intro to infectious diseases and epidemiology of nosocomial infection
Upload: philippine-hospital-infection-contol-nurses-associaton-phicna-inc
Post on 14-Jan-2017
465 views
TRANSCRIPT

Arthur Dessi Roman, MD, MTM, FPCP,
FPSMIDInternal Medicine – Infectious Diseases
Infectious Diseases at the Forefront
@gonnabedess @gonnabedess
OutlineI. Why are infectious diseases unique
II. Introduction and Epidemiology of healthcare-associated infections

Most of them are communicable.Case of The Black Death Caused by Yersinia pestis carried by black rats one of the most devastating pandemics in human
history estimated to have killed 30–60% of Europe's
population reducing the world's population from an ~450M to between 350 and 375M in the 14th century
it took 150 years for Europe's population to recover
Why are infectious disease unique?
How infectious is MERS?
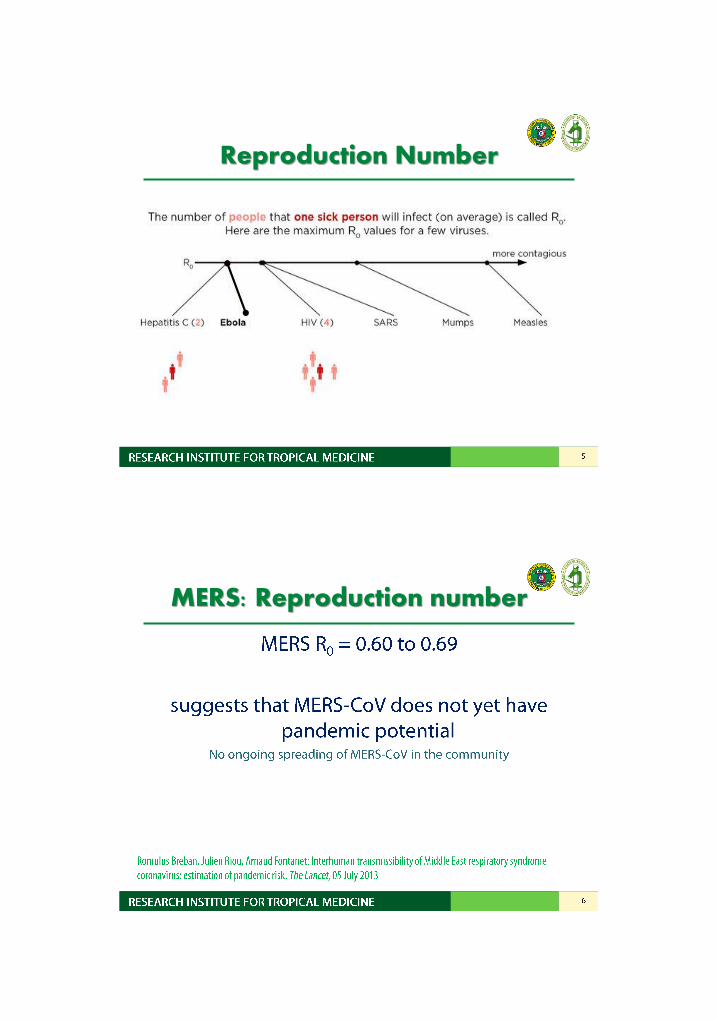
Reproduction Number
MERS: Reproduction number

