interventions in carotid, renal & other pad
DESCRIPTION
Giving back to SCRIBD . . . . its a great platform for allTRANSCRIPT
Interventions in Interventions in Carotid, Renal and Carotid, Renal and
other peripheral vesselsother peripheral vessels
Why peripheral interventions are important for everybody
PAD is often present in patients with established CAD
PAD may be the first and/or only manifestation of atherothrombosis in several pts
Peripheral complications during PCI or other cardiac interventions are not rare and should best be managed by YOU in the cath lab

A GLOBAL MANAGEMENT A GLOBAL MANAGEMENT APPROACH IS A MUSTAPPROACH IS A MUST

TAKE CARE AT PREPPING TAKE CARE AT PREPPING
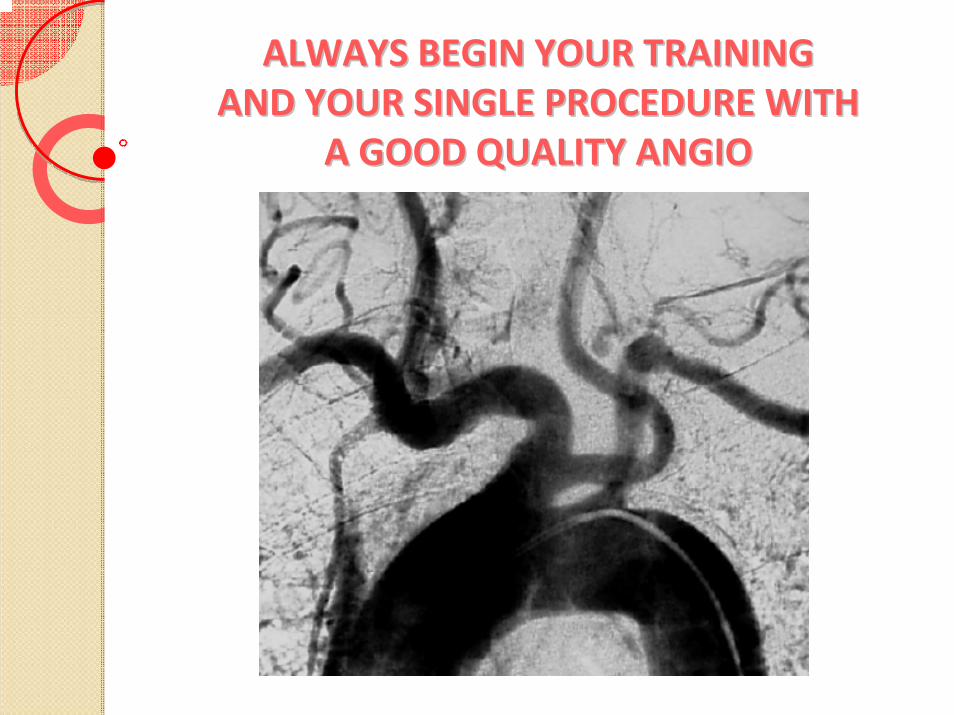
ALWAYS BEGIN YOUR TRAINING ALWAYS BEGIN YOUR TRAINING AND YOUR SINGLE PROCEDURE WITH AND YOUR SINGLE PROCEDURE WITH
A GOOD QUALITY ANGIOA GOOD QUALITY ANGIO
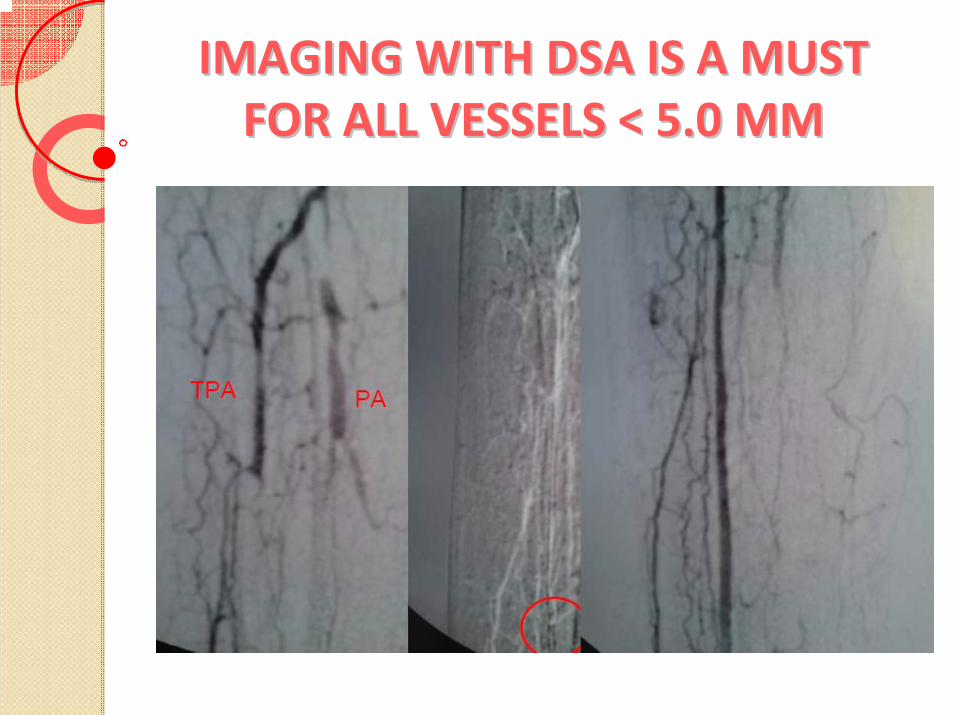
