introduction to protozoa general account unicellular animal with full functions distribute widely:...
TRANSCRIPT
Introduction to ProtozoaIntroduction to Protozoa

General Account
• Unicellular animal with full functions
• Distribute widely: water,soil, etc.
• Total species 65,000
– Free-living: majority
– Parasitic: about 10,000
Medical Protozoa
• Pathogenic protozoa
• Opportunistic parasite( 机会致病 )
– Not normally pathogens
– Become pathogenic due to impairment of host
resistance
– Clinical importance of the AIDS epidemic
Basic Structures• Plasma membrane: 侵袭致病 , 免疫反应• Cytoplasm
– Ectoplasm: locomotion , ingestion, etc– Endoplasm: metabolism
• Nuclear– Vesicular form( 泡状核 ) or compact form
• Locomotive organelle– Pseudopodium( 伪足 ), flagellum( 鞭毛 ), cilia
( 纤毛 )

Mode of Reproduction• Asexual reproduction
– Binary fission( 二分裂法 ): results in 2 daughter cells– Schizogony( 裂体增殖 ): multiple fission, results in mu
ltiple cells– Endodyogony( 内二芽增殖 ): by internal budding
results in 2 cells
• Sexual reproduction– Conjugation( 接合生殖 ): exchange of nuclear
materials of 2 – Gametogony( 配子生殖 ) : sexually differentiated cells
unit zygote
Life Cycle Patterns• One stage form( 简单型 )
– Trophozoite ( take food, be mobile, multiply)
• Two-stage form ( 简单型 )– Trophozoite & cyst (not mobile, with cyst wall)
• Two-host form– Mammals – mammals( 循环传播型 )– Mammals - insect vectors( 昆虫传播型 )

Characteristics of Protozoan in Infection
• Proliferation-parasitemia
• No larva and adult differentiation but stage differences
• May be intracellular lodgment
• Opportunistic & accidental infections (free-living)
Medical Important Species
• Amebae
• Flagellates
• Sporozoites
• Ciliates

Pathogenic Intestinal AmoebaPathogenic Intestinal Amoeba
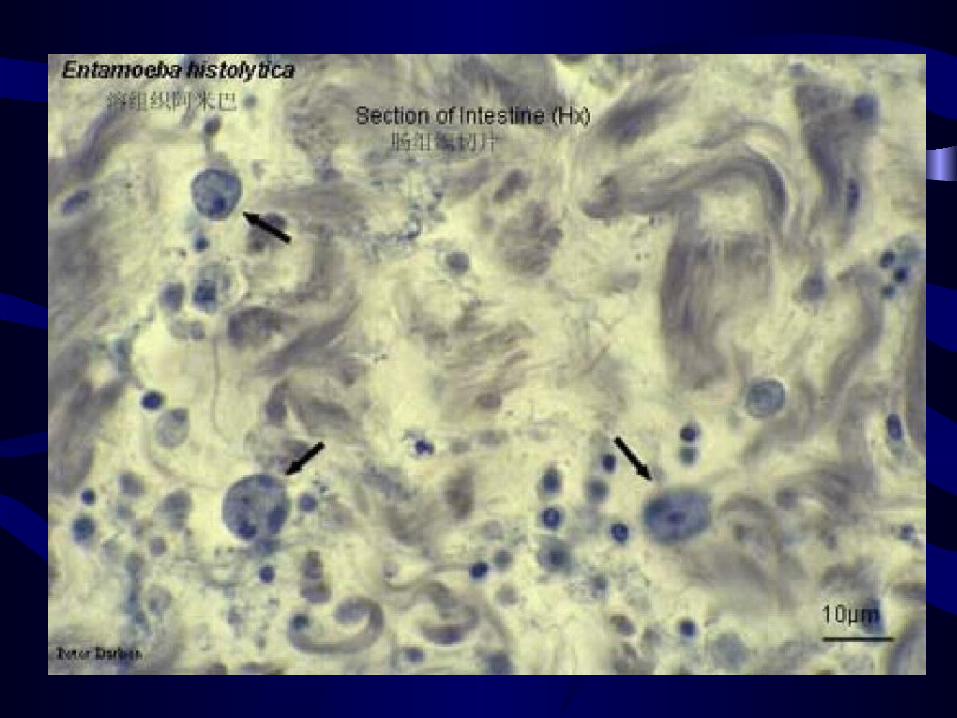
Entamoeba histolyticaEntamoeba histolytica
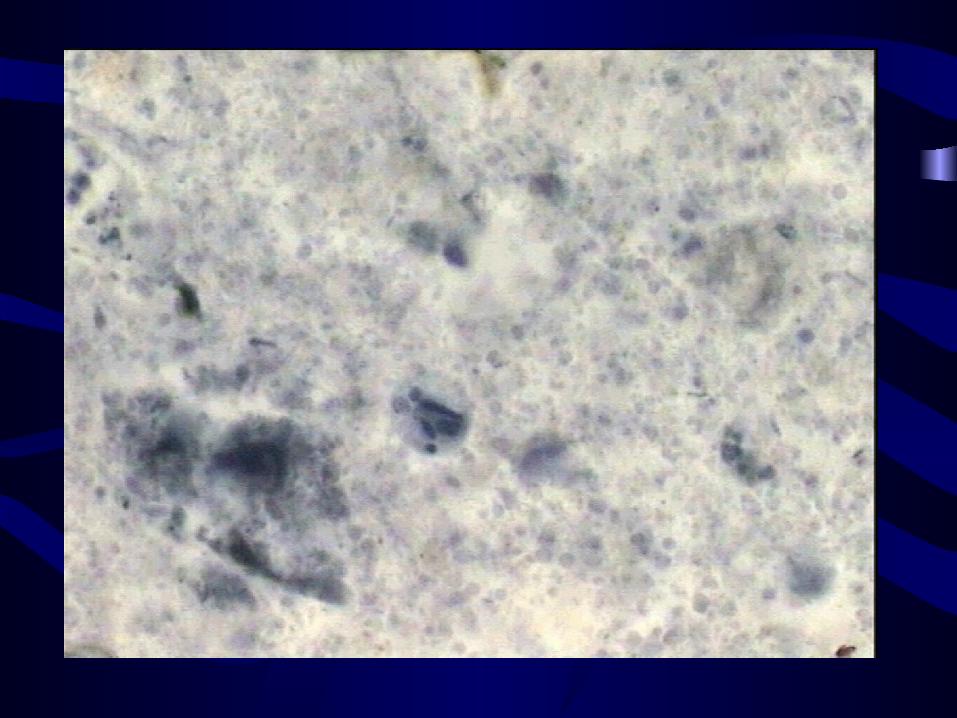
MorphologyMorphology
• Trophozoite
– Size: 10-40 m
– Shape: ovoid with pseudopodium
– Basic structure: cytoplasm, vesicular nucleus (c
hromatin granules, nuclear membrane, karyoso
me)



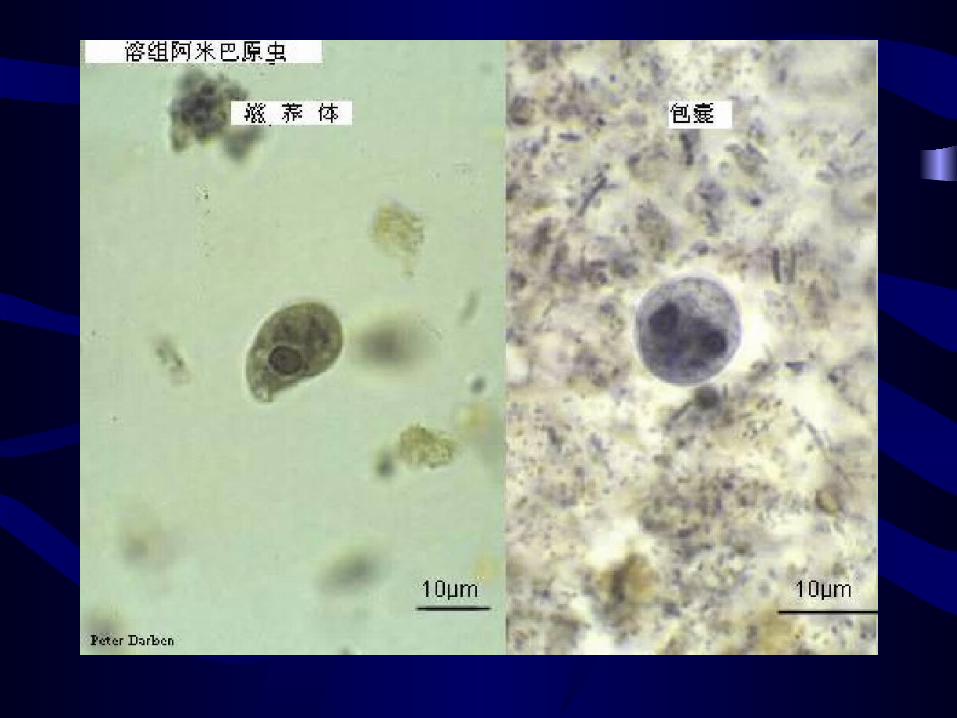

• Cyst– Size: 10-20 m– Structure: cyst wall, 1-4 nuclei, chromatoid bod
y– Physiological function:
• The stage of discharge
• Resistant to external surroundings
• The infective stage

