irish pharmacy news - issue 9 - 2012
DESCRIPTION
In this issue: NEWS: Drug pricing debate rages as prices shown to be cheaper in North - PROFILE: We chat exclusively to Leonora O'Brien as she presents a 360 degree view of pharmacy - NEWS: Which Irish pharmacies made it into the Retail Excellence Top 30 Stores shortlist? - CPD: The pharmacist role in managing Osteoporosis patients - FEATURE:Common winter skin conditions presenting in the pharmacy - AWARDS: We find out what won itfor Locum of the Year Hilary DolanTRANSCRIPT

Shortlisted BUSINESS TO BUSINESS MAGAZINE OF THE YEAR 2009
THE INDEPENDENT VOICE OF PHARMACY
September 2012 Volume 4 Issue 9
NEWSACHETFORMAT
ALWAYS READ THE LABELcontains Ibuprofen Date of preparation: July 12. Item number CADR-IRE-02-07-08-12
NEW
Available in pharmacy only
In this issue:
NEWS: Drug pricing debate rages as prices shown to be cheaper in North Page 4
PROFILE: We chat exclusively to Leonora O'Brien as she presents a 360 degree view of pharmacy Page 9
NEWS: Which Irish pharmacies made it into the Retail Excellence Top 30 Stores shortlist? Page 14
CPD: The pharmacist role in managing Osteoporosis patients Page 33
FEATURE: Common winter skin conditions presenting in the pharmacy Page 38
AWARDS: We find out what won it for Locum of the Year Hilary Dolan Page 42

Ireland has a NEW King of Hearts!
Ireland’s No. 1 Generic Healthcare Specialists
Reduces Total Cholesterol and LDL Cholesterol1
Helps prevent cardiovascular events in patients at risk of first event1
Abbreviated prescribing information: Torvan 10 mg/ 20 mg/ 40 mg and 80 mg Film-coated tablets. Presentation: Torvan is supplied as film-coated tablets of 10 mg/ 20 mg/ 40 mg or 80 mg of atorvastatin. Indications: Torvan is indicated as an adjunct to diet for reduction of elevated total cholesterol (total-C), LDL-cholesterol (LDL-C), apolipoprotein B, and triglycerides in adults, adolescents and children aged 10 years or older with primary hypercholesterolaemia including familial hypercholesterolaemia (heterozygous variant) or combined (mixed) hyperlipidaemia (Corresponding to Types IIa and IIb of the Fredrickson classification) when response to diet and other nonpharmacological measures is inadequate. Atorvastatin is also indicated to reduce total-C and LDL-C in adults with homozygous familial hypercholesterolaemia as an adjunct to other lipid-lowering treatments (e.g. LDL apheresis) or if such treatments are unavailable. Used for the prevention of cardiovascular events in patients estimated to have a high risk for a first cardiovascular event (see section 5.1), as an adjunct to correction of other risk factors. Dosage: The patient should be placed on a standard cholesterol-lowering diet before receiving atorvastatin and should continue on this diet during treatment with atorvastatin. The dose should be individualized according to baseline LDL-C levels, the goal of therapy, and patient response. The usual starting dose is 10 mg once a day. Adjustment of dose should be made at intervals of 4 weeks or more. The maximum dose is 80 mg once a day. Atorvastatin is for oral administration. Each daily dose of atorvastatin is given all at once and may be given at any time of day with or without food. Contraindications: Hypersensitivity to the active substance or to any of the excipients of this medicinal product. Active liver disease or unexplained persistent elevations of serum transaminases exceeding 3 times the upper limit of normal. During pregnancy, while breast-feeding and in women of child-bearing potential not using appropriate contraceptive measures. Special warnings and precautions for use: Liver function tests should be performed before the initiation of treatment and periodically thereafter and in patients who develop any signs or symptoms suggestive of liver injury (monitor raised transaminase levels until they resolve). Should an increase in transaminases of greater than 3 times the upper limit of normal (ULN) persist, reduction of dose or withdrawal of atorvastatin is recommended. For patients with prior hemorrhagic stroke or lacunar infarct, the balance of risks and benefits of atorvastatin 80 mg is uncertain, and the potential risk of hemorrhagic stroke should be carefully considered before initiating treatment. Torvan should be prescribed with caution in patients with pre-disposing factors for rhabdomyolysis and a CK (creatine kinase) level should be measured before treatment. If CK levels are significantly elevated at baseline (> 5 times ULN), treatment should not be started. Patients with muscle pain, cramps, or weakness especially if accompanied by malaise or fever should have their CK levels monitored. Torvan must be discontinued if clinically significant elevation of CK levels (> 10 x ULN) occur, or if rhabdomyolysis is diagnosed or suspected. If muscular symptoms are severe and cause daily discomfort treatment discontinuation should be considered. The risk of myopathy may also be increased when administered with other medicinal products that have a potential to induce myopathy. In cases where co-administration of these medicinal products with Torvan is necessary, the benefit and the risk of concurrent treatment should be carefully considered. The concurrent use of atorvastatin and fusidic acid is not recommended, therefore, temporary suspension of atorvastatin may be considered during fusidic acid therapy. Exceptional cases of interstitial lung disease have been reported with some statins. If it is suspected a patient has developed interstitial lung disease, statin therapy should be discontinued. Patients with diabetes should be monitored both clinically and biochemically according to national guidelines. Developmental safety in the paediatric population has not been established. Drug Interactions: CYP3A4 inhibitors, CYP3A4 inducers, Transport protein inhibitors, Gemfibrozil / fibric acid, derivatives, Ezetimibe, Colestipol, Fusidic acid, Digoxin, Oral contraceptives, Warfarin, Tipranavir, Ritonavir, Ciclosporin, Lopinavir, Clarithromycin, Saquinavir, Darunavir, Itraconazole, Fosamprenavir, Nelfinavir, Grapefruit Juice, Diltiazem, Erythromycin, Amlodipine, Cimetidine, Efavirenz, Rifampin, Gemfibrozil, Fenofibrate, Phenazone. Pregnacy and lactation: Torvan should not be used in women who are pregnant, trying to become pregnant or suspect they are pregnant. Treatment with atorvastatin should be suspended for the duration of pregnancy or until it has been determined that the woman is not pregnant. Undesirable effects: Common side effects include: nasopharyngitis, allergic reactions, hyperglycaemia, pharyngolaryngeal pain, epistaxis, constipation, flatulence, dyspepsia, nausea, diarrhoea, myalgia, arthralgia, pain in extremity, muscle spasms, joint swelling, back pain, liver function test abnormal, blood creatine kinase increased, headache, abdominal pain, alanine aminotransferase increased, blood creatine phosphokinase increased, For further undesirable effects, please refer to the SPC. Shelf Life: 18 months in bottles, 21 months in blisters. Marketing Authorisation Holder: Pinewood Laboratories Ltd, Ballymacarbry, Clonmel, Co. Tipperary. Marketing Authorisation Holder Numbers(s): PA 281/150/001 - 004. This medicine is a prescription only product. Further prescribing information is available on request. Date of revision: July 2012 Reference 1: Torvan Summary of Product Characteristics, July 2012 Date of preparation: July 2012
Torvan IPN Ad (210x297mm).indd 1 16/08/2012 11:21

IPN • September 2012 3
PUBLISHERIPN Communications Ireland Ltd. Carmichael House, Lower Baggot Street, Dublin 2 00353 (01) 6024715
MANAGING DIRECTORNatalie Maginnis [email protected]
GROUP SALES MANAGER UK & IRELANDDebbie Graham [email protected] 7865594809
EDITORBridget Casey [email protected]
SUB EDITORKelly Jo [email protected]
EDITORIAL [email protected]
ACCOUNTS Lorraine Moore [email protected]
ADVERTISING MANAGERNicola [email protected]
CONTRIBUTORSEamonn Brady
ART DIRECTEDSmart Page Design
EDITORBridget Casey
ForewordContents
Irish Pharmacy News is Circulated to all independent, multiple and hospital pharmacist, pre reg pharmacists, students pharmacy student’s offi cial bodies, government offi cials and departments, Pharmacy Managers, Manufactures, Wholesalers. Buyers of pharmacy groups and healthcare outlets. Circulation is free to all pharmacists Subscription rate
for Irish Pharmacy News 60euro plus vat per year
All rights reserved by Irish Pharmacy News. All material published in Irish Pharmacy News is copyright and no part of this magazine may be reproduced, stored in a retrieval system of transmitted in any form without written permission. Pharmacy Communication Ireland have taken every care in compiling the magazine to ensure that it is correct at the time of going to press, however the publishers assume no responsibility for any effects from omissions or errors.
9
14
42
18
4 Pharmacy profession turned to in times of recession
6 Digital overhaul for McCauleys Chemists
14 Pharmacies celebrate being shortlisted in REI's Top 30 stores competition
18 We debate the generic substitution and reference pricing issue
26 TCD School of Pharmacy researchers discover folic acid developments
42 Locum of the Year Hilary Dolan
56 The adventures of working as a pharmacist in New Zealand
Regulars9 360 degree view of pharmacy with Leonora O'Brien of Pharmapod
33 CPD - Pharmacy management of Osteoporosis
38 As we head into September we feature Winter Skin conditions
50 Feature on presenting viral infections in the pharmacy
60 Product News
66 Appointments
Fine Gael and Labour came into power with all guns blazing, trumpeting that they were going to revolutionise the Health Service In Ireland, since when, in modern parlance, they have done ‘not a lot’ and been conspicuously quiet about it.
A couple or so new Primary Care Health Centres have opened (which were already in the pipeline) and Government has been a very long time making up its mind about generic substitution, with the result that some people are doubtful whether this would prove beneficial to all patients, see page 14 and are worried about supplies and also the amount of savings, although any savings are better than none. But, when it comes to health insurance, the question we raise here is: Who has been consulted to advise Government? It is all well and good for parties to send representatives to look at how other schemes work in different countries but the problem here is that most, if not all come back thinking that they are an authority on this particular system or that. They are not.
Government should be seeking out their own citizens, who have actually worked at the coal face to obtain their opinions and advice - but are they? If they are, we should like to know who their consultants are.
For example, an Irish pharmacist, who has worked in the UK as well as in Ireland believes that the UK health service really has it ‘sorted’ when it comes to generic substitution because people do not expect to be given branded drugs these days. She thinks that, unless a (total) public awareness campaign is implemented in Ireland and that doctors also get behind this project, then the public will be resistant to change. (See page 18).
Fine Gael and Labour have the Herculean task of introducing universal health insurance (UHI) by 2016 and have looked at the system in the Netherlands, which finds favour with well over 90 per cent of the Dutch people. IPN covered this in their early publications but the Dutch principle is a system of compulsory social insurance, involving competing insurers, with the hope of driving costs down but this has now hit snags. Cracks are also beginning to appear in the price of the Dutch healthcare system, with annual costs rising up to 7% above the rate of inflation per annum, to name just one problem, although many others are beginning to surface.
This month’s profile is on Leonara O’Brien, (see page 9) a pharmacist, who has spent many years working in Europe and has had first hand experience of how many of the European countries operate, including the Netherlands and the UK and is another person who would, no doubt give the Government some practical advice. Government needs all the help that it can get from people, who do not have an axe to grind or anything to gain either in status and prestige or in monetary terms, or both.
Experienced friends and countryman would willingly give of their advice but would Government give of its ears?
*****
Afinitor, a treatment for patients with the most common form of advanced breast cancer has been approved by the European Medicines’ Agency for use recently but, unfortunately the development of bapineuzumab, a drug aimed at stopping the build-up of plaque in the brain, known to accelerate Alzheimer’s disease has hit snags and its development has been discontinued.
Citizens around the world have come to expect such research and development as a matter of course, almost as a right. However, scientists spend their lives in the service of the nations of the world, trying to find miracle cures. Some do and some fail but IPN hails them all for their persistence, perseverance and perfection in continually trying to eradicate the world of disease.

4 September 2012 • IPN
News
news briefPatients crossing the Border to obtain prescriptionsPrivate patients in Border counties are buying prescription drugs in Northern Ireland at much cheaper prices than they would pay in the Republic, according to a report in The Irish Times last month.
It was revealed that cardiovascular patients without medical cards can make savings of up to €80 on a month’s supply of six commonly prescribed cardiac drugs (€960 per year) if they are dispensed in Northern Ireland. One particular drug in the Republic can, typically cost four times the total cost of the six drugs combined in the North.
Prices quoted by two pharmacies in Co Donegal apparently came to a total of €96.54 and €96 respectively for a month’s supply of aspirin, clopidogrel, simvastatin, bisoprolol, ramipril and a glyceryl trinitrate spray, whilst another quoted £30 (euros 38.15) . In contrast, two pharmacies in Derry City quoted just £14 (€17.80) and £17 (€21.62) for a month’s supply of the equivalent drugs.
Legislatively, there is no issue with patients from the Republic having their prescriptions dispensed in Northern Ireland because both jurisdictions are part of the European Union.
“A report produced for the HSE expressed the view that international comparisons of prices cannot be relied on as each market is different in terms of size, structure and regulations,” an Irish Pharmacy Union spokeswoman told the paper.
“Prices vary from pharmacy to pharmacy and patients will go to the pharmacy that best suits their needs, not alone in terms of price but also in terms of the nature of the professional service that they receive.
“Over the past two years, there have been numerous cuts to the price of medicines in Ireland. This has led to a significant decrease in the cost of commonly prescribed medicines. All of these reductions have been passed on to patients,” added the spokeswoman.
Recession-hit public relying on pharmacistsThe general public are increasingly turning to community pharmacists for healthcare advice, as the ongoing recession continues to affect disposable incomes.
This is one of the results of a new survey, which was carried out by PricewaterhouseCoopers (PwC) on behalf of the Irish Pharmacy Union (IPU). It also revealed that 91 per cent of community pharmacists reported growing numbers of people seeking their expertise and services.
These services include advice on minor ailments, health promotion (such as advice and support on obesity and smoking cessation) and basic health screenings for cholesterol, body mass index and blood pressure.
According to IPU President Rory O’Donnell, community pharmacies are the most accessible part of the healthcare system, with the average pharmacy opening 63 hours per week. He said that previous IPU research had found that a person visits a pharmacy about 19 times a year.
In the last 18 months, the role of the pharmacist has expanded, with pharmacists now supplying emergency contraception without a prescription, as well as the flu vaccine. However, the full
healthcare potential of the community pharmacy sector remains significantly under-exploited in Ireland, particularly when compared with other countries.
This fact is reflected in the PwC survey, which reported that 97 per cent of community pharmacists surveyed believe their healthcare potential is being under-exploited.
“Pharmacists in other countries provide many
healthcare services to their patients,” said O’Donnell. “For example, pharmacists in Scotland carry out Medicines Use Reviews for some patients on behalf of the NHS. This ensures patients are getting the full benefit from their medicines and are taking only those medicines which are clearly necessary for their treatment. This reduces medicine wastage and, therefore, the cost to the State.”
He called on the Department of Health to engage with the IPU to enable Irish patients to benefit from many more extended services, which are provided by pharmacists in other countries.
The new survey follows on from IPU research carried out earlier this year, which showed that nine out of 10 Irish adults, who were surveyed would like pharmacists to be given a greater role in the health service.
Pharmacists are being urged to advise parents on screening children routinely for head lice every week when they return to school in the coming weeks. It is also essential to warn parents not to treat their child for head lice as a precaution as products used to treat head lice do not prevent the infection from occurring.
Pharmacist Grainne O’Leary says,“Unfortunately there is no way of preventing head lice, but the earlier the infection is detected, the easier it is to
Back to school advicemanage. We are advising parents to check their children’s heads for head lice and nits (eggs) routinely every week by wet combing the hair.
“Products used to treat head lice do not prevent the infection from occurring and children should not be exposed to treatment unless it is necessary. In the long run, screening saves time and distress to children, parents and other family members who will also need to be treated if an infestation occurs”, Ms O’Leary said.

IPN • September 2012 5
The Irish Pharmacy Union (IPU) has said that, although the base price of medications in Ireland is higher than in the UK a straightforward comparison between the two countries cannot be made.
IPU President Rory O’Donnell was speaking in light of the revelations last month that patients in Ireland are paying up to 12 times more than their UK counterparts for the same medicines. Drug firms are charging the Health Service Executive more than the UK-based NHS because of the deal sanctioned by the Department of Health. Under the two-year-old agreement, manufacturers of generic drugs are allowed to charge the HSE as much as 98 per cent of the price of the original branded product.
For example, the HSE currently pays €37 for clopidogrel, a blood-thinning medication, while its British equivalent pays just €3. A generic 28-pack of the cholesterol medicine atorvastatin costs €7.80 in Britain but it costs €24.08 in Ireland.
“We have been saying for years that the base price is more expensive in Ireland,” said O’Donnell. “I could not say that it is ‘too expensive’, due to the fact that there are ongoing negotiations between the manufacturers, the Irish Pharmaceutical
Lower medication prices in pipeline
News
Healthcare Association and the HSE – I would not like to prejudice the negotiations.
“However, the price of medications will certainly fall in the near future and we welcome that on behalf of patients.”
O’Donnell said that, in his experience patients understood that community pharmacists had nothing to do with deciding the base prices of medicines, which are set by agreement between the HSE and the major pharmaceutical manufacturers.
“From conversations I have with customers in my own pharmacy in Donegal, it is clear that patients understand the situation,” he said, "and the IPU has not received an increase in the number of complaints from the public with regard to prices, which bears this out.
"Many factors influence drug costs in this country," he continued, "such as the cost of doing business, regulation and the cost of repackaging.” Drug companies would no longer have to use Ireland-specific packaging on their medicines, under the proposals being developed by the Department of Health to encourage them to drop their prices.
“There is a separate regulatory process required in order to get generics on the
The staff at Market Point Pharmacy in Mullingar have had double reasons to celebrate recently. Susan Tomey, Hannah Buchannon, Jennifer Moran and Noeleen Boyce (pictured) felt the burn as they recently completed a local triathlon. Feeling exhuberant, they along with pharmacist John Keane were delighted to discover the pharmacy has made it inton the Top 20 'National Store of the Year' 2012.
John opened his pharmacy in September 2008. Like all independent retail pharmacies,
Double success for Market Point
Rory O'Donnell
market in Ireland,” O’Donnell explained. “Also, in this country, there is less than a 20 per cent generic penetration, whereas the figure is 80 per cent in the UK. We have a population of fewer than five million people, whereas the UK has around 63 million. Unfortunately, it’s no surprise that there is a price difference.
“The price of medications has come down in recent times though, and this is set to continue,” he concluded.
he has witnessed a lot of change in the sector since then. He told Irish Pharmacy News that the REI nomination is a reward for all the effort that he and his staff have put in to the pharmacy to keep it up to date.
“We are really proud of what we've achieved as a small independent pharmacy. To get recognised for this, alongside national and international retailers has been a huge boost for us. We were lucky to have made it to the final last year so, to make it again this year is a great achievement for all the team at Market Point Pharmacy.”
Susan Tormey, Hannah Buchannon, Jennifer Moran and Noeleen Boyce
6 September 2012 • IPN
News
news briefMcCauley’s gets digital revampThe Sam McCauley chain of pharmacies has re-launched its website, which has had a complete redesign to facilitate ease of shopping and encourage repeat business.
“We wanted to make the shopping process easier for our customers. In a way, it is like doing a refit,” said Sinead McDonald, marketing manager. “We wanted to increase the number of ranges that are offered on line and make the whole shopping experience better for our customers – and of course to increase our sales as well! We felt that a revamp would bring better returns."
Sam McCauley’s has been running a website for a number of years and, after the first refit in 2008, sales soared. However, as with anything, it was paramount to keep up with the latest advances in technology and ensure that all the latest developments were incorporated.
“The redesign took longer than we had hoped and was quite an undertaking,” said McDonald. “It was such an extensive redesign; it really changed the whole online process and the way we think about it. It involved a number of departments and we did not want to launch the new site until we were completely happy with it, although it will be constantly updated and improved."
The new site, offering over 5,000 products has many additional features, such as Paypal,3D secure and a guest check-out function, which does not require anyone to register before placing an order.
“It was our aim to make it user-friendly,” said McDonald. “We wanted take advantage of the redesign to improve the user experience, allowing our customers to browse easily and to make their way to the checkout with the least amount of hassle. Customers are now able to access their chosen product with only two clicks of the mouse, instead of four.”
According to IPHA Chief Executive Anne Nolan, Government needs to tread carefully with the Health (Pricing and Supply of Medical Goods) Bill and its expected route forward as 'it has the potential to restrict the supply of innovative medicines to Irish patients, as well as damaging the sustainability of the pharmaceutical industry in this country.
The Bill will put in place a legislative framework for the introduction of a system of reference pricing and generic substitution for the supply of medicines. While having
reservations about the merits of this model, particularly regarding its possible impact on patient compliance and ability to generate real savings to the State, IPHA had been expecting such legislation. However, the Bill goes well beyond this to include pricing mechanisms and reimbursement parameters to cover all pharmaceutical products in Ireland.
She says: “The new Bill has gone way
Health Bill needs to be amedend says IPHA Chief
beyond what we had envisaged and in giving
the HSE alone the power to decide what
medicines will be reimbursed under the State schemes and in what circumstances, will undermine the authority of the prescriber in choosing the medicine for
patients under his/her care.
"This could result in shortages of some
vital medicines and due to the size of the Irish market, a
steep fall in prices could lead to certain products becoming uneconomical, and as a consequence they could be withdrawn from the Irish market altogether.
"We know how little room for manoeuvre the Government has when it comes to savings; however, bad law is not good law. This Bill could seriously undermine an industry that employs over 25,000 people and hinder the supply of innovative medicines and treatments to Irish people. It needs to be significantly amended before becoming law.”
The Health Bill is due to be debated in the Dail this autumn.
The Irish Medicines Board has removed the requirement for Patient Information Leaflets to be submitted as part of a clinical trial application.
The organisation states that such documents are for review by the ethics committee and not the medicines’ regulator.
IMB removes patient information leafl ets
This represents the removal of a significant potential delay for members and a barrier to the efficient set up of clinical trials in Ireland. It is expected that this will result in a saving of up to 8 weeks in the commencement time for clinical trials, which is good news for patients.

think smart medicine
your TrustedPartner


IPN • September 2012 9
Laying the foundations for future services
Leonora O’Brien has what can only be described as a 360-degree view of the pharmacy sector. All that the founder and CEO of Pharmapod Ltd wishes to do now is to improve pharmacy standards and patient safety. She hopes to carry this out by developing ‘a web-based platform to help pharmacists deliver structured clinical services, monitor the incidents that happen in their pharmacies and share knowledge with their peers’.
O’Brien has worked in many aspects of pharmacy, including being a community pharmacist, chief superintendent of a major pharmacy chain, European manager of professional pharmacy services for a multinational in Germany and in pharmacy governance and professional development at the Pharmaceutical Society of Ireland (PSI). She has now struck out on her own, developing Pharmapod, in order to provide software that will benefit both patients and pharmacists alike.
“I have been a qualified pharmacist for 16 years but, after seven years in pharmacy, I went back to study journalism, which taught me some valuable skills and disciplines that have been of great benefit when drafting, for example, guidance documents and policies,” O’Brien told Irish Pharmacy News. “But I returned to pharmacy as I have always found it rewarding and I really missed the interaction with patients.”
In January 2009, O’Brien took
Profi le
I worked on pharmacy practice development at the PSI, which gave me the opportunity to work with the liaison pharmacists within the HSE’s Clinical Strategy and Programmes Directorate.
up the post of superintendent pharmacist of the Unicare and DocMorris pharmacies. Her responsibilities covered 72 pharmacies around Ireland and it helped to lay the foundations for her current work.
“The superintendent role was new at the time, so it was challenging,” she explained.
“There are fewer than 10 superintendents responsible for large numbers of pharmacies in Ireland. The role made me acutely aware of how important

10 September 2012 • IPN
Profi le
it is to have a good IT system across the pharmacies, to help operationally. Going from a single professional, being responsible for your own actions to, overnight, having a legal accountability for a large number of individual practices, means you must adopt effective virtual solutions.
“Every superintendent understands the pressures of having to demonstrate personal control on a full-time basis. Effective IT systems can help streamline reporting and identify underperformance through, for example, pharmacy audits. It can also help monitor progress, year on year. In company terms, the superintendent role is equivalent to ‘chief officer’, carrying full-time responsibility and accountability, which is the intention of the legislation.”
O’Brien said that although this puts pressure on pharmacists, she believes this accountability structure is one of the key drivers of patient safety within the Pharmacy Act.
“Similar accountability systems are being introduced in all professions across the healthcare system, in line with the Patient Safety Commission’s framework. This learning was reinforced for me through working with the PSI.”
EUROPEAN EXPERIENCE
Before working with the pharmacy regulator, O’Brien spread her wings and went to Stuttgart in Germany, where she worked as European manager of professional pharmacy services at Celesio AG, Unicare’s parent company. This role primarily involved the development and implementation of a pharmacy services’ strategy in Belgium, Czech Republic, Germany, Ireland, Italy, the Netherlands and Norway.
“I was also involved in cross-divisional activity with wholesale, a division, which was active in 27 countries,” said O’Brien. “It was interesting to take part in designing services and rolling them out across countries that were so culturally different. Although we are increasingly operating under the same Directives, how the
various countries approached implementation of the legislation differed entirely.”
O’Brien said that the work in Stuttgart gave her a valuable overview of the profession across jurisdictions and an insight into where the pockets of best practice lay. She said that, for example, the UK was progressive, in terms of policy and having the pharmacist’s role in the primary healthcare team officially underpinned by the Pharmacy White Paper. She also found the Netherlands to be progressive in such areas as IT infrastructure and its approach to the pharmacist-doctor relationship, where pharmacists and their local doctor colleagues meet about seven times per year in structured, recorded Pharmaceutical Therapeutic Audit Meetings.
“It is good to learn about the benefits of other systems but it is also important to examine the risks associated with them,” she said. “The Dutch pharmacy model, which in ways we are now edging towards, is not without its challenges. Collective negotiation is not
Leonora O'Brien presents at the NDRC in the Digital Exchange
permitted, so pharmacists spend a lot of resources negotiating complex contracts with health insurers, which detracts from their patient-facing time. They then invest in training and implementation of the contracted service only to find the health insurer may not continue the contract for the following year, making it hard to plan, sustain or continually improve services for patients.
“Since 2011, reimbursement in the Netherlands for pharmacists is not based on dispensing, as it is here,” she continued. “They have moved to a service-based reimbursement system. It all changed in 2005 when they introduced what is called a DBC system, which in English stands for diagnostic and treatment combinations. With this system, payment is based on a ‘lump sum’ approach, for all activities related with certain diseases or incidents. For example, they established what it would cost on average for a healthcare professional to treat a diabetic patient for a year and this is what was reimbursed per diabetic patient.”
This system started in secondary care, where hospitals and private clinics competed on the lump sum prices for a particular patient group. Then it moved to primary care. In pharmacy, the annual lump sum for a patient includes the total pharmaceutical costs, including dispensing.
“So, dispensing is viewed simply as logistics rather than a core service,” O’Brien explained. “The Dutch also implemented their preference policy as early as June 2008 and only the lowest-priced generics are reimbursed.”
She said that Ireland needs to be fiscally austere in the current climate, but incremental changes will not bring us the savings required on our health spend.
“We need a total systems overhaul but it is important, in our consideration of other models, that we learn from the healthcare professionals at the coalface in the originating country and understand the full repercussions for patients.”
PHARMACY GOVERNANCE
Armed with this insight into other countries’ systems,

