intractable stokes-adams disease: a method of emergency management
TRANSCRIPT

Intractable Stokes-Adams disease
A method of emergency management
Benson B. Roe, M.D., F.A.C.S. San Francisco, Cdl’.
T otal heart block with Stokes-Adams attacks is often fatal, and the average
life expectancy after the first attack is less than 2 years. Because both the occurrence of the attacks and the return of systolic action are unpredictable, the patient is rarely able to receive medical care in time for death to be averted. In our experience, most of the patients who do survive fre- quently recurring or intractable Stokes- Adams attacks (usually by taking an inotropic drug which they keep available) can be satisfactorily supported with intra- venous isoproterenol which stimulates a ventricular focus. However, this drug causes ventricular fibrillation in patients with highly irritable ventricles, and other patients unresponsive to it do not main- tain a satisfactory ventricular rate. Cntil an implantable pacemaker can be inserted, such patients must be supported by an external pacemaker.
The electrical impulse from an external pacemaker can be carried to the heart either through the chest wall via skin electrodes, as described by Zoll,’ or through a cardiac catheter, as advocated by Par- sonnet? and Schwedel.Y Although either method may prove to be effective, each has important disadvantages.
The external electrodes deliver a dis- tinctly uncomfortable and frequently pain- ful shock to the skin at the point of contact. Because of the high resistance of the skin, a larger current is required, which may re-
Fig. 1. Close-up view of needle and electrode.
Fig. 2. Cut-away view of a dog’s heart, showing left x-entricular chamber with one wire still in place (left) and the second wire (right) after being with- drawn. Arrow (right) points to site of puncture and withdrawal. Both wires were inserted during life.
From the Ikpartment of Surgery. ITniversity of California Medical School, San Francisco, Calif. Received for publication June 2, 1964.
470
Volume 69 Number 4 Intractable Stokes-Adams disease 471
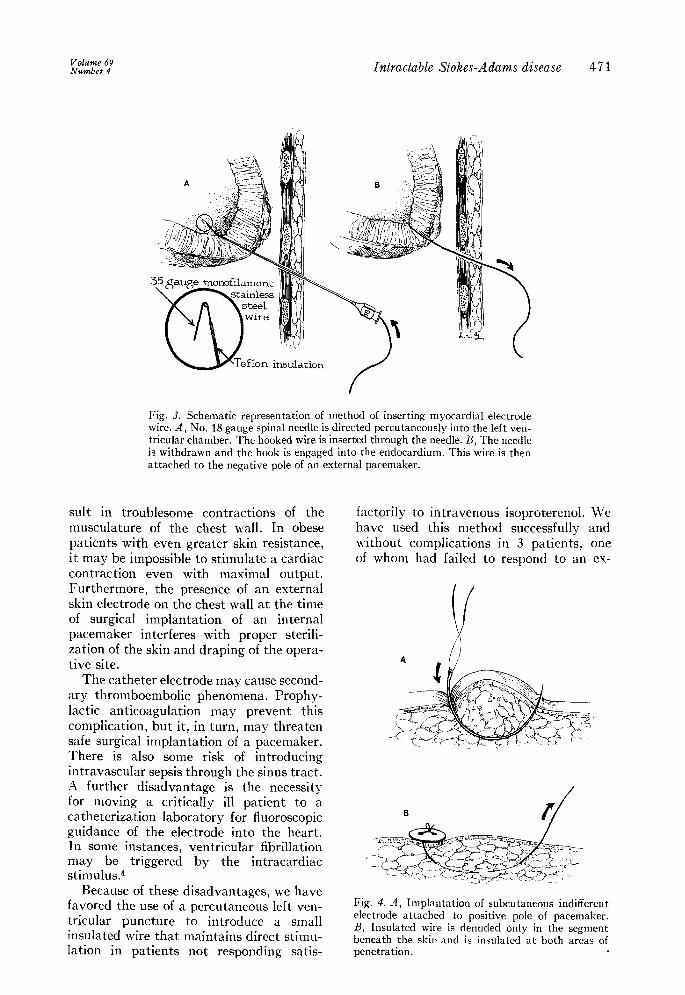
Fig. 3. Schematic representation of method of inserting myocardial electrode wire. A, No. 18 gauge spinal needle is directed percutaneously into the left ven- tricular chamber. The hooked wire is inserted through the needle. B, The needle is withdrawn and the hook is engaged into the endocardium. This wire is then attached to the negative pole of an external pacemaker.
suit in troublesome contractions of the musculature of the chest wall. In obese patients with even greater skin resistance, it may be impossible to stimulate a cardiac contraction even with maximal output. Furthermore, the presence of an external skin electrode on the chest wall at the time of surgical implantation of an internal pacemaker interferes with proper sterili- zation of the skin and draping of the opera- tive site.