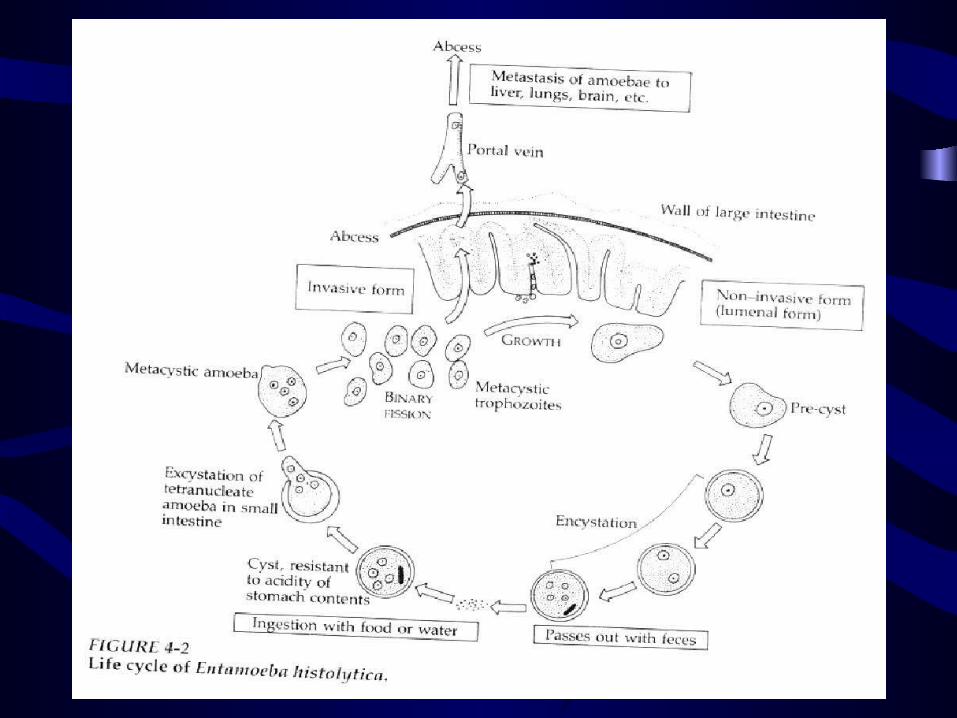
Main Points of Life Cycle
• Cycle: cyst—trophozoite—cyst
• Host: human being
• Lodgment: large intestine
• Infective stage: 4 nuclei cyst
• Infective route: mouth

Pathogenesis
• Pathogenic factor– Virulence– Species:
• E.histolytica (pathogenic species)
• E.dispar (non-pathogenic species)
– Immunity of host– Bacteria flora
• Mechanism: contact lysis
• Pathology: flask-like ulcer
• Clinical manifestation– Non symptomatic carriers– Intestinal amebiasis: dysentery, colitis– Extraintestinal amebiasis: liver abscess


Diagnosis
• Etiological diagnosis:– Stool examination of cyst or trophozoite– Sigmoidoscopy or aspiration– Immunological diagnosis

Epidemiology
• Cosmopolitan: 110 population
• China: 3%~10%; Rural area>urban
• Source of infection: carriers
• Transmit route: water contamination
• Insects: fly, cockroaches
Prevention and Control
• Patients and carriers: – Intestinal amoebiasis —metronidazole – Extra~ amoebiasis —diloxanide
• Water & nightsoil control
• Insect vector control
• Personal hygienic health education

Plasmodium
Introduction
• Most important tropical disease
– 300 million cases with one million deaths world
wide in 1999;
– 30 million cases before liberation and 24000
cases reported with 39 death in 2000 in china;
• 4 species infecting human
– Plasmodium falciparum( 恶性疟原虫 )
– Plasmodium vivax( 间日疟原虫 )
– Plasmodium malariae( 三日疟原虫 )
– Plasmodium ovale( 卵形疟原虫 )
Life Cycle & Morphology
• Cycle in human (intermediate host)
– Exoerythrocytic stage( 红细胞外期 )
– Erythrocytic stage( 细胞内期 )
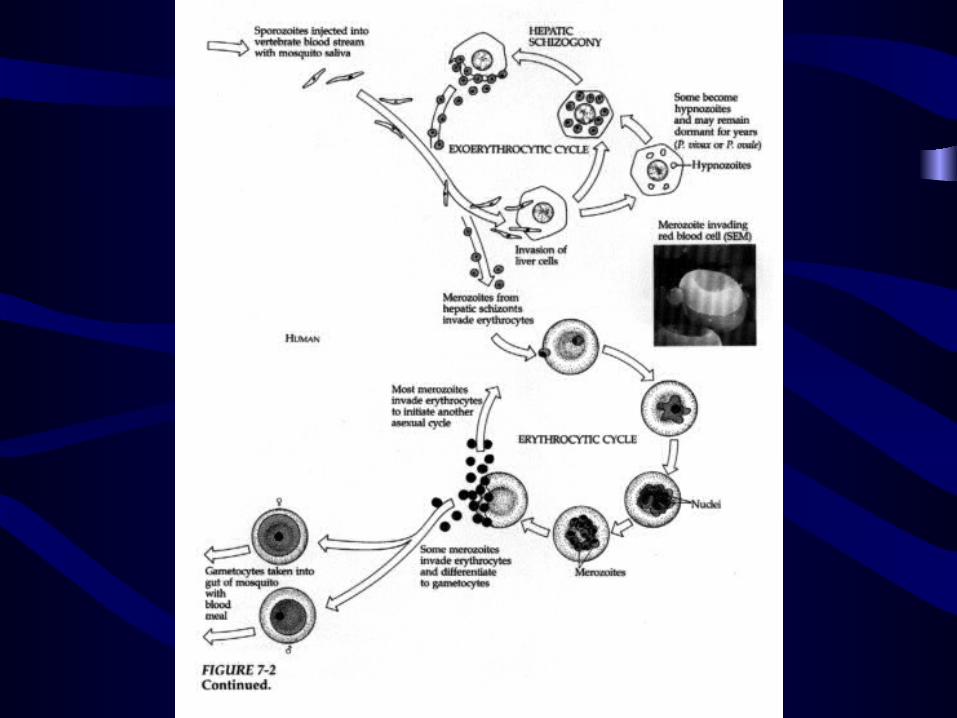
红细胞外期 ( 肝细胞内增殖 ) Exo-erythrocytic cycle
(速发型) 子孢子 红外裂殖体 裂殖子
sporozoite E-E Schizont Merozoite(迟发型 P.v. )
进入红细胞 P.v. 8d; P.f. 6d; P.m. 12d
红细胞内期 (RBC 内增殖 ) Erythrocytic cycle
•发育:环形滋养体 大滋养体 (Ring form) (Trophozoite)•增殖:早期裂殖体 (Immature schizont) RBC 内发育 成熟裂殖体 ( 子 ) 配子体形成 (Mature schizont) M 吞噬

