investigating general liver disease/transaminitis
TRANSCRIPT
Investigating general liver
disease/transaminitis
Emmanuel A. Tsochatzis
Senior Clinical Lecturer and Consultant Hepatologist
UCL Institute of Liver and Digestive Health
Royal Free Hospital Institute for Liver and Digestive Health
BHIVA Autumn Conference
London 14 October 2016

Talk outline
Causes of transaminitis
How to investigate
NAFLD
Who needs referral to the hepatologist
Treatment

Liver disease in HIV infected patients
• Viral hepatitis
• Alcohol
• Drug toxicity
• NAFLD
• Infection
• Cancer/lymphoma
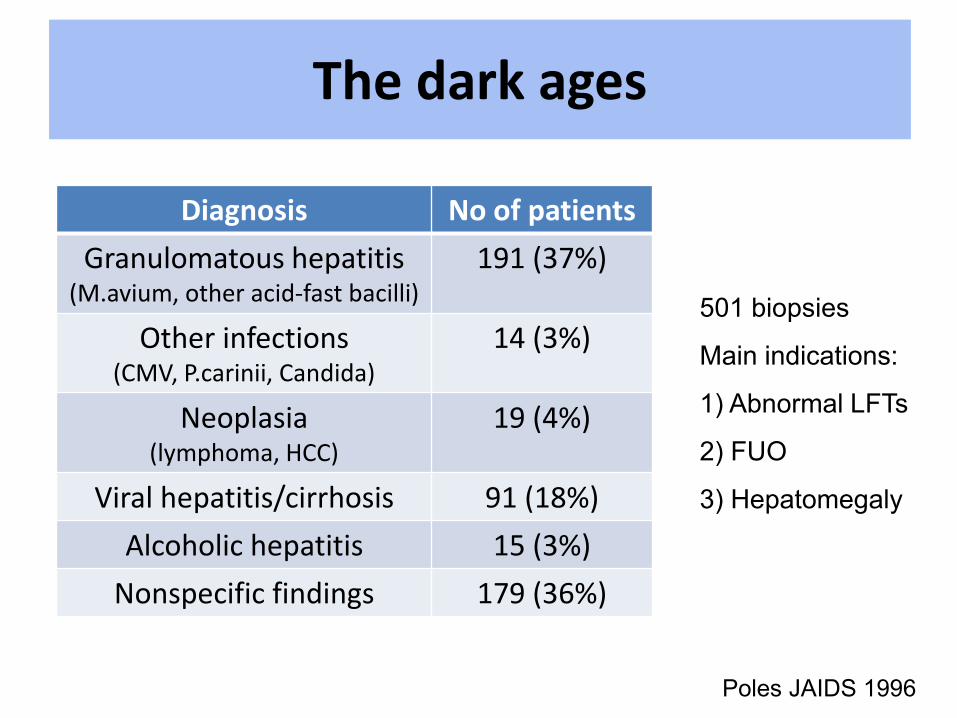
The dark ages
Diagnosis No of patients
Granulomatous hepatitis (M.avium, other acid-fast bacilli)
191 (37%)
Other infections (CMV, P.carinii, Candida)
14 (3%)
Neoplasia (lymphoma, HCC)
19 (4%)
Viral hepatitis/cirrhosis 91 (18%)
Alcoholic hepatitis 15 (3%)
Nonspecific findings 179 (36%)
501 biopsies
Main indications:
1) Abnormal LFTs
2) FUO
3) Hepatomegaly
Poles JAIDS 1996
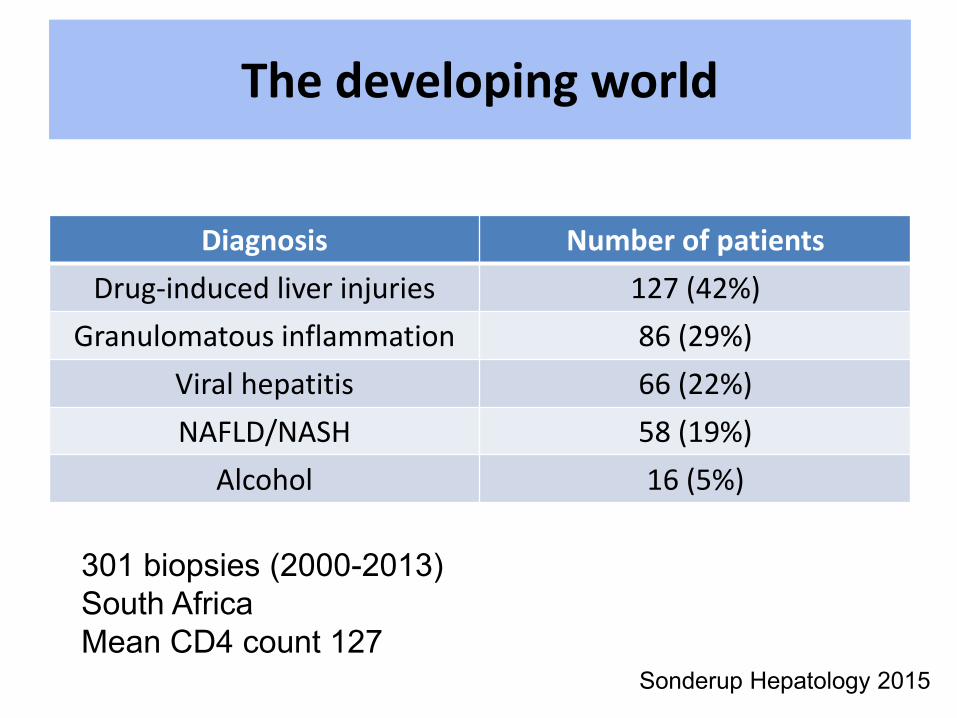
The developing world
Diagnosis Number of patients
Drug-induced liver injuries 127 (42%)
Granulomatous inflammation 86 (29%)
Viral hepatitis 66 (22%)
NAFLD/NASH 58 (19%)
Alcohol 16 (5%)
301 biopsies (2000-2013)
South Africa
Mean CD4 count 127 Sonderup Hepatology 2015
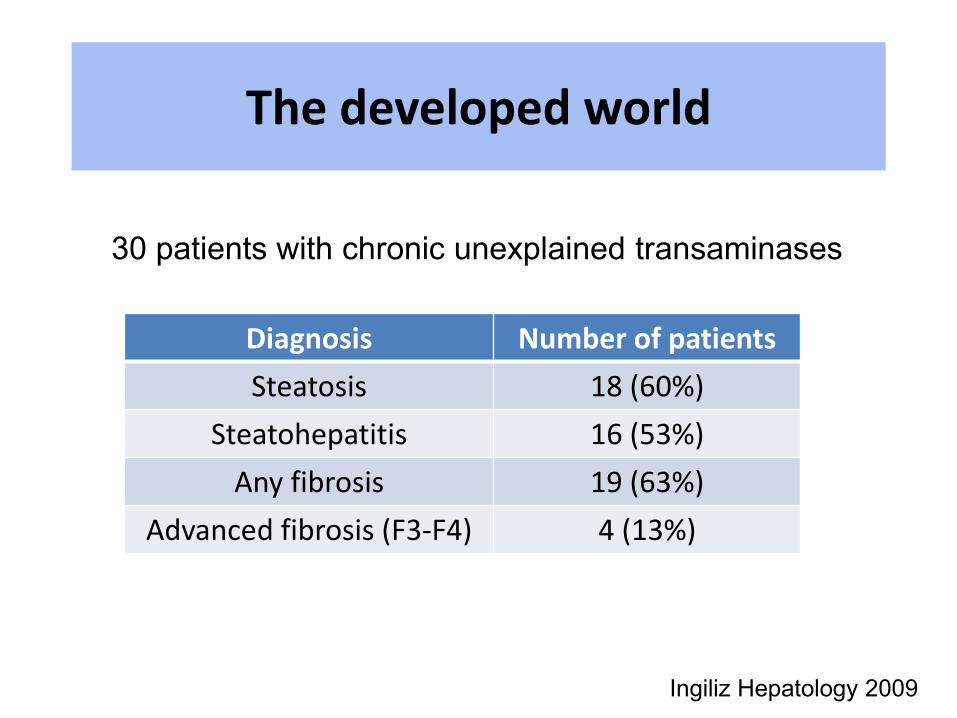
The developed world
Ingiliz Hepatology 2009
Diagnosis Number of patients
Steatosis 18 (60%)
Steatohepatitis 16 (53%)
Any fibrosis 19 (63%)
Advanced fibrosis (F3-F4) 4 (13%)
30 patients with chronic unexplained transaminases

