investigational brochure reg1 … brochure . reg1 anticoagulation system . version number: 5.4 ....
TRANSCRIPT

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 1 of 105 CONFIDENTIAL
INVESTIGATIONAL BROCHURE
REG1 ANTICOAGULATION SYSTEM
Version Number: 5.4
Release Date: 09 Oct 2013
Replaces Previous Version Number:
5.3
Previous Version Date: 16 Jul 2013 (Version 5.3)
IND Number: 63,275
Sponsor: Regado Biosciences, Inc.
120 Mountain View Boulevard, 1st
Basking Ridge, NJ 07920
Floor
Confidentiality Statement
The confidential information in the following document is provided to you as an Investigator, potential Investigator, or consultant for review by you, your staff, and applicable Institutional Review Board. The information contained herein should not be disclosed to others, without written authorization from Regado Biosciences, Inc., except to the extent necessary to obtain informed consent from those persons to whom the drug will be administered.


REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 3 of 105 CONFIDENTIAL
TABLE OF CONTENTS
TABLE OF CONTENTS .................................................................................................................3
LIST OF ABBREVIATIONS ........................................................................................................10
1. SUMMARY ................................................................................................................12
1.1. Clinical Rationale for the REG1 Anticoagulation System .........................................12
1.1.1. What is the REG1 Anticoagulation System? ..............................................................12
1.1.2. Acute Care Anticoagulation ........................................................................................13
1.1.3. Rationale for Targeting Coagulation FIXa Activity ...................................................13
1.2. Physical, Chemical and Pharmaceutical Properties of the REG1 Anticoagulation System ..............................................................................................16
1.3. Nonclinical Studies .....................................................................................................16
1.3.1. Pharmacology Summary .............................................................................................16
1.3.2. Pharmacokinetic Summary ........................................................................................17
1.3.3. Toxicology Summary ..................................................................................................18
1.4. Clinical Studies ...........................................................................................................20
1.5. Section 1 References ...................................................................................................21
2. PHYSICAL, CHEMICAL AND PHARMACEUTICAL PROPERTIES AND FORMULATION ..............................................................................................24
2.1. Description of Drug Substance ...................................................................................24
2.1.1. Description and Composition of Pegnivacogin Injection ...........................................25
2.1.2. Description and Composition of Anivamersen Injection ...........................................25
2.2. Storage and Handling ..................................................................................................26
2.3. Preparation of Drug Product Injection ........................................................................26
2.3.1. Pegnivacogin Drug Product Injection .........................................................................26
2.3.2. Anivamersen Drug Product Injection .........................................................................26
3. NONCLINICAL STUDIES ........................................................................................27
3.1. Introduction .................................................................................................................27
3.2. Nonclinical Pharmacology ..........................................................................................28
3.2.1. Integrated Discussion of Nonclinical Pharmacology Data .........................................28
3.3. Pharmacokinetics (Toxicokinetics) ............................................................................29
3.3.1. Integrated Discussion of Toxicokinetic Data ..............................................................29
3.4. Toxicology ..................................................................................................................31

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 4 of 105 CONFIDENTIAL
3.4.1. Rationale for Types of Studies, Species Selection and Study Design Elements .....................................................................................................................31
3.4.2. Types of Studies ..........................................................................................................31
3.4.3. Selection of Species ....................................................................................................32
3.4.4. Study Design Elements ...............................................................................................33
3.4.5. Extrapolation of Doses Across Species ......................................................................33
3.4.6. Integrated Discussion of the Nonclinical Toxicity Study Findings ............................34
3.4.7. Monkey Safety Pharmacology Studies .......................................................................34
3.4.8. Initial Single- and Repeat-dose Intravenous Toxicity Study in Monkeys ..................36
3.4.9. 14-Day Intravenous Study in Mice .............................................................................37
3.4.10. Two-week Intravenous Toxicity Study in Monkeys ...................................................38
3.4.11. Two and Four-week Subcutaneous Toxicity Studies of Pegnivacogin.......................39
3.4.12. Comments on Immunogenicity and Immunotoxicity .................................................39
3.4.13. Blood Compatibility Study and Vascular Tolerability ...............................................40
3.4.14. Genetic Toxicity Studies .............................................................................................40
3.4.15. Conclusions About REG1 Safety ...............................................................................41
3.5. Section 3 References ...................................................................................................43
4. EFFECTS IN HUMAN SUBJECTS ..........................................................................45
4.1. Overview of Clinical Studies ......................................................................................45
4.1.1. REG1-CLIN101 ..........................................................................................................47
4.1.2. REG1-CLIN102 ..........................................................................................................47
4.1.3. REG1-CLIN103 ..........................................................................................................48
4.1.4. REG1-CLIN210 ..........................................................................................................49
4.1.5. REG1-CLIN220a ........................................................................................................50
4.1.6. REG1-CLIN211 (RADAR) ........................................................................................50
4.2. Total exposure ............................................................................................................56
4.3. Clinical Pharmacology ................................................................................................58
4.3.1. Measures of Coagulation ............................................................................................58
4.3.2. Pharmacodynamic drug interactions ...........................................................................59
4.3.3. Overview of Clinical PD and PK/PD Studies .............................................................64
4.3.4. Clinical Pharmacokinetics ..........................................................................................66
4.3.5. REG1-CLIN211 Pharmacokinetic Sub-Study Results ...............................................70

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 5 of 105 CONFIDENTIAL
4.3.6. Clinical Pharmacodynamics .......................................................................................71
4.3.7. Conclusions.................................................................................................................77
4.4. Anivamersen Reversal of Pegnivacogin .....................................................................78
4.4.1. Analysis of the Anivamersen Anticoagulant Reversal Dose Response ......................78
4.4.2. Anivamersen Anticoagulant Reversal Effects in Elective PCI ...................................79
4.4.3. Anivamersen Anticoagulant Reversal Effects in ACS ...............................................80
4.4.4. Conclusions.................................................................................................................83
4.5. Safety of REG1 ...........................................................................................................83
4.5.1. Phase 1 Adverse Events ..............................................................................................84
4.5.2. Phase 1 Adverse Events Summary .............................................................................85
4.5.3. Phase 2a Adverse Events ............................................................................................86
4.5.4. Phase 2b Adverse Events (REG1-CLIN211) .............................................................87
4.5.5. Serious Adverse Events ..............................................................................................91
4.5.6. Reference Safety Information .....................................................................................95
4.6. Summary and Conclusions from Clinical Studies ......................................................96
4.7. Marketing Experience .................................................................................................98
4.8. Section 4 References ...................................................................................................98
5. SUMMARY OF DATA AND GUIDANCE FOR THE INVESTIGATOR .....................................................................................................100
5.1. Indications and Usage ...............................................................................................100
5.2. Dosage and Administration ......................................................................................100
5.3. Dosage Forms and Strengths ....................................................................................100
5.4. Contraindications ......................................................................................................100
5.5. Warnings/Precautions ...............................................................................................100
5.6. Adverse Events .........................................................................................................101
5.7. Drug Interactions ......................................................................................................102
5.8. Use in Specific Populations ......................................................................................102
5.9. Drug Abuse and Dependence....................................................................................103
5.10. Overdosage ...............................................................................................................103
5.11. Description ................................................................................................................103
5.12. Clinical Pharmacology ..............................................................................................104
5.13. Nonclinical Pharmacology ........................................................................................104

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 6 of 105 CONFIDENTIAL
5.14. Nonclinical Toxicology ............................................................................................104
5.14.1. Carcinogenesis, Mutagenesis, Impairment of Fertility .............................................104
5.14.2. Animal Toxicology ...................................................................................................104
5.15. Clinical Studies .........................................................................................................105
5.16. How Supplied/Storage and Handling .......................................................................105
5.17. Patient Counseling Information ................................................................................105

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 7 of 105 CONFIDENTIAL
LIST OF TABLES
Table 1: Listing of Nonclinical Pharmacology Studies of the REG1 System...........................16
Table 2: Listing of Nonclinical Studies with Pharmacokinetic Endpoints ...............................17
Table 3: Listing of Toxicity Studies of the REG1 System and Components ............................19
Table 4: Listing of Clinical Studies Conducted with REG1 .....................................................46
Table 5: Randomized and treated patients in CLIN211 ............................................................51
Table 6: Treatment Strategies for REG1-CLIN211 ..................................................................52
Table 7: REG1-CLIN211 Bleeding Events (ITT Population) through Day 30 .........................53
Table 8: REG1 Subject Exposure and Duration of Follow-up .................................................56
Table 9: Continued (REG1 Subject Exposure and Duration of Follow-up) .............................57
Table 10: Listing of Clinical Studies with Pharmacokinetic and Pharmacodynamic Data .............................................................................................................................65
Table 11: Summary of Pegnivacogin Pharmacokinetic Parameters in Humans .........................69
Table 12: REG1-CLIN211 PK results ........................................................................................71
Table 13: REG1-CLIN211 PD (aPTT) results ............................................................................76
Table 14: Comparison of the Predicted PD Responses of Anivamersen to the Observed Response of Relative aPTT by Timepoint: PP Population (with No Prior Heparin) .......................................................................................................81
Table 15: Summary of Adverse Event Occurring in ≥2 REG1 Subjects for Study REG1-CLIN101 ..........................................................................................................84
Table 16: Summary of Adverse Events Occurring in ≥2 REG1 Subjects for Study REG1-CLIN102 ..........................................................................................................85
Table 17: Summary of Adverse Event Occurring in ≥2 REG1 Subjects for Study REG1-CLIN103 ..........................................................................................................85
Table 18: Summary of Non-bleeding Adverse Event Occurring in ≥2 REG1 Subjects for Study REG1-CLIN210 ...........................................................................86
Table 19: Summary of Bleeding Adverse Event Occurring in ≥2 REG1 Subjects for Study REG1-CLIN210 ................................................................................................87
Table 20: Number (Incidence) of Treatment-Emergent Adverse Events and Relationship to Study Medication for in Study REG1-CLIN211 ...............................88
Table 21: Summary of Treatment-Emergent Adverse Events Occurring in ≥2 REG1 Subjects and Classified with a “Possible” or “Probable” Relationship to Study Medication for Any Dose Group in Study REG1-CLIN211 ............................89
Table 22: Summary of Non Bleeding, Drug Related Adverse Events Occurring in >1 REG1 Subjects (by Frequency and Severity) ........................................................95

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 8 of 105 CONFIDENTIAL
LIST OF FIGURES
Figure 1: Coagulation Reaction ..................................................................................................14
Figure 2: The REG1 Anticoagulation System ............................................................................24
Figure 3: Low Intra- and Inter-Subject Variability with Repeat Doses of pegnivacogin and Anivamersen (Study REG1-CLIN103) .........................................49
Figure 4: REG1-CLIN211 ACUITY Bleeding – ITT Population Through Day 30 ..................54
Figure 5: REG1-CLIN211 Bleeding Through Hospital Discharge ............................................54
Figure 6: REG1-CLIN211 Composite Ischemic Events ITT Population Through Day 30 .........................................................................................................................55
Figure 7: REG1-CLIN211 Composite Ischemic Events Through Discharge .............................55
Figure 8: FIX Activity Assay Standard Curve in Human Plasma ..............................................59
Figure 9: Interaction of Pegnivacogin with Heparin and Lepirudin: aPTT Results. ..................60
Figure 10: Interaction of Pegnivacogin with Heparin and Lepirudin: CAT Results. ...................61
Figure 11: Interaction of Pegnivacogin with Warfarin. ................................................................63
Figure 12: Interaction of Pegnivacogin with rFVIIa and aPCC. ..................................................64
Figure 13: Mean Anivamersen Plasma Concentration vs Time Profile (REG1-CLIN101) ....................................................................................................................66
Figure 14: Mean pegnivacogin Plasma Concentration vs Time Profile in Subjects Treated with REG1 (REG1-CLIN101) .......................................................................67
Figure 15: Mean pegnivacogin Plasma Concentration vs Time Profile (REG1-CLIN101) ....................................................................................................................68
Figure 16: Relationship between aPTT Response and Pegnivacogin Dose (mg dose) ................72
Figure 17: Percent FIX inhibition vs. dose for healthy volunteers (REG1-CLIN101) and patients with coronary artery disease (REG1-CLIN102) .....................................73
Figure 18: REG1-CLIN210 Intraprocedure Plasma aPTT Results ..............................................74
Figure 19: REG1-CLIN210 Intraprocedure POC aPTT Results ..................................................74
Figure 20: REG1-CLIN210 Intraprocedure ACT Results ............................................................75
Figure 21: CLIN211- Relative aPTT vs Plasma Pegnivacogin Concentration ............................76
Figure 22: Percent FIX Inhibition (all Post Dose Time points) ...................................................77
Figure 23: Anivamersen Anticoagulant Reversal Dose Response ...............................................78
Figure 24: Pharmacodynamic Effects of Pegnivacogin and Reversal Effects of Anivamersen in PCI ....................................................................................................79
Figure 25: The REG1 Anticoagulation System ..........................................................................103

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 9 of 105 CONFIDENTIAL
REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 10 of 105 CONFIDENTIAL
LIST OF ABBREVIATIONS ACS Acute coronary syndromes ACT Activated clotting time AE Adverse event ANOVA Analysis of variance APTT Activated partial thromboplastin time CABG Coronary artery bypass grafting CHO Chinese hamster ovary CPB Cardiopulmonary bypass ECG Electrocardiogram FV Coagulation Factor V FVa Activated coagulation Factor Va FVIII Coagulation Factor VIII FVIIIa Activated coagulation Factor VIII FIX Coagulation Factor IX FIXa Activated coagulation Factor IXa FX Coagulation Factor X FXa Activated coagulation Factor FXa FXI Coagulation Factor XI FXIa Activated coagulation Factor XIa HIT Heparin-induced thrombocytopenia HITT Heparin-induced thrombocytopenia with thrombosis IV Intravenous LLOQ Lower limit of quantitation LMWH OPCAB
low molecular weight heparins Off-pump coronary artery bypass graft surgery
NSTE Non-ST Elevation myocardial infarction PD Pharmacodynamic PCI Percutaneous coronary intervention PD Pharmacodynamic PEG Polyethylene glycol PK Pharmacokinetic PT Prothrombin Time RB006 Pegnivacogin - anticoagulant component of REG1 RB007 Anivamersen - control agent component of REG1 RNA Ribonucleic acid

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 11 of 105 CONFIDENTIAL
SAE Serious adverse event ULN Upper limit of normal USP United States Pharmacopeia UFH Unfractionated heparin

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 12 of 105 CONFIDENTIAL
1. SUMMARY
1.1. Clinical Rationale for the REG1 Anticoagulation System
1.1.1. What is the REG1 Anticoagulation System?
The REG1 Anticoagulation System is a novel exploitation of the aptamer-control agent strategy. It consists of a highly potent oligonucleotide-based aptamer against coagulation Factor IXa (FIXa) and a specific control agent that can hybridize to the aptamer and neutralize its activity. The drug component of the REG1 Anticoagulation System (pegnivacogin or RB006a
The control agent component of the REG1 Anticoagulation System (anivamersen or RB007
) is a modified RNA aptamer, 31 nucleotides in length, which is stabilized against nuclease-mediated degradation. The nucleic acid portion of the aptamer is conjugated to a 40-kilodalton polyethylene glycol (PEG) carrier to increase its blood half-life and permit administration of a single intravenous dose to maintain anticoagulation over an extended period of time. Nonclinical pharmacology studies have shown that the aptamer molecule can effectively inhibit coagulation in a variety of in vitro and in vivo models.
a
Regado Biosciences, Inc. (Regado) is developing the REG1 Anticoagulation System to provide real time direct control of anticoagulation to the physician to address the unmet clinical need for an effective, safe and rapidly reversible anticoagulant. Specifically, REG1 is being developed for use as an anticoagulant system in coronary revascularization procedures to treat coronary and peripheral artery disease, for use in patients suffering from acute coronary syndromes (ACS), and as an anticoagulant for other indications in which it would be advantageous for the physician to have direct control of the agent employed for anticoagulant or antithrombotic therapy. Coagulation Factor IXa (FIXa) is an attractive target for the development of such an agent because inhibition of FIXa is anticipated to be effective in both the prevention and treatment of arterial and venous thrombosis, and because FIXa has been extensively validated in animal studies and – to a lesser extent – in human studies as a target for anticoagulant therapy in these indications. Nonclinical studies presented here demonstrate the anticoagulant and antithrombotic potency of pegnivacogin, as well as the ability of the control agent, anivamersen, to rapidly and dose dependently neutralize its effect, and thereby restore a desired level of hemostatic function. Clinical studies presented here
) is an RNA oligonucleotide, 15 nucleotides in length, which is complementary to a portion of pegnivacogin. The control agent component is also stabilized against nuclease degradation, to an extent that enables it to seek and bind pegnivacogin, but these modifications do not support extended in vivo activity. Studies described in subsequent sections show that the control agent binds to the anticoagulant and rapidly neutralizes its activity and that the inactive complex is cleared from circulation.
a Pegnivacogin is referred to as RB006 and anivamersen as RB007 in some publications, reports and documents.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 13 of 105 CONFIDENTIAL
demonstrate the anticoagulant potency, long duration and reproducibility of effect of pegnivacogin, and the ability of anivamersen to dose dependently neutralize a portion of, or all the anticoagulant activity of pegnivacogin. Both nonclinical and clinical studies attest to the safety and tolerability of the REG1 Anticoagulation System and its components.
1.1.2. Acute Care Anticoagulation
Clinicians must weigh the characteristics of various strategies of anticoagulation in choosing which method to use for an individual patient or patient-population. Considerations include whether immediate therapeutic anticoagulation is required; or if it is acceptable to slowly, over the course of hours or days, achieve therapeutic blood-thinning; what the estimated risk of an individual patient or patient population is to bleed given their demographic and clinical features; whether the patient requires chronic anticoagulation; how quickly anticoagulation can be reversed, if necessary; and whether reversal of anticoagulation results in diminished or delayed ability to repeat anticoagulation.
Given the central role of thrombosis in the pathobiology of acute ischemic heart disease, injectable (IV or subcutaneous) anticoagulants have become the foundation of medical treatment for patients presenting with ACS (unstable angina and myocardial infarction) and for those undergoing coronary revascularization procedures, either percutaneously or surgically (Harrington et al., 2004; Popma et al., 2004). Currently available anticoagulants include unfractionated heparin (UFH), the low molecular weight heparins (LMWH), and the direct thrombin inhibitors (e.g., recombinant hirudin, bivalirudin, and argatroban). The present paradigm, both for anticoagulant use and for continued antithrombotic drug development, is to establish a balance between efficacy (reducing the risk of ischemic events) and safety (minimizing the risk of bleeding) (Harrington et al., 2004). Each of the available agents carries an increased risk of bleeding relative to placebo. Therefore, despite the continued development of novel antithrombotics, a significant clinical need exists for safer and more effective anticoagulant agents.
1.1.3. Rationale for Targeting Coagulation FIXa Activity
In contrast to the traditional Macfarlane (Macfarlane 1964) and Davie and Ratnoff (Davie and Ratnoff. Science 1964) “waterfall” models, our current view of the process leading to fibrin deposition in vivo acknowledges the important interplay between the protease-driven coagulation process and the cells or surfaces upon which these reactions occur (Figure 1) (Monroe et al., 2002). In the cell-based coagulation model, the “extrinsic” and “intrinsic” pathways are merged into a staged series of events in which 1) the Tissue Factor (TF)–Factor VIIa (FVIIa) complex (extrinsic pathway) initiates coagulation, and 2) the intrinsic, or contact activation, pathway drives propagation of thrombin generation and fibrin clot formation.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 14 of 105 CONFIDENTIAL
Figure 1: Coagulation Reaction
Figure 1: During the initiation phase of coagulation, which occurs on TF-bearing cells, small amounts of
coagulation FXa and IXa (not shown) are generated, leading to generation of small amounts of thrombin (FIIa). Thrombin generated during initiation is insufficient to catalyze fibrinogen (Fg) cleavage. Rather, it activates small amounts of FV and FVIII to prime propagation, and activates platelets to establish the surface upon which propagation occurs. Thrombin generated during the propagation phase cleaves Fg to generate the fibrin (Fn) clot and feeds back into the cycle, further driving the process via activation of FXI to FXIa and continued generation of FVa and FVIIIa (Monroe et al., 2002).
In both the traditional and modern views of coagulation, amplification remains a common feature at every step from initiation to thrombin generation. Thus, two key considerations shape the choice of target for anticoagulant therapy. First, blocking the pathway before the significant amplification and positive feedback cycles should provide efficient blockade. Second, targeting the rate-limiting step should provide effective anticoagulation with the widest therapeutic window. The FVIIIa/FIXa complex drives propagation upstream of both the significant amplification at the FVa/FXa step and the positive-feedback cycle driven by thrombin generation. Furthermore, FVIIIa/FIXa-catalyzed activation of coagulation FX appears to be the rate-limiting step for thrombin generation (Hoffman et al., 1995; Rand et al., 1996; Butenas et al., 2004).
The earliest evidence of the critical role of FIXa as the limiting protease in thrombin generation comes from animal modeling (Gitel et al., 1977). Using purified, activated coagulation proteases, Gitel et al. (1977) investigated the thrombogenicity of FIXa, FXa and thrombin in the Wessler model of venous thrombosis. FIXa was ~7-fold more thrombogenic than FXa and 60-fold more thrombogenic than thrombin. Similarly, inhibition of venous thrombosis initiated by FIXa required heparin doses that were 2-4–fold lower than those

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 15 of 105 CONFIDENTIAL
required to inhibit clot formation when venous thrombus generation was initiated by FXa or thrombin (Gitel et al., 1977). Thus FIXa is rate-limiting in thrombus generation, and, based upon the relative sensitivities to heparin, inhibition of FIXa versus FXa or thrombin might provide a wider therapeutic window.
Multiple orthogonal studies have confirmed these early discoveries. In vivo and in vitro investigations of the thrombogenicity of prothrombin-complex concentrates demonstrated that the FIXa level determines the thrombogenic potential of these factor-replacement concentrates (Gray et al. 1995). Molecular genetic studies using FIX-deficient mice have shown that FIXa is a critical regulator of thrombin generation, and that in vivo FIXa activity determines susceptibility to occlusive venous thrombus formation in a murine model of saphenous vein thrombosis (Buyue et al. 2008). Similarly, loss of the intrinsic pathway protects mice from pulmonary embolism (PE) induced by polyphosphate, the molecular trigger linking coagulation initiation and platelet activation to coagulation propagation (Müller et al. 2009).
Further evidence for FIXa as a viable target for anticoagulant therapy resides in the manifestations of FIX deficiency in patients with and carriers of hemophilia B. The clinical phenotype of Hemophilia B depends on the plasma FIX level. Spontaneous bleeding occurs in patients with severe hemophilia (< 1% FIX activity), whereas bleeding occurs only with trauma or surgery in those with moderate hemophilia (1%–5% FIX activity). The tendency to bleed from small wounds and during surgery decreases as factor levels increase in patients with mild hemophilia (> 5% FIX activity) and Hemophilia B carriers (median FIX activity 60%) (Plug et al. 2006). Mild FIX deficiency may not prolong activated partial thromboplastin time (aPTT) or require prophylaxis to prevent bleeding during minor procedures, but, in epidemiological studies, it has been associated with fewer cardiovascular events (Šrámek et al. 2003; Tuinenberg et al. 2009). The narrow window for clinically important bleeding with a wider window for reduced cardiovascular events in Hemophilia B carriers lends further support for FIXa as an attractive target for anticoagulant therapy.
Generation of FIXa inhibitors using traditional active-site, small-molecule approaches is challenging because the active site of FIXa does not adopt its functional structure until allosteric activation upon complex formation with FVIIIa (Fay et al. 1998; Misenheimer et al. 2007). Consequently, most FIX/FIXa inhibitors evaluated in preclinical models have been designed to block protein–protein or other macromolecular interactions, such as active site-inhibited FIXa (Benedict et al. 1991; Choudhri et al. 1999), which blocks formation of the FVIIIa/FIXa complex; monoclonal antibodies against the FIX/IXa gla-domain (Toomey et al. 2000), which block binding of FIX/FIXa to cell surfaces; or nucleic-acid aptamers (Rusconi et al. 2002), which block the interaction of FX with the FVIIIa/FIXa complex.
Consistent with mechanistic, molecular genetic, and epidemiological data, evaluations of anti-FIXa agents in arterial thrombosis models have validated FIXa as an optimal target for treatment and prophylaxis of arteriothrombotic indications. Results of preclinical evaluations in venous thrombosis models, although rarer, are consistent with those conducted in arterial thrombosis models and suggest that FIX/FIXa inhibition is as efficacious as unfractionated heparin (UFH) treatment and might have a wider therapeutic window (Feuerstein et al. 1999).