There is sometimes a need for urgency for control.
Why are infectious disease unique?
MERS South Korean South Korean outbreak: May - July 2015
• Index case: 68/M, (+) travel to Bahrain, UAE, Saudi Arabia, and Qatar; diagnosed with MERS 9 days after initial medical consult
• Total of 186 cases with 36 deaths
Korean Centers for Disease Control and Prevention. Available from www.mers.go.kr. Accessed on 11 August 2015.
MERS Economic toll on South Korea
• Department store sales: down by 17% (June 2016)
• No. of people going to the movies, amusement parks, baseball games and museums also recorded large slumps, ranging from 38% to 82%
• No. of trips cancelled: 100,000 foreign travelers
• Tourist arrivals in the first 11 days of the month have fallen by 25%
http://www.businessinsider.com/mers-outbreak-hurting-korean-retail-and-tourism-2015-6
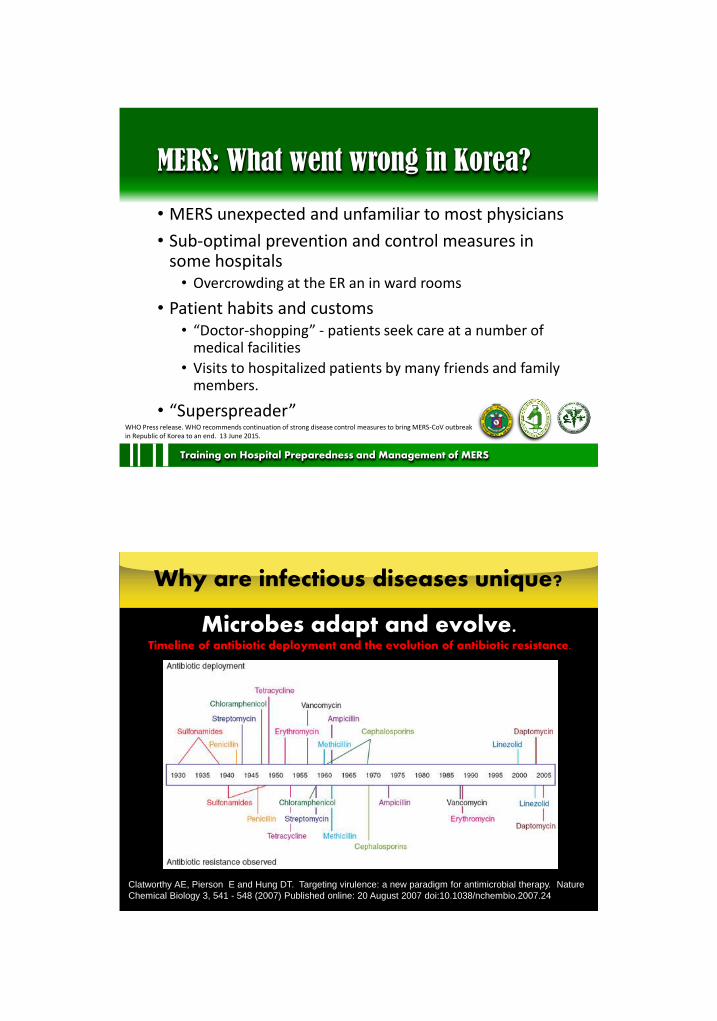
MERS: What went wrong in Korea?
• MERS unexpected and unfamiliar to most physicians
• Sub-optimal prevention and control measures in some hospitals
• Overcrowding at the ER an in ward rooms
• Patient habits and customs• “Doctor-shopping” - patients seek care at a number of
medical facilities
• Visits to hospitalized patients by many friends and family members.
• “Superspreader”
Training on Hospital Preparedness and Management of MERS
WHO Press release. WHO recommends continuation of strong disease control measures to bring MERS-CoV outbreak in Republic of Korea to an end. 13 June 2015.
Why are infectious diseases unique?
Microbes adapt and evolve.
Clatworthy AE, Pierson E and Hung DT. Targeting virulence: a new paradigm for antimicrobial therapy. Nature
Chemical Biology 3, 541 - 548 (2007) Published online: 20 August 2007 doi:10.1038/nchembio.2007.24
Timeline of antibiotic deployment and the evolution of antibiotic resistance.

They are sometimes occur with environmental, ecological and even behavioral events.
• Ondoy left Metro Manila flooded in September 26, 2009
• DOH: 2,272 leptospirosis cases, 174 deaths between October 1 and November 3, 2009 in 15 hospitals in Metro Manila.
• peak incidence reached
2-3 weeks after
Why are infectious diseases unique?
Factors Leading to the Emergence of Infectious Diseases in the 21st Century

Factors Leading to the Emergence of Infectious Diseases in the 21st Century
They know NO boundaries.
Why are infectious diseases unique?
Before:9 countries affected (1970)
Now:~50 million dengue infections worldwide every year (WHO)
and 2/5 of the world's population at risk in over 100
countries
attributed to expanding geographic distribution of the
mosquito vectors, predominantly Aedes aegypti
Average annual number of dengue cases reported to the WHO, and of countries reporting dengue, 1955–2007.

Why are infectious diseases unique?
• Started in Mexico, with its greatest burden of critical illness and death occurring between March 18- June 1, 2009
• In 6 weeks, it has spread as far as previous pandemic influenza viruses have spread within six months.
• continues to be the dominant influenza virus in circulation in the world comprising more than 60% of all influenza positive specimens reported to WHOInfluenza A(H1N1)
They know NO boundaries.
Why is PH concerned about the threat of EIDs?
•
•
•

Why is PH concerned about the threat of EIDs?
3,983,627 tourists (Jan-Sep 2015)
10.76% higher than 2014
46.7 % are foreigner
Why is PH concerned about the threat of EIDs?

Why are infectious diseases unique?
Disease Associated Etiologic Agent
CAD and stroke Chlamydia pneumoniae, atypical microorganisms, Mycoplasma
Deafness, hearing loss Lassa fever virus
Gastric & duodenal ulcer Helicobacter pylori
Infertility Chlamydia trachomatis
Cervical carcinoma Human papillomavirus
Hepatocellular Ca Hepatitis B and C viruses
Kaposi’s sarcoma HHV-8
Non-Hodgkin’s lymphoma Hepatitis C virus
Lyme arthritis Borrelia burgdorferi
Reactive arthritis Campylobacter jejuni, Salmonella
Guillain-barre syndrome Campylobacter jejuni
They may be associated with malignancies and other chronic diseases.
Why are infectious diseases unique?
Host immunity is involved. Intergrity of the immune system (innate immune system,
humoral and cell-mediated immunity)
Extremes of age
State of immunity (vaccination status, presence of co-morbidities)
Presence of immunocompromised state