• Retrospective analysis 2002-2015
• Patients with viral hepatitis co-infection excluded
• Demographics, indication for biopsy, stage of HIV
related disease documented.
• Steatosis, fibrosis and inflammation were recorded
• Definitive diagnoses were noted
Royal Free Hospital experience
Lever EASL 2015
Results
• A total of 143 biopsies were performed on a cohort
consisting of 4456 HIV positive individuals (2.8%)
• 75% males, mean age 49.6 years at biopsy
• Mean time between HIV diagnosis and biopsy was
8.1 years (range 0.1 years to 29 years)
• Abnormal LFTs main biopsy indication (70%)

Steatosis/inflammation
None
31%
Mild
26%
Moderate
14%
Severe
5%
Inadequate
sample
3%
Not
commented
21%
Steatosis (n=143)
Minimal
19%
Mild
33%
Moderate
10%
Marked
3%
None
22%
Not
documented
9%
Inadequate
sample
4%
Inflammation
(n=143)
69% had some degree of steatosis 43% at least minimal inflammation

Fibrosis and other diagnoses
None
65%
Mild
8%
Moderate
6%
Severe
2%
Cirrhosis
3%
Other
0%
Inadequate
sample
8%
Not
commented
on
8%
Fibrosis (n=143)
Cholestasis
11%
Granulomas
27%
Lymphoma
22%
Other
neoplasm
5%
AIH
8%
Drug
reaction
16%
Tuberculosis
11%
Other Diagnoses on
Liver Biopsy (n=37)
Some fibrosis in 20%, no fibrosis in 65%

Liver test abnormalities in patients
with HIV mono-infection
• Cross-sectional audit of consecutive HIV mono-infected patients
• Patients with persistently elevated LFTs in at least two
measurements six months apart
• 156/2398 (6.5%) persistently elevated transaminases
Lombardi EASL 2016, manuscript submitted

Abnormal LFTs in HIV mono-infection
• 97% on cART treatment
• US in 42%, of which 71% had steatosis
• APRI <0.5 n=81 (51.9%), >1.5 n=5 (3.2%)
• FIB4>1.45 in 33%, >3.25 in 4%
• TE only in 19 patients
• Liver biopsy NASH 13/20 patients, 1 with cirrhosis
Lombardi EASL 2016, manuscript submitted