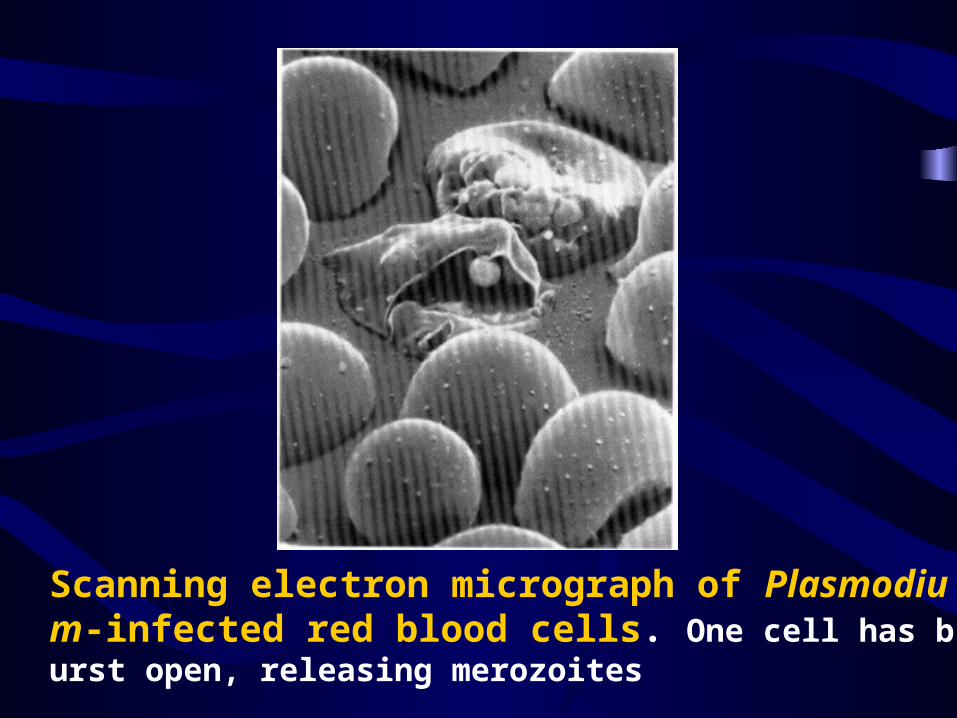
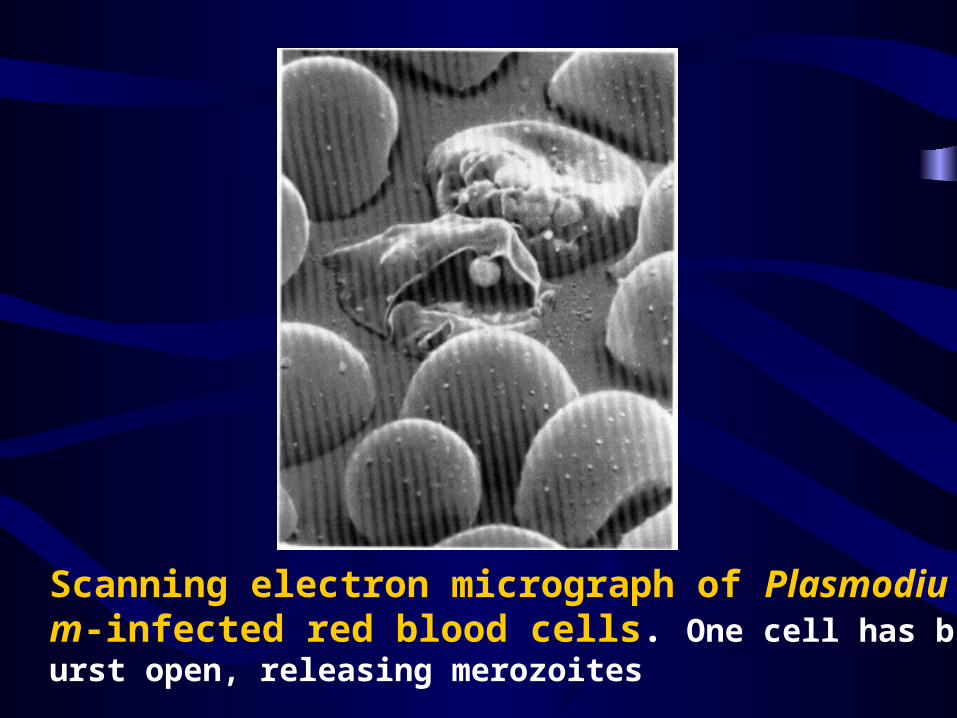
Scanning electron micrograph of Plasmodium-infected red blood cells. One cell has burst open, releasing merozoites

P.v P.f P.m P.o
红内期周期•P.v. 48h•P.f. 36-48h•P.m. 72h成熟裂殖体内裂殖子数和形态•P.v. 12-24 个,不规则•P.f. 8-36 个,不规则•P.m. 6-12 个,菊花状
配子体形成 (Gametocyte form)
• 红内期裂殖子 雌雄配子体 P.v. 2-3d P.f. 7-10d• <12 个 /mm3 不能传播
被寄生 RBC 的变化
•P.v. 胀大 薛氏小点•P.f. 正常 茂氏点•P.m. 正常 西门氏点
疟原虫对 RBC 的选择
•P.v. 幼稚红细胞•P.f. 各种红细胞•P.m. 衰老红细胞
• Cycle in female anopheline mosquito (definitive host)
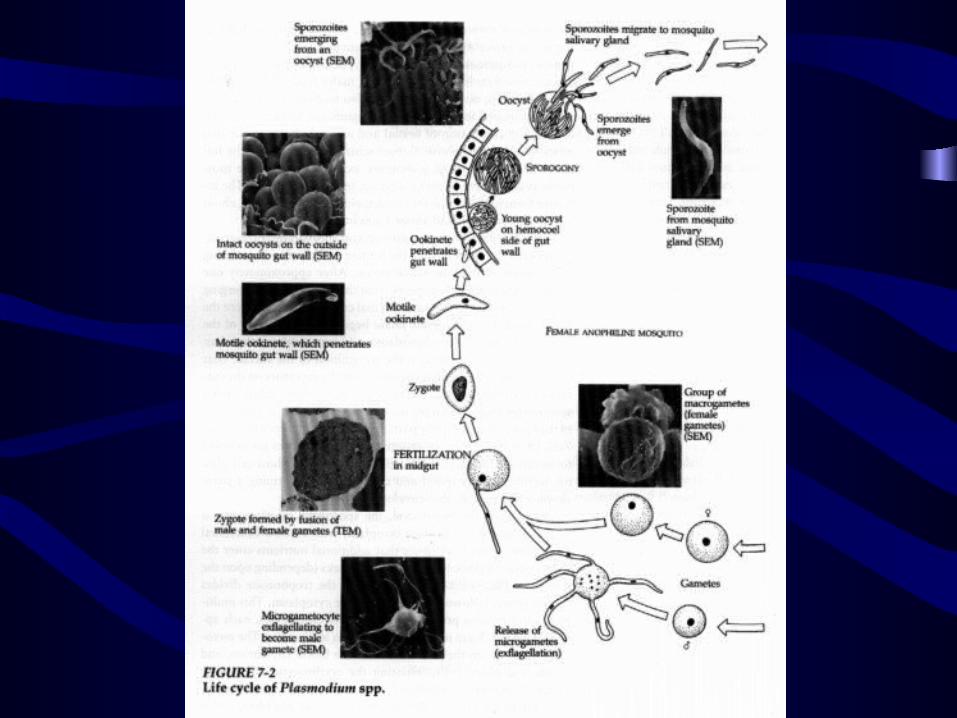

