intraoperative radiography dmi 63 2 28 2014 online ed
TRANSCRIPT

Intraoperative Radiography
DMI 63
2 28 2014 online ed.

Working in OR requires :
• Super awareness of sterile environment!
• Skill in use of portable machine and c-arm
• Skill in working OR table
• Using radiation protection appropriately
• Knowledge of anatomic landmarks- whether you can see them or not!
• Ability to work with surgery staff under high pressure circumstances

Mobile Image Intensifier
Commonly referred to as? C-arm
Is it sterile?
No!
Unless----

Portable X-ray UnitSterile?
No!
Unless covered with sterile plastic covers after portable brought into OR
(X-ray machine should be cleaned prior to entering each OR!)

OR table
Learn how to work control boxSterile?
No!
Unless-
Covered with sterile drapes!

Radiation Protection
Shield patient if possible!If it doesn’t interfere with exam
The mobile unit should not be used as shield by you
YOU must provide Lead aprons for all personnel!
Monitoring badges should be worn by all personnel
You are responsible for making sure all personnel who can or want to leave room prior to making an exposure are given a loud clear warning and have a chance to get out

Fluroscopy
When using the c-arm, the radiation source is generally under pt, so where should shielding should be placed?
Under the pt!between source and ptMust be done before pt is put on table

If you are not sure, consider it sterile!
During surgery
Technologist works under direction of surgeon not a radiologist
Who will appear to hate you!
You must be able to perform accurately and quickly! “Repeat” is no longer in your vocabulary!
Remember: it’s a high stress situation for all –but success or failure rests on surgeon’s shoulders

Check your ego at the door!You no longer have a name - you are “X-ray”
Only person lower than you is guy who cleans OR- at least they know his name! (Jose)
Expect some abuse!
Good part -if you screw up, they won’t recognize you outside OR!

You must be able to read minds!
• When running c-arm, when Dr. wants fluoro, he expects you to understand that:
– “X-ray”– “now” – “ OK”– “uh huh”– “ready”– grunt– mumble – Or maybe just a glance at monitor
• Mean: hit the fluoro pedal- even when used interchangeably
God help you if you fluoro when he didn’t want it!!!

3 Areas of OR
• Unrestricted• Semi-restricted• Restricted

Unrestricted areas of OR
• Provides outside to inside access
• No traffic restrictions
• Street clothes permitted
Semi-restricted areas of OR
Provides access from unrestricted area of OR to restricted area
Authorized personnel onlyPts and staff
Proper OR attire requiredScrubs, head and shoe covers
Examples of Semi-restricted area
• Hallways within OR rooms
• Instrument and supply processing area
• Non-sterile supply areas and utility rooms

Restricted Areas
Where surgical procedures are carried outProper OR attire and mask must be worn
Examples:Scrub sink areasSterile supply roomsOperating suites
The Surgical Suite
Restricted area!
•Scrub clothes must be worn, and covered with robe if leaving department
•Know Who is sterile and who isn’t! •Know What equipment is sterile and what isn’t!
•No items should be touched without permission of circulating nurse or person in charge!

Operating Room Attire
Clean, fresh attire, surgical “scrubs,” donned at beginning of each shift
Are they sterile?no
Change as necessary
Should soiled scrubs be worn outside OR suite?no!

What the surgery team wears!

Masks worn at all times in OR!
Are they sterile?
No!

Operating Room Attire
CapsWorn in all areas of OR to contain hair
Hoods available to cover any facial hair not contained by mask
Are they sterile?
No!

Surgical Shoe Covers
Purpose:
Top prevent you from tracking in contaminants
To prevent contaminants from soiling your shoes
Are they sterile?
NO!

Operating Room Attire for Techs
GlovesWorn to protect tech from body fluids –sterile?
No!
Radiation badge
Proper ID

Lead attire

Person with known transmittable infection should not be permitted in OR suite!
oColdoAcute infectionoOpen cold soreoSore throatoCarrier of transmittable conditions
Pathogens fall into two broad categories:Pathogens fall into two broad categories:Blood and body fluid borne Blood and body fluid borne AirborneAirborne

Universal Precautions
The practice in medicine of avoiding contact with patients' bodily fluids, by means of wearing of nonporous articles such as medical gloves, goggles, and face shields
to prevent exposure to pathogens of potential portals of entry for infection (nose, mouth, mucous surfaces, conjunctival membranes, abrasions and lacerations on skin, etc.)
Initially developed in 1987 by the Centers for Disease Control and Prevention in US
Surgical gloves now worn when performing simple procedures such as drawing blood from veins
and conducting intra-oral exam
OSHA (Occupational Safety and Health Administration) standards include procedures for cleaning and disposing of used surgical equipment, needles, and laundry, and for disposal of contaminated waste