A look for DDI hepatopathy
Refused bx
(n=5)
Normal Liver
(n=4)
Sampling frame
(n=376)
HBV/HCV co-infection
(84) or known DDI
related liver disease
(n=2) excluded
Bhagani S 2016

How to investigate transaminitis
• Drug history
• Alcohol history
• CD4 count
• Viral hepatitis markers
• Ferritin, transferrin saturation
• ANA, SMA, LKM, immunoglobulins
• Caeruloplasmin, a1-antithrypsin
• Liver ultrasound
• Non-invasive fibrosis assessment
(Fibroscan)

• Metabolic host-mediated (intrinsic and idiosyncratic)
• Hypersensitivity (early occurrence)
• Mitochondrial toxicity (prolonged exposure)
• Didanosine/stavudine more consistently associated
with advanced fibrosis
Drug toxicity
Soriano 2008; Blanco 2011; Mendeni 2011

What is NAFLD ?
Steatosis
Steatosis/inflammation Fibrosis Cirrhosis
Steatosis NASH Cirrhosis
• Non-Alcoholic Fatty Liver Disease
• Wide disease range from simple steatosis to cirrhosis
12-40% 15%

Non alcoholic fatty liver disease (NAFLD)
• Prevalence 20-25% of the general population
• Estimated 40-60% in patients with HIV
• 2-7% has steatohepatitis (NASH)
• Hepatic manifestation of metabolic syndrome
• >50% of secondary care referrals due to NAFLD

Kotronen, Arterioscler Thromb Vasc Biol 2008
NAFLD: Potential consequences

Epidemiology


Growing prevalence of obesity
Finucane Lancet 2011

Increasing prevalence of MS in HIV
33,347 patients – MS from 8.7% to 44.1% in 7 years
Worm AIDS 2010

Obesity in HIV patients
Crum-Cianflone 2010
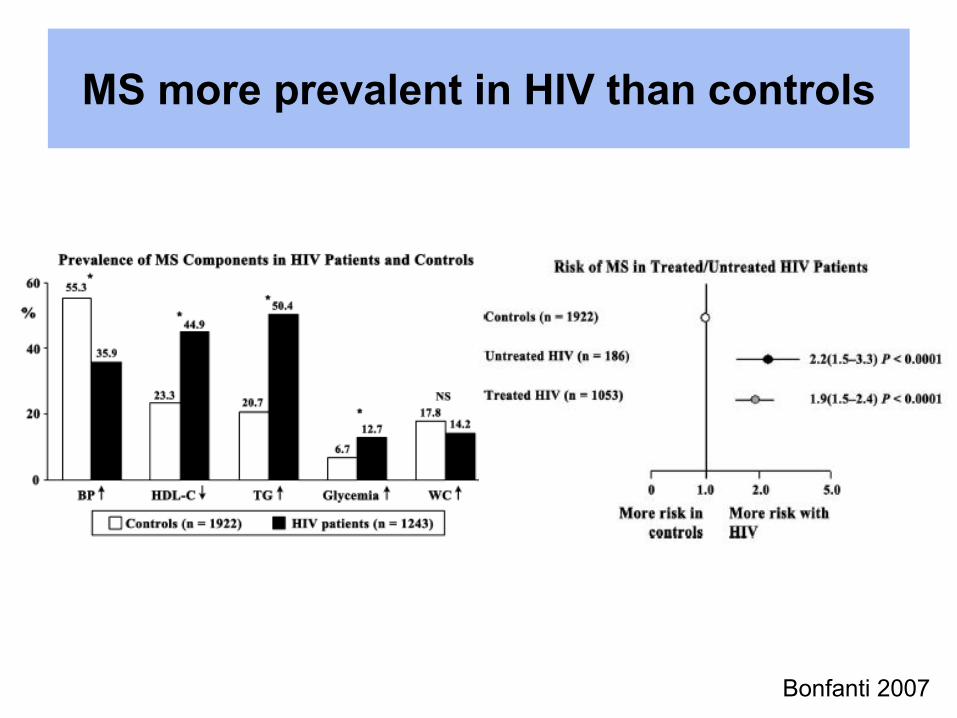
MS more prevalent in HIV than controls
Bonfanti 2007
NASH in HIV patients

1. HAART treatment
NRTIs, thymidine analogues (IR), didanosine
(mitochondrial toxicity)
2. Lipodystrophy
3. HIV virus
Mitochondrial damage, lipid levels
NASH in HIV patients

HAART
virus proteins
The Journal of Endocrinology and Metabolism 2003
Mitochondrial toxicity
Lipids level changes
Insulin resistance
Mitochondrial toxicity
Lipids level changes
Insulin resistance
NAFLD/NASH
NAFLD in HIV mono-infection

Mitochondrial toxicity
Ingiliz Hepatology 2009
No evidence of mitochondrial DNA depletion
Evidence of mitochondrial toxicity
No relation to the type of cART used