IPN • September 2012 11
Profi le
O’Brien returned to Ireland in June 2010 to work as pharmacy governance and professional development consultant within the Pharmaceutical Society of Ireland.
“I worked on pharmacy practice development at the PSI, which gave me the opportunity to work with the liaison pharmacists within the HSE’s Clinical Strategy and Programmes Directorate,” she said. “This aimed to improve the quality of care and cost effectiveness of healthcare services.”
O’Brien said that the Irish Pharmacy Act is ‘empowering’, in the sense that it provides for the development of the profession, as well as the identification of underperformance and the Fitness to Practice elements. Whilst at the PSI, she also became part of the National Pharmacist Reference Group, which was established (by the PSI) to progress the implementation of the Pharmacy Ireland 2020 strategy.
“I also worked on programmes with the Irish Centre for Continuing Pharmaceutical
Education, which was very rewarding and gave me an opportunity to meet pharmacists regularly and discuss professional issues and challenges. The superintendent sessions for example were beneficial. It gave superintendents an opportunity to get together and discuss concerns such as full-time accountability and to share insights on how best to manage their new responsibilities under the Act on a practical, day-to-day basis.’’
O’Brien has always had an interest in IT because of its potential to objectively capture the positive interventions and healthcare outcomes that pharmacy delivers.
“As a profession, not only in Ireland but in the majority of countries, we are losing a tremendous amount of important information because we are not pooling our data effectively – data which could be used to inform policies, target resources efficiently and secure reimbursement for future services,” she said. This is now a primary objective for Pharmapod.
CONTINUED PROFESSIONALISM
Pharmapod was established seven months ago and is supported by the National Digital Research Centre in Dublin, where it is also based. It has developed a web-based platform that helps pharmacists with the professional aspects of their practice, such as error and incident reporting and the delivery of high quality, structured clinical services. The platform also helps pharmacists comply with the new Pharmacovigilance Directive and share valuable knowledge amongst their peers.
“The site collates data at a national level, developing an evidence base for pharmacy practice and the expansion of the role of the pharmacist in the community,” O’Brien explained. “It has been developed by pharmacists for pharmacists.”
The first clinical service available on the system will be to help with next season’s influenza
vaccinations. “Pharmapod will also help pharmacists with their SOPs, practice policies and pharmacy audits,” said O’Brien. “Although pharmacists have had to have SOPs in place for some time now, we will help to keep the quality assurance documentation up to date and keep accurate records. Our aim is to provide a one-stop-shop solution for pharmacists.”
O’Brien said that he decision to set up her own company was a natural progression for her. She had worked on the project for 18 months in her spare time but came to realise that it needed a full time focus.
“It would be a pity to be risk-averse when you have a great product,” she said. “Although this is the first time that I have run a company, as pharmacists, we are used to being decision-makers in a team setting. Many pharmacists run their own businesses and do not have much peer contact, so I see this as being an extension of working autonomously in a pharmacy, or making decisions as a superintendent. Some would say it is a big step, but maybe I am missing the fear gene!”
EQUAL ACCESS
“We would like all pharmacists to have equal access to the same level of professional IT support, whether they are sole traders, hospital pharmacists or working for a large chain,” she continued. “I believe that everyone should have access to equal resources if we are to work together as a profession and drive patient safety and service through sharing our knowledge and experience.”
O’Brien believes that, as a profession, pharmacy must support and embrace new technologies because they will lay the foundations for the future health services – from detection and screening programmes to the virtual monitoring of patients.
“Technology allows us to share our professional experiences and data across borders,” she said. “Also, developments in pharmacogenetics mean that personalised medicine will become the norm and it is likely that routine genetic testing will drive prescribing patterns and decision-making. This will throw up some interesting challenges, such as genetic discrimination in the health insurance sector. New technologies like these will mean that pharmacy will keep on evolving.”
O’Brien added that although she misses the immediate rewards of patient-facing practice, she feels that by developing Pharmapod, she is still playing a role that will benefit patients.
“Pharmacists have so much to contribute and by sharing our knowledge through platforms like Pharmapod, we can demonstrate the positive interventions we make and help advance our profession,” she said. “We are working very hard to develop Pharmapod and I love the work. They say when you cannot tell the difference between work and play, you are in a good place – and that is where I am at the moment, thankfully.”
The system will be available to pharmacists from October of this year. See www.pharmapod.ie.
Pharmapod office at the NDRC

12 September 2012 • IPN
News
news briefNow is the time to raise osteporosis awareness With Osteoporosis Awareness Month coming up (in October), now is the time for pharmacists to plan events or campaigns to raise awareness of this bone condition, including how it can be prevented and treated.The Irish Osteoporosis Society estimates that 300,000 people in Ireland have osteoporosis. About one in five men and one in two women over 50 will develop a fracture due to osteoporosis in their lifetime. The numbers affected are set to rise because pensioners will account for one quarter of the population in the Republic within the next two decades.
The number of over-65s is expected to triple by 2041 to almost 1.4 million. This means that Ireland faces a potential osteoporosis explosion, making awareness campaigns even more important.
A number of drugs are licensed in Ireland for bone loss, such as bisphosphonates, strontium ranelate, selective oestrogen receptor modulators, parathyroid hormone and prescription calcium/vitamin D tablets. When filling these prescriptions, patients should be advised to closely follow the prescription directions to maximise treatment benefits.
For people who wish to maintain bone density in the future, the pharmacy can offer a range of supplements that can be of benefit. Calcium and vitamin D are the main building blocks for healthy bone production (and should always be taken together, as vitamin D aids calcium absorption). Other supplements that may help are magnesium, silica and zinc.
Life Pharmacies in Dundalk, Donabate, Santry and Rathmines offer an osteoporosis screening service, as do McCabe’s Pharmacies in Dundrum Town Centre and the Pavilions Shopping Centre in Swords.
Offering a range of products and advice to anyone interested in protecting their bones during Osteoporosis Awareness Month could not only help them to remain independent and well as they get older but will also encourage repeat visits, which will help to maximise pharmacy.
Pharmaceutical exports from Ireland to the US – its biggest overseas market – have slumped by 30 per cent in the first half of this year, according to the Irish Exporters Association (IEA).
Exports to the US, which were worth €11 billion in the period from January to June last year, dropped to €8.7 billion in the first half of this year, according to the IEA’s Half-Year Export Industry Review 2012. The Association said that this represented a severe downturn and was due to the ending of patent protection hitting drug exports.
IEA chief executive John Whelan commented that Ireland’s over-dependency on pharmaceutical exports to the United States was “coming home to roost”.
“Patent protection is by market,” he said, “so the impact will vary according to the export country destination. Exports to the USA were mostly impacted, as the early patent registrations were made there and hence the patent protection has come to an end earliest there.”
He also said that the industry had been calling for more streamlined approval processes, particularly within the European Union, which would help to lower the development and launch costs of new
Pharma exports drop with end of patent protection
medicines.
The review said that this would tend to level the playing field between companies that develop new drugs and those that copy existing products, removing the patent cliff that is currently impacting the industry.
It added that many of the major Irish-based exporters of pharmaceutical and active chemical ingredients for the life sciences industry were facing sustained price pressures, as patent-protected markets were now open to generic manufacturers, who were free to compete without the overhead burdens of the original producers.
The review also said that market development has impacted on exports from the sector, which fell by 5 per cent in the first half of the year. This will have a major impact on the total Irish export values for 2012 because the sector represents over 50 per cent of manufacturing export sales from Ireland.
Exports to the EU continued their long-term trend growth of 6 per cent and there was a 33 per gain in pharmaceutical and chemical exports to the UK during the period covered by the review. This was boosted by the falling value of the euro against sterling.
Michele O'Brien, Osteoporosis society
IEA chief executive John Whelan

11 sachet daily
Protelos (strontium ranelate) abbreviated prescribing information: Please refer to the Summary of product Characteristics before prescribing. Presentation: Sachet containing 2g of strontium ranelate granules for oral suspension. Indication: Treatment of postmenopausal osteoporosis to reduce the risk of vertebral and hip fractures. Treatment of osteoporosis in men at increased risk of fracture. Dosage and Administration: The recommended daily dose is one 2g sachet once daily by oral administration at bedtime, preferably at least two hours after eating. The granules in the sachets must be taken as a suspension in a glass of water. Due to the nature of the treated disease, strontium ranelate is intended for long-term use. Patients treated with strontium ranelate should receive vitamin D and calcium supplements if dietary intake is inadequate. Elderly (>65): No dosage adjustment is required in relation to the elderly. Renal Impairment: No dosage adjustment is required in patients with mild-to-moderate renal impairment (30-70 ml/min creatinine clearance). Strontium ranelate is not recommended for patients with severe renal impairment (creatinine clearance below 30 ml/min). Hepatic Impairment: As strontium ranelate is not metabolised, no dosage adjustment is required in patients with hepatic impairment. Paediatric Population: The safety and efficacy of Protelos in children aged below 18 years have not been established. No data are available. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Current or previous venous thromboembolic events (VTE), including deep vein thrombosis and pulmonary embolism. Temporary or permanent immobilisation due to e.g. post-surgical recovery or prolonged bed rest. Precautions: VTE: Protelos is associated with an increased risk for VTE. The cause of this finding is unknown. Protelos should be used with caution in patients at risk of VTE. When treating patients over 80 years at risk of VTE, the need for continued treatment with PROTELOS should be re-evaluated. Skin reactions: Life-threatening cutaneous reactions (Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN) and drug rash with eosinophilia and systemic symptoms (DRESS)) have been reported with the use of Protelos. Patients should be advised of the signs and symptoms and monitored closely for skin reactions.Interaction with laboratory test: Strontium interferes with colorimetric methods for the determination of blood and urinary calcium concentrations. Therefore, in medical practice, inductively coupled plasma atomic emission spectrometry or atomic absorption spectrometry methods should be used to ensure an accurate assessment of blood and urinary calcium concentrations. Excipient: Protelos contains a source of phenylalanine which could be harmful for people with phenylketonuria. Interactions: Food, milk and derivative products, and medicinal products containing calcium may reduce the bioavailability of strontium ranelate, therefore, administration of Protelos and such products should be separated by at least two hours. It is preferable to take antacids at least two hours after Protelos, however, when this dosing regimen is impractical due to the recommended administration of Protelos at bedtime, concomitant intake remains acceptable. Protelos therapy should be temporarily suspended if a patient is on a course of oral quinolone or tetracycline antibiotics as it may hinder their absorption. Fertility, pregnancy and lactation: There are no data from the use of strontium ranelate in pregnant women. Physicochemical data suggest excretion of strontium ranelate in human milk. Protelos should not be used during breast-feeding. No effects were observed on males and females fertility in animal studies. Undesirable effects: Overall incidence rates for adverse events with strontium ranelate did not differ from placebo and adverse events were usually mild and transient. Adverse reactions, defined as adverse events considered at least possibly attributable to strontium ranelate treatment in phase III studies are listed below using the following convention (frequencies versus placebo): very common (>1/10); common (>1/100, <1/10); uncommon (>1/1,000, <1/100); rare (>1/10,000, <1/1,000); very rare (<1/10,000); not known
(cannot be estimated from the available data). Common: nausea (7.1% vs. 4.6%), and diarrhoea (7.0% vs. 5.0%), headache (3.3% vs. 2.7%), memory loss (2.5% vs. 2.0%), disturbance of consciousness (2.6% vs. 2.1%), dermatitis (2.3% vs. 2.0%), eczema (1.8% vs. 1.4%), venous thromboembolism (2.7% vs. 1.9%), increases in blood creatinine phosphokinase (1.4% vs. 0.6%), Rare: DRESS Very rare: Severe cutaneous adverse reactions- SJS and TEN. Frequency was unknown include: alopecia; oral mucosal irritation; bronchial hyperreactivity, hepatobiliary disorders, hepatitis, bone marrow failure, insomnia, dyspepsia, gastroesophageal reflux, constipation, flatulence. Undesirable effects associated with hypersensitivity skin reactions include pyrexia, lymphadenopathy and eosinophilia. See Summary of Product Characteristics for further details. Presentation: Box containing 28 sachets. Legal Category: POM. Marketing Authorisation Numbers and Holder: EU/1/04/288/001-006, Les Laboratoires Servier, 50, rue Carnot 92284 Suresnes cedex France. Date of Preparation or Last Review: June 2012. Full prescribing information is available from: Servier Laboratories, Block 2, West Pier Business Campus, Old Dunleary Road, Dun Laoghaire, Co. Dublin. Tel: (01) 6638110, Fax: (01) 6638120. Date of Preparation of item: July 2012.1. Protelos Summary of Product Characteristics PRTPA004
Strontium ranelate
Improve Strength Reduce Fractures1
Protelos is proven to be an effective long term 1st line osteoporosis treatment option in postmenopausal women, to reduce the risk of vertebral and hip fractures, and in men at increased risk of fracture1
New in MaleOsteoporosis1
3894 Advert.indd 1 13/08/2012 13:35

14 September 2012 • IPN
News
The pharmacy sector is at the forefront of the retail industry in Ireland, with three pharmacies listed among Retail Excellence Ireland’s (REI’s) 30 finalists for 'National Store of the Year' 2012.
Ireland’s largest retail industry body has listed the following three pharmacies in its prestigious Top 100 list: Market Point Pharmacy, Mullingar, Co Westmeath; DocMorris Pharmacy, Santry, Dublin 9 and McCabe’s Pharmacy in Swords, Co Dublin.
The 'National Store of the Year' 2012 is part of the annual REI Awards, which were established in 1997 to promote best practice standards in the Irish retail industry.
PHARMACY REACTIONS
John Keane, pharmacist at Market Point in Mullingar, opened his pharmacy in September 2008. Like all independent retail pharmacies, he has witnessed a lot of change in the sector since then. He told Irish Pharmacy News that the REI nomination is a reward for all the effort that he and his staff have put in to the pharmacy to keep it up to date.
“We are really proud of what we've achieved as a small independent pharmacy,” Keane said. “To get recognised for this, alongside national and international retailers has been a huge boost for us. We were lucky to have made it to the final last year so, to make it again this year is a great achievement for all the team at Market Point Pharmacy.”
Pharmacy shines in fi nal 30 storesAisling Gargan, assistant manager at McCabe's Pharmacy in Swords said: “We have entered a couple of times now and we won both the 'Extra-Large Store' category and the overall 'Store of the Year' award in 2006. We reached this same stage of the competition last year, so we are hoping to go all the way this time around,” she said. “Our
manager, Elaine O'Neill was also highly commended in the Manager of the Year' category in 2011.
“We have excellent staff here. They all want to do their best and offer very high standards,” she explained. “That comes across to anyone who comes into the pharmacy, whether it is a customer or a judge from Retail Excellence Ireland.”
Gargan also said that the pharmacy team could hardly wait until the awards ceremony and have been on a high since the news came through that they were finalists.
The team at DocMorris, Santry, Dublin
CHANGING TIMES
Jeni Gilmartin has worked as the manager in the DocMorris Pharmacy in Santry's Omni Park Shopping Centre for almost 16 years. The pharmacy has expanded and changed during its 20-year history and, in March of this year, it unveiled its latest look.
“Our new pharmacy has a bigger, brighter and better layout,” said Gilmartin. “We now have a qualified beauty therapist, a dedicated room for Dermalogica skincare treatments, and a designated 'Skin Secrets' section, where our customers can receive specialist advice on their skincare needs.
“We have a more accessible medicines counter, so our pharmacists can engage easily with our patients and customers,” she continued, “and we have a brand-new patient care room for private consultations. We have even included a children's play area in the front of shop.”
Gilmartin said the REI nomination was recognition of more than just the four walls of the pharmacy; it was about the dedication that the team puts in.
“They carry out a lot of extra work in the community, running health and beauty events for patient groups and charities," she said. "It is all about their passion for their work, not just what the pharmacy looks like – it is the team, which ensures that customers receive an excellent experience when they visit us.
“The entire team, including me, is ecstatic to have made it this far,” Gilmartin concluded.
The team at McCabes Pharmacy, Pavilion Shopping Centre, Swords

GSKCH 2011/0362
Product Information for Panadol Extra 500mg/65mg Soluble Effervescent Tablets. Therapeutic Indications The tablets are recommended for use as an analgesic in the relief of mild to moderate pain such as is associated with rheumatism, neuralgia, musculoskeletal disorders, headache, and of discomfort associated with influenza, feverishness and feverish colds, toothache and dysmenorrhoea. Posology and Method of Administration For oral administration. Panadol Extra Soluble should be dissolved in at least half a tumbler full of water. Adults (including the elderly) and children aged 12 years and over: 2 tablets up to four times daily. Do not exceed 8 tablets in 24 hours. Children under 12 years: Not recommended for children under 12 years of age. Minimum dosing interval: 4 hours. Do not exceed the stated dose. Should not be used with other paracetamol-containing products. Patients with renal or hepatic impairment should seek medical advice before taking this medicine. Contraindications Known hypersensitivity to paracetamol, caffeine or any of the other ingredients. Special Warnings or Precautions for Use. Patients who have been diagnosed with liver or kidney impairment must seek medical advice before taking this medication. Underlying liver disease increases the risk of paracetamol related liver damage. Excessive intake of caffeine (e.g. coffee, tea and some canned drinks) should be avoided while taking this product. Prolonged use except under medical supervision may be harmful. Do not exceed the stated dose. Take only when necessary. If symptoms persist, consult your doctor. Each tablet contains 425 mg of sodium. To be taken into consideration by patients on a controlled sodium diet. Each tablet contains sorbitol powder (E 420) at 50 mg per tablet. Patients with rare hereditary problems of fructose intolerance should not take this medicine. Keep out of reach and sight of children. Interactions with other Medicaments and other forms of Interactions Paracetamol may increase the elimination half-life of chloramphenicol. The absorption of paracetamol may be increased by metoclopramide and decreased by cholestyramine. Oral contraceptives may increase the rate of clearance of paracetamol. The anticoagulant effect of warfarin and other coumarins may be enhanced by prolonged regular daily use of paracetamol with increased risk of bleeding; occasional doses have no significant effect. Pregnancy and Lactation Pregnancy Paracetamol Human and animal studies have not identified any risk of paracetamol in pregnancy or embryo-foetal development. Caffeine Paracetamol-caffeine is not recommended for use during pregnancy due to the possible increased risk of spontaneous abortion associated with caffeine consumption
Lactation Paracetamol and caffeine are excreted in breast milk. Paracetamol Human studies with paracetamol at the recommended doses have not identified any risk to lactation or the breast-fed offspring. Caffeine Caffeine in breast milk may potentially have a stimulating effect on breast fed infants but significant toxicity has not been observed. Side Effects of paracetamol: All very rare: Thrombocytopaenia, Anaphylaxis, Cutaneous hypersensitivity reactions including skin rashes, angiodema, and Stevens Johnson syndrome, Bronchospasm in patients sensitive to aspirin and other NSAIDs, Hepatic dysfunction. Side Effects of caffeine: Nervousness, Dizziness. When the recommended paracetamol-caffeine dosing regimen is combined with dietary caffeine intake, the resulting higher dose of caffeine may increase the potential for caffeine-related adverse effects such as insomnia, restlessness, anxiety, irritability, headaches, gastrointestinal disturbances and palpitations. Overdose Paracetamol Immediate medical attention (in-hospital, if possible) is required in the event of overdose, even if there are no significant early symptoms. Caffeine Symptoms and Signs Overdose of caffeine may result in epigastric pain, vomiting, diuresis, tachycardia or cardiac arrhythmia, CNS stimulation (insomnia, restlessness, excitement, agitation, jitteriness, tremors and convulsions). MARKETING AUTHORISATION HOLDER GlaxoSmithKline Consumer Healthcare (Ireland) Ltd, Stonemasons Way, Rathfarnham, Dublin 16. Further information is available on request from: GlaxoSmithKline, Consumer Healthcare, Stonemason’s Way, Rathfarnham, Dublin 16. Tel: 01 495 5000 | Fax: 01 495 5525. Marketing Authorisation Number PA 678/39/10. Date of (Partial) Revision of the Text December 2010. Legal Category: Pharmacy Only.
*When compared to standard Paracetamol, Panadol Extra Soluble can give 30% more pain relieving power.
CONTAINS PARACETAMOL. ALWAYS READ THE LABEL/LEAFLET.
Exclusive to pharmacy
*
Panadol Extra Soluble provides your patients with a non-codeine soluble solution
MGS1401 EX sol press ad A4.indd 1 23/11/2011 10:40

16 September 2012 • IPN
News
news briefNew jobs for WaterfordDrugsmaker Eirgen Pharma is to create 30 jobs in Co Waterford following support from Enterprise Ireland. The jobs are being created to support the increased focus on in-house research and development &of a range of oncology products for global markets.
Eirgen Pharma specialises in the development and licensing of oncology drugs for the global medications market.
The jobs are due to come on-stream over the coming months. Jobs Minister Richard Bruton described the development as an indication of how Ireland’s economy could recover.
“A central part of the Government’s plan for jobs and growth is creating a powerful engine of indigenous, export-focused companies. Today’s announcement that EirGen, an Irish pharmaceuticals manufacturing company founded by two former employees of a large multinational in the sector, is expanding with the creation of 30 jobs is great news for Waterford and for indigenous industry.
“EirGen is a prime example of the successful companies that will help drive our economic recovery. Through continued implementation of the Action Plan for Jobs, I am determined to ensure that we can see more announcements like this around the country over the coming years," he said.
PMI Breakfast SeminarThe Pharmaceutical Managers Institute of Ireland is holding a breakfast presentation entitled, "Pharmacy in an Evolving Healthcare Environment" and presented by Paul Fahey President of The Pharmaceutical Society of Ireland.
The presentation will be held at Finnstown House Hotel on Tuesday, September 18, 2012 at 7.30am for 8.00am sharp. Guests are welcome but must be accompanied by a PMI Member and pre-registered min of 48 hrs in advance. Contact Clodagh on01 2352310.
Celesio AG has seen an increase in its first-half operating profit, after writing down units sold and those still to be sold. The company is sticking to its forecast for 2012, after adjusting last year's figures.
The operating profit for the first six months of 2012 rose to €283.5 million from €257.5 million for the same period last year. Celesio said it defined operating profit as earnings before interest, taxes, depreciation and amortisation, excluding restructuring charges and adjusted for revaluation and tax effects. Sales increased to €11.25 billion from €11.06 million.
Celesio recently sold two of its major subsidiaries as part of its strategic business realignment. In July, the Movianto Group, which specialises in third-party logistics for the healthcare and pharmaceutical and industries, was sold for €130 million to US medical products distributor and logistics provider Owens & Minor.
“The decision to sell is mainly driven by the buyer’s reputation for quality and integrity, thus defending the best interest of the Movianto employees,” said Celesio chief executive Markus Pinger in a statement. “With Owens & Minor, we have found a potential investor who will drive Movianto’s successful development, offering new prospects. This is an all-round positive solution for all parties concerned.”
Meanwhile, United Drug, the Irish pharmaceutical services conglomerate, recently bought the German contract sales and vacancy management company Pharmexx from Celesio for €35 million. Celesio also said it will sell its Czech wholesale and retail business to Penta Investments for €84.5 million.
“The sale of Movianto, Pharmexx and the activities in the Czech Republic all happened earlier than expected,” Pinger said. “We can now focus on accelerating growth in our core business.” The disposal of Pharmexx was targeted for completion on August 31, pending regulatory approval, according to Celesio.
Meanwhile it has been revealed United Drug have reached agreement to acquire the UK and US clinical services businesses
Profi ts and acquisitions for United
(combined “Bilcare Global Clinical Supplies” or “Bilcare GCS”) from Bilcare Limited for a total consideration of $61 million. The acquisition is expected to complete on 31 August 2012 subject to the fulfilment of usual closing conditions. As part of this agreement, Bilcare Limited will retain its clinical supplies business in Asia.
Commenting on the announcement, Liam FitzGerald, Chief Executive of United Drug said: “The Bilcare acquisition is another very important step in the development of United Drug as we focus on margin expanding, international opportunities.
"This business fits well alongside our existing packaging businesses in the US and Europe and will position us as a leading provider of services in the growing clinical trials materials market.
"Along with the recent Watermeadow and Pharmexx acquisitions, this transaction extends United Drug’s position and reputation as an international provider of outsourced services to life sciences companies with an unrivalled service offering.”
Liam-Fitzgerald

ABBREVIATED PRESCRIBING INFORMATION. Product Name: Atorvas 10mg, 20mg, 40mg and 80mg Film-coated Tablets. Composition: Each film-coated tablet contains 10mg, 20mg, 40mg or 80mg atorvastatin respectively. Description: 10mg, 20mg and 40mg tablets: Light yellow, dappled, glossy, round biconvex film-coated tablets, debossed with ‘HLA 10’, ‘HLA 20’ and ‘HLA 40’ on one side respectively. 80mg tablets: Light yellow, dappled, glossy, oval biconvex film-coated tablets, debossed with ‘HLA 80’ on one side. Indication(s): Hypercholesterolaemia and prevention of cardiovascu-lar disease. Dosage: Adults and elderly: Usual starting dose is 10mg daily with or without food. Primary hypercholesterolaemia and mixed hyperlipidaemia: 10mg daily, maintained for chronic therapy. Maximum therapeutic response seen after 4 weeks. Heterozygous familial hypercholesterolaemia: Initially 10mg daily. Adjust every 4 weeks to 40mg daily. Dose may still be increased to 80mg daily, or add a bile acid sequestrant with 40mg Atorvas as daily dose. Homozygous familial hypercholesterol-aemia: Limited data available. Dose is 10mg to 80mg daily or as an adjunct to other lipid lowering treatments (i.e. LDL apheresis). Prevention of cardiovascular disease: Dose of 10mg daily may be increased to attain (LDL-) cholesterol levels in line with guidelines. Renal impairment: No adjustment of dose. Hepatic impairment: Caution. Paediatric use: Only by a specialist. Experience is limited to age group 4-17 years with severe dyslipidaemias at a starting dose of 10mg increased to 80mg daily. Contraindi-cations: Hypersensitivity to the active or excipients. Active liver disease or unexplained persistent elevations of serum transaminases exceeding 3 times the upper limit. Pregnancy, breast-feeding and women of childbearing potential not using adequate contraception. Warnings and Precautions for Use: Liver effects: Monitor liver
function tests regularly. Caution in patients with liver disease or high alcohol intake. Stroke prevention by aggressive reduction in cholesterol levels: Increase in incidence of stroke with 80mg dose in prior haemorrhagic stroke or lacunar infarct. Caution as risks and benefits of 80mg dose is uncertain. Skeletal muscle effects: In rare occasions: myalgia, myositis, myopathy that may lead to rhabdomyolysis characterised by elevated creatine kinase (CK) levels, myoglobinaemia and myoglobinuria. Caution in predisposing factors for rhabdomyolysis; measure CK levels before treatment in the following situations: renal impairment, hypothyroidism, personal or familial history of muscular disorders, previous history of muscular toxicity with a statin or fibrate, previous history of liver disease or high alcohol intake, where an increase in plasma levels may occur, such as possible interactions, special populations. Increased CK levels 5 times higher than normal and if confirmed after 5 to 7 days; unsuitable for treatment. If patients complain about muscle pain, cramps, weakness with malaise, measure CK levels and act accordingly. Caution when taking drugs that may increase plasma concentration of atorvastatin (potent inhibitors of CYP3A4 or transport proteins, e.g. ciclosporin, telithromycin, clarithromycin, delavirdine, stiripentol, ketoconazole, voriconazole, itraconazole, posaconazole and HIV protease inhibitors). Higher risk of myopathy with gemfibrozil, other fibric acid derivatives, erythromycin, niacin, ezetimbe. Adjust dose of atorvastatin if use is necessary. Interstitial lung disease: Have been reported with long term therapy, discontinue atorvastatin. Interactions: Caution: CYP3A4 inhibitors: See above if given with potent inhibitors of CYP3A4. Moderate CYP3A4 inhibitors, e.g. erythromycin, verapamil, fluconazole: Monitor patients and give lower dose of atorvastatin. CYP3A4
inducers: Lower plasma levels of atorvastatin with efavirenz, rifampicin, St John’s Wort. Transport protein inhibitors: Ciclosporin can increase systemic exposure of atorvastatin. Gemfibrocil/fibric acid derivatives, Ezetimbe: Higher risk of muscle related events. Colestipol: Lower atorvastatin plasma levels, but lipid effects were greater when given in combination. Fusidic acid: Avoid. Digoxin: Monitor as digoxin levels may increase. Oral contraceptives: Increased plasma levels of norethindrone and ethinyl estradiol. Warfarin: Monitor prothrombin time. First 4 days of an 80mg dose gave a slight decrease in prothrombin time that normalised after 15 days of atorvastatin treatment. See SPC for recommended dosage schedules in combination with other drugs. Pregnancy and Lactation: Contraindicated. Ability to Drive and Use Machinery: Negligible influence. Undesirable Effects: Nasopharyngitis, allergic reactions, hyperglycaemia, headache, constipation, pharyngolaryngeal pain, epistaxis, flatulence, dyspepsia, nausea, diarrhoea, myalgia, arthralgia, pain in extremity, muscle spasms, joint swelling, back pain, liver function tests abnormal, and blood creatine kinase increased. Marketing Authorisation Holder: Rowex Ltd, Bantry, Co. Cork. Marketing Authorisation Numbers: PA 711/180/1-4. Further information and SPC are available from: Rowex Ltd, Bantry, Co. Cork. Freephone: 1800 304 400 Fax: 027 50417 E-mail [email protected] Legal Category: Subject to medical prescription. Date of Preparation: April 2012.
Ref 1: PMID:21873710.
Edition 1 05/12 CCF No: 14111
Medicinal products subject to prescription. Further information and SPC available from Rowex Ltd., Bantry, Co. Cork.
Manufacturing in Ireland from our Bantry base, we believe in investing in the best
medicines for your patients
The power to reduce cardiovascular events1
Atorvas Advert a4.pdf 1 25/05/2012 14:07