IMAGING WITH DSA IS A MUST IMAGING WITH DSA IS A MUST FOR ALL VESSELS < 5.0 MMFOR ALL VESSELS < 5.0 MM

MINIMIZE RADIATION RISKMINIMIZE RADIATION RISK
6 MONTHS AFTER
PROCEDURE
2 MONTHS AFTER
PROCEDURE
2 YEARSAFTER
PROCEDURE
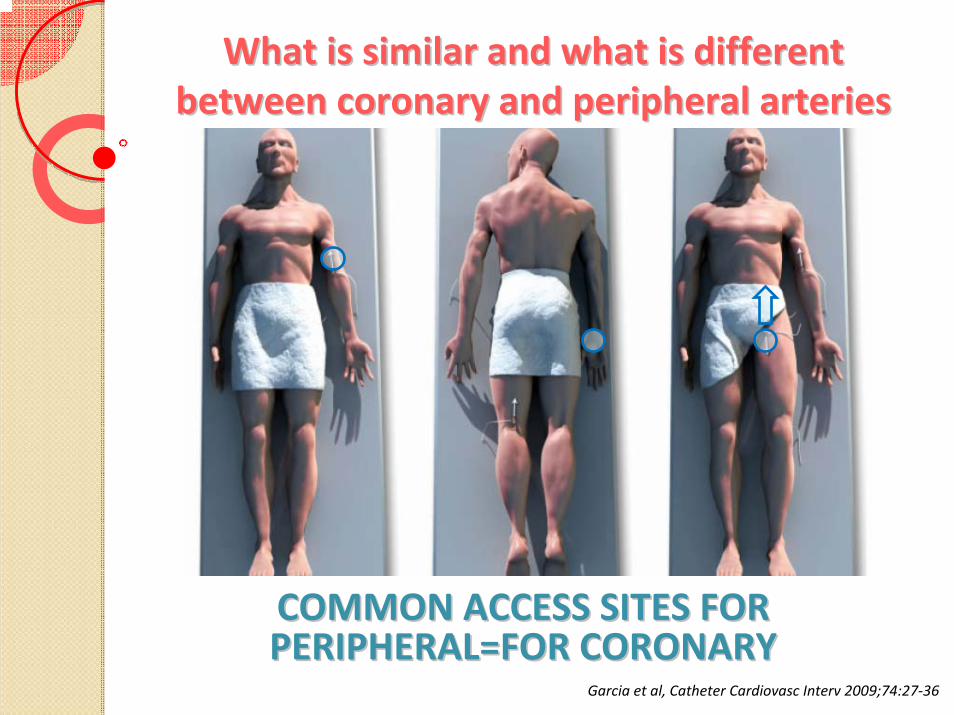
What is similar and what is different What is similar and what is different between coronary and peripheral arteriesbetween coronary and peripheral arteries
COMMON ACCESS SITES FOR COMMON ACCESS SITES FOR PERIPHERAL=FOR CORONARYPERIPHERAL=FOR CORONARY