蚊体内发育 ( 有性 ) Grouth in the mosequito 雌配子体 Gametocyte 雌雄配子 受精 雄配子体 (Gametogony) 动合子 Ookinete 合子 Zygote 卵囊 Oocyst (内含子孢子 Sporozoit
e )
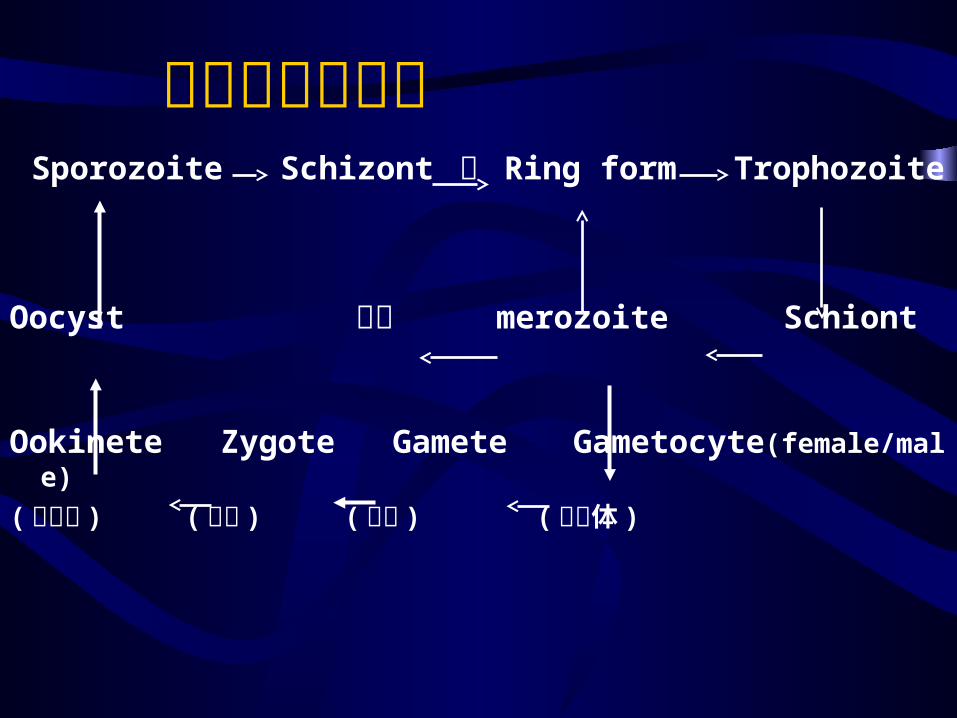
疟原虫发育过程 Sporozoite Schizont 子 Ring form Trophozoite Oocyst 吞噬 merozoite Schiont
Ookinete Zygote Gamete Gametocyte(female/male)
( 动合子 ) ( 合子 ) ( 配子 ) ( 配子体 )


• Infective form: Sporozoite
• Period of one erythrocytic stage:– P.V 48h; P.M 72h; P.F 36-48h
• Resting stage of sporozoite of P.V & P.O:– Hypnozoite (brady sporozoite) in liver cell

Morphology

P.v P.f P.m P.o

Pathogenesis
• Primary attack
– Infected erythrocyte rupture products of schizont, stimulate the release of
cytokines (TNF) paroxysm (shiver, fever,
sweat)
Scanning electron micrograph of Plasmodium-infected red blood cells. One cell has burst open, releasing merozoites

• Relapse:
– It is a recurrence that taken place after complete
initial clearing of the erythrocytic infection and
implies reinvation of the blood stream by meroz
oites from activated hypnozoites in liver.
• Recrudescence
– It is a recurrence of symptoms in a patient
whose blood stream infection has previously
been at such a low level as not to be clinically
demonstrable or cause symptoms.
Complications
• Anemia– Hemolysis of infected erythrocytes– Hypersplenism– Autoimmunization of uninfected erythrocytes – TNF-
• Splenomegaly:• Malarious nephrosis• Cerebral malaria
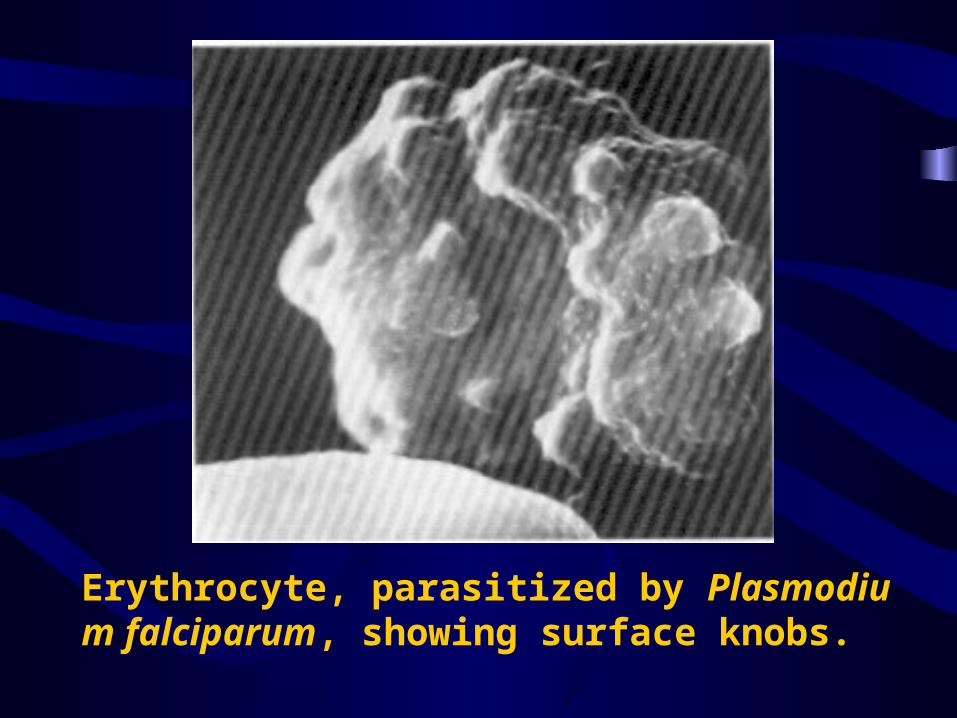
Erythrocyte, parasitized by Plasmodium falciparum, showing surface knobs.
Diagnosis
• Parasitological diagnosis:Parasite; Species; Density– Thin blood films (species identification)– Thick blood films
• 2. Immuno-diagnosis
– Specific antibody detection
past malaria
– Antigen detection
– Specific DNA or RNA detection
Immunity
• Congenital immunity– Duffy-negative erythrocytes are resistant to P.v
in West Africans
• Premunition– The protective immunity persists while the mal
aria parasites are still in the host.
• Evasion of immunity: An ability of malaria parasite to evade host immunity.
• Possible mechanism of evasion– 1) Antigenic variation– 2) Sequestration (avoiding exposure to immune effect
or mechanisms)– 3) Poor immunogenicity of its antigens (analogy exist
s between parasitic antigens and host molecules)
Treatment
• 1. Classes of antimalarial drugs– 1) Blood schizonticides (quinine; chloroquine; artem
isinin; mefloquine; sulfadoxin-pyrimethamine)
– Effect on erythrocytic stage, use for acute attack
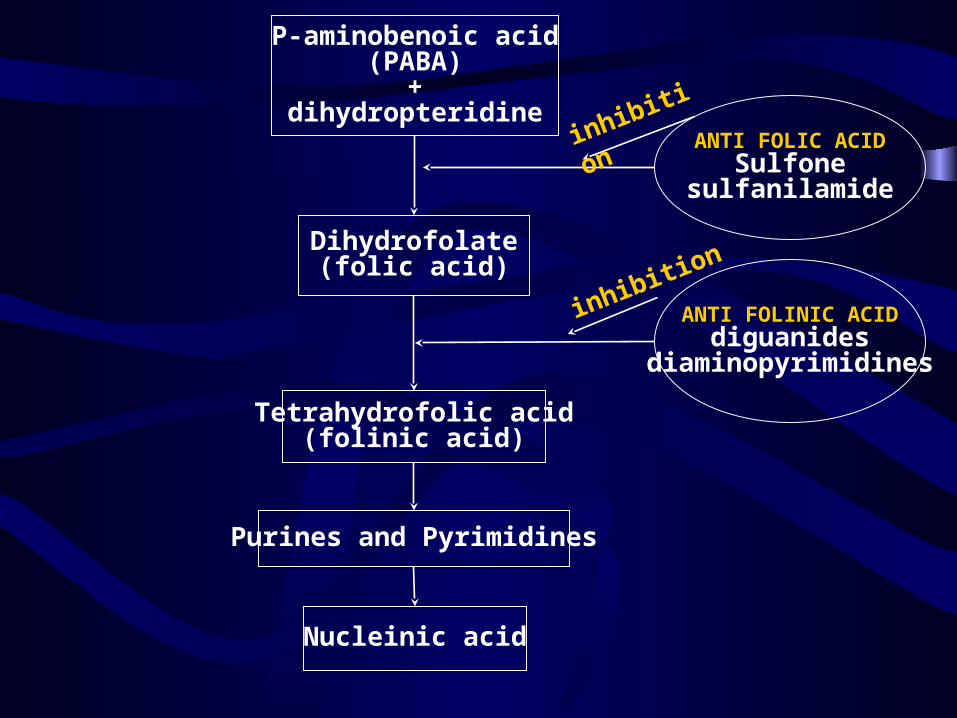
P-aminobenoic acid(PABA)
+dihydropteridine
Dihydrofolate(folic acid)
Tetrahydrofolic acid(folinic acid)
Purines and Pyrimidines
Nucleinic acid
ANTI FOLIC ACIDANTI FOLIC ACIDSulfone
sulfanilamide
ANTI FOLINIC ACIDANTI FOLINIC ACIDdiguanides
diaminopyrimidines
inhibition
inhibition
– 2) Tissue schizonticides (Primaquine)
– Effect on the stages in liver (including hypnozoit
e), use for prevent relapse (radical cure) of P.v or
P.o malaria
• 2. Choice of drugs– 1) Treatment of vivax, malariae, ovale and chloroqui
ne-sensitive falciparum malaria: chloroquine– 2) Radical cure of vivax or ovale malaria: chloroquin
e + primaquine– 3) Treatment of chloriquine-resistant falciparum mala
ria: artemisinin or mefloquine or quinine

