involvement & engagement in developing sexual health services a participatory action research...
TRANSCRIPT

Involvement & engagement in developing Sexual Health Services
A participatory action research study
Anne McNall - Senior Lecturer, HCES, Northumbria [email protected]
Principal Supervisor – Dr Sue Carr, Reader in Public Health, HCES, Northumbria University.
In partnership with: Dr. Helen McIlveen – Sexual Health
Lead, North Tyneside PCT Ian Atkinson – Commissioner,
NorthTyneside PCT

This presentation aims to
Explain background/rationale for study Explore the approach used Highlight issues linked to this approach Consider usefulness of approach to other
contexts Example of outcomes – what can we learn
Locally, regionally, nationally
Commissioners and Services should: Promote active user participation and involvement in
the planning and organization of services Develop their understanding of the various
communities they serve Recognise and respond to social exclusion,
discrimination and power imbalances (such as those between genders or individuals) in a way that enhances access, and promotes effective use of services
Ensure all staff involved in sexual health services are committed to non-discriminatory working practices and delivery of care”
Recommended Standards for Sexual Health Services, MedfASH 2005, p33

Why do people access sexual health services?
Sexually transmitted infectionSexually assaultedUnintended pregnancy, may want an abortionSexual difficulty, eg erectile dysfunctionContraception/ CondomsHIV positive
Just as many people with sexual health need never access services (NATSAL 2000)

What is known about the needs of service users in the context of sexual health? Comparatively little is known about sexual health service
user views (McNall 2003, 2006) The evidence available can be criticized for its failure to
explore perceived need, relying instead on positivist approaches to demonstrate satisfaction with what is offered (McNall 2003, 2006)
Studies identify expressed sexual morbidity, perceived stigma, unmet needs and dissatisfaction with the diagnosing health care providers counselling on emotional and sexual issues
Sexual health patients felt responsible that their problem(s) resulted from their own behaviours or inadequacies, felt stigmatized, were reluctant to give negative feedback, and therefore could reasonably be defined as disempowered.
Evans & Farquhar (1996), Holgate et al (1998), Duncan et al (2001), Scoular et al (2001), Nack (2001), and Dixon- Woods (2001)

PSA targets/Indicator metrics Reduce rate of under 18 conceptions by 55% by 2010 Increase uptake of long acting methods of contraception to 24%
by 2010 Increase percentage of sexually active population aged 15-24
screened for chlamydia from 17% last year, 35 % this year Guaranteed access to a GUM clinic within 48 hours
Percentage of abortions performed at < 10 weeks gestation Number of repeat abortions in <25 year olds Number of new diagnosis of gonorrhoea Proportion of HIV diagnosis where CD4 count is under 200 at time
of diagnosis Proportion of those reporting sexual assault seen within specialist
sexual assault services And so on……….

How can service users be involved and engaged in developing sexual health services?
An approach is needed that is able to align the apparent paradox of community and user need with strategic direction and local priorities in an area of practice where stigma and power imbalances militate against this.

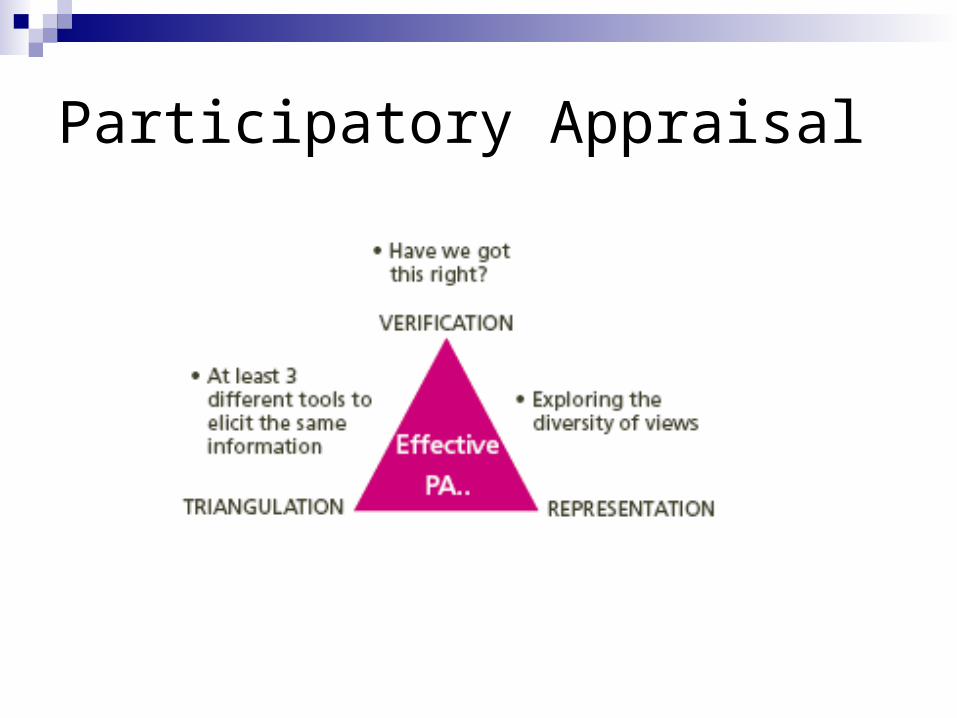
What is participatory appraisal? (Rapid Appraisal)
Flexible and practical participatory action research approach
Provides a framework to bring together communities and decision makers
Uses simple visual tools to increase inclusion Is interactive rather than extractive Is a rapid way of moving from insight to action
at low cost Results in policy change

