introduction to temperature therapy and cooling. temperature therapy perspectives on cooling vital...
TRANSCRIPT
Introduction to Temperature Therapy and Cooling

Temperature Therapy Perspectives on Cooling
• Vital sign• Maslov’s hierarchy of needs - shelter• Nature’s design-metabolic protection
– Hibernation- Self protection mechanism– Animals seek cool environment when ischemic
• Intuitive-”Cooling prevents spoilage”• Learned-”Ice on injuries reduces swelling and
tissue damage”• Physiological and biochemical rationale
– Tissue metabolic rates decrease as body temperature decreases

Levels of Hypothermia-°C
36.6-37.5=Normothermia
34-36.5=Mild hypothermia
28-33.5=Moderate hypothermia
17-27.5=Deep hypothermia
4-16.5=Profound hypothermia
35.5 = Shivering
>37.5=Hyperthermia
36.5 = Vasoconstriction
37.5 = Vasodilatation
Temperature Therapy
• Historically, limited to temperature preservation, i.e. warming in surgery, shock, etc.
• Investigation of cooling as a therapy limited by body’s complex thermoregulatory mechanisms– Core vs. peripheral dynamics– Tolerance to change varies significantly
individual to individual– Inability to cool with any precision and
predictability– Requirement to paralyze/anesthetize patient to
overcome thermoregulatory responses– Significant complications that occur below 28°C
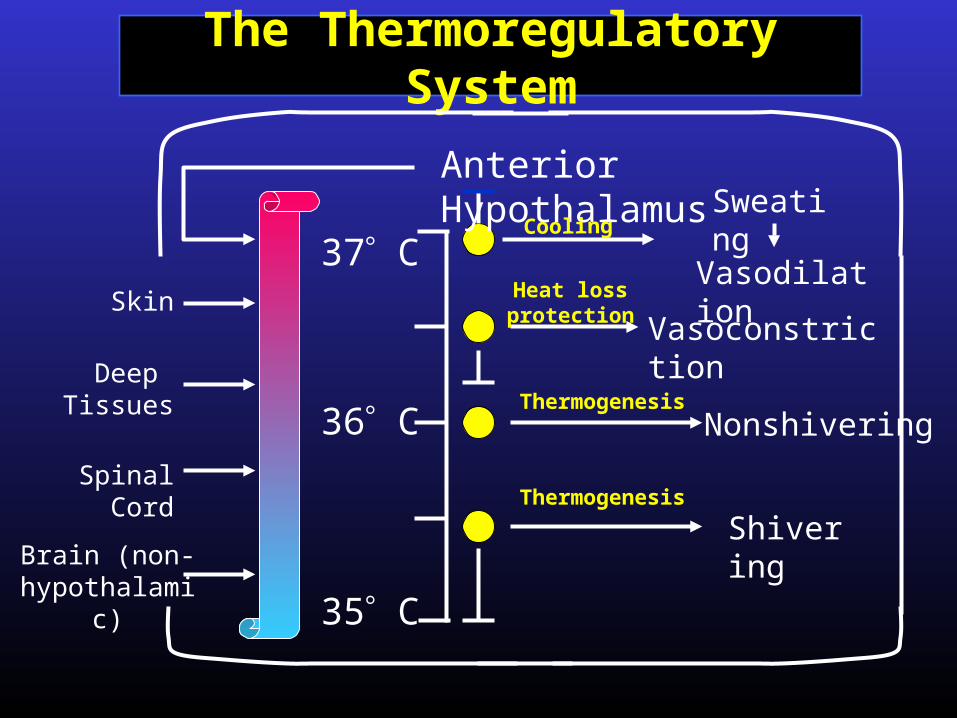
The Thermoregulatory System
35 C
36 C
37 C
Anterior Hypothalamus
VasodilationVasoconstrictio
n
Nonshivering
ShiveringBrain (non-
hypothalamic)
Spinal Cord
Deep Tissues
Skin
SweatingCooling
Heat loss protection
Thermogenesis
