralbehavioral therapy therapy helped even though patients in this study helped even though patients in this study did notdid not have any psychiatric diagnoses.have any psychiatric diagnoses.
Gut-directed or gut-specific Gut-directed or gut-specific hypnotherapyhypnotherapy or self- or self-hypnosis is one of the most promising areas of hypnosis is one of the most promising areas of IBS treatment. Current research shows that IBS treatment. Current research shows that symptom reduction/elimination from IBS symptom reduction/elimination from IBS hypnotherapy can last at least five years.hypnotherapy can last at least five years.

Acupuncture Acupuncture The The meta-analysismeta-analysis by the by the
Cochrane CollaborationCochrane Collaboration concluded 'Most of the concluded 'Most of the trials included in this review were of poor trials included in this review were of poor quality and were heterogeneous in terms of quality and were heterogeneous in terms of interventions, controls, and outcomes interventions, controls, and outcomes measured. With the exception of one outcome measured. With the exception of one outcome in common between two trials, data were not in common between two trials, data were not combined. Therefore, it is still inconclusive combined. Therefore, it is still inconclusive whether acupuncture is more effective than whether acupuncture is more effective than sham acupuncture or other interventions for sham acupuncture or other interventions for treating IBStreating IBS

Alternative treatmentsAlternative treatments ProbioticsProbiotics are generally accepted to be potentially are generally accepted to be potentially
beneficial strains of bacteria and yeast, often found in the beneficial strains of bacteria and yeast, often found in the human gut.human gut.
One research study has shown a clear link between the One research study has shown a clear link between the ingestion of Lactobacillus plantarum LP299V and sufferers ingestion of Lactobacillus plantarum LP299V and sufferers of IBS who reported resolution of their abdominal pain. of IBS who reported resolution of their abdominal pain.
B. infantis 35625, a strain of Bifidobacteria in normalizing B. infantis 35625, a strain of Bifidobacteria in normalizing bowel movement frequency in sufferers of IBS. bowel movement frequency in sufferers of IBS.
VSL #3?VSL #3?
A prospective placebo-controlled study found patients with A prospective placebo-controlled study found patients with diarrhoea predominant IBS taking diarrhoea predominant IBS taking Saccharomyces Saccharomyces boulardiiboulardii, a probiotic yeast, had a significant reduction on , a probiotic yeast, had a significant reduction on the number and improvement in consistency of bowel the number and improvement in consistency of bowel movements.movements.

Psychological interventionPsychological intervention
Hypnotherapy: good results for refractory Hypnotherapy: good results for refractory cases with limited psychopathologycases with limited psychopathology
Significant improvement vs. counselling Significant improvement vs. counselling (Whorwell (Whorwell et alet al Lancet 1984) Lancet 1984)
Reduced motor and sensory gastrocolonic Reduced motor and sensory gastrocolonic response post hypnotherapy (Simren response post hypnotherapy (Simren et alet al Psychosomatic Medicine 2004)Psychosomatic Medicine 2004)
CBT shown significant results in trialsCBT shown significant results in trials Expensive and time consumingExpensive and time consuming

BSG Guidelines 2000

SummarySummaryAim to make a positive
diagnosis with Rome criteria history, examination
Beware alarm symptoms:Wt loss, PR bleeding, recent change
in bowel habit etc
Basic Ix: stool culture, FBC, U&E, LFT, CRP, TFT, anti TTG Ab, glucose, Ca
Refer for further investigation
IBS-C IBS-D Pain/bloating
Explanation, reassurance, dietary and lifestyle advice
Increase dietary fibre / fluidBulk forming laxative(s)Consider citalopram
Dietary modification Anti-diarrhoeal agentsConsider amitriptyline
Reduced fibre intakeIncreased fluidsAntispasmodicsConsider TCADs/citalopram
In refractory cases consider counselling, hypnotherapy, biofeedback, role of probiotics

ConclusionsConclusions
A complex multifactorial ‘disease’A complex multifactorial ‘disease’ Huge resource useageHuge resource useage Targeted drug therapy difficultTargeted drug therapy difficult New therapies but modest resultsNew therapies but modest results Probably grossly over investigated in Probably grossly over investigated in
many cases many cases