NAFLD in HIV patients
• 225 mono-infected patients, NAFLD in 83
• Mean BMI 23.8 kg/m2
Guaraldi Clin Infect Disease 2008
Variable 95% CI P
ALT/AST ratio 4.59 (2.09–10.08) <0.001
Male sex 2.49 (1.07–5.81) <0.001
Cumulative NRTI 1.12 (1.03–1.22) <0.001
Waist circumference 1.07 (1.03–1.11) <0.001
NASH in HIV patients
• 128 consecutive HIV mono-infected patients
• Mean BMI 24.5 kg/m2
• 55% NAFLD on US
• 18% Fibroscan >7.4 Kpa
• Age and MS independent predictors of >7.4 KPa
Lombardi, Digestive Liver Diseases 2016

APRI>1.5 in 8.3% of 432 patients
T2DM and detectable HIV viraemia independent predictors
Cohort also included patients who used alcohol
NASH in HIV patients
DallaPiazza BMC Infect Dis 2008
Prognosis – hepatology referrals

Natural history of NAFLD
P=NS P=0.01
Simple steatosis NASH
Ekstedt, Hepatology 2006
129 patients
Mean follow-up 13.7 years
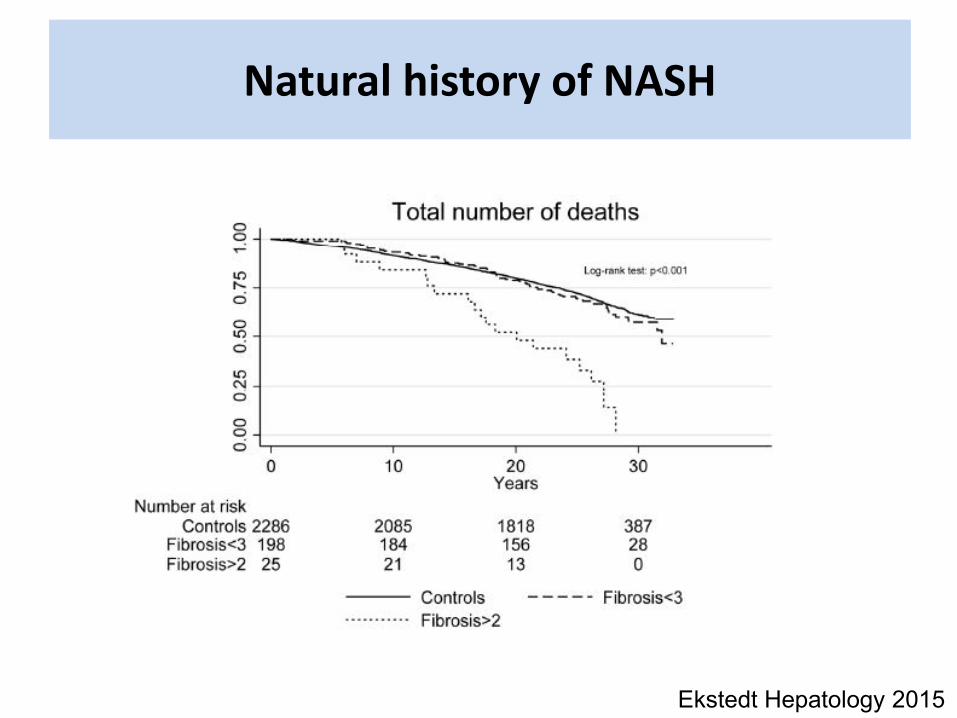
Natural history of NASH
Ekstedt Hepatology 2015
• Age (mitochondrial dysfunction)
• All metabolic syndrome components
- Obesity/increased WC
- T2DM
- Hypertension
- Dyslipidaemia
• Smoking
Factors associated with progression

NASH and mortality
• CVS main cause of death
• Liver disease only 3d cause of mortality
Ekstedt, Hepatology 2006
Soderberg, Hepatology 2010

NAFLD – referral pathways
• High prevalence, low severity
• No liver-specific treatment
• How to select patients for referral?
• Non-invasive fibrosis assessment

Simple non-invasive clinical scores for F>2
• FIB4
Age, ALT, AST, PLT
• NAFLD fibrosis score
Age, BMI, hyperglycemia, AST/ALT, PLT, albumin
Angulo Hepatology 2007 Shah Clin Gastroenterol Hepatol 2009
Calculation of simple NITs
FIB-4: http://gihep.com/?page_id=9
NAFLD fibrosis score: http://nafldscore.com
Liver calculator Free application for smartphones

Risk classification according to simple NITs
60%
35%
5%
Low risk for >F2 Indeterminate risk for >F2 High risk for >F2
FIB4<1.3 1.3<FIB4<3.25 FIB4>3.25