Thermogenesis
Techniques to Induce Hypothermia
• Surface cooling techniques– Slow and imprecise– Cumbersome– Limited in depth with non-paralyzed patient
• Lavage – Moderately invasive and uncomfortable– Slow and imprecise
• IV infusions– Limited volumetric capacity
• Cardiopulmonary bypass– Invasive and resource intensive
Cooling as a Therapy
• Despite challenges, long history of clinical and research investigation
• 1940 - Neurosurgeon Temple Fay reported on first whole body cooling*
• 1950 – Bigelow and Shumway published on hypothermia as a cardioprotective agent that is the foundation for today’s modern CPB technique**
• Transplant surgeons and cell physiologists routinely use cooling to preserve cells and tissues
• Cooling is gold standard in many cardiac surgery and neurosurgery procedures
* NY State J. Med 1940; 40: 1351-54 * NY State J. Med 1940; 40: 1351-54
** Ann Surg 1950; 132: 849** Ann Surg 1950; 132: 849
Cooling as TherapyBackground
• Extensive research and evidence of the beneficial effects and mechanisms of cooling– Pre-clinical evidence of mechanisms, basic science– Clinical trials evidencing the clinical benefits of
cooling
• Despite current technical challenges of cooling, several recently published clinical studies demonstrate the benefits of cooling in:– Cardiac Arrest*– Stroke**
* NEJM 2002; 345: 549-56, NEJM 2002; 346: 557-63** Stroke 2002; 32: 1847-54

Cooling as Therapy InCardiac Arrest Trial Results
• Two independent studies utilized surface cooling on intubated, paralyzed patients vs. standard of care