18 September 2012 • IPN
Debate
The Health (Pricing and Supply of Medical Goods) Bill 2012 has been causing some ripples in pharmacy and medical circles since it was published in July. The Bill – which sets out statutory procedures governing the supply, reimbursement and pricing of medicinal products under the General Medical Services (GMS) and Community Drugs Schemes – is intended to promote competition between generic medicines and to ensure value for money in the supply of medicines.
In a country where fewer than one in five prescribed drugs are generic (compared to four in five in the UK), the Department of Health has said that it hopes to cut the drug bill by €50 million a year using generics.
Under the present system, pharmacists are not permitted by law to provide medication other than the brand specified on the prescription. The Bill, which is expected to pass into law before the end of the year, introduces the concept of interchangeable medicinal products and will enable pharmacists to sell and substitute generic drugs to patients, even though the doctor has prescribed brand-name medicines. Pharmacists must offer the lowest-cost product to all patients, not just those on the drugs' schemes. But, patients will have the opportunity to co-pay if they want an alternative brand.
Research published in April by the Irish Pharmacy Union (IPU) showed that there was a broad welcome from patients for the supply of generic medicines. Some 88 per cent of those surveyed agreed with the following statement: ‘Pharmacists should be allowed to offer cheaper, equivalent generic medicines where they are available and suitable to the patient.’ It would seem that pharmacists around the country are equally as supportive of the proposals to introduce generic substitution.
PHARMACIST VIEWS
Brian O’Donoghue, a pharmacist in O’Donoghue’s Pharmacy in Virginia, Co Cavan, said he was very much in favour of generic substitution and that it should have been introduced years ago, for the sake of patients and also for the state of Ireland’s health service.
“As long as it is done fairly, I wholeheartedly welcome the substitution of branded drugs with generics,” he said. “I think it is the only way forward. It has worked well in so many
Is generic substitution good news for all?
countries, all over the world. We are lagging behind because we are only introducing it now, but ‘better late than never’. In the interests of patients, the price of drugs just has to come down further.”
O’Donoghue said that Government strategies that worked well in the past must move with the times to suit Ireland's current economic situation.
“It made sense during the 1970s to encourage the use of branded drugs because we were trying to entice the major pharmaceutical companies to set up in Ireland – and that seemed to work. But the Government’s 2011 ‘Health at a Glance’ report showed that Ireland spent 11.4 per cent of its gross national income on healthcare (ranking 6th out of the 27 countries for which details were available) and it has to bring down the costs of drugs, to start with.”
In a recent report on pharmaceutical pricing, the Economic and Social Research Institute said that drug costs account for about 17.5 per cent of public health expenditure in Ireland, up from 14 per cent in 2000.
“Introducing generic substitution would, in turn, surely bring down the cost of branded drugs and the market would level out,” O’Donoghue continued. “At the end of the day, the patient is always our priority and interchangeable medications would be of benefit to them because they could get similar medications for a cheaper price. The fact that it would also help lessen the health spend is another major bonus.”
Anne Murray, a pharmacist in Care Pharmacy in Galway’s Salthill, agreed with O’Donoghue that introducing interchangeable medications was a step in the right direction.
“I think that the introduction of generic substitution is a positive development for the healthcare system in general, and especially for patients,” she said. “It means that patients can have a choice when it comes to paying for their medications. That can only be a good thing. Of course, it will mean extra work for pharmacists but I think that the extra effort is well worth it if it brings benefits to our customers and patients.”
Another pharmacist, who is a locum and works in pharmacies around the west of Ireland, said that one of the biggest hurdles to be overcome was not necessarily the extra workload but changing the mindset of the public and, indeed the medical profession when it came to generics.
“I was trained in England and worked for two years over there,” she told Irish Pharmacy News. “I welcome the introduction of generic substitution in Ireland, as I’ve seen it working well in the UK. But, it is a different kettle of fish over here. The NHS covers the vast majority of medications in the UK and the health service really has it sorted when it comes to substitution – that is just the way it is done and patients do not expect to be given branded drugs. However, it is different here, where people are more loyal to their brands and this is a new concept.
“I think the Irish public would be more resistant to the idea of having their drugs switched to generics, especially if they have been on a certain medication for a long time. If we really want this to be accepted here, then I think the Government needs to
Brian O’Donoghue

implement a public awareness campaign, reassuring people that their new generic drug works in exactly the same way as their old, branded one.
“Doctors also need to get behind this to make it work. There would be no extra workload for pharmacists if doctors prescribed generics in the first place. It would also be easier for pharmacists to deal with any patient who might have an issue with a substituted drug if we could clearly show them that it was what their doctor had prescribed.
"Doctors should also put on the prescription what the medicine is to be used for. This would make it a lot easier for pharmacists to substitute generics for branded products," she concluded.
IMPLEMENTATION
Morgan Power, the south-east’s regional representative of the IPU and a pharmacist at Power’s Pharmacy in Ballybricken, Waterford welcomed the proposals because the Union has been campaigning for such a system for a number of years. However, he was critical of the delay in the introduction of the policy in Ireland.
"The delay in introduction of generic substitution has led to a loss for the Exchequer and patients, and it is now critical that the practice is introduced as quickly as possible, to help achieve savings. It is also vital that the HSE and the Department of Health work closely with the IPU to ensure that the change is brought about as smoothly as possible, to ensure that patient health is not compromised in the transition.”
He said that the Government, the HSE and the Department of Health needed to be very clear in their communications regarding generic substitution.
“They need to go slowly and let pharmacists know, at all times what is happening,” said Power. “They need to be aware of all the potential pitfalls and anticipate them. If all medications were replaced with generics at the same time, supply would be used up too quickly. There could also be problems with too few generic suppliers to deal with massive orders in the case of an immediate switchover, so parallel imports must be considered and monopolies prevented. And, of course, if the reference price is too low, companies may even pull out of Ireland because our small market would not be worthwhile to them.”
He said that although there would be some increase in pharmacists’ workload, pharmacists already have the necessary knowledge and expertise to offer generic
substitution to patients, consequently additional SOP guides would not be required.
“It is also important that the HSE provides GMS codes for generic products as soon as the brand comes off patent. For example, the patent for Lipitor expired earlier this year and we understood that generic companies were having difficulty getting a GMS code for atorvastatin,” Power continued. “I do not anticipate this being a recurring problem but it is something that should be flagged up now to the HSE, so that it does not become an issue.”
INDUSTRY VIEW
Philip Hannon, Communications and Public Affairs Manager at the Irish Pharmaceutical Healthcare Association (IPHA), said that the Association was still considering the new Bill and the proposed legislation’s position on generic substitution.
"In the meantime," he added, "the IPHA’s opinion on interchangeability remained the same and the Association still has concerns about the introduction of generics' substitution in this country."
“Ireland currently has a fair and equitable
single tier system, whereby all patients, regardless of income, have access to a secure supply of the medicines, which their doctors believe are most suitable for them," said another IPHA spokesperson. "This has been achieved through the delivery of successive supply agreements between the IPHA, the Department of Health and the Health Service Executive, which have provided significant value for the taxpayer, as well as ensuring continuity of supply. This current system is providing, and can continue to do so in future, real and meaningful savings.”
The Association said that the proposed introduction of generic substitution would remove the distinction between prescribing and dispensing, which has served doctors, pharmacists and patients well in the past.
“Currently, doctors are free to exercise their own professional judgement as to what is the appropriate treatment for their individual patients. Generic substitution would fundamentally undermine this important freedom, altering the doctor-patient relationship and, possibly, also reducing the quality of life of Irish patients.
“The financial benefits for the State of such
Morgan Power
Debate

20 September 2012 • IPN
Debate
a step are also questionable and there would be significant downsides, in terms of the potential reduction in patient adherence to their medication. The position in Austria and Belgium, where substitution is prohibited, demonstrates that there is no need for a reference pricing system to be accompanied by substitution.”
The Bill also allows the HSE to set the price of products based on a wide range of criteria and also to conduct regular reviews.
“The proposed resetting of reference prices, up to four times a year could see patients being regularly switched from one medicine, which they are doing well on, to another product,” said the IPHA. “This could result in an increase in the already high level of non-compliance by patients with their medication, leading to poorer health outcomes.”
PATIENT GROUPS’ CONCERNS
Some patient groups also have reservations when it comes to generic substitution of branded drugs. Brainwave, the Irish Epilepsy Association, is concerned about the variability between brand and generic anti-epilepsy drugs (AEDs) and how this can impact on seizure control.
“We have campaigned on the issue of generic substitution in epilepsy for years, citing international evidence that substituting branded epilepsy medications with their generic equivalents or switching from one generic drug to another generic version of the same drug can lead to the recurrence of seizures in some people, whose epilepsy was otherwise controlled,” said Peter Murphy, deputy CEO of Brainwave.
“We were reassured in 2010 that AEDs would be excluded from any generic substitution scheme on the grounds of patient safety. But, under the current Government, we have heard nothing more in this regard.
“The Bill does not mention any exclusions so far. We wrote to the IMB about it last month, outlining the relevant points, once again. If someone is newly diagnosed with epilepsy, there is no problem with starting them on generics but Brainwave is keen to ensure that AEDs remain outside the scope of the new legislation and that people with epilepsy are not switched from a branded AED to a generic version of that AED, or from one generic version to another.”
The Irish Osteoporosis Society also has concerns about switching patients from branded osteoporosis drugs to generics. It has lobbied to prevent this scheme from including osteoporosis medications and has pointed to several studies, which show that switching between bisphosphonates can increase the risk of upper-GI events, with one case study of generic switching showing that it had potentially contributed to the death of a patient.
Morgan Power, however, said that while pharmacists appreciate these fears, the Irish Medicines Board had responsibility for determining which drugs should not be substituted.
“An exemption is provided for under the legislation, which will allow doctors to write on a prescription that a particular drug should not be substituted for clinical reasons,” he said. “The IMB will designate which medicines are interchangeable and the Board is a safe pair of hands. Criteria will be outlined as to why products may not be interchangeable, such as where there are issues with bioavailability or delivery.”
It would seem that the pharmacy community has broadly welcomed the Bill’s provisions for a system of generic substitution. However, there are still outstanding issues to be resolved regarding the roll-out of the scheme.
Philip Hannon
news briefEnbrel licence expanded The European Commission (EC) has expanded the licence for Pfizer's Enbrel to include five sub-types of juvenile idiopathic arthritis (JIA) and has also approved a more convenient, once-weekly dosing regimen.
The Commission has given the all clear for the use of Enbrel (etanercept) in: polyarthritis; extended oligoarthritis in children and adolescents from the age of two who have not responded or are intolerant to methotrexate; psoriatic arthritis in children aged 12 years and above, who have not responded or are intolerant to methotrexate; and enthesitis-related arthritis in those from the age of 12 years, who have not responded or are intolerant to conventional therapy.
Clearance came in the wake of new data from a 12-week open label study, which showed that in each of the JIA sub-types studied, the majority of patients met response criteria and demonstrated clinical improvement in secondary endpoints, including the number of tender joints.
The original paediatric indication for Enbrel was for the treatment of polyarticular JIA. With its additional approvals, the drug has become the only biologic to be cleared for use in more than one sub-type of JIA.
Pharmacy student's 'wordly' experiencePharmacy student Rebecca Maguire is back on home territory after a five-week gruelling competition as she competed in the Miss World contest as Miss Ireland. Stunning Rebecca has just returned home from Inner Mongolia after battling 115 candidates for the title.
She has described the the long days, with frequent 4am starts but has ultimately labelled it as the 'experience of a lifetime' during which time she made lifelong friends and created unique memories.
The student will continue to be Miss Ireland until September of next year. No doubt the experience will have been a fantastic training exercise for when she qualifies as a fully fledged pharmacist!

Product Names: Calpol 120 mg/5 ml Sugar Free Infant Oral Suspension. Composition: Calpol Sugar Free Infant Oral Suspension contains 120 mg Paracetamol in each 5 ml. Indications: Calpol Sugar Free Infant Suspension is indicated for the treatment of pain (including teething pain), and as an antipyretic. Calpol Sugar Free Infant Suspension is indicated for the relief of headache, migraine, neuralgia, toothache and teething pains, sore throat, rheumatic aches and pains, influenza, feverishness and feverish colds. Dosage: Infants aged 2-3 months: Post-vaccination fever and Other causes of Pain and Fever - if your baby weighs over 4 kg and was born after 37 weeks: One 2.5 ml (small end of spoon). If necessary, after 4-6 hours, give a second 2.5 ml dose. Do not give to babies less than 2 months of age. Do not give more than 2 doses. Leave at least 4 hours between doses. If further doses are needed, talk to your doctor or pharmacist. It is important to shake the bottle for at least 10 seconds before use. Children aged 3 months – 6 years: 3 – 6 months: One 2.5 ml spoonful (small end) 4 times. 6 – 24 months: One 5 ml spoonful (large end) 4 times. 2 – 4 years: One 5 ml spoonful (large end) and one 2.5 ml spoonful (small end), 4 times. 4 – 6 years: Two 5 ml spoonfuls (large end), 4 times. Do not give more than 4 doses in any 24 hour period. Contra-indications: Calpol Sugar Free Infant Suspension is contra-indicated in patients with known hypersensitivity to paracetamol, or any of the other components. Special warnings and special precautions: Calpol Sugar Free Infant Suspension should be used with caution in moderate to severe renal impairment or severe hepatic impairment. The label contains the following statements: Store below 25°C. Protect from light. Contains paracetamol. Do not exceed the stated dose. Keep out of reach of children. Do not take more than 4 doses in 24 hours. Dose 4 times a day. Do not repeat doses more frequently than 4 hourly. Do not give for more than 3 days without consulting a doctor.If symptoms persist consult your doctor. If you child is taking any other medicine, consult your doctor or pharmacist before taking this product. Immediate medical advice should be sought in the event of an overdose, even if you feel well. (label). Immediate medical advice should be sought in the event of an overdose, even if you feel well, because of the risk of irreversible liver damage. (leaflet). Do not take with any other paracetamol containing products. The following precautions should be followed when taking this medicine:Do not take with any other paracetamol-containing products. Never give more medicine than shown in the table. Do not overfill the spoon.Always use the spoon supplied with the pack. Do not give to babies less than 2 months of age. For infants 2-3 months no more than 2 doses should be given. Do not give more than 4 doses in any 24 hour period. Leave at least 4 hours between doses. Do not give this medicine to your child for more than 3 days without speaking to your doctor or pharmacist. As with all medicines, if your child is currently taking any medicine consult your doctor or pharmacist before taking this product. Keep out of reach and sight of children. Undesirable effects: Paracetamol has been widely used and, when taken at the usual recommended dosage, side effects are mild and infrequent and reports of adverse reactions are rare. Chronic hepatic necrosis has been reported in a patient who took daily therapeutic doses of paracetamol for about a year and liver damage has been reported after daily ingestion of excessive amounts for shorter periods. A review of a group of patients with chronic active hepatitis failed to reveal differences in the abnormalities of liver function in those who were long-term users of paracetamol nor was the control of the disease improved after paracetamol withdrawal. Nephrotoxic effects following therapeutic doses of paracetamol are uncommon. Papillary necrosis has been reported after prolonged administration.Adverse effects of paracetamol are rare but hypersensitivity, including anaphylaxis and skin rash may occur. Blood and the lymphatic system disorders: Thrombocytopenic purpura, haemolytic anaemia, agranulocytosis. Hepato-biliary disorders: Anaphylaxis, Chronic hepatic necrosis, liver damage, Nephrotoxic effects. Immune system disorders: Papillary necrosis. Skin and subcutaneous: Skin rashes (with or without itching). Social circumstances: Overdosage. Name address of the holder of the marketing authorisation: McNeil Healthcare (Ireland) Ltd, Airton Road, Tallaght, Dublin 24, Ireland. Marketing authorisation number: PA 823/10/5. Date of revision of text: December 2011. Classification: General sale in child resistant packs containing not more than 60ml of the 120mg/5ml dose form. Retail sale through pharmacy in child resistant packs containing not more than 140ml of the 120mg/5ml dose form. Further information available upon request from Johnson & Johnson (Ireland) Ltd.
IRE/CA/12-0051*Based on combined annual fi gures - IMS Health & Neilsen Data MAT May 2012
The fi rst immunisation might leave babies feeling a bit unsettled. Calpol provides gentle pain and fever relief for babies as young as 2 months right up to 12 years.
The no.1 pain and fever reliever for children*.
P30717 J&J Calpol Butterfly IrPharNews A4 jc.indd 1 23/08/2012 17:16
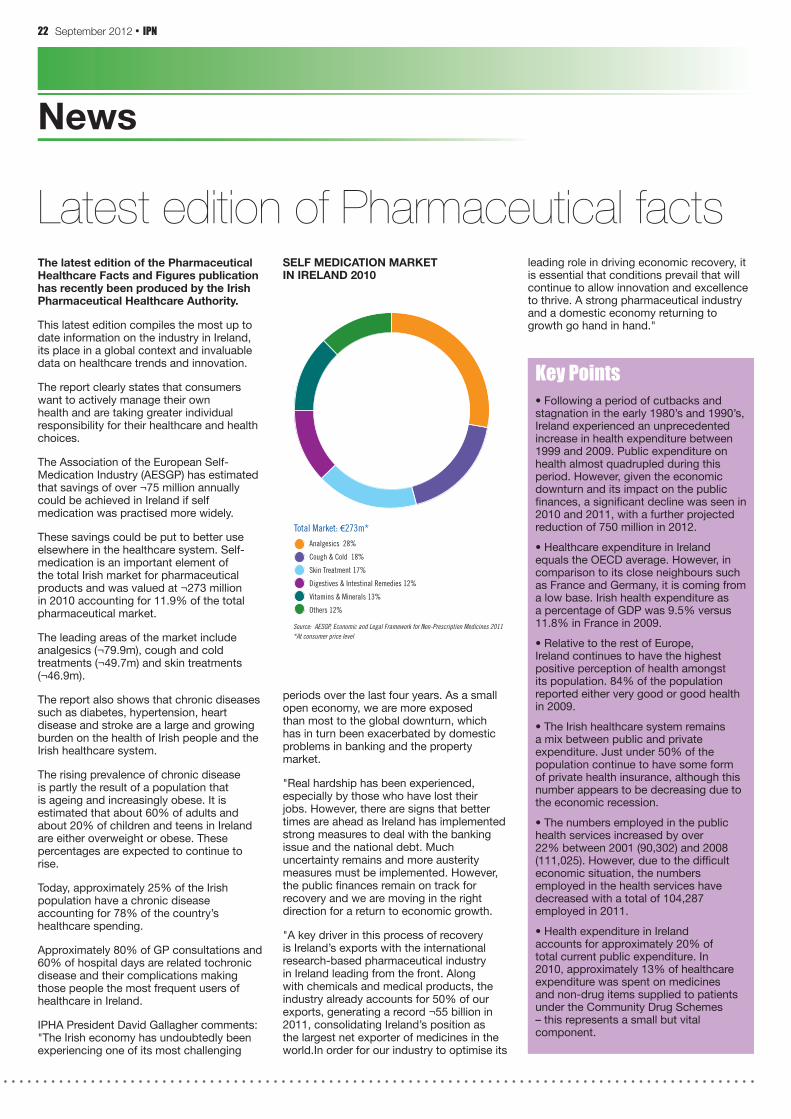
22 September 2012 • IPN
News
Key Points• Following a period of cutbacks and stagnation in the early 1980’s and 1990’s, Ireland experienced an unprecedented increase in health expenditure between 1999 and 2009. Public expenditure on health almost quadrupled during this period. However, given the economic downturn and its impact on the public finances, a significant decline was seen in 2010 and 2011, with a further projected reduction of 750 million in 2012.
• Healthcare expenditure in Ireland equals the OECD average. However, in comparison to its close neighbours such as France and Germany, it is coming from a low base. Irish health expenditure as a percentage of GDP was 9.5% versus 11.8% in France in 2009.
• Relative to the rest of Europe, Ireland continues to have the highest positive perception of health amongst its population. 84% of the population reported either very good or good health in 2009.
• The Irish healthcare system remains a mix between public and private expenditure. Just under 50% of the population continue to have some form of private health insurance, although this number appears to be decreasing due to the economic recession.
• The numbers employed in the public health services increased by over 22% between 2001 (90,302) and 2008 (111,025). However, due to the difficult economic situation, the numbers employed in the health services have decreased with a total of 104,287 employed in 2011.
• Health expenditure in Ireland accounts for approximately 20% of total current public expenditure. In 2010, approximately 13% of healthcare expenditure was spent on medicines and non-drug items supplied to patients under the Community Drug Schemes – this represents a small but vital component.
The latest edition of the Pharmaceutical Healthcare Facts and Figures publication has recently been produced by the Irish Pharmaceutical Healthcare Authority.
This latest edition compiles the most up to date information on the industry in Ireland, its place in a global context and invaluable data on healthcare trends and innovation.
The report clearly states that consumers want to actively manage their own health and are taking greater individual responsibility for their healthcare and health choices.
The Association of the European Self-Medication Industry (AESGP) has estimated that savings of over ¬75 million annually could be achieved in Ireland if self medication was practised more widely.
These savings could be put to better use elsewhere in the healthcare system. Self-medication is an important element of the total Irish market for pharmaceutical products and was valued at ¬273 million in 2010 accounting for 11.9% of the total pharmaceutical market.
The leading areas of the market include analgesics (¬79.9m), cough and cold treatments (¬49.7m) and skin treatments (¬46.9m).
The report also shows that chronic diseases such as diabetes, hypertension, heart disease and stroke are a large and growing burden on the health of Irish people and the Irish healthcare system.
The rising prevalence of chronic disease is partly the result of a population that is ageing and increasingly obese. It is estimated that about 60% of adults and about 20% of children and teens in Ireland are either overweight or obese. These percentages are expected to continue to rise.
Today, approximately 25% of the Irish population have a chronic disease accounting for 78% of the country’s healthcare spending.
Approximately 80% of GP consultations and 60% of hospital days are related tochronic disease and their complications making those people the most frequent users of healthcare in Ireland.
IPHA President David Gallagher comments: "The Irish economy has undoubtedly been experiencing one of its most challenging
Latest edition of Pharmaceutical facts
periods over the last four years. As a small open economy, we are more exposed than most to the global downturn, which has in turn been exacerbated by domestic problems in banking and the property market.
"Real hardship has been experienced, especially by those who have lost their jobs. However, there are signs that better times are ahead as Ireland has implemented strong measures to deal with the banking issue and the national debt. Much uncertainty remains and more austerity measures must be implemented. However, the public finances remain on track for recovery and we are moving in the right direction for a return to economic growth.
"A key driver in this process of recovery is Ireland’s exports with the international research-based pharmaceutical industry in Ireland leading from the front. Along with chemicals and medical products, the industry already accounts for 50% of our exports, generating a record ¬55 billion in 2011, consolidating Ireland’s position as the largest net exporter of medicines in the world.In order for our industry to optimise its
leading role in driving economic recovery, it is essential that conditions prevail that will continue to allow innovation and excellence to thrive. A strong pharmaceutical industry and a domestic economy returning to growth go hand in hand."
16
Self Medication Market in Ireland 2010
Source: AESGP, Economic and Legal Framework for Non-Prescription Medicines 2011*At consumer price level
Analgesics 28%
Cough & Cold 18%
Skin Treatment 17%
Digestives & Intestinal Remedies 12%
Vitamins & Minerals 13%
Others 12%
Total Market: €273m*
SELF MEDICATION MARKETIN IRELAND 2010

HAVE YOU THOUGHT ABOUT JOININGRETAIL EXCELLENCE IRELAND?
Here are a few reasons to become part of Ireland’s largest retail industry group:
For further details please contact Susan Meade at: 065 6846927 or [email protected].
Join the • REI Pharmacy Network and benefit from peer to peer case studies, pharmacy member networking, pharmacy specific learning interventions, bespoke pharmacy market intelligence et al.
Receive complimentary over the phone human resource management advice•
Receive a quarterly pharmacy sector productivity review investigating dispensary, OTC and retail sales trends. •The report also insights payroll cost, rent cost, average transaction values and retail space productivity
Receive complimentary over the phone legal and financial advice•
Benefit from REI’s representation of Ireland’s largest industry including our plans to revive Ireland’s towns and cities•
Enjoy a wide range of leading retail industry learning interventions•
Receive Retail Times Magazine every two months•
Enjoy regular member e-mail updates highlighting pertinent retail industry issues •
Join a vibrant community of more than 400 progressive and professional pharmacy stores who are REI members •

24 September 2012 • IPN
News
RTE presenter Brian Ormond, a native of Clondalkin, Deputy Mayor of South Dublin County Council, Councillor Gus O'Connell (Ind), along with local public representatives Cllr Trevor Gilligan (FF) and Cllr Matthew McDonagh (SF)
news briefSwitching medicines progress The progress of the Switch on to Self-Care working group continues and the Self Care First Framework document is due to be launched on September 20th. The working group was established in 2010 with theaim of switching moe medicines to OTC status in the Irish market.
The working group recently met with senior Department of Health officials to discuss the Self-Care First Framework, which will be launched at a seminar jointly hosted by the IPHA and IPU.
A broad expression of support has been demonstrated for a more extensive use of switching in Ireland and the IPHA recently revised and developed further its proposals for increased OTC medicine status.
Do's and Don'ts Guide An online guide entitled 'Common Ailments in Babies and Young Children', which provides practical healthcare advice to parents to help manage common illnesses that occur in a child's early years, has been launched by the Irish Pharmacy Union. Ailments such as colds, coughs, pain and fever, teething, and colic are covered in the Guide. The Guide also contains safety tips on the Dos and Don'ts of giving medicine to young children.
Launching the Guide, IPU Vice-President Kathy Maher said, "Babies and young children are susceptible to common infections and bugs that, most of the time, are easily treated. Pharmacists can advise on what course of treatment is required and whether a parent needs to take their child to a doctor.
"When giving any medicine to a child, it is important that the right dose is given as overdosing can be dangerous. If a parent has any concerns, they should ask the advice of their pharmacist and always follow the instructions on the information leaflet supplied with the medicine. We have included some dos and don'ts on the correct way to give medicines to children in our Guide to assist parents", Ms Maher continued.
Pharmacy chain creates26 new jobsBoots Ireland has opened a new store and expanding an existing one with the creation of 26 new jobs. The pharmacy chain opened a new store in the Mill Shopping Centre, Clondalkin earlier this month and has also unveiled a major extension of its store in Pavillion Shopping Centre, Swords.
The revamped Swords store in the Pavilions Shopping Centre will create 12 new jobs, bringing the total number of employees at the store to 62. The store expanded its premises from 525 square metres to 750 square metres and now accommodates new premium cosmetic offerings, a range of children's clothing, and a new range of baby bedding, travel and bath products.
The new store is located in The Mill Shopping Centre and was formally opened by RTE presenter Brian Ormond, a native of Clondalkin. The store will be managed by Jackie Doyle and has provided a welcome jobs boost for the town, creating 14 new full-time and part-time jobs.
According to Debbie Smith, Managing Director, Boots Ireland, the expansion in the greater Dublin area is a sign of the company’s commitment to long-term investment in the country. “The major expansion of our store in Swords is due to the strong performance of the store and will accommodate the increasing number of customers visiting the store,” she added.
"We are very pleased to be creating jobs and providing customers with extensive product ranges and excellence in pharmacy goods and services."
The DocMorris pharmacy chain has expanded yet again, with a new pharmacy in Limerick coming under its umbrella.
Located in the Grove Island retail complex in the Corbally area of Limerick, the latest pharmacy to rebrand is now the sixth DocMorris store in the city.
Pharmacy Manager Mary Irwin said that although the business was re-branding under the DocMorris name, the pharmacy’s current six staff were being retained.
“We are very excited about our relaunch as part of the DocMorris pharmacy group,” added Irwin.
The Mayor of Limerick, Cllr Gerry McLoughlin, officially re-launched the pharmacy, and staff presented two cheques of €250 each to the Simon Community and to Limerick Animal Welfare to mark the event.
DocMorris expands in LimerickWith over 70 pharmacy outlets throughout the country, DocMorris is Ireland’s largest pharmacy group. In recent months, five pharmacies in Limerick have re-branded under the DocMorris banner. These are located at the Parkway, Jetland and Roxboro shopping centres and at William Street and Thomondgate.