Transmission and Prevention
• 1. Factors of transmission– 1) Infected human (gametocyte-bearing)– 2) Suitable species of anopheles (60 species are
considered to be vectors of malaria, major vectors in China: A. sinensis, A. minimus)

– 3) Resistance of Anopheles to insecticides of re
sistance plasmodium to antimalarial drugs.
– 4) Susceptible population
– 5) Other transmission mode: by transfusion, syr
inge, congenital transmission
• 2. Prevention: breaking the human-mosquito-human cycle
– 1) Control of the source of infection by chemotherapy
– 2) Control of transmission route: • residual insecticides, avoidance of infected mosquitoes (b
ed nets impregnated with permethrin; mosquito repellents (diethyl-metatoluamide)
– 2) Chemoproplylaxis
taking suppressive drugs, beginning one week b
efore travel to endemic area and continuing unti
l 6 weeks after return
– 3) Malaria vaccines

Flagellate
Phylum sarcomastigophora
Class zoomastigophorea
Leishmania donovani
杜氏利什曼原虫

General Introduction
• Zoonotic parasite
• One of the 5 major parasitic diseases
• Endemic northern to Yangtse river
• 0.5 million patients before 1949
• Basically eradicated in 1958

Visceral leishmaniasis has a wide geographic distribution.
Morphology
• Amastigote (leishman-donovan body):– Human phase, reside in macrophage– Very, very minute elliptical body – No free flagellum– Nucleus: deep red, located at one side– Cytoplasm: blue (after right stain)– Kinetoplast: basal body; rhizoplast

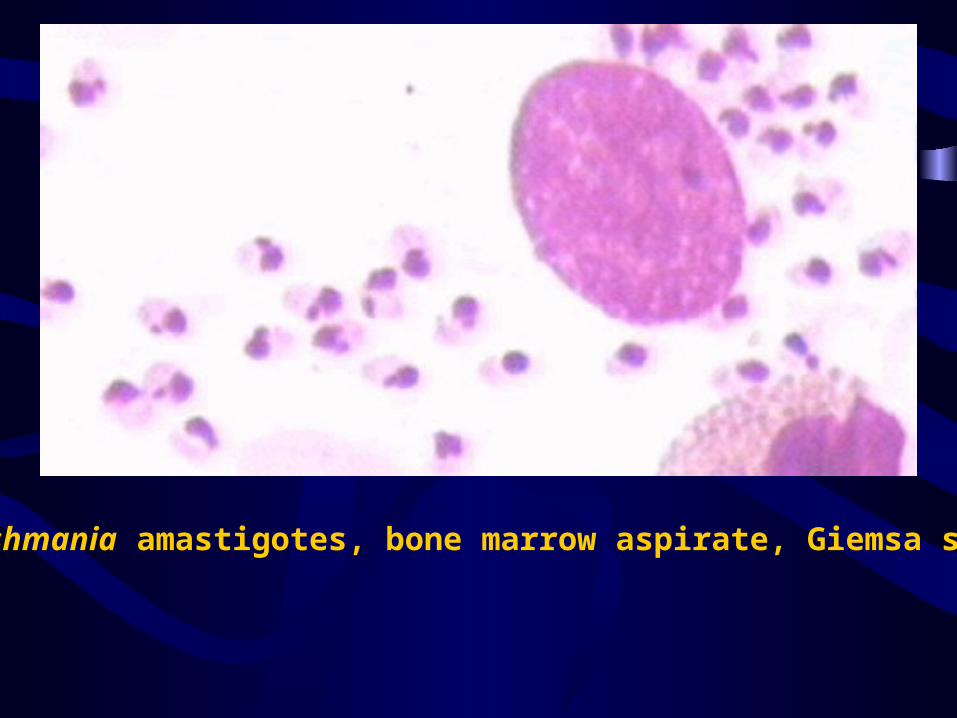
Leishmania amastigotes, bone marrow aspirate, Giemsa stain