The Smallpox Threat
• Eradicated in 1979 (WHO)
• Routine vaccination stopped in 1974 (US)
• Last documented case 1949 (US)
• More the 3/4 of the world’s population is now
susceptible
Why are infectious disease unique?
They deal with more than one population.With complex interactions among them
Reservoir
(animals)Dogs
and
sheep/goats –
Echinococcus;
mice and ticks
– Borrelia
Host (e.g. humans)Infectious agents
(helminths,
bacteria, fungi,
protozoa,
viruses,
prions)
Vectors
Mosquito
(malaria), snails
(schistosomiasi
s), blackfly
(onchocerciasis
)

Measures of Disease Frequency
CaseMeasuring disease frequency in populations requires
the stipulation of diagnostic criteria. In clinical practice the definition of "a case" generally
assumes that, for any disease, people are divided into two discrete classes - the affected and the non-affected. For most acquired diseases the real question in
population studies is not "Has the person got it?" but "How much of it has he or she got?"
BMJ. Epidemiology for the uninitiated. Accessed from http://www.bmj.com/about-bmj/resources-readers/publications/epidemiology-uninitiated/2-quantifying-disease-populations
Measures of Disease Frequency
“Case Definition” A set of uniform criteria used to define a disease for
public health surveillance. Enable public health to classify and count cases
consistently across reporting jurisdictions, and should not be used by healthcare providers to determine how to meet an individual patient’s health needs.
http://wwwn.cdc.gov/nndss/case-definitions.html

Measures of Disease Frequency
“Case Definition” Should be precise and unambiguous Essential to define and standardize the methods of
measuring the chosen criteria.
BMJ. Epidemiology for the uninitiated. Accessed from http://www.bmj.com/about-bmj/resources-readers/publications/epidemiology-uninitiated/2-quantifying-disease-populations
Measures of Disease Frequency
Prevalence no. of cases of disease at a particular point in time includes old and new cases better in detecting burden of disease in a particular
population

In the Philippines, what is the prevalence of HIV among MSM?
A. <1%
B. 12%
C. 30%
D. 51%
Question
~12 positivity rate at the RITM Satellite Clinic.
~12 incidence in the MSM Cohort study
MSM and HIV in PH
Personal communication with Dr. Rossana Ditangco, Head, HIV/AIDS Research Group

What city in Metro Manila has the greatest prevalence of HIV among MSM?
A. Manila
B. Quezon City
C. Mandaluyong
D. Caloocan
Question
• NCR• Region 4A (Batangas,
Cavite, Laguna, Rizal, Quezon, Tagaytay)
• Region 7 (Bohol, Cebu, Negros Oriental, Siquijor)
• Region 3 (Aurora, Bataan, Bulacan, Nueva Ecija, Pampanga, Tarlac)
• Region 11 (Compostela Valley, Davao del Norte, Davao del Sur and Davao)
MAY 2015

Prevalence rate of HIV among MSM (DOH 2015)
– Quezon City - 6.6%
– Manila - 6.7%
– Caloocan - 5.3%
– Cebu - 7.7%
– Davao - 5.0%
– Cagayan de Oro - 4.7%
http://www.rappler.com/move-ph/93344-700-hiv-cases-philippines-highest-1984
MAY 2015
Measures of Disease Frequency
Incidence no. of new cases of disease in a defined time period better in detecting outbreaks
BMJ. Epidemiology for the uninitiated. Accessed from http://www.bmj.com/about-bmj/resources-readers/publications/epidemiology-uninitiated/2-quantifying-disease-populations

What is the current rate of HIV diagnosis in PH?
A. 100 new cases per month
B. 10 new cases per week
C. 10 new cases per day
D. 1 new case per hour
Question
What is the current rate of HIV diagnosis in PH?
A. 100 new cases per month
B. 10 new cases per week
C. 10 new cases per day
D. 1 new case per hour
Question
INTRODUCTION TO HEALTHCARE-ASSOCIATED
INFECTIONS (HAIs)Arthur Dessi E. Roman MD MTM FPCP FPSMID
9 February 2016
gonabedess @gonnabedess
Question
Of the total SARS infections (n-=8,422), what percentage are HCWs?
A. <10%
B. 21%
C. 48%
D. 80%WHO/CDS/CSR/GAR/2003.11. Consensus document on the epidemiology of severe acute respiratory
syndrome (SARS)

Question
Of the total SARS infections (n-=8,422), what percentage are HCWs?
A. <10%
B. 21%
C. 48%
D. 80%
WHO/CDS/CSR/GAR/2003.11. Consensus document on the epidemiology of severe acute respiratory
syndrome (SARS)
OUTLINE
I. Definition of Terms
II. Overview of HAIsA. Hospital epidemiology
B. Common Sites of HAIs
C. Factors Promoting HAIs
D. HAI Rates : Local and Global
E. Cost and Burden of HAIs
III. Chain of HAIs

Epidemiology
the study of the distribution or occurrence of a disease or event in a given population or geographical area including the factors that
contributed to these
Hospital Epidemiology
the identification, understanding and development of strategies to eliminate or minimize the risk of acquiring healthcare-
associated infections by applying techniques of epidemiology