LISTERINE®
TOTAL CARE ZEROHighly effective yet alcohol-free for a less intense taste
No 1
Daily
Use
Mouth
wash
*
Suitable for patients 6+.References: 1. Data on file 45348, McNEIL-PPC, Inc. 2. Data on file D (Microbiology), McNEIL-PPC, Inc. 3. Data on file 103-0214, McNEIL-PPC, Inc. 4. Le Geros RZ et al. Am J Dent 1999; 12(2): 65-71.
*52 w/e 17.06.12 Irish Nielsen Data
ToTal Care ZeroAdds zero alcohol to the LISTERINE® TOTAL CARE range
POWERED BY 4 ESSENTIAL
OILS
CONTAINS ZINC
CHLORIDE
CONTAINS 220 ppm
FLUORIDE
LISTERINE® TOTAL CARE ZERO
is alcohol-free yet retains the
LISTERINE® brand’s 4 essential oils.
So it has a softer taste1 but it kills up
to 99% of plaque bacteria in vitro,
more than the leading alcohol-free
daily use mouthwash brand.2
In addition, TOTAL CARE ZERO
contains 220 ppm (0.05%) fluoride
with high uptake3 for extra enamel
protection, and zinc chloride to
reduce calculus formation4 and
help keep teeth white.
So when patients want a less
intense, alcohol-free mouthwash,
why not add LISTERINE®
TOTAL CARE ZERO to their
oral care routine?
IRE/LI/12-0054

26 September 2012 • IPN
News
news briefBag yourself a prize Drontal Photo CompetitionPet health remains an untapped business opportunity in many pharmacies. To help promote this service, pharmacists can enter this year’s Drontal Photo Competition, which is sponsored by Bayer. Pharmacists have until 21 September to submit their entry. There will also be a prize for the pharmacy with the best window display.
“The potential for pharmacists to maximise their business opportunities in this area is huge, as pets are such an integral part of so many families,” said Philip Bergin of Bayer Animal Health. “Customers come into pharmacies seeking advice regarding their own health and for medications, so it makes sense for people to be able to buy wormers, dog shampoo and animal vitamin supplements while they are there. The pharmacy can be a one-stop shop in the community for the whole family – including the family pet.
Pet owners need to be educated about why it is so important to worm their pets routinely, Bergin continued.
“This understanding will provide motivation for them to establish a regular worming routine. Regular worming will help to safeguard the health of both the pet and the family.”
Pharmacists interested in hosting the competition in their locality can contact Bayer directly. They will receive:
•aDrontalpharmacyguide,containinginformation about worms and Drontal, which will help them to answer any queries they may receive from customers;
•adataprotectiondocument,whichsets out the pharmacy’s responsibilities regarding data protection;
•detailsoftermsandconditions,sothat that pharmacists are aware of the conditions of entry for their customers.
Contact Sinead Boyle at Bayer HealthCare to obtain a start kit. She will also answer any queries regarding the competition. Telephone: (01) 299 9313.
Staff at Adrian Dunne pharmacy in Balbriggan recently ran the mini-marathon in aid of the Ballbriggan Cancer Support Group.
The ladies along with their friends and
Pharmacy staff raise €1,000families raised a whopping €1,000. A big Thank You to everyone who sponsors the ladies and well done on their great achievement.
Ramona's secret is out!Cara Pharmacy joint Managing Director Ramona Nicholas will be hitting the TV screens shortly demonstrating the extremely generous side to her nature as she battles to help drug addicts and alcoholics in Galway.
Ramona will be seen on televisions across Ireland in September featuring on RTE's 'The Secret Millionaire' programme as she travels to Galway in a bid to support those less fortunate than herself. Those she helps are not aware of her true identity until the final moments on the show when she gives them some of her own money to financially get them back on their feet.
Ramona says: "It was without doubt the best experience of my life and the show is as real as it gets. I will remember every moment of it forever. But as always I wouldnt have been able to do it without the support of a small number of people who are always at my side, and it was extremely tough leaving and coming back to a reality that I didn't feel I was worthy off.
"If I'm honest, I'm still coming to terms with it...an amazing experience, for which I am very grateful to have been offered. I
really appreciate all the messages that I've received."
Offering their words of admiration through a local networking site, her staff praise Ramona's caring nature. '(She) is one of the most generous and caring people we have ever met and we have no doubt she will have truly touched the lives of everyone during her journey. We truly admire the hard work, passion, energy and effort Ramona puts into every aspect of her life and work and we know the show will be a shining example of this.'
Ramona Nicholas, Cara Pharmacy

PA Holder: McNeil Healthcare (Ireland) Limited, Airton Road, Tallaght, Dublin 24, Ireland. PA Number: 823/56/2. Product not subject to medical prescription. Full prescribing information available on request. IRE/IM/12-0055a
Effective relief from
Diarrhoea

28 September 2012 • IPN
Researchers at Trinity College Dublin have broken boundaries in folic acid studies
Report
New research by medics at Trinity College Dublin suggests that folic acid plays a vital role in preventing a major birth defect. This is in addition to the established protection against neural birth defect such as spina bifida The findings show that the risk of having Cleft Lip and Palate (CLP) was more than four times higher if mothers had not taken folic acid in the first trimester.
Trinity postgraduate research student and pharmacist Ms Dervla Kelly is the first author on the paper and Dr Udo Reulbach, an epidemiologist and Clinical Research Fellow, HRB Centre for Primary Care Research and Department for Public Health and Primary Care, Trinity College Dublin, is the joint senior author.
Vital role in folic acid discovered
A cleft lip (CL) is a separation in the upper lip. A cleft palate (CP) is an opening in the roof of the mouth. Clefts result from incomplete development of the lip and/or palate in the early weeks of pregnancy.
During this time the face is being formed - the top and the two sides develop at the same time and grow towards each other, finally fusing in the middle. The lip and primary palate develop at 4 to 6 weeks of gestation, while the secondary palate develops at approximately nine weeks.
According to the cleft lip and palate association of Ireland, clefts affect approximately 1 in every 700 babies in Ireland.
Commenting on the significance of the
research, Trinity’s Professor of General Practice Tom O’Dowd, a senior author on the paper stated: “This study supports the hypothesis of a further significant role of a daily folic acid supplement of 0.4mg taken 4 weeks before conception and in the first 12 weeks of pregnancy in the prevention of Cleft Lip and Palate”.
Using a sample of 11,134 nine-month-olds from the Growing Up in Ireland study, a national study led by TCD and the Economic and Social Research Institute (ESRI), researchers found that over a third of mothers did not take a folic acid supplement prior to becoming pregnant while a minority did not during the first trimester. The main reason for women not taking a supplement was their being unaware that they were pregnant.
This study also highlights the socioeconomic factors associated with not taking folic acid during the first trimester. The benefits of this safe, simple and cheap supplement need to be promoted to all women who have any chance of becoming pregnant, according to the authors.
The Growing up in Ireland study is following the progress of almost 20,000 children across Ireland to collect a host of information to help improve understanding of all aspects of children and their development.The study is taking place over seven years and following the progress of two groups of children; 8500 nine-year-olds and 11,000 nine-month-olds. During this time they have carried out two rounds of research with each group of children.
The main aim of the study is to paint a full picture of children in Ireland and how they are developing in the current social, economic and cultural environment. This information will be used to assist in policy formation and in the provision of services which will ensure all children will have the best possible start in life.
6th All Ireland ConferenceThe 6th All Ireland Pharmacy Conference is being held this year on the 12th and 13th November 2012 at the Ballyscanlon House Hotel, Dundalk. This Conference is held every two years and is funded by the Northern Ireland Centre for Pharmacy Learning and Development (NICPLD) and the Irish Centre for Continuing Pharmaceutical Education (ICCPE).
Its focus is to share good practice in pharmaceutical care across the primary and secondary care sectors and is an important forum that enables pharmacists, pharmaceutical assistants and technicians to exchange ideas for pharmaceutical service development in the North and in the Republic of Ireland.
Visit www.iccpe.ie for more information.


30 September 2012 • IPN
News
news briefWorld Alzheimer's Day to focus on carersSeptember 21 marks World Alzheimer’s Day, when people from 77 countries who are affected by Alzheimer’s disease and related dementias unite in solidarity to raise awareness about these conditions globally.
This year, the focus of World Alzheimer’s Day is to highlight the role and value of dementia carers. In Ireland, more than 50,000 carers are caring for someone with symptoms of dementia. According to a recent survey carried out by the Alzheimer Society of Ireland, many people are caring for more than 14 hours per day without adequate support services, financial supports or training. Social isolation and stress have a significant impact on the health and wellbeing of carers, the survey also revealed.
Pharmacy customers should be advised to visit their doctor if they are experiencing changes to their memory, mood or ability to manage everyday life – for example, if they forget the names of friends or everyday objects regularly; if they find it harder to follow conversations or television programmes; if they regularly start repeating themselves or lose their train of thought when speaking; and feel anxious, angry or frustrated by the changes they are experiencing.
The Alzheimer Society recommends that, in order to reduce the risk of developing dementia, people should: be physically active; be socially active; and eat healthily. Pharmacists can advise customers to eat plenty of fruit and vegetables, oily fish and wholemeal or wholegrain breads and cereals, while reducing the amount of sugar, fat and saturated fat and cutting down on salt. The Alzheimer Society also recommends that people quit smoking and avoid too much alcohol.
There are more than 41,740 people in Ireland with dementia, with the number expected to be in excess of 104,000 by 2036 unless there is a medical breakthrough. Between 2002 and 2036, the number of people with dementia in Ireland is expected to increase by 303 per cent.
Family carers provide 57 per cent of the value of informal care without compensation, while less than 10 per cent of the cost of dementia in Ireland is attributable to community care services
For details on World Alzheimer’s Day events or to inquire about hosting an event in the pharmacy, contact the Alzheimer Society on (01) 207 3800 or [email protected].
Recently published figures have shown a reduction in the number of people waiting for opiod substitution treatment. The figures, compiled by the HSE that show that there was a 19% reduction in the number of people waiting for opioid substitution treatment in the 13 month period from the end of March 2011 to the end of April 2012.
Róisín Shortall, Minister of State at the Department of Health with responsibility for Primary Care said: “I welcome the reduction from 230 to 187 in the number of people on waiting lists for opioid substitution treatment. The provision of timely treatment greatly increases the likelihood of successful outcomes for the patients involved”.
The Minister continued: “Since taking on
Opioid substitution reductionresponsibility for the implementation of the National Drugs Strategy I have made the provision of treatment a priority, with a particular focus on helping people to move on to drug-free lifestyles. The figures released today show that the work being done is having positive outcomes, though much more remains to be done.
“The HSE reported that 22 of its 48 clinics have no waiting times, and that 33 of the 48 have waiting times of less than a month. The longest waiting times are in the Midlands, the North-East and in pockets of Dublin. However even in areas where waiting times remain high, there is a very significant downward trend – from 10 months to 3 months in Athlone, from 7.5 months to less than a month in the City Clinic in Dublin, from 7 months to one month at the Dr. Steven’s Clinic, from 7 months to four months in Louth, and from 7 months to 2 months in Waterford.
“At a time of cut-backs, HSE management and frontline staff deserve credit for making good progress and for doing more with less,” said Ms. Shortall.
The Minister acknowledged that there is a need to develop services further to ensure the provision of access to drug misuse treatment for all within one month of assessment, in line with the aims of the National Drugs Strategy.
University College Dublin student Annalise Murphy received a rapturous reception as she returned home from the Olympic games earlier this month.
Science student Annalise came first in the first four races but suffered the disappointment of a fifth place in the Laser Radial Sailing medal race to finish fourth overall, narrowly missing out on a medal.
Achievement of Olympic standards
Róisín Shortall

See the benefits of combining Ebixa®
with an established cholinesterase
inhibitor earlier in the treatment
of Alzheimer’s Disease1-10*
Ebixa®
Cholinesterase Inhibitor
Ebixa®*
Cholinesterase Inhibitor*
Ebixa®*
Cholinesterase
Inhi
bito
r*
Life is better together
EB3/1/12
* Ebixa (memantine) indicated for moderate to severe Alzheimer’s Disease7
* Cholinesterase inhibitors indicated for symptomatic treatment of mild to moderately severe Alzheimer’s dementia8-10
Abbreviated Prescribing Information: For full prescribing information refer to the Summary of Product Characteristics. Name: Ebixa. Active Substance: Memantine Hydrochloride. Indication: Treatment of patients with moderate to severe Alzheimer’s disease. Dosage & Administration: Treatment should be initiated and supervised by a physician experienced in the diagnosis and treatment of Alzheimer’s dementia. Therapy should only be started if a caregiver is available who will regularly monitor the intake of the medicinal product by the patient. Regular review to assess clinical benefit: The tolerance and dosing of memantine should be assessed regularly, with the first assessment within three months of the start of treatment and thereafter regularly according to current clinical guidelines. Maintenance treatment can be continued for as long as a therapeutic benefit/tolerability continues for the patient. Discontinuation should be considered when therapeutic benefit/tolerability for the patient is no longer present. Treatment is orally either as tablets (10 mg) or solution (5 mg/pump actuation) taken with or without food once a day at the same time every day. The solution should only be dosed onto a spoon or into a glass of water using the pump. Maintenance dose is 20 mg/day (two tablets or 2 ml solution equivalent to 4 pump actuations). Treatment starts with 5 mg/day (half a tablet or 0.5 ml solution equivalent to 1 pump actuation) for the first week; the 2nd week 10 mg/day (one tablet or 1 ml solution equivalent to 2 pump actuations); the 3rd week 15 mg/day (one and a half tablets or 1.5 ml solution equivalent to 3 pump actuations) and the 4th week 20 mg/day (two tablets or 2 ml solution equivalent to 4 pump actuations). Moderate renal impairment 10 mg/day (one tablet or 1 ml solution equivalent to 2 pump actuations) if well tolerated after 7 days the dose could be titrated up to 20 mg/day (two tablets or 2 ml solution equivalent to 4 pump actuations). Severe renal impairment- dose is 10 mg/day (one tablet or 1 ml solution equivalent to 2 pump actuations). Mild-moderate hepatic impairment- no dose adjustment. Severe hepatic impairment- no data available, not recommended. Children & Adolescents: Not recommended. Contraindications: Hypersensitivity to the active substance or any of the excipients. Pregnancy and Lactation: Pregnancy: Ebixa should not be used in pregnant women unless clearly necessary. Lactation: Women taking Ebixa should not breast-feed. Special Warnings and Precautions for use: Caution is recommended in patients with epilepsy. Caution is advised in patients with raised urine pH as this may elevate plasma levels. Clinical trial data are limited on patients with recent myocardial infarction, uncompensated congestive heart failure and uncontrolled hypertension and patients with these conditions should be closely supervised. Avoid concomitant use of NMDA antagonists (see also interactions). Patients should be warned to take special care if driving and using machines as Ebixa has minor to moderate influence on these tasks. Oral solution only: Patients with rare hereditary problems of fructose intolerance should not take Ebixa 5 mg/pump actuation oral solution as it contains sorbitol. Interactions: Effects of L-Dopa, dopaminergic agonists and anticholinergics may be enhanced. Effects of barbiturates and neuroleptics may be reduced. Concomitant administration of Ebixa with antispasmodic agents e.g. dantrolene and baclofen can modify their effects, dose adjustments may be necessary. Increased plasma levels could occur with concomitant use of cimetidine, ranitidine, procainamide, quinidine, quinine and nicotine. Co-administration with hydrochlorothiazide (HCT) may lead to a reduced serum level of HCT. Concomitant use of NMDA antagonists (amantadine, ketamine and dextromethorphan) or phenytoin should be avoided. Close monitoring of prothrombin time or INR is advisable for patients treated concomitantly with oral anticoagulants. Adverse reactions: Common (≥1/100 to <1/10) headache, somnolence, hypertension, constipation, dizziness, dyspnoea and drug hypersensitivity. Uncommon reactions (≥1/1,000 to <1/100): cardiac failure, fatigue, fungal infections, confusion, hallucinations (mainly in patients with severe Alzheimer’s disease), venous thrombosis/thromboembolism, vomiting, gait abnormal. Very rare (<1/10,000): seizures. Not known: Isolated cases of pancreatitis and psychotic reactions have been reported post-marketing. Alzheimer’s disease has been associated with depression, suicidal ideation and suicide. In post-marketing experience these events have been reported in patients treated with Ebixa. Overdose: Symptomatic treatment. Elimination: Mainly in unchanged form via the kidneys. Legal Category: POM. Marketing Authorisation Holder: H.Lundbeck A/S, Ottiliavej 9, DK-2500 Valby, Denmark. Marketing Authorisation Numbers: EU/1/02/219/005 Ebixa 5 mg/pump actuation oral solution-50 ml bottle. EU/1/02/219/006 Ebixa 5 mg/pump actuation oral solution-100 ml bottle. EU/1/02/219/007 Ebixa 10 mg film-coated tablets, 28 pack size. EU/1/02/219/008 Ebixa 10 mg film-coated tablets, 56 pack size. Further information may be obtained from: Lundbeck (Ireland) Ltd., 7 Riverwalk, Citywest Business Campus, Dublin 24.Date of Preparation: October 2011.
References: 1. Patel L et al. Drugs Aging 2011;28(7):539-546. 2. Herrmann N et al. Expert Opin Pharmacother 2011;12(5):787-800. 3. Tariot PN et al. JAMA 2004 Jan 21;291(3):317-24. 4. Feldman HH et al. Alzheimer Dis Assoc Disord 2006 Oct-Dec;20(4):263-8. 5. Lopez OL et al. J Neurol Neurosurg Psychiatry 2009;80(6):600-7. 6. Atri A et al. Alzheimer Dis Assoc Disord 2008 Jul-Sep;22(3):209-21. 7. Ebixa Summary of Product Characteristics. 8. http://www.medicines.ie/searchresults.aspx?term=donepezil. 9. http://www.medicines.ie/searchresults.aspx?term=rivastigmine. 10. http://www.medicines.ie/searchresults.aspx?term=galantamine.
CombinationTherapy
ebixa_advert_mar_2012_A4.indd 1 14/03/2012 11:57

Must Stock OralHealthcare Essentials
Can’t floss, won’t floss? TePe Interdental brushes are the answer to removing plaque and impacted food from between the teeth - and easier to use than floss. The TePe Interdental Brush family includes the ever popular original range and now the TePe Angle.Available in seven colour coded sizes - pink through to purple. www.tepe.comEmail [email protected] for further information - Tel: 01934 710022
bonjela teething gel Teething can be distressing time for mums as your baby may experience some pain and discomfort as those first little teeth start to appear .
Help bring back their smile with New Bonjela Teething Gel. Its specifically designed for babies and can be used from 4 mths . The NEW fast gel not only helps to relieve your baby’s teething pain but also fights infection and reduces gum inflammation. Available in pharmacy and Grocery.
Oral B 3D White BrillianceOral B New 3D White Brilliance Tooth Paste provides a whiter smile in just 2 weeks removing up to 80% of surface stains. Its 3D technology helps clean the front, back and visible gaps between teeth, meaning teeth are naturally white from every angle. The unique Dual Silica Cleaning and Polishing System - whitens teeth by gently tackling and lifting stains revealing the natural whiteness of the teeth. Pyrophosphate Chemical Stain and Tartar Prevention System – enforces stain prevention. The Fluoride Technology helps strengthen and protect teeth.
Oral B 3D White Brilliance 75ml RRP* €4.65*All pricing is at the sole discretion of the retailer.
For more information visit www.oralb.co.uk
Oral B Trizone BrushAfter seven years of clinical trials, Oral-B has launched a new innovation in power brushes. The new Oral BTri-Zone has been designed to look and feel like an ordinary manual toothbrush -with the incredible cleaning benefits of a power brush. It works unlike any other brush to deliver an invigorating in-between teeth clean. Its dynamic triple zone bristles brush away 2X more plaque ** and reach plaque hidden deep between teeth.
For more information visit www.oralb.co.ukOral B Trizone 600 RRP* €66.49
Refill head 2 pack RRP* €13.99 *All Pricing is at the sole discretion of the retailer**than a manual tooth brush
Our mouths are one of our most valuable workplace tools and yet, we put them through so much without even thinking about it.
Endless tea and coffee swishing can cause stains, nervous pen-chewing can fill our mouths with germs and can damage our gums, naughty, sugary office treats can cause plaque and cavities and those lunches on-the-go can leave you with bad breath.
But thanks to LISTERINE, you can protect your top professional asset from the perils of everyday life.
The new iWhite Pure Professional is an instant teeth whitening kit for professional whitening results at home.
You will see an immediate effect after the first application! This innovative, one step system will also actively remove stains and strengthen your teeth. It’s easy to wear and to use.
The product is composed of 10 thin and flexible trays to ensure a comfortable fit and maximum performance.
Price €29.99
Now available in Northern Ireland
Ph: 01 2762291E-mail:[email protected]
CYMEX CREAMCymex 5 g Cream offers effective fast relief from cold sores and starts working from the moment you use it.
Cymex Cream has a unique triple action formula. It acts by soothing the tingling sensation of cold sores, relieves painful chapped lips and controls infection helping to get your lips back in top form. Available from Actavis Ireland Ltd.
Always read the Label. Contain Oromucuosl Gel , Choline salicylate 8.71% , Cetalkonium choloride 0.010%

Biography - Eamonn Brady MPSI is the owner of Whelehans Pharmacy in Mullingar. He graduated from the Robert Gordon University in Aberdeen in 2000 with a Masters in Pharmacy. He worked for Boots in the UK before moving back to Ireland in 2002. He bought Whelehans Pharmacy in Mullingar in 2005. He undertakes clinical training for nurses in the midlands.
CPD 21: OSTEOPOROSIS
Osteoporosis
SponsoredbyPfizer
60SecondSummaryOsteoporosis literally means "porous bones". It's a condition where bones lose density causing them to become weak and more likely to fracture. About one in two women and one in five men over 50 will fracture a bone because of osteoporosis.
Osteoporosis is usually diagnosed in hospital, often after a fall or a bone fracture. Bone density is measured using a dual-energy X-ray absorptiometry (DEXA) scanner. Osteoporosis is diagnosed when bone density is found to be significantly lower than average. DEXA scans are the gold standard for the diagnosis of osteoporosis.
There is no comprehensive osteoporosis screening programme in Ireland. People generally only get a DEXA when referred by their GP. Non-pharmacological management includes prevention of falls and modification of risk factors including: diet, smoking and excessive alcohol intake.
Learning, Evaluation, Accredited, Readers, Network | www.learninpharmacy.ie
SYMPTOMS OF OSTEOPOROSIS
Osteoporosis may have no symptoms initially, and patients may be unaware of any problems until they fracture a bone or start to lose height.
Symptoms can include:
• Sudden, severe episodes of upper, middle or lower back pain
• Loss of height (greater than 2cm)
• Development of a hump on the back or a change in body shape, for example, the rib cage may rest on pelvic rim or a pot belly develops
COMPLICATIONS OF OSTEOPOROSIS
Broken wrists, hips and spinal bones are the most common fractures in people with osteoporosis. Fractures can, however, occur in any bone. They can result in pain, disability, loss of independence and a drop in self esteem.
DIAGNOSIS OF OSTEOPOROSIS
Osteoporosis is usually diagnosed in
hospital, often after a fall or a bone fracture. Bone density is measured using a dual-energy X-ray absorptiometry (DEXA) scanner. Osteoporosis is diagnosed when bone density is found to be significantly lower than average. DEXA scans are the gold standard for the diagnosis of osteoporosis. Scans are painless and take approximately 10 to 20 minutes.
The results of the scan will be made available immediately or very soon after, depending on where it is done. Scan results will be given in the form of a T-score. A T-score value greater than -1 shows that bone density level is normal and there is no osteoporosis. A T-score value of between -1 and -2.5 indicates osteopenia. This is the early stage of osteoporosis and is a warning that a patient must start taking care of their bones. A T-score of below -2.5 meanwhile indicates osteoporosis.
There is no comprehensive osteoporosis screening programme in Ireland. People generally only get a DEXA when referred by their GP. The average waiting time to get a DEXA scan in 2008 for public patient was 20 weeks15. Private patients can get a scan
1. REFLECT - Before reading this module, consider the following: Will this clinical area be relevant to my practice.
2. IDENTIFY - If the answer is no, I may still be interested in the area but the article may not contribute towards my continuing professional development (CPD). If the answer is yes, I should identify any knowledge gaps in the clinical area.
3. PLAN - If I have identified a knowledge gap
- will this article satisfy those needs - or will more reading be required?
4. EVALUATE - Did this article meet my learning needs - and how has my practise changed as a result?Have I identified further learning needs?
5. WHAT NEXT - At this time you may like to record your learning for future use or assessment. Follow the 4 previous steps, log and record your findings.
Published by IPN and supported with an unrestricted educational grant from Pfizer Healthcare Ireland. Copies can be downloaded from www.irishpharmacytraining.ie
Disclaimer: All material published in CPD and the Pharmacy is copyright and no part of this can be used within any other publication without the permission of the publishers and author.
Osteoporosis literally means “porous bones”. It’s a condition where bones lose density causing them to become weak and more likely to fracture. About one in two women and one in five men over 50 will fracture a bone because of osteoporosis. According to the Osteoporosis Society of Ireland, it is estimated that 300,000 people in Ireland have osteoporosis. Osteoporosis can affect all age groups, but it’s most common in postmenopausal women. Having osteoporosis doesn’t automatically mean that bones will fracture; it just means that it’s more likely. In Europe osteoporosis accounts for more disability than many non-communicable diseases including rheumatoid arthritis, Parkinson’s disease and breast cancer1.