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 16 of 105 CONFIDENTIAL
1.2. Physical, Chemical and Pharmaceutical Properties of the REG1 Anticoagulation System
The REG1 Anticoagulation System consists of a highly potent oligonucleotide-based aptamer against coagulation Factor IXa and an active control agent that can hybridize to the aptamer and neutralize its activity.
1.3. Nonclinical Studies Regado Biosciences, Inc. has conducted a comprehensive program of nonclinical studies to characterize the pharmacology, disposition and toxicology of the REG1 Anticoagulation System and its individual components in vitro and in animals in support of the clinical evaluation of the system. A summary of this program is provided herein.
1.3.1. Pharmacology Summary
Regado Biosciences has conducted a number of nonclinical pharmacology studies of the REG1 Anticoagulation System and its components to provide an understanding of the pharmacology of the System in animals, and verify the pharmacologic activity of the System in the key toxicology species. In particular, studies were designed to test the efficacy of pegnivacogin in preventing clot formation induced by a number of clinically relevant stimuli and to verify the safety and efficacy of reversal of pegnivacogin anticoagulation by the anivamersen control agent in clinically relevant settings. A listing of these studies is provided in Table 1, and an integrated discussion of the findings from these studies is provided in Section 3
Table 1: Listing of Nonclinical Pharmacology Studies of the REG1 System
.
Type of Study Species Experimental System Salient Findings
Arterial thrombosis Mouse FeCla 3 Anti-FIXa aptamer blocked occlusive thrombus formation
damage of carotid artery, with thrombus formation analyzed by Doppler flow and histology
Bleeding challenge Mousea Anti-FIXa aptamer administered at 20X the effective antithrombotic dose, followed by tail transection and control agent administration with measurement of total blood loss over a 15-minute window
High doses of anti-FIXa aptamer induced bleeding upon surgical challenge, and the control agent prevented bleeding

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 17 of 105 CONFIDENTIAL
Cardiopulmonary bypass/CABG
Pig Various studies evaluating the ability of pegnivacogin to support cardiopulmonary bypass circuits, including pump times out to 4 hr; some studies included coronary artery bypass grafting
Pegnivacogin, as the sole anticoagulant, supported CPB and CABG
Pharmacodynamic effect
Cynomolgus monkey b
IV administration of pegnivacogin with or without subsequent anivamersen administration, with collection of PD data for 7 days
Pegnivacogin dose-dependently prolonged aPTT and ACT; anivamersen rapidly and durably reversed this effect
a The less potent prototypes of the drug and control agent, referred to as RB002 and RB004, respectively, were used in the mouse studies
b
1.3.2. Pharmacokinetic Summary
Pharmacodynamic effects of the REG1 System in monkeys were evaluated as part of REG1-TOX001, "An Assessment of the Potential Cardiovascular, Respiratory, and Neurologic Effects of REG1 (Aptamer/Control Agent Combination) Administered Intravenously to Cynomolgus Monkeys”
Regado has conducted a comprehensive program of nonclinical studies to determine the pharmacokinetic properties of pegnivacogin, anivamersen and the complex of pegnivacogin and anivamersen formed upon administration of anivamersen to animals previously receiving pegnivacogin. State-of-the-art bioanalytical methods were developed and validated to enable quantification of the concentrations of free pegnivacogin, free anivamersen, and the pegnivacogin/anivamersen complex in plasma from monkeys and mice. These methods were applied to the analysis of plasma samples collected from the toxicology studies listed in Table 2.
An integrated discussion of the findings from these studies can be found in Section 3.3.
Table 2: Listing of Nonclinical Studies with Pharmacokinetic Endpoints
Abbreviated Title
Regado Study Number
Species Number of Dose Levels
Number of Animals per Sex per Group
Duration of Study
Safety Pharmacology IV Study
REG1-TOX001
Cynomolgus monkeys
2 2 a 7 days
14-day repeat-dose toxicity study
REG1-TOX002
Mice 3a 8 14 days

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 18 of 105 CONFIDENTIAL
Abbreviated Title
Regado Study Number
Species Number of Dose Levels
Number of Animals per Sex per Group
Duration of Study
14-day single- and repeat-dose IV toxicity study
REG1-TOX003
Cynomolgus monkeys
4a 2 ,b 14 days
14-day IV toxicity study
REG1-TOX006
Cynomolgus monkey
3a 5 ,c 14 days
Exploratory SC PK, PD study
REG1-PHRM010
Cynomolgus monkey
3 2d 7 days e
14-day SC toxicity study
REG1-TOX006
Cynomolgus monkey
3 3 at lower dose levels
5 at highest dose level
14 days
28-day SC toxicity study
TOX-RB006-10-001
Rats 3 6 28 days
28-day SC toxicity study
TOX-RB006-10-002
Dogs 3 3 at lower dose levels
5 at highest dose level
28 days
a Each study contained dose groups treated with pegnivacogin, anivamersen or pegnivacogin followed by anivamersen (REG1). Analysis of each of the 3 analytes (pegnivacogin, anivamersen, pegnivacogin /anivamersen complex) was included in each study.
b Four single dose pegnivacogin dose levels, 2 single dose and 1 repeated dose anivamersen dose levels, 3 REG1 single dose and 1 repeat dose levels.
c 3 pegnivacogin dose levels, 1 REG1 dose level. d 2 dose levels each of single dose SC pegnivacogin, single dose SC pegnivacogin followed by IV anivamersen,
and repeat dose SC pegnivacogin e
1.3.3. Toxicology Summary
Males only, 2 per dose level in each treatment group
Regado Biosciences has conducted a comprehensive series of nonclinical toxicity studies to support clinical trials. These are listed in Table 3. The general rationale for the types of studies conducted with the REG1 Anticoagulation System, the selection of species and the primary design considerations are presented below in Section 3.4.1., and an integrated discussion of the overall study findings is presented in Section 3.4.6.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 19 of 105 CONFIDENTIAL
Table 3: Listing of Toxicity Studies of the REG1 System and Components
Abbreviated Title Regado Study Number
Test Facility Testing Facility
Study No.
GLP Status
28-day repeat dose SC toxicity study of pegnivacogin in dogs
TOX-RB006-10-002
ITR Laboratories 60666 Yes
28-day repeat dose SC toxicity study of pegnivacogin in rats
TOX-RB006-10-001
ITR Laboratories 71092 Yes
14-day repeat dose SC toxicity study of pegnivacogin in cynomolgus monkeys
REG1-TOX007 Charles River Laboratories
Nevada
PBK00015 Yes
14-day single- and repeat-dose IV toxicity study in cynomolgus monkeys
REG1-TOX003 Charles River Laboratories
Sierra Division
PBK00002
a
Yes
14-day repeat-dose toxicity IV study in mice
REG1-TOX002 ClinTrials BioResearch
500155 b
Yes
Safety pharmacology IV study in cynomolgus monkeys
REG1-TOX001 Charles River Laboratories
Sierra Division
PBK00001
a
Yes
Safety pharmacology IV study comparing 2 batches of pegnivacogin in cynomolgus monkeys
TOX-RB006-10-003
MPI Research 1278-002 Yes
14-day IV toxicity study in cynomolgus monkeys
REG1-TOX006 Charles River Laboratories
Nevada
PBK00011 Yes
In vitro blood compatibility study REG1-TOX005 ClinTrials BioResearch
600076 b
Yes
Bacterial mutagenicity assay REG1-TOX004a BioReliance AA97RZ-SB.503.BTL
Yes
Chromosome aberrations assay in Chinese hamster ovary cells
REG1-TOX004b BioReliance AA97RZ-SA.331.BTL
Yes
Chromosome aberrations assay in human peripheral blood leukocytes
REG1-TOX004d BioReliance AA97RZ-SB.341.BTL
Yes
In vivo mouse micronucleus assay REG1-TOX004c BioReliance AA97RZ-SB.123.BTL
Yes
In Vitro Evaluation of pegnivacogin as an Inhibitor of Human Cytochrome P450 Enzymes
PHARM-RB006-09-01
XenoTech XT085099 Yes
In Vitro Evaluation of pegnivacogin /anivamersen Duplex as an Inhibitor of Human Cytochrome P450 Enzymes
PHARM-RB006-09-02
XenoTech XT085105 Yes
REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 20 of 105 CONFIDENTIAL
a Currently referred to as Charles River Laboratories Nevada b
1.4. Clinical Studies
Currently referred to as Charles River Laboratories Montreal
See Section 4 for a detailed review of all completed studies using the REG1 System. A list of all clinical studies conducted with REG1 is presented in Table 4.
REG1 has been investigated in six clinical studies to date (three Phase 1 and three Phase 2 studies), with a total of 839 subjects exposed to investigational agent (REG1, heparin or placebo) across the studies.
Three Phase 1 studies (REG1-CLIN101, REG1-CLIN102, and REG1-CLIN103) assessed the single- and multiple-dose safety, tolerability, pharmacokinetics, and pharmacodynamics of the anticoagulant (pegnivacogin) and anticoagulation controlling agent (anivamersen) in healthy volunteers and in subjects with coronary artery disease (CAD). Overall, the results for all three Phase 1 studies were consistent. Treatment with pegnivacogin resulted in a dose-dependent, stable increase in activated partial thromboplastin time, while treatment with the anticoagulant controlling agent (anivamersen) rapidly and durably reversed the measurable pharmacologic activity of the anticoagulant. There were no observable trends in safety parameters across the studies.
The first Phase 2 study (REG1-CLIN210) indicated that pegnivacogin can support the conduct of elective PCI, and that its effects can be reversed in this population with no overt bleeding or the development of ischemic events. The safety analysis from these studies indicated that the REG1 System did not present any significant risks. A second phase 2 study (REG1-CLIN220a) in subjects undergoing off-pump CABG was terminated after enrolling one patient.
A third Phase 2 study (REG1-CLIN211) was a randomized, partially-blinded study conducted to assess the safety and efficacy of using REG1 versus heparin (UFH or LMWH) in patients with acute coronary syndrome (ACS) undergoing early cardiac catheterization. In this study, REG1 subjects received open-label pegnivacogin 1mg/kg, followed by a blinded dose of anivamersen to achieve various levels of pegnivacogin reversal (25%, 50%, 75% or 100% reversal); the goals being to determine the appropriate anivamersen dose range for pegnivacogin reversal as assessed by impact on bleeding after cardiac catheterization, to confirm the PK/PD profile of pegnivacogin 1mg/kg in an ACS population, and to assess the overall effect of the REG1 system in subjects with acute coronary syndrome by assessing composite ischemic events undergoing early cardiac catheterization. A dose-range was established for anivamersen based upon bleeding rates and the 1 mg/kg dose of pegnivacogin was verified as causing near complete factor IX inhibition. The Data Safety and Monitoring Board stopped the lowest-dose anivamersen arm (25% reversal) early on in the trial per protocol because of a high bleeding rate. The three remaining arms (50%, 75% and 100%) demonstrated a rate of total ACUITY bleeding similar to heparin, with a stepwise numerical reduction in major bleeding with higher doses of the reversal agent (> 50% reversal). In the overall REG1 population there was a numerical reduction in the rate of ischemic events compared to heparin. Adverse events other than bleeding and ischemic events were rare and

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 21 of 105 CONFIDENTIAL
evenly distributed among the study groups with the exception of 3 severe allergic reactions that occurred clustered late in the study. See Section 4.5.5.2 for a discussion on these three severe allergic reactions.
Primary publications describing the results of each Phase 1 and 2A study have been published (Dyke et. al. Circulation, 2006; Chan et. al., Circulation, 2008; Chan et. al., JTH, 2008; Cohen et. al. Circulation, 2010). The design of the Phase 2b study has been published (Povsic, 2011) and the results were reported at the American College of Cardiology 2011 Scientific Sessions (Povsic). The PK/PD results from a subset of patients of the REG1-CLIN211 study has been accepted for publication in the European Heart Journal (Povsic).
1.5. Section 1 References Benedict CR, Ryan J, Wolitzky B, Ramos R, Gerlach M, Tijburg P, Stern D. Active site-blocked factor IXa prevents intravascular thrombus formation in the coronary vasculature without inhibiting extravascular coagulation in a canine thrombosis model. J Clin Invest 1991; 88:1760 –1765.
Butenas S, Orfeo T, Gissel MT, Brummel KE, Mann KG. The significance of circulating factor IXa in blood. J Biol Chem 2004; 279: 22875-22882.
Buyue Y, Whinna HC, Sheehan JP. The heparin-binding exosite of factor IXa is a critical regulator of plasma thrombin generation and venous thrombosis. Blood 2008; 112: 3234-3241.
Chan MY, Cohen MG, et. al., 2008 Phase 1b Randomized Study of Antidote-Controlled Modulation of Factor IXa Activity in Patients With Stable Coronary Artery Disease. Circulation. 2008; 117:2865-2874.
Chan MY, Rusconi CP, et. al. A randomized, repeat-dose, pharmacodynamic and safety study of an antidote-controlled factor IXa inhibitor. J Thromb Haemost. 2008; 6:789-796.
Choudhri TF, Hoh BL, Prestigiacomo CJ, Huang J, Kim LJ, Schmidt AM, Kisiel W, Connolly ES, Pinsky DJ. Targeted inhibition of intrinsic coagulation limits cerebral injury in stroke without increasing intracerebral hemorrhage. J Exp Med 1999; 190:91–99.
Cohen MG, Purdy DA, et. al., First clinical application of an actively reversible direct factor IXa inhibitor as an anticoagulation strategy in patients undergoing percutaneous coronary intervention. Circulation 2010; 122(6):614-22.
Dyke CK, Steinhubl SR, Kleiman NS, Cannon RO, Aberle LG, Lin M, et al. First-in-human experience of an antidote-controlled anticoagulant using RNA aptamer technology. A phase 1a pharmacodynamic evaluation of a drug-antidote pair for the controlled regulation of factor IXa activity. Circulation. 2006;114, 2490-2497.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 22 of 105 CONFIDENTIAL
Davie EW, Ratnoff OD. Waterfall sequence for intrinsic blood clotting. Science 1964;145:1310-1312.
Fay PJ, Koshibu K. The A2 subunit of factor VIIIa modulates the active site of factor IXa. J Biol Chem 1998; 273:19049-19054.
Feuerstein, G.Z., Toomey, J.R., Valocik, R., Koster, P., Patel, A. & Blackburn, M.N. An inhibitory anti-factor IX antibody effectively reduces thrombus formation in a rat model of venous thrombosis. Thromb Haemost 1999; 82:1443-1445.
Gitel S, Stephenson RC, Wessler S. In vitro and in vivo correlation of clotting protease activity: Effect of heparin. PNAS 1977; 74: 3028-3032.
Gray E, Tubbs J, Thomas S, Oates A, Bolsclair M, Kemball-Cook G, Barrowcliffe TW. Measurement of activated factor IX in factor IX concentrates: Correlation with in vivo thrombogenecity. Thrombosis and Haemostasis 1995; 73: 675-679.
Harrington RA, Becker RC, Ezekowitz M, Meade TW, O'Connor C M, Vorchheimer DA, and Guyatt G H. Antithrombotic therapy for coronary artery disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126:513S-548S.
Hoffman, M., Monroe, D. M., Oliver, J. A., and Roberts, H. R. Factors IXa and Xa play distinct roles in tissue factor-dependent initiation of coagulation. Blood 1995; 86: 1794-1801.
Kjalke M, Monroe DM, Hoffman M, Oliver JA, Ezban M, and Roberts HR. Active site-inactivated factors VIIa, Xa, and IXa inhibit individual steps in a cell-based model of tissue factor-initiated coagulation. Thromb Haemost 1998; 80:578-584.
MacFarlane RG. An enzyme cascade in the blood clotting mechanism, and its function as a biological amplifier. Nature 1964; 202:498-499.
Misenheimer TM, Buyue Y, Sheehan JP. The heparin-binding exosite is critical to allosteric activation of factor IXa in the intrinsic tenase complex: the role of arginine 165 and factor X. Biochemistry 2007; 46:7886-7895.
Monroe DM, Hoffman M, Roberts HR. Platelets and thrombin generation. Arterioscler Thromb Vasc Biol 2002; 22:1381-1389.
Monroe DM, Hoffman M, and Roberts HR. Transmission of a procoagulant signal from tissue factor-bearing cell to platelets. Blood Coagul Fibrinolysis 1996; 7:459-464.
Müller F, Mutch NJ, Schenk WA, Smith SA, Esterl L, Spronk HM, Schmidbauer S, Gahl, WA, Morissey JH, Renné T. Platelet polyphosphates are proinflammatory and procoagulant mediators in vivo. Cell 2009; 139: 1143-1156.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 23 of 105 CONFIDENTIAL
Plug I, Mauser-Bunschoten EP, Brocker-Vriends AH, van Amstel HK, van der Bom JG, van Diemen-Homan JE, Willemse J, Rosendaal FR. Bleeding in carriers of hemophilia. Blood 2006, 108: 52-6.
Popma JJ, Berger P, Ohman EM, Harrington RA, Grines C and Weitz JI. Antithrombotic therapy during percutaneous coronary intervention: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004; 126:576S-599S.
Povsic TJ, Cohen MG, Mehran R, et. al. A randomized, partially blinded, multicenter, active-controlled, dose-ranging study assessing the safety, efficacy, and pharmacodynamics of the REG1 anticoagulation system in patients with acute coronary syndromes: Design and rationale of the RADAR Phase IIb trial. AHJ 2011; 161:261-268.
Rand MD, Lock JB, van t Veer C, Gaffney DP, Mann KG. Blood clotting in minimally altered whole blood. Blood 1996; 88: 3432-3445.
Rusconi, C.P., Scardino, E., Layzer, J., Pitoc, G.A., Ortel, T.L., Monroe, D. and Sullenger, B. A.: RNA aptamers as reversible antagonists of coagulation factor IXa. Nature 2002; 419: 90-94.
Šrámek A, Kriek M, Rosendaal FR. Decreased mortality of ischaemic heart disease among carriers of haemophilia. Lancet 2003; 362: 351-4.
Toomey JR, Blackburn MN, Storer BL, Valocik RE, Koster PF, Feuerstein GZ. Comparing the antithrombotic efficacy of a humanized anti-factor IX(a) monoclonal antibody (SB 249417) to the low molecular weight heparin enoxaparin in a rat model of arterial thrombosis. Thromb Res 2000; 100:73-79.
Tuinenburg A, Mauser-Bunschoten EP, Verhaar MC, Biesma DH, Schutgens RE. Cardiovascular disease in patients with hemophilia. J Thromb Haemost 2009; 7:247–254.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 24 of 105 CONFIDENTIAL
2. PHYSICAL, CHEMICAL AND PHARMACEUTICAL PROPERTIES AND FORMULATION
2.1. Description of Drug Substance The REG1 Anticoagulation System consists of a highly potent oligonucleotide-based aptamer against coagulation Factor IXa and a control agent that can hybridize to the aptamer, via Watson-Crick base pairing, and neutralize its activity. The drug component (pegnivacogin) is a modified RNA aptamer, 31 nucleotides in length. The nucleic acid portion of the aptamer is conjugated to a 40-kilodalton PEG carrier to increase its blood half-life and permit administration of a single IV dose to maintain anticoagulation over an extended period of time. The control agent component (anivamersen) is a 2′-O-methyl RNA oligonucleotide, 15 nucleotides in length, which is complementary to a portion of the REG1 drug component. The structures of the aptamer and control agent are shown in Figure 2.
Figure 2: The REG1 Anticoagulation System
Figure 2: Pegnivacogin (drug component) is a modified RNA aptamer composed of 2’-fluoro residues (upper
case), 2'-O-methyl residues (lower case) and a single 2’ hydroxyl residue (underlined). Pegnivacogin is conjugated to a 40-KDa polyethylene glycol carrier (P) via a hexylamino linker (L).
Pegnivacogin and anivamersen are synthesized chemically and lyophilized. Pegnivacogin and anivamersen Injections are manufactured by reconstitution, dilution, and aseptic fill. Clinical trial materials are supplied as sterile solutions and must be stored at 2 – 8 °C in controlled temperature storage. Both the pegnivacogin Injection and anivamersen Injection

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 25 of 105 CONFIDENTIAL
solutions are suitable for administration, or can be diluted in Sterile Saline Injection (USP) prior to bolus IV administration.
2.1.1. Description and Composition of Pegnivacogin Injection
Pegnivacogin Injection is supplied as a sterile solution in a Type 1 clear glass vial sealed with a butyl rubber stopper and aluminum flip-off overseal. Each vial contains pegnivacogin substance, dibasic sodium phosphate heptahydrate, monobasic sodium phosphate monohydrate, sodium chloride, hydrochloric acid, sodium hydroxide, methionine, and water for injection.
Physical Appearance: Clear, colorless solution free of particulates
pH: 6.8 ± 0.5
Volume in container: ≥ 5.0 mL
Stability: Current data indicate that pegnivacogin Injection at 24 mg/mL is stable for up to 24 months when stored at 2 – 8 °C
Manufactured by: Althea Technologies Inc, San Diego, CA, USA
Storage: Vials of pegnivacogin Injection must be stored at 2°-8°C
Retest: 2 years
2.1.2. Description and Composition of Anivamersen Injection
Anivamersen Injection is supplied as a sterile solution in a Type 1 clear glass vial sealed with a butyl rubber stopper and aluminum flip-off overseal. Each vial contains anivamersen substance, dibasic sodium phosphate heptahydrate, monobasic sodium phosphate monohydrate, sodium chloride, hydrochloric acid, sodium hydroxide, and water for injection.
Physical Appearance: Clear, colorless solution free of particulates
pH: 7.4 ± 1.0
Volume in container: ≥ 2.5 mL
Stability: Current data indicate that anivamersen Injection at 48 mg/mL is stable for up to36 months when stored at 2 – 8 °C
Manufactured by: Althea Technologies Inc, San Diego, CA, USA
Storage: Vials of the anivamersen Injection must be stored at 2-8 °C
Retest: 3 years

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 26 of 105 CONFIDENTIAL
2.2. Storage and Handling Pegnivacogin Injection and Anivamersen Injection sterile solutions must be stored at 2 – 8 °C in controlled temperature storage. Stability studies are ongoing at this time and the clinical study site will be notified as stability is extended for the study drug products.
2.3. Preparation of Drug Product Injection
2.3.1. Pegnivacogin Drug Product Injection
Each vial of pegnivacogin sterile solution contains 5.0 mL of deliverable volume. pegnivacogin injection may be used as supplied, but may also be diluted (if necessary) in Sterile Saline Injection (USP) to a target concentration that will deliver the desired dose.
2.3.2. Anivamersen Drug Product Injection
Each vial of anivamersen sterile solution contains 2.5 mL of deliverable volume. Anivamersen injection may be used as supplied, but may also be diluted (if necessary) in Sterile Saline Injection (USP) to a target concentration that will deliver the desired dose.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 27 of 105 CONFIDENTIAL
3. NONCLINICAL STUDIES
3.1. Introduction The pharmacologic activity of the REG1 Anticoagulation System and its individual drug and control agent components was demonstrated in vitro and in clinically relevant animal models. The results from these studies provide the impetus for the clinical development of the REG1 Anticoagulation System. The anticoagulant activity of the anti-FIXa aptamer was evaluated in various pig models, including systemic anticoagulant studies (Rusconi et al., 2004) and cardiopulmonary bypass studies with and without coronary artery bypass grafting, and in safety pharmacology and toxicity studies in cynomolgus monkeys. The anti-thrombotic activity of the anti-FIXa aptamer was demonstrated in a mouse arterial damage model (Rusconi et al., 2004). The drug neutralization activity of the control agent was demonstrated in vitro in human plasma (Rusconi et al., 2002), in various pig models, in mouse models of surgical trauma (i.e., tail transection of highly anticoagulated animals) (Rusconi et al., 2004) and in safety pharmacology and toxicity studies in cynomolgus monkeys.
Characterization of the pharmacokinetics of the REG1 Anticoagulation System required a bioanalytical strategy that relied on novel methodology to quantify the levels of pegnivacogin, anivamersen and the pegnivacogin/anivamersen complex in plasma samples. These methods were applied to samples collected from the in vivo toxicity studies, which permitted determination of the pharmacokinetics of all three molecular entities under conditions of single and repeated dosing in monkeys and mice.
A thorough safety assessment of the REG1 Anticoagulation System and its individual pegnivacogin and anivamersen components was conducted. The original toxicity studies that supported the IND application were performed in monkeys and mice under dosing conditions that simulated the intended use of the product in initial clinical trials (i.e., with sequential administration of aptamer followed 3 hours later by control agent administration). Small-to- large clinical multiples of each component were tested in the same dose ratio as intended for initial clinical use, and for both species, the effects of the pegnivacogin and anivamersen were tested separately. Specialized endpoints were included in the toxicity studies to assess pharmacodynamic responses, exposure to REG1 components, and the class effects of oligonucleotides. The core toxicity studies were supplemented with safety pharmacology evaluation in monkeys (using radiotelemetry), a battery of genetic toxicity assays, and a blood compatibility study.
Subsequent to the initial IND submission, additional studies were conducted, including twice-daily intravenous administration of pegnivacogin for 14 days in monkeys, subcutaneous administration of pegnivacogin for 14 days in monkeys and 28 days in rats and dogs, and an additional intravenous safety pharmacology study of pegnivacogin in monkeys to further assess the safety of pegnivacogin and the REG1 System. Among the various endpoints evaluated in these studies include some that reflect on the absence of immunostimulatory, immunotoxicity and immunogenicity. Lastly, two in vitro studies were

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 28 of 105 CONFIDENTIAL
conducted to assess potential interactions of pegnivacogin and REG1 with the hepatic cytochrome P450 system, to assess possible drug interactions.
3.2. Nonclinical Pharmacology
3.2.1. Integrated Discussion of Nonclinical Pharmacology Data
The pharmacology of the REG1 Anticoagulation System, and its individual components was evaluated in a variety of animal models in several animal species. Studies were designed to test the efficacy of pegnivacogin in preventing clot formation induced by a number of clinically relevant stimuli. Specifically, these studies were designed to characterize the dose-response relationship for inhibition of Factor IXa by pegnivacogin and the safety and effectiveness of anivamersen in negating the activity of pegnivacogin. In addition, this program was designed to verify the pharmacologic potency of the REG1 Anticoagulation System in the key toxicology species (see Table 3 for a complete list of studies). From these studies, the following properties of the REG1 Anticoagulation System and its individual components have been documented:
• The anti-FIXa aptamer exhibits pharmacologic effects in mice, as demonstrated by its ability to prevent tissue factor-induced occlusive clot formation in arterial damage models and its ability to induce bleeding at supratherapeutic doses.
• The control agent for the anti-FIXa aptamer demonstrated effective control of the aptamer’s pharmacologic activity by preventing blood loss induced by supratherapeutic doses of the anti-FIXa aptamer in surgical challenge studies in the mouse.
• Cardiopulmonary bypass studies in the pig, with and without coronary artery bypass grafting, have demonstrated the anticoagulant efficacy of pegnivacogin upon insult of the blood by contact with foreign materials, mechanical damage to blood cells via a CPB pump, and surgical trauma.
• The tolerability of complete reversal of pegnivacogin activity by anivamersen administration following coronary revascularization has been demonstrated by post-graft implant angiographic analysis as well as necropsy and histopathology in the pig coronary artery bypass graft model.
• The anticoagulant effect of pegnivacogin has been demonstrated in toxicity studies in rats and dogs.
• The anticoagulant effect of pegnivacogin and reversal of its activity by anivamersen have been demonstrated in safety pharmacology and toxicity (Section 3.4) studies in monkeys, and these studies have shown that the effects of pegnivacogin on aPTT and ACT prolongation are very similar between monkeys and humans.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 29 of 105 CONFIDENTIAL
In summary, nonclinical pharmacology studies have demonstrated the intended anticoagulant and anticoagulant reversal activities of the REG1 Anticoagulation System in mice, rats, dogs and monkeys, the key toxicology species. Evidence for efficacy in clinically relevant models employing varied insults to induce clot formation has been demonstrated for pegnivacogin in mice and pigs, providing further validation of FIXa as a target for the development of anticoagulant agents, and thus serving as an impetus for the clinical development of pegnivacogin. Evidence for efficacy and safety of rapid reversal of anticoagulant activity using the control agent has been demonstrated in mouse surgical challenge models as well as pig models of coronary revascularization. Finally, evaluation of the pharmacodynamic activity of pegnivacogin and anivamersen in monkeys has demonstrated that the activity of both components can be readily monitored by standard clinical lab tests such as the aPTT, as well as by point-of-care coagulation tests such as the ACT.
3.3. Pharmacokinetics (Toxicokinetics)
3.3.1. Integrated Discussion of Toxicokinetic Data
Regado developed methodology to enable determination of plasma levels of each of the three molecular entities resulting from administration of the REG1 Anticoagulation System (pegnivacogin, anivamersen, and the pegnivacogin/anivamersen complex). Plasma pegnivacogin and anivamersen levels are determined using a sandwich-type hybridization assay with an enzyme-linked immunoassay (ELISA) for detection. In each case, analyte-specific hybridization capture and detection probes enable specific measurement of the intact species. A direct method for measurement of the concentration of the pegnivacogin/anivamersen complex has proven challenging to develop. Therefore, in lieu of a direct measurement method, the level of pegnivacogin/anivamersen complex is calculated by measuring total pegnivacogin (i.e., pegnivacogin not bound to anivamersen + pegnivacogin bound to Anivamersen) and free pegnivacogin, and subtracting free pegnivacogin from total pegnivacogin to arrive at the level of pegnivacogin/anivamersen complex.
These methods were applied to analysis of samples collected from the various toxicity studies, listed in Table 3. For all studies, the toxicokinetic results were similar with respect to documenting the following properties of the REG1 anticoagulation system:
• The plasma concentrations of pegnivacogin following intravenous injection of single doses are dose-proportional over a broad dose range, with a modest degree of inter-animal variation. No gender differences were apparent.
• The clearance of pegnivacogin from plasma following bolus intravenous injection is relatively slow (i.e., the estimated half-life was at least 12 hours in monkeys and ~8 hours in mice). This slow clearance was expected based on the PEGylated structure of pegnivacogin and is consistent with literature reports on the pharmacokinetics of other PEGylated oligonucleotides. The slow clearance of pegnivacogin, in combination with its high Factor IXa inhibitory potency, provides stable anticoagulation over an extended period following dosing.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 30 of 105 CONFIDENTIAL
• Intravenous injection of anivamersen alone yields low levels in plasma when measured 10-15 minutes after dosing. Anivamersen levels measured at these early times were orders of magnitude lower than those of pegnivacogin (i.e., in those groups that had received pegnivacogin alone), despite the fact that the anivamersen dose levels were twice as high. Collectively, the data indicate that anivamersen has a very short half-life in plasma. No accumulation of anivamersen in plasma occurred when it was administered at a relatively high dose level (30 mg/kg) to monkeys every other day for 7 doses (14 days).
• Administration of anivamersen 3 hours after pegnivacogin (i.e., the complete REG1 Anticoagulation System) results in an abrupt reduction in free pegnivacogin plasma concentration. Within minutes following anivamersen administration, pegnivacogin levels were reduced to below or slightly above the limits of quantification, indicating complete binding of the circulating aptamer by anivamersen. This elimination of free pegnivacogin by anivamersen binding was persistent, and there no evidence of significant reversal of the complex formation based on the absence of all but trace levels of free pegnivacogin for at least 21 hours after anivamersen dosing. As was seen with administration of anivamersen alone, there were very low levels of free anivamersen under these conditions. The binding of pegnivacogin by anivamersen was associated with virtually complete neutralization of pegnivacogin activity (see Section 3.2), consistent with the intended performance of the REG1 Anticoagulation System.
• Concurrent with elimination of free pegnivacogin, the pegnivacogin/anivamersen complex was detected in plasma at levels consistent with the complete binding of pegnivacogin by anivamersen. The complex was eliminated from plasma at a rate slightly faster than that of the free pegnivacogin (i.e., by comparison to the rate of pegnivacogin clearance in groups treated with pegnivacogin only), but at a much slower rate than free anivamersen, as would be expected from the presence of the PEG moiety within the complex (derived from pegnivacogin). Extensive elimination of the pegnivacogin/anivamersen complex from plasma was evident within 21 hours following anivamersen dosing. With repeated administration of pegnivacogin and anivamersen to monkeys every day for two weeks, there was no accumulation of the complex in the blood or of free pegnivacogin, and no change in pegnivacogin pharmacokinetics (i.e., during the period prior to anivamersen dosing).
• When pegnivacogin was administered to monkeys by IV injection twice daily for 14 days (doses approximately 12 hours apart), plasma levels of pegnivacogin accumulated in a manner consistent with the long (12 hours or greater) half-life of pegnivacogin in monkeys. Consequently, there were substantial levels of pegnivacogin in plasma prior to dosing on Day 14. However, when anivamersen was administered 3 hours after the dose of pegnivacogin, there was no accumulation of pegnivacogin, reflecting the complete binding (and inactivation) of pegnivacogin by anivamersen. In addition, while an appreciable level of