• Multi-center, prospective, randomized trial in Australia*– 77 pts: 43 hypothermia, 34 control– 33°C x 12 hours following resuscitation from cardiac arrest– Good neurologic outcome : 49% of cooled, 26% of controls
(p=.046)
• Multi-center, prospective, randomized trial in Europe **– 275 pts: 137 hypothermia, 138 control– 32°C to 34°C x 24 hours– Good neurologic outcome in: 55% of cooled, 39% of controls
(p=.009)– Mortality 41% in cooled vs 55% control, P=.02
* NEJM 2002; 346: 557-63** NEJM 2002; 345: 549-56

Hypothermia in Malignant Stroke*
• Study Design– Single center trial of mild cooling– 25 patients with severe MCA strokes and increased
ICP– Cooling via surface cooling, cool infusions and cold
washing– Cooling to 33°C within 14 hours after stroke, for 48 -
72 hours
• Results– Decreased ICP with mortality of 44%, as compared to
80% in historical controls– Concluded that moderate hypothermia in the
treatment of severe cerebral ischemia is not associated with severe side effects and may help control critically elevated ICP values and improve clinical outcome in these patients
* Stroke 1998;29: 2461-2466

Hypothermia in Head Trauma
• Single center, prospective, randomized trial*– 82 patients (40 - hypothermia to 33°C x 24 hrs)– Improved outcome at 3 and 6 months in pts with
initial Glasgow Coma Scale score 5 - 7
• Multicenter, prospective, randomized trial **– 392 pts (199 - hypothermia to 33°C x 48 hrs)– Overall results negative– Positive results in patients < 45 years who were
normovolemic
* NEJM 1997; 336: 540-6** NEJM 2001; 344: 556-63
Surface Cooling Limitations
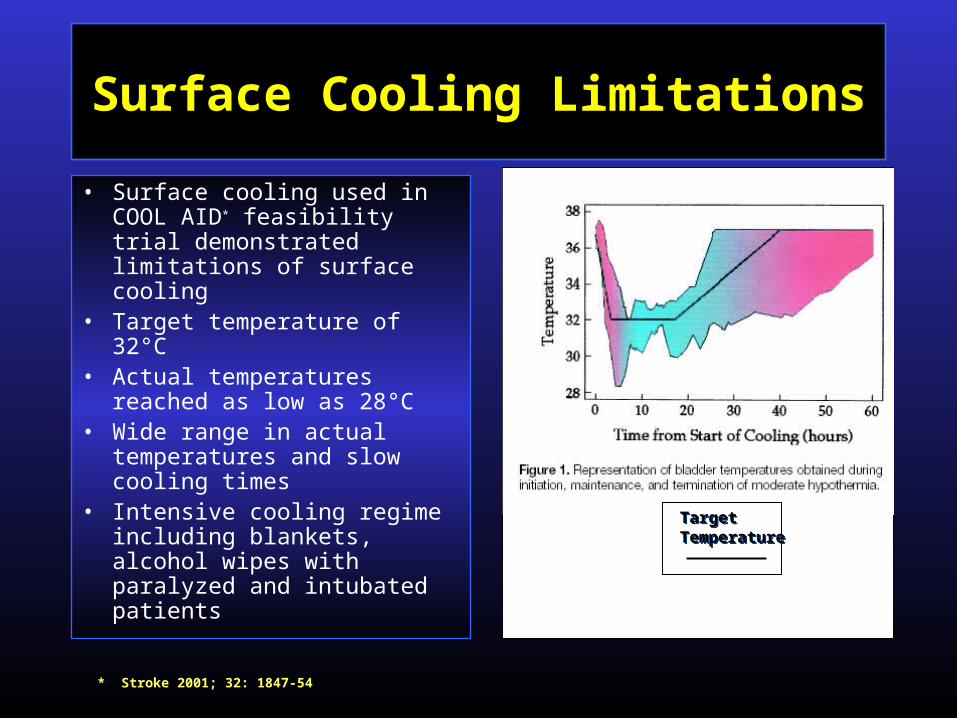