Hospital Epidemiology
“in the current era…,hospital epidemiology has expanded and
become relevant beyond the acute care hospital to all settings where
healthcare is delivered…”
Healthcare settings
• Hospitals: acute care facilities, critical access hospitals• Long term care facilities (LTCF)

Healthcare settings
• Outpatient settings
dialysis centers ambulatory surgical centers
Healthcare settings
• Outpatient settings
Physician’s offices Ambulatory chemotherapy centers

Infection
the state or condition in which the body or part of the body is invaded by a pathogenic agent (bacteria,
virus, parasites etc.) which under favorable conditions multiplies and produces injurious effects
Question
The Latin term nosocomium means:
A. Reverse or ironic
B. Hospital
C. Hands
D. Doctor

Question
The Latin term nosocomium means:
A. Reverse or ironic
B. Hospital
C. Hands
D. Doctor
Healthcare-associated Infections (HAIs)
• Previously termed hospital-acquired infection or nosocomial infection
‒“nosocomium” (latin) – hospital
‒ reflects their original association with hospitalized patients
‒ concern to separate the terminology of events from fear of liability that might have interfered with identification and control efforts [of the hospital]
Healthcare-associated Infections
• A localized or systemic condition resulting from an adverse reaction to the presence of an infectious agent(s) or its toxin(s).
• There must be no evidence that the infection was present or incubating at the time of admission to the acute care setting.
Am J Infect Control 2008;36:309-32.
Healthcare-associated Infections
• Presently the preferred term
• Infection acquired 48 hours after admission to hospital- not present or incubating at the time of admission
• Infection acquired while in the hospital and developed during admission or after discharge [up to 6 weeks]

OUTLINE
I. Definition of Terms
II. Overview of HAIsA. Hospital epidemiologyB. Common Sites of HAIs
C. Factors Promoting HAIsD. HAI Rates : Local and GlobalE. Cost and Burden of HAIs
III. Chain of HAIs
52
Fundamental roles of hospital epidemiology
1. Identify risks (what)2. Understand risks (how, why)3. Eliminate or minimize risks

53
Areas of interest to a hospital epidemiologist
• Surveillance for nosocomial infection• bloodstream infections
• pneumonia
• urinary tract infections
• surgical wound infections
• Patterns of transmission of nosocomial infections
• Outbreak investigation
• Isolation and other transmission-based precautions
• Evaluation of exposures
• Employee health
• Disinfection and sterilization
• Hospital engineering and environment
• water supply
• air filtration
• Reviewing policies and procedures for patient care
54
Areas of interest to a hospital epidemiologist
• Antibiotic use
• Antibiotic resistant pathogens
• Microbiology support
• National regulations on infection control
• Infection control committee
• Quantitative methods in epidemiology
• Education
• CQI strategies

OUTLINE
I. Definition of Terms
II. Overview of HAIsA. Hospital epidemiologyB. Common Sites of HAIs
C. Factors Promoting HAIsD. HAI Rates : Local and GlobalE. Cost and Burden of HAIs
III. Chain of HAIs
Common Sites of HAIs
Urinary tractRespiratory tractGastrointestinalBlood streamSkin, Wound, BurnSurgical wound infection

Most common HAIs
Central Line Associated Bloodstream Infection (CLABSI)
Surgical-site Infection (SSI)
Most common HAIs
Ventilator Associated Pneumonia (VAP) Catheter-associated Urinary
Tract Infection (CAUTI)

OUTLINE
I. Definition of Terms
II. Overview of HAIsA. Hospital epidemiologyB. Common Sites of HAIs
C. Factors Promoting HAIsD. HAI Rates : Local and GlobalE. Cost and Burden of HAIs
III. Chain of HAIs
Factors Promoting HAIs
• Prolonged and inappropriate use of medical devices• Extremes of age• Duration of hospitalization• Insufficient application of standard, isolation and
transmission-based precautions• Surgery (type of operation) and other medical
procedures
http://www.who.int/gpsc/country_work/burden_hcai/en/

Factors Promoting HAIs• Immune status: chemotherapy, radiation therapy, malignancy
• Understaffing
• Overcrowding
• Poor knowledge and application of basic IC measures
• Inadequate environmental hygienic conditions and waste disposal
• Poor infrastructure
• Lack of knowledge of injection and blood transfusion safety
http://www.who.int/gpsc/country_work/burden_hcai/en/
OUTLINE
I. Definition of Terms
II. Overview of HAIsA. Hospital epidemiology
B. Common Sites of HAIs
C. Factors Promoting HAIs
D. HAI Rates : Local and Global
E. Cost and Burden of HAIs
III. Chain of HAIs

Healthcare-Associated Infections
Of every 100 hospitalized patients at any given time, 7 in developed and 10 in developing countries will
acquire at least one health care-associated infection.
Healthcare-Associated Infections
http://www3.gehealthcare.com.co/~/media/images/product/product-categories/healthcare-
it/it%20department/hai-data-visualization.png