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 31 of 105 CONFIDENTIAL
unbound anivamersen was present following the anivamersen dose, this oligonucleotide was rapidly cleared and/or metabolized, consistent with the intended kinetics of this component of the REG1 Anticoagulation System.
• Following SC injection in three different species, pegnivacogin was slowly taken up into the systemic circulation, and the plasma levels were typically maximal at 24 hours post-injection, and, for the higher dose levels, as late as 48 hours after dosing. Although the preponderance of the absorption occurred within the first 6-8 hours after injection, plasma levels continued to rise thereafter, indicating ongoing further absorption. The long absorption phase pegnivacogin following SC injection is attributable to the large size of the PEGylated aptamer (~40 KDa), which dictates slow migration into or out of blood.
In summary, the REG1 Anticoagulation System performed as expected in with respect to: 1) generally dose-proportional plasma concentrations of pegnivacogin following bolus IV injection that were maintained over an extended period (at least six hours) following dosing; 2) rapid and complete elimination of free pegnivacogin (and associated cessation of anticoagulation activity) following injection of anivamersen, resulting from the hybridization of these two oligonucleotides to form a stable complex that is steadily cleared from the blood compartment; 3) minimal exposure to free anivamersen following IV dosing, owing to the rapid clearance of unbound anivamersen from plasma; 4) continuous plasma levels of pegnivacogin when administered by IV injection every other day (and some accumulation in plasma with twice-daily IV dosing) and 5) a long absorption phase for pegnivacogin following subcutaneous administration with accumulation following every other day or twice weekly administration, and prolonged exposure following as compared to intravenous administration.
3.4. Toxicology
3.4.1. Rationale for Types of Studies, Species Selection and Study Design Elements
The general rationale for the types of studies conducted with the REG1 Anticoagulation System, the selection of species and the primary design considerations are presented herein. An integrated discussion of the overall study findings is presented in Section 3.4.6.
3.4.2. Types of Studies
As per international regulatory guidance, the primary nonclinical toxicity studies were conducted in two species: mice and cynomolgus monkeys. Also, a comprehensive safety pharmacology study was conducted in cynomolgus monkeys. These core safety studies were intended to support initial single-dose clinical trials and were supplemented with an in vitro blood compatibility study and a battery of three genetic toxicity assays. Since the initial clinical trial in normal subjects (conducted under U.S. IND 63,275) included groups that were treated only with pegnivacogin or anivamersen (to assess the safety of these components when given alone), dedicated groups were included in the toxicity studies that were similarly treated with the individual components.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 32 of 105 CONFIDENTIAL
Although the initial clinical trials were limited to single-dose treatment, as is the case for most intended clinical applications of the REG1 Anticoagulation System, the supporting toxicity studies included groups that were given repeated doses. The dosing schedule utilized for those groups (every other day IV injection) was not selected to mimic any intended clinical regimen, but rather was based on the known or expected pharmacokinetics of pegnivacogin, i.e., the long circulation half-life (see Section 3.3). A subsequent repeat-dose (14-day) IV study in monkeys (study No. REG1-TOX006) was conducted to further comply with regulatory expectations to assess repeat-dose toxicity for the REG1 System (i.e., administration of pegnivacogin, followed by anivamersen), and to support possible repeated dosing with pegnivacogin for clinical applications requiring sustained anticoagulation. For the latter purpose, groups were treated with pegnivacogin by twice-daily IV injection (every 12 hours), to mimic the most aggressive possible clinical dosing scenario.
It is important to note that repeated dosing with the highly potent pegnivacogin aptamer at large clinical-multiple doses renders the animals complete Factor IXa knockouts, such that the study animals must be carefully managed with respect to controlling stasis at sites of venipuncture and avoiding tissue trauma that leads to excessive local hemorrhage. As is evident from the study summaries presented herein, technical difficulties were encountered due to excessive and prolonged anticoagulation that led to loss of some animals at high dose levels. This only occurred in groups that received pegnivacogin alone without follow-on administration of anivamersen. In some studies, bleeding problems at venipuncture sites were controlled with the use of surgically implanted venous ports to enable blood sample collection, but there was still a tendency for local bruising due to handling in the groups that received high doses of pegnivacogin.
Repeat dose studies employing subcutaneous administration of pegnivacogin using an every other day dosing schedule in monkeys (14 day; REG1-TOX007), or twice weekly dosing for 28 days in rats (TOX-RB006-10-001) and dogs (TOX-RB006-10-002) were conducted to support clinical studies evaluating single and repeat dose subcutaneous administration of pegnivacogin.
An additional comprehensive safety pharmacology study of pegnivacogin in cynomolgus monkeys was conducted in response to the severe allergic SAEs in REG1-CLIN211 to further assess the impact of intact or degraded pegnivacogin on a broad array of immune-related biomarkers, including a full complement panel, histamine, and infusion related cytokines.
3.4.3. Selection of Species
The four species that were chosen for the primary nonclinical toxicity studies of the REG1 anticoagulation system are monkeys (cynomolgus), dogs, rats, and mice (CD-1 strain). Cynomolgus monkeys were chosen, in part, because of the extensive historical experience in assessing oligonucleotide safety in this species. Rats and dogs were employed in 28-day subcutaneous repeat dose studies because their larger size allowed for more intense sample collection as compared to monkeys and mice. However, the primary basis for selecting these species for REG1 toxicity testing is that pegnivacogin has been shown to be pharmacologically active in all four of these species. The Factor IXa inhibitory activity of

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 33 of 105 CONFIDENTIAL
pegnivacogin and the neutralizing action of anivamersen were well characterized in mice, as described in Section 3.2
3.4.4. Study Design Elements
. Similarly, the performance of both pegnivacogin and anivamersen in monkeys, rats and dogs was clearly demonstrated in the toxicity studies conducted with the REG1 Anticoagulation System.
The basic design of the initial mouse and monkey toxicity studies, as well as the safety pharmacology study in monkeys, included separate groups that received pegnivacogin alone (or the PBS control article) at time zero, followed by anivamersen (or PBS) three hours after pegnivacogin (or PBS). This required three separate groups (pegnivacogin alone, anivamersen alone, or pegnivacogin followed by anivamersen [REG1 Anticoagulation System]) for each dose level tested. This design element, in combination with the above-described regulatory requirement to address repeat-dose toxicity in support of single-dose clinical trials, translated into very large studies (e.g., 13 treatment groups in the original monkey toxicity study); hence, the group sizes were the minimum recommended by regulatory guidelines.
The staggered dosing with pegnivacogin and anivamersen (or control articles) 3 hours apart was intended to simulate the regimen proposed for initial clinical trials, and the ratio between the pegnivacogin and anivamersen doses was identical to that intended for initial clinical trials. In all intravenous toxicity studies, the doses of both pegnivacogin and anivamersen were given by bolus (slow-push) injection.
Studies supporting subcutaneous administration were primarily focused on evaluating the toxicity of prolonged exposure to pegnivacogin, and therefore utilized repeat dosing schedules of pegnivacogin alone.
3.4.5. Extrapolation of Doses Across Species
For drugs with a site of action in the blood compartment and for which nearly all manifestation of toxicity stem from interaction with a blood protein, it is customary to compare doses across species on a body weight-relative basis (mg/kg), hence conventional allometric scaling based on body surface area (BSA) was not applied. In addition, for the general class of oligonucleotides, there is a regulatory guidance suggesting that BSA-based allometric scaling is not appropriate (http://www.fda.gov/cber/gdlns/dose.pdf). This exception for oligonucleotides is based on the published work of Geary et al. (see Geary et al., 1997). In particular, the FDA’s guidance document mentions that the blood-level-related affects of oligonucleotides are those for which interspecies extrapolation on a mg/kg body weight basis is valid. Since the anticoagulant component of REG1 exerts its effects by direct interaction with a blood protein (Factor IXa), this mechanism of action falls clearly within the scope of the conditions cited in the FDA guidance document. Further, since all of the effects of the REG1 Anticoagulation System documented in the nonclinical toxicity studies were attributable to the exaggerated pharmacologic action of pegnivacogin, it is considered most valid to compare doses across species (i.e., from animals to humans) on the basis of the mg/kg dose levels.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 34 of 105 CONFIDENTIAL
3.4.6. Integrated Discussion of the Nonclinical Toxicity Study Findings
The initial toxicity studies conducted with the REG1 Anticoagulation System were 1) the safety pharmacology study in monkeys (REG1-TOX001); 2) the single/repeat-dose study in monkeys (REG1-TOX003); and 3) the 14-day repeat-dose study in mice (REG1-TOX002). In all of these studies, the pegnivacogin and anivamersen were tested separately and in combination by dosing in a staggered manner, as intended for clinical trials. It is Regado’s view that the results obtained with a single dose IV administration of the REG1 Anticoagulation System are the most relevant to predicting the safety of the product for one-time IV use in patients. For completeness, however, groups were included in the initial mouse and monkey studies (REG1-TOX002 and –TOX003) that were dosed intravenously with the components or the System (REG1) every other day over a 2-week period. Subsequently, an additional study was conducted in monkeys with twice daily IV dosing of REG1 daily for 14 days (REG1-TOX006) to strengthen the nonclinical safety database in support of single-dose applications, and to extend the support for possible repeated dosing with pegnivacogin. These core studies were supplemented with a battery of three genetic toxicity assays, an in vitro blood compatibility study, and two in vitro studies to characterize potential interactions with the hepatic cytochrome P450 drug metabolizing system. Single and repeat-dose subcutaneous administration of pegnivacogin is supported by the 14-day repeat-dose study in monkeys (REG1-TOX007) and the 28-day repeat-dose studies in rats (TOX-006-10-001) and dogs (TOX-006-10-001). Finally, an additional safety pharmacology study of pegnivacogin was conducted in monkeys to further assess the effects of intact and degraded pegnivacogin on immune-related biomarkers.
3.4.7. Monkey Safety Pharmacology Studies
The first toxicity study that was conducted with the REG1 Anticoagulation System was the safety pharmacology study in monkeys (REG1-TOX001). This study fulfilled several objectives, including serving as a single-dose range-finding study, as well as an investigation of potential adverse effects on cardiovascular, respiratory and neurologic function. The animals used in this study were equipped with radiotelemetry devices for continuous monitoring of cardiovascular parameters and body temperature, and they were also surgically prepared with an arterial access port (located subcutaneously) for which the catheter portion was routed subcutaneously and inserted in a femoral artery. This configuration of the dosing procedure most closely mimics the intended clinical procedure for the planned patient trials with the REG1 Anticoagulation System. It should be noted that there was minimal handling of the animals in this study, relative to other monkey toxicity studies, as they were dosed only on one occasion, and blood sampling was sparse, in keeping with the objective of monitoring cardiovascular parameters via telemetry in undisturbed animals.
Under these conditions, the individual components pegnivacogin and Anivamersen and the REG1 Anticoagulation System were very well tolerated by monkeys in REG1-TOX001. At doses of pegnivacogin alone up to 30 mg/kg or of anivamersen alone up to 60 mg/kg, or of the combination given 3 hours apart at up to 30/60 mg/kg, there were no effects on the various cardiovascular parameters (blood pressure heart rate, and electrocardiographic activity), body temperature, respiratory function parameters (blood gases and respiration rate)

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 35 of 105 CONFIDENTIAL
or neurologic function (assessed by conducting a detailed neurologic examination). There were also no clinical signs, changes in body weight or food consumption, or any indications of an adverse effect on the animals. Hematology and clinical chemistry parameters were unaffected, and there was no elevation in the plasma levels of the complement split product Bb, which is a marker for alternative complement pathway activation that has been shown to be induced by phosphorothioate oligonucleotides. The absence of any complement activation was expected, as neither pegnivacogin nor anivamersen contain any phosphorothioate residues. There were also no histopathologic changes in key organs for animals that were given a single dose of 30 mg/kg pegnivacogin.
The only effect observed in the REG1-TOX001 monkey safety pharmacology study was the expected prolongation of activated partial thromboplastin time (aPTT) and activated clotting time (ACT), reflecting the pharmacologic activity of the pegnivacogin aptamer. Prothrombin time was unaffected, consistent with the Factor IXa specificity of pegnivacogin. The prolongation of aPTT by pegnivacogin was dose-dependent over the range of doses tested (5 to 30 mg/kg), and this dose relationship for pharmacodynamic activity has been confirmed in several other monkey studies. Anticoagulation occurs very quickly, and aPTT prolongation was maximal by the first sampling time point following pegnivacogin dosing (15 minutes in this study). aPTT was not appreciably diminished over a 3-hour period following pegnivacogin administration, and aPTT very gradually returned towards baseline values in the animals that received pegnivacogin only, reflecting the long circulation half-life (at least 12 hours). In contrast, administration of anivamersen 3 hours after pegnivacogin abruptly reduced aPTT to the baseline range, and mean aPTT remained in the normal range through the last sampling time point (up to 5 days after dosing). A similar pattern was observed for ACT following dosing with pegnivacogin and neutralization with anivamersen. The absence of free pegnivacogin in circulation following anivamersen administration was confirmed by the toxicokinetic analysis, which showed little or no free pegnivacogin after dosing with anivamersen (see Section 3.3).
A second monkey safety pharmacology study, TOX-RB006-10-003 was conducted in response to the severe allergicSAEs in REG1-CLIN211. This study assessed the effects of 20 mg/kg doses of intact or degraded pegnivacogin alone, administered as an intravenous bolus injection over 1 minute, on the same cardiovascular, body temperature, respiratory, and neurologic parameters as REG1-TOX001. As compared to the REG1-TOX001 study, TOX-RB006-10-003 expanded the analysis of complement factors beyond Bb to include classical pathway markers C3a, C4a and total hemolytic complement activity (CH50). Additionally, this study also included analysis of plasma histamine levels, and the infusion related cytokines IFNγ, TNFα, MIP-1α., MCP-1 and IL-6 pre-dose and at selected timepoints post pegnivacogin administration. As in the REG1-TOX001 study, pegnivacogin was well tolerated, with no findings in TOX-RB006-10-003 beyond the expected elevation of the aPTT due to the anticoagulant activity of pegnivacogin.
At the lowest dose level tested in the REG1-TOX001 safety pharmacology study, plasma pegnivacogin concentration remained well above the range shown to completely inhibit FIXa for at least 6 hours and was still in the range associated with extensive FIXa inhibition at 24 hours after injection. Therefore, the monkeys were rendered complete or nearly complete

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 36 of 105 CONFIDENTIAL
FIXa knockouts over an extended period, particularly in the group that received pegnivacogin without anivamersen neutralization. Therefore, the absence of any adverse effects in either safety pharmacology study under these conditions strongly attests to the safety of the REG1 System. Furthermore, the absence of effects of intact or degraded pegnivacogin on any complement biomarker, plasma histamine level or measured cytokine level, when administered at doses 20-30 fold higher than the intended clinical dose, strongly attests to the low potential for pegnivacogin or degradants of pegnivacogin to activate the innate immune system or elicit an immunostimulatory effect in general.
3.4.8. Initial Single- and Repeat-dose Intravenous Toxicity Study in Monkeys
Subsequently to the REG1-TOX001 safety pharmacology study, a comprehensive toxicity study (REG1-TOX003) was conducted in monkeys, with 13 different treatment groups (both single and repeated dosing of pegnivacogin, anivamersen and the combination), 3 sacrifice times, and a multitude of pharmacodynamic and safety endpoints. The study was conducted in a staggered manner, with the single-dose groups initiated prior to the repeat-dosing groups. On the first day of dosing for the single-dose groups, several animals that received high doses (5 or 45 mg/kg) of pegnivacogin were sacrificed due to bleeding complications. These events were attributed to a failure to achieve clotting at sites of venipuncture in a major vessel (femoral vein) for animals that had been rendered virtual FIXa knockouts. The importance of the protection against such catastrophic bleeding events afforded by the use of vascular access ports for dosing and blood sampling, as was employed in the safety pharmacology study, was not fully appreciated at the time of initiation of the REG1-TOX003 study. Also, the frequency of blood sampling and intensity of animal handling were much greater in this study. The hemorrhages occurred within hours after dosing, during periods where the animals were free to move about their cage, which apparently disrupted the temporary clot formation. For the remainder of the study, the blood sampling sites were restricted to smaller vessels (typically the saphenous veins), and special care was taken to achieve complete stasis at venipuncture sites. With these precautions, there were no further occurrences of uncontrolled bleeding. In fact, the group that received REG1 at a dose level of 15/30 mg/kg over 13 days (every other day for 7 doses) had no bleeding complications at venipuncture sites nor any histologic evidence of an abnormal amount of hemorrhage at these sites. Thus, the moribundity that occurred in this study, while clearly a consequence of the exaggerated pharmacologic action of pegnivacogin, was not considered clinically relevant. In addition, the doses at which these events occurred are substantial clinical multiples.
Apart from the above-described hemorrhage-related moribundity, pegnivacogin and Anivamersen were well tolerated by the monkeys. All effects observed in the single- and repeat-dose groups were related to the anticoagulant action of pegnivacogin, and no toxicity from anivamersen was observed. For all treatment groups, there were no effects on body weight, food consumption, electrocardiograms, ophthalmic examinations, plasma chemistry, and organ weights. There was also no effect of either REG1 component on platelet aggregation. Changes in hematology parameters were limited to decreases in the indicators of circulating red blood cell mass in those animals with confirmed hemorrhage. Coagulation parameters were affected in a predictable manner, as observed in the safety pharmacology study. Specifically, aPTT and ACT were prolonged by pegnivacogin in a dose-dependent

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 37 of 105 CONFIDENTIAL
manner, and this effect dissipated slowly in animals that were not given anivamersen, consistent with the relatively long plasma half-life of pegnivacogin. However, when anivamersen was administered to animals that had received pegnivacogin three hours prior, the anticoagulant activity of pegnivacogin was rapidly and completely negated, with no reversal of pegnivacogin inactivation over an extended period.
From the anatomic pathology evaluation, there were two key observations: 1) confirmation of the exacerbation of hemorrhage at sites of venipuncture; and 2) a possible increase in the incidence and severity of hemorrhagic lesions in the heart. Both types of findings were clearly attributable to pegnivacogin only in the groups that received single doses of 5 or 45 mg/kg, and primarily in the groups that were not subsequently treated with anivamersen. Areas of hemorrhage in the heart were observed microscopically as a background finding in this study (in fact, one of the most pronounced lesions was seen in a control animal), but there was a suggestive increased incidence of this background finding in groups that received 5 or 45 mg/kg pegnivacogin. These lesions were not considered to be highly adverse, especially because their severity did not exceed that observed in a control animal. It was hypothesized that the background hemorrhagic findings in the heart were attributable to the vigorous activity of this organ (especially in monkeys that are repeatedly subject to physical restraint and other stresses associated with study procedures), and that the anticoagulant activity of pegnivacogin simply exacerbated this condition at high dose levels. Importantly, there were no treatment-related cardiac hemorrhages or exacerbation of hemorrhage at venipuncture sites (or any other treatment-related findings) in animals that received repeated injections (7 times over two weeks) of a high dose level (15/30 mg/kg) of the pegnivacogin/anivamersen combination. This regimen represents a substantial exaggeration of the clinical use of this product, with respect to both the dose and frequency of administration. Hence the absence of adverse effects under these conditions strongly attests to the safety of the REG1 Anticoagulation System.
3.4.9. 14-Day Intravenous Study in Mice
The repeat-dose mouse study (REG1-TOX002) was also a very comprehensive study, with 10 groups of animals receiving various doses of pegnivacogin alone, anivamersen alone, or the combination (separated by 3 hours). This was a technically difficult study to perform, mainly with respect to the twice-daily injection of test material or PBS control article into the tail veins of all study animals for 14 days. However, the toxicokinetic data demonstrated a very clear dose-dependent exposure of the animals; in terms of the plasma concentrations of pegnivacogin and anivamersen (see Section 3.3). Despite the repeated administration of large clinical-multiple doses (up to 22.5 mg/kg/day of pegnivacogin and 45 mg/kg/day of anivamersen), no adverse effects were observed on any of the parameters in this study, including a complete battery of clinical and anatomic pathology evaluations. The reason why there were no fatal bleeding episodes in the mice (as seen in the single/repeat-dose monkey study) is probably attributable to the very small lumen of the tail veins used for injection and the fact that the gauge of the needles used for injection were small by comparison to those used for collecting blood samples from the monkeys (thus resulting in smaller venipuncture sites). In addition, there was no repetitive blood sampling in this study.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 38 of 105 CONFIDENTIAL
No prolongation of aPTT was observed in the mice that were treated with pegnivacogin. Pegnivacogin has been shown to be active in mice, but the maximum prolongation of the aPTT in response to complete FIXa inhibition in this species is only around 1.5 to 2-fold (Rusconi et al., 2004). This magnitude of change was likely obscured by the very large variation in aPTT that anomalously occurred in this study. In addition, the blood samples for assessment of these parameters were collected at necropsy on the day following the last dose (i.e., approximately 24 hours or more after the last dose). Considering the approximately 8-hour half-life of pegnivacogin, blood concentrations would have substantially diminished over the period between the last dose and sample collection.
3.4.10. Two-week Intravenous Toxicity Study in Monkeys
An additional repeat-dose (2-week) intravenous study was conducted in cynomolgus monkeys (REG1-TOX006) to support single-dose applications of the REG1 Anticoagulation System (i.e., to fulfill regulatory requirements) and possible repeated clinical dosing with pegnivacogin or the REG1 System. The effects observed in this study were quite similar to those reported for the previous REG1-TOX003 study. All effects were related to the pharmacologic activity of pegnivacogin. However, the dosing regimen was more intensive than that the every-other-day schedule utilized in REG1-TOX003, i.e., doses of pegnivacogin were given twice daily (12 hours apart) at three different dose levels, and the REG1 System (pegnivacogin, followed 3 hours later by anivamersen) was administered daily for 14 consecutive days. As discussed in Section 3.3, the blood half-life of pegnivacogin is at least 12 hours, such that when administered at approximate 12-hour intervals, accumulation of pegnivacogin in circulation is inevitable. Therefore, relatively low doses would be expected to render the animals completely deficient in Factor IXa, with the attendant susceptibility to bleeding events. In this study, doses were injected and blood samples were collected via a surgically-implanted vascular access port to minimize hemorrhage at venipuncture sites. Nevertheless, several of the animals that received the highest dose level of pegnivacogin (5 mg/kg twice daily, without anivamersen neutralization) developed complications, including excessive bruising incurred during restraint for study procedures and other possible sequelae that apparently stemmed from excessive and prolonged anticoagulation, which led to their early termination. Microscopic examination of tissues confirmed the presence of hemorrhage and edema in multiple organs of the animals terminated early. Reduction of the dose level to 2 mg/kg (twice daily) ameliorated the problems in remaining high-dose animals. In addition, there were fewer and less severe hemorrhagic lesions in the animals that received a higher dose level of pegnivacogin (10 mg/kg/day) but were neutralized 3 hours after each pegnivacogin by injection of 20 mg/kg anivamersen, indicating that the shorter period (3 hours per day) of extreme anticoagulation resulted in fewer bleeding complications.
Measurement of aPTT also confirmed the cumulative anticoagulation in the monkeys that were dosed twice daily with pegnivacogin and once again demonstrated the complete and persistent inactivation of pegnivacogin upon anivamersen injection. The hemorrhagic lesions that were observed microscopically in high-dose animals were also noted with lesser incidence and severity in lower dose groups, but at the lowest pegnivacogin dose level (0.25 mg/kg twice daily), histologic changes were limited to two animals and consisted of mild edema and/or hemorrhage in skeletal muscle or skin (presumably reflecting handling trauma

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 39 of 105 CONFIDENTIAL
that was exacerbated by the anticoagulation), with no hemorrhagic lesions in any internal organs. Therefore, all manifestations of toxicity were related to pegnivacogin pharmacologic activity, and there were no findings that would raise concern about repeated twice-daily intravenous dosing in a lower clinical range (e.g., 0.25 mg/kg and lower) or at somewhat higher doses under conditions where bleeding complications were well controlled.
3.4.11. Two and Four-week Subcutaneous Toxicity Studies of Pegnivacogin
The 4-week SC toxicity studies in rats and dogs and the 14-day SC toxicity study in monkeys are considered the pivotal supporting general toxicity studies for the subcutaneous pegnivacogin program. The design of these studies adhered to ICH guidance with respect to the group sizes, number of dose levels, parameters evaluated and the inclusion of recovery subgroups. The dosing schedule for the monkey study was every other day, and the schedule for the 4-week rat and dog studies was twice weekly, which was chosen to mimic the maximum anticipated clinical dosing frequency. However, the clinical dosing regimen for subcutaneous pegnivacogin will likely be less frequent, with a dose interval of every 7-10 days following an initial loading dose for repeat-dose indications, or as a single dose for indications where anticoagulation for periods of <7 days is required.
No adverse effects of pegnivacogin were observed in the primary 4-week SC toxicity studies in rats and dogs up to the highest dose levels tested of 25 and 10 mg/kg/dose, respectively, administered twice weekly. Apart from the expected prolongation of aPTT, reflecting the intended inhibition of Factor IXa, the only other pegnivacogin-related finding in these studies was vacuolation of macrophages in the SC injection sites, which simply reflects uptake of the PEGylated aptamer. Similarly, in the 2-week SC study in monkeys, pegnivacogin was well tolerated up to the highest dose level of 5 mg/kg/dose, administered every other day for 13 days (7 doses). All of the anatomic pathology findings in the latter study were of a hemorrhagic nature and were not highly adverse, and nearly all of these findings appeared to be secondary to minor tissue injury caused by study procedures, which would be expected to produce more extensive bruising/hemorrhage in highly anticoagulated animals. The occurrence of these types of lesions in monkeys and not in dogs or rats most likely reflects the more intensive restraint conditions required to conduct studies in monkeys. Hence, there were no findings in any of the SC toxicity studies that would elicit concern for human safety associated with single or repeat-dose administration of pegnivacogin.
3.4.12. Comments on Immunogenicity and Immunotoxicity
Although immunogenicity and immunotoxicity were not directly assessed in the REG1 toxicity studies, some of the study endpoints reflect on whether such effects could be elicited by the REG1 Anticoagulation System. In all six studies that included groups treated for up to 14 days with pegnivacogin, anivamersen or the combination administered intravenously in mice (REG1-TOX002) and monkeys (REG1-TOX003; REG1-TOX006) or subcutaneously in monkeys (REG1-TOX007), or for 28 days with subcutaneous administration of pegnivacogin in dogs (TOX-RB006-10-002) and rats (TOX-RB006-10-001), there were no effects on lymphoid organs that would suggest any immunomodulatory activity of the oligonucleotides. In addition, there was no suggestion of any immunogenic potential (i.e., a neutralizing

