introduction basic science clinical aspects platelets
TRANSCRIPT
2/8/2012
1
IntroductionBasic science clinical aspectsPlatelets
P2Y12Pro thrombotic factors
Thrombin
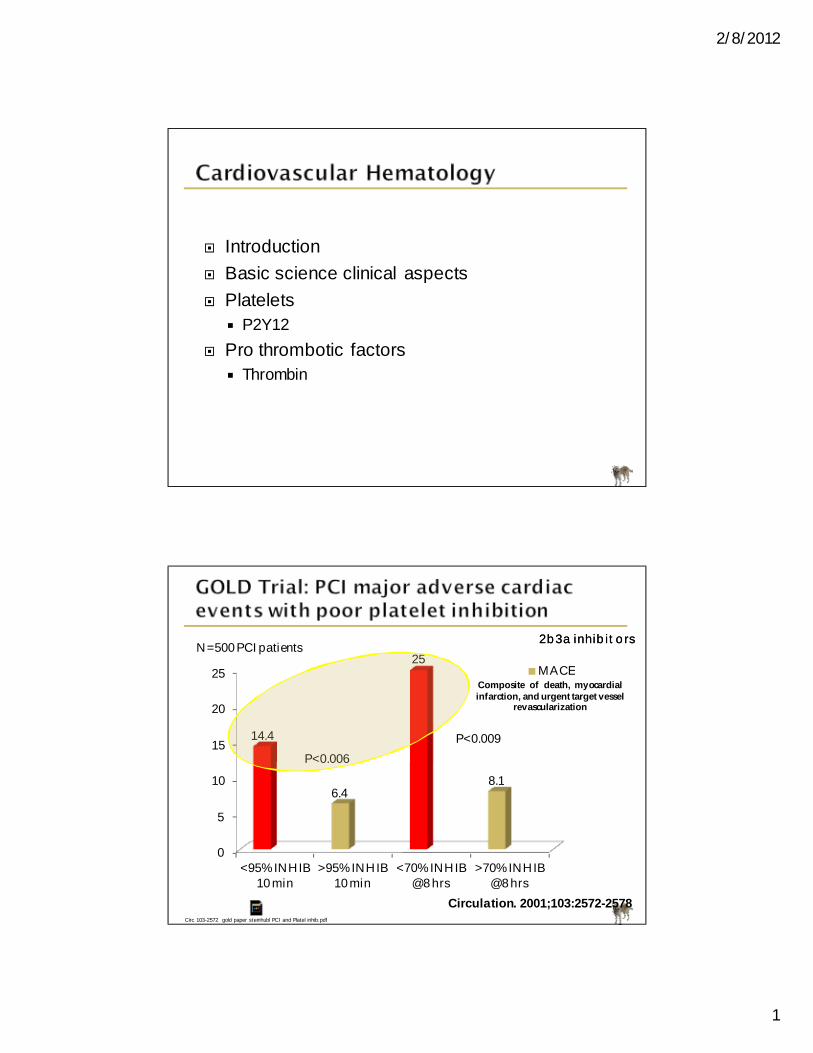
0
5
10
15
20
25
<95% INHIB 10 min
>95% INHIB 10 min
<70% INHIB @ 8 hrs
>70% INHIB @ 8 hrs
14.4
6.4
25
8.1
MACE
P<0.009P<0.006
N=500 PCI patients2b3a inhibitors2b3a inhibitors
Circulation. 2001;103:2572-2578Circ 103-2572 gold paper steinhubl PCI and Platel inhib.pdf
Composite of death, myocardialinfarction, and urgent target vessel
revascularization

2/8/2012
2
45 y/o Hispanic women45 y/o Hispanic women--type 2 DMtype 2 DM
molecular changes during MI.pdf
Events leading to Reperfusion Events leading to Reperfusion Induced “ Induced “ inflammatoryinflammatory “ Injury“ Injury
Ambrosio Am Heart J 1999;138:s69
01020304050607080
40 minutes 3 hours 6 hours Closed
28
70 7279
% Necrosis
Reperfused @
Reimer KA. Lab Invest. 1979 Jun;40(6):633-44
Most viable area subepicardial tissue
Time is Muscle