CPD 21: OSTEOPOROSIS
upon request in private facilities. The website of the Osteoporosis Society of Ireland has a comprehensive list of all locations in Ireland where DEXA scans are performed. It lists DEXA scan locations on a county by county basis and includes both private and public hospitals and clinics. Click on “Arrange a scan” on the Osteoporosis Society website to find a location closest to you.
CAUSES OF OSTEOPOROSIS
Healthy bone consists of a strong mesh made of protein and minerals (particularly calcium). This mesh is living tissue that is constantly being renewed by two types of cells. One type builds up new bone (osteoblast cells) and the other breaks down old bone (osteoclast cells). Up to our mid-20s our skeleton is strengthened, but from our 40s onwards our bones gradually lose their density as a natural part of ageing.
There is a genetic influence on osteoporosis so women with family members with the condition are more at risk. However other factors increase the risk of osteoporosis.
The breakdown of bone is quicker in women who have been through the menopause. This is because of a lack of the hormone oestrogen. Oestrogen reduces the amount of bone broken down and so helps to protect against osteoporosis. In women, oestrogen is made in the ovaries from puberty until the menopause. Anything that reduces the number of years that a woman produces oestrogen may increase the risk of osteoporosis. These include:
• an early menopause (before the age of 45)
• a hysterectomy before the age of 45 (especially if both ovaries are removed)
• excessive exercising - this can reduce hormone levels and as a result, periods may stop for a prolonged time
Other factors include:
• age - the risk increases with age
• race - Caucasian or Asian races are at greater risk than African-Caribbean
• gender - women have smaller bones than men
• a family history of osteoporosis, particularly a history of hip fracture in a parent
• a previous fragility fracture (fracturing a bone after only a minor accident)
• long-term immobility (e.g. confined to bed)
• a very low body mass index
• excessive alcohol consumption or smoking
• low levels of vitamin D or dietary calcium
Some medication and disorders can increase risk including:
• long-term use of corticosteroids
• long-term use of heparin
• aromatase inhibitors (for breast cancer treatment)
• overactive thyroid disorders
• rheumatoid arthritis
• digestive disorders that affect nutrient absorption, such as Crohn’s Disease, chronic liver disease, or coeliac disease
CAUSES IN PRE-MENOPAUSAL WOMEN
Oestrogen generally prevents osteoporosis in pre menopausal women. However there are certain medical conditions and medication which reduce oestrogen level and hence causing early onset osteoporosis.
Examples include:
• Hypogonadotropic hypogonadism due to low weight, eating disorders, excessive exercise, hyperprolactinemia, and hypopituitarism.
• Hypergonadotropic hypogonadism (premature ovarian failure) is associated with bone loss if oestrogen is not replaced. Women with Turner syndrome (condition which occurs in less than 1 in 2500 due to abnormal X chromosome) may have an additional selective reduction in bone mineral density that is independent of oestrogen exposure.
• In premenopausal women with breast cancer, chemotherapy often results in premature ovarian failure, and as a result, oestrogen deficiency and bone loss.
Drugs that may be associated with bone loss in premenopausal women include glucocorticoids, anticonvulsants (e.g.) phenytoin, antidepressants (e.g.) Lithium and anticoagulants (e.g.) warfarin and heparin.
NON PHARMACOLOGICAL MANAGEMENT
Non-pharmacological management includes prevention of falls and modification of risk factors including: diet, smoking and excessive alcohol intake. Important measures aimed at preventing falls include attention to modifiable factors including: checking eyesight, exercise, reduced consumption of medication that alters alertness and balance, and improvement of the home environment. There is controversy on the use of hip protectors to prevent fractures, with recent evidence casting doubt on this preventive measure.2, 3. Attention to diet is important, because there is a high prevalence of calcium and vitamin D insufficiency in the elderly, particularly those with chronic conditions. Calcium is necessary for maintaining bone health and vitamin D enhances the absorption of calcium. A diet with adequate calcium (>1,200mg daily) and vitamin D (800 IU daily) is recommended for those with risk factors.
Adults over 50 years often only consume 700mg calcium daily, so the use of supplements, including fortified food products, may be required.
Evidence for the use of calcium and vitamin D supplements to maintain optimum bone density in healthy adults with normal dietary intake is limited.4, 5 However a recent systematic review found that the ingestion of calcium or calcium with vitamin D reduced osteoporotic fractures in men and women over 50 years by 12%.6 They should be considered for patients in nursing/residential homes and the housebound elderly. Immobilisation is an important cause of bone loss and should be avoided whenever possible.
SponsoredbyPfizerLearning, Evaluation, Accredited, Readers, Network | www.learninpharmacy.ie

SponsoredbyPfizerLearning, Evaluation, Accredited, Readers, Network | www.learninpharmacy.ie
CPD 21: OSTEOPOROSIS
SELF HELP
Osteoporosis patients need to be careful of vigorous, high-impact exercise. However, leading an active lifestyle will improve balance, coordination and develop muscle strength. All these can reduce the risk of falling and fracturing a bone.
Beneficial exercise includes swimming, gardening, walking and golf. Eating a diet rich in calcium is important for maintaining healthy bones. Dairy products and green leafed vegetables are good sources of calcium. Low or non-fat versions of dairy products deliver just as much if not more than their fattier counterparts. If a patient cannot stomach dairy, calcium-fortified orange, grapefruit, and apple juice contain just as much as milk does.
The body also needs vitamin D to absorb calcium properly. Vitamin D is found in certain foods, including cod liver oil, oily fish such as sardines and herrings, margarine and egg yolks. It’s also made by the skin when exposed to sunlight. The National Osteoporosis Society recommends about 20 minutes of sun exposure to the face and arms, every day during the summer, to provide enough vitamin D for the year. Avoid fizzy drinks and reduce caffeine, salt or animal protein, as these can affect the balance of calcium in the body.
NEW RESEARCH ON VITAMIN D
New research has found that a daily supplement of 700 to 1000IU of vitamin D reduces the risk of fractures from falls among older people by 19%. In-fact the British Medical Journal shows that a dose of less than 700IU per day has no effect in reducing fractures. For example, an Ideos® or a Calcichew D3® tablet only has 400IU (500mg) of vitamin D, therefore it important that a patient takes two daily to get the sufficient amount of vitamin D.
RISK OF OSTEOPOROSIS FROM CORTICOSTEROIDS
Patients on corticosteroids require preventive treatment for osteoporosis if the patient is starting oral corticosteroids and is likely to be on these for at least 3 months. More than three or four courses of corticosteroids taken in the previous 12 months is considered to be equivalent to more than 3 months of continuous treatment. If the intermittent courses are spread over a much longer term, the risk is not as high. Evidence supports the use of bisphosphonates as a first line treatment.
PHYSIOTHERAPY FALLS PREVENTION PROGRAMME
Many physiotherapy departments in Ireland have a falls prevention programme that GPs or hospital consultants can refer patient to.
Patients with a history of falls, fear of falling and/or reduced mobility are often referred to a physiotherapy falls prevention programme. The programme is often based on the OTAGO exercise programme and aims to strengthen muscles thus preventing falls and reducing the risk of fracture if the patient does fall. Contact the physiotherapy department at your local hospital to check if this programme is available in your area.
HSE FALL PREVENTION POLICY
The following is the HSE fall prevention policy outlined in their 2008 fall prevention report.15:
All older persons should be asked the following at least once a year:
• Have you fallen during the past year? If yes, did you fall more than once?
• Have you any problems with your balance?
• Are you afraid of falling?
Older persons who have had a single explained fall should be tested for gait and balance annually.
Older persons who:
• have recurrent falls (2 or more in the last year)
• had an unexplained fall
• have problems with gait and balance or
• have a fear of falling
should undergo a multi-factorial assessment carried out by an experienced clinician.
The HSE state in their report that the following risk factors and interventions that have been shown to reduce falls and should be included in multi-factorial assessment and intervention are:
• Individualised exercise programme that includes a combination of resistance training, gait, balance, and co-ordination training
• Medication review and withdrawal of psychotropic and other medications
• Home environment assessment and modification by health professional
• Managing postural hypotension.
• Vision assessment and referral for intervention
• Assessment for Vitamin D deficiency and insufficiency and treated if identified
• Identification of foot problems and
appropriate treatment
• Behavioural modification and educational programmes should be considered
The following is a recommendation for Residential Long Stay Care settings in the 2008 HSE Fall prevention report.15
• All residential care settings should have a fall prevention policy and be resourced to implement it.
• All residents should receive a Fall Risk Assessment annually. A Fall Risk Assessment should also take place on admission and when health status changes occur.
• Falls in residential care and nursing care homes should be recorded on a register. Each fall should be critically analysed for corrective action.
The fall prevention procedures of residential care homes are assessed in all Health Information and Quality Authority (HIQA) inspections.
MEDICATION
Bisphosphonates. Examples include Alendronic Acid, Risedronic Acid and Ibandronic Acid. They work by slowing down bone loss. They are taken once weekly but Ibandronic Acid (Bonviva®) is once a month. They can reduce the frequency of fractures by 50%. Bisphosphonates have been used in trial extensions for up to 10 years, which suggest that bone quality remains normal and that reductions in fracture risk are sustained for as long as treatment continues.7 However, it is important it is reviewed every two years. There is no difference in the efficacy or safety profiles of biphosphonates in the patients aged under 65 and over 65.
The oral bioavailability of bisphosphonates is
SponsoredbyPfizerLearning, Evaluation, Accredited, Readers, Network | www.learninpharmacy.ie
CPD 21: OSTEOPOROSIS
low and impaired by food. Oral formulations must be taken fasting, sitting upright with a full glass of water, followed by no food for up to 1 hour. This is to reduce the gastrointestinal effects experienced by patients. Compliance with treatment is a problem, particularly in view of these requirements. 8,9,10 The most common side effects are gastrointestinal including non-ulcer dyspepsia, oesophagitis, oesophageal strictures (narrowing of oesophagus), gastric and duodenal ulcers. Bisphosphonates are contraindicated in the presence of abnormalities of the oesophagus, and hypocalcaemia. There have been reports of osteonecrosis of the jaw (ONJ) reported with their use, particularly with IV formulations given in high doses for metastatic bone disease.11-13 ONJ is a condition where the jaw breaks. The prevalence of ONJ with biphosphonates has been estimated to be about 1 in 100,000 patient-years, which is similar to the prevalence in the overall population.13
Strontium ranelate (e.g.) Protelos® may be prescribed this if a patient can’t take bisphosphonates. This drug stimulates new bone to grow and reduces bone loss. It is taken once daily, it is a sachet put in water. Trials show it reduces vertebral fractures by 41% and hip fractures by 36%. It should be used with caution in patients at increased risk of venous thromboembolism (VTE); there have been reports of VTE, even though a causal relationship has not been established.4
Parathyroid hormone peptides (e.g.) Forsteo®. It works through the fact it is very similar to parathyroid hormone; this hormone helps to regulate calcium levels and the activity of cells involved in bone formation. It is a subcutaneous injection (into side of stomach usually), one injection is used daily. A trained nurse from Lilly will give training in the patient’s home initially for free. Trials show it reduces fractures by average of 41%. It is only used if a patient cannot tolerate other treatments. The most common adverse effects are nausea, limb pain, headache and dizziness. Contraindications include severe renal impairment, pre-existing hypercalcaemia and metabolic bone disease other than primary osteoporosis
The selective oestrogen receptor modulator (e.g.) Raloxifene (Evista®). This is a synthetic hormone that mimics the effect of oestrogen on the bones. One tablet is taken daily. It reduces risk of fractures by approx 47%.
There have been no studies to show the effect of Evista® for more than 5 years. However according to the manufacturer there is no minimum time that Evista should be used once an improvement has been shown.
Raloxifene has been associated with an increased risk of venous thrombosis similar to that for hormone therapy, and with exacerbation of hot flushes.14 An increased risk of death due to stroke has been reported with raloxifene, and it should be used with caution in women with a history of, or risk factors for, stroke. It is contraindicated in women with child-bearing potential, history of venous thromboembolism (VTE) or unexplained uterine bleeding, hepatic impairment and severe renal impairment.
Hormone replacement therapy (HRT) relieves symptoms of the menopause by restoring hormones to a premenopausal level. HRT has also been shown to reduce osteoporosis. The use of HRT for osteoporosis prevention is restricted to short-term use for younger post-menopausal women with menopausal symptoms at high risk of fracture.1
References
1 National Osteoporosis Guideline Group - Executive summary of Osteoporosis: Clinical guideline for prevention and treatment downloaded from http://www. shef.ac.uk/NOGG
2 Sawka A, Boulos P, Beattie K, Thabane L, Papaioannou A et al, Do Hip protectors decrease the risk of hip fracture in institutional and community dwelling elderly? A systematic review and meta-analysis of randomized controlled trials. Osteoporosis International 2005; 16:1461-1474
3 Kiel D, Magaziner J, Zimmerman S, Ball L, et al, Efficacy of a hip protector to prevent hip fracture in nursing home residents. JAMA 2007; 298:413-422
4 Kanis JA, Burlet N, Cooper C, Delmas PD, Position Paper: European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporosis International 2008; 19:399-428
5. Qaseem A et al, Pharmacologic Treatment of Low Bone Density or osteoporosis to prevent fractures: a clinical practice guideline from the American college of physicians. Ann Intern Med 2008; 149:197-213
6. Tang BMP, Eslick GD, Newson C, Smith C, Bensousson A, Use of supplementation or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: a meta-analysis. Lancet 2007; 370:657-66
7. Liberman UA, Long-term safety of bisphosphonate therapy for osteoporosis – a review of the evidence. Drugs Ageing 2006; 23: 289-298
8. Rabenda V et al, Adherence to bisphosphonate therapy and hip fracture risk in osteoporotic women. Osteoporosis Int 2008; 19: 811-818
PfizerHealthcareIrelandarecommittedto supporting the continuous professional development of pharmacists in Ireland. We are delighted to be partnering with Irish Pharmacy News in order to succeed with this.
Throughout the year, Irish Pharmacy News will deliver 12 separate modules of continuous professional development, across a wide range of therapy areas. These topics are chosen to support the more common interactions with pharmacy patients, and to optimise the patient experience with retail pharmacy.
We began the 2011 programme with a section on the Gastrointestinal System. Other topics include Diabetes (Types I and II), the Cardiovascular System, Smoking Cessation, Infections, Parkinson’s Disease, Alzheimer’s Disease, Depression and others. Wehopeyouwillfindvalueinalltopics.
Pfizer’ssupportofthisprogrammeisthe latest element in a range of activities designedtobenefitretailpharmacy.Otherinitiatives include the Multilingual Pharmacy Tool, a tailored Medical Communications Programme, Educational Meetings and Grants, our Patient Information Pack, new pharmacy Consultation Room brochures and other patient-assist programmes including the Quit with Help programme and www.mysterypain.ie.
If you would like additional information on any of these pharmacy programmes, pleasecontactPfizerHealthcareIrelandon01-4676500 and ask for the Established Products Business Unit.
EPBU/2012/066
9. Chaiamnuay S, Saag K, postmenopausal osteoporosis. What have we learned since the introduction of bispohosphonates? Rev Endocrine Metabolic Disorder 2006; 7:101-112
10 Lekkerkerker F et al, Adherence to treatment of osteoporosis: a need for study, Osteoporosis International 2007; 18:1311-1317
11 Edwards B et al, Pharmacovigilance and reporting oversight in US FDA fast-track process: bisphosphonates and osteonecrosis of the jaw. Lancet oncology 2008; 9:1166-1172
12 Bisphosphonates and osteonecrosis of the jaw in Drugs Safety Newsletter, Irish Medicines Board 2006; 23: 2. Available on www.imb.ie
13 Reid IR, Cundy T, Osteonecrosis of the jaw. Skeletal Radiolog 2009; 38:5-9
14. SPC for Evista® (raloxifene) www.medicines.ie
15 HSE. Strategy to prevent falls and fractures in Ireland’s ageing population. Report of the National Steering Group on the Prevention of Falls in Older People and the Prevention and Management of Osteoporosis throughout Life. June 2008; p66, 69

• Costs 40% less thannearest competitor1*
• No.1 in Ireland*
• Available in 100 tablet and 60 tablet packs
CALCICHEW-D3 FORTE CHEWABLE TABLETS PRESCRIBING INFORMATION.(Please refer to full Summary of Product Characteristics whenprescribing). Presentation: Chewable tablet containing 1250mg calciumcarbonate (equivalent to 500mg of elemental calcium) plus 400IU colecalciferol(equivalent to 10 micrograms vitamin D3). Uses: Prevention and treatment ofvitamin D/calcium deficiency. Supplementation of vitamin D and calcium as anadjunct to specific therapy for osteoporosis, in pregnancy, in established vitaminD dependent osteomalacia and in other situations requiring therapeuticsupplementation of malnutrition. Dosage and administration: Oral (suck orchew). Adults and elderly: Two tablets daily. Children: Not intended for use inchildren. Hepatic impairment: No dose adjustment required. Renal impairment:Should not be used in patients with severe renal impairment.Contraindications: Diseases and/or conditions resulting in hypercalcaemiaand/or hypercalciuria, severe renal impairment, renal stones, hypervitaminosisD, hypersensitivity to ingredient(s) Precautions: Monitor serum calcium andcreatinine levels, particularly in patients on cardiac glycosides or diuretics andin patients with high tendency to calculus formation. Use with caution inpatients with impaired renal function. Take into account risk of soft tissuecalcification. Avoid in patients with phenylketonuria or sugar intolerance.
Prescribe with caution in patients with sarcoidosis. Use with caution inimmobilised patients. Additional doses of calcium or vitamin D should only betaken under close medical supervision. Interactions: Tetracyclines (take 2hours before, or 4 to 6 hours after Calcichew-D3 Forte), bisphosphonates orsodium fluoride (take 3 hours before Calcichew-D3 Forte), Quinolone antibiotics(take two hours before or after), levothyroxine (take four hours before or after),thiazide diuretics, corticosteroids, cardiac glycosides, ion exchange resins(cholestyramine), laxatives (paraffin oil). Calcichew-D3 Forte should not betaken within 2 hours of eating foods high in oxalic acid (e.g. spinach andrhubarb) or phytic acid (e.g. whole cereals). Side effects: Hypercalcaemia,hypercalciuria, constipation, dyspepsia, flatulence, nausea, abdominal pain,diarrhoea, pruritus, rash, urticaria. Very rarely (usually only seen on overdose)milk-alkali syndrome. Use in pregnancy and lactation: Can be used in case ofcalcium and vitamin D deficiency. Daily intake in pregnancy should not exceed1500mg calcium and 600IU colecalciferol (15 micrograms vitamin D3). Avoidoverdose as permanent hypercalcaemia affects developing foetus. Calcium andvitamin D3 pass into breast milk so consider this when giving additional vitaminD to the child. Pharmaceutical precautions: Do not store above 30°C. Keepcontainer tightly closed to protect from moisture. Legal category: Pharmacy
product. Product Authorisation No: 535/1/3. Product Authorisation holder:Shire Pharmaceuticals Ltd., Hampshire International Business Park, Chineham,Basingstoke, Hampshire RG24 8EP UK. Distributed in Republic of Ireland by:Cahill May Roberts, P.O. Box 1090, Chapelizod, Dublin 20, Republic of Ireland.Further information is available on request. Date of revision: May 2011.CALCICHEW is a registered trademark of Shire Pharmaceuticals Ltd in theRepublic of Ireland.
Adverse events should be reported to the Pharmacovigilance Unit atthe Irish Medicines Board (IMB) ([email protected]).Information about adverse event reporting can be found on the IMBwebsite (www.imb.ie). Adverse events may also be reported to ShirePharmaceuticals Ltd on +44 1256 894000.
Reference: 1. MIMS May 2012.
Date of preparation: June 2012.Item Code: IRE/BU/CDF/12/0007.*According to IMS unit sales data April 2012.
Their strength is our forte
HELP PROTECT THEFRAGILE ELDERLY
NEW60 TABLETPACK
Calcichew New Pack A4_Layout 1 03/07/2012 15:30 Page 1

38 September 2012 • IPN
Skincare
As the nights draw in and the weather gets a little colder, people tend to cover up as T-shirts and sandals are packed away for another year. This is the time of year which brings its own skincare issues. It also offers pharmacies an opportunity of meeting the needs of customers who struggle with dry skin.
Before addressing aesthetic issues, it is important to stress to customers the importance of year-round sun protection factors (SPFs). It is a myth that overcast skies mean that one can cut back on sunscreen use. Depleting ozone levels have led to stronger UVB burning rays, while clouds do little to filter out the UVA ageing rays.
In addition, the typical Irish complexion – fair, with light-coloured skin that freckles or burns easily – is particularly susceptible to skin cancer. Skin cancer is the most common cancer in Ireland, with just over
Winter Skincare
8,000 new cases diagnosed in this country every year.
According to the Nation Cancer Registry of Ireland, the incidence of invasive melanoma for women in Ireland is one of the highest in Europe (fourth highest of 26 countries). The incidence rates for men in Ireland are lower in relative terms (eighth out of 26), but is still above the European average. The good news is that customers can be assured that nine out of every ten cases of skin cancer can be prevented.
PERSONALISED SERVICE AND ADVICE
Much of the Irish Cancer Society advice could be passed on to pharmacy customers – bearing in mind that they would not otherwise receive such advice from a supermarket or a grocer. The pharmacy can offer an extra level of personalised service and advice.
The Society states that sunscreens should be worn all the year round and they should be applied 30 minutes before going out into the sun. They should also offer protection against both UVA and UVB rays and have a SPF of at least 15.
In winter, when skin tends to be drier, customers should be counselled on the necessity of using a moisturiser with a broad-spectrum SPF 15 to hydrate and protect. People with dry skin should be advised to use richer, creamier formulations than they would in summer. Milder and gentler soaps should also be used during the colder months. Even oily skin is affected by cold weather. And, without some added protection, the skin’s barrier function becomes compromised, which means that pollution and other damaging elements can affect it, while moisture is lost.
If a customer’s skin is oily, they should be advised to try a gel or lotion formula in winter, rather than forego moisturisers. Customers with combination skin may need different moisturisers for different areas – they should be advised to try a richer, creamier formulation for dry patches and a lighter formula for oily areas such as the ‘T-zone’ (forehead, nose and chin). Take advantage of the opportunity to provide a better buying experience to the customer than they would receive in another retail store.
In typical cases of dry, winter skin, fine lines become more visible; the skin feels rough and appears dull and flaky. In more advanced cases, ‘fishnet’-like cracks occur – these may resemble the fine lines of cracked porcelain. Dry skin, otherwise called xerosis or asteatosis, occurs most commonly on the arms, legs and feet, but can also affect the trunk of the body.
It is important to recognise the difference between typical dry skin and something more problematic. Colder weather, unfortunately, may prompt flare-ups of problem skin conditions.
SPECIFIC SKIN CONDITIONS
When dry skin becomes red and inflamed, as well as being dry and scaly, dermatitis may have developed. This will look like

Oatmeal has long been used for its soothing and cleansing qualit ies as an
essential part of the management of dry skin conditions.
Committed to advancing the science behind oats, AVEENO® scientists have
recently discovered and isolated Avenanthramides, a polyphenolic extract of
oats that enhances the anti-irritant benefits of colloidal oatmeal.
Avenanthramides are the most potent fraction of oats,
outper forming other oat components 5 to 1 in terms of reducing
UV-induced redness 24 hours af ter dermal application.1
A four week clinical study in regimen on 23 subjects with dry
skin conditions aged between 3 months and 5 years old,
found that the daily use of DERMEXA Soothing Emoll ient
Wash and a twice daily application of DERMEXA Soothing
Emoll ient Cream showed a signif icant improvement in the
condition of dry skin. At 4 weeks, dermatologist grading
showed a decrease in skin dryness of 41.5%,, a 48.9%
reduction in roughness with itching declining 50.2% 2
versus baseline.
AVEENO® DERMEXA, uniquely formulated with
oat extracts + Ceramides + Panthenol soothes skin,
reduces itch and helps replenish the skin barrier.
The Power of Oats;
To Soothe and Hydrate Dry Skin Conditions
Suitable for babies as young as 3 months
1. Vollhardt J. Fielder D, Redmond MJ. Identif ication and Cosmetic Application of Power ful Anti- Irritant Constituents of Oat Grain. XXIst IFSCC International Congress 2000, Berlin, Proceedings: 395-402. 2. % Improvement in Mean Scores vs. Baseline, p<0,001vs.baseline
+ Fragrance Free
+ Clinically Tested
+ Well tolerated by adults and children as young
as three months with dry skin

40 September 2012 • IPN
Skincare
round, scaly, itchy, red patches, which are scattered over the legs, arms and trunk (nummular eczema). The appearance of yellow crusts or pus in these areas indicate that a bacterial infection is developing. Such cases would require specific antibiotic therapy and customers should be referred to their doctor.
Patients may also present to the pharmacy with eczema. Although this is most commonly found in children, it can continue into adulthood. It is not contagious and, generally, is associated with itchy, swollen skin. It can also become cracked and weepy, resulting in discomfort if not managed properly. It is commonly found on the inside of joints, such as knees and elbows.
If a patient is experiencing a stubborn flare-up, the pharmacist should refer the patient to the GP or dermatologist. If the skin has become drier during the colder months, they should be advised to follow their skincare regime more stringently. Regular moisturising with emollient creams will help to protect the skin’s barrier and reduce the risk of further flare-ups. Eczema is also treated with ointments, steroids and antihistamines, depending on the severity of the symptoms.
Over-the-counter strength cortisone creams and ointments can be helpful, but prescription-strength products are often required to calm severe flare-ups. Customers should be advised that OTC cortisone cream or ointment should only be applied to affected areas, and no more than twice daily. When using both a cortisone product and an emollient, they should always use the cortisone first and the moisturiser second.
The differences between dermatitis and eczema are not always easy for a pharmacist to spot, since the conditions are quite similar. In either instance, customers should be advised to opt for balms, ointments, creams, lotions and emollients that do not contain perfumes, chemicals or other allergens. Many pharmacy-only brands are better suited to treating affected skin than those commonly available in supermarkets. Some of these derma-skincare products include thermal water in their formulations and many have been subject to rigorous trials to verify their effectiveness.
Most commercial soaps wash away the oils produced by the skin, which normally serve to prevent drying. Advising customers to use a soap substitute, such as aqueous cream, can also help keep the skin moisturised.
Psoriasis is easier for a pharmacist to
determine. This is when the skin’s cells grow too quickly and these skin cells are not shed sufficiently quickly. They pile up on the skin’s surface, causing raised patches or plaques of dry skin, commonly found on the scalp, elbows and knees. Customers should be advised to take note of any flare-up triggers during the winter months and to maintain a good skin regime to help control the symptoms.
Apart from topical treatments, pharmacists might also consider stocking products such as humidifiers to address problem winter skin – using a humidifier will increase moisture levels in the home. Pharmacists should advise customers that keeping the humidity level between 30 per cent and 50 per cent will yield the maximum benefit to parched skin.
(MARKET TRENDS
From a business point of view, the market for skincare in Ireland has traditionally been strong. According to Datamonitor, a provider of global business information, this market increased at a compound annual growth rate of 3.3 per cent between 2004 and 2009 (with the facial care category accounting for a share of 59.2 per cent).
Even the demise of the Celtic Tiger has not dampened Irish enthusiasm for skincare products, with premium skin care holding its own in the Irish market. Euromonitor International, which specialises in strategy research for consumer markets, has reported that the sector continued to perform positively last year. Despite the adverse economic conditions, current value growth for the year was 2 per cent. Premium face masks did particularly well, recording 13 per cent value growth – just the thing for treating dry, winter skin.
Premium firming/anti-cellulite body care, meanwhile, saw current value growth of 5 per cent, and premium facial moisturisers recorded growth of 2 per cent, indicating that although disposable incomes have been reduced, the market potential for premium products still remains strong in Ireland.
Sun care is also performing strongly. In fact, by the end of 2012, Euromonitor has forecast that the sun care market will beworth�9.9millioninIreland,withanexpected compound annual growth rate (CAGR) of 2.6 per cent.
Euromonitor surmised that this growth is down to the ‘lipstick effect’, meaning that women in Ireland are willing to pay a little extra to treat themselves to something, which they consider will be beneficial, especially in relation to their skincare routines.
Sun care is expected to see a constant value CAGR of 1 per cent over the forecast period. Growth is expected to be driven by sun protection and self-tanning, as Irish consumers continue to consider tanned skin more desirable than their natural, paler skin tones.
The recession has failed to dent the customer's desire to look good and maintain healthy skin. This is unlikely to change in the immediate future. Euromonitor states that ongoing innovation and new product development will help to retain interest in the category, ensuring growth into the future. The challenge, it would seem, as consumers become ever more price conscious is to offer more value for money and added services.