The catheter electrode may cause second- ary thromboembolic phenomena. Prophy- lactic anticoagulation may prevent this complication, but it, in turn, may threaten safe surgical implantation of a pacemaker. There is also some risk of introducing intravascular sepsis through the sinus tract. A further disadvantage is the necessity for moving a critically ill patient to a catheterization laboratory for fluoroscopic guidance of the electrode into the heart. In some instances, ventricular fibrillation may be triggered by the intracardiac stimulus.4
Because of these disadvantages, we have favored the use of a percutaneous left ven- tricular puncture to introduce a small insulated wire that maintains direct stimu- lation in patients not responding satis-
factorily to intravenous isoproterenol. We have used this method successfully and without complications in 3 patients, one of whom had failed to respond to an ex-
Fig. 4. A, Implantation of subcutaneous indifferent electrode attached to positive pole of pacemaker. B, Insulated wire is denuded only in the segment beneath the skin and is insulated at both areas of penetration.

ternal pacemaker and had rtpeatedl>- tie- veloped ventricular fibrillation n-hen a catheter electrode was inserted.
Method
A thin-walled Ko. 18 spinal needle is introduced percutaneously over the apical impulse and is directed toward the tip of the right scapula. L\s the left ventricle is entered, the obturator of the needle is lvithdrawn in order to verify its presence in the lumen. A1 fine (Grade 35) monofila- ment stainless-steel wire insulated with Teflon is then introduced through the needle (Fig. 1). The terminal 15 mm. of the \\-ire is bared and kinked back upon itself so that a doubled end is introduced through the needle. The needle is then \vithdra\vn over the n-ire, \vhich is pulled back so that its end can be engaged as a somen-hat pliable barb against the endo- cardium (Figs. 2 and 3). Fixation to the skin is nlaintained with a suture and a tape flag. The n-ire is attached to the negative pole of an external pacemaker, and the positive pole is grounded to an indifferent electrode. In an emergency, an ordinar\- skin electrode placed with con- ductive paste can be used for the indif- ferent site, but for longer maintenance Eve prefer to use a wire inserted subcutane- ously (Fig. 4).
Although this method carries a slight hazard (but one as yet not experienced) of pericardial tamponade through puncture of a coronary artery at the apes, it has the advantage of providing an effective con- tact to the heart that can be introduced at the bedside with a minimum of delav. It is not recommended for long-term stimu-
lation and should be replaced with ;III implantable pacemaker as soon as practi- cable. The presence of the \\-ire at the oper- ative site, traversing the incision, has not proved to be the problem that we expected, since it is possible to drape over the punc- ture site and to dissect around the x\.ire while entering the chest. AAs a precautionnr). measure an additional sterile needle-elec- trode is maintained in the operative field in case the v\ire should become dislodged.
Summary
;1 method is described for rapid percu- taneous implantation of a myocardial electrode for temporary external electrical pacing prior to implantation of an internal pacemaker. This technique is useful in patients who cannot be satisfactorily con- trolled with intravenous isoproterenol, and would appear to be preferable to the al- ternative techniques of transcutaneous or transvenous stimulation.
REFERENCES
1. Zoll, I’. M., Linenthal, A. J., and Norman, L. I<.: Treatment of Stokes-Adams disease by external electric stimulation of the heart, Circulation 9:482, 1954.
2. Parsonnet, V., Zucker, I. K., Gilbert, L., and Asa, WI. M.: The development of an intra- cardiac dipolar catheter electrode for the treat- ment of complete heart block, Surg. Forum 13:179, 1962.
3. Schwedel, J. B., Furman, S., and Escher, D. J. W. : Use of an intracardiac pacemaker in the treatment of Stokes-Adams seizures, I’rog. Cardiovas. Dis. 3:170, 1960.
4. Roe, B. B., and Katz, H. J.: Complete heart block with intractable asystole and recurrent ventricular fibrillation; report of a case with sur\-ival Am. J. Cardiol. (In press.)