Participatory Appraisal www.northumbria.ac.uk/peanut

Participatory Appraisal
Participatory Appraisal

A hierarchy of participation (Hart 1996)Mode of participation Involvement of local people Relationship of research and
action to local people
Co-optionToken; representatives are chosen, but no real input or power
On
ComplianceTasks are assigned, with incentives; outsiders decide agenda and direct the process
For
ConsultationLocal opinions asked;outsiders analyse and decide on a course of action
For /with
Co-operationLocal people work together with outsiders to determine priorities; responsibility remains with outsiders for directing the process
With
Co-learning
Participatory Appraisal
Local people and outsiders share their knowledge, to create new understanding, and work together to form action plans, with outside facilitation
With/by

The study
Commissioned by North Tyneside PCT SH implementation group– neighbourhood renewal funding
Recruited 3 teams of 3 co researchers – 3 public health practitioners, 6 volunteers from; voluntary sector, community development, social work, local authority, community health council
18 days in total 5 days training in PA 10 weeks to conduct study 3 days for development of reports

Ethical challenges Whilst PA offers a potentially innovative way to develop
practice, it has ethical considerations and challenges common to AR and PAR Williamson & Prosser (2002) AR
Khanlou & Peter (2005) PAR Offer a framework for evaluating studies
Social or scientific value Scientific validity Fair subject selection Informed consent Respect for potential and enrolled participants Favourable risk/benefit ratio Independent review

Social or scientific value
Aim is to improve public health & wellbeing Acknowledge the political and power imbalances
involved in stigmatized areas of practice Emancipatory – gives those disempowered or
without influence the opportunity to contribute at individual and service development level (THT 2004, 2005 1/3 of PCTs have not undertaken a sexual health needs assessment)
Philosophy of PA

Scientific validity Peiro et al (2002) see PA as enabling comparison of
health strategies in a way that can be understood by lay people as well as professionals.
Provides insight into participants beliefs and value systems through their perception of their needs. Wide reaching.
Range of qualitative data collection methods and triangulation of questions and tools
User need can not be the only determinant - allows sharing of quantitative data/ targets to inform decision making

Fair subject selection Must include diverse population to be
representative, specifically those with greatest sexual health need and/or excluded from involvementYoung people, children in the looked after system,
MSM, refugee and asylum seekers, those with MH problems, victims of domestic abuse, physical impairment or learning difficulty.
Must use large number of participants until saturation of data is reached

Fair subject selection – how?
Target established community groups, using co researcher community knowledge
(3 co-researcher teams, approx 3 groups per day x 10 days = 90 groups)
Some streetwork (2 hours, 90 responses) Staff working in sexual health services Decision makers in the Sexual Health
Implementation Group

Respect for potential and enrolled participants Co researchers:
Informed consent, time involvement, political & professional implications of questioning current practice.
Research involvement contract (Involve, 2005) Reimbursement of expenses or payment, and implications if in receipt
of benefits (DH 2006) Beebe (1995) PA tools are powerful, quickly uncover important and
potentially sensitive information, and requires the co researcher to give information.
Co-researcher training, philosophy and tools of PA, applied to SH context.
Working in co researcher teams of 3, one of whom is a registered accountable practitioner with subject specific and local service knowledge, and interpersonal skills to manage situations arising - stay within sight of each other.