Soothes irritated, reddened hands.
Nourishes very dry and damaged skin.
Protects from external factors such as cold, sun, wind, use of detergents…
MAVA-PLUS Hand Cream will calm, soften and smoothe even sensitive skin.
�M�A�V�A�-�P�L�U�S��c�a�n��b�e��o�r�d�e�r�e�d��f�r�o�m��P�e�m�b�e�r�t�o�n��I�n�t�e�r�n�a�t�i�o�n�a�l��L�t�d�,��o�n��0�1��4�6�3�2�4�2�4��o�r��t�h�e�i�r��P�e�m�b�e�r�t�o�n��S�a�l�e�s��R�e�p�r�e�s�e�n�t�a�t�i�v�e�.
SWITZERLAND
Extreme Carefor Hands
Annonce MAVA+ Montagne A 210x297mm.indd 1 30.08.12 13:49
your

42 September 2012 • IPN
Award Category Winner 2012
Locum Pharmacist of the Year Award Winner 2012 - Hilary Dolan
Merging flexibility with changeIt is not always easy being a locum, but the experience brings with it many challenges, as well as rewards. Locums have the opportunity to work across a broad spectrum of pharmacies, from independents to chains, from town to village, from area to area and they can work whenever they want
S P O N S O R E D B Y
Hilary Dolan

IPN • September 2012 43
to work. No two days will be the same and no two pharmacies will be the same.
The winner of the 2012 Locum of the Year Award was nominated for her reliability, honesty and wonderful work ethic. Hilary Dolan worked as a relief pharmacist with
PharmaConex from last September to June of this year. Barbara Kelly, locum co-ordinator with PharmaConex, described Hilary as 'outstanding'.
“It is not easy being a locum,” she said. “They have to be flexible and work to a varying schedule so it is hard for many to establish good working relationships. To be a good locum, the person has to be dedicated, flexible, outgoing and hard-working. That's exactly how I would describe Hilary.”
According to Kelly, the feedback regarding Dolan was consistently excellent on every score, from punctuality down to confidence with customers.
“Hilary worked in over 30 locations all over Dublin during her time with us – and all of the pharmacies in which she worked asked for her to come back,” said Kelly. "She seemed to fit in with the staff and customers wherever she worked."
Dolan returned to Ireland from Scotland last summer, where she had been a
student at the Robert Gordon University in Aberdeen.
“I registered with the Pharmaceutical Society of Ireland in the August,” she told Irish Pharmacy News. “After that, I got a few weeks' work in Donegal, where I am from, before starting as a locum with PharmaConex last September.
“As a new graduate, it was tough,” she said. “But very soon, I came to enjoy locum work and if you really like your work, I think it's easier to do a good job.”
Kelly described how Dolan was an ideal for their company.
“When she started with us, she just got her head down and got on with it. Even when it came to days off or location changes, Hilary was always happy to help in every way.
“As locum co-ordinator, I have worked with hundreds of locums and Hilary would stand out by far as the most suitable person for Locum Pharmacist of the Year in my eyes,” said Kelly.
According to Kelly, Dolan always had time for patients and got to know them individually. Additionally, she worked hard within the dispensary with new initiatives and schemes.
“I just really liked the variety,” Dolan said. “It was such great experience for me. I was the only one of my group from university to work as a locum, but I'd recommend it to any new graduate.”
Flexibility is the key to being a good locum, she said. “You have to be adaptable and you have to always give your best, even though you're only there for a short time. Follow-up is also really important. If I was working in a particular pharmacy one day but in a different one the next day, I would always leave my number with them, in case they needed to query anything.
“Similarly, I'd often call the pharmacy where I worked the previous day if I felt that I needed to follow up on something. I also tried to meet any requests coming from PharmaConex, such as switching pharmacies.
Kelly agreed: “Hilary was the most obliging locum I've ever worked with.”
Dolan stressed that it was also very important to be able to work as a team. “You have to rely on the experience of the others
in the pharmacy, as they know the patients and customers. I would say being able to work as part of a team is also vital if you want to be a good locum.”
It was a busy day in the pharmacy when Kelly said she was going to nominate Dolan for the IPN award. “There were 20 scripts to be filled and I was up to my eyes, so I didn't really realise, initially what Barbara was asking,” she explained. “But I was very flattered. I never really thought I had a chance because I was a newcomer, just out of university and I was amazed even to be shortlisted. To be honest, I was absolutely amazed when I won. I also got the fright of my life!”
The night of the awards ceremony was actually the first time that Kelly and Dolan had met face to face, despite having spoken on the telephone many times.
“It was great evening at the Burlington Hotel and it was the first time that I had met Barbara. Afterwards, I received many messages from other pharmacists for whom I had stood in. That was really nice.”
Dolan has now secured a full-time job and works in Rathgar Pharmacy. Her new employers think it great to have an award-winning member of staff.
“They joked that I'll have to do something brilliant this year so that they can nominate me for a different category next year!” said Dolan.
Kelly is very pleased that Dolan has decided to take on a permanent job and said that PharmaConex were sorry to lose her – as were the many pharmacies that had repeatedly asked for her when they needed a locum.
“It's great to be able to say that we had an award-winning locum working with us,” she concluded.
Hilary Dolan is pictured with Richard Morton, Director, TTM Healthcare

44 September 2012 • IPN
Award Category Winner 2012
Hospital Pharmacist of the Year 2012 - Tim Delaney
Having faith in the anchor that is Tim DelaneyThe lynchpin of all issues pertinent to pharmacy. That is how Tim Delaney has been described by his peers. The executor of awareness and education in patient safety is another.
However on a night of celebration and recognition held in the Burlington Hotel in May of this year, the title simply bestowed upon him was that of 'Hospital Pharmacist of the Year' at the prestigious Irish Pharmacy Awards 2012.
Tim has been working within the hospital pharmacy sector in Ireland for over twenty years and in positions ranging from working within the dispensary to liaising with the profession on behalf of matters related to patient medication safety.
Tim is currently employed as the Medication Safety Programme Lead for the Health Services Executive in Ireland. This is a programme established within the Quality & Patient Safety Directorate. Tim says, "In light of the
S P O N S O R E D B Y
Tim Delaney
Roche Products (Ireland) Limited

IPN • September 2012 45
findingsandrecommendationsintheReportof the Commission on Patient Safety and Quality Assurance, the HSE established the Medication Safety Programme in 2010 and set a number of priority goals.
TASKED WITH ACHIEVING GOALS
"By achieving these goals, we will make practical improvements to the way we manage medicines, and these improvements will result in better treatment for patients and the avoidance of harm." The priorities for 2011-2012 are:
• StandardisetheMedicationPrescription& Administration Record in acute hospitals tofacilitateefficientcareandminimisemedication errors caused by documentation processes.
• Implementmedicationreconciliationattransitions of care between hospitals, long-stay facilities and the community to reduce errors at hand-over of care.
• DevelopanationalMedicationSafetyStandard for Acute Hospitals and a Self-Assessment Tool.
• Establishanaudittoassurecompliancewith safe practice guidance on oral methotrexate for non-cancer treatment (arthritis and psoriasis) in the community.
• AssisttheNationalCancerControlProgramme in designing a system of safe management of Oral Anticancer Medicines for cancer patients.
• Developapracticeresearchprogrammeincollaboration with the universities to ensure that there is a robust collection of evidence to support changes to the way medications are managed.
• Worktowardsintroductionoftechnologytounderpinsafe,efficientworkpracticesin medication management (electronic prescribing with decision support, automated dispensing systems, bar-code technology in drug administration, seamless electronic communication of data throughout the patient journey).
The Medication Safety Programme is charged with making practical improvements to the way medicines are managed, to deliver better, moreefficientcareforpatientsandavoidharm. As Programme Lead, Tim is responsible for a number of initiatives including the standardisation of Medication Prescriptions & Administration Records to minimise medication errors caused by documentation processes as well as addressing the introduction of technology to underpin safe,efficientworkpracticesinmedicationmanagement. These technologies include electronic prescribing with decision support, automated dispensing systems, bar-code technology in drug administration and the seamless electronic communication of data throughout the patient journey.
Prior to taking up this job Tim was Head of Pharmacy and Director of Process
Improvement at Tallaght Hospital, Dublin and from there he was seconded to the HSE. Aswellashispharmacyqualifications,Timearned a Masters degree in Organisational Behaviour from the IMI/Trinity College Dublin. He is a Six Sigma Green belt, which is a processimprovementqualification.
However he is ever humble about his award, and the high regards he is obviously held in by his colleagues within the profession. He says, "I am delighted to receive this Award andIseeitasanaffirmationofmyworkinmedication safety, which is gratifying. I have been fortunate in my hospital pharmacy career to have worked with many excellent colleagues, both pharmacists and technicians whose enthusiasm, intelligence and hard work made so many developments possible.
"However I would like to dedicate this award tothefirstpharmacisIrecruitedwhenIbecame a Chief Pharmacist. Denise Ward Molloy worked with me for twelve years in the Adelaide and Tallaght Hospital. She played a key role in the forging of one team from three as we moved from our three small city centre hospitals to one large one. Her untimely death, just one week before this ceremony, leaving her husband David and two boys bereft, reminds us of how precious and unpredictable life is. I dedicate this award to her."
A WEALTH OF KNOWLEDGE AND EXPERTISE
Tim has extensive experience in pharmacy and healthcare management having held positions as the Head of Pharmacy in Adelaide Hospital (1989-1994), Chief executiveOfficer,AdelaideHospital(1994-1998) and Chief Pharmacist, Tallaght Hospital (1998-2010). He was a member of the Management Team in Tallaght Hospital, with responsibility for Pharmacy, Process Improve, Medical Physics and Clinical Engineering and Catering. Whilst in Tallaght Hospital, Tim establishedIreland'sfirstMedicationSafetyProgramme in the acute healthcare setting, providing a national blueprint for the reporting of medication safety incidents for the purpose of organisational learning and systems improvements.
Tim was a Member of the Commission on Patient Safety and Quality Assurance, convened by the Minister for Health and Children in Ireland to develop recommendations to improvement patient safety. He adds, "The report from the Commission, Building a Culture of Patient Safety, 2008, has since been accepted as Irish government policy. I came to work as National Lead in Medication Safety for the HSE because I was excited about being able to help make coordinated improvements in the way we use medication at national level.
"In my most recent post, amongst other projects, I leads the development of a national medication prescription and administration record (MPAR) for use in acute hospital settings across Ireland."
This project involves extensive consultation, collaboration, feedback and consensus of healthcare professionals at a national level. TheprojectbenefitsfromTim'sconsiderableexperience in continuous improvement and organisational management. This is an extremely complex endeavour, charged with optimising safe use of medication for the management of acute on chronic episodes in multimorbid, polypharmacy patients, with consideration of anticoagulation, blood glucose monitoring and nutritional management. The undertaking of this project will not only result in a national standardised approach for medication management in the acute hospital setting in Ireland but also provides an opportunity to disseminate and share key learnings in organisational change with national and international colleagues.
CAREER PATHWAY
Tim Delaney graduated from Trinity College Dublin with a B.Sc. (Pharm.) degree in 1983 and completed his hospital pharmacy pre-registration training at St Vincent's Hospital, Dublin in November 1984.He worked in various pharmacy posts at the MeathHospital,theCharitableInfirmaryand Beaumont Hospital in Dublin, before becoming Chief Pharmacist at the Adelaide Hospital, Dublin in 1989.In January 1994 hebecameChiefExecutiveOfficerofthe Adelaide Hospital, which was one of three hospitals about to merge to form The Adelaide & Meath Hospital, Dublin Incorporating the National Children's Hospital, When the new hospital opened in June 1998, Mr Delaney became a member of the management executive with portfolio responsibilities for Research, Accreditation & Quality, Medical Physics & Clinical Engineering & Catering, in addition to his role as Head of Pharmacy.
Mr Delaney is a former Secretary and President of the Hospital Pharmacists' Association of Ireland and a former Secretary of the European Association of Hospital Pharmacists (EAHP).He was Executive Vice-Chairman of EAHP Congresses from 1997 to 2000.At Madrid in 2000, he received an EAHP award for outstanding service to European Pharmacy. Mr Delaney is a Governor and member of the Board of the Adelaide Hospital Society and sits on their Health Policy Sub-committee.He is a member of the External Drug Policy Validating Group for St Anne's Service, Roscrea, Ireland - a health system with a mission to care for people with intellectual disabilities. He is an honorary life member of the British Guild of Hospital Pharmacists.
Mr Delaney is a founding member of the Course Co-ordinating and Advisory Committee of the TCD Masters' Degree in Hospital Pharmacy.He lectures on health service structure and funding, and quality management, in that course.
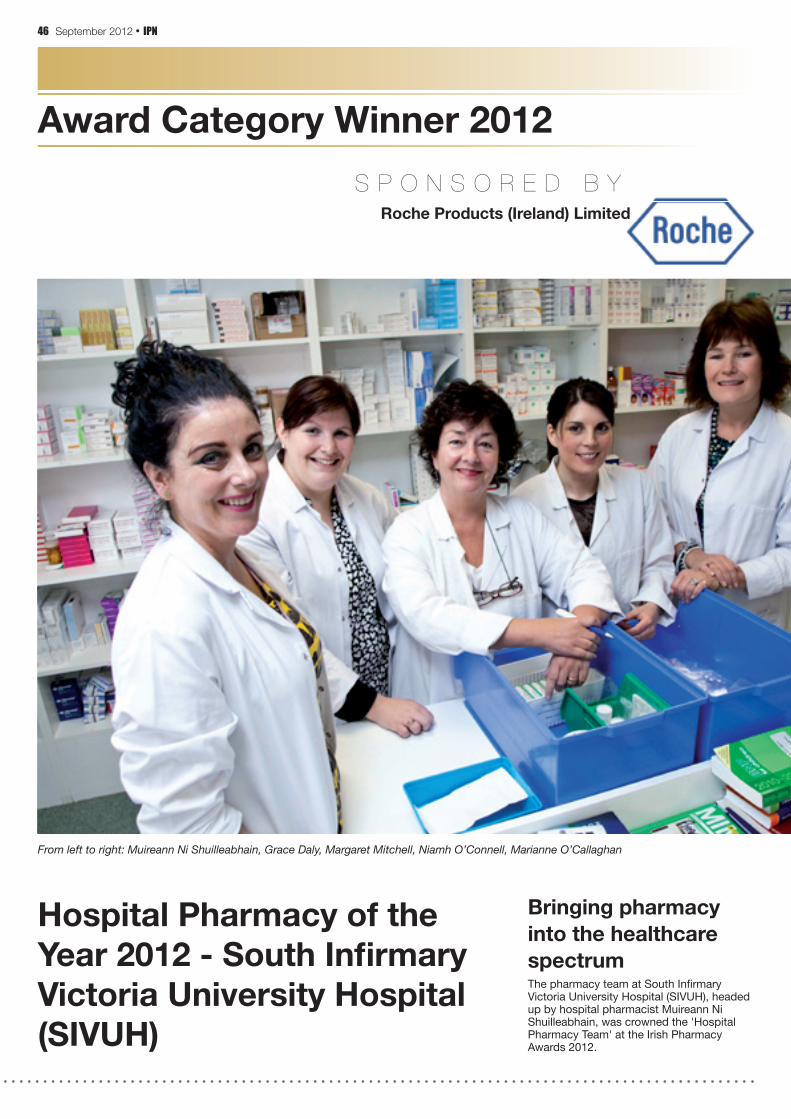
46 September 2012 • IPN
Award Category Winner 2012
Hospital Pharmacy of theYear 2012 - South Infi rmary Victoria University Hospital (SIVUH)
Bringing pharmacy into the healthcare spectrumThepharmacyteamatSouthInfirmaryVictoria University Hospital (SIVUH), headed up by hospital pharmacist Muireann Ni Shuilleabhain, was crowned the 'Hospital Pharmacy Team' at the Irish Pharmacy Awards 2012.
From left to right: Muireann Ni Shuilleabhain, Grace Daly, Margaret Mitchell, Niamh O’Connell, Marianne O’Callaghan
S P O N S O R E D B YRoche Products (Ireland) Limited

IPN • September 2012 47
Muireann and her team fought off tough competition at the prestigious awards held in May of this year at the Burlington Hotel in Dublin. The glittering ceremony aims to recognise the positive innovation and dedication ongoing within the pharmacy profession in Ireland, both in the community
and hospital sectors.
Muireann picks up the story, "2012 has been the year where two of our patient safety andstaffefficiencyprojects have come together and been realised. Our focus has been to bring the Pharmacy team into the wider spectrum of the hospital organisation and the whole pharmacy team has worked tirelessly towards this goal, overcoming many obstacles (mainly logistical and cultural) along the way.
"While both projects are diverse, we think that they showtheflexibilityand complexity of the Pharmacy Department’s services, all of which are rotational, in the delivery of patient centered pharmaceutical care."
ACHIEVING THE IDEAL
The team have been focusing on two novel projects in particular; one looking at a pharmacist medicines reconciliation service and the other focusing on increased efficienciesachievedwith restructuring an
existing model of pharmaceutical care. The timelines for these projects were extremely close, both being implemented December 2011/ January 2012. "This was not ideal, but the pharmacy team realised that this was an opportunity that could not be missed," she says.
The Pharmacy Department at St Vincent's provides a comprehensive range of pharmaceutical services to patients and staff in SVUH. Muireann adds, "Our principal objective is to provide patient-focused pharmaceutical care in order to achieve definiteoutcomesthatimprovepatients’
quality of life. The department has a skill mix of pharmacists and pharmaceutical technicians.
"Clinical pharmacists work closely with doctors, nurses and other members of the multi-disciplinary team to ensure that patients receive optimal pharmaceutical care while attending the hospital. They have a key role in monitoring and reviewing patients and their medications, providing medication counselling where appropriate and liaising with community pharmacy colleagues and GPs to promote seamless pharmaceutical care after discharge."
Thefirstteamprojectinvolvedtheintroduction of a pharmacist in the medicines reconciliation process in the pre assessment stage for elective orthopaedic patients. This involved lengthy proposals, discussions, piloting and planning with a wide team including Planning&Development,Reconfiguration,Anaesthetics, Medical & Surgical teams, Nursing and Hospital Management staff.
"In the medication reconciliation process we focus on the concept of a single list to document patient’s current medications. This list is completed by the pharmacist at the pre assessment interview stage and then utilised as the “one source of truth” medication list by all medical, nursing, pharmacy and other HCP staff. The list is verifiedbythepreassessmentpharmacist(rotational) with the community pharmacist/ GP or family member as appropriate. This list becomes the documented source of medication reconciliation from then on through to the admission process and beyond. A “Patient Own Drug” (POD) scheme is planned to follow on from the Pre Assessment stage, which will include technician involvement. This service is at the finalstagesanditisintendedtohaveitinprogress by mid 2012. The involvement of a pharmacist at pre assessment has been audited and has been shown to be very successful as a patient safety initiative."
UTILISING PHARMACY AS KEY STAKEHOLDERS
The second team project involves the Pharmacy as key stakeholders in the developments of the day infusion unit at SIVUH, thereby facilitating a more streamlined,efficientandmultidisciplinaryteam based service. The multidisciplinary team included members from Pharmacy, Nursing, Medical, Surgical, Management, Admissions, Medical Records and Planning & Development. The positive changes seen from the key involvement in this multidisciplinary team collaboration shows improvement in overall scheduling of patients, documentation, more inclusive team environment, enhanced communication facilitated by an electronic shared folder, more easily accessible data
andmeasurablecostssavings/efficiencies.
The pharmacy team is now an integral part of the Day Infusion Unit service at SIVUH.
"The commitment to both of these projects in consultation with the wider hospital team has shown very positive results in terms of patient safety, measurable cost savings and enhanced working relationships throughout the hospital team environment. The Pharmacy Department‘s team ethos facilitatesasafer,costefficientuseofresources in delivering complex patient centered pharmaceutical care," she adds.
The Medicines Information service (MI) provided at the hospital strives to optimise patient care through the provision of accurate, up-to-date, unbiased information on medication use to health care professionals within the organisation, both in terms of individual patient care, and in the provision of general information on safe use of medicines and SVUH has a busy oncology and haematology service. The pharmacy has a Aseptic Services Unit (ASU) that operates under Good Clinical Practice, where all the chemotherapy for patients in the hospital is prepared under sterile conditions. The ASU is also involved in the preparation of products for ENT, Transplant patients, Ophthalmology, Interventional Radiology, Urology and other departments.
"In addition, our team here is actively involved in supporting ongoing research projects, in particular clinical research in oncology. Pharmacists are also involved in teaching and tutoring undergraduate and postgraduate healthcare personnel and in clinical training of pharmacists in particular for the M.Sc. in Hospital Pharmacy in Trinity College Dublin and the National Pharmacy Internship Programme. The pharmacy department co-ordinates the production and publication of the Medicines Guide for the hospital," adds Muireann.

48 September 2012 • IPN
Award Category Winner 2012
Hospital & Community Pharmacy Alliance Award Winner 2012 - Palliative Care Meds Info Service
Working hand inhand to optimise patient careThe importance of cross-discipline working can never be underestimated and thebenefitstobederivedfromworkingin tandem can be immense. Whether pharmacists are working within the
S P O N S O R E D B Y
Cliona Hayden and Eimear O'Dwyer
THE INDEPENDENT VOICE OF HOSPITAL PHARMACY

IPN • September 2012 49
hospital setting or in a retail business unit in the community, the ultimate goal is the enhancement of patient care and ensuring patients and customers receive the highest possible level of service and the greatest access to necessary medications.
To this end the pharmacy team at Our Lady's Hospice in Dublin established an initiative to work closer together with those healthcare professionals caring for patients with life-limiting illnesses throughout Ireland. Their display of excellence scooped them the Hospital and Community Pharmacy Alliance Award at the Irish Pharmacy Awards 2012 in the Burlington Dublin.
PROVIDING PRACTICE-BASED MEDICINES
Senior Pharmacist within the Palliative Meds Info Service, Cliona Hayden picks up the story: "The team here at Our Lady's Hospice were receiving numerous phone calls from community pharmacists, home care teams and allied professionals asking questions about palliative care medicines.
"We are a small department and found itdifficulttorespondtothese queries within an adequate timeframe. It was unsatisfactory from a safety point of view in terms of changing guidelines and the advice we gave."
With no established mechanism for feedback,theteamidentifiedaneedwithinthe community for a service catering to healthcare professionals needs within the palliative care sector and the idea for the Palliative Meds Info Service was borne.
The ‘Palliative Meds Info Service’ responds to telephone and email enquiries from healthcare professionals caring for patients with life-limiting illnesses.
Team member and Chief II Pharmacist at
Our Lady's, Eimear O'Dwyer states: "There are several specialist medicines information centres throughout the UK. However, the PalliativeMedsInfoserviceisthefirstspecialist medicines information service in theRepublicofIrelandandthefirstspecialistpalliative care service in both the UK and Ireland.
"The necessary use of drugs beyond licence in palliative care presents a challenge in that readily available, relevant medicines information may not be easily available to all professionals involved in caring for patients with palliative care needs. This service supportsthesafe,effectiveandefficientuseof medicines by the provision of evidence-based information and advice on their therapeutic use."
The service provides medicines information to both specialist and non-specialist practitioners (including GP’s, community pharmacists) to ensure that accurate and up-to-date information is continuously available. The service provides hospice based expertise to practitioners in the community, who infrequently care for palliative care patients and help to overcome regional inequalities in the availability of hospice services throughout Ireland.
The Palliative Meds Info service has developed an enquiry answering service that follows a standardised search pattern of the literature incorporating specialised palliative care information sources. The standardised search pattern covers a wide range of reliable literature sources to ensure a comprehensive and up-to-date review of all available information. The information available is linked with clinical interpretation to provide the advice to the enquirer.
Since the service has been launched in 2009, there has been a steady stream of enquiries received from a range of health care professionals working with patients care needs in different settings, including hospitals, hospices, palliative care home care teams, palliative care specialists, GPs and community pharmacists throughout the country. The Palliative Meds Info service is sharing the expertise of a specialist palliative care setting in a safe and convenient way for healthcare professionals.
ESTABLISHING EASE OF ACCESS
The support the service provides to healthcare professionals will hopefully improve the patients’ experience with medicines, reduce the risk of side effects and produce quicker or more effective relief of symptoms and improve the quality of life of patients and their families facing the problems associated with life-threatening illness.
Once the idea was initiatiated, a steering group was gathered and Liz Hoctor was nominated by the Irish Pharmaceutical
Union to serve on the board representing community pharmacists.
The steering committee contributes expert input and knowledge on the provision of the service and to advise on the continuing improvement of the service. It is also composed of the Chief Pharmacist at OLH, the Director of Pharmacy at St James’s Hospital, the Director of Clinical Services at OLH, the Medical Director of palliative care at OLH or a medical representative of his choice, the director of the National Medicines Information Centre, a representative from the Irish Hospice Foundation (IHF), a palliative care clinical nurse specialist, a GP representative and an IAPC pharmacists group representative.
Oneofthefirstserviceslaunchedwasthe introduction of a methadone supply protocol which community pharmacists found invaluable and the team have recently launched their own webpage at www.olh.ie. This site publishes all new materials and a quarterly newsletter keeping healthcare professionals even better informed about developments.
"The provision of medicines information and support to healthcare professionals in making informed treatment decisions when caring for patients with life-limiting illnesses will contribute to the quality of life for both the patient and their family at the end-of-life. Palliative Meds Info is committed to upholding the core values of Our Lady’s Hospice and Care Services and to the delivery of integrated palliative care services in the community and other healthcare settings," says Cliona.
Eimear adds: "The service is building up an extensive database of enquiries. It is allowing us to identify areas and issues where proactive and readily available information is needed. The service is developing information sheets to address these issues. The accessibility of this information will support healthcare professionals in caring for palliative care patients and help the transition of patients from hospice/hospital setting to their homes, which is often done with very short notice and out-of hours."
Turning to the future Eimear adds: "We hope to continue to grow the service. This year has been incredibly proactive and we envisage developing the service to include educational resources and we would like to audit it to see how we can improve to include this as part of a wider service.
"Winning the Hospital and Community Pharmacy Alliance award was such a tremendous boost in recognising the vital need this service provides and highlights how important it is for us, as pharmacy professionals, to continue to grow and develop as a team"

50 September 2012 • IPN
Viral Infections
With the onset of the colder weather, it is likely that pharmacies will see an increase in the number of customers seeking advice regarding infections. Both bacterial and viral infections can present with similar symptoms and it is sometimes difficult to distinguish between the two. This is important, particularly because antibiotics will not cure a viral infection.
Viral infections are generally systemic and involve a number of body parts simultaneously. For example, a patient with a viral infection may suffer from a runny nose, sinus congestion, cough and/or body ache. They can at times, however, be localised – for example, viral conjunctivitis. There are a few viral infections that are painful, such as shingles or herpes, and that pain is often described as being ‘itchy’ or ‘burning’.
COLDS AND FLU
The flu season runs from October to May. Cold and flu viruses – which are some of the most common viral infections – usually last up to 10 days, while bacterial illnesses usually last more than two weeks. Flu is best avoided by taking advantage of the flu vaccination programme. Pharmacists should particularly advise customers in vulnerable patient groups – the elderly; those whose immune systems are suppressed; those who have recently had surgery or have a chronic illness – to have a flu shot at the start of the flu season.
Although supplements have never been proven to be completely effective at preventing colds and flu, a few are said to boost a patient's immune system. If customer wishes to begin a course of supplements, they will need to obtain some professional advice from the pharmacy, especially if they have existing health concerns. Supplements thought to
help the immune system include zinc, garlic, echinacea, elderberry and vitamin C. Even so, these will not necessarily ward off colds and flu over the winter months.
Normal symptoms of colds include runny noses, watery eyes, sore throats, dry coughs, chills, aches and pains, all of which are caused by a virus. However, although a cough/cold will run its course, many products can be bought over the counter to help to relieve these symptoms.
Analgesics help aches and pains, and reduce fever; antihistamines dry runny noses and watery eyes; expectorants
Massive savings to be made replacing medicines with OTCs
thin mucus, so that it can be coughed up more easily; cough suppressants quieten a dry (non–mucus-producing) cough; and decongestants reduce nasal congestion. Paracetamol helps to ease any painful symptoms and to ‘sweat out’ a viral infection.
The Irish Medicines Board (IMB) wrote to pharmacists last September, stating that the risk-benefit balance in children aged between two and six years of age has not been shown to be favourable when it comes to OTC cough and cold remedies. There was also some evidence that these products were linked to allergic reactions and drowsiness in children.
The advice for children aged 6-12 years remains unchanged, however, because the incidence of coughs and colds reduces as children get older, and tolerances increase with the child’s size. The IMB also feels that older children can better articulate if the product is helping or, indeed, having an unwanted effect. Therefore, the advice is that these products should continue to be offered, up to daily recommended allowances.
“Recommendations reflect an evolution in therapeutic strategy over time rather than as a result of any new or specific development,” said the IMB.
According to Euromonitor International, which specialises in strategy research for consumer markets, cough and cold remedies in Ireland are expected to have a compound annual growth rate of 2 per cent between 2012 and 2016.
MUMPS, MEASLES AND CHICKENPOX
Mumps, measles and chickenpox largely affect children but can also strike adults. Common symptoms of mumps are: painful inflammation of the neck parotid glands, swelling of the temporomandibular area, sore throat, headache, fever and/or face pain. Other symptoms of this disease that occur in men are testicle lumps and pain and/or scrotal swelling.
There is no need for a patient to necessarily visit a doctor because there is no specific treatment for mumps. Applying ice packs or heat packs to the neck can help and paracetamol can be used for pain relief. Aspirin is not recommended, due to a possible link with Reye's syndrome. Warm salt-water gargles, soft foods and extra fluids may also help.
The symptoms of measles include fever,
cough, runny nose, red eyes and a generalised erythematous rash. It is caused by the rubeola virus and is contained in the thousands of droplets that are formed when a person with measles coughs or sneezes. These are then breathed in by another person or they can be picked up after they have settled on surfaces, where they can survive for a few hours.
Once inside the body, the virus will multiply in the back of the throat and lungs before spreading throughout the body, including the respiratory system and the skin. The patient will be infectious from two to four days prior to and until five days after the onset of the rash.
Like mumps, patients should be advised that there is no specific treatment for the infection but they should specifically be warned to keep away from anyone who is pregnant. Most people recover with rest, and paracetamol to treat the fever and any pain. In rare cases, patients may experience complications with measles, such as pneumonia, ear infections, bronchitis or encephalitis. While there is no specific treatment for measles-related encephalitis, antibiotics are required for bacterial pneumonia, sinusitis and bronchitis that can follow measles.
Chickenpox, which is caused by the varicella zoster virus, is more prevalent in children under the age of 10. It usually starts with a rash on the body. It may be more concentrated in some areas. The spots will itch and, if scratched, may leave permanent pockmarks.
Chickenpox is spread through coughing or sneezing or through direct contact with secretions from the spots. A person with chickenpox is infectious one to two days before the rash appears and remains contagious until all the blisters have crusted over. Calamine lotion may help to prevent itchiness and other OTC anti-itching creams, lotions, mousses and cooling gels may also help.
Even though effective vaccines have been developed, some parents prefer to believe that it is better for children to contract mumps, measles and chickenpox rather than take them to a clinic to be given a vaccination. However, the vaccine is generally a safer bet than the risk of any complications that can occur.
The chickenpox infection in adults tends to be more severe than in children. Although the remedies to ease adult chickenpox