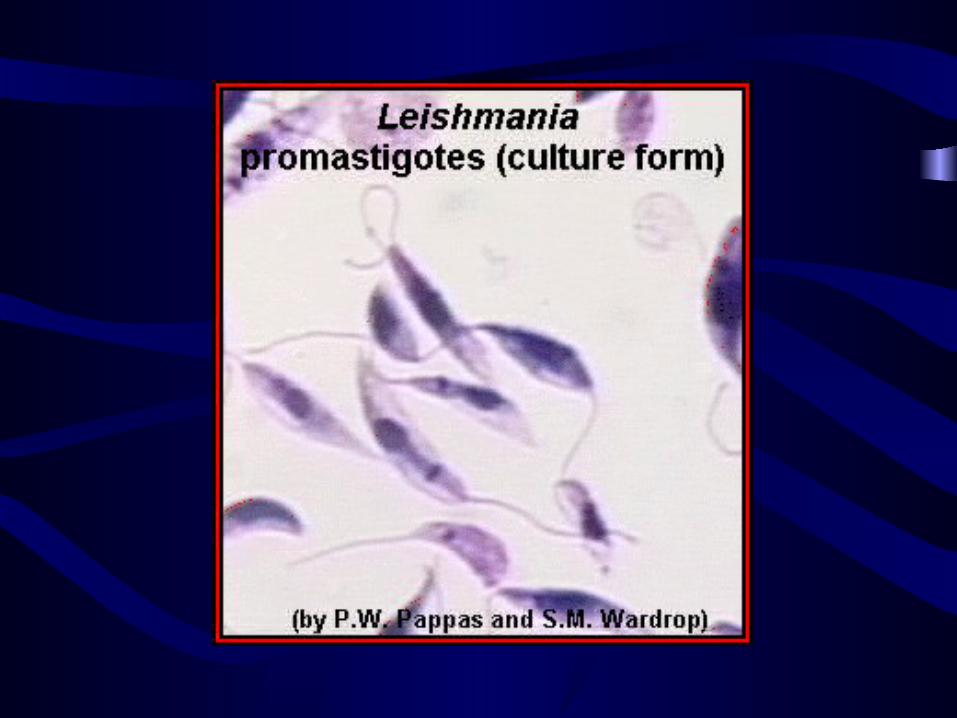
• Promastigote:– Vector phase– Reside in the gut of sandfly– Spindle shaped with 1 free flagellum– Nucleus; cytoplasm; kinetoplast; basal body; rh
izoplast– Chrysanthemum-like in culture medium
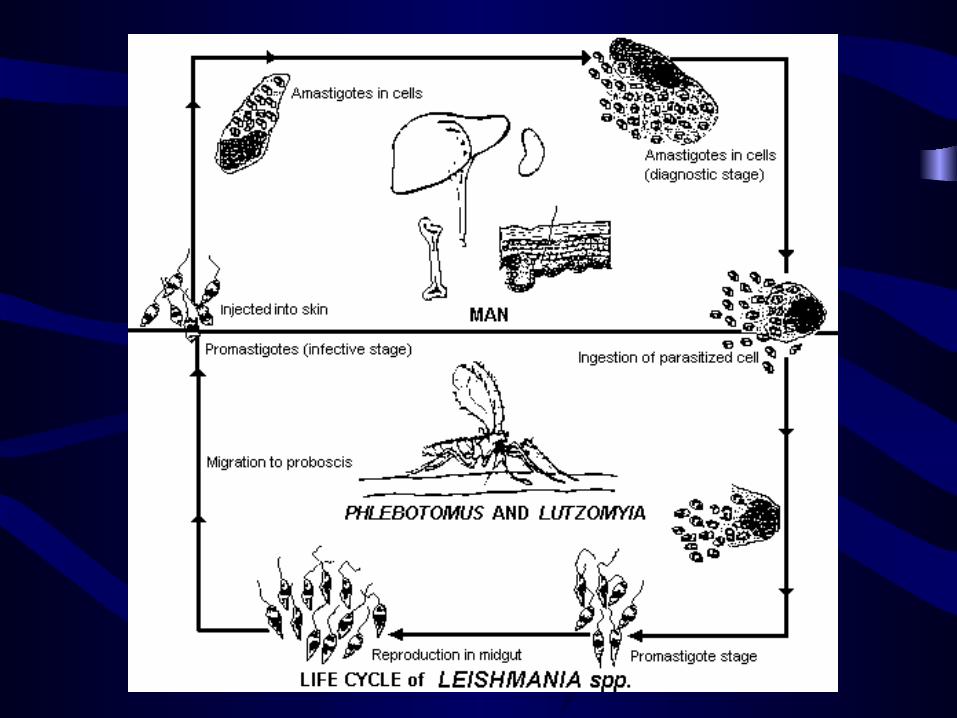
Main Points of Life Cycle
• Host: man and sandfly
• No sexual development in the host
• Residing site: macrophage
• Infective stage: promastigote
• Infective route: inoculation of sandfly
• Reservoir host: dog
• Infection could also via transfusion
Clinical Feature
• Irregular, long term fever
• Skin pigmentation—Kala-azar (india)
• Very poor prognosis: die within 1-2 year without treatment
• Reason: lack of immunity after infection;
• But may gain sterilizing immunity after effectively cured
Clinical Manifestation
• Hepatosplenomegaly
• Pancytopenia (hypersplenofunction, immune lysis)
• Epistaxis (nosebleed)
• Nephrosis: albuminuria, hematuria
• Skin lesion: PKDL
• Enlargement of lymphaden
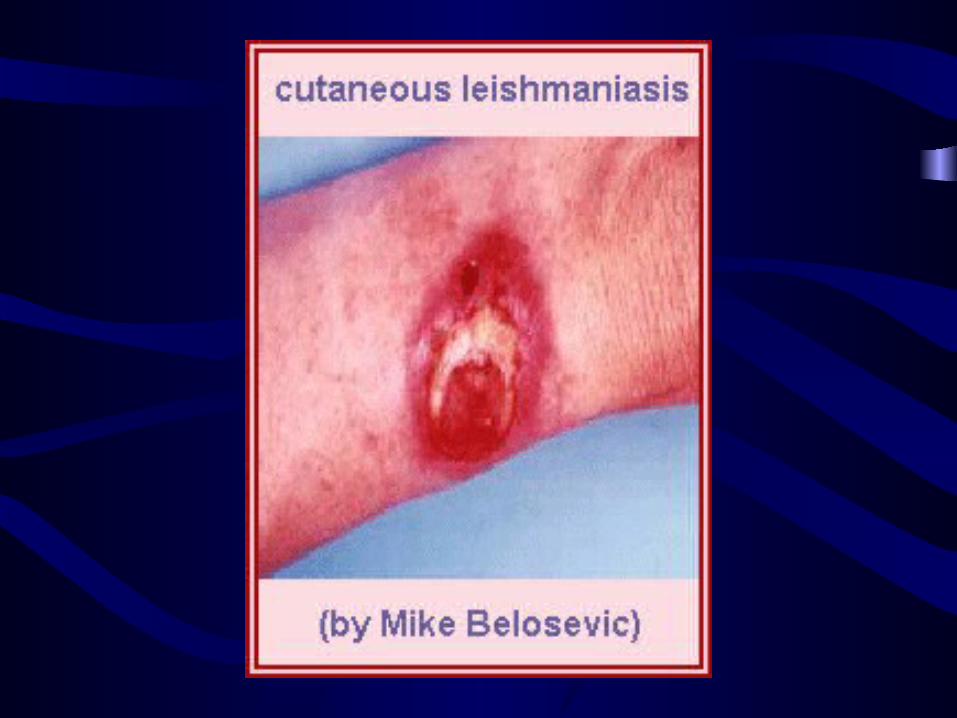

Cutaneous leishmaniasis of the face
Laboratory Diagnosis
• Etiological diagnosis• Puncture smear
– Bone marrow: safe, of first choice
– Lymphaden: treatment evaluation
• Skin biopsy• Tissue cultivation• Animal inoculation• Probe test: DNA or McAb
Epidemiology
• Cosmopolitan: Asia, Africa, Latin, America
• Distribution in China—3 types of areas
• Plain type– Shangdon, dom. P.sinensis
• Hilly type– Qinghai, wild P.sinensis
• Desert type– Xinjiang, wild P.sinensis
The infection is transmitted by various species of Phlebotomus, the sand fly.

Epidemic Links
• Source of infectin: patients and dogs
• Route of infection: phlebotomus spp.
• Susceptible population: all human beings ( but potent immunity developed after cure)

Control
• Treatment of patients: • Sodium stibogluconate• Kill infected dogs• Eradicate sandfly: weak points
– Limited flying capacity– Long breeding course– Short seasonal prevalence– Sensitive to insecticide
Reasons for a Successful Control in China
• Free charge of treatment
• Potent immunity after being cured
• Large production effective drug
• Weak points of sandfly
Giardia lambia
蓝氏贾第鞭毛虫
Morphology
• Trophozoite– Like badminton racket / “gost face”– 2 discs– 2 nuclei– 4 pairs of flagella– Axostyles
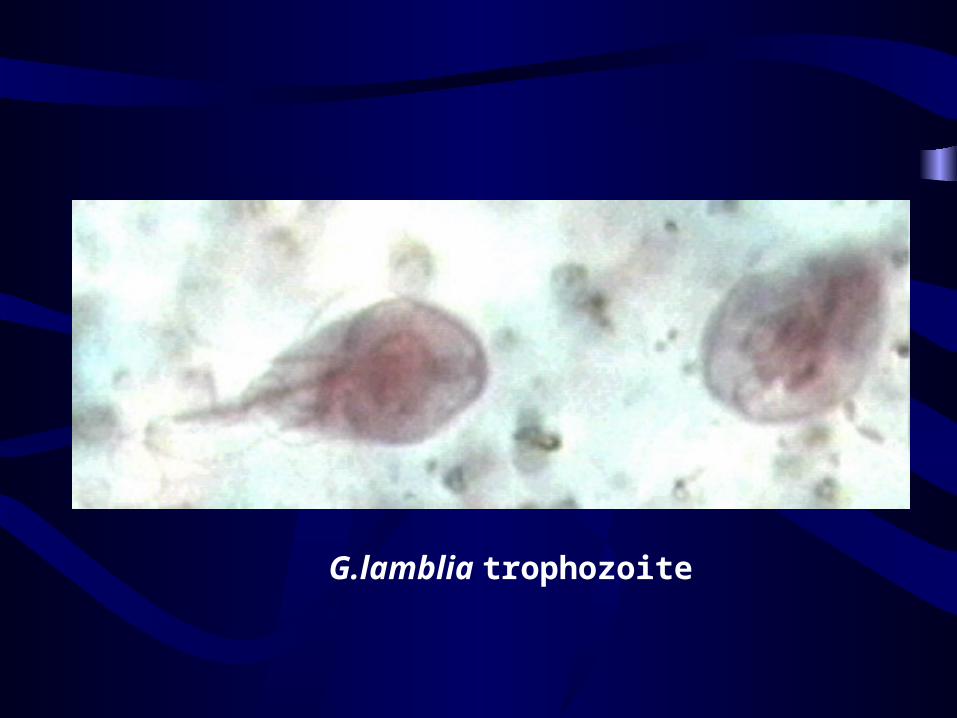
G.lamblia trophozoite
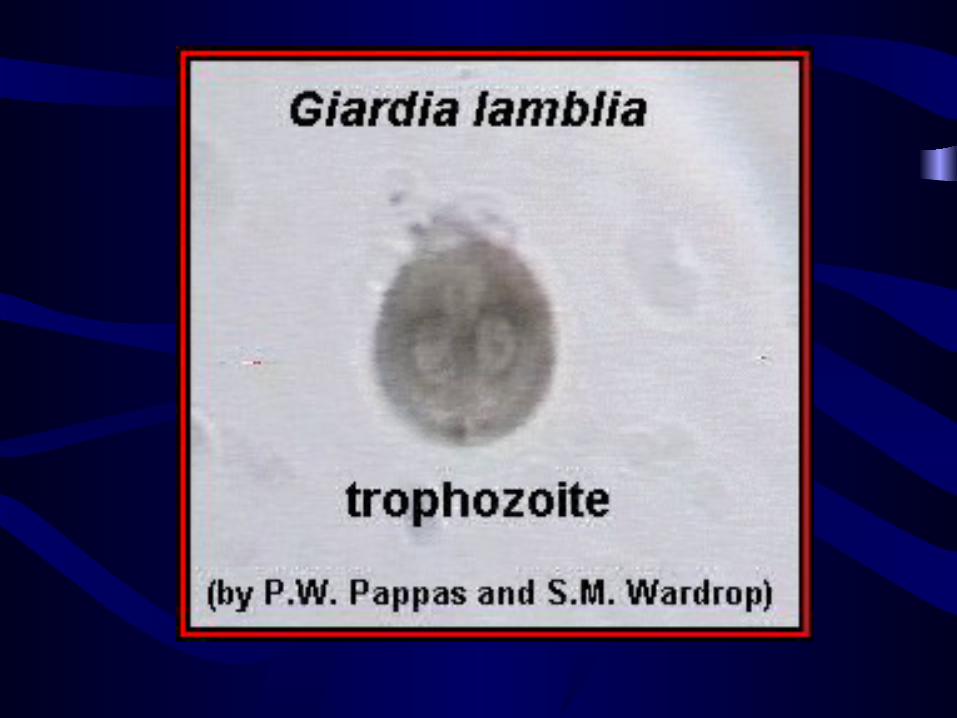