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 40 of 105 CONFIDENTIAL
antibody response) for pegnivacogin in any of the repeat-dose studies, based on the persistence of pharmacologic activity over the 2-week or 4-week treatment periods. On the contrary, pharmacologic activity (reflected by aPTT prolongation) was cumulative in some studies at high dose levels and with more frequent dosing. Primary antibody responses to antigens develop in 9-10 days and can be completely neutralizing within two weeks. Hence, the 14-28 day treatment durations constitute a relevant exposure for assessing immunologic effects.
3.4.13. Blood Compatibility Study and Vascular Tolerability
A conventional blood compatibility study, including assessment of both hemolysis and flocculation in human blood, did not reveal any effects of pegnivacogin, anivamersen or the combination. Also, there was no evidence for blood incompatibility or vascular intolerability during any of the toxicity studies conducted in monkeys or mice. As discussed above, considerable extravasation of pegnivacogin and anivamersen doses occurred in the 14-day mouse study in which injections were made twice daily into very small tail veins for 14 consecutive days. Hence, this condition represented a “worst-case” perivascular exposure scenario. However, no local toxicity was evident either macroscopically or microscopically. Therefore, it is concluded that pegnivacogin and anivamersen do not exhibit significant local tissue intolerability when repeatedly injected into small veins, and both components of the REG1 Anticoagulation System are highly compatible with whole human blood.
3.4.14. Genetic Toxicity Studies
Four studies were conducted to assess the genetic toxicity potential of the REG1 Anticoagulation System and the pegnivacogin and anivamersen components. These included a bacterial mutagenicity assay, two in vitro chromosomal aberrations assay (one with Chinese hamster ovary [CHO] cells and one with human peripheral blood leukocytes [PBLs]), and an in vivo mouse micronucleus assay. In all of these studies, pegnivacogin and anivamersen were tested separately and in combination, and the dose levels tested were the maximum “limit” doses stipulated in regulatory guidance documents (e.g., ICH).
No positive responses were observed in these studies, with the exception of a weak positive response in the chromosomal aberrations assay with CHO cells for both pegnivacogin and anivamersen at the higher concentrations tested (typically only at 5000 µg/mL, but occasionally at lower concentrations). However, there was no consistent pattern to the responses with respect to which incubation conditions were positive or negative (i.e., relative to the incubation time and with or without the metabolic activation system). Also, although a statistical test for a dose-response was positive for some incubation conditions, close scrutiny of the data did not reveal any clear dose-responsiveness. Even more puzzling was the similarity of the apparent randomly positive responses for both pegnivacogin and anivamersen, as these two molecules are highly different in structure (see Section 2, and Figure 2 for a detailed description of the chemistry). Furthermore, other oligonucleotides have been shown to be uniformly negative in genetic toxicity assays (reviewed by Levin et al., 1998). Therefore, the positive responses in the CHO-based assay were suspect.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 41 of 105 CONFIDENTIAL
It has been reported that approximately half of the agents that yield positive responses in the chromosomal aberrations assay do not exert their effect through known mechanisms of genotoxicity. For many of these, the positive result can be shown to be secondary to some form of cellular toxicity that may not be reflected by the conventional indicators of cell viability such as mitotic index (Galloway, 2000). In the opinion of the genetic toxicologist considered to be the leading expert on chromosomal aberrations assays (Sheila Galloway), agents that are found to be positive in the chromosomal aberrations assay that are shown not to have direct DNA damaging capacity (i.e., are negative in mutagenicity assays), and that are negative in an in vivo clastogenicity assay (e.g., the mouse micronucleus assay) at a dose level that represents a reasonably large margin of exposure over human exposure, are unlikely to pose any risk of genotoxicity to humans. “In these cases, in vitro chromosome aberration induction may be considered biologically non-relevant” (Galloway, 2000).
To further address the significance of the findings in the CHO cell-based assay, another chromosomal aberrations assay was conducted with human PBLs. In this study, there was no hint of a positive response over the same concentration range tested in the CHO-based system (up to 5000 µg/mL). Furthermore, the in vivo test for clastogenicity (i.e., the mouse micronucleus assay) did not reveal any positive responses at very high dose levels of pegnivacogin and anivamersen (up to 2000 and 1500 mg/kg, respectively). Therefore, the weight of the evidence casts considerable doubt on the predictive value of the results obtained in the CHO-based system. Considering the limited use of the REG1 Anticoagulation System for clinical applications, there is no concern about genetic toxicity.
3.4.15. Conclusions About REG1 Safety
All treatment-related effects observed in the in vivo toxicity studies were directly or indirectly related to the intended pharmacologic activity of pegnivacogin. No effects of the anivamersen control agent were observed at doses that represent large clinical multiples. The absence of toxicity for anivamersen is not surprising considering its chemical structure (i.e., it contains a natural phosphodiester backbone, without phosphorothioate modification) and its rapid metabolism and clearance in vivo. The toxicokinetic data (summarized in Section 3.3) indicate that anivamersen is sufficiently stable to bind to and completely inactivate pegnivacogin present in circulation, but the unbound oligonucleotide is eliminated very rapidly without any adverse effects in animals; even when large doses are repeatedly administered. In addition, there was no evidence of toxicity related to the pharmacologically inactive complex that forms when anivamersen binds to pegnivacogin, although this complex tended to persist in circulation much longer than anivamersen alone, owing to the PEG moiety derived from pegnivacogin.
Pegnivacogin and anivamersen (alone or in combination) did not induce complement activation at the large clinical multiples tested, pegnivacogin did not stimulate histamine release or cytokine elevation at the large clinical multiples tested, and neither of the REG1 components, or the combination, produced any effects on cardiovascular, respiratory or neurologic function. The REG1 Anticoagulation System was shown to be compatible with human blood, and the weight of the evidence from the genotoxicity battery indicated a lack of this activity.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 42 of 105 CONFIDENTIAL
Thus, the safety profile of REG1 is entirely dictated by the potent pharmacologic activity of pegnivacogin in inhibiting Factor IXa. The salient effects observed at large clinical-multiple doses of pegnivacogin can be summarized as follows:
• Expected dose-dependent prolongation of coagulation times (aPTT and ACT), reflecting Factor IXa inhibition, was observed in monkeys given intravenous doses ranging from 0.25 to 45 mg/kg and in dogs, rats and monkeys that received subcutaneous doses ranging from 0.5 to 25 mg/kg. The anticoagulant effect was closely related to the plasma concentration of pegnivacogin and exhibited a long duration of action that paralleled the slow blood clearance of the aptamer. The duration of aPTT prolongation was particularly lengthy following SC dosing, in part owing to the long absorption phase from the injection site. The anticoagulant activity of pegnivacogin was rapidly and completely inhibited by anivamersen, and this inactivation was associated with almost complete elimination of free pegnivacogin in plasma for an extended period of time after anivamersen administration. [Note: For the repeat dose SC pegnivacogin applications, anivamersen is not intended to be routinely used in combination with pegnivacogin for reversal of anticoagulation (unlike the REG1 system), but may be occasionally employed to modulate excessive anticoagulation. For single dose SC pegnivacogin applications, anivamersen will be administered intravenously following the SC pegnivacogin dose.]
• The anticoagulant activity of pegnivacogin was rapidly and completely inhibited by anivamersen, as predicted from pharmacology studies, and this neutralization of activity was associated with almost complete elimination of free pegnivacogin for an extended period of time after anivamersen administration. Thus, the REG1 Anticoagulation System behaved exactly as designed across a broad dosage range.
• Single doses of pegnivacogin up to 30 mg/kg had no adverse effects on cynomolgus monkeys when given under conditions in which stasis at injection and blood sampling sites was controlled. Similarly, repeated intravenous injection in mice for 14 consecutive days at doses up to 22.5 mg/kg did not produce any adverse effects.
• Single high doses (≥ 5 mg/kg) of pegnivacogin to monkeys under conditions in which hemorrhage at venipuncture sites was not effectively controlled resulted in bleeding complications that led to loss of some animals. However, subsequent implementation of proper procedures to prevent uncontrolled bleeding eliminated such problems, and large clinical-multiple doses were generally well tolerated henceforth. As expected, the tolerability of monkeys to repeated dosing with pegnivacogin was influenced by dose and dosing schedule and was distinctly improved when the dose of pegnivacogin was followed by injection of Anivamersen three hours later on each dosing occasion (i.e., when the period of anticoagulation on each dosing day was limited).

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 43 of 105 CONFIDENTIAL
• Significant intolerability to repeated dosing with pegnivacogin was observed in a two-week study in monkeys in which the animals were given large doses of pegnivacogin (5 mg/kg) by intravenous injection twice daily for 14 days, without neutralization by anivamersen. Under these conditions, the animals were profoundly and persistently anticoagulated to an extent that resulted in hemorrhages at sites of tissue trauma from handling and in several internal organs. Several of the animals with these sequelae were terminated early in apparent poor condition. aPTT measurement and toxicokinetic data confirmed the cumulative and pronounced degree of anticoagulation under these extreme exposure conditions, which are not clinically relevant. Importantly, the incidence and severity of hemorrhages were markedly reduced when pegnivacogin was given once daily (at a 10 mg/kg dose level) followed by neutralization 3 hours later with Anivamersen (20 mg/kg). In addition, lower doses of pegnivacogin given twice daily were well tolerated by monkeys.
• In all of the repeat-dose toxicity studies, there were no changes in lymphoid tissues or any other clinical or anatomic pathology changes suggestive of immunotoxicity. The confinement of pegnivacogin and the pegnivacogin/anivamersen complex to the blood compartment, as well as the rapid elimination of anivamersen from circulation, would very likely preclude any potential for immunotoxicity. In addition, there was no suggestion of any immunogenic potential (i.e., a neutralizing antibody response) for pegnivacogin or anivamersen in any of the repeat-dose studies, based on the absence of any loss of pharmacologic activity over a 14-28day treatment period, a window sufficient for generation of a primary antibody response (i.e. >9-10 days).
Thus, no effects of the REG1 Anticoagulation System were revealed by the nonclinical toxicity studies that would raise concern about planned clinical evaluations. Manifestations of exaggerated pharmacology that translated into deleterious effects on monkeys occurred when large clinical-multiple doses of pegnivacogin alone were given under conditions in which no measures to control bleeding at venipuncture sites were implemented or when such large doses were given frequently (i.e., twice daily) without neutralization by anivamersen, which cumulated in profound and persistent anticoagulation. These exposure circumstances are not clinically relevant.
3.5. Section 3 References Galloway S M. Cytotoxicity and chromosome aberrations in vitro: experience in industry and the case for an upper limit on toxicity in the aberration assay. Environ Mol Mutagen 2000; 35:191-201.
Geary RS, Leeds JM, Fitchett J, Burckin T, Truong L, Spainhour C, Creek M, Levin AA. Pharmacokinetics and metabolism in mice of a phosphorothioate oligonucleotide antisense inhibitor of C-raf-1 kinase expression. Drug Metab Dispos 1997; 25(11):1272-81.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 44 of 105 CONFIDENTIAL
Guyton, Arthur C & Hall, John E (Ed.). Textbook of Medical Physiology, 11th Edition. (2005) Philadelphia, PA : Elsevier Inc.
Levin A A, Monteith D K, Leeds JM, Nicklin P L, Geary R S, Butler M, Templin M V, and Henry S P (1998). Toxicity of oligonucleotide therapeutic agents, In Handbook of Experimental Pharmacology, G. V. R. e. a. Born, ed. (Berlin: Springer-Verlag), pp. 169-215.
Rusconi CP, Roberts JD, Pitoc GA, Nimjee S M, White RR, Quick G, Scardino E, Fay WP, and Sullenger BA. Antidote-mediated control of an anticoagulant aptamer in vivo. Nat Biotechnol 2004; 22:1423-1428.
Rusconi C P, Scardino E, Layzer J, Pitoc GA, Ortel T L, Monroe D, and Sullenger BA. RNA aptamers as reversible antagonists of coagulation factor IXa. Nature 2002; 419: 90-94.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 45 of 105 CONFIDENTIAL
4. EFFECTS IN HUMAN SUBJECTS
4.1. Overview of Clinical Studies Regado has conducted a comprehensive Phase 1 program of the REG1 Anticoagulation System, and has completed one Phase 2a study investigating the feasibility of using REG1 to support the conduct of elective PCI. A second Phase 2a study investigating the feasibility of using REG1 to support the conduct of off-pump coronary artery bypass grafting was terminated. A Phase 2b study to evaluate the safety and efficacy of the REG1 in Non-ST Elevation (NSTEMI) acute coronary syndrome (ACS) patients undergoing early cardiac catheterization was completed. A list of all clinical studies conducted with REG1 is presented in Table 4 followed by discussions of each study in Section 4.1. Primary publications describing the results of each Phase 1 and 2A study have been published (Dyke et. al. Circulation, 2006; Chan et. al., Circulation, 2008; Chan et. al., JTH, 2008; Cohen et. al. Circulation, 2011). The design of the Phase 2b study has been published (Povsic, 2011) and the results were reported at the American College of Cardiology 2011 Scientific Sessions (Povsic). The PK/PD results from a subset of patients of the REG1-CLIN211 study has been accepted for publication in the European Heart Journal (Povsic).

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 46 of 105 CONFIDENTIAL
Table 4: Listing of Clinical Studies Conducted with REG1
a A total of 85 and 50 subjects were randomized in CLIN101 and CLIN102, respectively, but one subject in each study was withdrawn prior to dosing with study drug. b
A total of 640 subjects were randomized, but 623 received study drug.
Protocol Number REG1-CLIN
Countries Study Design and
Phase
Treatment Groups
Number of
Subjects Dosed
Status
CLIN101 US Phase 1, single dose, dose escalation in healthy volunteers
IV injection of pegnivacogin (15, 30, 60, 90 mg) and anivamersen (30, 60, 120, 180 mg) alone and in combination; and placebo/placebo
84 Study a Completed
(01APR2006)
CLIN102 US Phase 1, single dose, dose escalation in patients with stable coronary artery disease (CAD)
IV injection of pegnivacogin (15, 30, 50, 75 mg) alone and in combination with anivamersen (30, 60, 120, 150 mg); and placebo/placebo
49a Study Completed
(03APR2007)
CLIN103
US
Phase 1, multiple dose in healthy volunteers
IV injection of pegnivacogin (0.75 mg/kg) followed by anivamersen (dose ranging from 0.094 to 2 mg/kg) every other day for 6 days; and placebo/placebo
39
Study Completed
(28DEC2006)
CLIN210
US and Argentina
Phase 2, single dose in patients with CAD undergoing elective percutaneous coronary intervention
IV injection of pegnivacogin (1 mg/kg) followed by anivamersen (2 mg/kg) administered as a single bolus or as 2 partial dose injections 4 hrs apart; and placebo
26 Study Completed (8OCT2008)
CLIN220a US
Phase 2, single dose in patients with CAD undergoing elective Off-pump coronary artery bypass graft (OPCAB) surgery
IV injection of pegnivacogin (1.5 mg/kg) followed by anivamersen (1.5 mg/kg)
1 Study terminated
CLIN211 Poland, US, Germany, Canada, France &
Netherlands
Phase 2B, single dose in patients with NSTE ACS undergoing cardiac catheterization
IV injection of pegnivacogin (1 mg/kg) followed by anivamersen ( 1 mg/kg, 0.4 mg/kg, 0.2 mg/kg or 0.075 mg/kg; and heparin
623 Study Completed b
(14FEB2011)

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 47 of 105 CONFIDENTIAL
4.1.1. REG1-CLIN101
REG-CLIN101 was a multi-center, subject-blinded, dose-escalation, placebo-controlled study in healthy volunteers. The primary objective was to evaluate the safety of ascending single doses of the REG1 Anticoagulation System (RNA aptamer FIXa inhibitor pegnivacogin with and without the control agent anivamersen) in this population. The secondary objective was to evaluate tolerability and pharmacokinetic/pharmacodynamic relationships of the REG1 Anticoagulation System. The following doses of the REG1 anticoagulation System were administered: pegnivacogin alone at 15 mg, 30 mg, 60 mg, and 90 mg; anivamersen alone at 30 mg, 60 mg, 120 mg, and 180 mg; and pegnivacogin + anivamersen (pegnivacogin administered at time 0 and anivamersen administered 3 hours later) at 15/30 mg, 30/60 mg, 60/120 mg, and 90/180 mg. At each dose level, subjects were sequentially randomized to three groups: Anivamersen alone treatment group, followed by the pegnivacogin + anivamersen treatment group, followed by the pegnivacogin alone treatment group.
Eighty-four (84) of the planned 96 subjects were treated. The study was halted during the enrollment of the High dose pegnivacogin + anivamersen group (90 mg pegnivacogin + 180 mg Anivamersen) upon achievement of pre-defined upper aPTT limit stopping criteria in 1 subject. The majority (65%) of the subjects were male. The median age was 32 years and the median weight was 79 kg. A predictable dose pharmacodynamic response, reflected in activated partial thromboplastin time (aPTT) measurements, was seen after administration of the bolus of pegnivacogin, with a clear correlation between the peak post treatment aPTT and post hoc weight-adjusted dose of drug. In subjects treated with pegnivacogin, Anivamersen administration reversed the pharmacological activity of the drug, with a rapid (mean time, 1 to 5 minutes across all dose levels) and sustained return of aPTT to within the normal range. The activated clotting time (ACT) followed a similar anticoagulant response and reversal pattern. As anticipated, prothrombin time (PT) remained unchanged compared with baseline.
The most frequently reported AEs were bruising at needle insertion sites, headache, dizziness, epistaxis, pruritis, vomiting, and dysguesia. One serious adverse event, an episode of transient encephalopathy, occurred in a subject receiving the low intermediate dose of pegnivacogin. The subject’s symptoms resolved rapidly, and no further sequelae occurred. There were no significant adverse safety signals for bleeding or other drug-related side effects, and overall, both the drug and control-agent were well tolerated. No significant differences were found in median hemoglobin, platelet, creatinine, liver function studies or complement split Bb.
4.1.2. REG1-CLIN102
REG1-CLIN102 was a multi-center, single-dose, dose-escalation study in subjects with stable coronary artery disease (CAD) on oral antiplatelet therapy (aspirin [>80 mg/day] or clopidogrel [≥75 mg/day] or both). The primary objective was to evaluate the safety of a range of doses of the REG1 Anticoagulation System compared to placebo in this target population. The secondary objectives were to evaluate the pharmacokinetic/ pharmacodynamic relationships of the REG1 Anticoagulation System. The following doses of the REG1 Anticoagulation System were administered: pegnivacogin alone at 15 mg,

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 48 of 105 CONFIDENTIAL
30 mg, 50 mg, and 75 mg; and pegnivacogin + anivamersen (pegnivacogin administered at time 0 and Anivamersen administered 3 hours later) at 15/30 mg, 30/60 mg, 50/100 mg, and 75/150 mg.
Forty-nine (49) of the planned 50 subjects were treated. The majority (80%) were male. The mean age was 62 years and the mean weight was 87.8 kg. A predictable dose-response of aPTT was seen following bolus administration of pegnivacogin. ACT followed a similar pattern as the aPTT. As expected, PT remained unchanged compared to baseline. In subjects treated with pegnivacogin followed by Anivamersen, a rapid and sustained return to baseline aPTT was observed.
The most frequently reported AEs were dizziness, vessel puncture site hematoma, and vessel puncture site hemorrhage. All other AEs were reported by only a single subject in any treatment group. All AEs were judged to be mild, with the exception of two AEs judged to be moderate. There were no significant adverse safety signals for bleeding or other drug-related side effects. No significant differences were found in median hemoglobin, platelet, creatinine, liver function, or complement split Bb.
4.1.3. REG1-CLIN103
REG1-CLIN103 was a single-center, randomized, double-blind, placebo-controlled study in healthy volunteers. The primary objective was to evaluate the safety of repeated doses of the REG1 Anticoagulation System compared to placebo in this population. The secondary objectives were to evaluate the pharmacokinetic/pharmacodynamic of repeated doses of the REG1 Anticoagulation System, and to determine the optimal dose ratio of control-agent (anivamersen) for reversal of pegnivacogin-induced anticoagulation. Pegnivacogin dosing (0.75 mg/kg) was selected based on the body weight-adjusted response of subjects’ aPTT (2-fold average elevation) in Study REG1-CLIN101. Anivamersen was administered 1 hour later at the following drug dosing ratios: 2:1(1.5:0.75 mg/kg), 1:1 (0.75:0.75 mg/kg), 0.5:1 (0.375:0.75 mg/kg), 0.3:1 (0.225:0.75 mg/kg), 0.2:1 (0.15:0.75 mg/kg), and 0.125:1 (0.094:0.75 mg/kg).
Thirty-nine (39) of the planned 40 subjects were treated. The majority (64%) were male. The mean age was 30 years and the mean weight was 77 kg. In all three treatment groups, elevation of subjects’ aPTT was observed following administration of drug (pegnivacogin) at 0.75 mg/kg, but not placebo. Repeat doses of pegnivacogin achieved highly reproducible aPTT levels with low intra-subject variability (see Figure 3 while repeat doses of anivamersen reversed the aPTT levels dose-dependently and reproducibly. Planned variable anivamersen reversal demonstrated a rapid, dose related dose:dose (anivamersen:pegnivacogin) reversal of aPTT .
No safety issues were observed following repeated dosing. The most frequently reported AEs were dizziness and nausea. There was no evidence that repeated dosing of the REG1 Anticoagulation System increased the incidence or severity of AEs. There were no significant adverse safety signals for bleeding or other drug-related side effects. No significant

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 49 of 105 CONFIDENTIAL
differences were found in median hemoglobin, platelet, creatinine, liver function, or complement split Bb.
Figure 3: Low Intra- and Inter-Subject Variability with Repeat Doses of pegnivacogin and Anivamersen (Study REG1-CLIN103)
Figure 3: Bars represent the mean + upper 95% confidence interval.
4.1.4. REG1-CLIN210
The REG1-CLIN210 was a Phase 2a study of the feasibility of using REG1 in the setting of elective percutaneous coronary intervention (PCI), as compared to unfractionated heparin plus GPIIbIIIa inhibitors. For subjects assigned to REG1, pegnivacogin was the sole anticoagulant used in support of the PCI procedure, and anivamersen was administered post-PCI to fully reverse pegnivacogin anticoagulation in either a step-wise manner over 4 hours, or immediately, followed by sheath removal 10 minutes after pegnivacogin anticoagulation was fully reversed. Based upon the role of FIXa in coagulation, pegnivacogin effects on measures of coagulation, and pharmacodynamic modeling of the pegnivacogin effects in Phase 1 studies, a pegnivacogin dose of 1 mg/kg was used in the CLIN210 study. The expectation was that this dose would yield substantial (>99%) inhibition of FIX activity, and would support the conduct of PCI in this patient population.
A roll-in group (n=2) treated with REG1 + GP IIb/IIIa inhibitors with step-wise administration of anivamersen (total anivamersen dose 2 mg/kg) was followed by 2 groups randomized 5:1 to REG1 (1 mg/kg pegnivacogin) or heparin. In group 1 (n=12), pegnivacogin was reversed in a step-wise fashion, with a partially reversing dose of anivamersen administered immediately post-PCI and the remaining fully reversing dose administered 4 hours later followed by immediate sheath removal (total anivamersen dose 2 mg/kg). In group 2 (n=12), pegnivacogin was fully reversed with anivamersen upon completion of the procedure, followed by immediate sheath removal. Heparin was dosed to an ACT>250 sec. All subjects received aspirin and clopidogrel 600 mg prior to PCI. The

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 50 of 105 CONFIDENTIAL
primary endpoint was major bleeding within 48 hours. The important secondary endpoints were the composite of death, MI or urgent TVR within 14 days and pharmacodynamic measures.
A total of 22 PCI procedures were conducted using REG1 (including 2 pilot cases). All cases were successful, with final TIMI 3 blood flow and no thrombotic complications. Clinical events included 1 MI and 1 TVR in the REG1groups and 1 MI and 1 major bleed in subjects treated with UFH. Anivamersen rapidly reversed pegnivacogin in a dose-dependent manner. There was no safety issues reported in the study. Both reversal strategies allowed for scheduled sheath removal. PK, PD and PK/PD analyses including data obtained in the CLIN210 study are presented in Sections 4.3.4.2 and 4.3.6.1 below.
4.1.5. REG1-CLIN220a
REG1-CLIN220a was a Phase 2a, multi-center, open label, study to evaluate the feasibility of using REG1 in subjects who were scheduled for elective OPCAB surgery via midline sternotomy. Subjects were to receive weight-adjusted doses of REG1 components (pegnivacogin and anivamersen) during surgery and remain under observation up to discharge or Day 7, whichever occurred first. Subjects were assigned to receive the REG1 Anticoagulation System (open-label), comprised of pegnivacogin (study anticoagulant) and anivamersen (anticoagulant control agent). The primary objective of this trial was to test the feasibility and safety of using the REG1 Anticoagulation System (REG1) in the clinical setting of elective OPCAB surgery in low risk subjects. Secondary endpoints were coagulation measures during OPCAB surgery.
This study planned to enroll up to 10 subjects and the study was discontinued after one subject was enrolled. The subject had the formation of a clot in one of three coronary bypass grafts placed with need for rescue heparin, and was discharged from the hospital in stable condition. The study was discontinued to allow for future studies to better define intra-operative applications of pegnivacogin.
4.1.6. REG1-CLIN211 (RADAR)
REG1-CLIN211 (RADARa
a A Randomized, Partially-Blinded, Multi-Center, Active-Controlled, Dose-Ranging Study Assessing the Safety, Efficacy, and Pharmacodynamics of the REG1 Anticoagulation System Compared to Unfractionated Heparin or Low Molecular Heparin in Subjects with acute coronary syndrome
) was a randomized, partially blinded, multi-center study to evaluate the safety and efficacy of the REG1 in Non-ST Elevation (NSTEMI) acute coronary syndrome (ACS) patients undergoing cardiac catheterization within 24 hours of randomization. The objectives of the trial were: 1) verify that the 1 mg/kg dose of pegnivacogin results in near complete factor IX inhibition; 2) determine the dose response of anivamersen-mediated pegnivacogin reversal as assessed by bleeding to allow prompt safe sheath removal post procedure and; 3) assess the efficacy of REG1 (based on ischemic event rates) as a anticoagulation system in the study population.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 51 of 105 CONFIDENTIAL
A total of 640 subjects were randomized in an open-label design to receive either 1.0 mg/kg pegnivacogin (N=479) or heparin - UFH or LMWH (N=161). Provisional glycoprotein IIb/IIIa inhibitors could be added to the REG1 treatment group for procedural or angiographic complications. Glycoprotein IIb/IIIa inhibitor were recommended for the heparin group. The pegnivacogin subjects received blinded anivamersen in four groups in an adaptive design. The number of randomized and treated patients is summarized below in Table 5.
Table 5: Randomized and treated patients in CLIN211
REG1 25% reversal 0.075 mg/kg
REG1 50% reversal 0.2 mg/kg
REG1 75% reversal 0.4 mg/kg
REG1 100% reversal 1.0 mg/kg
Heparin
Randomized 41 117 120 201 161
Treated 39 113 117 196 158
NOTE: There were 19 subjects who received repeat doses of pegnivacogin and 33 subjects with repeat doses of anivamersen.
Baseline characteristics were well balanced between patients randomized to REG1 versus heparin. The median ages of the REG1- and heparin-treated patients were 64.9 and 62.5 years. The majority (68% of REG1 patients and 72% heparin patients) of the subjects were male. The median weights of the REG1- and heparin-treated groups were 81 kg and 83 kg. The majority of subjects in all treatment groups had cardiovascular histories that included hypertension and dyslipidemia. About 47% had a previous MI and about 30% of the subjects were diabetics. PCI was performed in 58.4% of the REG1 patients and 68.9 % of the heparin patients during the study.
The primary endpoint was the composite incidence of major and minor bleeding (not related to CABG) through Day 30 using the ACUITY criteria. The key secondary endpoint was the proportion of subjects with a composite of ischemic events defined as death, nonfatal myocardial infarction (MI), and recurrent ischemia in target vessel distribution or urgent target vessel revascularization (TVR) through Day 30. All of these endpoints were adjudicated by an independent Clinical Events Committee.
The various treatment strategies are summarized in Table 6.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 52 of 105 CONFIDENTIAL
Table 6: Treatment Strategies for REG1-CLIN211
Treatment Strategy REG1
N=473
Heparin
N = 161
Study Drug, % 98.3 95.0
Anivamersen % (of Patients Treated with REG1) 99.4 -
Aspirin, % 99.6 95.7
Thienopyridine, % 79.9 82.6
GP 2b/3a Inhibitor, % 9.7 16.6
Vascular Closure Device, % 12.9 16.8
Management Strategy
Catheterization, % 99.4 99.4
Medical Therapy, % 30.9 25.5
PCI, % 58.4 68.9
CABG, % 9.1 6.2
In a sub-study of patients the 1 mg/kg dose of pegnivacogin was confirmed as demonstrating near complete factor IX inhibition (Section 4.3.5). The data safety and monitoring board stopped the lowest-dose anivamersen arm (25% reversal) early in the trial per protocol because that arm exceeded a pre-defined bleeding rate. In the three other arms, the rate of total ACUITY bleeding was similar to heparin, with a stepwise numerical reduction in major bleeding with higher doses of the reversal agent. The results of bleeding events reported in REG1-211 are summarized in Table 7 below. Bleeding rates for the ITT population through Day 30 (primary end-point) are shown in Figure 4
In the overall REG1 population there was a numerical reduction in the rate of ischemic events (3.0% vs. 5.7% on heparin). Most of the events were myocardial infarctions (2.6% in the overall REG1 group vs. 4.5% in the heparin group). The composite event rates for ischemic events of the ITT population through Day 30 are shown in Figure 6. Sheaths were removed an average of 24 minutes after the procedure in the REG1 patients vs. three hours in the heparin group.
In addition, there was less early bleeding (before discharge) and more bleeding reported after discharge in REG1-treated subjects than in heparin subjects. The bleeding rates through hospital discharge are shown in Figure 5. Overall, a smaller percentage of subjects in the combined REG1 group had composite ischemic events before discharge than the heparin group although this difference was not statistically significant. The ischemic events through hospital discharge are shown in Figure 7.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 53 of 105 CONFIDENTIAL
Table 7: REG1-CLIN211 Bleeding Events (ITT Population) through Day 30
Outcome REG1 25% reversal N=40 (%)
REG1 50% reversal N=116 (%)
REG1 75% reversal N=119 (%)
REG1 100% reversal N=198 (%)
Heparin N=161
Total ACUITY bleeding 65.0 32.8 34.5 29.8 31.1
Major bleeding 20.0 10.3 8.4 7.1 9.9
REG1 25% vs. REG1 100%: p<0.001 REG1 100% vs. Heparin: p=0.9