2/8/2012
3
Basic science
Highlight summary
Poor platelet inhibition is associated with increased CV risk
Time is muscle…70% of heart muscle dead in 120 minutes w/o blood
Highlight summary
Poor platelet inhibition is associated with increased CV risk
Time is muscle…70% of heart muscle dead in 120 minutes w/o blood
Healthy vascular endothelium Prevents
Platelet adhesion and activation
(antithrombotic factors)
CD39 (ectoADPase), prostaglandin, nitric oxide, heparin, matrix
metalloproteinase-9,protein S, and thrombomodulin
2/8/2012
4
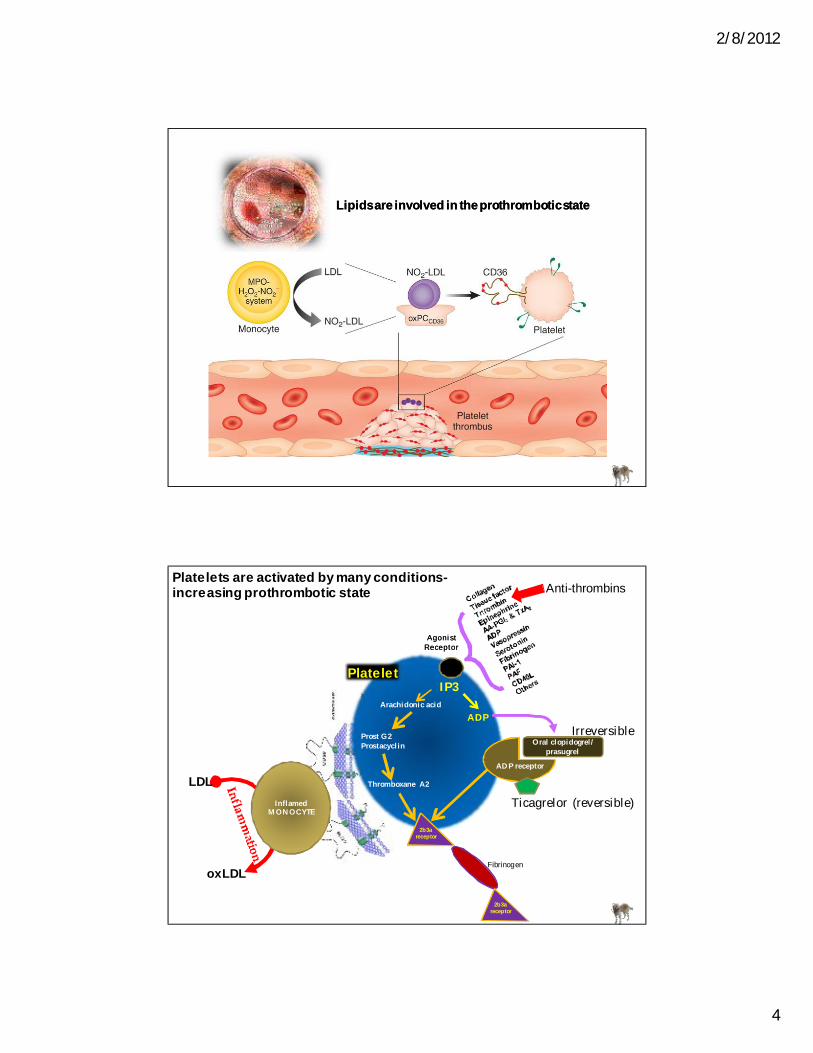
Lipids are involved in the prothrombotic stateLipids are involved in the prothrombotic state
LDL
oxLDL
InflamedMONOCYTE
IP3
ADPTxA2others
Platelets are activated by many conditions-increasing prothrombotic state
Platelet
2b3a receptor
Fibrinogen
IP3
ADP
Anti-thrombins
Arachidonic acid
ADP receptor
Prost G2Prostacyclin
Thromboxane A2
AgonistReceptorAgonist
Receptor
Oral clopidogrel/ prasugrel
Irreversible
Ticagrelor (reversible)
2b3a receptor

2/8/2012
5
Chest pain for 2 hours …waited in University ER for 8 hours
Microparticles with tissue factor are released
Microparticles with tissue factor are released
Tissue Factor bearing cell
Prothrombin
ThrombinThrombinVa
Factor XFactor X
Xa PlateletPlatelet
VIII/vWFOthers
Activated platelets
FibrinogenFibrinogen
FibrinFibrin
ClotClot

