intravascular lipoma of the left internal jugular vein … · intravascular lipoma of the left...
TRANSCRIPT
INTRAVASCULAR LIPOMA OF THE LEFT INTERNAL JUGULAR VEIN
Dev Kamdar, MD; Shamit Chopra, MBBS; Corey Treadway, MD; Natasha Robinette, MD; Mehsati Herawi, MD; Ho-Sheng Lin, MDBarbara Ann Karmanos Cancer Institute, Wayne State University, Detroit, MI
ABSTRACTIntravascular lipomas are quite rare. There have been very few cases reported in literature, and all of these have been lipomas arising in the venae cavae and the femoral veins. To our knowledge, no cases have ever been described of intravascular lipomas arising from the vessels in the head and neck. Here, we present the case of a 63-year-old man who was discovered to have an intravascular lipoma arising from his left internal jugular vein with particular emphasis on the radiologic and pathologic findings.
CASE REPORTA 63 year-old man with a history of two pulmonary embolisms with negative workups presented with an one year history of dysphagia. A CT scan of the neck revealed a multilobular thyroid gland on the left side. At that time, a left neck mass, which looked like a lipoma, was also noted. A fine needle aspiration of both masses was reported negative. On repeat CT of the neck, the left neck mass was reported as having increased in size and the possibility of liposarcoma was raised. The patient was referred to the Karmanos Cancer Institute for further evaluation and management. A review of the CT scan revealed a fatty soft tissue mass in the left neck which seemed to arise from and partially occlude the left internal jugular vein (IJV) and was extending intraluminally into the left subclavian vein (SCV). A MRI of the neck was peformed which seemed to confirm the intravascular and likely benign nature of this tumor. Given the progression in size and the patient’s history of pulmonary emboli, the patient was given the option of surgical resection of this tumor.
Intraoperatively, dissection down to the IJV revealed a large perivascular component of the tumor adjacent to the vessel. The IJV superiorly was of normal caliber but as the dissection was meticulously carried inferiorly, a dilation of the vessel wall was noted and the intravascular component of the lipoma was palpated. The perivascular component extended down below the clavicle to the SCV. As it was dissected away from the junction of the IJV and the SCV, the thoracic duct was identified and ligated. The intravascular component was also palpated within the SCV and with compression this was pushed back into the IJV. The IJV was then clamped and ligated and the specimen was removed. Dissection of the specimen with reflection of the wall of the IJV revealed the well encapsulated intravascular component of the lipoma.
Final pathology on the specimen confirmed the diagnosis. All thirty-five lymph nodes present within the specimen were reported negative. The patient’s postoperative course, however, was complicated by a chyle leak. He was taken to the operating room for a muscle flap closure after conservative measures failed to resolve the leak. The patient was then started on his normal diet which he tolerated quite well. The Jackson-Pratt drain was removed and the patient was discharged home in stable condition.
RADIOLOGY SURGERY DISCUSSION
PATHOLOGY
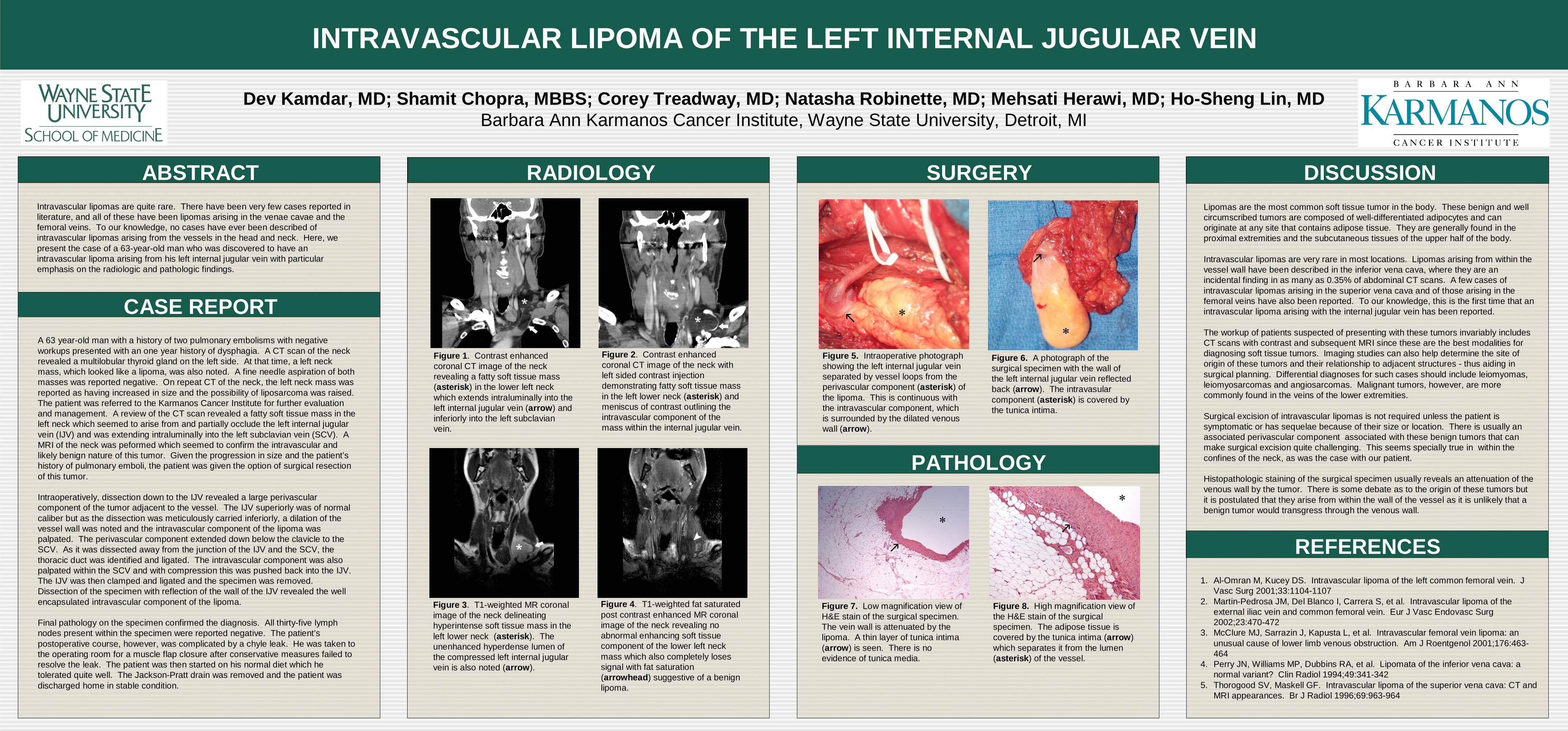
Figure 1. Contrast enhanced coronal CT image of the neck revealing a fatty soft tissue mass (asterisk) in the lower left neck which extends intraluminally into the left internal jugular vein (arrow) and inferiorly into the left subclavian vein.