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 54 of 105 CONFIDENTIAL
Figure 4: REG1-CLIN211 ACUITY Bleeding – ITT Population Through Day 30
Figure 5: REG1-CLIN211 Bleeding Through Hospital Discharge
N 40 116 118 197 160
N 40 116 118 197 160
Ble
ed
ing
,%
32.8 29.723.4
10.3 8.5 5.110.0
62.5
30.6
20.0
0
10
20
30
40
50
60
70
REG1-25% REG1-50% REG1-75% REG1-100% Heparin
Total BleedingMajor Bleeding

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 55 of 105 CONFIDENTIAL
Figure 6: REG1-CLIN211 Composite Ischemic Events ITT Population Through Day 30
Figure 7: REG1-CLIN211 Composite Ischemic Events Through Discharge
Dea
th, M
I, R
ecur
rent
Is
chem
ia, U
rgen
t TVR
,%
1.9
5.7
0
2
4
6
REG1 Heparin
OR = 0.3, 95% CI 0.1 – 0.8, p = 0.024
No significant study medication related changes were found in platelet, renal function or liver function studies. Adverse events other than bleeding and ischemic events were rare and evenly distributed among the study groups with the exception of three severe allergic reactions.
There were three severe allergic SAEs clustered late in the trial that occurred shortly after administration of pegnivacogin (3-20 minutes) ranging from a patient with a mild dermal reaction to one patient who needed extended hemodynamic support. REG1-CLIN211 AEs are discussed in detail in Section 4.5.4 and SAEs in Section 4.5.5.2.
3.0
5.7
0
2
4
6
REG1 Heparin
OR = 0.5, 95% CI 0.2 1.3, p = 0.2

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 56 of 105 CONFIDENTIAL
The study enrollment was paused after the third severe allergic SAE after 640 subjects were enrolled (the first reaction occurring after 439 subjects were enrolled). After careful consideration, the Steering Committee recommended terminating the study, a recommendation accepted by the sponsor. This decision was based on a blinded assessment of bleeding and ischemic events which revealed that the number of events were sufficient to meet the primary (and first secondary) objective of the study.
4.2. Total exposure Table 8: REG1 Subject Exposure and Duration of Follow-up
Study Number (REG1-CLIN)
Pegnivacogin Treatment Anivamersen Treatment Duration of Follow-up Dose Number of
Exposures Dose Number of
Exposures
101: Single dose study of
REG1 and components in
healthy volunteers
15 mg
a
14 30 mg 14 Clinical safety and PK/PD follow-up
for 7 days 30 mg 13 60 mg 13
60 mg 14 120 mg 14
90 mg 4 180 mg 11
102: Single dose study of
REG1 and pegnivacogin in
subjects with stable CAD
15mg
b
9 30 mg 6 Clinical safety follow-up for 14
days; PK/PD for 7 days
30 mg 9 60 mg 6
50 mg 11 100 mg 7
75 mg 12 150 mg 8
103: Repeat dose study of REG1 System
in healthy volunteers
0.75 mg/kg 91 1.5 mg/kg c 45 Clinical safety follow up for 14
days; PK/PD follow-up for 6
days (24 hrs post last pegnivacogin
dose)
d
0.75 mg/kg 18
0.375 mg/kg 8
0.225 mg/kg 4
0.15 mg/kg 10
0.094 mg/kg 6
Total Phase 1 Pegnivacogin Total
177 Anivamersen Total
170

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 57 of 105 CONFIDENTIAL
Table 9: Continued (REG1 Subject Exposure and Duration of Follow-up)
210: single dose in patients with
CAD undergoing elective PCI
1.0 mg/kg 22 0.2 mg/kg 12 Clinical safety follow-up for 14
days; PK/PD follow-up for 24 hrs post anivamersen or
discharge
1.8 mg/kg 12
2.0 mg/kg 10
220a: single dose in patients
with CAD undergoing
elective OPCAB surgery
1.93 mg/kg 1 1.93 mg/kg 1
Clinical safety follow-up for 7 days; PK/PD
follow-up for 24 hrs post anivamersen
Re-dosed e Re-
dosed f
211: single dose in ACS patients
undergoing cardiac
catheterization
1.032 mg/kg 465 19 0.075 mg/kg 25 12 Clinical safety and efficacy follow-up for 30 days;
PK/PD (in a subset of patients from dosing through end of catheterization)
0.2 mg/kg 107
6
0.4 mg/kg 111 6
1.0 mg/kg 185 9
Total Phase 2 Pegnivacogin Total 488 Anivamersen
Total 496
Total exposure for all studies
Pegnivacogin Total 665 Anivamersen
Total 666
a Totals for pegnivacogin and anivamersen exposures include subjects receiving pegnivacogin and anivamersen alone, as well as subjects receiving pegnivacogin followed 3 hrs later by anivamersen
b Totals for pegnivacogin and anivamersen exposures include subjects receiving pegnivacogin alone, as well as subjects receiving pegnivacogin followed 3 hrs later by anivamersen
c Totals for pegnivacogin are for total pegnivacogin exposures, with pegnivacogin being administered to each subject on days 1, 3 and 5 of the study
d Totals for anivamersen at the 1.5 mg/kg dose are for total exposures, with 12 subjects receiving anivamersen at this dose on days 1, 3 and 5, and a separate cohort of 9 subjects receiving this dose on day 1 of dosing
e Redosing of pegnivacogin was a variable dose based upon aPTT or ACT results f
A total of 665 and 666 individual exposures to pegnivacogin and anivamersen, respectively, have been reported in three Phase 1 clinical studies (REG1-CLIN101, REG1-CLIN102, and REG1-CLIN103) and the three Phase 2 clinical studies (REG1-CLIN210, REG1-CLIN220a and REG1-CLIN211). The majority of pegnivacogin exposures (529) in the program were reported in subjects with coronary artery disease that were taking aspirin and/or clopidogrel/prasugrel while the majority of individual pegnivacogin exposures in Phase 1 (136) were in healthy volunteers.
Anivamersen redosing was at 1mg/kg in an unblinded fashion

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 58 of 105 CONFIDENTIAL
4.3. Clinical Pharmacology
4.3.1. Measures of Coagulation
Standard measures of coagulation include the plasma-based (PT) and aPTT assays, and whole blood POC activated clotting time (ACT) and aPTT assays. While the activators used to initiate coagulation in each of these assays are different, they share the common feature of clot formation as the endpoint for the assay. Importantly, in these in vitro assays, low levels of thrombin, ~10-30 nM, are sufficient to produce enough fibrin to reach the endpoint. This level of thrombin represents conversion of only 3-5% of prothrombin to thrombin, and is consistent with the amount of thrombin generated during the initiation phase of the coagulation reaction (Butenas et al., 2003; Mann et al., 2003). Thus, these assays report largely on the initiation phase. Therefore, for specific inhibitors of coagulation factors with a primary role in propagation, such as FIXa, these measures are expected to exhibit modest increases as compared to nonspecific anticoagulants such as unfractionated heparin.
The manner in which the standard clot-based assays reflect FIX/IXa activity is exemplified by their ability to detect or not detect abnormal coagulation measures in individuals with severe hemophilia A (FVIII deficiency) or B (FIX deficiency). A hallmark of hemophilia is the isolated prolongation of the aPTT, as individuals with hemophilia have abnormal aPTTs, but normal PTs (Bolton-Maggs and Pasi, 2003). The cell-based model of coagulation explains this paradox. The PT assay is initiated with supra-physiologic levels of tissue factor, enough to yield a clot in 11-15 seconds. The high levels of tissue factor-FVIIa complex used to initiate the reaction rapidly produce FXa in amounts sufficient to yield enough thrombin to reach the clot endpoint, even in the absence of FVIII or FIX. Thus, pharmacologic inhibitors of FIXa, such as the anti-FIXa aptamer pegnivacogin, are not expected to prolong PT values.
aPTT assays are initiated with a charged particulate, such as celite or kaolin, a phospholipid surface, and calcium in sufficient quantities to yield a clot in ~28-35 seconds. Individuals with hemophilia B (and A) register abnormal aPTT values. The magnitude of the prolongation of aPTT in these individuals is finite, that is, it yields a limit value, as the assay largely reports on the initiation phase of coagulation. In general, the observed prolongation of the aPTT increases with the severity of hemophilia B. However, a strict correlation between the severity of hemophilia B and aPTT prolongation have not been derived. Therefore, to determine a quantitative relationship between FIX activity levels and aPTT prolongation we’ve used the plasma FIX assay. The relationship of aPTT prolongation to Factor IX levels is shown in Figure 8 and shows an approximate log-linear relationship between loss of FIX activity and aPTT prolongation, reaching a maximum prolongation of an approximately 2 to 2.5-fold increase over baseline when the plasma FIX activity is < 1-3% of normal (i.e., reduced by > 97-99%).

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 59 of 105 CONFIDENTIAL
Figure 8: FIX Activity Assay Standard Curve in Human Plasma
Because point of care assays such as the ACT and whole blood aPTT are used primarily to monitor anticoagulation during surgical and interventional procedures, little data exist as to how these assays are impacted by reduced FIX/FIXa activity, as individuals with hemophilia are typically treated with factor replacement therapy (or a similar therapy) prior to undergoing such procedures. In addition, due to the limited availability of FIX deficient whole blood, factor titrations cannot be performed in this matrix to define the effect of loss of specific coagulation factors on whole blood assays. However, as these POC assays are endpoint assays initiated with charged particulates, the effect of pharmacologic inhibition of FIXa in these assays likely mirrors that observed in the aPTT assay. That is, prolongation of the whole blood POC assays is not expected to occur until a substantial degree of FIXa inhibition is achieved (>50%), and a saturation or peak effect level in response to FIXa inhibition is expected to be observed.
4.3.2. Pharmacodynamic drug interactions
The interaction of pegnivacogin with other anticoagulant and procoagulant agents has been evaluated in vitro using both the aPTT and CAT assays to evaluate the effect of combining these agents.
The interaction of pegnivacogin with low concentrations of heparin or lepirudin was evaluated in vitro by Tanaka et al. (Tanaka et al. 2009). Data presented in Figure 9 and Figure 10 is reproduced directly from this publication. As shown in Figure 9, the addition of low concentrations of heparin to plasma containing increasing concentrations of pegnivacogin leads to an increased prolongation of aPTT beyond that achieved by pegnivacogin alone. The magnitude of the increase is similar at pegnivacogin concentrations ranging from 6-24 µg/mL. Similar results are presented in Figure 8 for the addition of low concentrations of the direct thrombin inhibitor lepirudin to increasing concentrations of pegnivacogin. As with heparin, the addition of lepirudin to plasma containing pegnivacogin

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 60 of 105 CONFIDENTIAL
leads to an increased prolongation of aPTT beyond that achieved by pegnivacogin alone. However, in the case of plasma samples containing both pegnivacogin and lepirudin, the magnitude of the prolongation in the aPTT in the presence of lepirudin increases as the concentration of pegnivacogin increases.
Figure 9: Interaction of Pegnivacogin with Heparin and Lepirudin: aPTT Results.
Figure 9: Plasma was spiked with heparin or lepirudin and increasing concentrations of pegnivacogin, and
aPTT measured. Reversal of pegnivacogin by anivamersen is shown at each pegnivacogin concentration.
Figure 10 shows the interaction of pegnivacogin with heparin and with lepirudin, as assessed by measuring thrombin generation in the CAT assay. As with the interaction assessment using the aPTT assay, the addition of heparin or lepirudin to plasma samples containing pegnivacogin further increases the inhibition of thrombin generation observed in the presence of pegnivacogin alone. Likewise, as in the aPTT assay, the magnitude of the increase in inhibition is greater when the direct thrombin inhibitor lepirudin is combined with pegnivacogin as compared to heparin. Comparable results were obtained using thromboelastometry as the read-out.
REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 61 of 105 CONFIDENTIAL
Figure 10: Interaction of Pegnivacogin with Heparin and Lepirudin: CAT Results.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 62 of 105 CONFIDENTIAL
Figure 10: Plasma was spiked with heparin or lepirudin and increasing concentrations of pegnivacogin, and
CAT assays were performed using actin as the activator. The dose-response to pegnivacogin alone and reversal by anivamersen is shown in Panel A.
The interaction of pegnivacogin with warfarin was assessed in vitro by Szlam et al. (Szlam et al. 2010). Data presented in Figure 11 are reproduced directly from this publication. The interaction of pegnivacogin with warfarin was assessed by the addition of pegnivacogin to warfarin plasma samples with a therapeutic International Normalized Ratio (INR), followed by performance of CAT assays. As shown in Figure 11 (upper panel), addition of pegnivacogin at concentrations ranging from 6-24 µg/mL to warfarin plasma (INR 2.1) nearly abrogates thrombin generation. Quantification of inhibition of thrombin generation upon addition of pegnivacogin to warfarin plasma (INR 2.1 and 3.1) is shown in Figure 11 (lower panel). In higher INR plasma (INR 3.1), addition of pegnivacogin ranging from 6-24 µg/mL eliminates thrombin generation.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 63 of 105 CONFIDENTIAL
Figure 11: Interaction of Pegnivacogin with Warfarin.
Figure 11: Warfarin plasma (INR 2.1 or 3.1; George King Biomedical, Overland Park, KS) was spiked with
increasing concentrations of pegnivacogin, and CAT assays were performed using 5 pM TF as the activator. The data in lower panel are presented as mean ± SD.
The interaction of pegnivacogin with the procoagulant agents activated prothrombin complex concentrate (aPCC) or recombinant FVIIa (rFVIIA) was assessed in vitro by Bolliger et al. (Bolliger et al. 2010). Data presented in Figure 11 are reproduced directly from this publication. The interaction of pegnivacogin with rFVIIa and aPCC was assessed by addition of 60 nM rFVIIa or 0.4 U/mL aPCC to plasma containing 48 µg/mL pegnivacogin

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 64 of 105 CONFIDENTIAL
(concentrations of rFVIIa and aPCC added are consistent with therapeutic doses to treat bleeding in patients with hemophilia). As shown in Figure 12, addition of rFVIIa has a minimal impact on the inhibition of thrombin generation by pegnivacogin, causing a small decrease in lag time and a small increase in peak thrombin generation. The observed effect of rFVIIa on pegnivacogin inhibition of thrombin is consistent with the model of coagulation in which TF/FVIIa produces limited FXa during initiation to yield a small amount of thrombin, and in which the majority of thrombin generation is driven by FVIIIa/FIXa in the propagation phase. In contrast, addition of aPCC to plasma anticoagulated with pegnivacogin largely restores thrombin generation, presumably by increasing the plasma concentration of Factors VII, IX, X and prothrombin and by the addition of trace levels of FVIIa and FXa. Comparable results were obtained using aPTT and thromboelastometry as the read-outs.
Figure 12: Interaction of Pegnivacogin with rFVIIa and aPCC.
Figure 12: Plasma containing pegnivacogin was spiked with either rFVIIa or aPCC and CAT assays performed
using 2 pM TF as the activator. A representative thrombogram is shown.
4.3.3. Overview of Clinical PD and PK/PD Studies
A listing of studies with PD and PK data is presented in Table 10. Based on the nonclinical PK/PD relationships observed for pegnivacogin, the most predictable PD effects would be expected with mg/kg dosing of pegnivacogin. Therefore, in the initial Phase 1 studies (REG1-CLIN101 and 102), pegnivacogin was administered on a fixed dose basis to generate a broader range of mg/kg pegnivacogin doses. Subsequently, mg/kg dosing was used in the third Phase 1 study (REG1-CLIN103) and the Phase 2a study (REG1-CLIN210) to test the reproducibility of the PD effect upon weight-adjusted pegnivacogin dosing, and the PD and PK/PD relationships derived from analysis of the CLIN101 and CLIN102 data. Anivamersen dosing is a weight:weight ratio of the pegnivacogin dose.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 65 of 105 CONFIDENTIAL
Table 10: Listing of Clinical Studies with Pharmacokinetic and Pharmacodynamic Data
Study (REG1-)
Design Pegnivacogin
Dose Levels
Number of
Subjectsa
Available Data
b
CLIN101 Single dose safety and PK/PD in healthy volunteers
pegnivacogin+anivamersen: 0, 15, 30, 60 and 90 mgs over 3 hrs
pegnivacogin alone: 0, 15, 30 and 60 mgs
24
21
PK and PD with intensive sampling
CLIN102 Multi-center dose-ranging Phase 1b study in patients with CAD
-0, 15, 30, 50 and 75 mg 41 PD over 3 hours
CLIN103 Repeat dose safety of REG1 in healthy volunteers
-0.75 mg/kg on Days 1, 3 and 5
31 PD data for 1 hr post each pegnivacogin dose, prior to anivamersen administration
CLIN210 Multi-center dose-ranging Phase 2a study in patients undergoing elective PCI
-1.0 mg/kg 22 PK and PD at 5 and 15 minutes post pegnivacogin dose and pre anivamersen
CLIN211 REG1 CLIN211 Pharmacokinetics and Pharmacodynamic Sub-Study Results
-1.0 mg/kg 33 Just prior to administration of pegnivacogin, approximately 20 minutes post pegnivacogin administration, just prior to catheterization and before the administration of anivamersen.
c
a Anivamersen dose was a 2:1 weight:weight dose for CLIN101 and 102, and varied in CLIN103. (See Section 4.4.1).
b Subjects receiving active drug. c All Subjects in REG1-CLIN211 had aPTT measurements, although not all of them were included in the
PK/PD analysis

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 66 of 105 CONFIDENTIAL
4.3.4. Clinical Pharmacokinetics
4.3.4.1. REG1-CLIN101
Pharmacokinetic data for REG1 components pegnivacogin and anivamersen were obtained during the First-Time-In-Human Phase 1 study for REG1. REG-CLIN101 was a Phase 1a, randomized, multi-center, placebo-controlled, subject-blinded, single intravenous dose-escalation study in healthy volunteers (See Section 4.1.1).
At each dose level, a total of 8 subjects were planned to be randomized 7:1, with 7 subjects receiving study drug and 1 subject receiving placebo (sodium chloride injection 0.9% USP), sequentially to treatments groups receiving anivamersen alone, pegnivacogin followed 3 hrs later by anivamersen, or pegnivacogin alone. Therefore, 24 subjects were to be randomized to receive REG1 (or a component of REG1) or placebo at each of the 4 dose levels, for a total of 96 planned subjects, including 84 subjects planned to receive a component of, or REG1. The study was halted during the enrollment of the pegnivacogin + anivamersen High dose group (90 mg pegnivacogin + 180 mg anivamersen) upon achievement of pre-defined upper aPTT limit stopping criteria in 1 subject.
4.3.4.1.1. Anivamersen Component Alone:
The pharmacokinetic profile of anivamersen was established in subjects treated with anivamersen alone. Anivamersen doses of 30 (n=5), 60 (n=6), 120 (n=7) and 180 mg (n=7) were administered as an IV bolus. Mean anivamersen concentration-time data are plotted in Figure 13 over a 9-minute time interval, highlighting the rapid disappearance of anivamersen from plasma.
Figure 13: Mean Anivamersen Plasma Concentration vs Time Profile (REG1-CLIN101)
0.01
0.1
1
10
100
1 2 3 4 5 6 7 8 9Time (min)
30 mg 60 mg 120 mg 180 mg
Arm=1

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 67 of 105 CONFIDENTIAL
Plasma anivamersen concentrations decayed rapidly following the peak with half-lives ranging from 1.4 to 5.4 minutes. AUCINF values increased from 10 to 64 µg/mL. Both CMAX and AUCINF
4.3.4.1.2. REG1 Anticoagulation System (pegnivacogin followed by anivamersen):
tended to increase in proportion to the increase in dose. CL was very high, averaging 2.9 to 6.6 L/min and Vss ranged from 12 to 38 liters. MRT values were short, ranging from just 3.6 to 3.9 minutes.
The effects of anivamersen on the plasma concentrations of pegnivacogin were evaluated in subjects receiving pegnivacogin followed by anivamersen. Pegnivacogin doses of 15 (n=7), 30 (n=6), 60 (n=5) and 90 mg (n=4) were administered as an IV bolus followed 3 hours later by anivamersen doses of 30, 60, 120 and 180 mg (Figure 14).
Figure 14: Mean pegnivacogin Plasma Concentration vs Time Profile in Subjects Treated with REG1 (REG1-CLIN101)
0
5
10
15
20
25
30
0 1 2 3 4 5 6Time (hr)
15 mg 30 mg 60 mg 90 mg
Pharmacokinetic analysis of the concentration-time data was not possible due to the dramatic effects of anivamersen on the pegnivacogin concentrations in the plasma.
In general, pegnivacogin concentrations increased with increase in dose but show a rapid decline to near the lower limit of quantification immediately after administration across all dose ranges of anivamersen. However, within 15 minutes of control agent administration, low but measurable pegnivacogin concentrations were observed at all dose levels tested.
4.3.4.1.3. Pegnivacogin Component Alone:
The pharmacokinetic profile of pegnivacogin was established in subjects treated with pegnivacogin alone. Pegnivacogin dose of 15 (n=7), 30 (n=7), and 60 mg (n=7) were administered as an IV bolus. Non-compartmental pharmacokinetic analysis was performed

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 68 of 105 CONFIDENTIAL
using WinNonlin® version 5.2, (Pharsight Corp) to derive estimates of CMAX, TMAX, AUC0-t, AUCINF, λz, t½, CL, and Vss
Mean pegnivacogin concentration-time data are plotted in
.
Figure 15. In general, pegnivacogin concentrations increased with increase in the administered dose and persisted for at least 1 week (168 hours) in plasma.
Figure 15: Mean pegnivacogin Plasma Concentration vs Time Profile (REG1-CLIN101)
0
2
4
6
8
10
12
14
16
18
0 20 40 60 80 100 120 140 160 180Time (hr)
15 mg30 mg60 mg
Pegnivacogin pharmacokinetic parameters are summarized in Table 11. The mean plasma half-life of pegnivacogin was long, ranging from a mean of 96.4 to 116 hours. Mean CL values ranged from 28 to 39 mL/hr while the steady-state volume of distribution (Vss
Dose proportionality and linearity analyses indicated that pegnivacogin displayed dose proportional pharmacokinetics over the dose range of 15 to 60 mg for the two primary exposure parameters, C
) values averaged 4.4 to 5.8 L. This volume of distribution is approximately equal to total blood volume.
MAX and AUCINF and regression analysis of CL/F indicated that pegnivacogin displays linear kinetics.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 69 of 105 CONFIDENTIAL
Table 11: Summary of Pegnivacogin Pharmacokinetic Parameters in Humans
Dose
(mg)
Statistic C
(µg/mL) MAX T
(hr) MAX t½
(hr)
AUC
(hr*µg/mL) LAST AUC
(hr*µg/mL) INF CL
(L/hr)
V
(L) SS MRT
(hr) INF
15 mg N 6 6 6 6 6 6 6 6
Mean 5.25 0.312 116 366.2 581.6 0.0275 4.46 170.2
SD 1.22 0.227 39.3 94.54 151.0 0.00817 1.19 61.00
Min 4.12 0.02 68.2 268.0 360.3 0.0194 2.32 102.8
Median 4.97 0.38 114 347.4 603.5 0.0251 4.68 162.5
Max 7.32 0.52 172 536.6 773.6 0.0416 5.72 263.7
CV% 23.2 72.7 34.0 25.8 26.0 29.7 26.7 35.8
30 mg N 7 7 7 7 7 7 7 7
Mean 10.8 1.26 109 628.4 939.3 0.0393 5.76 152.5
SD 3.89 2.20 28.6 203.8 316.9 0.027 3.58 38.04
Min 7.26 0.017 69.8 209.7 300.0 0.0246 3.57 106.1
Median 9.96 0.25 111 694.4 923.0 0.0325 4.18 150.9
Max 19.0 6.0 148 819.5 1219 0.100 13.6 204.8
CV% 35.9 173.9 26.4 32.4 33.7 68.7 62.1 24.9
60 mg N 7 7 7 7 7 7 7 7
Mean 19.3 1.26 96.4 1244 1905 0.0327 4.38 138.3
SD 3.35 1.24 24.8 211.8 420.3 0.00665 0.809 35.13
Min 13.9 0.083 71.7 982.3 1362 0.022 3.21 101.8
Median 19.2 1.0 89.4 1277 1810 0.0332 4.40 132.6
Max 24.2 3.0 131 1620 2728 0.0441 5.92 187.9
CV% 17.3 98.0 25.7 17.0 22.1 20.3 18.5 25.4
4.3.4.2. REG1-CLIN210 Pharmacokinetic Results
Samples for pegnivacogin PK assessments were collected prior to pegnivacogin dosing, at 5 and 15 minutes post pegnivacogin dosing, at the end of the PCI procedure, and 5 and 15 minutes post anivamersen dosing in the REG1-CLIN210 Study. For the purposes of evaluating the concentrations achieved post administration of the 1 mg/kg pegnivacogin dose, only results from pegnivacogin measures obtained prior to anivamersen administration will be presented.
Peak pegnivacogin plasma concentrations were achieved within 5 minutes post pegnivacogin administration, and remained essentially unchanged throughout the conduct of the PCI procedure. Median plasma pegnivacogin concentrations 5 minute post administration were 26.15 µg/mL (interquartile range of 18.65 to 30.38 µg/mL), and mean plasma concentrations were 24.63 µg/mL (95% confidence interval of 21.49 to 27.76 µg/mL). By comparison, at