Garcia et al, Catheter Cardiovasc Interv 2009;74:27‐36
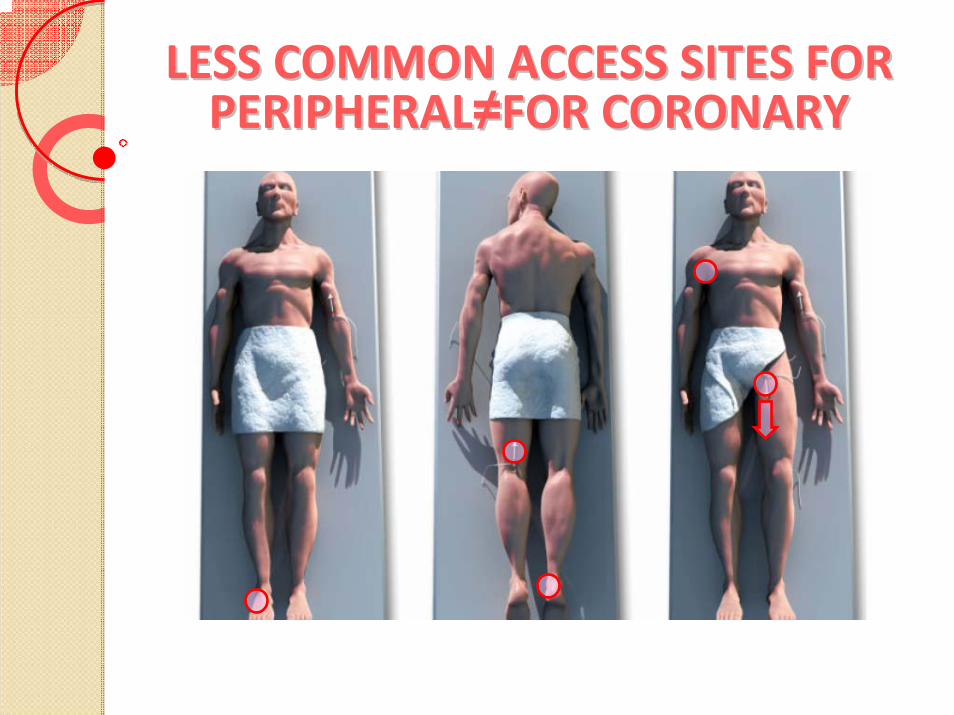
LESS COMMON ACCESS SITES FOR LESS COMMON ACCESS SITES FOR PERIPHERALPERIPHERAL≠≠FOR CORONARYFOR CORONARY
DEVICE TYPES ARE ALSO DEVICE TYPES ARE ALSO BROADLY SIMILARBROADLY SIMILAR
SheathsShuttle sheathsGuidewiresBalloonsStentsFiltersThrombectomy catheters
BUT DEVICE SIZES AND FEATURES BUT DEVICE SIZES AND FEATURES ARE VERY DIFFERENT!ARE VERY DIFFERENT!
Sheaths (3‐9 Fr)Shuttle sheaths (30‐90 cm)