• Surface cooling used in COOL AID* feasibility trial demonstrated limitations of surface cooling
• Target temperature of 32°C
• Actual temperatures reached as low as 28°C
• Wide range in actual temperatures and slow cooling times
• Intensive cooling regime including blankets, alcohol wipes with paralyzed and intubated patients
TargetTemperatureTargetTemperature
* Stroke 2001; 32: 1847-54
Endovascular Temperature Therapy-Goals
Safe Rapid cooling to target therapeutic levels in
ischemic tissues Precise cooling, maintenance, and re-warming
capabilities Minimally invasive, venous catheter-based
method Comfortably cool awake patients Ease of use in a variety of locations, ICU,
CCU, ER, etc. Minimize resource intensity Minimal hemodynamic effects
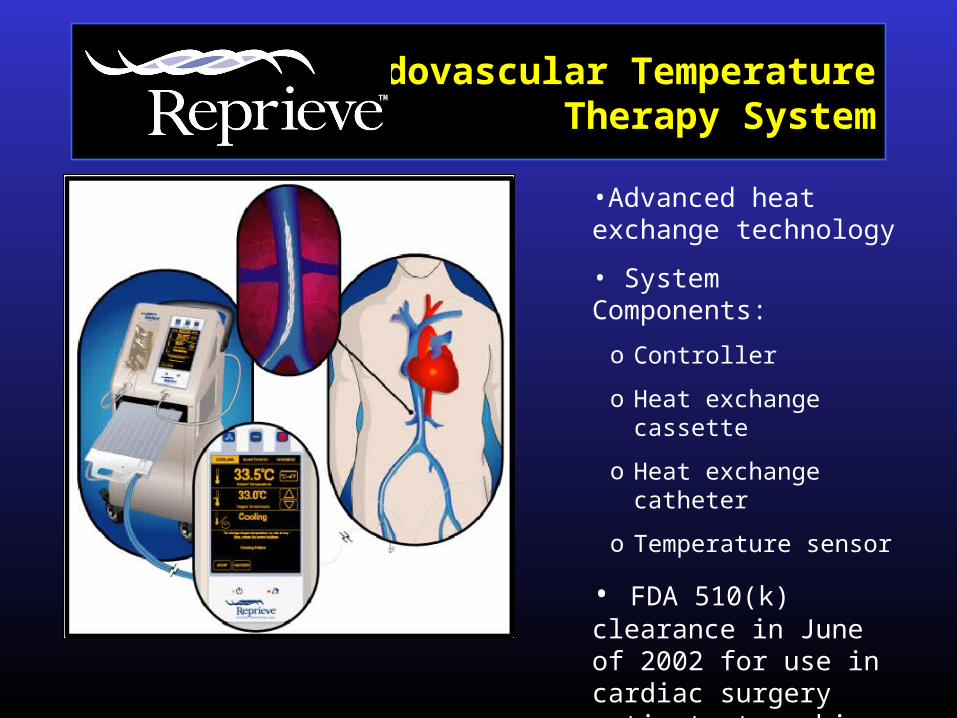
Endovascular TemperatureTherapy System
•Advanced heat exchange technology
• System Components:
o Controller
o Heat exchange cassette
o Heat exchange catheter
o Temperature sensor
• FDA 510(k) clearance in June of 2002 for use in cardiac surgery patients to achieve and/or maintain normothermia
TM
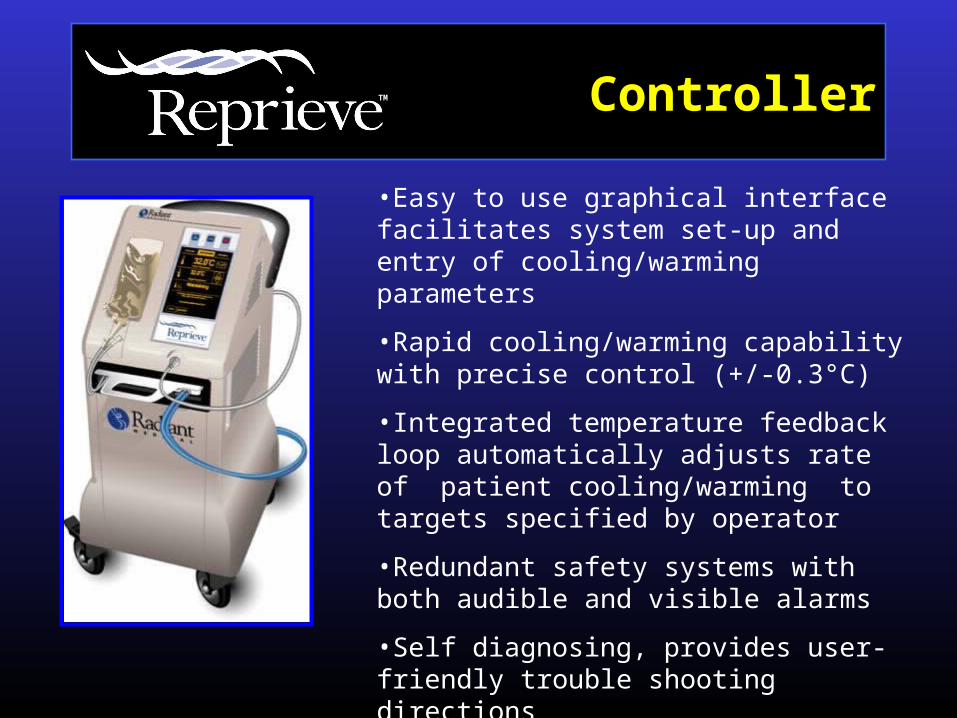
•Easy to use graphical interface facilitates system set-up and entry of cooling/warming parameters
•Rapid cooling/warming capability with precise control (+/-0.3°C)
•Integrated temperature feedback loop automatically adjusts rate of patient cooling/warming to targets specified by operator
•Redundant safety systems with both audible and visible alarms
•Self diagnosing, provides user-friendly trouble shooting directions
ControllerTM