Also available as Distaclor LA 375mg tabs,125mg/5ml and 250mg/5ml Distaclor suspension.
Abbreviated Prescribing Information. Presentations: Distaclor LA Forte 500mg prolonged release tablets, equivalent to 500mg cefaclor. Distaclor LA Tablets 375mg, prolonged release tablets equivalent to 375mg cefaclor. Distaclor granules for suspension containing 125mg cefaclor/5ml, Distaclor granules for suspension containing 250mg cefaclor/5ml. Uses: Distaclor LA presentations and Distaclor suspensions are indicated for the treatment of upper and lower respiratory tract, skin and skin structure, and urinary tract infections when due to susceptible micro-organisms. Additionally, Distaclor is indicated for otitis media and as part of the management of sinusitis. Dosage and Administration: (For full information see Summaries of Product Characteristics [SPCs]). SPCs should be referred to before prescribing. Cefaclor is administered orally. Adults and the elderly: Distaclor LA Tablets 375mg: The usual dosage is 375mg twice daily. Pneumonia -750mg twice daily. Distaclor LA Forte 500mg Tablets: One tablet twice daily in bronchitis. LA tablets should be taken with meals. Distaclor Suspensions: The usual dosage is 250mg every eight hours. For more severe infections or those caused by less susceptible organisms, doses may be doubled. Distaclor may be administered in the presence of impaired renal function. Under such conditions dosage is usually unchanged (see ‘Precautions’). Children: Distaclor Suspensions are available (Distaclor LA tablets are not recommended). The usual daily dosage for children is 20mg/kg/day in divided doses every 8 hours. In more serious infections, otitis media, sinusitis and infections caused by less susceptible organisms, 40mg/kg/day in divided doses is recommended, up to a daily maximum of 1g. For otitis media and pharyngitis, 12-hourly dosing may be used. In the treatment of beta-haemolytic streptococcal infections, therapy should be continued for at least 10 days. Contra-indication: Hypersensitivity to cephalosporins. Warnings: Cephalosporins should be given cautiously to patients with known penicillin sensitivity. Cross hypersensitivity (including anaphylaxis) has been reported occasionally in patients receiving beta-lactam antibiotics. If an allergic reaction occurs, the drug should be discontinued. The diagnosis of pseudomembranous colitis should be considered if diarrhoea occurs. Usage in pregnancy and lactation: Although animal studies have shown no evidence of teratogenicity, caution should be exercised. Small amounts of cefaclor have been detected in breast milk following administration of single 500mg doses. Caution should be exercised when administering to a nursing woman. Precautions: In patients with markedly impaired renal function, administer Distaclor with caution (see SPCs). Broad-spectrum antibiotics should be prescribed with caution in individuals with a history of gastro-intestinal disease, particularly colitis. Prolonged use of cefaclor may result in the overgrowth of non-susceptible organisms. Positive direct Coombs’ and false-positive glycosuria tests have been reported. Drug interactions: There have been rare reports of increased prothrombin time, with or without clinical bleeding, in patients receiving cefaclor and warfarin concomitantly. Renal excretion is inhibited by probenicid. Diminished absorption of Distaclor LA with concomitant magnesium hydroxide or aluminium hydroxide. Side-effects: Gastro-intestinal: Diarrhoea, nausea, vomiting, dyspepsia, colitis. Hypersensitivity: Allergic reactions (urticaria, morbilliform eruptions, pruritis) serum sickness-like reactions, fever, arthralgia/arthritis, rare reports of erythema multiforme major (Stevens-Johnson syndrome), toxic epidermal necrolysis, and anaphylaxis (see SPCs). Haematological: Eosinophilia, positive Coombs’ tests and, rarely, thrombocytopenia. Transient lymphocytosis, leucopenia and, rarely, haemolyticanaemia, aplastic anaemia, agranulocytosis, and reversible neutropenia of possible clinical significance. Hepatic: Transient hepatitis and cholestatic jaundice have been reported rarely, sight elevations in AST, ALT, or alkaline phosphatase values. Renal: Reversible interstitial nephritis has occurred rarely, slight elevations in blood urea or serum creatinine, or abnormal urinalysis. Central nervous system: Reversible hyperactivity, agitation, nervousness, insomnia, confusion, hypertonia, dizziness, hallucinations, somnolence, headache and agitation. Miscellaneous: Genital pruritis, vaginal moniliasis, and vaginitis. Legal Category: S.1.A Product Authorisation Numbers and Holders: Distaclor LA Forte 500mg tablets: PA 1226/1/5 Distaclor LA Tablets 375mg: PA 1226/1/4. Distaclor Suspension 125mg/5ml: PA 1226/1/2.Distaclor Suspension 250mg/5ml: PA 1226/1/3. Flynn Pharma Ltd, Alton House, 4 Herbert Street, Dublin, Ireland. Distributed in Ireland by Clonmel Healthcare Ltd, Waterford Road, Clonmel, Co. Tipperary. Date of preparation or Last Review: August 2009 SPCs are available on request from: Flynn Pharma Ltd, The Maltings, Bridge Street, Hitchin, Herts SG5 2DE. Tel 0044 1462 458974 email: [email protected] or from Clonmel Healthcare Ltd at www.clonmel-health.ie *Community acquired bacterial infections. Distaclor (cefaclor) and Distaclor LA (cefaclor LA) are trademarks of Flynn Pharma Ltd. 2009/ADV/CEF/158

52 September 2012 • IPN
Viral Infections
symptoms are the same as those for children, adults are more often prescribed antiviral medication to reduce the severity of the condition and the likelihood of complications.
Patients who have had chicken pox as children are more susceptible to shingles (herpes zoster) in later life, often accompanied by post-herpetic neuralgia, a painful condition that makes it difficult to sleep. Even after the shingles' rash has disappeared, pain may still continue.
Topical creams and lotions can help and analgesics can be used to relieve the pain. Once the spots have crusted over, capsaicin cream can be recommended. Topical lidocaine and nerve blocks may also reduce the pain, while gabapentin, along with antivirals may relieve post-herpetic neuralgia.
COLD SORES AND EYE ISSUES
The herpes simplex virus is commonly known as a cold sore. Some patients have a ‘prodrome’ before the actual sores appear – a burning or tingling sensation that precedes the appearance of blisters by a day or two. As the cold sore forms, the area may become reddened and small, fluid-filled blisters may occur.
Cold sores (the HSV-1 virus) are closely related to genital herpes (HSV-2) and are spread from person to person by close personal contact. Blisters may return sporadically as there is no cure for the virus. If used correctly, however, antiviral cold sore creams may speed up the healing time of a recurrent infection. They usually contain aciclovir or penciclovir.
These creams are widely available over the counter from pharmacies without a prescription. However, they are only effective if they are applied as soon as the first signs of a cold sore appear. Using an antiviral cream after this initial period is unlikely to have much effect. There are also cold sore patches that contain hydrocolloid gel. The
patch is placed over the cold sore and hides the sore while it heals.
Several non-antiviral creams are also available over the counter from pharmacies. These may help ease the irritation of cold sores, but will not help them to heal faster.
Viral conjunctivitis spreads by contact involving tears or the fluid from an infected person. Pharmacists are trained to diagnose this complaint and most effective medications are on prescription. The patient will need to adhere to a strict hygiene regime because the conjunctivitis is highly contagious.
Steroid drops are sometimes helpful but they should only be used if prescribed by a doctor, as the inappropriate use of steroid eye-drops can cause more serious problems.
Chloramphenicol is the first-choice topical antibiotic for infectious conjunctivitis but, even if the infection is viral, chloramphenicol can still be used, because topical chloramphenicol products can help to prevent secondary bacterial infections. Contact lens wearers should see their optometrist, contact lens practitioner or GP before using OTC treatments, and they should stop using lenses for as long as their eye is red and/or continues to discharge.
By helping consumers to make the best use of self-medication this autumn and winter, pharmacists can help to improve their patients’ health and ensure customer satisfaction because they can buy many of their medicines from the pharmacy without needing to visit a doctor.
The European Self-Medication Industry Association, of which the Irish Pharmaceutical Healthcare Association is a member, has estimated that effective self-medication in Ireland could result in annual savings of €75 million if there was a 5 per cent shift to non-prescription medicines – many of these would, undoubtedly, include treatments for viral infections.
Bacterial infectionsClassic symptoms of bacterial infections are localised redness, heat and swelling. Localised pain, caused by bacteria, is another hallmark. For example, if a cut has been infected, pain will occur at the site of the infection.
Pain on one side of the throat is also a sign of bacterial infection. Similarly, an ear infection is more likely to be bacterial if the pain occurs in only one ear.
The following signs and symptoms, which usually last for two weeks or longer suggest bacterial infection: a high, persistent temperature; a thick, coloured discharge from a break in the skin; and/or a chronic cough.

IPN • September 2012 53
Adult 3gFosfomycin (as Trometamol)
Name of mediciNal Product: monuril 3g granules for oral solution. Each single-dose sachet contains 5.631g fosfomycin – trometamol (1:1) equivalent to 3g fosfomycin. It is a white granular powder for oral solution with a characteristic odour and flavour of mandarin. TheraPeutic iNdicatioNs: Treatment of acute uncomplicated urinary tract infections due to sensitive organisms in adults. Posology aNd admiNistratioN: Adults only: A single dose of 3g taken on an empty stomach, preferably before bedtime, after bladder emptying. The contents of the sachet should be dissolved in water and the solution swallowed immediately. Elderly patients: Not recommended due to diminished urinary excretion. Paediatric population: It is not for use in children coNtraiNdicatioNs: Hypersensitivity to the active substance or to any of the excipients. Monuril should not be used in patients with impaired renal function (creatine-clearance <80 ml/min). WarNiNgs aNd sPecial PrecautioNs for use: Clostridium difficile associated diarrhoea (CDAD) has been reported with use of nearly all antibacterial agents, including fosfomycin trometamol, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile. C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents. If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C.difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated. this medicinal product contains sucrose. Patients with rare hereditary problems of fructose intolerance, glucose galactose malabsorption or sucrase-isomaltase insufficiency should not take this medicine. Do not use more than one single dose of Monuril to treat a single episode of acute cystitis. Prolonged use of an anti-infective may result in the development of super infection due to organisms resistant to that anti-infective. iNteractioNs: When co-administered with fosfomycin, metoclopramide lowers the serum and urine concentrations of fosfomycin. Other drugs that increase gastrointestinal motility may produce similar effects. No information is available on the interaction between fosfomycin and oral contraceptives, nevertheless there is a potential for interaction between oral contraceptives and antibiotics. PregNaNcy aNd lactatioN: Pregnancy: Data on a limited number of exposed pregnancies indicate no adverse effects of fosfomycin on pregnancy or on the health of the foetus/new-born child. To date, no other relevant epidemiological data are available. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition or postnatal development. Caution should be exercised when prescribing to pregnant women. Lactation: Due to lack of safety information, the use of fosfomycin during human lactation cannot be recommended usiNg moNuril With food & driNk: Take Monuril on an empty stomach (2-3 hrs after a meal) as food delays and reduces the absorption of fosfomycin trometamol, resulting in reduced blood and urinary concentrations. driviNg aNd usiNg machiNery: Monuril oral solution has no influence on the ability to drive and use machines. uNdesirable effects: commoN (1/100 to <1/10): Headache, Dizziness, Diarrhoea, Nausea, Vulvo-vaginitis, Dyspepsia and Asthenia uNkNoWN Anaphylactic shock, Allergic reaction, Asthma, Vomiting, Abdominal pain, Angioedema, Rash, Urticaria and Pruritus overdose: Symptoms: The following events have been observed in patients who have taken MONURIL 3g granules for oral solution in overdose: vestibular loss, impaired hearing, metallic taste, and general decline in taste perception. Treatment in the event of overdose: In the event of over dosage, treatment should be symptomatic and supportive. PharmacodyNamic ProPerties: Fosfomycin trometamol [mono (2-ammonium-2-hydroxymethil-1,3-propandiol) (2R-cis) (3- methiloxyranil) phosphonate] is a broad spectrum antibiotic, derived from phosphonic acid, for the treatment of urinary tract infections. The antibacterial activity of fosfomycin is due to an inhibition of bacterial cell wall synthesis. Its particular mechanism of action, specific inhibition of enol pyruviltransferase, results in lack of cross resistance with other classes of antibiotic, and the possibility of synergism with other antibiotics (in vitro synergic effect with amoxicillin, cephalexin, pipedimic acid and aztrenam). Pharmacokinetic properties: Fosfomycin trometamol which is an orally well absorbed salt of fosfomycin, in which the formulation is completely soluble in water. Fosfomycin, unbound to the plasma proteins, is eliminated mainly unchanged through the kidneys and this results in very high urinary concentrations (about 3000mcg/ml) within 24 hours. Therapeutic concentrations of the active moiety in the urine are usually maintained for at least 36-48 hours. In patients with moderately reduced renal function (including elderly patients) the serum half-life of fosfomycin is slightly prolonged but urinary concentration remains therapeutically adequate. legal category: POM Package Quantities: Sachets are supplied in cardboard outer containing 1 sachet. date of last Pi revision: Nov 11.
marketiNg authorisatioN holder: Zambon S.p.A. via Lillo del duca, 10 20091-Bresso, Milano. marketiNg authorisatioN Number: PA1441/2/2 distributor: Sinclair IS Pharma Ireland Ltd. marketed iN irelaNd by: faNNiN ltd, faNNiN house, leoPardstoWN, dubliN 18.
for a copy of the smPc or further medical information, please contact [email protected] adverse events should be reported to fannin ltd, Pharmacovigilance at 01 2907000 or [email protected]
fN2012-07-003. date of Preparation: August 2012
NEW in Ireland
One-dose sachetdissolves in water
One Treatment. One Solution.
al Product: monuril 3g granules for oral solution. al Product:al Product:
the one dose
Treats acute uncomplicated UTIs with just one dose
Monuril Advert concepts 02-08.indd 1 15/08/2012 12:48

54 September 2012 • IPN
www.colgateprofessional.ieYOUR PARTNER IN ORAL HEALTH
54% of adults have gingival
bleeding.1
new colgate® total® pro gum health
toothpaste is medically licensed to
“improve gingival health and
reduce the progression
of periodontitis”.of periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitisof periodontitis ....
YOUR PARTNER IN ORAL HEALTH
Triclosan A highly effective, broadspectrum antibacterial agent
CopolymerForms a physical network thatentraps and stores Triclosan
triclosan & copolymer – unique technology for effectiveplaque reduction
A review of 198 published scientific and clinical studies,together with two systematic reviews concluded:Overall the current evidence suggests that with thetwice daily use of a Triclosan & Copolymer toothpastepatients will:
• Gain clinically significant improvements in plaque control and gingivitis • Benefit from slower progression of periodontal disease
Blinkhorn A et al. (2009) British Dental Journal 2007: 117-126
• Triclosan acts effectively against plaque bacteria and is been proven to be safe and effective in a number of long term clinical studies3 • Copolymer ensures retention and delivery of Triclosan to the surfaces of teeth and oral mucosa (including gingivae) to create an antibacterial protective barrier
• Over time, Triclosan is slowly released from the Copolymer to provide sustained antibacterial action for 12 hours
YOUR PARTNER IN ORAL HEALTH
toothpaste
management for patients at
increased risk of, or with evidence
of developing periodontal diseases
colgate total pro gum health contains
clinically proven triclosan & copolymer
technology to improve gingival health.
Significant improvement in antiplaque and antigingivitis
effects, compared to a normal fluoride toothpaste
Recommend Colgate Total Pro Gum
Health Toothpaste as part of your
treatment and maintenance of your
patientsÕ periodontal health.Active ingredients:Triclosan 0.3% and Sodium Fluoride 0.32% (1450ppm F)Active ingredients:Active ingredients:
Control
2
1.6
1.2
0.8
0.4
06 Weeks 6 Months
1.5
1.3‡
1.6
1.2‡
1.5
1.1‡
1.51.6
3 MonthsBaseline
Clinical results – Improved gingival index scores2
* p < 0.05; † p < 0.01;
‡ p < 0.001
Triclosan/Copolymer
Loe-
Siln
ess
Gin
giva
l Ind
exLONG-L
ASTI
NG a
nti b
acte
rial actio
n
DIRECT anti-inflamm
atory action
12hours
NEW
YOUR PARTNER IN ORAL HEALTH
product informationName of the medicinal product: Colgate TOTAL Pro Gum Health Toothpaste. Active ingredients: Triclosan 0.30% w/w, Sodium Fluoride 0.32% w/w (1450ppm F). Indications: To reduce dental caries, to improve gingival health and to reduce the progression of periodontitis. Dosage and administration: Apply a 1 cm line of paste across the head of a toothbrush and brush the teeth thoroughly for one minute twice daily. Spit out after use. Children under 7, use a pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Contraindications: None known. Special warnings and precautions for use: Children under 7, use a pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Undesirable effects: None known. Marketing authorisation number: PA 320/5/1. Marketing authorisation holder: Colgate-Palmolive (U.K.) Ltd. Guildford Business Park, Middleton Road, Guildford, Surrey, GU2 8JZ. Recommended selling price: €4.59 (75ml tube). Date of revision of text: October 2011.
For full prescribing information, please contact the marketing authorisation holder, Colgate-Palmolive (U.K.) Ltd., Guildford Business Park,Middleton Road, Guildford, Surrey, GU2 8JZ.
1 UK Adult Dental Health Survey 2009, NHS Information Centre for Health and Social Care.2 Lindhe J et al. (1993) J Clin Periodontal; 20(5):327-334.3 Ayad et al. (2011) J Clin Dent; 22(Spec Iss): 204-212.
• Toothpaste• Daily Mouthwash• Dental Floss• Interdental Brushes• Toothbrush
recommend a system of clinicallyproven products to help your patientssupport their gingival health
system
NEW
www.colgateprofessional.ie

PRODUCT INFORMATIONName of the medicinal product: Colgate TOTAL Pro
Gum Health Toothpaste. Active ingredients: Triclosan 0.30% w/w, Sodium Fluoride 0.32% w/w (1450ppm F). Indications: To reduce dental caries, to improve
gingival health and to reduce the progression of periodontitis. Dosage and administration: Apply a 1 cm line of paste across the head of a toothbrush and brush the teeth thoroughly for one minute twice daily. Spit out after use. Children under 7, use a pea-sized
amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist.
Contraindications: None known. Special warnings and precautions for use: Children under 7, use a
pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Undesirable effects: None known. Marketing
authorisation number: PA 320/5/1. Marketing authorisation holder: Colgate-Palmolive (U.K.) Ltd.
Guildford Business Park, Middleton Road, Guildford, Surrey, GU2 8JZ. Recommended selling price: €4.59
(75ml tube). Date of revision of text: October 2011.
For full prescribing information, please contact the marketing authorisation holder, Colgate-Palmolive
(U.K.) Ltd., Guildford Business Park, Middleton Road, Guildford, Surrey, GU2 8JZ.
1 UK Adult Dental Health Survey 2009, NHS Information Centre for Health and Social Care.
2 Lindhe J et al. (1993) J Clin Periodontal; 20(5):327-334.
3 Ayad et al. (2011) J Clin Dent; 22(Spec Iss): 204-212.
YOUR PARTNER IN ORAL HEALTH
product informationName of the medicinal product: Colgate TOTAL Pro Gum Health Toothpaste. Active ingredients: Triclosan 0.30% w/w, Sodium Fluoride 0.32% w/w (1450ppm F). Indications: To reduce dental caries, to improve gingival health and to reduce the progression of periodontitis. Dosage and administration: Apply a 1 cm line of paste across the head of a toothbrush and brush the teeth thoroughly for one minute twice daily. Spit out after use. Children under 7, use a pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Contraindications: None known. Special warnings and precautions for use: Children under 7, use a pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Undesirable effects: None known. Marketing authorisation number: PA 320/5/1. Marketing authorisation holder: Colgate-Palmolive (U.K.) Ltd. Guildford Business Park, Middleton Road, Guildford, Surrey, GU2 8JZ. Recommended selling price: €4.59 (75ml tube). Date of revision of text: October 2011.
For full prescribing information, please contact the marketing authorisation holder, Colgate-Palmolive (U.K.) Ltd., Guildford Business Park,Middleton Road, Guildford, Surrey, GU2 8JZ.
1 UK Adult Dental Health Survey 2009, NHS Information Centre for Health and Social Care.2 Lindhe J et al. (1993) J Clin Periodontal; 20(5):327-334.3 Ayad et al. (2011) J Clin Dent; 22(Spec Iss): 204-212.
• Toothpaste• Daily Mouthwash• Dental Floss• Interdental Brushes• Toothbrush
recommend a system of clinicallyproven products to help your patientssupport their gingival health
system
NEW
www.colgateprofessional.ie
YOUR PARTNER IN ORAL HEALTH
product informationName of the medicinal product: Colgate TOTAL Pro Gum Health Toothpaste. Active ingredients: Triclosan 0.30% w/w, Sodium Fluoride 0.32% w/w (1450ppm F). Indications: To reduce dental caries, to improve gingival health and to reduce the progression of periodontitis. Dosage and administration: Apply a 1 cm line of paste across the head of a toothbrush and brush the teeth thoroughly for one minute twice daily. Spit out after use. Children under 7, use a pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Contraindications: None known. Special warnings and precautions for use: Children under 7, use a pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Undesirable effects: None known. Marketing authorisation number: PA 320/5/1. Marketing authorisation holder: Colgate-Palmolive (U.K.) Ltd. Guildford Business Park, Middleton Road, Guildford, Surrey, GU2 8JZ. Recommended selling price: €4.59 (75ml tube). Date of revision of text: October 2011.
For full prescribing information, please contact the marketing authorisation holder, Colgate-Palmolive (U.K.) Ltd., Guildford Business Park,Middleton Road, Guildford, Surrey, GU2 8JZ.
1 UK Adult Dental Health Survey 2009, NHS Information Centre for Health and Social Care.2 Lindhe J et al. (1993) J Clin Periodontal; 20(5):327-334.3 Ayad et al. (2011) J Clin Dent; 22(Spec Iss): 204-212.
• Toothpaste• Daily Mouthwash• Dental Floss• Interdental Brushes• Toothbrush
recommend a system of clinicallyproven products to help your patientssupport their gingival health
system
NEW
www.colgateprofessional.ie
IPN • September 2012 55
www.colgateprofessional.ie
everyday use to protect against gum
bleeding and inflammation
a clinically proven, alcohol-free formula to help reduce the
formation of plaque bacteria.
Recommend a clinically provenalcohol-free mouthwash toprotect against gum bleedingand inflammation
mouthwash
Colgate Total Pro Gum Health group
showed significant reduction in dental
plaque and gingival bleeding, compared
to control mouthwash group
Controlmouthwashwith fluoride
Reduction of dental plaque3
Colgate TotalPro Gum HealthMouthwash
Plaq
ue in
dex
Baseline 3 months 6 months
NEW
0
0.5
1.0
1.5
2.0
2.5
3.0
amount for supervised brushing to minimise swallowing.
YOUR PARTNER IN ORAL HEALTH
product informationName of the medicinal product: Colgate TOTAL Pro Gum Health Toothpaste. Active ingredients: Triclosan 0.30% w/w, Sodium Fluoride 0.32% w/w (1450ppm F). Indications: To reduce dental caries, to improve gingival health and to reduce the progression of periodontitis. Dosage and administration: Apply a 1 cm line of paste across the head of a toothbrush and brush the teeth thoroughly for one minute twice daily. Spit out after use. Children under 7, use a pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Contraindications: None known. Special warnings and precautions for use: Children under 7, use a pea-sized amount for supervised brushing to minimise swallowing. If using fluoride supplements, consult your Dentist. Undesirable effects: None known. Marketing authorisation number: PA 320/5/1. Marketing authorisation holder: Colgate-Palmolive (U.K.) Ltd. Guildford Business Park, Middleton Road, Guildford, Surrey, GU2 8JZ. Recommended selling price: €4.59 (75ml tube). Date of revision of text: October 2011.For full prescribing information, please contact the marketing authorisation holder, Colgate-Palmolive (U.K.) Ltd., Guildford Business Park,Middleton Road, Guildford, Surrey, GU2 8JZ.
1 UK Adult Dental Health Survey 2009, NHS Information Centre for Health and Social Care.2 Lindhe J et al. (1993) J Clin Periodontal; 20(5):327-334.3 Ayad et al. (2011) J Clin Dent; 22(Spec Iss): 204-212.
• Toothpaste• Daily Mouthwash• Dental Floss• Interdental Brushes• Toothbrush
recommend a system of clinicallyproven products to help your patientssupport their gingival health
system
NEW
www.colgateprofessional.ie

56 September 2012 • IPN
News
Kathleen Downey is an Auckland-based pharmacist, who moved to New Zealand from Northern Ireland 20 years ago. According to Downey, she has never regretted the move because the country has given her and her family some wonderful opportunities.
“I previously lived in South Africa with my husband but we decided to move back to Ireland after the birth of our first two children. We were happy but we found that we were really missing the outdoor lifestyle so, once again, we decided to relocate but, this time to New Zealand because of the political situation in South Africa.”
In New Zealand, Downey went into retail pharmacy before working as an aged-care residential pharmacist for the Waitemata District Health Board (DHB), which covers an area to the north and west of Auckland city. It is a scenic location, where the pace of life is relaxed. However, it is the second-fastest growing patient population in New Zealand, with a population of more than 525,000 people.
“We arrived in 1992 and, whilst waiting for my registration to come through, I offered to help out in a local community pharmacy for a few hours per day, free of charge. After three weeks, the owner offered me a job and soon after that, he went away on holiday and left me on my own!” said Downey. “Thank goodness the pharmacy technician knew the ins and outs of the system and the legislation. Pharmacy technicians play a very important role in the New Zealand system.
JOB OPPORTUNITIES
Downey eventually decided to make the full transition to hospital pharmacy, after
Going into the new world
spending some time working between community and hospital work.
“When I moved full-time into hospital pharmacy, my employers also paid for my Postgraduate Diploma in Clinical Pharmacy, which I really appreciated,” said Downey.
"Waitemata Hospital is very advanced, in terms of technology," she continued. "We use a Pyxis Medstation system, which uses fingerprint technology when dispensing medications. It also allows the pharmacist to see all the drugs and their quantities in stock. The health board is 'always ahead of the game' in technology."
Waitemata DHB is currently recruiting a wide range of medical staff – and there is a pressing need for pharmacists.
"There is a good work/life balance here," said Downey, "as well as additional options, such as a subsidised massage service and a bike workshop for those who cycle in to work. There is also a global mobility team dedicated to recruiting and relocating healthcare professionals from overseas. The board also liaises with quite a few local companies to help 'the other partner' find employment.
“The education system here is excellent and the State healthcare is really good, too – I don’t have private health insurance. A friend of mine had a colonoscopy recently and needed further investigations. Within a week, he had a CT scan and also a PET. There aren’t many countries in the world where things move so quickly like that.”
HEALTH SYSTEM
Downey explained that people pay to see a GP but, if they are registered with a particular
GP in a Primary Care Organisation and always see that same doctor, then it costs them less money per visit.
“Some people go to after-hour GPs, just on demand, and that is more expensive. It costs about $65 to $70, depending on the time,” she said. “When visiting a GP with whom you are registered, it is about $50-$60 per visit and prescriptions are subsidised.”
New Zealand also has a good system for people who require a lot of medication. Such patients are issued with ‘High Use Health Cards’. Once the patient has paid for 20 prescribed items, any subsequent dispensing fees are waived and so there is no $3 charge per item. Downey explained that this system is great for people who are very sick and on a lot of medicines.
Pharmac, the funding agency, does not fund everything and some branded drugs have a part charge (on top of the $3 dollar per item charge). The generic brands are usually fully subsidised. Generic substitution is allowed unless otherwise specified by the prescriber.
The big issues in community pharmacy, according to Downey, is that the New Zealand Government wants community pharmacists to take a more active role in patient care – and of course, all the funding issues that go along with that sort of approach.
MAKING THE MOVE
However, if any Irish pharmacist is considering making a move to New Zealand, along with their partner or spouse, they should both be keen to make such a big life-change, according to Downey.
“It is no good being half-hearted about it," she advised. "Although it’s only a flight away, both people need to be ‘on the same page’ with regard to how long they’ll stay and so on."
For more information on jobs with Waitemata DHB, please visit:www.wdhbcareers.co.nz/home.php