Healthcare-Associated Infections
1-day survey
• 183 hospitals
• 11,282 patients
• 504 infections identified
in 452 (4%) patients
• 25.6% device-
associated
infections
Multi-state Point Prevalence Survey of
Healthcare-Associated Infections in the U.S.
N Engl J Med 2014;370:1198-208.
Healthcare-Associated Infections
0
2
4
6
8
10
12
14
16
SHIP NHSN INICC
CA-Urinary Tract Infection
CL-Associated Bloodstream Infection
Ventilator Associated Pneumonia
Comparison of Device-Associated Infections
(per 1000 device days)
SHIP 2013 / NHSN 2006-2008 / INICC 2004-2009
SHIP – Surveillance of Hospital Acquired Infections in the Philippines
NHSN – National Healthcare Safety Network
INICC – International Nosocomial Infection Control Consortium
American Journal of Infection Control 2012; 40(5):396-407.

OUTLINE
I. Definition of Terms
II. Overview of HAIsA. Hospital epidemiology
B. Common Sites of HAIs
C. Factors Promoting HAIs
D. HAI Rates : Local and Global
E. Cost and Burden of HAIs
III. Chain of HAIs
The “C ST” of HAIs
Personnel
• Need for hospitalization
• Income loss
• Pain and suffering
• Disfigurement/Disability
• Death
Institutions
• Loss of revenue
• Extra duty
• Liability insurance
• Malpractice
• Reputation
Increased resistance of microorganisms
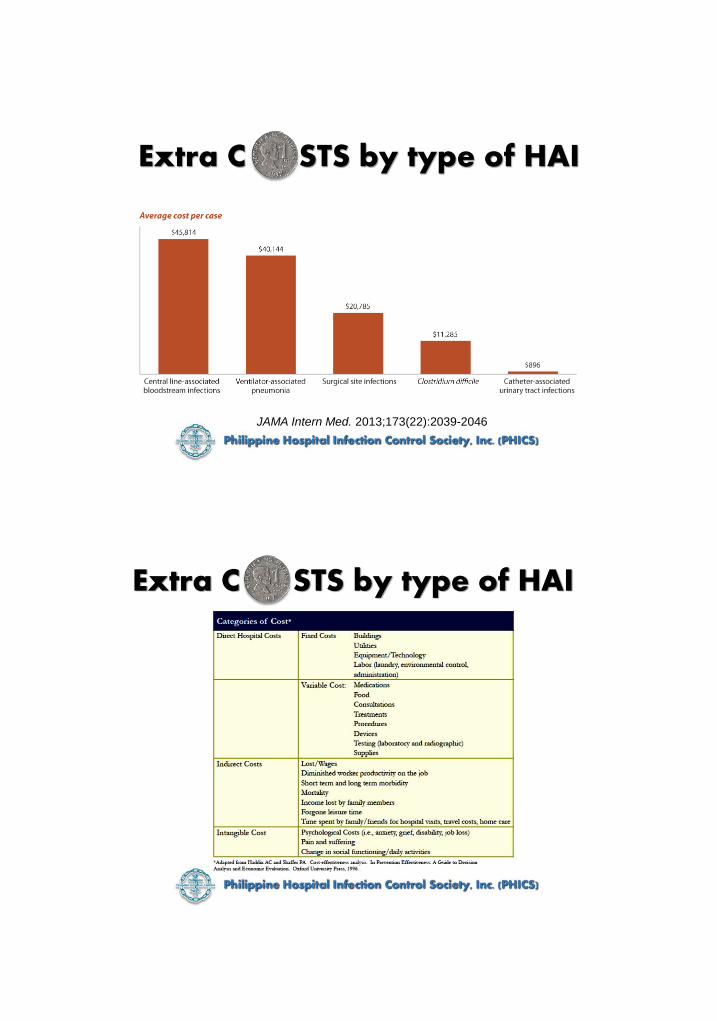