NITs and prognosis
• NITs initially developed as surrogate markers
of fibrosis with a view to replace LB
• Increasingly used to assess prognosis
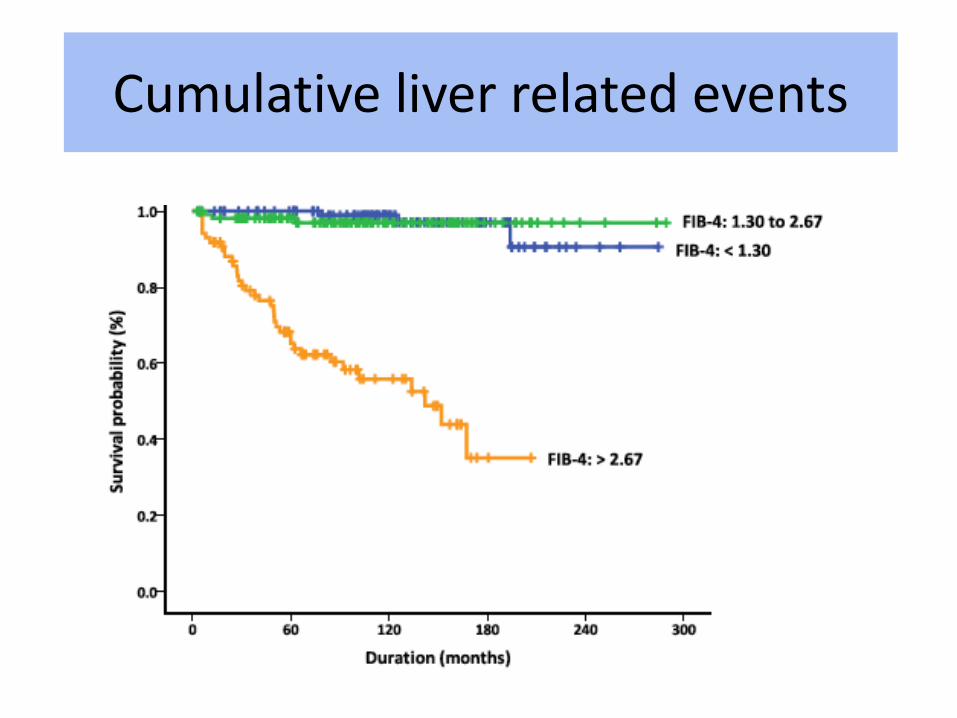
Cumulative liver related events
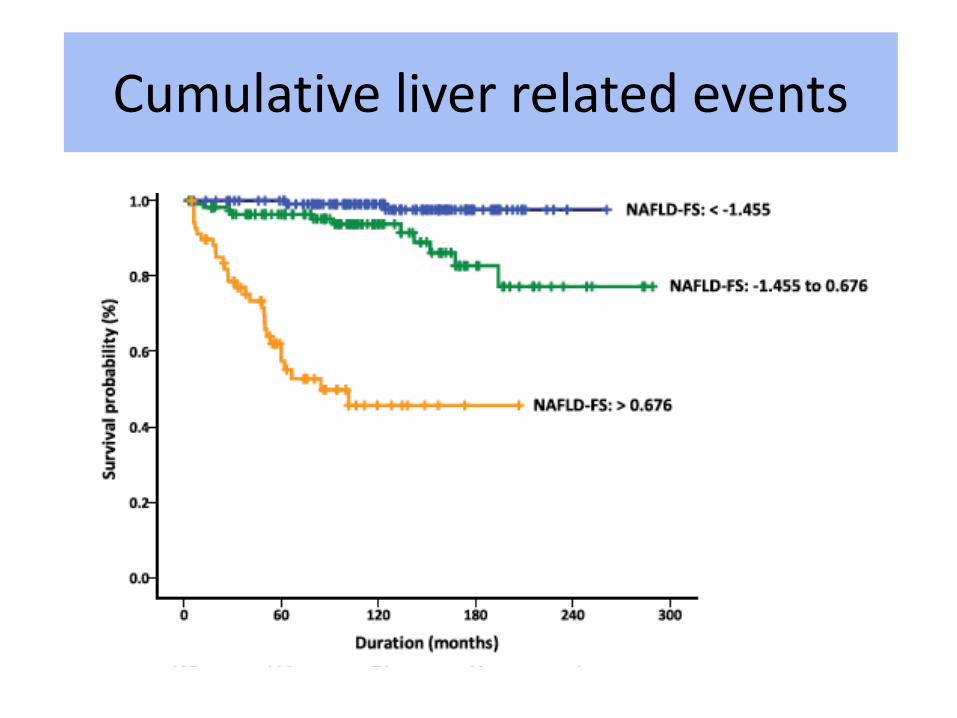
Cumulative liver related events
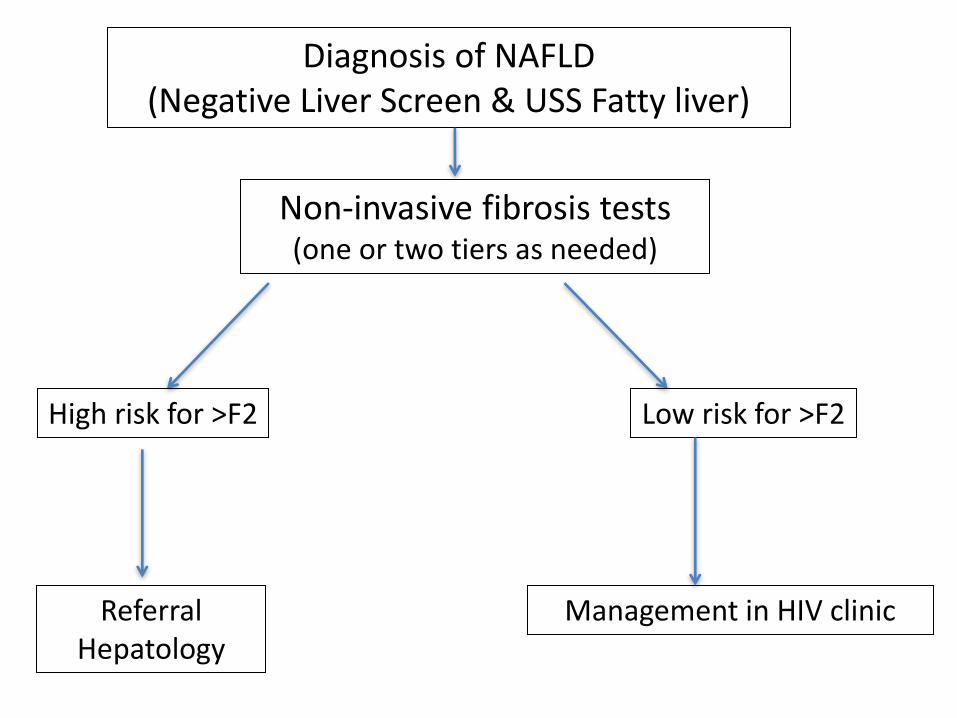
Diagnosis of NAFLD
(Negative Liver Screen & USS Fatty liver)
High risk for >F2 Low risk for >F2
Referral
Hepatology
Management in HIV clinic
Non-invasive fibrosis tests (one or two tiers as needed)