Another example of a Giardia lamblia trophozoite. The two nuclei are easy to see in this image.
• Cyst
– Ellipsoid
– Wall
– 4 nuclei
– Shrunken cytoplasm
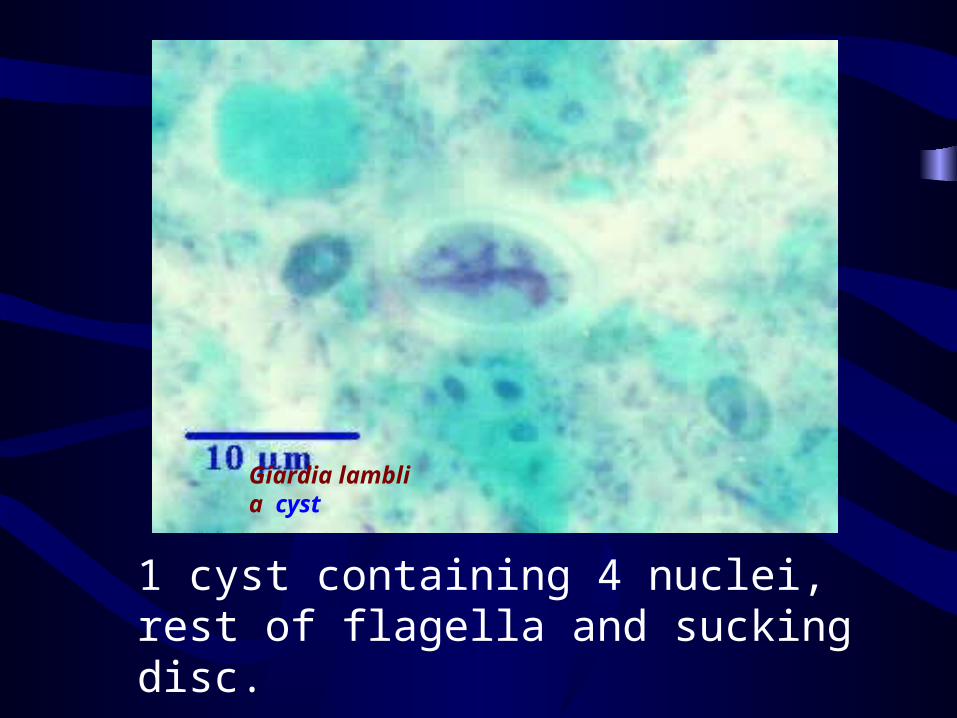
Giardia lamblia cyst
1 cyst containing 4 nuclei, rest of flagella and sucking disc.
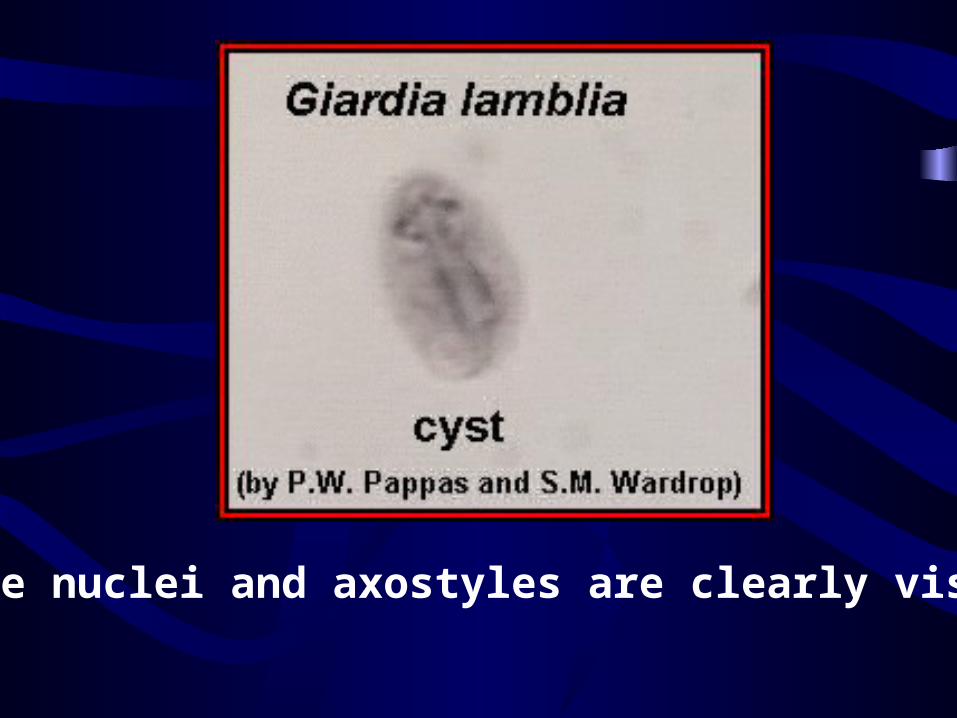
The nuclei and axostyles are clearly visible.
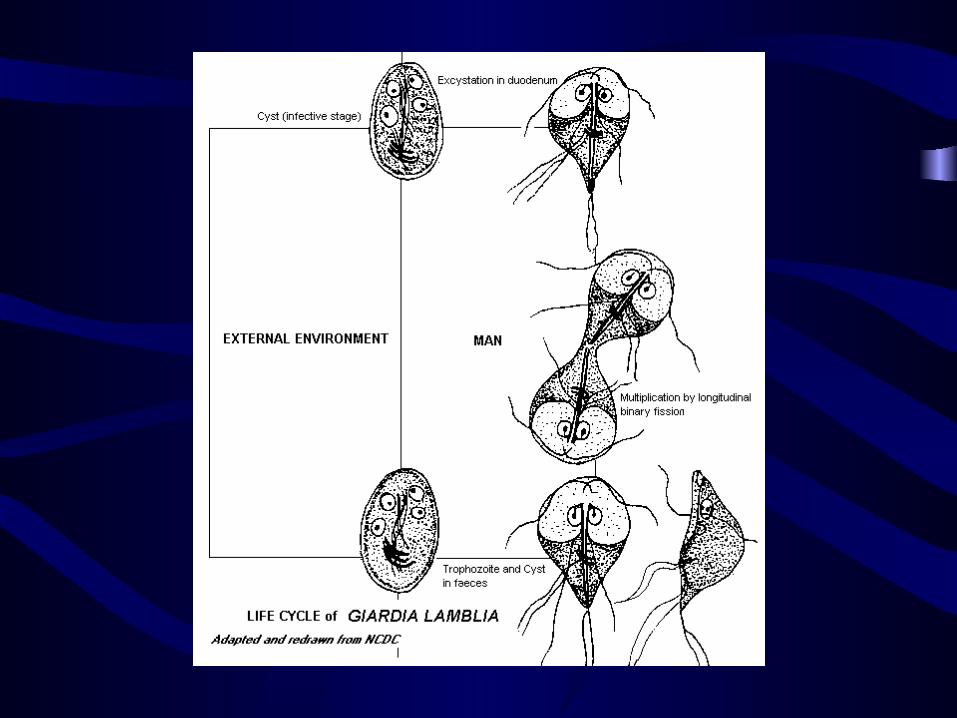