Extra C STS by type of HAI
JAMA Intern Med. 2013;173(22):2039-2046
Extra C STS by type of HAI
17
Extra
Costs
and
Length
of Stay
of HAIs
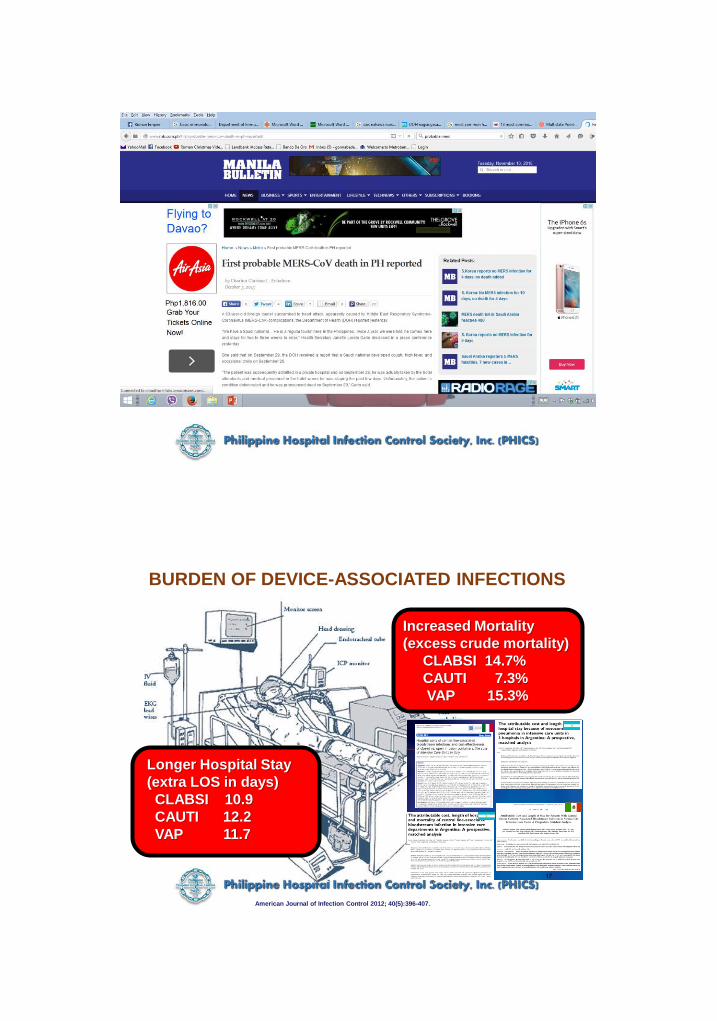
Increased Mortality
(excess crude mortality)
CLABSI 14.7%
CAUTI 7.3%
VAP 15.3%
BURDEN OF DEVICE-ASSOCIATED INFECTIONS
Longer Hospital Stay
(extra LOS in days)
CLABSI 10.9
CAUTI 12.2
VAP 11.7
American Journal of Infection Control 2012; 40(5):396-407.
OUTLINE
I. Definition of Terms
II. Overview of HAIsA. Hospital epidemiology
B. Common Sites of HAIs
C. Factors Promoting HAIs
D. HAI Rates : Local and Global
E. Cost and Burden of HAIs
III. Chain of HAIs
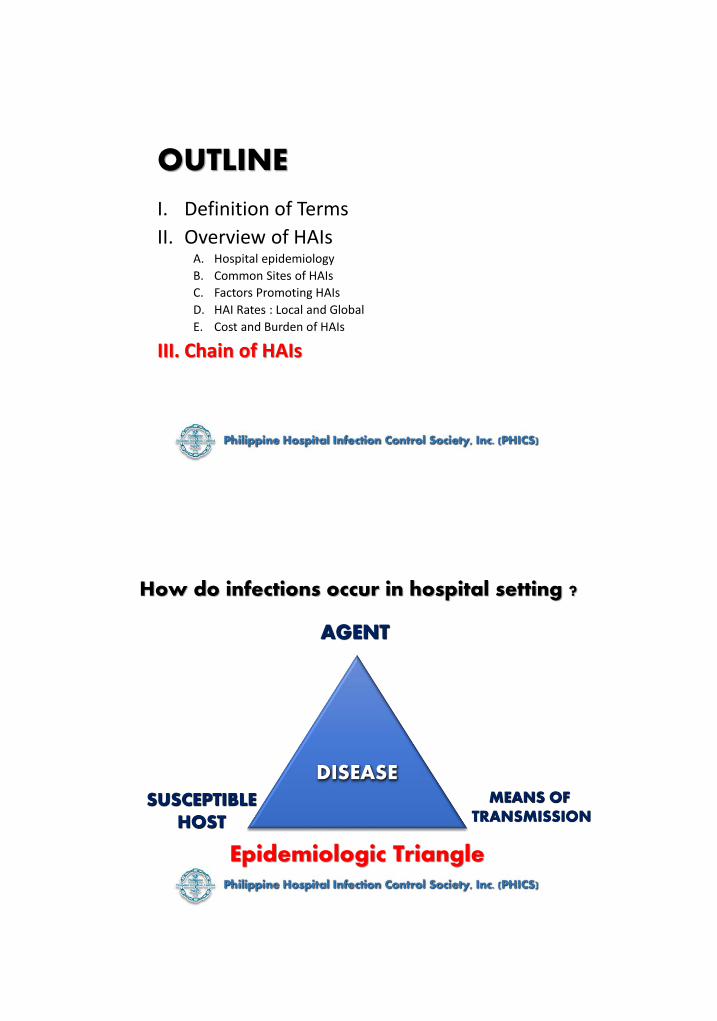
How do infections occur in hospital setting ?
AGENT
SUSCEPTIBLEHOST
MEANS OF TRANSMISSION
Epidemiologic Triangle
DISEASE
How do infections occur in hospital setting ?
AGENT
SUSCEPTIBLEHOST
MEANS OF TRANSMISSION
Epidemiologic Triangle
DISEASE
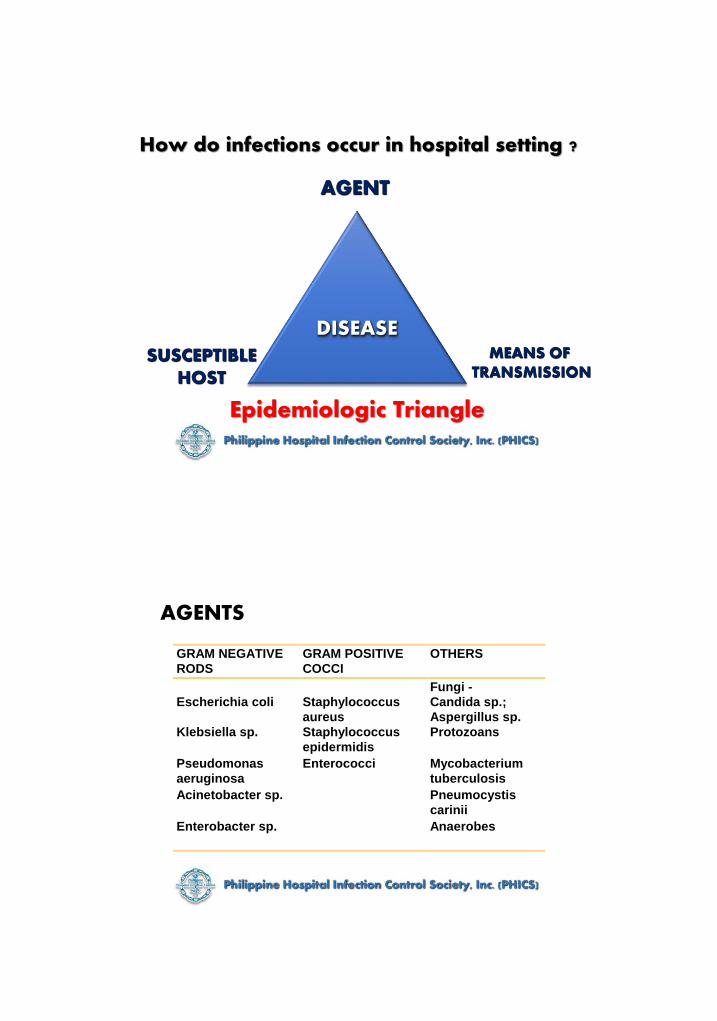
AGENTS
GRAM NEGATIVE
RODS
GRAM POSITIVE
COCCI
OTHERS
Escherichia coli Staphylococcus
aureus
Fungi -
Candida sp.;
Aspergillus sp.
Klebsiella sp. Staphylococcus
epidermidis
Protozoans
Pseudomonas
aeruginosa
Enterococci Mycobacterium
tuberculosis
Acinetobacter sp. Pneumocystis
carinii
Enterobacter sp. Anaerobes