Summary se and sp of NIT for NAFLD
TN/(TN+FN)
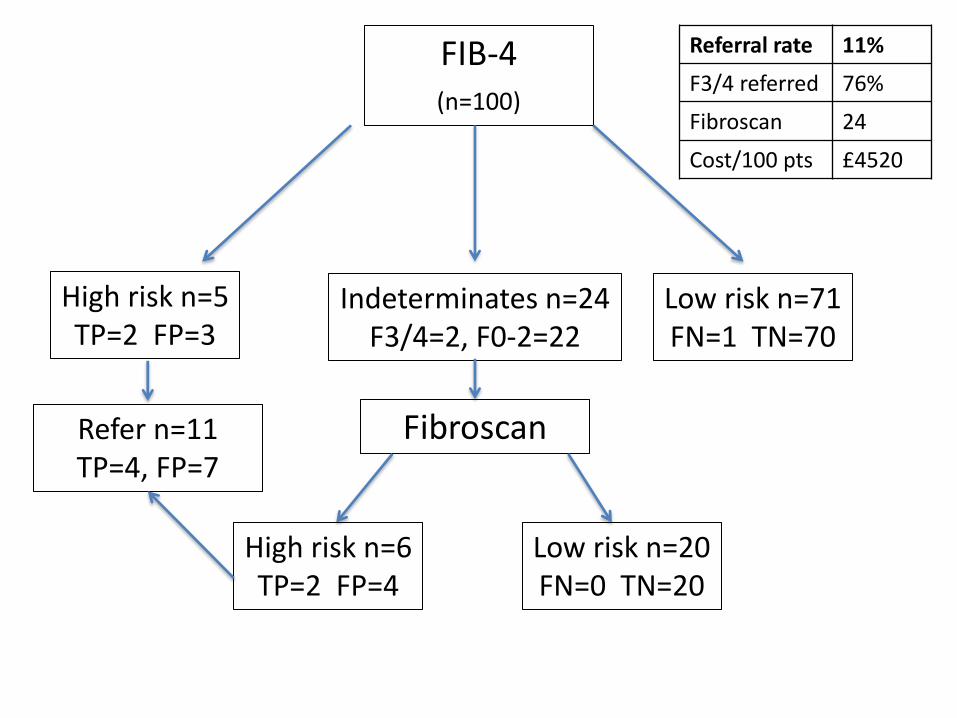
FIB-4
(n=100)
High risk n=5
TP=2 FP=3
Low risk n=71
FN=1 TN=70
Indeterminates n=24
F3/4=2, F0-2=22
Fibroscan Refer n=11
TP=4, FP=7
High risk n=6
TP=2 FP=4
Low risk n=20
FN=0 TN=20
Referral rate 11%
F3/4 referred 76%
Fibroscan 24
Cost/100 pts £4520
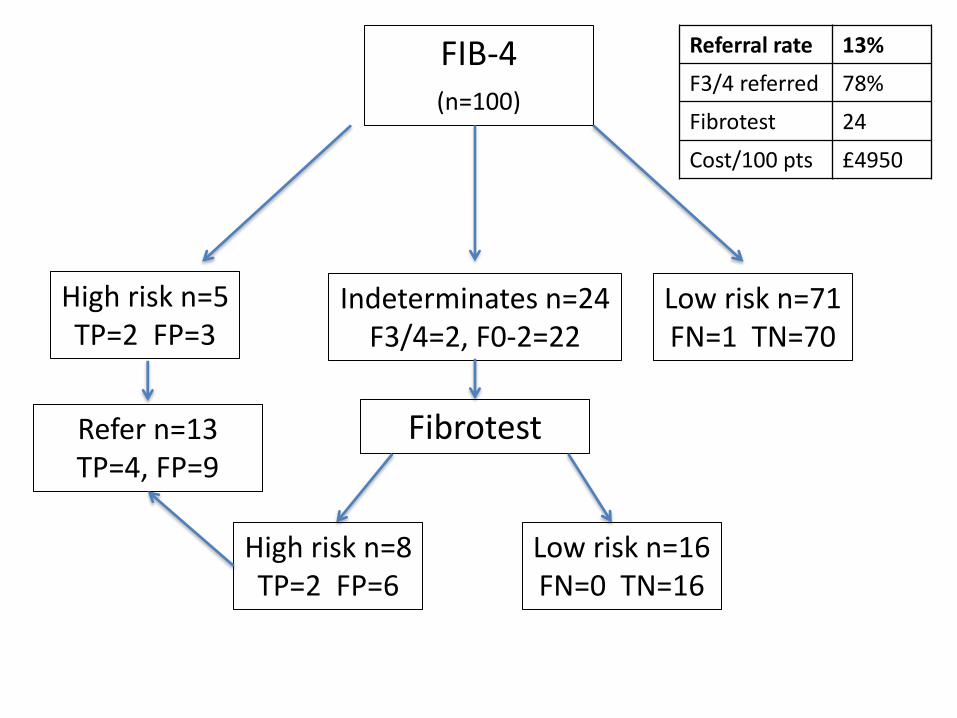
FIB-4
(n=100)
High risk n=5
TP=2 FP=3
Low risk n=71
FN=1 TN=70
Indeterminates n=24
F3/4=2, F0-2=22
Fibrotest Refer n=13
TP=4, FP=9
High risk n=8
TP=2 FP=6
Low risk n=16
FN=0 TN=16
Referral rate 13%
F3/4 referred 78%
Fibrotest 24
Cost/100 pts £4950