Guidewires (0.014”, 0.018”, 0.035”)Balloons (1.25‐15.0 mm)
Stents (balloon‐, self‐expandable)FiltersThrombectomy catheters (4‐6 Fr)
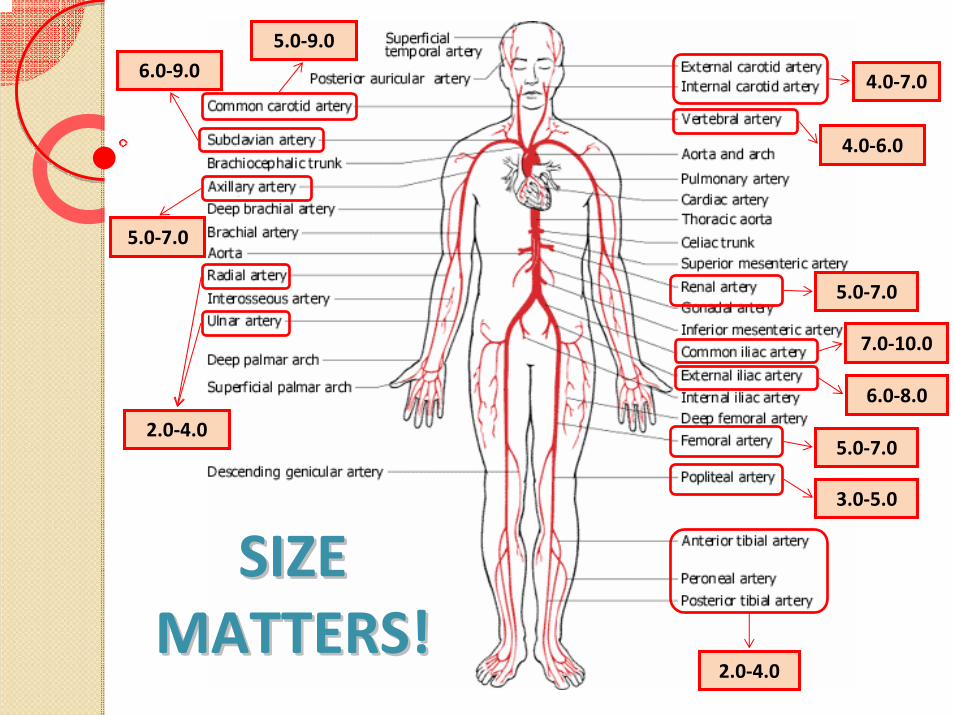
2.0‐4.0
5.0‐7.0
4.0‐7.0
4.0‐6.0
6.0‐9.05.0‐9.0
5.0‐7.0
7.0‐10.0
6.0‐8.0
2.0‐4.0
5.0‐7.0
3.0‐5.0
SIZE SIZE MATTERS!MATTERS!
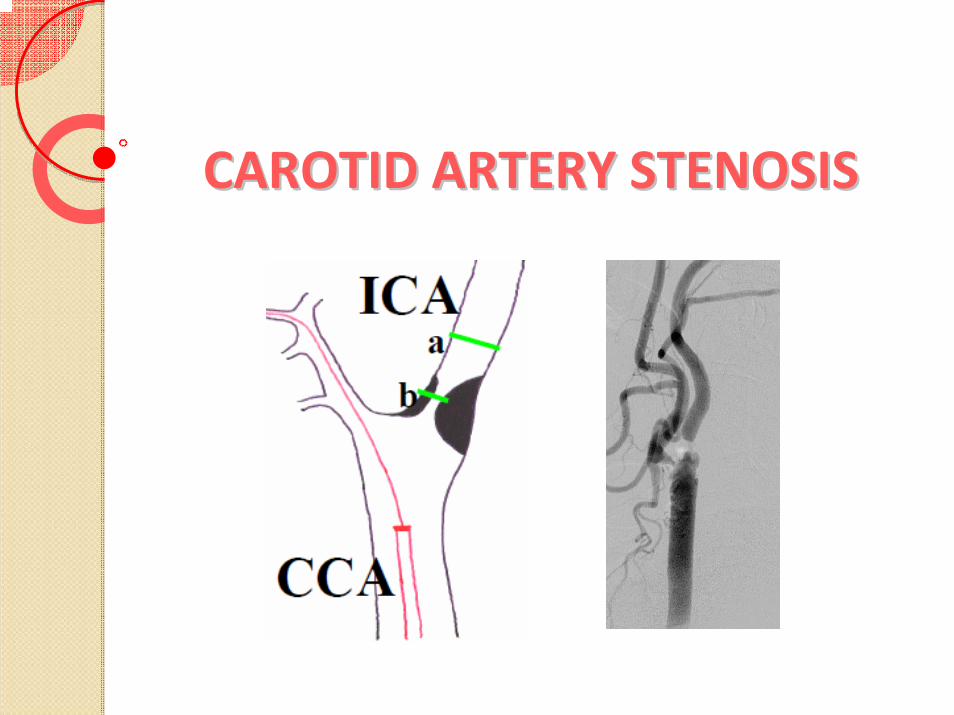
CAROTID ARTERY STENOSISCAROTID ARTERY STENOSIS
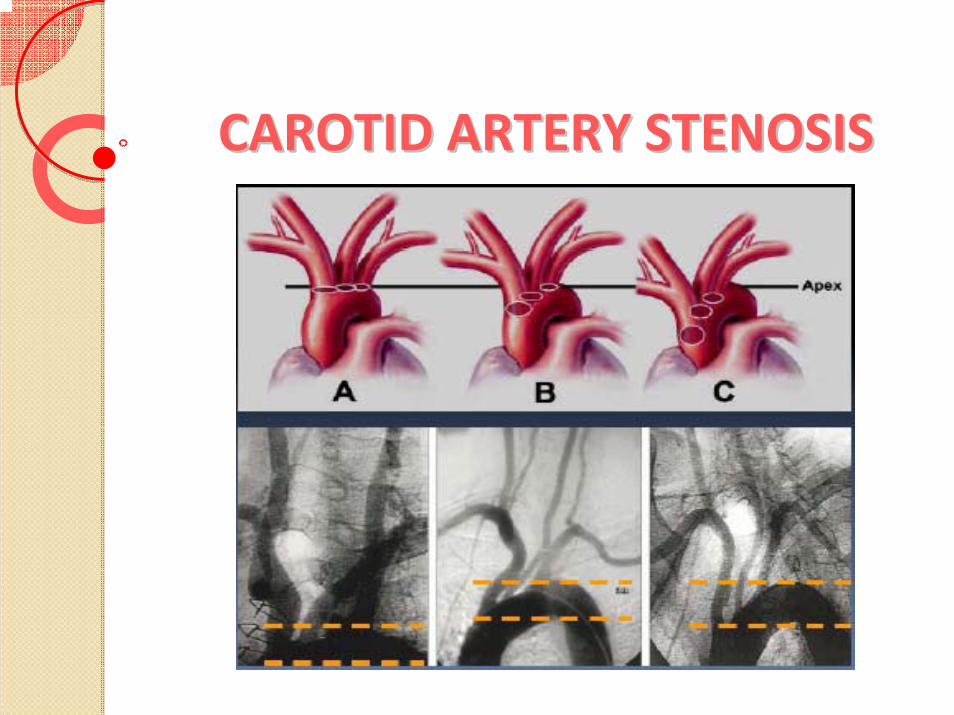
CAROTID ARTERY STENOSISCAROTID ARTERY STENOSIS
Natural Incidence of CVAIn Carotid Stenosis