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 70 of 105 CONFIDENTIAL
the end of the PCI procedure, median plasma pegnivacogin concentrations were 26.05 µg/mL (interquartile range of 19.03 to 28.23 µg/mL) and mean plasma concentrations were 24.66 µg/mL (95% confidence interval of 21.88 to 27.43 µg/mL). The stable pegnivacogin concentrations observed throughout the conduct of the PCI procedure are consistent with the stable PD measures observed (plasma aPTT and POC ACT and aPTT), as described in Section 4.3.6.1.
The pegnivacogin concentrations achieved following administration of the 1 mg/kg pegnivacogin dose (approximately 25 µg/mL) are consistent with the levels required to achieve maximal effects in both the plasma and POC aPTT assays. The dose response to pegnivacogin plateaus in the plasma aPTT assay at pegnivacogin concentrations of approximately >12-15 µg/mL, and this plateau occurs at maximal inhibition of plasma FIX activity. Similarly, maximal effects in the POC aPTT assay are achieved at pegnivacogin concentrations > 12 µg/mL. The observed peak increase in the POC aPTT assay in patients treated with 1 mg/kg pegnivacogin in the CLIN210 study is consistent with both complete inhibition of FIX activity and the pegnivacogin concentration measures obtained. For more information, see Section 4.3.6.1.
4.3.5. REG1-CLIN211 Pharmacokinetic Sub-Study Results
A PK/PD sub-study was planned 30 subjects randomized across all REG1 Treatment Groups in REG1-CLIN211 (with a minimum of 20 who did not receive heparin prior to randomization and administration of pegnivacogin). Plasma samples were obtained and sent to a central lab to confirm the anticoagulation properties of the pegnivacogin by measuring the pre-dose Factor IXa activity and pre and post-dose APTT. (The PD results are discussed in Section 4.3.6.2)
Blood samples to measure the plasma concentration of pegnivacogin were obtained just prior to administration of pegnivacogin, approximately 10 - 20 minutes post pegnivacogin administration, just prior to catheterization and before the administration of anivamersen.
Samples from a total of 33 subjects enrolled in the REG1-CLIN211 study who received pegnivacogin were obtained during the study and analyzed at the first DSMB meeting (100 subjects enrolled in the study). Samples were obtained from 21 subjects who did not receive heparin prior to treatment with pegnivacogin. Pharmacokinetic analysis was performed on viable samples from all 33 subjects.
Two subjects had all of their samples excluded since due to > 50% of the samples missing and inaccurate labeling of time of sampling. A total of 112 PK samples were viable for analysis. A total of 71 PD samples were viable for analysis.
Target concentration range > 15 ug/mL was achieved with a mean concentration at all time points achieved within targeted range of 20-30 ug/ml as demonstrated in Table 12.
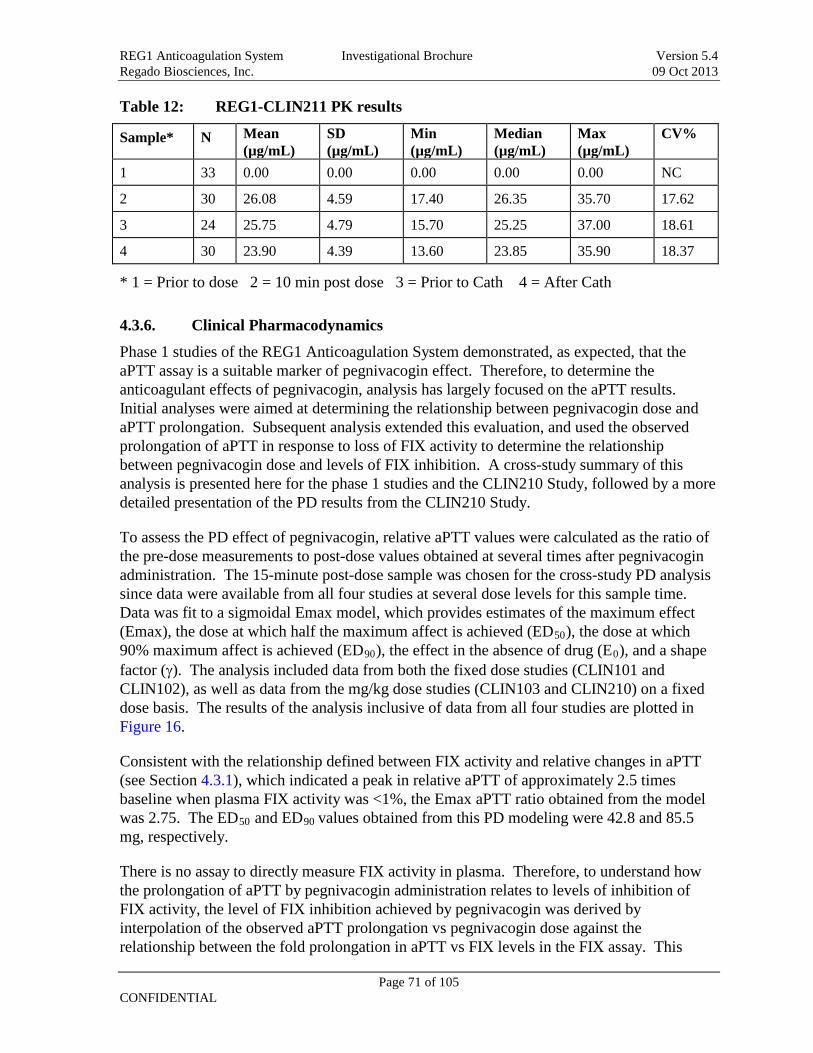
REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 71 of 105 CONFIDENTIAL
Table 12: REG1-CLIN211 PK results
Sample* N Mean (µg/mL)
SD (µg/mL)
Min (µg/mL)
Median (µg/mL)
Max (µg/mL)
CV%
1 33 0.00 0.00 0.00 0.00 0.00 NC
2 30 26.08 4.59 17.40 26.35 35.70 17.62
3 24 25.75 4.79 15.70 25.25 37.00 18.61
4 30 23.90 4.39 13.60 23.85 35.90 18.37
* 1 = Prior to dose 2 = 10 min post dose 3 = Prior to Cath 4 = After Cath
4.3.6. Clinical Pharmacodynamics
Phase 1 studies of the REG1 Anticoagulation System demonstrated, as expected, that the aPTT assay is a suitable marker of pegnivacogin effect. Therefore, to determine the anticoagulant effects of pegnivacogin, analysis has largely focused on the aPTT results. Initial analyses were aimed at determining the relationship between pegnivacogin dose and aPTT prolongation. Subsequent analysis extended this evaluation, and used the observed prolongation of aPTT in response to loss of FIX activity to determine the relationship between pegnivacogin dose and levels of FIX inhibition. A cross-study summary of this analysis is presented here for the phase 1 studies and the CLIN210 Study, followed by a more detailed presentation of the PD results from the CLIN210 Study.
To assess the PD effect of pegnivacogin, relative aPTT values were calculated as the ratio of the pre-dose measurements to post-dose values obtained at several times after pegnivacogin administration. The 15-minute post-dose sample was chosen for the cross-study PD analysis since data were available from all four studies at several dose levels for this sample time. Data was fit to a sigmoidal Emax model, which provides estimates of the maximum effect (Emax), the dose at which half the maximum affect is achieved (ED50), the dose at which 90% maximum affect is achieved (ED90), the effect in the absence of drug (E0), and a shape factor (γ). The analysis included data from both the fixed dose studies (CLIN101 and CLIN102), as well as data from the mg/kg dose studies (CLIN103 and CLIN210) on a fixed dose basis. The results of the analysis inclusive of data from all four studies are plotted in Figure 16.
Consistent with the relationship defined between FIX activity and relative changes in aPTT (see Section 4.3.1), which indicated a peak in relative aPTT of approximately 2.5 times baseline when plasma FIX activity was <1%, the Emax aPTT ratio obtained from the model was 2.75. The ED50 and ED90
There is no assay to directly measure FIX activity in plasma. Therefore, to understand how the prolongation of aPTT by pegnivacogin administration relates to levels of inhibition of FIX activity, the level of FIX inhibition achieved by pegnivacogin was derived by interpolation of the observed aPTT prolongation vs pegnivacogin dose against the relationship between the fold prolongation in aPTT vs FIX levels in the FIX assay. This
values obtained from this PD modeling were 42.8 and 85.5 mg, respectively.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 72 of 105 CONFIDENTIAL
analysis was performed from data obtained 10 or 15 minutes post pegnivacogin dosing in the CLIN101 and 102 studies respectively, as the same clinical coagulation lab was used in both studies. The results are displayed in Figure 17. By this analysis, doses of pegnivacogin >0.75 mg/kg are expected to yield near complete inhibition of plasma FIX activity. This analysis led to the selection of the 1mg/kg pegnivacogin dose for CLIN210, and is confirmed by the PD assessment of pegnivacogin, which yielded an E90
Figure 16: Relationship between aPTT Response and Pegnivacogin Dose (mg dose)
of 85.5 mg, or approximately 1 mg/kg for the populations enrolled in the studies analyzed. This dose was ultimately chosen for the REG1-CLIN211 study following confirmation of PK, PD and PK/PD effects in healthy volunteers (CLIN 101, 103), stable CAD (CLIN 102) and elective PCI (CLIN210).
0
0.5
1
1.5
2
2.5
3
3.5
4
0 20 40 60 80 100 120 Pegnivacogin Dose (mg)
CLIN101 CLIN102 CLIN103 CLIN210 Predicted

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 73 of 105 CONFIDENTIAL
Figure 17: Percent FIX inhibition vs. dose for healthy volunteers (REG1-CLIN101) and patients with coronary artery disease (REG1-CLIN102)
0
10
20
30
40
50
60
70
80
90
100
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6Dose (mg/kg)
4.3.6.1. REG1-CLIN210 Pharmacodynamic Results
Samples for PD assessments (plasma PT, aPTT and whole blood POC aPTT and ACT) were collected at the same time points as the PK samples (See Section 4.3.4.2). Only results from assays responsive to pegnivacogin (aPTT, ACT and POC aPTT) collected prior to anivamersen administration will be presented in this section. PD results following anivamersen administration are presented in Section 4.4.2
Plasma aPTT results are presented in
.
Figure 18. As shown in Figure 18, following administration of 1 mg/kg pegnivacogin to patients undergoing elective PCI, the plasma aPTT reached a maximum of approximately 2.5 fold above baseline 5 minutes post pegnivacogin administration, and remained at this level throughout the conduct of the procedure. The observed increase in aPTT to approximately 2.5 times the baseline value is consistent with loss of >99% of plasma factor IX activity. Furthermore, the plasma aPTT values obtained following administration of 1 mg/kg pegnivacogin are consistent with the maximum achievable increase of 2.6 to 2.7 in response to pegnivacogin administration obtained from modeling of the plasma aPTT results obtained from Phase 1 studies.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 74 of 105 CONFIDENTIAL
Figure 18: REG1-CLIN210 Intraprocedure Plasma aPTT Results
Whole blood POC aPTT results are presented in Figure 19. As observed in the plasma aPTT measures, POC aPTT values reached a maximum effect within 5 minutes of administration of 1 mg/kg pegnivacogin and remained at this level throughout the conduct of the PCI procedure. The median values observed are between 145-148.5 seconds. The observed maximum effect in response to pegnivacogin in this assay is 147.5 seconds (interquartile range of 141.5-155.6 seconds). Therefore, the 1 mg/kg pegnivacogin dose used in the 210 Study achieved the maximum response anticipated upon pegnivacogin administration, and remained consistently at this level throughout the conduct of the procedure.
Figure 19: REG1-CLIN210 Intraprocedure POC aPTT Results

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 75 of 105 CONFIDENTIAL
ACT results are presented in Figure 20. Again, consistent with both the plasma and POC aPTT assays, the ACT was elevated at 5 minutes post pegnivacogin administration. The median ACT 5 minutes post pegnivacogin administration was 223 seconds. ACT values measured 15 minutes post PCI and at the end of the procedure were modestly higher (236-237 seconds), but all values obtained during the procedure are within their respective interquartile ranges, and reflect the maintenance of a consistent level of anticoagulation throughout the procedure. Individual values obtained were generally in the range of 225 seconds, the ACT value regarded as a benchmark for conducting PCI post-heparin administration. Furthermore, based upon the consistency of effect observed between the three assays in response to pegnivacogin administration, the ACT effects observed in this study are likely to represent the maximum anticipated response to pegnivacogin in this assay, which from this study, appears to be a range of approximately 215-250 seconds.
Figure 20: REG1-CLIN210 Intraprocedure ACT Results
4.3.6.2. REG1-CLIN211 (RADAR) Pharmacodynamic Results
The CLIN211 sub-study is described in Section 4.3.5. Pharmacodynamic analysis was performed on viable samples from the 21 subjects who did not receive prior heparin. Samples were obtained prior to dosing with pegnivacogin, 10 – 20 minutes after dosing with pegnivacogin, just prior to heart catheterization (mean 2.3 hours after dosing) and at the end of cardiac catheterization prior to administration of blinded anivamersen mean 2.9 hours after dosing). Plasma aPTT, a reliable marker for FIX deficiency, was measured as the pharmacodynamic result. A target relative aPTT of > 2x baseline was achieved at all time points as represented by absolute aPTT levels in Table 13.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 76 of 105 CONFIDENTIAL
Table 13: REG1-CLIN211 PD (aPTT) results
Sample N Mean
(sec)
SD
(sec)
Min
(sec)
Median
(sec)
Max
(sec)
CV%
1 21 30.84 3.79 24.50 29.50 41.50 12.30
2 20 92.95 9.48 80.70 90.90 113.90 10.20
3 14 93.93 26.83 64.30 88.95 177.10 28.56
4 20 94.67 16.30 78.50 93.10 158.10 17.21
* 1 = Prior to dose 2 = 10 min post dose 3 = Prior to Cath 4 = After Cath
In relation to pegnivacogin concentration, the relative aPTT levels remained stable across all concentrations obtained across all time points consistent with the expected plateau effect as anticipated from the Phase 1 and 2a studies. (Figure 21)
Figure 21: CLIN211- Relative aPTT vs Plasma Pegnivacogin Concentration
20
40
60
80
100
120
0 5 10 15 20 25 30 35RB006 (µg/mL)
Post-dose Pre-dose
Inhibition of FIX was imputed using FIX dilution models in relation of plasma aPTT with an identical methodology as used from the prior REG1 studies. Near complete inhibition (>99%) was achieved in all but 1 sample (97.5% inhibition) at all-time points after dosing , as seen in Figure 22.
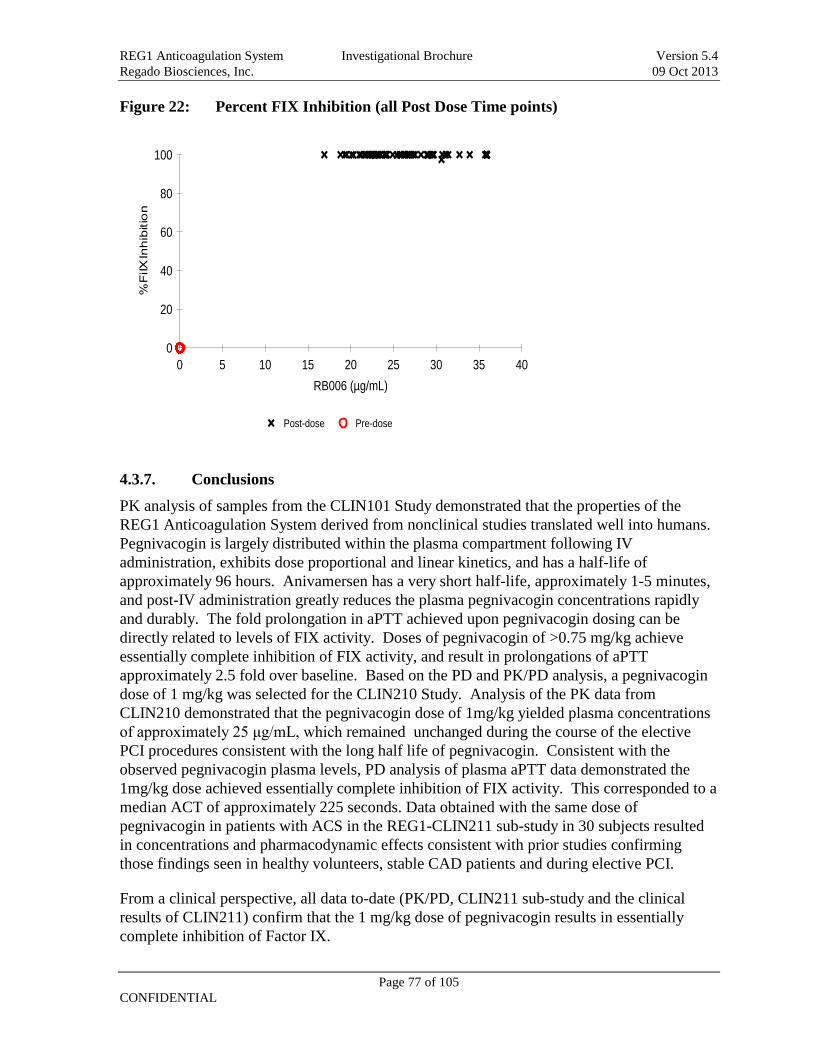
REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 77 of 105 CONFIDENTIAL
Figure 22: Percent FIX Inhibition (all Post Dose Time points)
0
20
40
60
80
100
0 5 10 15 20 25 30 35 40RB006 (µg/mL)
Post-dose Pre-dose
4.3.7. Conclusions
PK analysis of samples from the CLIN101 Study demonstrated that the properties of the REG1 Anticoagulation System derived from nonclinical studies translated well into humans. Pegnivacogin is largely distributed within the plasma compartment following IV administration, exhibits dose proportional and linear kinetics, and has a half-life of approximately 96 hours. Anivamersen has a very short half-life, approximately 1-5 minutes, and post-IV administration greatly reduces the plasma pegnivacogin concentrations rapidly and durably. The fold prolongation in aPTT achieved upon pegnivacogin dosing can be directly related to levels of FIX activity. Doses of pegnivacogin of >0.75 mg/kg achieve essentially complete inhibition of FIX activity, and result in prolongations of aPTT approximately 2.5 fold over baseline. Based on the PD and PK/PD analysis, a pegnivacogin dose of 1 mg/kg was selected for the CLIN210 Study. Analysis of the PK data from CLIN210 demonstrated that the pegnivacogin dose of 1mg/kg yielded plasma concentrations of approximately 25 μg/mL, which remained unchanged during the course of the elective PCI procedures consistent with the long half life of pegnivacogin. Consistent with the observed pegnivacogin plasma levels, PD analysis of plasma aPTT data demonstrated the 1mg/kg dose achieved essentially complete inhibition of FIX activity. This corresponded to a median ACT of approximately 225 seconds. Data obtained with the same dose of pegnivacogin in patients with ACS in the REG1-CLIN211 sub-study in 30 subjects resulted in concentrations and pharmacodynamic effects consistent with prior studies confirming those findings seen in healthy volunteers, stable CAD patients and during elective PCI.
From a clinical perspective, all data to-date (PK/PD, CLIN211 sub-study and the clinical results of CLIN211) confirm that the 1 mg/kg dose of pegnivacogin results in essentially complete inhibition of Factor IX.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 78 of 105 CONFIDENTIAL
4.4. Anivamersen Reversal of Pegnivacogin Analysis of the reversal of pegnivacogin anticoagulant effects by the anticoagulant control agent Anivamersen has been evaluated in all clinical studies of REG1. REG1-CLIN101 and CLIN102 evaluated doses of anivamersen anticipated, based on nonclinical studies, to achieve complete reversal of the PD effects of pegnivacogin (a 2:1 weight:weight ratio of Anivamersen:pegnivacogin). Evaluation of the PD data in CLIN101 and CLIN102 subjects receiving pegnivacogin followed by anivamersen demonstrated that this dose of anivamersen completely reversed the pharmacologic effects of pegnivacogin within 1-5 minutes, and that reversal effects were stable throughout the 7 day follow-up period (Dyke et al., 2006; Chan et al., 2008a). In this section, for the purposes of supporting the anivamersen dose selection in the 211 protocol, data from REG1-CLIN103, in which a range of anivamersen doses was evaluated, and data from REG1-CLIN210, in which two post PCI pegnivacogin reversal strategies were evaluated, will be presented.
4.4.1. Analysis of the Anivamersen Anticoagulant Reversal Dose Response
The response to varying doses of anivamersen following administration of a weight-adjusted dose of pegnivacogin (0.75 mg/kg) was investigated in the REG1-CLIN103 Study. In this study, anivamersen was administered 1 hour post pegnivacogin administration, a time frame when the pegnivacogin effects were expected to remain at maximal levels. Data for the anivamersen anticoagulant reversal dose response is shown in Figure 23.
Figure 23: Anivamersen Anticoagulant Reversal Dose Response
Anivamersen dose ratios of 2:1 and 1:1 fully reversed the observed PD effects of pegnivacogin, returning plasma aPTT values to pre-pegnivacogin dose values.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 79 of 105 CONFIDENTIAL
Anivamersen:pegnivacogin dose ratios less than 1:1 exhibited a graded reversal activity, with doses of 0.5:1, 0.3:1, 0.2:1 and 0.125:1 yielding anticoagulant reversal effects of 84±2.7%, 74±5.9%, 51±6.4% and 41±8.4% from baseline, respectively. The observed titration of the reversal effects of pegnivacogin as a function of anivamersen dose level is consistent with the anivamersen mechanism of action, in which anivamersen forms a 1:1 complex with pegnivacogin.
4.4.2. Anivamersen Anticoagulant Reversal Effects in Elective PCI
REG1-CLIN210 evaluated the feasibility of conducting elective PCI using REG1. A dose of 1 mg/kg pegnivacogin was employed as the sole anticoagulant to support the conduct of PCI. In this study, two post-PCI anticoagulant reversal strategies were evaluated: 1) A step-wise reversal strategy in which an anivamersen dose (0.2:1) targeting 50% reversal of the pegnivacogin anticoagulant activity was administered when the patient was stable post-PCI, followed by administration of the remaining reversal dose (1.8:1 anivamersen:pegnivacogin) 4 hours later and, 2) A full reversal strategy in which a 2:1 anivamersen:pegnivacogin reversal dose was administered when the patient was stable post-PCI. For both reversal strategies, sheath removal was planned to occur 10 minutes post administration of the fully-reversing dose of anivamersen. Anivamersen dosing in the CLIN210 Study was based upon the observed pegnivacogin anticoagulant reversal effects in the CLIN103 Study.
Figure 24: Pharmacodynamic Effects of Pegnivacogin and Reversal Effects of Anivamersen in PCI

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 80 of 105 CONFIDENTIAL
ACT data for the REG1-CLIN210 Study is shown in Figure 24 (data presented as median values with interquartile ranges). Administration of a 0.2:1 anivamersen:pegnivacogin dose followed by a fully reversing anivamersen dose 4 hours later yielded a step-wise reversal of pegnivacogin anticoagulant activity (purple symbols), as intended. Likewise, administration of a fully reversing dose of anivamersen immediately post-PCI (green symbols) yielded the anticipated complete neutralization of pegnivacogin anticoagulant activity.
Both pegnivacogin reversal strategies facilitated planned sheath removal 10 minutes post-administration of the fully reversing dose of anivamersen. No femoral sheath or thrombotic complications occurred in either reversal group.
4.4.3. Anivamersen Anticoagulant Reversal Effects in ACS
A comparison of the predicted PD responses of anivamersen to the observed responses of relative aPTT by timepoint (local lab) in subjects in the PP population with no prior heparin is provided in Table 14. In subjects with no prior heparin use, the predicted PD responses of anivamersen (100%, 75%, 50%, and 25% reversal) corresponded well with the observed mean % reversal of the relative aPTT values (92.6%, 75.6%, 52.5%, and 20.0%) and the differences from predicted reversal levels were not statistically significant. These results indicate the ability to predict reversal with use of REG1.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 81 of 105 CONFIDENTIAL
Table 14: Comparison of the Predicted PD Responses of Anivamersen to the Observed Response of Relative aPTT by Timepoint: PP Population (with No Prior Heparin)
REG1 Pegnivacogin + Anivamersen % Reversal
100% Group
(N = 115) 75% Group
(N= 65) 50% Group
(N = 59) 25% Group
(N = 16) REG1 Combined
(N = 255) aPTT (sec) Before Sheath Removal N 83 51 50 10 194 Mean 39.1 45.3 51.2 75.4 45.7 SD 22.44 14.63 16.18 31.73 21.34 Median 33.0 42.0 45.0 72.0 41.0 Min, Max 19, 200 27, 112 29, 92 47, 157 19, 200
Upon Completion of Catheterization N 66 49 45 5 165 Mean 92.3 91.5 83.3 87.0 89.4 SD 29.68 32.05 22.58 25.01 28.58 Median 87.5 88.0 82.0 97.0 86.0 Min, Max 37, 200 43, 200 40, 135 55, 111 37, 200
Baseline Value N 99 59 55 12 225 Mean 31.2 31.4 31.9 33.5 31.6 SD 10.42 4.96 10.45 12.00 9.36 Median 30.0 31.0 30.0 29.5 30.0 Min, Max 2, 95 23, 46 23, 100 22, 66 2, 100
% Reversal [1] N 63 44 41 4 152 Mean 92.6 75.6 52.5 20.0 75.0 SD 62.98 27.29 50.74 14.90 53.61

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 82 of 105 CONFIDENTIAL
REG1 Pegnivacogin + Anivamersen % Reversal
100% Group
(N = 115) 75% Group
(N= 65) 50% Group
(N = 59) 25% Group
(N = 16) REG1 Combined
(N = 255) Median 95.0 83.5 65.0 22.0 84.0 Min, Max -10, 533 -33, 108 -200, 105 0, 36 -200, 533
One-Sample t-test p-value 0.3569 0.8778 0.7552 0.5502