2/8/2012
6
Platelets and P2Y12
Highlight summary
Healthy vascular endothelium protects from atherothrombotic events
Elevated oxLDL/inflammation increased platelet and prothrombotic risk
Thrombin/tissue factor others activate platelets
Highlight summary
Healthy vascular endothelium protects from atherothrombotic events
Elevated oxLDL/inflammation increased platelet and prothrombotic risk
Thrombin/tissue factor others activate platelets
Molecular Steps in Platelet ActivationMolecular Steps in Platelet Activation
P2Y12 Inhibits adenylyl cyclase (AC) and a decrease in cyclic AMP (cAMP)
P2Y12 Inhibits adenylyl cyclase (AC) and a decrease in cyclic AMP (cAMP)
Nat Rev Drug Disc Bhatt 2- 15 p2y12 +++++++.pdf
3 subtypes of P2 receptors: P2X1, P2Y1, and P2Y12
Activation of P2Y12 receptor -responsible for sustained platelet
aggregation and secretion
Activation of P2Y12 receptor -responsible for sustained platelet
aggregation and secretion
Activated platelets secrete ADP, platelet-derived growth factor, and thromboxane
A2 (TXA2). ADP and TXA2 cause circulating platelets to change shape and
become activated.
Thromboxane A2 (TXA2), adenosine diphosphate (ADP),
thrombin, serotonin, epinephrine, and collagen
Platelet ActivatorsPlatelet Activators
2/8/2012
7
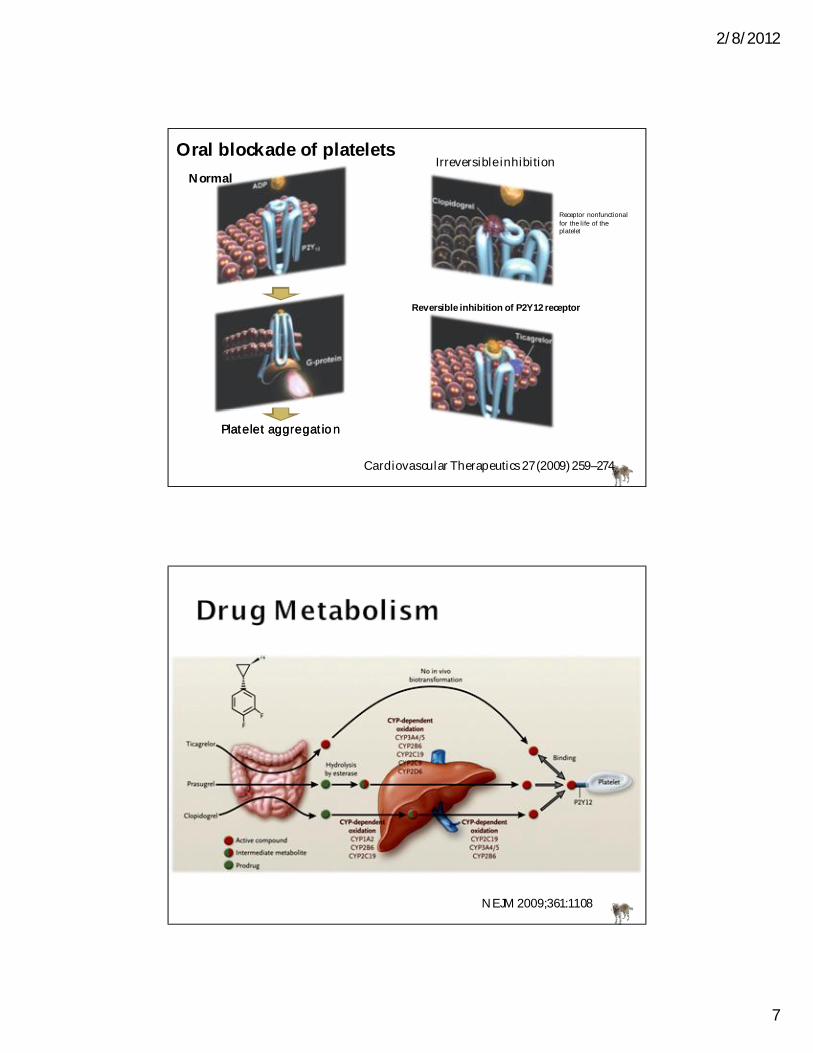
Platelet aggregationPlatelet aggregation
Irreversible inhibition
Reversible inhibition of P2Y12 receptor
Receptor nonfunctional for the life of the platelet
Normal
Cardiovascular Therapeutics 27 (2009) 259–274
Oral blockade of platelets
NEJM 2009;361:1108