• Asymptomatic 80% carotid stenosis‐6% / year
• Symptomatic carotid stenosis‐ 10% / year‐ 40% / 5 years
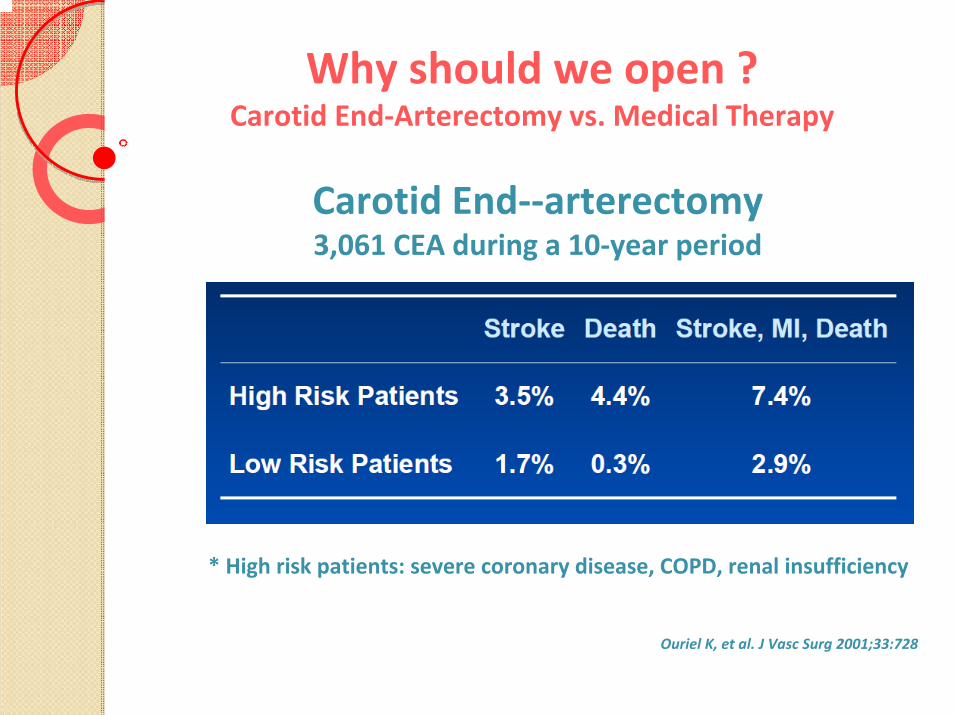
Why should we open ?Carotid End‐Arterectomy vs. Medical Therapy
Carotid End‐‐arterectomy3,061 CEA during a 10‐year period
* High risk patients: severe coronary disease, COPD, renal insufficiency
Ouriel K, et al. J Vasc Surg 2001;33:728
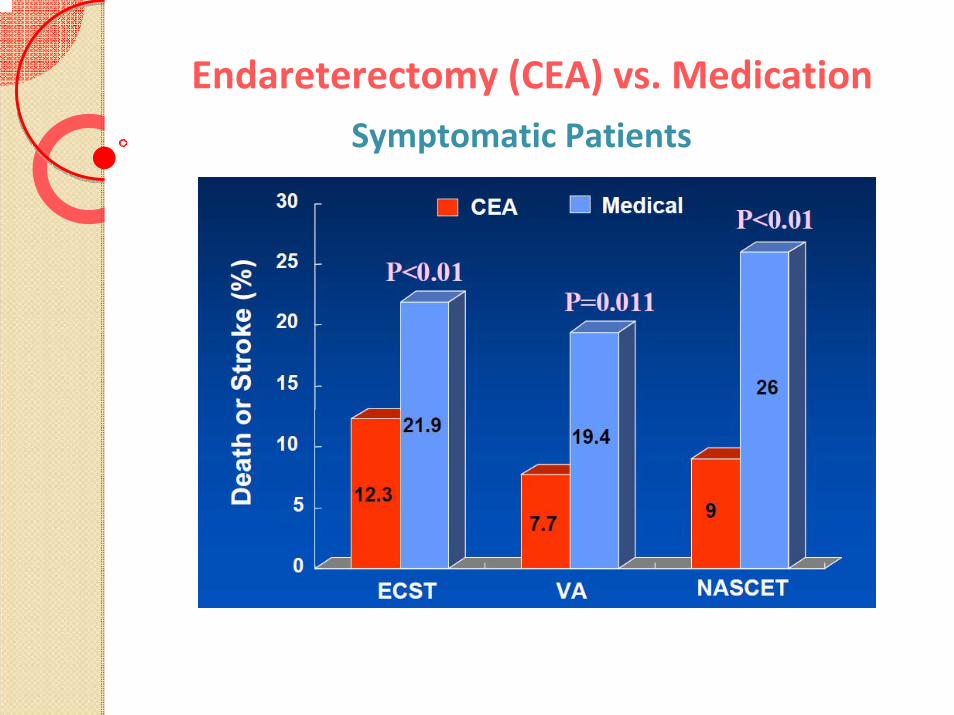
Endareterectomy (CEA) vs. MedicationSymptomatic Patients