42-43 Amiens St, Dublin 1 Tel: [01] 817 8886 Asthma Adviceline: 1850 44 54 64 Email: [email protected] www.asthmasociety.ie
A charitable organisation registered in Dublin No. 57125 as a non-profit Company limited by guarantee. Chy No. 6100
The Asthma Society of Ireland is dedicated to improving the health and well-being of the 470,000 people in Ireland with asthma.Our purpose is to provide information, advice and reassurance for people with asthma.
Urgent Appeal for Support
Details
Title Mr Mrs Miss Ms Dr Other Address
First name
Surname
Email Telephone
Mobile
Subscription type
€40 €100 €250
I would like to become a Professional Supporter by setting up a standing order Please pay the Asthma Society of Ireland the sum of: Bank account number
on the day of Bank sort code
and afterwards on the same day monthly quarterly annually Bank name
until further notice and please debit my account accordingly. Bank address
Signed Date
(Please make this at least a month from today’s date)
€
To subscribe by cheque or credit card please contact us by calling Tel: [01] 817 8886
Dear Pharmacist,
We are writing to urge you to become a Professional Supporter of the Asthma Society of Ireland. Over the last number of years the demand for our services has increased significantly. Despite a funding deficit we have succeeded in maintaining the level and quality of services to asthma patients and community pharmacists in 2011/2012; however this is not sustainable going forward into 2013 and we greatly need your support.
As a Professional Supporter of the Asthma Society of Ireland you will be helping to fund the following services to you and your patients;
• The Asthma Advice Line: allowing you and your patients to consult with a specialist nurse.
• Asthma Society of Ireland patient information publications.
• The E Learning Programme: provided free of charge by the Asthma Society of Ireland to pharmacists as part of the National Asthma Programme http://elearning.asthmasociety.ie/.
• www.asthmasociety.ie which provides a wealth of patient and professional resources such as inhaler technique videos, the latest news on asthma and free publication downloads.
• The Asthma Control in General Practice Guidelines produced in partnership with ICGP http://asthmasociety.ie/practice-resources/asthma-management-guidelines.
• The National Asthma Clinic Programme: available as a service to pharmacies throughout Ireland.
The Asthma Society of Ireland is the only independent provider of specialist asthma information in Ireland and we urgently need your support. To become a Professional Supporter of the Asthma Society of Ireland and support our vital work on behalf of you and your patients, please fill in and return the form below.
Many thanks for your support,
Yours Sincerely
Sharon Cosgrove Cicely Roche MPSICEO Health Care Professional Committee MemberAsthma Society of Ireland Asthma Society of Ireland

58 September 2012 • IPN
Out and About
Boots Night WalksOver 850 people took part in Boots Night Walks for Night Nurses in 34 locations around Ireland on Wednesday 29 August 2012 as part of Boots Ireland’s Charity of the Year Partnership with the Irish Cancer Society. Employees and customers of Boots stores throughout Ireland participated in the event to raise money for the Irish Cancer Society’s Night Nursing Service, which is available free of charge to cancer patients in their home. It is hoped that the events will raise €50,000 for the nursing service once all the sponsorship is counted.
The event, held in Dublin City University, was given extra special
support from GAA star Alan Brogan who came along to cheer on the Dublin Boots staff and Management Team, as well as the customers who took part in the event.
Pictured are Claire Brennan, Irish Cancer Society Night Nurse; Alan Brogan, GAA star; and Debbie Smith, Managing Director, Boots Ireland.
Primary care facilitity competitionOver 30 towns are competing to secure the new 20 primary healthcare facilities being promised under the recent government stimulus package.
The €2.25 billion package announced this month includes €115 million for the provision of 20 new facilities to be delivered in two ‘bundles’ of ten.
The €115 million programme will be conducted through the public-private partnership model, where private investment funds the construction of the facilities, with the government then repaying the costs on an incremental basis afterwards.
Announcing the programme public expenditure minister Brendan Howlin said the locations of the facilities had yet to be decided – but that the programmes would ultimately be awarded on a “first up, best dressed” system depending on local interest.
Sexual health awareness weekSexual Health Awareness Week (SHAW) is all about promoting sexual health awareness at a national level. The event took place recently within a mix of public meetings, debates and interactive workshops at the Royal College of Physician of Ireland.
Some SHAW events dealt with very topical sexual health issues, such as choice in contraceptive provision, skills for parents when talking to their children about sex, the age of consent for sexual activity, transgender patient issues and care for victims of rape and sexual assault. Pictured are Robert Obara, TCD; Dr Olive Smyth, Dr Brigid Gallagher and Dr Dominic O’Neill.
Oustanding achievement for Margaret
The Pfizer Outstanding Achievement in Healthcare Award has been won by Margaret Murphy. A renowned campaigner on patient welfare, she was influenced by the tragic loss of her 21 year old son Kevin in 1999, following a series of avoidable medical errors. Since then she has worked tirelessly as an advocate on the need to protect patients.
Her ability to create change and to influence healthcare systems to be different, was recognised in an invitation to join the Steering Group of the WHO’s Patients for Patient Safety. She was an inaugural member of the World Alliance for Patient Safety Collaborative Centre for Patient Safety Solutions, and at home she was appointed by the Minister for Health as patient representative to the Commission for Safety and Quality Assurance in Healthcare.
Pictured are Noel Daly, The Health Partnership; Minister for Children, Frances Fitzgerald; Category winner, Margaret Murphy; David Gallagher, Country Lead, Pfizer Healthcare.


60 September 2012 • IPN
September Product News
Salatac Gel is a topical gel for warts, verrucas, corns and calluses. Applied once daily, Salatac Gel dries to form a tough water-resistant barrier protecting the wart or verruca, thus avoiding the need for irritating and messy plasters. This means that treatment should not impact on day-to-day activities or swimming and outdoor hobbies.The complete Salatac Gel treatment kit includes a special nozzle for precise application, an emery board to abrade the surface of stubborn lesions and a useful advice leaflet (to achieve the best results). For further information contact Cahill May Roberts on(01) 6305555
Calcichew-D3
Shire Pharmaceuticals Ireland Limited wishes to announce that Calcichew-D3
Forte will now be available in a new 60 pack and the current 100 pack as of 1st September
2012.Calcichew-D3 Forte is indicated for vitamin D/calcium deficiency in the elderly,
adjunct in osteoporosis, pregnancy, vitamin D dependent osteomalacia.
Rimmel introduces ScandalEyes Waterproof Kohl Kajal EyelinerScandalEyes Waterproof Kohl Kajal Eyeliner is a fine tipped, crayon type pencil available in purple, bronze, black, silver and bright blue that glides on easily and precisely for a flawlessly beautiful defined line. ScandalEyes Waterproof Kohl Kajal Eyeliner works great by applying one shade, or combining several shades to create a complete and striking eye look.The eye pencil’s soft and creamy formula gives a supple, kohl texture and sensational staying-power. Feel is ultra soft whilst the pigments make sure your colour is sleek and stays put! Rimmel has made ScandalEyes Waterproof Kohl Kajal Eyeliner waterproof, sweat proof and heat proof so it lasts up to 10 hours. Rimmel ScandalEyes Waterproof Kohl Kajal Eyeliner is available in 5 shades from September 2012 priced at €4.95
Exterol is a gentle and effective fi rst line treatment for ear wax removal - it softens hardened ear wax and releases oxygen to break the wax down for clearance.
This can help remove the discomfort in the ear and hearing loss caused by compacted ear wax. For most people, using Exterol to soften and clear the hardened ear wax avoids the need for syringing, or makes syringing much easier1.
Reference: 1. S. Fahmy and M. Whitefi eld,Brit. J. Clin. Prac. 1982, 36, 197-204.
For further information contactCahill May Roberts on (01) 6305555
Mava+ Hand Cream - extreme day treatment for hands There is no need for anyone to be deprived of activities or gardening as MAVALA Laboratories have developed an intense repairing and moisturising treatment, MAVA+ which responds to an extreme condition of very stressed, reddened and irritated hands.
Its fragrance free formula contains a botanical complex with patterson's curse, sunflower oil and heart seed which form a protecting shield reinforcing the skin's barrier and soothing skin. Shea butter is also present for its repairing properties, ideal to soothe chapped and very dry hands.
From the first application, MAVA+ will calm, soothe and soften skin. It can be used as often as desired and is also suitable for men.
bBold is fast becoming Ireland’s number 1 self tanning brand with it’s unique formula combining natural red berry extract erythrulose and premium high grade DHA a more radiant natural brown tone can be enjoyed. Enriched with Aloe Vera and Vitamin E, bBold products help tone, protect and moisturise while antioxidants assist in improving skin texture and reduce signs of premature ageing. The range includes; bBold liquid 150ml, bBold lotion 250ml both available in Light/Medium or Medium/Dark and the bBold applicator mitt. For further information on how to become a complete bBold stockist please contact Pharmacy Supplies on 048 796 27889.
• Costs 40% less thannearest competitor1*
• No.1 in Ireland*
• Available in 100 tablet and 60 tablet packs
CALCICHEW-D3 FORTE CHEWABLE TABLETS PRESCRIBING INFORMATION.
(Please refer to full Summary of Product Characteristics when
prescribing). Presentation: Chewable tablet containing 1250mg calcium
carbonate (equivalent to 500mg of elemental calcium) plus 400IU colecalciferol
(equivalent to 10 micrograms vitamin D3). Uses: Prevention and treatment of
vitamin D/calcium deficiency. Supplementation of vitamin D and calcium as an
adjunct to specific therapy for osteoporosis, in pregnancy, in established vitamin
D dependent osteomalacia and in other situations requiring therapeutic
supplementation of malnutrition. Dosage and administration: Oral (suck or
chew). Adults and elderly: Two tablets daily. Children: Not intended for use in
children. Hepatic impairment: No dose adjustment required. Renal impairment:
Should not be used in patients with severe renal impairment.
Contraindications: Diseases and/or conditions resulting in hypercalcaemia
and/or hypercalciuria, severe renal impairment, renal stones, hypervitaminosis
D, hypersensitivity to ingredient(s) Precautions: Monitor serum calcium and
creatinine levels, particularly in patients on cardiac glycosides or diuretics and
in patients with high tendency to calculus formation. Use with caution in
patients with impaired renal function. Take into account risk of soft tissue
calcification. Avoid in patients with phenylketonuria or sugar intolerance.
Prescribe with caution in patients with sarcoidosis. Use with caution in
immobilised patients. Additional doses of calcium or vitamin D should only be
taken under close medical supervision. Interactions: Tetracyclines (take 2
hours before, or 4 to 6 hours after Calcichew-D3 Forte), bisphosphonates or
sodium fluoride (take 3 hours before Calcichew-D3 Forte), Quinolone antibiotics
(take two hours before or after), levothyroxine (take four hours before or after),
thiazide diuretics, corticosteroids, cardiac glycosides, ion exchange resins
(cholestyramine), laxatives (paraffin oil). Calcichew-D3 Forte should not be
taken within 2 hours of eating foods high in oxalic acid (e.g. spinach and
rhubarb) or phytic acid (e.g. whole cereals). Side effects: Hypercalcaemia,
hypercalciuria, constipation, dyspepsia, flatulence, nausea, abdominal pain,
diarrhoea, pruritus, rash, urticaria. Very rarely (usually only seen on overdose)
milk-alkali syndrome. Use in pregnancy and lactation: Can be used in case of
calcium and vitamin D deficiency. Daily intake in pregnancy should not exceed
1500mg calcium and 600IU colecalciferol (15 micrograms vitamin D3). Avoid
overdose as permanent hypercalcaemia affects developing foetus. Calcium and
vitamin D3 pass into breast milk so consider this when giving additional vitamin
D to the child. Pharmaceutical precautions: Do not store above 30°C. Keep
container tightly closed to protect from moisture. Legal category: Pharmacy
product. Product Authorisation No: 535/1/3. Product Authorisation holder:
Shire Pharmaceuticals Ltd., Hampshire International Business Park, Chineham,
Basingstoke, Hampshire RG24 8EP UK. Distributed in Republic of Ireland by:
Cahill May Roberts, P.O. Box 1090, Chapelizod, Dublin 20, Republic of Ireland.
Further information is available on request. Date of revision: May 2011.
CALCICHEW is a registered trademark of Shire Pharmaceuticals Ltd in the
Republic of Ireland.
Adverse events should be reported to the Pharmacovigilance Unit at
the Irish Medicines Board (IMB) ([email protected]).
Information about adverse event reporting can be found on the IMB
website (www.imb.ie). Adverse events may also be reported to Shire
Pharmaceuticals Ltd on +44 1256 894000.
Reference: 1. MIMS May 2012.
Date of preparation: June 2012.Item Code: IRE/BU/CDF/12/0007.*According to IMS unit sales data April 2012.
Their strength is our forte
HELP PROTECT THEFRAGILE ELDERLY
NEW60 TABLETPACK
Calcichew New Pack A4_Layout 1 03/07/2012 15:30 Page 1

Professor Fergal O’Brien and Dr. Daniel Kelly plan to bring the prominent World Congress of Biomechanics to Ireland in 2018.
It will mean 3,000 international delegates and a lot of work but they don’t have to do it alone. Fáilte Ireland are here to support them and off er the best advice to ensure their bid is a success.
With our fi nancial assistance, Fergal and Daniel hope to secure this congress which could mean a possible €4.2 million to our economy while advancing Ireland’s profi le in the global biomechanics industry. Smart thinking all round.
To become a Conference Ambassador visitwww.meetinireland.com/conferenceambassadoror call (01) 884 7169
G30343 FI Ambassador Club 2xGuys Ir. Pharmacy News 297x210 CB.indd 1 20/06/2012 15:06

62 September 2012 • IPN
Clinical Profi lesActavis launch Rivastigmine & Irprestan on Day One
Actavis Ireland is delighted to introduce Rivastigmine Actavis and Irprestan (Irbesartan) to its portfolio of products launched on the first day of patent expiry.
Delivering key products on Day One continues to be an important focus for Actavis Ireland. The launch of Irbesartan will bring the total number of Day One and first to market launches from Actavis already this year to ten. These latest launches continue to underlines Actavis’ position as the fastest growing pharmaceutical company on the Irish market1.
Rivastigmine is indicated for the treatment of mild to moderately severe Alzheimer’s dementia and dementia in patients with idiopathic Parkinson’s.2 Irbesartan is indicated for the treatment of essential hypertension and treatment of renal disease in patients with hypertension and type 2 diabetes mellitus as part of an antihypertensive medical product regimen.3
Rivastigmine is available in 1.5 mg, 3 mg, 4.5 mg & 6 mg x 56 hard capsules. Irbesartan is available under the brande name Irprestan in 75 mg, 150 mg & 300 mg x 28 Film-coated Tablets. Both products are GMS reimbursable and available from all wholesalers post patent expiry.
Rivastigmine & Irpresartan are both subject to medical prescription.
For further information on the Actavis portfolio please contact us in Cork today on 1890 33 32 31 or email on [email protected]
1 IMS June 2012. 2 Rivastigmine Actavis SmPC. 3 Irprestan SmPC.
Rowex Ltd. is pleased to announce the launch of Clorom (Clarithromycin)500mg Prolonged Release Tablets x 7’s.
Clorom XL is indicated for:
•Communityacquiredpneumonia•Acuteexacerbationofchronicbronchitis
•Acutebacterialsinusitis(adequatelydiagnosed)•Skinandsofttissueinfections(mildtomoderateseverity)
The details are as follows:
Clorom XL 500mg Prolonged Release Tablets x 7’s - €8.58
The presentations are fully reimbursable under the GMS.
For further information contact Rowex Ltd. Bantry Co. Cork. Freephone 1800 304 400, email [email protected]

Happiness is bone shaped
www.drontal.com
AS SEEN ON
TV
DRONTAL CONSUMER AD A4 Dogs Today.indd 1 08/03/2012 16:02
*Terms and conditions apply. Drontal Plus Flavour Bone Shape Tablets. Each tablet contains 50mg praziquantel, 144mg pyrantel embonate and 150mg febantel Drontal Plus Flavour Tablets. Each tablet contains 50mg praziquantel, 144mg pyrantel embonate and 150mg febantel. Drontal Plus XL Flavour Tablets. Each tablet contains 175mg praziquantel, 504mg pyrantel embonate and 525mg febantel. Drontal Cat Tablets. Each tablet contains 230mg pyrantel embonate and 20mg praziquantel. Drontal Cat XL Film-coated Tablets. Each tablet contains 345mg pyrantel embonate and 30mg praziquantel. Please refer to appropriate data sheet. Further information available on request. ® Registered Trade Mark of Bayer AG. Bayer Ltd., Animal Health Division, The Atrium, Blackthorn Road, Dublin 18. Tel: 01 299 9313. Use Medicines Responsibly
CAMCAM
CAM CAMCAM

64 September 2012 • IPN
Clinical Profi les
Rowex Ltd. is pleased to announce the launch of Irbesan (Irbesartan) 75mg, 150mg, & 300mgFilm-Coated Tablets x 28’s.
Irbesan is indicated for:
• Treatmentofessentialhypertension
• Treatmentofrenaldiseaseinpatientswithhypertension and type 2 diabetes mellitus as part of an antihypertensive medicinal product regimen.
The details are as follows:
Irbesan 75mg Film Coated Tablets x 28’s: €13.58
Irbesan 150mg Film Coated Tablets x 28’s: €16.82
Irbesan 300mg Film Coated Tablets x 28’s: €19.53
The presentations are fully reimbursable under the GMS.
For further information contact Rowex Ltd. Bantry Co. Cork. Freephone 1800 304 400, email [email protected]
PROCORALAN NOW RECOGNISED IN NEW ESC GUIDELINES FOR THE TREATMENT OF HEART FAILUREThe new ESC guidelines for the diagnosis and treatment of heart failure include the heart rate-lowering drug, Procoralan® (ivabradine)
Less than 2 years after the publication in The Lancet of the SHIFT study results demonstrating its benefits in heart failure, Procoralan® is now integrated in the new ESC guidelines for the management of heart failure.
The guidelines presented at the recent ESC Heart Failure Congress in Belgrade, Serbia, have been updated for the first time since 2008. They make recommendations for treatment based upon evidence for established and new diagnostic tests, and therapies for heart failure.
Heart failure patients with elevated heart rates are at a significantly greater risk of death or hospitalisation, which both impacts patients’ quality of life and ultimate outcome and puts pressure on healthcare systems.
In addition, a new indication for ivabradine in chronic heart failure was granted by the European Medicines Agency in February 2012. This was based on new data from the SHIFT study in which patients with an elevated heart rate of greater than or equal to 75 beats per minute (bpm) showed a significant reduction in the primary composite endpoint (CV death and hospitalisation for worsening heart failure) of 24% (p<0.0001), reduction in risk of cardiovascular death by 17% (p=0.0166), all-cause death by 17% (p=0.0109) and heart failure hospitalisation by 30% (p<0.0001).
The new indication and the new ESC guidelines for the treatment of heart failure are the two major advances which will allow heart failure patients to benefit from ivabradine.
About ivabradine
Procoralan® (ivabradine) is the only drug to reduce heart rate selectively by inhibiting one of the electrical signals that determine heart rate – the pacemaker If current. Procoralan reduces heart rate without significantly impacting the ability of the heart muscle to pump blood.
Procoralan was launched in January 2006 for the treatment of stable angina. It is indicated in the symptomatic treatment of chronic stable angina pectoris in coronary artery disease adults with normal (sinus) rhythm unable to tolerate or with a contraindication to the use of beta-blockers or in combination with beta-blockers in patients inadequately controlled with an optimal beta-blocker dose and whose heart rate is >60 bpm.
Procoralan was subsequently approved by the European Commission for the treatment of patients with chronic heart failure in February 2012. It is indicated in the treatment of chronic heart failure in patients with normal (sinus) rhythm and whose heart rate is 75 bpm or above, in combination with standard therapy including beta-blocker therapy or when beta-blocker therapy is contraindicated or not tolerated. The decision to authorise the indication for Procoralan in heart failure followed the review of data from the SHIfT trial, the largest ever morbidity-mortality study of treatments for chronic heart failure involving more than 6000 patients.
Cholesterol Lowering Product
Pemberton International Ltd. Tel: 01-4632424
Exclusive to PharmacyNon-Prescription
Natural Plant Sterols
Clinically Proven to Reduce Cholesterol
Suitable for Lactose Intolerance
Pharmacy Exclusive Product
€12m sales p.a in Irish Grocery for Plant Sterol Foods
RSP €24.95 for a months supply - Zero VAT24.95 for a months supply - Zero VAT
Produced in Ireland - FSAI Registered
12Aug_Viva IPN Ad_v6.indd 1 22/08/2012 3:52:09 PM

Make sure you are stockingthe Good Night Ring
Low space - High marginProven track recordMassive advertising
support
www.goodnightsnoring.comDistributed in Ireland by
Pharmaher Healthcare Ltd12E Duleek Business Park, Duleek, Co Meath Tel: 041-988-2255 www.pharmaher.ie
TV Magazines & RadioPR Point of Sale material
Money Back Guarantee
Anti-SnoringRing
"Good Night Anti-Snoring Rings are selling really well from my counter. The display stand is great because it enables
customers to select their correct ring size. Everyone is surprised at how well they work - not a single person has
requested their money back as per the guarantee."Kate Jones Le Quesne's Pharmacy
CPL Healthcare is Irelands largest
Healthcare Recruitment Agency
Dublin, Cork, Galway, Limerick, London
We have been helping Pharmacists, Pharmacy Technicians, OTC Assistants
& Pharmacy Store Managers to progress their career at every level for
over 13 years.
JOB SEEKERSWe are the Supplier of choice to the
retail Pharmacy sector
We are the exclusive supplier of Pharmacy staff to the HSE in the
South, East & Midlands
We are the preferred supplier to Private Hospitals nationally
EMPLOYERSWe offer: highly experienced &
thoroughly vetted staff - Permanent & Locum
We provide: advice on salaries & new employment legislation, market
information and a payroll service
Cpl Healthcare, 2nd Floor, 49 St. Stephen’s Green East, Dublin 2T: 061 208 647 E: [email protected]
W: www.cplhealthcare.com
JOB SEEKERS
We are the Supplier of choice to the retail Pharmacy sectorWe are the exclusive supplier of Pharmacy staff to the
HSE in the South, East & MidlandsWe are the preferred supplier to Private Hospitals nationally
Cpl Healthcare, 2nd Floor, 49 St. Stephen’s Green East, Dublin 2T: 061 208 647 E: [email protected]
W: www.cplhealthcare.com
CPL Healthcare is Irelands largest Healthcare Recruitment Agency
Dublin, Cork, Galway, Limerick, London
We have been helping Pharmacists, Pharmacy Technicians, OTC Assistants & Pharmacy Store
Managers to progress their career at every level for over 13 years.
EMPLOYERS
We offer: highly experienced & thoroughly vetted staff – Permanent & Locum
We provide: advice on salaries & new employment legislation, market information and a payroll service
JOB SEEKERS
We are the Supplier of choice to the retail Pharmacy sectorWe are the exclusive supplier of Pharmacy staff to the
HSE in the South, East & MidlandsWe are the preferred supplier to Private Hospitals nationally
Cpl Healthcare, 2nd Floor, 49 St. Stephen’s Green East, Dublin 2T: 061 208 647 E: [email protected]
W: www.cplhealthcare.com
CPL Healthcare is Irelands largest Healthcare Recruitment Agency
Dublin, Cork, Galway, Limerick, London
We have been helping Pharmacists, Pharmacy Technicians, OTC Assistants & Pharmacy Store
Managers to progress their career at every level for over 13 years.
EMPLOYERS
We offer: highly experienced & thoroughly vetted staff – Permanent & Locum
We provide: advice on salaries & new employment legislation, market information and a payroll service
JOB SEEKERS
We are the Supplier of choice to the retail Pharmacy sectorWe are the exclusive supplier of Pharmacy staff to the
HSE in the South, East & MidlandsWe are the preferred supplier to Private Hospitals nationally
Cpl Healthcare, 2nd Floor, 49 St. Stephen’s Green East, Dublin 2T: 061 208 647 E: [email protected]
W: www.cplhealthcare.com
CPL Healthcare is Irelands largest Healthcare Recruitment Agency
Dublin, Cork, Galway, Limerick, London
We have been helping Pharmacists, Pharmacy Technicians, OTC Assistants & Pharmacy Store
Managers to progress their career at every level for over 13 years.
EMPLOYERS
We offer: highly experienced & thoroughly vetted staff – Permanent & Locum
We provide: advice on salaries & new employment legislation, market information and a payroll service
JOB SEEKERS
We are the Supplier of choice to the retail Pharmacy sectorWe are the exclusive supplier of Pharmacy staff to the
HSE in the South, East & MidlandsWe are the preferred supplier to Private Hospitals nationally
Cpl Healthcare, 2nd Floor, 49 St. Stephen’s Green East, Dublin 2T: 061 208 647 E: [email protected]
W: www.cplhealthcare.com
CPL Healthcare is Irelands largest Healthcare Recruitment Agency
Dublin, Cork, Galway, Limerick, London
We have been helping Pharmacists, Pharmacy Technicians, OTC Assistants & Pharmacy Store
Managers to progress their career at every level for over 13 years.
EMPLOYERS
We offer: highly experienced & thoroughly vetted staff – Permanent & Locum
We provide: advice on salaries & new employment legislation, market information and a payroll service

66 September 2012 • IPN
Appointments
President of the Hospital Pharmacists Association of Ireland, Joan Peppard, has been elected for the first time to the Board of the European Association of Hospital Pharmacists. Joan was elected at the 2012 EAHP General Assembly along with Dr Petr Horak from the Czech Republic.
Joan Peppard is Chief Pharmacist at the Health Service Executive in the Republic of Ireland. The new Board Members will share the title of Director of Professional Development.
Terry O’Niadh has been appointed to the board of VHI Healthcare by Minister for Health, Dr James Reilly. O’Niadh is currently the chair of the Monitoring & Evaluation (Quality Assurance) Committee, Local Authority
Services, National Training Group and a part time tutor with the Institute of Public Administration.
He has much experience in local government and served for 10 years as North Tipperary county manager, six years as assistant county manager, Kildare County Council and eight years as county secretary,
Wicklow County Council.
Mr Tony O'Brien has been appointed as the new Director General-designate of the HSE. Mr O'Brien is currently the Chief Operating Officer of the Special Delivery Unit in the Department of Health.
He will formally assume the position once the new legislation allowing for structural changes in the HSE is passed by the Oireachtas in the Autumn.
ICON plc a global provider of outsourced development services to the pharmaceutical, biotechnology and medical device industries has announced appointments to the senior management teams of its Clinical and
Central Laboratories businesses.
Dr. Nuala Murphy has been appointed Executive Vice President, Global Clinical Operations and Data Management, while Dr. Mark Roseman has joined ICON as Executive Vice President, Global Scientific
Operations. Dr. Era Khurana has joined ICON’s Central Laboratories’ leadership team as Medical Director.
Enterprise-Ireland has announced the appointment of Dr Arthur Rosenthal as its Life SciencesStart-up Ambassador for the US, as part of its strategy to promote Ireland’s offering and encourage overseas entrepreneurs to locate start-up businesses in Ireland.
Dr Rosenthal has spent more than 38 years developing medial device technologies as individual contributor, technology executive and serial entrepreneur. He is recognized internationally as a leading expert in the field of medical technology.
Teva Pharmaceuticals have announced the appointments of Dr. Carlo De Notaristefani as President andChief Executive Officer of Global Operations, and Mr. Aharon (Arik) Yaari as the Executive Vice President
to the newly created organisation, Community and Institutional Affairs.
Both Dr. De Notaristefani and Mr. Yaari will report directly to Dr. Jeremy Levin, President and Chief Executive Officer of Teva Pharmaceutical Industries and will join the Executive Team.


NEW