Sources of Agents of Nosocomial Infections
EXOGENOUS
• Hands
• Instruments
• Catheters
• Respiratory equipments
• Transfusions
• IV system
• Linen
• Air
ENDOGENOUS
• Oropharynx
• Respiratory
• Gastrointestinal
• Skin
How do infections occur in hospital setting ?
AGENT
SUSCEPTIBLEHOST
Epidemiologic Triangle
DISEASEMEANS OF
TRANSMISSION

Means of Transmission of HAIs
CONTACT
AIRBORNE
DROPLET
VECTOR
VEHICLE
- direct or indirect
- measles, varicella, TB
- meningococcemia
- insects or animals
- food, water, blood,
medication
Means of Transmission of HAIs
CONTACT- most common means of transmitting microorganisms from one person to another

CONTACTA. Direct Contact
- occurs when one person touches another
- direct contact is an ongoing process in the hospital
- best vehicle : Hands
Means of Transmission of HAIs
CONTACTB. Indirect Contact
- occurs when a person touches an inanimate object contaminated by an infected patient
Means of Transmission of HAIs

Question
According to WHO, what percentage of HAIs are caused by poor hand hygiene?
A. <1%
B. 20%
C. 40%
D. 75%
Question
According to WHO, what percentage of HAIs are caused by poor hand hygiene?
A. <1%
B. 20%
C. 40%
D. 75%
How do infections occur in hospital setting ?
AGENT
Epidemiologic Triangle
DISEASEMEANS OF
TRANSMISSIONSUSCEPTIBLE
HOST
Factors that Increase Host Susceptibility to HAIs
• Chronic underlying diseases
• Immune deficiency states• Malignancies• Therapeutic measures• Immunosuppression• Antibiotic therapy
• Invasive devices
• Surgery
• Age

AGENTMeans of
Transmission
Susceptible
HostBacteria
Virus
Fungi
CONTACT
AIRBORNE
DROPLET
VEHICLE
VECTOR
Disease
AGENT
Susceptible
HOST
Means of
Transmission
The
CHAIN of
INFECTION
Break the chainof Infection

Susceptible
HOST
Breaking the
Chain of Infection
AGENT
Breaking the Chain of Infection: AGENT
The hands should be washed after handling infectious materials (e.g. bed linen, dressings, secretion and excretions).
The skin of the patient should be disinfected before invasive procedures