FIB-4
(n=100)
High risk n=5
TP=2 FP=3
Low risk n=71
FN=1 TN=70
Indeterminates n=24
F3/4=2, F0-2=22
ELF Refer n=9
TP=4, FP=5
High risk n=4
TP=2 FP=2
Low risk n=26
FN=0 TN=26
Referral rate 9%
F3/4
referred
76%
ELF 24
Cost/100 pts £3660/
5290

Natural history of NAFLD
Adams, Gastro 2005
77%
87%
420 patients
Mean follow up 7.6 years

0
200
400
600
800
1000
1200
1400
1600
March 2012-Feb 2013 March 2013 - Feb 2014 March 2014 – Feb 2015
601
837
1437
Ne
w E
lect
ron
ic c
od
es
for
NA
FLD
Annual new primary care electronic codes for NAFLD in
Camden and Islington London Boroughs
Annual new cases of NAFLD in C&I *population of Camden and Islington = 400,000
Post-pathway Pre-pathway Srivastava 2015

Initial impact of pathway *after evaluation of 40% of post pathway data at Royal Free London
Post-pathway Pre-pathway
Composite
consultant
judgment
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre-pathway (2012-2013) Non NAFLD pathway 2014-2015 NAFLD pathway (excluding normal
LFT's)
F fibrosis
F fibrosis
Srivastava 2015
Treatment

Who should be treated?
Simple steatosis:
Lifestyle advice, CVS factors
NASH, F0-F1 fibrosis:
Lifestyle advice, CVS factors, clinical trials
NASH, significant fibrosis:
Liver-specific interventions, clinical trials

Potential treatment targets
• Lifestyle changes
• Antioxidant factors
• Insulin resistance
• Fibrosis

Weight loss and NASH
Vila-Gomez Gastro 2015
293 patients
Dietary intervention
52 weeks

Statins in liver disease
437 patients with abnormal LFTs
LFT improvement
Less CVS events
Athyros Lancet 2010
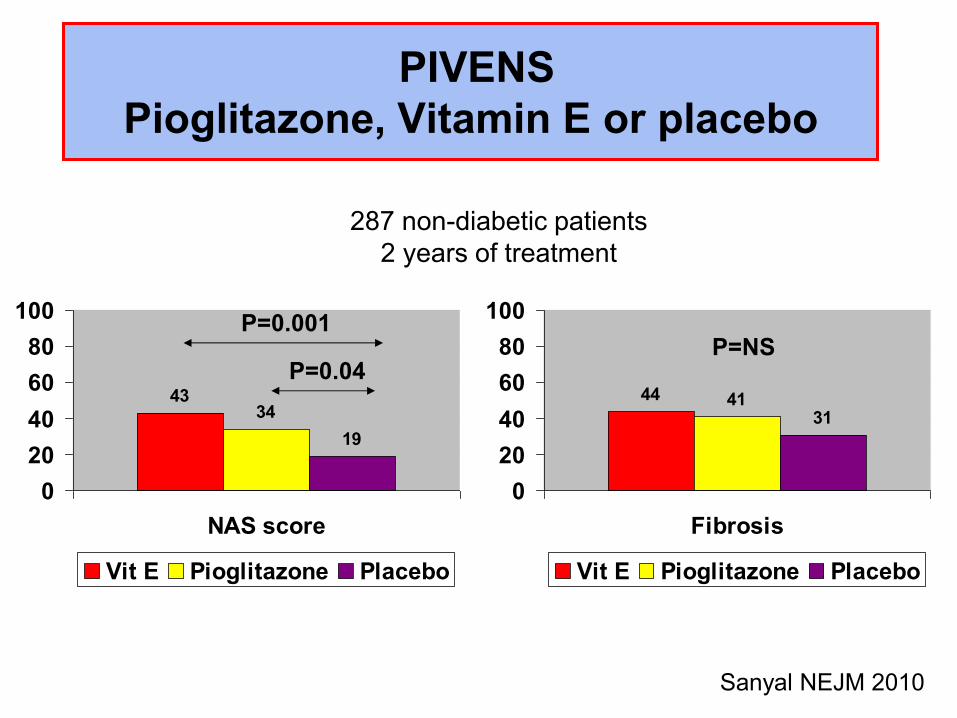
PIVENS
Pioglitazone, Vitamin E or placebo
4334
19
0
20
40
60
80
100
NAS score
Vit E Pioglitazone Placebo
44 4131
0
20
40
60
80
100
Fibrosis
Vit E Pioglitazone Placebo
P=NS P=0.001
P=0.04
Sanyal NEJM 2010
287 non-diabetic patients
2 years of treatment
Vitamin E: current evidence
• Effective in two RCTs (PIVENS, TONIC)
BUT:
– Increased mortality in doses >400 IU/day
– Increased risk of prostate cancer