• Supplement, not replace routine infection-control procedures, such as handwashing and use of surgical gloves
• Does not eliminate need for other categories of disease-specific isolation measures, such as isolation procedures used for open pulmonary tuberculosis and "enteric" procedures used for cases of infectious diarrhea
• At first regarded use of universal precautions as actually or potentially stigmatizing—tending to label patients as "contaminated" but this attitude has been overcome by careful explanation and educational material
Universal precautions are intended to:

Aseptic Vs Sterile
Aseptic :Free from pathogenic (disease
causing) microorganisms
Sterile:Free from all living
microorganisms

Nosocomial infections
Infections resulting from of treatment in a hospital or a healthcare service unit
Infections are considered nosocomial if they first appear:
48 hours or more after hospital admission
or within 30 days after discharge

Nosocomial infections (cont’d)
In US, Centers for Disease Control and Prevention estimates 1.7 million hospital-associated infections, cause or contribute to 99,000 deaths each year
Commonly transmitted when hospital officials become complacent and do not practice correct hygiene regularly
Increased use of outpatient treatment means people hospitalized are more ill and have more weakened immune systems than may have been true in past

Radiographers or other non-sterile personnel must maintain a safe margin from any sterile field-
What is worse than contaminating a sterile field?- not reporting it!

What is the sterile corridor?
• Area between instrument table and draped pt
• Must notnot be entered by any non-sterilenon-sterile personnel!
• NotifyNotify proper personnel immediatelyimmediately if a sterile field is contaminated!!

What parts of sterile gown are considered sterile?
On sleeves- elbow to cuffs
On body- shoulder to level of sterile field

Logistical Problems
• Getting c-arm or portable through jungle of equipment and people
• Getting cassette under pt without breaking sterile field
• Centering CR to pt and to cassette when you can’t see or touch either one!
• Grid cut off!
• When x-ray is performed table top, covered with sterile cloth- you can’t see body part!
• Watch out for your lead apron hitting field

Loading A Cassette in Sterile Cover
2 person job!
Tech
Tech
OR staff

Retrieving IR in Sterile Field
Why must Radiographer be wearing gloves?
in case IR cover is contaminated with blood or body fluids
Surgical tech or nurse gives covered IR to radiographer
OK to contaminate cover now, but not person handing you cassette!
Cover and gloves are disposed of properly before handling uncovered IR

After the exposure:
Hot foot it up department and develop image STAT and return with image to OR ASAP
Remember:Longer time pt. spends under anesthesia the
greater risk to patient
Prolonged exposure unnecessarily adds to the risk of infection
Longer time spent in the OR for pt, the greater the cost to pt!
Longer time you take, the angrier the Dr.s will be with you!

Cardiac Surgery
Anything pertaining to heart and related major blood vessels
Most common procedures: – pacemaker and automatic internal
cardiac defibrillator insertions (C-arm)
– Coronary artery bypass grafts
Post-op CXR generally required after above mentioned procedures

Cholangiogram

Neurosurgery
• Laminectomies– Requires x-table lateral
projections
• Shunt placements
• Transphenoidal cases– Requires C-arm or skull films
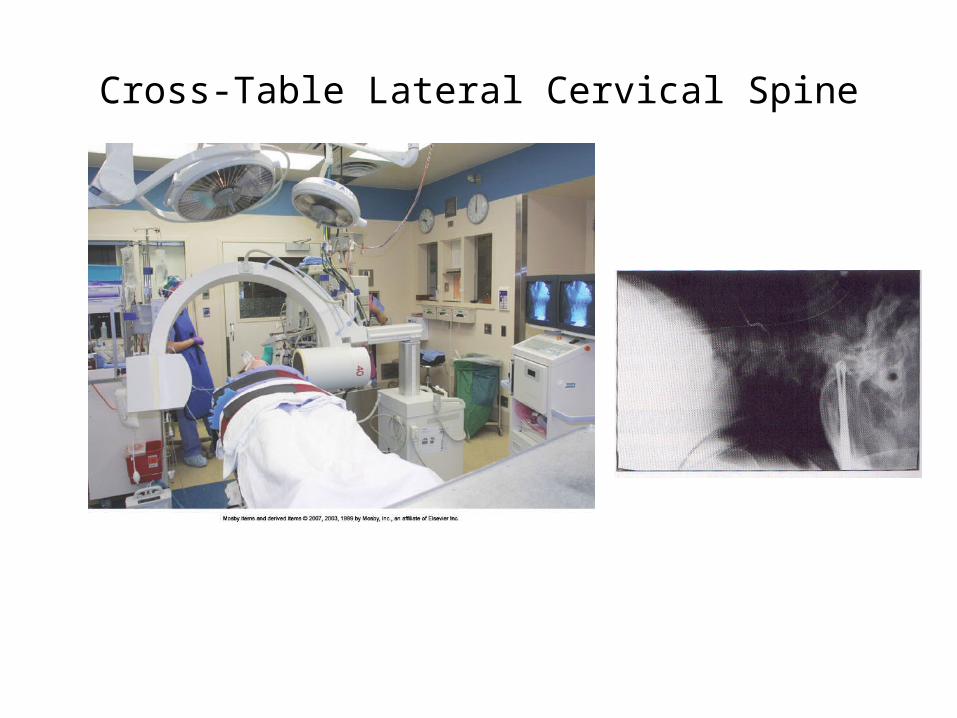
Cross-Table Lateral Cervical Spine