Emphasize HAND WASHING for personal hygiene
Breaking the Chain of Infection: AGENT
Rational Use of Devices
-avoiding or removing factors that impair host defenses.
- invasive devices should be avoided or should be removed as soon as possible.
Breaking the Chain of Infection: AGENT

Susceptible
HOST
Breaking the
Chain of Infection
Means of
TransmissionAGENT
Isolation techniques based on method of spread
Breaking the Chain of Infection

Protective or Reverse Isolation Rationale: decreasing the contact
of the immunocompromised host to potential pathogens
Breaking the Chain of Infection
Breaking the Chain of Infection
The environment should be HOSTILE to the multiplication of pathogens i.e. clean, dry, exposed to light and well ventilated
Breaking the Chain of Infection
All infectious materials (e.g. linen, clinical waste, sharps) should be safely contained, decontaminated or destroyed
Breaking the Chain of Infection
Use of disposable supplies and equipment in an attempt to limit the spread of infection by this means

Breaking the Chain of Infection
All instruments and equipments should be clean and dry. Invasive items should be sterilized and items in contact with mucous membranes, body fluids and potentially infectious materials should be disinfected
Breaking the Chain of Infection
Food should be hygienically prepared, properly cooked and stored at low temperatures until used

Breaking the Chain of Infection
Control of insect and rodents that serve as vectors in the spread of microorganisms
AGENT
Susceptible
HOST
Breaking the
Chain of Infection
Means of
Transmission

Breaking the Chain of Infection
Susceptible patients or sites should be protected from pathogenic microorganisms: i.e. aseptic technique practice during wound dressing, or
procedures
Immunotherapy, immunizations and other methods of reconstituting patients’ immune response maybe attempted
Breaking the Chain of Infection
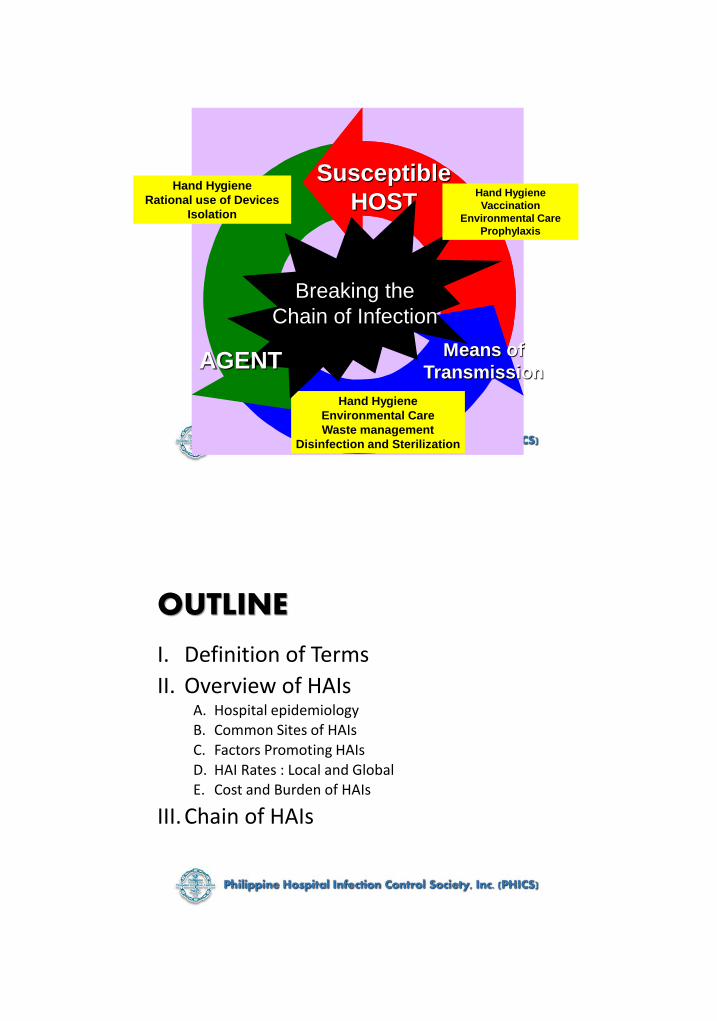
Susceptible
HOST
Means of
Transmission
Hand Hygiene
Environmental Care
Waste management
Disinfection and Sterilization
Hand Hygiene
Rational use of Devices
Isolation
Breaking the
Chain of Infection
Hand Hygiene
Vaccination
Environmental Care
Prophylaxis
AGENT
OUTLINE
I. Definition of Terms
II. Overview of HAIsA. Hospital epidemiologyB. Common Sites of HAIsC. Factors Promoting HAIsD. HAI Rates : Local and GlobalE. Cost and Burden of HAIs
III. Chain of HAIs

The Health Care Worker (HCW) should be aware of how infection is transmitted and the factors involved in the process
The HCW should be able to implement the MOST effective and applicable measures to prevent and control infection in his place of work
The HCW should have the proper attitude towards infection prevention and control.
INFECTION CONTROL is…

BUT…
is not too common.
Infection Control should be..... a WAY of LIFE
Thank you!