FXR nuclear receptor
Lipid metabolism
Reduces lipogenesis (SREBP1c)
Increases fatty acid oxidation
Liver
Reduces inflammation (NF-kB)
Antifibrotic
Carbohydrate metabolism
Improves insulin sensitivity
Reduces neoglucogenesis

Obeticholic acid
• Farnesoid X receptor agonist
• Non-cirrhotic NASH
• Double blind, phase II, placebo controlled trial
• 25 mg OCA (n=141), placebo (n=142) 72 weeks
• Primary endpoint = 2 point improvement in NAS with no
worsening of fibrosis
• Improvement in histology (50 OCA, 23 placebo)
• Increase in LDL
Neuschwander-Tetri Lancet 2014

FLINT - histological data
Feature OCA Placebo Relative Risk P value
Number of patients 102 98
Decrease of NAS score by
points with no worsening of fibrosis
50(45%) 23(21%) 1.9 (1.3-2.8) 0.0002
Improvement in Fibrosis 36(35%) 19(19%) 1.8(1.1-2.7) 0.004
Improvement in Ballooning 47(46%) 30(31%) 1.5(1.0-2.1) 0.03
Improvement in lobular
inflammation
54(53%) 34(35%) 1.6(1.1-2.2) 0.006
Improvement in Steatosis 62(61%) 37(38%) 1.7(1.2-2.3) 0.001
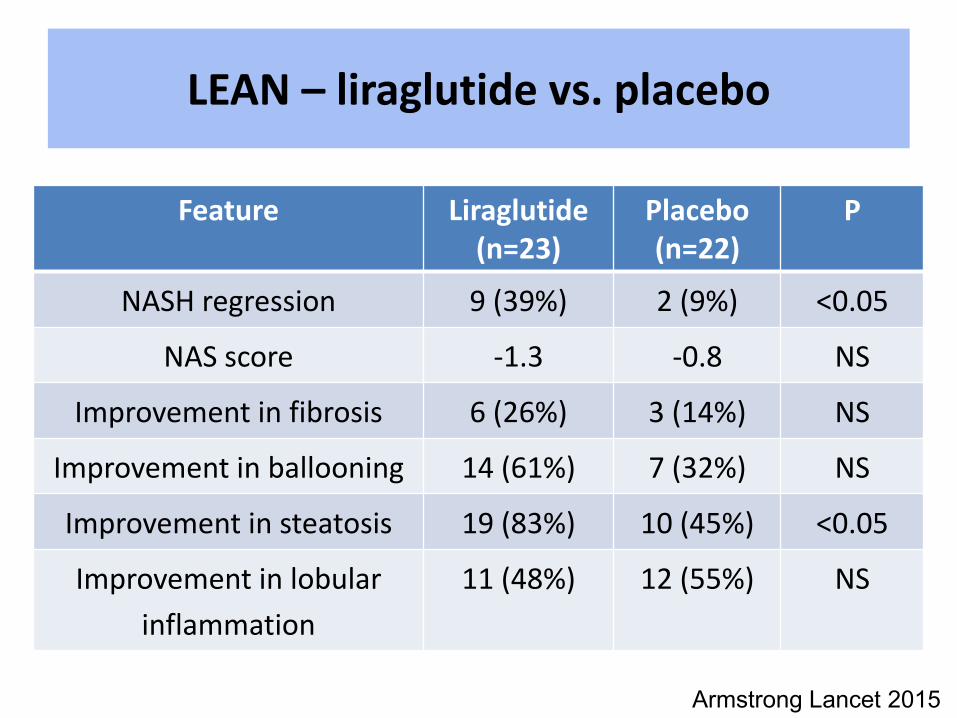
LEAN – liraglutide vs. placebo
Feature Liraglutide
(n=23)
Placebo
(n=22)
P
NASH regression 9 (39%) 2 (9%) <0.05
NAS score -1.3 -0.8 NS
Improvement in fibrosis 6 (26%) 3 (14%) NS
Improvement in ballooning 14 (61%) 7 (32%) NS
Improvement in steatosis 19 (83%) 10 (45%) <0.05
Improvement in lobular
inflammation
11 (48%) 12 (55%) NS
Armstrong Lancet 2015
Treatment of metabolic syndrome
components
• Obesity – exercise and diet
• T2DM– pioglitazone, metformin or liraglutide
• Hypertension – ΑΑΤ2
• Dyslipidaemia – statins
• Smoking cessation

Management of NAFLD by the HIV physician
Follow-up in HIV clinic of patients at low risk of fibrosis
-Annual LFTs
- >10% weight loss
- Treat components of metabolic syndrome
(hypertension, diabetes, hyperlipidaemia)
- In 3-5 years re-assess risk of advanced fibrosis
using non-invasive fibrosis assessment

Conclusions
• Transaminitis common in patients with HIV
• Viral hepatitis, alcohol, NAFLD, drug toxicity
• 10% of HIV patients might have NAFLD with fibrosis
• Only a minority needs hepatology referral
• Aggressive treatment of MS components