Figure 2. Contrast enhanced coronal CT image of the neck with left sided contrast injection demonstrating fatty soft tissue mass in the left lower neck (asterisk) and meniscus of contrast outlining the intravascular component of the mass within the internal jugular vein.
Figure 3. T1-weighted MR coronal image of the neck delineating hyperintense soft tissue mass in the left lower neck (asterisk). The unenhanced hyperdense lumen of the compressed left internal jugular vein is also noted (arrow).
Figure 4. T1-weighted fat saturated post contrast enhanced MR coronal image of the neck revealing no abnormal enhancing soft tissue component of the lower left neck mass which also completely loses signal with fat saturation (arrowhead) suggestive of a benign lipoma.
REFERENCES
Figure 7. Low magnification view of H&E stain of the surgical specimen. The vein wall is attenuated by the lipoma. A thin layer of tunica intima (arrow) is seen. There is no evidence of tunica media.
Figure 8. High magnification view of the H&E stain of the surgical specimen. The adipose tissue is covered by the tunica intima (arrow) which separates it from the lumen (asterisk) of the vessel.
Figure 5. Intraoperative photograph showing the left internal jugular vein separated by vessel loops from the perivascular component (asterisk) of the lipoma. This is continuous with the intravascular component, which is surrounded by the dilated venous wall (arrow).
Figure 6. A photograph of the surgical specimen with the wall of the left internal jugular vein reflected back (arrow). The intravasular component (asterisk) is covered by the tunica intima.
Lipomas are the most common soft tissue tumor in the body. These benign and well circumscribed tumors are composed of well-differentiated adipocytes and can originate at any site that contains adipose tissue. They are generally found in the proximal extremities and the subcutaneous tissues of the upper half of the body.
Intravascular lipomas are very rare in most locations. Lipomas arising from within the vessel wall have been described in the inferior vena cava, where they are an incidental finding in as many as 0.35% of abdominal CT scans. A few cases of intravascular lipomas arising in the superior vena cava and of those arising in the femoral veins have also been reported. To our knowledge, this is the first time that an intravascular lipoma arising with the internal jugular vein has been reported.
The workup of patients suspected of presenting with these tumors invariably includes CT scans with contrast and subsequent MRI since these are the best modalities for diagnosing soft tissue tumors. Imaging studies can also help determine the site of origin of these tumors and their relationship to adjacent structures - thus aiding in surgical planning. Differential diagnoses for such cases should include leiomyomas, leiomyosarcomas and angiosarcomas. Malignant tumors, however, are more commonly found in the veins of the lower extremities.
Surgical excision of intravascular lipomas is not required unless the patient is symptomatic or has sequelae because of their size or location. There is usually an associated perivascular component associated with these benign tumors that can make surgical excision quite challenging. This seems specially true in within the confines of the neck, as was the case with our patient.
Histopathologic staining of the surgical specimen usually reveals an attenuation of the venous wall by the tumor. There is some debate as to the origin of these tumors but it is postulated that they arise from within the wall of the vessel as it is unlikely that a benign tumor would transgress through the venous wall.
1. Al-Omran M, Kucey DS. Intravascular lipoma of the left common femoral vein. J Vasc Surg 2001;33:1104-1107
2. Martin-Pedrosa JM, Del Blanco I, Carrera S, et al. Intravascular lipoma of the external iliac vein and common femoral vein. Eur J Vasc Endovasc Surg 2002;23:470-472
3. McClure MJ, Sarrazin J, Kapusta L, et al. Intravascular femoral vein lipoma: an unusual cause of lower limb venous obstruction. Am J Roentgenol 2001;176:463-464
4. Perry JN, Williams MP, Dubbins RA, et al. Lipomata of the inferior vena cava: a normal variant? Clin Radiol 1994;49:341-342
5. Thorogood SV, Maskell GF. Intravascular lipoma of the superior vena cava: CT and MRI appearances. Br J Radiol 1996;69:963-964