2/8/2012
8
Inhibition of Platelet
Aggregation* Route Peak EffectOffset of Action
Consistency of Response
Clopidogrel 300 mg ~30% Oral ~ 4 hours ~5 days +Clopidogrel 600 mg ~40% Oral ~ 4 hours ~5 days ++
Prasugrel 60 mg 75–80% Oral 1 hour ~5 days +++AZD6140 90 mg BID 75–80% Oral 1–2 hours 1–2 days +++Cangrelor >90% IV minutes 20 min +++
SCH 530348 2.5 mg daily (>90% to TRAP) Oral
With load: hours Without load: days Weeks +++
Sabatine MS. Cleve Clin J Med. 2009;76 Suppl 1:S8-15.
Emerging Antiplatelet Therapies
*Adenosine 5'-diphosphate (ADP)-induced aggregation to ADPBID, twice daily; TRAP, thrombin receptor antagonist peptide
nejm plato 1045.pdf
SCH 530348 par 1 Lancet 373- 919.pdf
020406080
100120140160
30 ug 100 ug 15 ug 30 ug
114
150
109
140
AdenosineTicagrelor
Circulation 2007;116(Suppl):II-28:A-245
Perc
ent o
f Bas
elin
e
S. Husted and J.J .J . van Giezen CV Therap 27- 259 adenosine.pdf

2/8/2012
9
S. Husted and J.J .J . van Giezen CV Therap 27- 259 adenosine.pdf
Cardiovascular Therapeutics 27 (2009) 259–274
Abciximab is an ant ibodyAbciximab is an ant ibodySmall peptides
Type Monoclonal antibodyfragment
Small Molecular(KGD
sequence)
Small Molecular(RGD
sequence)Platelet bound
half lifeHours Seconds Seconds
Plasma half live Minutes 2.5 hours 1.8 hours
Drug to receptor ratio
1.5-2.0 250-2500 >260
½ of dose in bolus
75% <2-5% <2-5%
Renal adjust NONE YES YES
2b/3a receptor2b/3a receptor
FibrinogenFibrinogen
Platelet
IV platelet inhibition

2/8/2012
10
Only Abciximab is an antibody (do not repeat 2 weeks)Only Abciximab is an antibody (do not repeat 2 weeks)
Small peptides
Type Monoclonal antibody fragment
Small Molecular(KGD sequence)
Small Molecular(RGD sequence)
IIb/IIIa xxx xxx xxx
avb3 xxx x
Mac-1 x
Thrombingeneration
xx x x
ACT ++30 seconds +20 seconds 0
Reversible withoutplatelets
24 hrs 4 hrs 4 hrs
Reversible with platelets
YES no no
2b/3a receptor2b/3a receptor
FibrinogenFibrinogen
Platelet
Clinical trials
Highlight summary
Irreversible binding to P2Y12 receptor…clopidogrel & prasugrel
Ticagrelor reversible binding to P2Y12, given bid in preclinical trials, and releases adenosine in animal studies
IV 2b/3a inhibitors: 7E3 is antibody and should not be given for 2 weeks after treatment, but is the only platelet reversible compound
Highlight summary
Irreversible binding to P2Y12 receptor…clopidogrel & prasugrel
Ticagrelor reversible binding to P2Y12, given bid in preclinical trials, and releases adenosine in animal studies
IV 2b/3a inhibitors: 7E3 is antibody and should not be given for 2 weeks after treatment, but is the only platelet reversible compound

2/8/2012
11
Irreversible P2Y12 receptor antagonistProdrug metabolized by CYP450 enzymesCYP2C19 reducedreduced--functionfunction allele (CYP2C19*2) associated with 32% reduction in exposure to active metabolite of clopidogrel
Mega JL, et al. N Engl J Med. 2009;360(4):354-362.
Acute (<1 month)•N=544•Coronary stenting/ volunteers/ HF/stroke
Long term (>1 month)•N=359•Coronary stenting/stroke
41.9 ±20.8%* 52.9 ±8.1%*
Serebruany VL, et al. Am Heart J. 2007;153(3):371-377.Serebruany VL, et al. J Am Coll Cardiol. 2005;45(2):246-251.
*Mean ±SD
0 10–20 30–40 50–60 70–80 >90
5 M ADP Platelet Aggregation (%)
60
120
180
0
Inhibition of Platelet Aggregation (%)
35–40 41–45 45–50 51–55 56–60 61–65 66–70
40
0
20
60
80
100
No.
of
Pati
ents
No.
of
Pati
ents