Endareterectomy (CEA) vs. MedicationAsymptomatic Patients
MRC Asymptomatic Carotid Surgery Trial (ACST)
‐ Total 3,120 asymptomatic patients
‐ Randomized to CEA vs medical therapy or deferred surgery
‐ Inclusion Criteria: ≥ 60% stenosis on ultrasound
‐ 30 Countries, 126 Hospitals
‐ In the immediate CEA patients (n=1,560)
• 2.8% of perioperative stroke or death
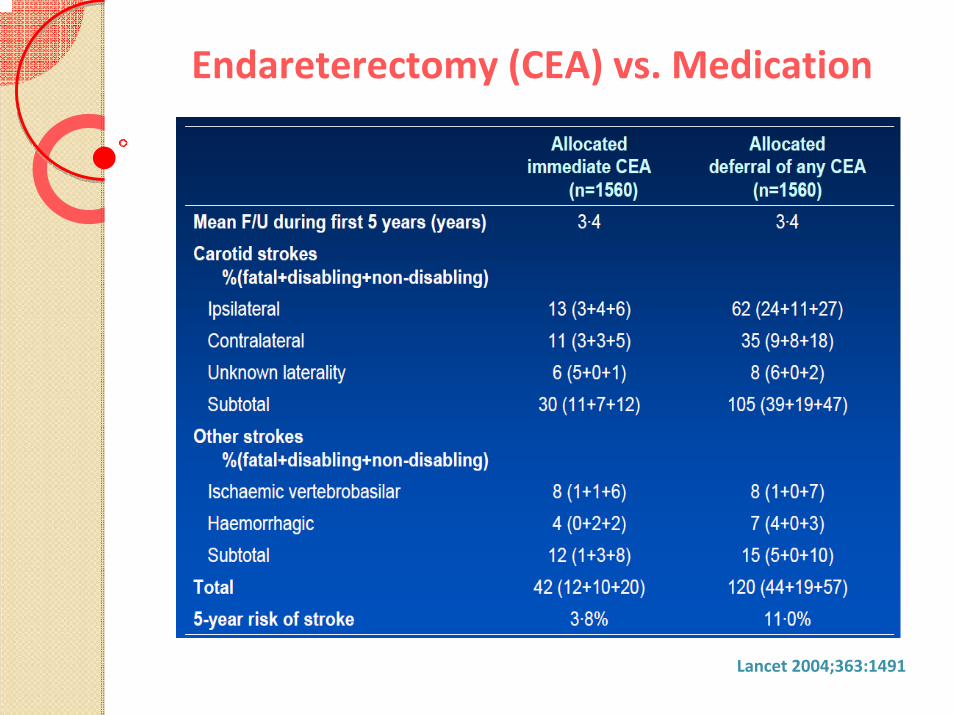
Endareterectomy (CEA) vs. Medication
Lancet 2004;363:1491
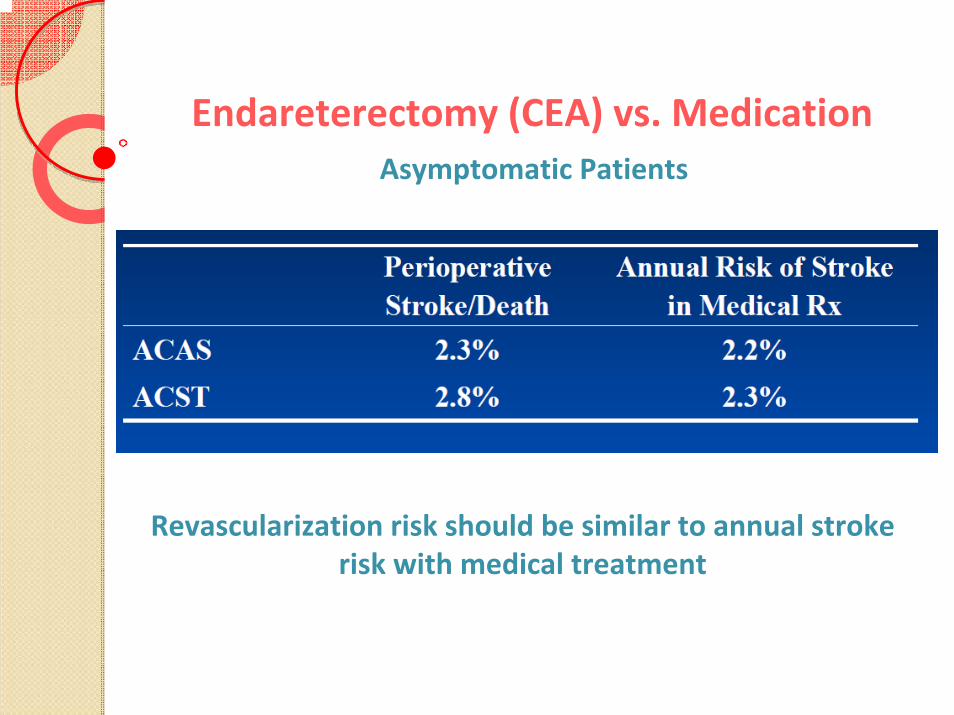