Oncology
Catheter placementsUsually by C-armRequires a post-op CXR
Brachytherapy localizationRequires two views at right angle to each other
Cesium Implant

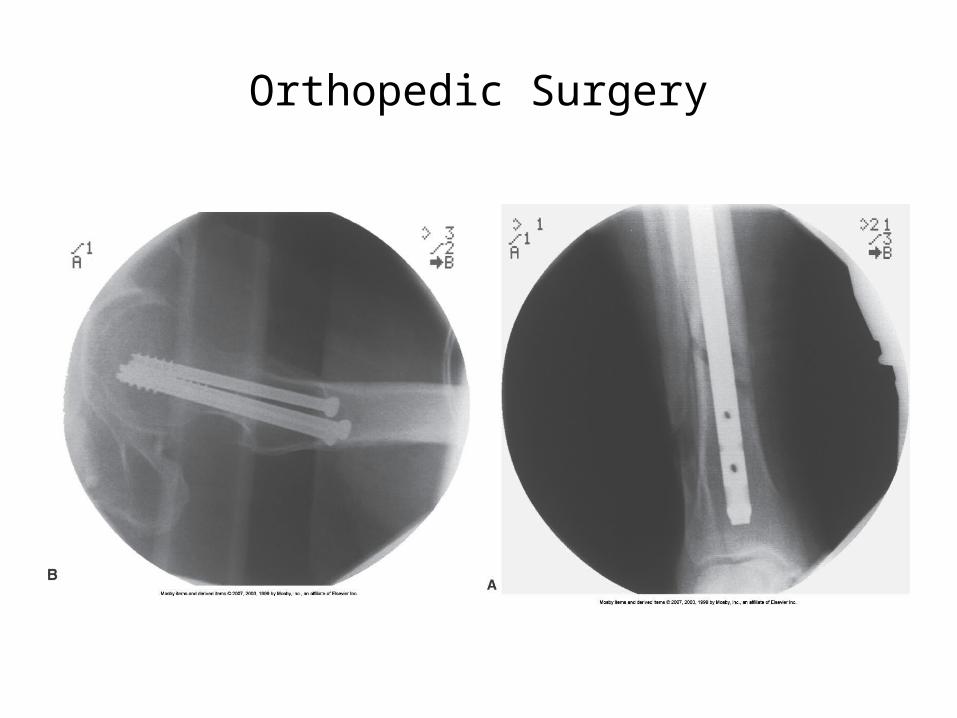
Orthopedic Surgery
ORIF stands for?
Open reduction internal fixationMay require C-arm or plain film radiography
Closed reduction is what?No surgical incision- just manipulationC-arm or plain films

Joint Replacement
Orthopedic Surgery

Pain Management
• Requires C-arm to locate injection site for facet block
• Usually in:– Lumbar spine or– SI joint or– Cervical spine

Vascular Surgery
Utilizes both plain film and mobile fluoroscopy
AV fistulas, AV grafts are most common procedures
What is an AV fistula? abnormal connection or passageway
between artery and vein)

Urology Suite
Retrograde Pyelograms (contrast flows from bladder up to kidney)
IVU’s
Kidney & gallstone extractions
Percutaneous Nephrolithotomy (removal stones from kidney by small puncture wound (up to about 1 cm) through skin)

Summation of Important Things To Remember in OR!
• Upon entering OR, alert all staff of your presence and purpose
• Be aware of sterile fields and personnel• Enlist aid of circulating nurse to move equipment
out of way• Any cassettes placed in sterile field must be
covered first by a sterile member of the team• Allow team to clear room prior to making the
exposure• Do it right the first time!!!