2/8/2012
12
Pharmacogenomics of Antiplatelet Intervention Study (PAPI)7 days clopidogrelN=429 healthy Amish Platelet aggregometryGenome wide association study
JAMA. 2009;302(8):849-858
Carriers of the CYP2C19*2 genotype have higher cardiovascular Carriers of the CYP2C19*2 genotype have higher cardiovascular event rates compared with event rates compared with noncarriersnoncarriers
(20.9% vs 10.0%; hazard ratio [HR], 2.42; 95% CI, 1.18-4.99; P=.02)
CYP2C19 reducedreduced--functionfunction allele (CYP2C19*2) associated with 32% reduction in exposure to active metabolite of clopidogrel JAMA. 2009;302(8):849-858

2/8/2012
13
White population: 24% have at least 1 alleleMexican population: 18%African American population: 33%Asian population: 51%
Clin Pharmacol Ther. 2006;80(1):33-40Pharmacogenetics. 1996;6(3):265-267
FDA…The CYP2C19*2 and *3 alleles have no functional metabolism of Plavix.
GI absorption is limited by the P-glycoprotein efflux-transporter encoded by the adenosine triphosphate-binding cassette containing gene ABCB1, also known as the multidrug resistant (MDR1) gene
AMI populationPrimary EP (death, nonfatal MI, or stroke at 1 year)
Abnormal genotype (carriers)-15.5%Normal genotype (noncarriers)-10.7% (HR 1.72 (1.20,2.47))
Patients with 2 CYP2C19 loss of function alleles and 1 ABCB1 variant allele----HR 5.31 (2.13-13.20)
JACC 2010;56:321ACCF-AHA Clopidogrel Clinical Alert JACC 56- 321 holmes.pdf

2/8/2012
14
Prospective, observational, single center, cohort studyN=1069All receive clopidogrel for PCI5 Tests
VerifyNOW P2y12Plateletworks assaysIMPACT-RPFA-100PFA P2YPrimary endpoint: all cause death, MI, thrombosis, stroke
JAMA. 2010;303(8):754-762
Platelet blockedHigh Reactivity0
5
10
15
6 5.7 6.1
11.7 13.3 12.6
% of Patients - Primary EP
All p<0.001
VerifyNow and Plateletworks good in post stent patients preds events JAMA 303- 754 Werkum.pdf
Amish studyPatients with the CYP2C19*2 variant (reduced function) were more likely (20.9% vs 10.0%) to have a CV ischemic event or death during 1 year of follow-up
Other studies support the clinical importance of risk allele CYP2C19*2Loss of function genotype varies in different ethic groupsCombination of both ABCB1 polymorphism with CYP2C19*2 increases risk for CV event 5X
Clopidogrel-CYP2C19*2 reduced function allele (drug not metabolized to active form). 150 mg qd increase cost to level higher than prasugrel

2/8/2012
15
Prasugrel..TRITON-TIMI 38 trial-FDA approvedTicagrelor..PLATO trial pending FDA approval
Contra-indication /caution by FDA-History of transient ischemic attack or stroke
75 years of age<60 kg
Prasugrel
Double-blind, randomized phase III
Wiviott SD, et al. N Engl J Med. 2007;357(20):2001-2015.
13,608 patientsACS (STEMI/NSTE ACS) and planned PCI
Treatment duration: 6–15 mo
Aspirin75–162 mg
•1° composite endpoint: CV death/nonfatal MI/nonfatal stroke•2° endpoints at 30 and 90 days: composite of CV death/nonfatal MI/nonfatal
stroke, composite of CV death/nonfatal MI/urgent target vessel revascularization (uTVR)
•2° endpoints: stent thrombosis; composite (CV death, nonfatal MI/stroke stroke, rehospitalizationfor cardiac ischemic event)
•Safety endpoints: TIMI major and life-threatening bleeds
Prasugrel.pdf

2/8/2012
16
Wiviott SD, et al. N Engl J Med. 2007;357(20):2001-2015.
Overall Days 0–3
Prasugrel: TRITON–TIMI 38
Days 3–450
1° composite endpoint: CV death/nonfatal MI/nonfatal
stroke
Randomized double blind, multicenter
Targeted number of 1780 primary endpoints
Primary endpoint @ 1 yearComposite: Death from v ascular disease, MI, Stroke
TicagrelorOral reversible, direct inhibitor of ADP receptor p2y12180 mg load90 mg bidStent thrombosis 71/5640 (1.3%)
Clopidogrel600 load75 mg qdStent thrombosis 106/5649 (1.9%) p<0.009
nejm plato 1045.pdf
N Engl J Med 2009;361:1045-57
0
5
10
15
Ticagrelor Clopidogrel
9.8 11.7
4.55.9
Primary EP Death Vascular Dx
1 year
ARR 1.9% (HR 0.84-0.77,0.92)
Major bleeding (not CABG)Ticagrelor 4.5%Clopidogrel 3.8%
P<0.03