Respect for potential and enrolled participants/Informed consent Research participants
Informed consent Groups.Written information in a range of accessible formats
sent to established groups 1 -2 weeks in advance. NB. Not being accessed as service users (although some will be) Choice of attending group session for PA study.
Streetwork. Verbal information given, written info if appropriate
Staff Usual information & consent forms with signature Anonymity & Confidentiality
Sexual health service users are given the choice of whether to provide personal identifying data (DH 2000)
Principles of informed consent read again at group meeting - co researchers verify that this was done. No individual signatures requested
Reminded of confidentiality risk of sharing personal information in group –option to provide individual feedback..

Respect for potential and enrolled participants/ informed consent Research participants
Vulnerable groups Exclude under 13’s (not able to consent under
sexual offences Act 2003) 13-16 Year olds assessed using the North
Tyneside assessment tool (Based on Fraser/DH guidelines 2004) for their competence to consent.
If deemed competent, would be given access to information and sexual health services without parental consent.
Those with learning difficulty, mental health problems also assessed using same tool

Favourable risk/ benefit ratio
PAR – potential for raising awareness and consciousness, but also expectations
PA asks participants to identify issues, solutions and prioritise actions, therefore is realistic in what it can achieve, and highlighted in information sheets.
Service user perspectives are required aspect of contemporary practice– little evidence of this occurring in SH – transferable approach for other areas of practice.
Potential risk to research participants - CRB checks, training, support of co researcher team.

Tools/ questions asked
Mapping Time lines Force field analysis Pie charts Venn diagrams Daily schedules Flow charts
Causal impact diagrams
Criteria ranking Impact ranking Evaluation wheel Spider diagram Card sorting Completing statements

Findings Feed back of PA findings
To sexual health implementation group (providers, voluntary agencies, managers, commissioner)
Aiming for direction for next phase – what else do we need to ask, who do we need to include?
Translational research findingsCritical discourse analysis of discussion – can
user views established via PA approach influence decision making?

Strengths of PA for involvement and engagement in a stigmatised context
Seeks opinions from a community not previously involved in decision making
Explores local knowledge – essential component in social marketing
Looks at whole systems/ all stakeholders Rigorous - validity of data/ triangulation Flexible - adapt as you progress Variety of data collection tools – acceptable, low
literacy requirement Quick/ low cost – reality! Empowering- plans rooted in local context – reality!

Limitations Defining the community – huge area PA often ceases to be participatory after the data collection
stage (Ong 1996) Rigour
does opening up the process to unskilled participants affect the quality and credibility of data?
Do people know what they need? Bias –
which informants? Need to include many individuals and groups in the process
Research governance! – Is PA research or evaluation?

Outcomes- Translational research in public health
Critical discourse analysis - transferable learning to inform potential of involvement and engagement to change practice in a challenging context.Hodge (2002)

Outcomes –
Insight from this broader doctoral study has enabled National policy change on workforce development - need
practitioners able to lead sexual health needs assessment
DH(2008) Sexual Health Advising – Developing the Workforce
Regional workforce development innovation project – develop capacity for change in NHS NE
Sexual Health Adviser Pathway of Specialist Community Public Health Nursing Programme
Curriculum development- PA as a participatory action research method – with potential to practice skills


References Beebe, J. (1995) Basic concepts and techniques of rapid appraisal. Human Organization
54(1) 42-51 Chambers, R. (1993) Treading more carefully: participatory rural appraisal – past , present
and future. New Ground 13, 12-13. Hart R (1996) Children’s Participation: The Theory and practice of Involving Young Citizens
In Community Development and Environmental Care, UNICEF Hodge, S. (2005) Participation, discourse and power: a case study in service user
involvement. Critical Social Policy 25 (2) 164-171 Khanlou, N. Peter, E. (2005) Participatory action research: considerations for ethical review.
Social Science and Medicine 60, 2333-2340 Lawlor, D. et al. (1999) Rapid participatory appraisal of young people’s sexual health needs:
an evaluation of meta-planning. Health Education Journal 58, 228-238. Nack, A. (2001) Damaged Goods. The sexual self-transformations of women with chronic
STD’s. Unpublished PhD thesis. University of Colorado Ong, B.N. (1996) Rapid Appraisal and Health Policy. Chapman & Hall Peiro, R. et al (2002) Rapid Appraisal Methodology for “Health for all” policy formulation
Health Policy 62 (3) 309-328 Philip, K. (2001) Young people’s health needs in a rural area: lessons from a participatory
rapid appraisal study. Youth & Policy (71), 5-24. Taket, A . White, L. (1998) Experience in the Practice of One Tradition of Multimethodology.
Systemic practice and action research. 11(2) 154 -168 Williamson, GR. & Prosser, S. (2002) Action Research: politics, ethics and participation.
Journal of Advanced Nursing. 40 (5) 587-593