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 83 of 105 CONFIDENTIAL
4.4.4. Conclusions
Titration of the anivamersen dose relative to the administered pegnivacogin dose yields a graduated reversal of pegnivacogin activity. Reversal of pegnivacogin activity, in either a partially reversing step-wise or fully-reversing fashion following cardiac catheterization with or without PCI was well tolerated in the REG1- CLIN210 and CLIN211 Studies, and enabled early sheath removal. Reversal with variable doses of anivamersen demonstrated a reliable level of reversal in a dose:dose manner in the ACS population after early cardiac catheterization and PCI. Reversal levels > 50% resulted in numerically less major bleeding after early sheath removal.
4.5. Safety of REG1 A general overview of the safety profile of the REG1 Anticoagulation System is presented here. In the following sections, details of the safety findings are presented as follows: Adverse Events of Phase 1 (Section 4.5.1 and 4.5.2); Adverse Events of Phase 2a (Section 4.5.3); Adverse Events of Phase 2b (Section 4.5.3), Serious Adverse Events (Section followed by a general conclusion of the clinical safety findings of the REG1 System (Section 4.6).
The Safety Population includes three Phase 1 and three Phase 2 studies. A total of 123 normal volunteers have received REG1 or its components in Phase 1 studies (104 receiving single doses of pegnivacogin, anivamersen or both and 19 receiving placebo), as have 49 volunteers with stable coronary artery disease (41 receiving single doses of pegnivacogin or pegnivacogin followed by anivamersen and 8 receiving placebo). In Phase 2 studies, 667 patients with CAD have been studied (502 receiving single doses of pegnivacogin followed by anivamersen and 165 receiving heparin): 26 while undergoing coronary stent placement; 1 while undergoing OPCAB surgery; and 640 undergoing cardiac catheterization (387 having PCI).
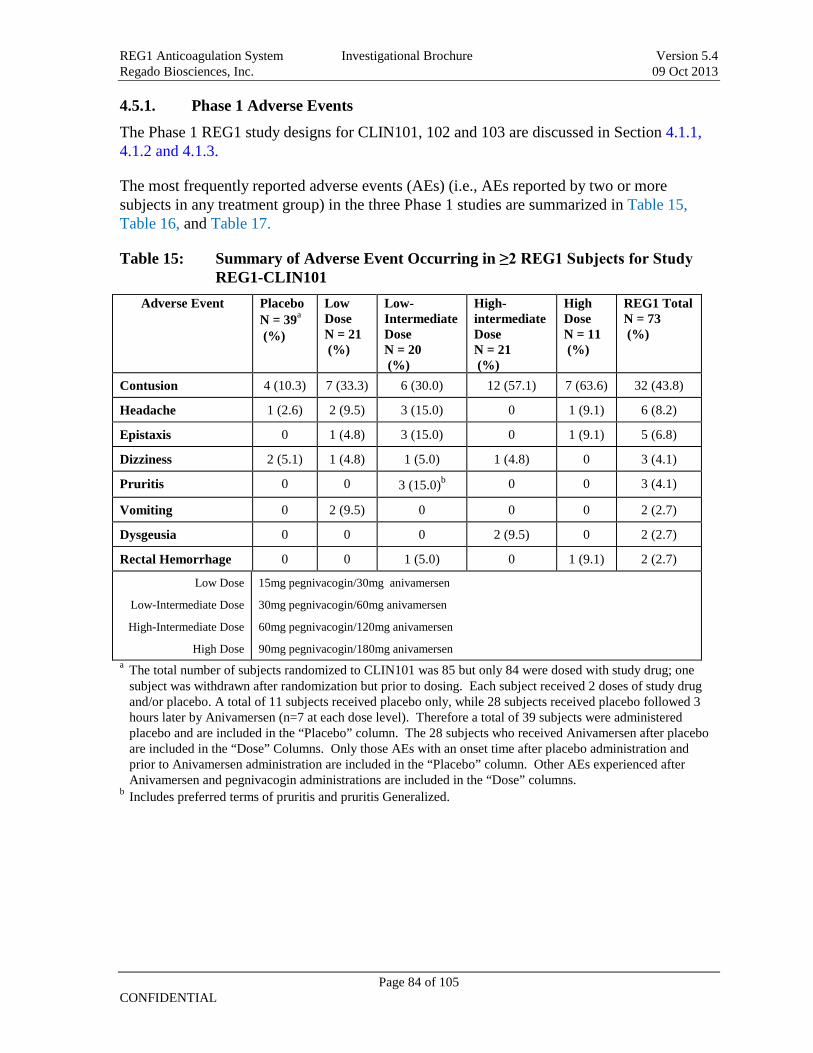
REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 84 of 105 CONFIDENTIAL
4.5.1. Phase 1 Adverse Events
The Phase 1 REG1 study designs for CLIN101, 102 and 103 are discussed in Section
The most frequently reported adverse events (AEs) (i.e., AEs reported by two or more subjects in any treatment group) in the three Phase 1 studies are summarized in
4.1.1, 4.1.2 and 4.1.3.
Table 15, Table 16, and Table 17.
Table 15: Summary of Adverse Event Occurring in ≥2 REG1 Subjects for Study REG1-CLIN101
Adverse Event Placebo N = 39 (%)
a Low Dose N = 21 (%)
Low-Intermediate Dose N = 20 (%)
High-intermediate Dose N = 21 (%)
High Dose N = 11 (%)
REG1 Total N = 73 (%)
Contusion 4 (10.3) 7 (33.3) 6 (30.0) 12 (57.1) 7 (63.6) 32 (43.8)
Headache 1 (2.6) 2 (9.5) 3 (15.0) 0 1 (9.1) 6 (8.2)
Epistaxis 0 1 (4.8) 3 (15.0) 0 1 (9.1) 5 (6.8)
Dizziness 2 (5.1) 1 (4.8) 1 (5.0) 1 (4.8) 0 3 (4.1)
Pruritis 0 0 3 (15.0) 0 b 0 3 (4.1)
Vomiting 0 2 (9.5) 0 0 0 2 (2.7)
Dysgeusia 0 0 0 2 (9.5) 0 2 (2.7)
Rectal Hemorrhage 0 0 1 (5.0) 0 1 (9.1) 2 (2.7)
Low Dose
Low-Intermediate Dose
High-Intermediate Dose
High Dose
15mg pegnivacogin/30mg anivamersen
30mg pegnivacogin/60mg anivamersen
60mg pegnivacogin/120mg anivamersen
90mg pegnivacogin/180mg anivamersen a The total number of subjects randomized to CLIN101 was 85 but only 84 were dosed with study drug; one
subject was withdrawn after randomization but prior to dosing. Each subject received 2 doses of study drug and/or placebo. A total of 11 subjects received placebo only, while 28 subjects received placebo followed 3 hours later by Anivamersen (n=7 at each dose level). Therefore a total of 39 subjects were administered placebo and are included in the “Placebo” column. The 28 subjects who received Anivamersen after placebo are included in the “Dose” Columns. Only those AEs with an onset time after placebo administration and prior to Anivamersen administration are included in the “Placebo” column. Other AEs experienced after Anivamersen and pegnivacogin administrations are included in the “Dose” columns.
b Includes preferred terms of pruritis and pruritis Generalized.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 85 of 105 CONFIDENTIAL
Table 16: Summary of Adverse Events Occurring in ≥2 REG1 Subjects for Study REG1-CLIN102
Adverse Event Placebo N = 8 (%)
Low Dose N = 9 (%)
Low-Intermediate Dose N= 9 (%)
High-intermediate Dose N = 12 (%)
High Dose N = 12 (%)
REG1 Total N = 42 (%)
Vessel puncture site hematoma
2 (25.0) 1 (11.1) 0 2 (16.7) 2 (16.7) 5 (11.9)
Dizziness 0 0 0 2 (16.7) 2 (16.7) 4 (9.5)
Vessel puncture site hemorrhage
0 0 1 (11.1) 2 (16.7) 0 3 (7.1)
Pruritis 0 1 (11.1) 0 1 (8.3) 0 2 (4.8)
Contact Dermatitis 0 0 0 1 (8.3) 1 (8.3) 2 (4.8)
Nausea 0 0 1 (11.1) 0 1 (8.3) 2 (4.8)
Vomiting 0 0 1 (11.1) 1 (8.3) 0 2 (4.8)
Low Dose
Low-Intermediate Dose
High-Intermediate Dose
High Dose
15mg pegnivacogin/30mg anivamersen
30mg pegnivacogin/60mg anivamersen
50mg pegnivacogin/100mg anivamersen
75mg pegnivacogin/150mg anivamersen
Table 17: Summary of Adverse Event Occurring in ≥2 REG1 Subjects for Study REG1-CLIN103
Adverse Eventa,b, Placebo = 8 c (%)
REG1 Group 1 N = 12
(%)
REG1 Group 2 N = 9 (%)
REG1 Group 3 N = 10
(%) Dizziness 2 (25) 1 (8) 2 (22) 0
Fatigue 0 0 1 (11) 1 (10)
Gingival Bleeding 0 1 (8) 1 (11) 0
Headache 0 0 1 (11) 1 (10) a More than one AE category per subject possible.
b Subjects reporting the same Preferred Term (PT) multiple times were counted only once per PT.
c
4.5.2. Phase 1 Adverse Events Summary
pegnivacogin was administered at 0.75 mg/kg on Days 1, 3, and 5. Anivamersen was administered one hour later at varied doses
No significant safety issues were observed in Phase 1. The most frequently reported adverse events (i.e., AEs reported by two or more subjects in any treatment group) were related to bleeding; bruising at needle insertion site – (also described as vessel puncture site hematoma), contusion, epistaxis, gingival and rectal bleeding.
The most frequent non-bleeding AEs seen in the Phase 1 studies were headache, dizziness, pruritis, vomiting, contact dermatitis and dysguesia. The incidence of dizziness was similar to placebo and none of the dizziness was associated with documented hypotension. The overall

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 86 of 105 CONFIDENTIAL
adverse event rate did not differ from placebo. There was no evidence that repeated dosing of the REG1 System increased the incidence or severity of AEs. The majority of AEs were judged to be mild or moderate.
There was one SAE event in all the Phase 1 studies (See Section 4.5.5.1)
4.5.3. Phase 2a Adverse Events
The Phase 2a REG1 study designs for CLIN210 and CLIN220a studies are discussed in Sections 4.1.4 and 4.1.5.
There was only a single subject in study CLIN220a. In this off-pump coronary artery bypass graft surgery (OPCAB) study, the subject had the formation of a clot in one of three coronary bypass grafts placed with need for rescue heparin, and was discharged from the hospital in stable condition. The study was discontinued to allow for future studies to better define intra-operative applications of pegnivacogin. Review of this case along with further in vitro studies suggest that although the patient was adequately anti-coagulated based on systemic blood measurements, there were areas of local stasis in which pegnivacogin levels may have been too low as a result of technical issues in administering the drug during surgery.
The most frequently reported adverse events (AEs) (i.e., AEs reported by two or more subjects in any treatment group) for REG1-210 are summarized in Table 18 and Table 19.
Table 18: Summary of Non-bleeding Adverse Event Occurring in ≥2 REG1 Subjects for Study REG1-CLIN210
AE Partial Reversal Group
Total Reversal Group
Combined Roll-In, Partial, and Total Reversal Groups
REG1 (N=10) N (%)
REG1 (N=10) N (%)
REG1 (N=22) N (%)
UFH (N=4) N (%)
Total (N=26) N (%)
Chest Discomfort 3 (30) 1 (10) 4 (18) 0 4 (15)
Dizziness 1 (10) 1 (10) 2 (9) 0 2 (8)
Nausea 0 1 (10) 1 (5) 1 (25) 2 (8)
Angina Pectoris 0 1 (10) 1 (5) 0 1 (4)
Anxiety 1 (10) 0 1 (5) 0 1 (4)
Arthralgia 1 (10) 0 1 (5) 0 1 (4)
Back Pain 1 (10) 0 1 (5) 0 1 (4)
Chills 1 (10) 0 1 (5) 0 1 (4)
Drug Intolerance 1 (10) 0 1 (5) 0 1 (4)
Hypotension 1 (10) 0 1 (5) 0 1 (4)
Musculoskeletal Discomfort
1 (10) 0 1 (5) 0 1 (4)

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 87 of 105 CONFIDENTIAL
Myocardial Infarction 1 (10) 0 1 (5) 1 (25) 2 (8)
Oropharyngeal Blistering 0 1 (10) 1 (5) 0 1 (4)
Post Procedural Swelling 1 (10) 0 1 (5) 0 1 (4)
Urinary Retention 1 (10) 0 1 (5) 0 1 (4)
Contusion 0 0 0 1 (25) 1 (4)
Feeling Cold 0 0 0 1 (25) 1 (4)
Table 19: Summary of Bleeding Adverse Event Occurring in ≥2 REG1 Subjects for Study REG1-CLIN210
Site/Type of Bleeding Partial Reversal Group
Total Reversal Group
Combined Roll-In, Partial, and Total Reversal Groups
REG1 (N=10) N (%)
REG1 (N=10) N (%)
REG1 (N=22) N (%)
UFH (N=4) N (%)
Total (N=26) N (%)
Access site bleeding 1 (10) 0 3 (14) 0 a 3 (12)
Hematoma ≥5 cm at puncture site
0 1 (10) 1 (5) 1 (25) 2 (8)
Right Groin Ecchymosis 1 (10) 0 1 (5) 0 1 (4) a
The three most common non-bleeding AEs (AEs reported by two or more subjects in any treatment group) reported for REG1 in CLIN210 were chest discomfort, dizziness, and nausea. No patterns or trends in AEs related to bleeding were observed in the study and the bleeding AEs were consistent and expected in any study with arterial and venipuncture, in particular if an anticoagulant is being used and/or injected.
Includes 2 roll-in patients who had received glycoprotein IIb/IIIa inhibitors
One SAE was reported in CLIN210 that was not considered related to study drug (See Section 4.5.5.2).
4.5.4. Phase 2b Adverse Events (REG1-CLIN211)
The Phase 2b CLIN211 study design represents the largest study to-date conducted with the anticipated marketed dose of pegnivacogin and potential doses of anivamersen. The study design is discussed in Section 4.1.6.
The incidence of AEs in relation to study medication for CLIN211 is summarized in Table 20 and frequently reported adverse events (AEs reported by two or more subjects in any treatment group) for REG1-211 are summarized in Table 21 .

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 88 of 105 CONFIDENTIAL
Table 20: Number (Incidence) of Treatment-Emergent Adverse Events and Relationship to Study Medication for in Study REG1-CLIN211
100% Group N=196
75% Group N=117
50% Group N=113
25% Group N=39
REG1 Combined N=465
Heparin N=163
All Patients N=628
Number of Subjects with ≥1 TEAE
112 ( 57) 73 ( 62) 65 ( 58) 32 ( 82) 282 ( 61) 91 ( 56) 373 ( 59)
Not Related 45 ( 23) 28 ( 24) 22 ( 19) 5 ( 13) 100 ( 22) 47 ( 29) 147 ( 23)
Unlikely 20 ( 10) 16 ( 14) 13 ( 12) 5 ( 13) 54 ( 12) 18 ( 11) 72 ( 11)
Possible 38 ( 19) 17 ( 15) 24 ( 21) 17 ( 44) 96 ( 21) 19 ( 12) 115 ( 18)
Probable 9 ( 5) 12 ( 10) 6 ( 5) 5 ( 13) 32 ( 7) 7 ( 4) 39 ( 6)

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 89 of 105 CONFIDENTIAL
Table 21: Summary of Treatment-Emergent Adverse Events Occurring in ≥2 REG1 Subjects and Classified with a “Possible” or “Probable” Relationship to Study Medication for Any Dose Group in Study REG1-CLIN211
100% Group N=196
75% Group N=117
50% Group N=113
25% Group N=39
REG1 Combined
N=465
Heparin
N=163
All Patients N=628
Blood & lymphatic disorders
Eosinophilia 3 ( 2) 1 ( 1) 1 ( 1) 0 5 ( 1) 2 ( 1) 7 ( 1) Possible 2 ( 1) 1 ( 1) 1 ( 1) 0 4 ( 1) 0 4 ( 1) Probable 0 0 0 0 0 0 0 Cardiac disorders Bradycardia 4 ( 2) 2 ( 2) 1 ( 1) 1 ( 3) 8 ( 2) 2 ( 1) 10 ( 2) Possible 0 0 0 0 0 0 0 Probable 0 1 ( 1) 0 0 1 ( <1) 0 1 ( <1) Myocardial infarction
3 ( 2) 2 ( 2) 1 ( 1) 1 ( 3) 7 ( 2) 4 ( 2) 11 ( 2)
Possible 0 0 0 1 ( 3) 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Gastrointestinal disorders
Abdominal pain 1 ( 1) 1 ( 1) 0 1 ( 3) 3 ( 1) 1 ( 1) 4 ( 1) Possible 0 0 0 1 ( 3) 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Nausea 3 ( 2) 3 ( 3) 0 3 ( 8) 9 ( 2) 3 ( 2) 12 ( 2) Possible 1 ( 1) 0 0 0 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 General disorders Chest pain 1 ( 1) 3 ( 3) 0 1 ( 3) 5 ( 1) 2 ( 1) 7 ( 1) Possible 1 ( 1) 0 0 0 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Injury, poisoning and procedural complications
Accidental needle stick
0 0 0 1 ( 3) 1 ( <1) 0 1 ( <1)
Possible 0 0 0 1 ( 3) 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Contusion 1 ( 1) 1 ( 1) 3 ( 3) 1 ( 3) 6 ( 1) 0 6 ( 1) Possible 0 1 ( 1) 0 0 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Investigations Coagulation time prolonged
0 0 0 1 ( 3) 1 ( <1) 0 1 ( <1)
Possible 0 0 0 1 ( 3) 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Musculoskeletal and connective tissue disorders
Groin pain 0 1 ( 1) 1 ( 1) 2 ( 5) 4 ( 1) 0 4 ( 1) Possible 0 0 0 1 ( 3) 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 90 of 105 CONFIDENTIAL
Nervous system disorders
Headache 4 ( 2) 2 ( 2) 0 3 ( 8) 9 ( 2) 6 ( 4) 15 ( 2) Possible 0 0 0 0 0 0 0 Probable 1 ( 1) 0 0 0 1 ( <1) 0 1 ( <1) Paraesthesia 1 ( 1) 2 ( 2) 0 0 3 ( 1) 1 ( 1) 4 ( 1) Possible 1 ( 1) 0 0 0 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Respiratory, thoracic and mediastinal disorders
Dyspnoea 4 ( 2) 3 ( 3) 2 ( 2) 0 9 ( 2) 0 9 ( 1) Possible 1 ( 1) 0 0 0 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Vascular disorders Catheter site hematoma
15 ( 8) 24 ( 21) 15 ( 13) 12 ( 31) 66 ( 14) 20 ( 12) 86 ( 14)
Possible 10 ( 5) 10 ( 9) 7 ( 6) 6 ( 15) 33 ( 7) 6 ( 4) 39 ( 6) Probable 2 ( 1) 6 ( 5) 3 ( 3) 2 ( 5) 13 ( 3) 3 ( 2) 16 ( 3) Catheter site hemorrhage
19 ( 10) 7 ( 6) 11 ( 10) 9 ( 23) 46 ( 10) 17 ( 10) 63 ( 10)
Possible 10 ( 5) 4 ( 3) 8 ( 7) 5 ( 13) 27 ( 6) 9 ( 6) 36 ( 6) Probable 3 ( 2) 2 ( 2) 1 ( 1) 1 ( 3) 7 ( 2) 2 ( 1) 9 ( 1) Catheter thrombosis 4 ( 2) 0 0 0 4 ( 1) 0 4 ( 1) Possible 1 ( 1) 0 0 0 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Ecchymosis 3 ( 2) 0 0 0 3 ( 1) 1 ( 1) 4 ( 1) Possible 2 ( 1) 0 0 0 2 ( <1) 0 2 ( <1) Probable 0 0 0 0 0 0 0 Epistaxis 2 ( 1) 3 ( 3) 1 ( 1) 0 6 ( 1) 2 ( 1) 8 ( 1) Possible 0 0 0 0 0 1 ( 1) 1 ( <1) Probable 0 0 0 0 0 0 0 Gastrointestinal hemorrhage
0 0 0 1 ( 3) 1 ( <1) 1 ( 1) 2 ( <1)
Possible 0 0 0 1 ( 3) 1 ( <1) 0 1 ( <1) Probable 0 0 0 0 0 0 0 Hematoma 22 ( 11) 12 ( 10) 6 ( 5) 5 ( 13) 45 ( 10) 5 ( 3) 50 ( 8) Possible 10 ( 5) 6 ( 5) 5 ( 4) 1 ( 3) 22 ( 5) 1 ( 1) 23 ( 4) Probable 3 ( 2) 0 0 1 ( 3) 4 ( 1) 1 ( 1) 5 ( 1) Hemorrhage 7 ( 4) 3 ( 3) 6 ( 5) 6 ( 15) 22 ( 5) 7 ( 4) 29 ( 5) Possible 2 ( 1) 0 2 ( 2) 2 ( 5) 6 ( 1) 1 ( 1) 7 ( 1) Probable 1 ( 1) 0 1 ( 1) 1 ( 3) 3 ( 1) 0 3 ( <1) Hypotension 4 ( 2) 4 ( 3) 2 ( 2) 6 ( 15) 16 ( 3) 4 ( 2) 20 ( 3) Possible 0 0 1 ( 1) 0 1 ( <1) 0 1 ( <1) Probable 0 1 ( 1) 0 0 1 ( <1) 0 1 ( <1) Thrombosis 2 ( 1) 0 0 1 ( 3) 3 ( 1) 0 3 ( <1) Possible 2 ( 1) 0 0 0 2 ( <1) 0 2 ( <1) Probable 0 0 0 0 0 0 0 Vascular pseudo aneurysm
3 ( 2) 1 ( 1) 4 ( 4) 1 ( 3) 9 ( 2) 1 ( 1) 10 ( 2)
Possible 1 ( 1) 0 2 ( 2) 1 ( 3) 4 ( 1) 0 4 ( 1) Probable 0 0 0 0 0 1 ( 1) 1 ( <1)

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 91 of 105 CONFIDENTIAL
The majority of adverse events were related to the endpoints of the study (bleeding, coronary ischemia – see Section 4.1.6) and cardiac catheterization procedure (vascular injury at puncture site). Consistent with the primary endpoint, the REG1 25% reversal group had a numerically higher rate of bleeding endpoints (65%). All other REG1 reversal arms had a similar rate of all adverse events and non-endpoint related adverse events as compared to the heparin group.
No significant study medication related changes were found in platelet, renal function or liver function studies. One subject in the REG1 group received dialysis after CABG; two subjects in the REG1 group had an elevated creatinine after catheterization. All three events were considered not to be related to REG1 and were attributed to complications of the procedures.
No non-serious adverse events led to discontinuation of study drug in CLIN211.
Three subjects in the REG1-CLIN211 study experienced severe allergic SAEs after dosing of pegnivacogin which are described below in the SAE Section 4.5.5.2
4.5.5. Serious Adverse Events
4.5.5.1. Serious Adverse Events - Phase 1
One SAE was reported in REG1-CLIN101. A 38-year-old female with no reported significant medical history, experienced an SAE of encephalopathy. The subject received a single administration of study drug (pegnivacogin, 30mg – low-intermediate dose group) and per protocol, placebo control agent, 5 ml, was given.
The subject experienced a transient encephalopathy characterized by speech impairment (Grade 2), mood alteration/agitation (Grade 1), confusion (Grade 1) and right eye droop (Grade 1). In response, anivamersen 30 mg (half the protocol-specified rescue dose) was given. The subject's symptoms were noted to have resolved completely within 30 minutes of receiving the anivamersen dose. An emergent head CT was negative. A neurology consult revealed a normal physical examination. The subject admitted to a recent history of smoking crack cocaine (approximately 2 months prior). This history was not disclosed during the initial exam prior to study enrollment and would have excluded the subject from the study. Urine toxicity was negative. Laboratory evaluations were not clinically significant. The subject was discharged in stable condition. The study physician assessed the causal relationship between pegnivacogin administration and the serious adverse event as “possible.”
4.5.5.2. Serious Adverse Events Phase 2
REG1-CLIN210:
One subject in CLIN210 who received the REG1 system experienced an SAE of unstable angina. The SAE had an onset time of 5.7 days after pegnivacogin administration and was judged severe. Of note, repeat coronary angiography demonstrated no evidence of complications or thrombosis at the stented site. After intravascular ultrasound evaluation, a

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 92 of 105 CONFIDENTIAL
stent was placed in a proximal lesion that was initially deemed to be non-significant. The SAE was determined to be not related to study drug
REG1-CLIN211:
Among patients treated in REG1-CLIN211, rates of serious adverse events for the REG1 (total) was 15%, while the heparin group showed a rate of 11%. The majority of the events were related to study endpoints (bleeding and ischemic events). All but three were not reported to be study drug related. Three cases of cardiac arrest
4.5.5.3. Severe Allergic SAEs
were reported but considered as “not related” to study drug; all were catheter induced arrhythmias that occurred during cardiac catheterization. One case of renal failure was reported and also considered to be “not related” to study drug by the investigators, as the one case was post-CABG.
Three subjects in the REG1-CLIN211 study experienced severe allergic SAEs considered to be related to study drug shortly after dosing of pegnivacogin (3-20 minutes) which are described below. All three SAEs occurred during the period from October 1, 2010 until November 10, 2010 (the 14th
A 71 year old female complained of general malaise, nausea, headache, skin pruritus over the whole body five minutes after administration of pegnivacogin. Shortly thereafter she developed severe anaphylactic shock with shortness of breath, hypotension (50/0 mm Hg), sweating, pale skin, and bronchial obstruction during lung auscultation was recorded. The patient did not suffer from swelling of face, body, throat or larynx. Due to safety reasons the patient was not administered anivamersen. The patient’s general condition gradually improved. The patient received a total of 2.5 L fluids intravenously during several hours. The event was considered resolved after 6 hours. The patient was conscious and hemodynamically stable (blood pressure 110/65 mmHg; heart rate 73 beats/min), without dyspnea and bronchial obstruction. All supportive medications were discontinued prior to time of recovery. The subject was discharged in stable condition.
month of enrollment after enrollment of 439 subjects). Two of these occurred in Germany and 1 in Poland, all three subjects were female. These three subjects did not receive anivamersen.
A 44 year old female experienced the adverse event of severe allergic reaction approximately twenty (20) minutes after receiving a single intravenous dose of pegnivacogin which required treatment with IV Prednisolone, Clemastin and Ranitidine. Symptoms included urticaria and flushing, the latter of which was restricted to the skin and most prominent on the face, neck and chest (but also on the rest of the body surface, including arms and legs). There was no swelling of the throat, mouth, or any other area. Furthermore, no respiratory insufficiency was reported, nor were any other signs or symptoms reported. There were no hemodynamic changes, no hypotension or change in heart rate reported by the investigator. The event resolved at that day, approximately 25 minutes following treatment. The subject was discharged in stable condition without any further reactions.
A 68 year-old female experienced the adverse event of anaphylactic shock approximately three (3) minutes after receiving a single intravenous dose of pegnivacogin. Initial onset consisted of tingling in the chest and agitation, followed by severe dyspnea, reddening of the

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 93 of 105 CONFIDENTIAL
entire body (especially of the extremities), and sinus tachycardia. Initial treatment included intravenous Fenistil, Tagamet and Solu-Decortin, followed by Atrovent, Sultanol and Suprarenin (adrenaline) for inhalation. Approximately two (2) minutes following the latter treatment, the patient experienced supraventricular tachycardia that degraded to wide complex tachycardia requiring cardiopulmonary resuscitation which resulted in restoration of independent breathing, peripheral pulses and spontaneous motor function; however, due to persistent respiratory insufficiency, prophylactic intubation was performed and the subject transferred to the ICU. There was no excessive swelling of the tongue observed during intubation. The subject did not receive planned reversal with Anivamersen and therefore remained anticoagulated. Within 24 hours of dosing, the patient experienced diffuse bleeding from the nose, mouth and lungs, resulting in a drop of hemoglobin requiring treatment with IV Prothromplex and complete resolution of bleeding approximately 1- 2 days later. On the same day the bleeding stopped, the subject was extubated with adequate neurological function. Two days following extubation, the subject was transferred to the intermediate care unit and remained there for three days before being transferred to the general ward. The cardiac catheterization, which had been postponed due to the event, was performed during her stay at the Intensive Care Unit without any complications. The catheterization was performed uneventfully. The patient was discharged from the hospital after 6 days in the general ward in stable condition with resolution of the reaction and stable condition.
In summary, there were 3 severe allergic SAEs that occurred clustered late in the study in 3 female subjects in Europe temporally related shortly after treatment with pegnivacogin (3-20 minutes). Two of the three reactions were anaphylactoid in nature with cutaneous, respiratory and hemodynamic manifestations. The third reaction was limited to cutaneous manifestations with no other organ system involvement and the subject did not exhibit an anaphylactoid presentation. All resolved after treatment without sequelae.
4.5.5.3.1. Retrospective Review of Adverse Events for Allergy Signals
All studies where REG1 was administered were reviewed in detail using the MEDRA coded AE terms. All subjects who met criteria for review had all case report forms reviewed in detail including physical examination, vital signs, concomitant treatments, adverse event reporting and laboratory assessments. All terms included in the NIAID (National Institute of Allergy and Infectious Diseases) and AAAAI (American Academy of Allergy, Asthma, and Immunology) guidance documents on anaphylactic definitions and drug allergy practice parameters were included in this search. (Sampson et. al., 2005) (Solensky et. al., 2010).
A cut-off of 2 hours was used to define and further delineate terms that met the search criteria as “possibly related events.” This cut-off was based upon the conclusion that relevant allergic reactions would occur within 1 hr of pegnivacogin administration, which was arrived at after consideration of the timing of the onset of the severe allergic SAEs in REG1-CLIN211 coupled to the fact that maximal plasma concentrations of pegnivacogin are obtained 1-10 minutes after bolus IV administration.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 94 of 105 CONFIDENTIAL
Phase 1 and 2a:
A full review of all adverse events in the three Phase 1 and one Phase 2a studies was reviewed as noted above. There were a total of 4 adverse events which met the criteria for retrospective database review. In considering temporal relationship to dosing, constellation and description of signs and symptoms, concomitant laboratory analysis, concomitant vital signs and physical exam, and the lack of reproduction of symptoms after re-challenge with the REG1 system it appears there is one possible allergic reaction in these studies (in the REG1-CLIN102 study). This was an episode of erythema of the neck and face associated with nausea and vomiting and transient blurred vision in the right eye with onset of 15 minutes after dosing of pegnivacogin in a female subject. This episode was considered mild in severity resolved spontaneously without treatment after 14 minutes without a BP change, respiratory symptoms or urticaria.
All subjects in the Phase 1 program were domiciled for at least 24 hours (REG1-CLIN103 for 7 days) and followed by medical staff during the domicile period, including vital signs and brief physical exam. All subjects in the Phase 2a study were hospitalized for a minimum of 24 hours or more after dosing, dependent on standard of care after PCI at that institution. In Phase 1 and 2a, there were no changes in physical exams, vital signs or laboratory abnormalities suggestive of a hypersensitivity reaction. Every subject in the Phase 1 program was tested and had no change in their complement Bb split products.
Phase 2b:
In the ACS Phase 2b study (CLIN211), three subjects experienced severe allergic SAEs considered to be related to study drug after dosing of pegnivacogin. These 3 events are described in detail above in Section 4.5.5.3 .
A retrospective analysis of adverse events within 24 hours of dosing in the Phase 2b REG1-CLIN211 study showed, when excluding the 3 severe allergic SAEs, that no correlation was observed for these AEs of interest when comparing the REG1 treated subjects and the heparin treated subjects. Hypotension and dyspnea were the most frequently reported AEs during this period, with most considered of mild or moderate severity and not related to study drug and showing no difference from the heparin group.
Three subjects in the REG1-CLIN211 study had adverse events that led to further investigation. Two of these met a description of events consistent with a potential allergic reaction. One subject had symptoms of redness of the hands with itching but no hives or rash 12 minutes after receiving pegnivacogin and also shortly after starting IV Levaquin. An additional subject had hypotension and bradycardia at the end of cardiac catheterization with hives at a later time after resolution of the hemodynamic symptoms. This event was more closely temporally related to the cardiac catheterization, administration of contrast dye and Integrilin than pegnivacogin administration and is less likely to be related to pegnivacogin due to the timing and interceding therapies and procedures.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 95 of 105 CONFIDENTIAL
In summary, in addition to the 3 subjects with severe allergic SAEs there were two other subjects in the entire REG1 clinical development program with adverse events consistent with possible milder allergic reactions. Including the 3 severe allergic SAEs in REG1-CLIN211, there were a total of 5 (0.8%) potential allergic reactions out of 633 exposed subjects in the REG1 development program, with 3 of these being deemed serious (the 3 severe allergic SAEs in REG1-CLIN211) (0.5%) and 2 (0.3%) anaphylatic reactions (2 of 3 the severe allergic SAEs in REG1-CLIN211).
4.5.6. Reference Safety Information
Bleeding events and related terms are considered expected events with all anticoagulant agents, and were collected specifically as efficacy in the REG1-CLIN210 and REG1-CLIN211 studies. For the purpose of future studies, all bleeding events and related terms will be considered as expected adverse events for reporting purposes. Non-bleeding drug related AEs occurring in >1 REG1 subjects are summarized in Table 22 by frequency and severity. For future studies, all events listed in Table 22 will be considered as expected adverse events for reporting purposes.
Table 22: Summary of Non Bleeding, Drug Related Adverse Events Occurring in >1 REG1 Subjects (by Frequency and Severity)
Adverse Event Term System Organ Class REG1 Combined (n = 623)
Severity
Chest Discomfort or pain General Disorders and Administrative Site Conditions
3 (<1%) 2 Mild 1 Moderate
Angina Pectoris Cardiac Disorders 1 (<1%) Moderate
Post Procedural Swelling Injury, Poisoning, and Procedural Complications
1 (<1%) Mild
Contusion Injury, Poisoning, and Procedural Complications
4 (<1%) Mild
Encephalopathy Neurological Disorders 1 (<1%) Severe
Nausea and vomiting Gastrointestinal Disorders 2 (<1%) Mild
Blurred vision Neurological Disorders 1 (<1%) Mild
Erythema Skin and Subcutaneous Tissue Disorders
2 (<1%) Mild
Phlebitis Vascular Disorders 1 (<1%) Mild
Fatigue General Disorders and Administrative Site Conditions
2 (<1%) Mild
Abdominal pain Gastrointestinal Disorders 2 (<1%) 1 Mild 1 Moderate
Pruritus Skin and Subcutaneous Tissue Disorders
2 (<1%) Mild
Headache Nervous System Disorders 2 (<1%) Mild
Anaphylactic shock Immune System Disorders 2 (<1%) Severe
Hypersensivity reaction Immune System Disorders 1 (<1%) Severe
Urticaria Immune System Disorders 1 (<1%) Moderate