2/8/2012
17
nejm plato 1045.pdf
Primary end point: death from vascular causes, MI, or stroke
N Engl J Med 2009;361:1045-57
STEMI-38%NSTEMI-42%PVDx-6.2%HT-65%Abn Lipids-46%DM-25%Prior MI-20%Statins-89%
NEJM 2009;361:1108

2/8/2012
18
First time in decades: new class of oral thrombin inhibitor
Non inferiority trialRandomized 18,113Atrialfibrillation
Risk for stroke
F/Y 2 yearsPrimary endpoint: preventionof stroke or systemic embolism
Non inferiority trialRandomized 18,113Atrialfibrillation
Risk for stroke
F/Y 2 yearsPrimary endpoint: preventionof stroke or systemic embolism
RELY trial dabigatran nejm 361- 1056.pdf
Dabig 110 mg (182/6015) 3%Dabig 150 mg (134/6076) 2.2%Warfarin (INR 2-3) (199/6022) 3.3%
ARR 1.1%ARR 1.1%P<0.001
150-mg dose of dabigatran was associated with lower rates of stroke and systemic embolism but with a similar rate of major hemorrhage N Engl J Med 2009;361:1139-51
NNT 90 for 2 yearsNNT 90 for 2 years

2/8/2012
19
Dabig 110 mg (182/6015) 3%Dabig 150 mg (134/6076) 2.2%Warfarin (INR 2-3) (199/6022) 3.3%
Dabig 110 mg (322/6015) 5.3%Dabig 150 mg (375/6076) 6.1%Warfarin (INR 2-3) (397/6022) 6.59%
ARR 1.1% (NNT=90 for 2 years)ARR 1.1% (NNT=90 for 2 years)
Major BleedingMajor Bleeding
Prevent stroke/systemic embolismPrevent stroke/systemic embolism
AR Increase 0.49% (NNH=204 for 2 years)AR Increase 0.49% (NNH=204 for 2 years)
RELY trial dabigatran nejm 361- 1056.pdf N Engl J Med 2009;361:1139-51
204 patient treated for 2 years with dabigatranbefore 1 major bleed
was prevented vs warfarin
prevent 2 strokes if treat 200 patients for 2 years 1 bleed for each 200 patients treated for 2 years
Dabigatran-RE-LY trial reduces strokes in Afib vswarfarin (direct thrombin inhibitor)New agents-pending
Factor Xa inhibitorsRivaroxaban (Xarelto)
Bayer/J&JROCKET-AF
Stroke prevention studyAHA Nov 2010
ApixabanBristol-Myers Squibb/PfizerFDA application on f ileARISTOTLE
2011AVERROES trial
Lower strokes and systemic embolic events vs ASAFXa and its co-factor FVa form the prothrombinase complex, which activates prothrombin to thrombin

2/8/2012
20
Condition Points
C Congestive heart failure 1
H
Hypertension: blood pressure consistently above 140/90 mmHg
(or treated hypertension on
medication)
1
A Age >/=75 years 1
D Diabetes Mellitus 1
S2 Prior Stroke or TIA 2
Annual Stroke Risk
CHADS2Score
Stroke Risk %
95% CI
0 1.9 1.2–3.0
1 2.8 2.0–3.8
2 4.0 3.1–5.1
3 5.9 4.6–7.3
4 8.5 6.3–11.1
5 12.5 8.2–17.5
6 18.2 10.5–27.4
Score Risk Anticoagulation Therapy Considerations
0 Low Aspirin Aspirin daily
1 Moderate Aspirin or Warfarin
Aspirin daily or raise INR to 2.0-3.0,
depending on factors such as patient
preference
2 or greater Moderate or High Warfarin
Raise INR to 2.0-3.0, unless contraindicated
(e.g. clinically significant GI bleeding,
inability to obtain regular INR screening)
Risk factors and inflammation increases prothrombotic cardiovascular risk
Oral P2Y12 inhibitors have very different actions, but all work if platelets are inhibitedIV 2b/3a inhibitors: 7E3 is reversible with platelets
Atrial fibrillation patients: dabigatran (first direct oral thrombin inhibitor) was associated with lower rates of stroke and systemic embolism but with a similar rate of major hemorrhage to warfarin
Thank you