• Delivered through standard 10Fr sheath
• Expands to 27Fr when inflated
• Surface treatment to minimize thrombogenicity
• 25 cm long heat exchanger
• Central lumen for OTW placement
• Helical multi-lumen construction maximizes surface area for heat exchange
CatheterTM
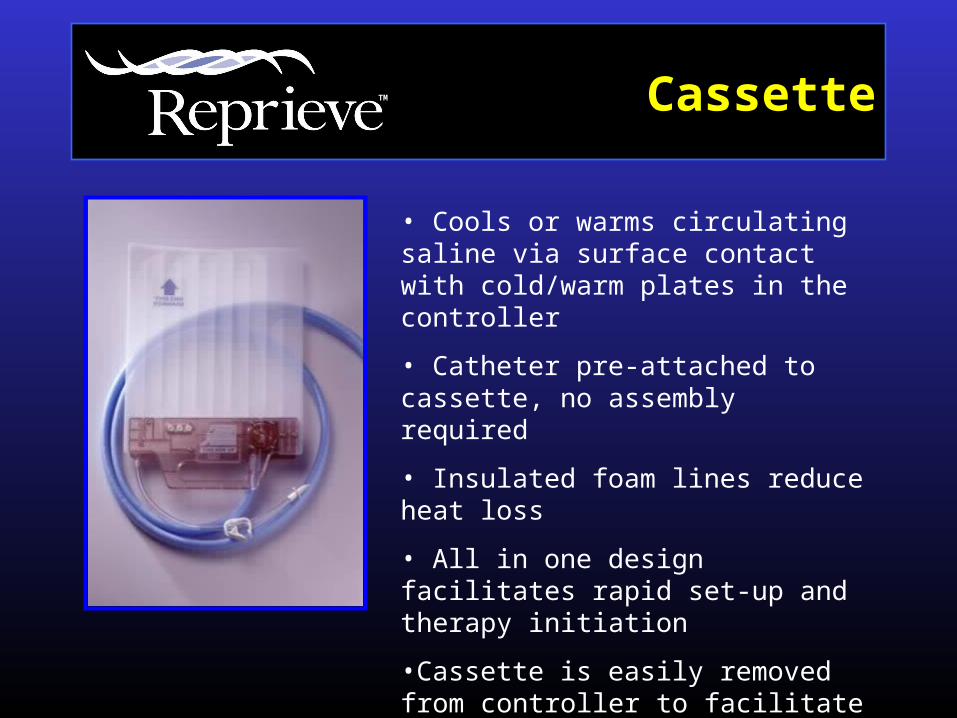
• Cools or warms circulating saline via surface contact with cold/warm plates in the controller
• Catheter pre-attached to cassette, no assembly required
• Insulated foam lines reduce heat loss
• All in one design facilitates rapid set-up and therapy initiation
•Cassette is easily removed from controller to facilitate patient transfer
CassetteTM

Shivering Management
Skin Sensor
Management
Drug-Brain
Threshold
Endovascular
Temperature
Optimal Endovascular Therapy is dependent on successfully managing three interdependent
factors•Buspirone and Meperidine to reduce shivering threshold
•Use of warm air blanket to “fool” skin receptors
•Rate of core cooling and maintenance
Cooling the Awake PatientTreatment Procedure
• Administer Buspirone and Meperidine• Prepare System • Place catheter and temperature sensor• Initiate cooling to target of 33°C• Place warming blanket• Maintain at 33°C for prescribed
duration• Re-warm to normothermia at controlled
rate• Remove catheter and warming blanket

Clinical Trials of Cooling
• Ongoing or completed trials – AMI (Radiant Medical - Endovascular)
– Ischemic Stroke (Radiant Medical -Endovascular)
– Hemorrhagic Stroke (Endovascular)
– Cardiac Arrest (Surface)
– Aneurysm Surgery (Endovascular & Surface)
– Brain Injury (Surface)