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 96 of 105 CONFIDENTIAL
Adverse Event Term System Organ Class REG1 Combined (n = 623)
Severity
Groin Pain Musculoskeletal and Connective Tissue Disorders
1 (<1%) Mild
Paresthesias Nervous System Disorders 1 (<1%) Mild
Dyspnea Respiratory, Thoracic and Mediastinal Disorders
1 (<1%) Mild
Hypotension Vascular Disorders 2 (<1%) Moderate
Thrombosis Vascular Disorders 3 (<1%) 2 Mild 1 Moderate
Eosinophilia Blood and Lymphatic Disorders 4 (<1%) 3 Mild 1 Moderate
Vascular pseudoaneurysm Vascular Disorders 4 (<1%) 1 Mild 2 Moderate
1 Severe
Bradycardia Cardiac Disorders 1 (<1%) Moderate
Myocardial infarction Cardiac Disorders 1 (<1%) Mild
Erysipelas Infections and Infestations 1 (<1%) Mild
Blood creatinine increase Investigations 1 (<1%) Mild
Blood creatinine kinase increase
Investigations 1 (<1%) Moderate
4.6. Summary and Conclusions from Clinical Studies The present paradigm both for anticoagulant use and for continued antithrombotic drug development is to establish a balance between efficacy (reducing the risk of ischemic events) and safety (minimizing the risk of bleeding) (Harrington et. al., 2004). Generally, cardiovascular clinicians have been willing to trade off an increased risk of bleeding when a drug can reduce the ischemic complications of either the acute coronary syndromes or of coronary revascularization procedures. Despite the continued development of novel antithrombotics, a significant clinical need exists for safer and more effective anticoagulants. The ideal parenteral anticoagulant would be deliverable by intravenous (IV) or subcutaneous injection, immediately effective, easily dosed so as not to require frequent monitoring, and immediately and predictably reversible.
The REG1 Anticoagulation System is a two component system. The active drug component (pegnivacogin) elicits an anticoagulant effect by blocking the Factor VIIIa (FVIIIa)/Factor IXa (FIXa)-catalyzed conversion of Factor X (FX) to Factor Xa (FXa). Pegnivacogin is rapidly neutralized by its active control agent, anivamersen.
Three Phase 1 and three Phase 2 studies have been conducted using the REG1 Anticoagulation System.
A total of 123 normal volunteers have received REG1 or its components in Phase 1 studies (104 received either singles doses of pegnivacogin, anivamersen, or both; 19 received placebo), as have 49 volunteers with stable coronary artery disease (41 received single doses of pegnivacogin or pegnivacogin followed by anivamersen; 8 received placebo).

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 97 of 105 CONFIDENTIAL
In Phase 2 studies, 650 patients with stable CAD and acute coronary syndrome have been studied: 26 while undergoing coronary stent placement; 1 while undergoing OPCAB surgery and; 623 with coronary syndrome undergoing catheterization of which 387 had PCI.
The largest controlled study to-date was REG1-CLIN211 (RADAR) was a randomized, partially blinded, multi-center study to evaluate the safety and efficacy of the REG1 in Non-ST Elevation (NSTEMI) acute coronary syndrome (ACS) patients undergoing cardiac catheterization within 24 hours of randomization. The control agent was heparin (UFH or LMH). REG1 was administered in four groups – pegnivacogin 1.0 mg/kg with pegnivacogin dosed to produce 25%, 50%, 75% or 100% reversal. The data safety and monitoring board stopped the lowest-dose anivamersen arm (25% reversal) early on in the trial per protocol because of a high bleeding rate. In the three other arms, the rate of total ACUITY bleeding was similar to heparin, with a stepwise numerical reduction in major bleeding with higher doses of the reversal agent. In the overall REG1 population there was a numerically reduced rate of ischemic events (3.0% vs. 5.7% on heparin). Sheaths were removed an average of 24 minutes after the procedure in the REG1 patients vs. three hours in the heparin group. The 1.0 mg/kg dose of pegnivacogin was confirmed as causing near complete factor IX inhibition.
In summary, the REG1-CLIN 211 study in patients undergoing cardiac catheterization showed that the REG1 system can provide high levels of Factor IX inhibition with active control resulting in numerically lower numbers of major bleeding events and composite ischemic events both at 30 days and at hospital discharge. This provides the rationale for a potential benefit for patients to be investigated in future clinical morbidity/mortality Phase 3 trials.
There were three severe allergic SAEs in the CLIN211 study shortly after administration of pegnivacogin ranging from a mild dermal reaction to two patients with hypotension and respiratory symptoms. The study was placed on hold and terminated when it was determined that there was an adequate amount of completed subjects and events to make conclusions about the pre-defined endpoints. There were no other significant or drug-related SAEs across all studies except for study endpoints of bleeding and cardiac ischemic events.
No patterns or trends in AEs related to bleeding were observed across all studies (except bleeding endpoints in CLIN211) and the bleeding AEs were consistent and expected in any study with venipuncture or cardiac catheterization, in particular if an anticoagulant is being used. The following adverse events have been reported across all studies with the REG1 Anticoagulation System (including trials with placebo and heparin control), irrespective of causality or incidence relative to controls:
Abdominal pain, Access site bleeding, Aggression, Agitation, Angina pectoris, Anxiety, Arthralgia, Atelectasis, Atrial fibrillation, Back pain, Bradycardia, Catheter site hemorrhage, Catheter thrombosis, Chest pain/discomfort, Chills, Coagulopathy, Coagulation time prolonged, Confusional state, Contact dermatitis, Contusion, Drug intolerance, Dizziness, Dysgeusia, Dyspnoea, Ecchymosis, Eosinophilia, Electrocardiogram ST segment elevation, Epistaxis, Fatigue, Feeling cold, Gastro intestinal hemorrhage, Gingival bleeding, Graft thrombosis, Groin ecchymosis, Groin pain, Headache, Hematoma, Hemorrhage,

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 98 of 105 CONFIDENTIAL
Hypoglycemia, Hypotension, Lung infiltration, Musculoskeletal discomfort, Myocardial infarction, Nausea, Oropharyngeal blistering, Paraesthesia, Pleural effusion, Post procedural swelling, Pruritis, Rectal Hemorrhage, Speech disorder, Thrombosis, Urinary retention, Vascular pseudo aneurysm, Vessel puncture site hematoma, Vessel puncture site hemorrhage, Vomiting, Wheezing.
In aggregate across the studies completed, there were a few sporadic changes in vital signs and laboratory data; however, there were no patterns of clinically significant changes nor trends indicating an adverse effect of REG1 on laboratory values except for the anticipated changes in measures of coagulation.
In summary, the clinical results to-date suggests that the REG1 Anticoagulation System may offer an alternative to present agents used for cardiovascular procedures. The potential for allergic reactions remains unexplained and must be considered a major Warning/Precaution when using REG1.
4.7. Marketing Experience The REG1 Anticoagulation System is not approved for marketing in any country.
4.8. Section 4 References Bolliger D, Szlam F, Molinaro RJ, Escobar MA, Levy JH, Tanaka KA. Thrombin generation and fibrinolysis in anti-FIXa aptamer treated blood and plasma spiked with factor VIII inhibitor bypassing activity or recombinant factor VIIa. Haemophilia 2010; 16:510-517.
Bolton-Maggs P H and Pasi K J. Haemophilias A and B. Lancet 2003; 361:1801-1809.
Butenas S, Brummel K E, Bouchard BA and Mann K G. How factor VIIa works in hemophilia. J Thromb Haemost 2003; 1:158-1160.
Chan MY, Cohen MG, et. al. Phase 1b Randomized Study of Antidote-Controlled Modulation of Factor IXa Activity in Patients With Stable Coronary Artery Disease. Circulation 2008; 117:2865-2874.
Chan MY, Rusconi CP, et. al. A randomized, repeat-dose, pharmacodynamic and safety study of an antidote-controlled factor IXa inhibitor. J Thromb Haemost 2008; 6:789-796.
Cohen MG, Purdy DA, et. al. First clinical application of an actively reversible direct factor IXa inhibitor as an anticoagulation strategy in patients undergoing percutaneous coronary intervention. Circulation 2010; 122(6):614-22.
Dyke CK, Steinhubl SR, Kleiman NS, Cannon RO, Aberle LG, Lin M, et al. First-in-human experience of an antidote-controlled anticoagulant using RNA aptamer technology. A phase 1a pharmacodynamic evaluation of a drug-antidote pair for the controlled regulation of factor IXa activity. Circulation 2006; 114: 2490-2497.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 99 of 105 CONFIDENTIAL
Harrington RA, Becker RC, et. al. Antithrombotic therapy for coronary artery disease: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest
Mann, K G, Brummel, K, and Butenas, S. What is all that thrombin for? J Thromb Haemost 2003; 1: 1504-1514.
2004; 126(3 Suppl):513S-548S.
Povsic TJ, et. al. A Phase 2, randomized, partially blinded, active-controlled study assessing the efficacy and safety of variable anticoagulation reversal using the REG1 system in patients with acute coronary syndromes: results of the RADAR trial. European Heart Journal (2013) 34, 2481–2489.
Sampson, HA, Munoz-Furlong A, Bock A, et. al. Symposium on the Definition and Management of Anaphylaxis: Summary Report. Journal of Allergy and Clinical Immunology 2005; 115:584-91.
Szlam F, Luan D, Bolliger D, Szlam AD, Levy JH, Varner JD, Tanaka KA. Anti-FIXa aptamer reduces propagation of thrombin generation in plasma anticoagulated with warfarin. Thromb Res. 2010; 125: 432-437.
Solensky R, Khan DA. Et. al., Drug Allergy: An Updated Practice Parameter. Annals of Allergy, Asthma & Immunology 2010; 105:273.e1-e78.
Tanaka KA, Szlam F, Rusconi, CP, Levi JH. In-Vitro evaluation of anti factor IXa aptamer on thrombin generation, clotting time, and viscoelastometry. J Thromb Haemost 2009; 7(5):827-33.
Povsic TJ, Cohen MG, Mehran R, et. al. A randomized, partially blinded, multicenter, active-controlled, dose-ranging study assessing the safety, efficacy, and pharmacodynamics of the REG1 anticoagulation system in patients with acute coronary syndromes: Design and rationale of the RADAR Phase IIb trial. AHJ 2011; 161:261-268.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 100 of 105 CONFIDENTIAL
5. SUMMARY OF DATA AND GUIDANCE FOR THE INVESTIGATOR
5.1. Indications and Usage The REG1 Anticoagulation System is under development as a reversible anticoagulant in coronary revascularization procedures to treat coronary and peripheral artery disease, as a reversible anticoagulant for use in patients suffering from acute coronary syndromes, and potentially as an anticoagulant for other indications in which it would be advantageous for the physician to have direct control of the agent employed for anticoagulant or antithrombotic therapy.
5.2. Dosage and Administration Both the pegnivacogin Injection and anivamersen Injection components of the REG1 Anticoagulation System may be used as supplied but may be diluted (if necessary) in Sterile Saline Injection (USP) to a target concentration that will deliver the desired dose.
5.3. Dosage Forms and Strengths The recommended dosage of pegnivacogin is 1.0 mg/kg for ACS/PCI followed by the reversal agent anivamersen at a dose that results in > 50% reversal of pegnivacogin.
5.4. Contraindications The REG1 Anticoagulation System is contraindicated in patients with active major bleeding known coagulopathy or known sensitivity to the components of the REG1 System.
5.5. Warnings/Precautions The REG1 Anticoagulation System is not intended for intramuscular injection.
The REG1 Anticoagulation System should be used with caution in patients with disease states associated with an increased risk of bleeding.
Excess bleeding was observed in patients receiving anivamersen at the 25% reversal rate (0.075 mg/kg). Anivamersen should not be used at < 50% (0.2 mg/kg) reversal of pegnivacogin 1mg/kg in patients undergoing cardiac procedures.
Allergic reactions (some serious) including anaphylactic reactions have been reported with use of pegnivacogin. Precautions should be taken for the treatment of anaphylactic reactions within the first hour after pegnivacogin administration including having facilities and treatment to provide respiratory and hemodynamic support. Patients should be monitored for allergic reactions for 1 hour following pegnivacogin administration.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 101 of 105 CONFIDENTIAL
The REG1 Anticoagulation system has not been extensively studied
Currently, no clinical studies for REG1 are planned in children.
in embryo-fetal developmental toxicology. Until additional reproductive toxicology data becomes available, women of childbearing potential who are participating in clinical studies will be required to use two means of birth control. Similarly, male participants are recommended to take contraceptive precautions.
5.6. Adverse Events There were three severe allergic reactions shortly after administration of pegnivacogin ranging from a mild dermal reaction to two patients with hypotension and respiratory symptoms. The events occurred 3-20 minutes after the administration of pegnivacogin. There were no other significant or drug-related SAEs across all studies except for study endpoints of bleeding and cardiac ischemic events.
No patterns or trends in AEs related to bleeding were observed across all studies (except bleeding endpoints in REG1-CLIN211) and the bleeding AEs were consistent and expected in any study with venipuncture or cardiac catheterization, in particular if an anticoagulant is being used. Excess bleeding was observed when anivamersen was used at < 50% (0.2 mg/kg) reversal doses of pegnivacogin 1mg/kg..
The following adverse events have been reported across all studies with the REG1 Anticoagulation System (including trials with placebo and heparin control), irrespective of causality or incidence relative to controls:
Abdominal pain, Access site bleeding, Aggression, Agitation, Angina pectoris, Anxiety, Arthralgia, Atelectasis, Atrial fibrillation, Back pain, Bradycardia, Catheter site hemorrhage, Catheter thrombosis, Chest pain/discomfort, Chills, Coagulopathy, Coagulation time prolonged, Confusional state, Contact dermatitis, Contusion, Drug intolerance, Dizziness, Dysgeusia, Dyspnoea, Ecchymosis, Eosinophilia, Electrocardiogram ST segment elevation, Epistaxis, Fatigue, Feeling cold, Gastro intestinal hemorrhage, Gingival bleeding, Graft thrombosis, Groin ecchymosis, Groin pain, Headache, Hematoma, Hemorrhage, Hypoglycemia, Hypotension, Lung infiltration, Musculoskeletal discomfort, Myocardial infarction, Nausea, Oropharyngeal blistering, Paraesthesia, Pleural effusion, Post procedural swelling, Pruritis, Rectal Hemorrhage, Speech disorder, Thrombosis, Urinary retention, Vascular pseudo aneurysm, Vessel puncture site hematoma, Vessel puncture site hemorrhage, Vomiting, Wheezing.
In aggregate across the studies completed, there were a few sporadic changes in vital signs and laboratory data; however, there were neither patterns of clinically significant changes nor trends indicating an adverse effect of REG1 on laboratory values except for the anticipated changes in measures of coagulation.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 102 of 105 CONFIDENTIAL
5.7. Drug Interactions The REG1 Anticoagulation System has been tested in 3 studies in which patients received concomitant oral antiplatelet therapy. In a study in patients with stable coronary artery disease on REG1, patients received aspirin (>80 mg/day) and/or clopidogrel (≥75 mg/day) or both. In a study of patients undergoing elective PCI on REG1, patients received loading doses of aspirin (250-500 mgs) and clopidogrel (600 mgs if clopidogrel naïve; 300 mg if already on clopidogrel). In a study in patients with ACS, patients received loading doses of aspirin and Clopidogrel or Prasugrel. Subjects with ACS also received doses of REG1 after receiving unfractionated heparin with no change in PK parameters of pegnivacogin. No apparent interactions between the REG1 System and these medications have been observed.
The interaction of pegnivacogin with other anticoagulant and procoagulant agents has been evaluated in vitro using both the aPTT and CAT assays to evaluate the effect of combining these agents.
Pegnivacogin interactions with heparin, LMWH (lepirudin) were tested using aPTT and thrombin generation and demonstrated additive effects on both measurements in vitro. This can be found in section 4.3.2.
The interaction of pegnivacogin with warfarin showed no additional effects on INR but additive effets can be seen on thrombin generation with warfarin at higher doses. This can be found in section 4.3.2.
Addition of rFVIIa has a minimal impact on the inhibition of thrombin generation by pegnivacogin. The observed effect of rFVIIa on pegnivacogin inhibition of thrombin is consistent with the model of coagulation in which TF/FVIIa produces limited FXa during initiation to yield a small amount of thrombin, and in which the majority of thrombin generation is driven by FVIIIa/FIXa in the propagation phase. In contrast, addition of aPCC to plasma anticoagulated with pegnivacogin largely restores thrombin generation, presumably by increasing the plasma concentration of Factors VII, IX, X and prothrombin and by the addition of trace levels of FVIIa and FXa. Comparable results were obtained using aPTT and thromboelastometry as the read-outs. A full description can be found in Section 4.3.2.
No interactions were seen between REG1 and the CYP450 system.
No other data on drug interactions in clinical studies are currently available.
5.8. Use in Specific Populations One Phase 1 study and two Phase 2 studies support the use of the REG1 Anticoagulation System in subjects with stable CAD, acute coronary syndrome and elective PCI receiving all standard background therapies including oral antiplatelet therapy (aspirin or clopidogrel or prasugrel). The usage in special populations has also been supported; studies to-date have included >70% of patients who were greater than 70 years old and the female population was >33%. About 30 % of the population in the ACS study were diabetic. Approximately 9% of the population in the ACS study had renal insufficiency.

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 103 of 105 CONFIDENTIAL
The safety and effectiveness of the REG1 Anticoagulation System in other populations has not been established.
5.9. Drug Abuse and Dependence No data on drug abuse and dependence are available to date.
5.10. Overdosage In case of overdosage of the pegnivacogin Injection, a 1:1 weight:weight dose of Anivamersen should be administered.
5.11. Description The REG1 Anticoagulation System consists of a highly potent oligonucleotide-based aptamer against coagulation Factor IXa and a control agent that can hybridize to the aptamer, via Watson-Crick base pairing, and neutralize its activity. The drug component (pegnivacogin) is a modified RNA aptamer, 31 nucleotides in length. The nucleic acid portion of the aptamer is conjugated to a 40-kilodalton PEG carrier to increase its blood half-life and permit administration of a single IV dose to maintain anticoagulation over an extended period of time. The control agent component (anivamersen) is a 2′-O-methyl RNA oligonucleotide, 15 nucleotides in length, which is complementary to a portion of the REG1 drug component. The structures of pegnivacogin and anivamersen are shown in Figure 25
Figure 25: The REG1 Anticoagulation System
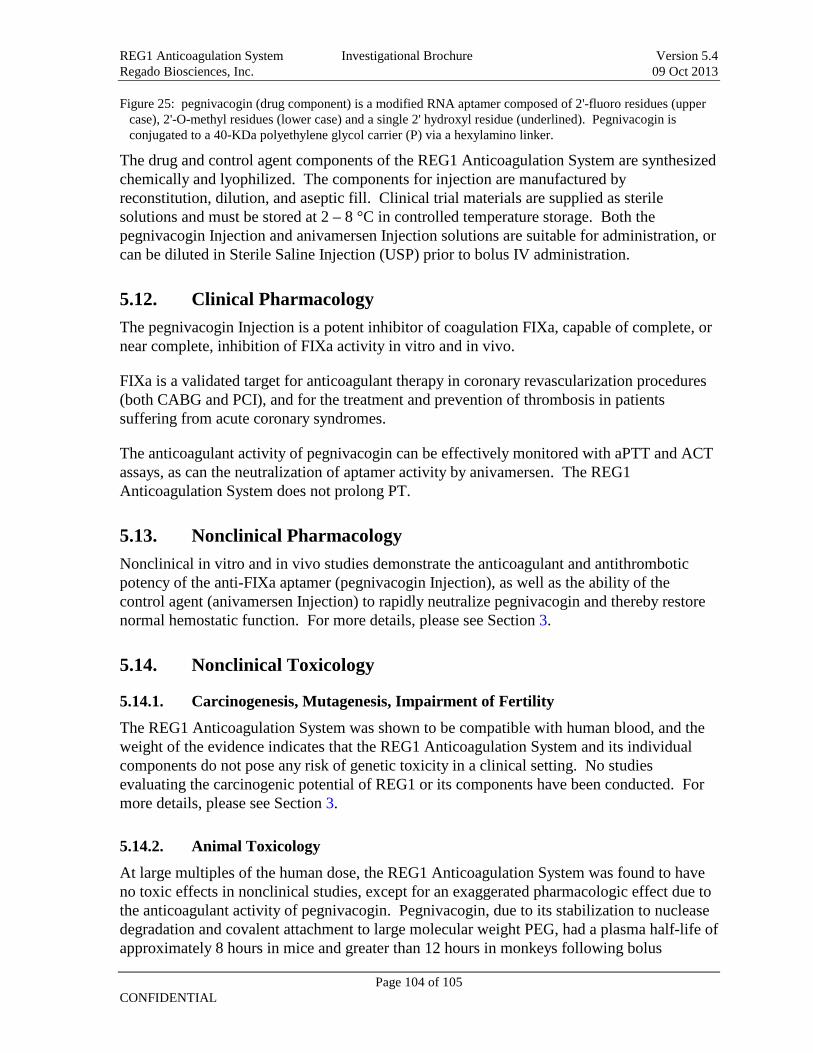
REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 104 of 105 CONFIDENTIAL
Figure 25: pegnivacogin (drug component) is a modified RNA aptamer composed of 2'-fluoro residues (upper case), 2'-O-methyl residues (lower case) and a single 2' hydroxyl residue (underlined). Pegnivacogin is conjugated to a 40-KDa polyethylene glycol carrier (P) via a hexylamino linker.
The drug and control agent components of the REG1 Anticoagulation System are synthesized chemically and lyophilized. The components for injection are manufactured by reconstitution, dilution, and aseptic fill. Clinical trial materials are supplied as sterile solutions and must be stored at 2 – 8 °C in controlled temperature storage. Both the pegnivacogin Injection and anivamersen Injection solutions are suitable for administration, or can be diluted in Sterile Saline Injection (USP) prior to bolus IV administration.
5.12. Clinical Pharmacology The pegnivacogin Injection is a potent inhibitor of coagulation FIXa, capable of complete, or near complete, inhibition of FIXa activity in vitro and in vivo.
FIXa is a validated target for anticoagulant therapy in coronary revascularization procedures (both CABG and PCI), and for the treatment and prevention of thrombosis in patients suffering from acute coronary syndromes.
The anticoagulant activity of pegnivacogin can be effectively monitored with aPTT and ACT assays, as can the neutralization of aptamer activity by anivamersen. The REG1 Anticoagulation System does not prolong PT.
5.13. Nonclinical Pharmacology Nonclinical in vitro and in vivo studies demonstrate the anticoagulant and antithrombotic potency of the anti-FIXa aptamer (pegnivacogin Injection), as well as the ability of the control agent (anivamersen Injection) to rapidly neutralize pegnivacogin and thereby restore normal hemostatic function. For more details, please see Section 3.
5.14. Nonclinical Toxicology
5.14.1. Carcinogenesis, Mutagenesis, Impairment of Fertility
The REG1 Anticoagulation System was shown to be compatible with human blood, and the weight of the evidence indicates that the REG1 Anticoagulation System and its individual components do not pose any risk of genetic toxicity in a clinical setting. No studies evaluating the carcinogenic potential of REG1 or its components have been conducted. For more details, please see Section 3.
5.14.2. Animal Toxicology
At large multiples of the human dose, the REG1 Anticoagulation System was found to have no toxic effects in nonclinical studies, except for an exaggerated pharmacologic effect due to the anticoagulant activity of pegnivacogin. Pegnivacogin, due to its stabilization to nuclease degradation and covalent attachment to large molecular weight PEG, had a plasma half-life of approximately 8 hours in mice and greater than 12 hours in monkeys following bolus

REG1 Anticoagulation System Investigational Brochure Version 5.4 Regado Biosciences, Inc. 09 Oct 2013
Page 105 of 105 CONFIDENTIAL
intravenous administration. Anivamersen rapidly disappeared from the circulation and was virtually non-detectable 15 minutes after dosing. The pegnivacogin /anivamersen complex, also due to the PEG covalently bound to pegnivacogin, was found in the circulation for as late as 21 hours following the anivamersen dose. For more details, please see Section 3.
5.15. Clinical Studies Regado has conducted a comprehensive Phase 1 program of REG1, and has completed one Phase 2a study investigating the feasibility of using REG1 to support the conduct of elective PCI. A second Phase 2a study investigating the feasibility of using REG1 to support the conduct of off-pump coronary artery bypass grafting was terminated. A third Phase 2b study, (CLIN211/RADAR) investigating using the REG1 System in patients with acute coronary syndrome undergoing cardiac catheterization confirmed earlier suggestive data that the REG1 system can provide high levels of Factor IX inhibition with active control resulting in numerically lower numbers of major bleeding events and composite ischemic events both at 30 days and at hospital discharge. These results provide the rationale for a potential benefit for patients to be investigated in future clinical morbidity/mortality Phase 3 trials. For more detail, please see Section 4.
5.16. How Supplied/Storage and Handling The pegnivacogin Injection and anivamersen Injection components of the REG1 Anticoagulation System are supplied as sterile solutions and must be stored at 2 – 8 °C in controlled temperature storage.
5.17. Patient Counseling Information Patients should be told to report any unusual signs of bleeding. Patients should report any signs or symptoms of an allergic reaction to their physician. These reactions are most likely to occur within minutes and up to 1 hour after dosing.
The risk of allergic reactions including severe allergic reactions (including anaphylactoid reactions) should be explained to patients.