Main Points of Life Cycle
• Host: human being
• Residing site: small intestine
• Infective stage: 4 nuclei cyst
• Infective route: mouth
Clinical aspects
• Vomiting
• Flatulence
• Diarrhea
• Malabsorption syndrome
• Cholecystitis
Diagnosis
• Examination of stool for trophozoite or cyst
• Duodenal aspiration

Epidemiology
• Cosmopolitan
• Source of infection: carriers and patients
• Transmission route: faeces----mouth
• Susceptible population: traveler, AIDS patients, homosexual population

Prevention and Control
• Patients and carriers: metronidazole
• Water & nightsoil control
• Insect vector control (fly, cockroach)
• Personal hygienic health education
Opportunistic ProtozoaOpportunistic Protozoa
Opportunistic Parasite
• Parasites which are not normally pathogens but become so due to impairment of host resistance.
• These are assuming increasing clinical importance in AIDS epidemic.
• Opportunistic protozoa – Toxoplasma gondii, Giadia lamblia, etc.

Toxoplasma gondiiToxoplasma gondii
刚地弓形虫刚地弓形虫
General Features
• A world wide distribution : 1/3 population
• Opportunistic parasite
• Intracellular parasite
• Zoonotic parasite
Life Cycle and Morphology
• Two host pattern with alternation of
generation
• Definitive host: cat (acts also as I.H.)
• Intermediate host: human being and other
animals (herbivores, carnivores, omnivores)
Development in Cat
• Intestinal phase (sexual and asexual stage)
Schizogony merozoites (schizont)
Gametogony: micro and macrogametocyte m
icro and macrogamete zygote oocyst
Sporogony: sporozoites (mature oocyst) (outsid
e of the cat)
Development in Man
• Extraintestinal phase (asexual)– Infective stage
• Oocyst
• Tachyzoite
• Cyst
• Infective route: mouth
• Residing site: tissue cells


T. gondii: lysis of a THP-1 cell with release of tachizoites in culture.

Tachyzoites of Toxoplasma gondii in macrophages of mouse in peritoneal exudate. (SEM)
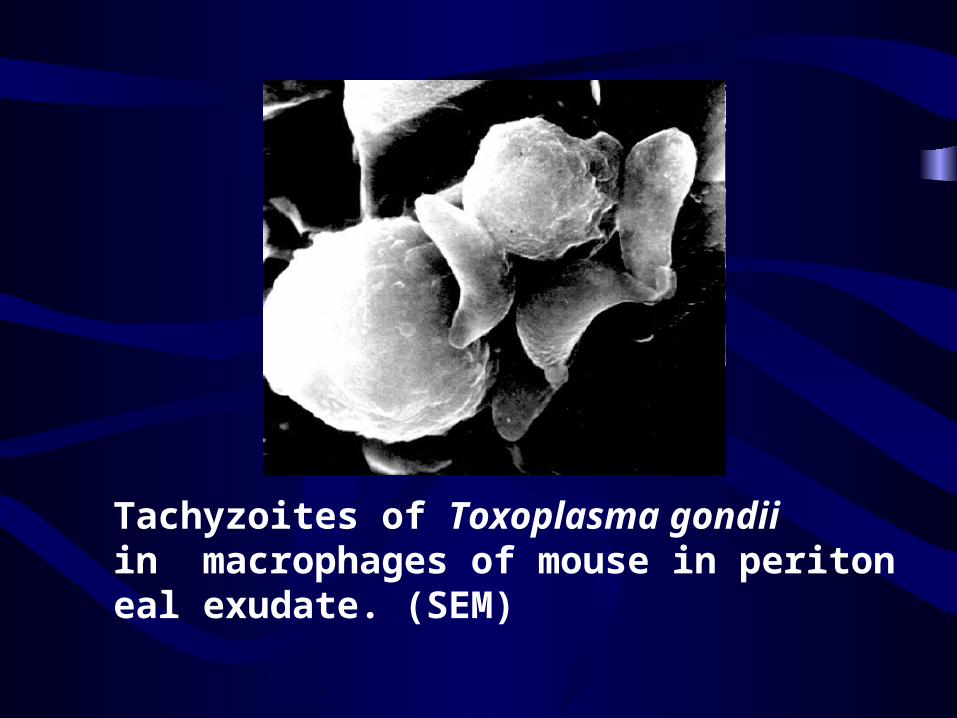
Tachyzoites of Toxoplasma gondii in macrophages of mouse in peritoneal exudate. (SEM)

In cell cultures, T.gondii proliferates to form a pseudocyst of 8-20 parasites.
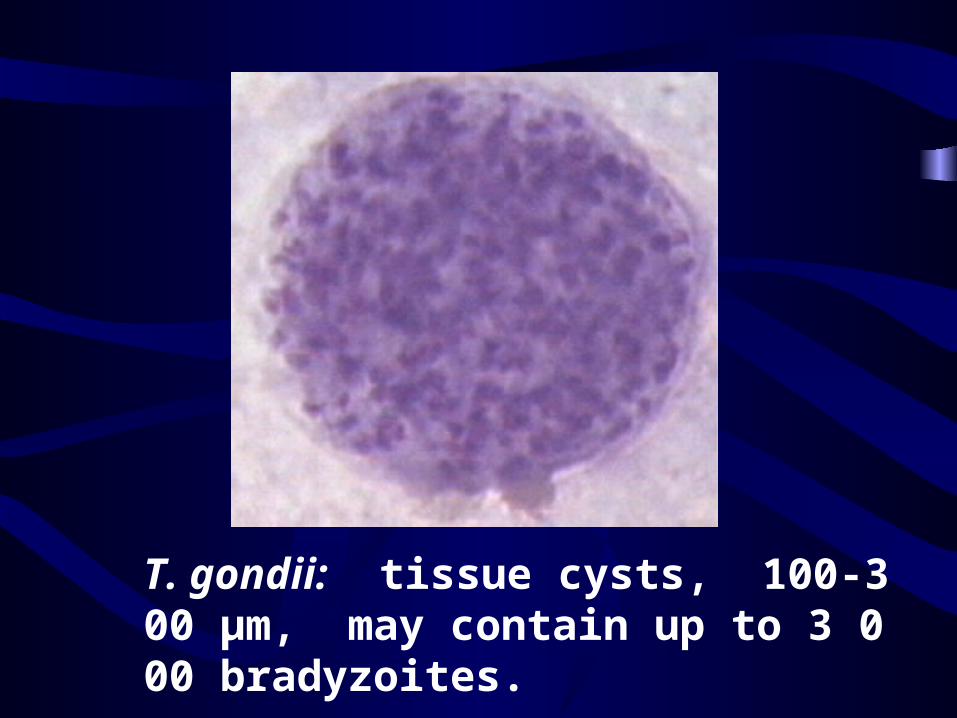
T. gondii: tissue cysts, 100-300 µm, may contain up to 3 000 bradyzoites.
Pathogenesis
• Acquired toxoplasmosis: eye lesion (uveitis,
choroiditis, choroidoretinitis); lymphadenop
athy
• Congenital toxoplamosis:
– Abortion;
– Still birth (abnormities): hydrocephalus, menta
l retardation

Pathogenesis
• Toxoplamosis in immunoincompetent hosts
– Encephalitis
– Pneumonitis
– Myocarditis
– Hepatitis, etc.
Diagnosis
• Immunological diagnosis of specific IgG or IgM (first choice), eg:DT, ELISA, IFA, IHA, etc
• Histological exams
• Animal inoculation
• PCR
Main Points
• Multi-cellular parasitism
• Transmission mode– Congenital– I.H. I.H– D.H I.H– I.H D.H
Epidemiology
• Cosmopolitan
• France: 45-85%
• Africa: 46%
• USA : 25-36%
• China : 30%
Epidemiological Factors
• Consuming raw or undercooked meat contai
ning cyst
• Contact with cats ( oocyst consumption)
Prevention Control
• Drug: pyrimethamine +sulfadiazine spira
mycin (for pregnant women)
• Avoid contact with the cats ?
• Avoid eat raw or undercooked meat