Endareterectomy (CEA) vs. MedicationAsymptomatic Patients
Revascularization risk should be similar to annual strokerisk with medical treatment
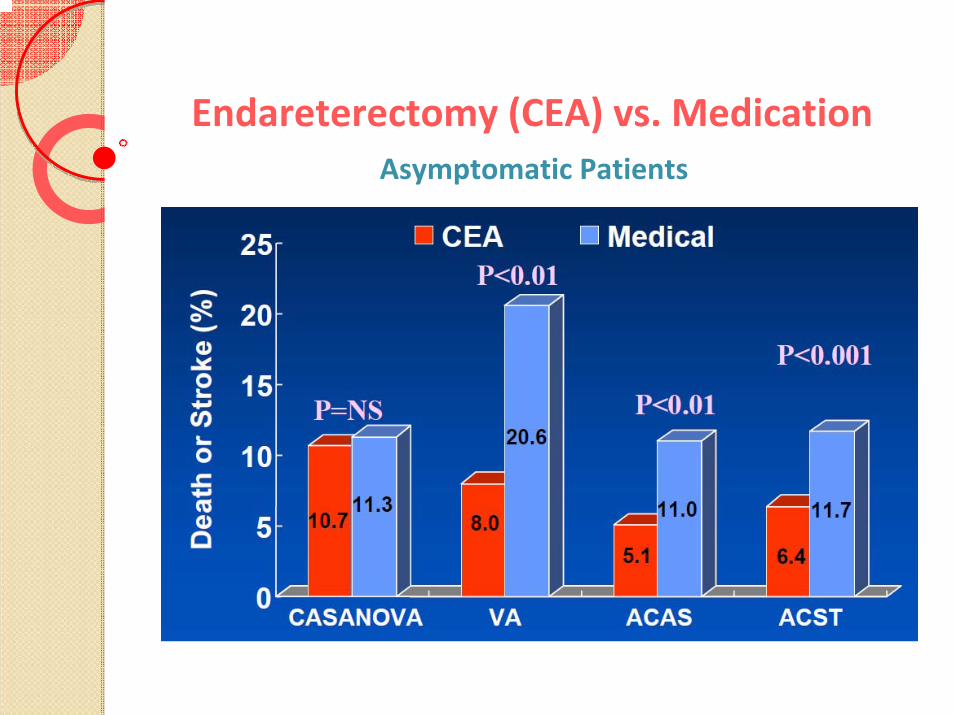
Endareterectomy (CEA) vs. MedicationAsymptomatic Patients
Limitations of CEA
• Perioperative stroke for low risk patients: ~6%
• Anatomic considerations
• Cranial nerve palsies: 7~27%
• Restenosis: ~15%
• > 50% have severe coronary artery disease
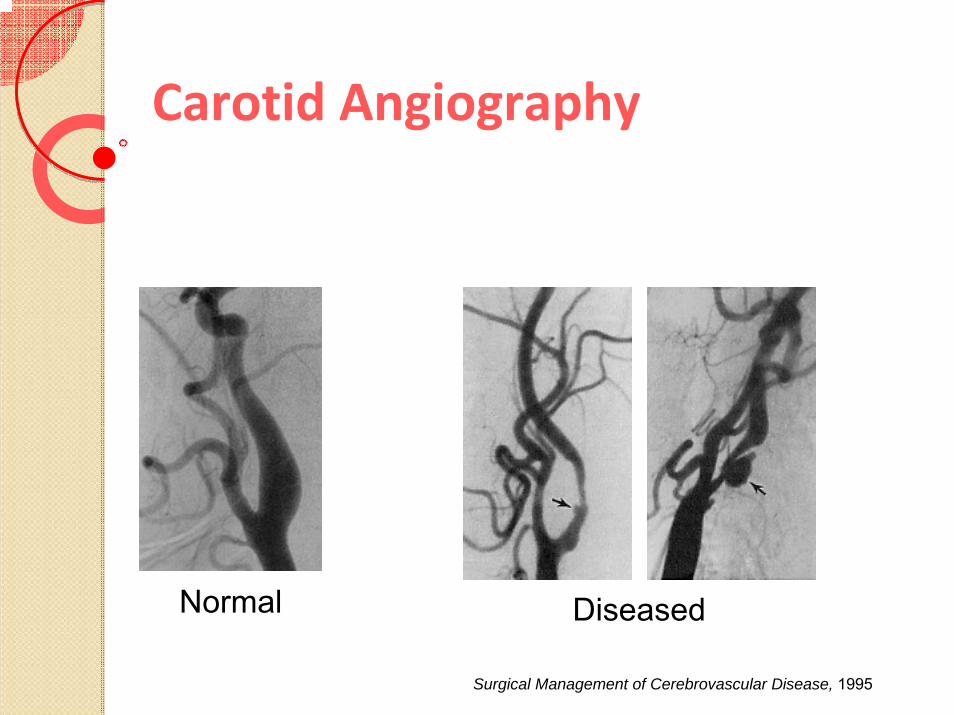
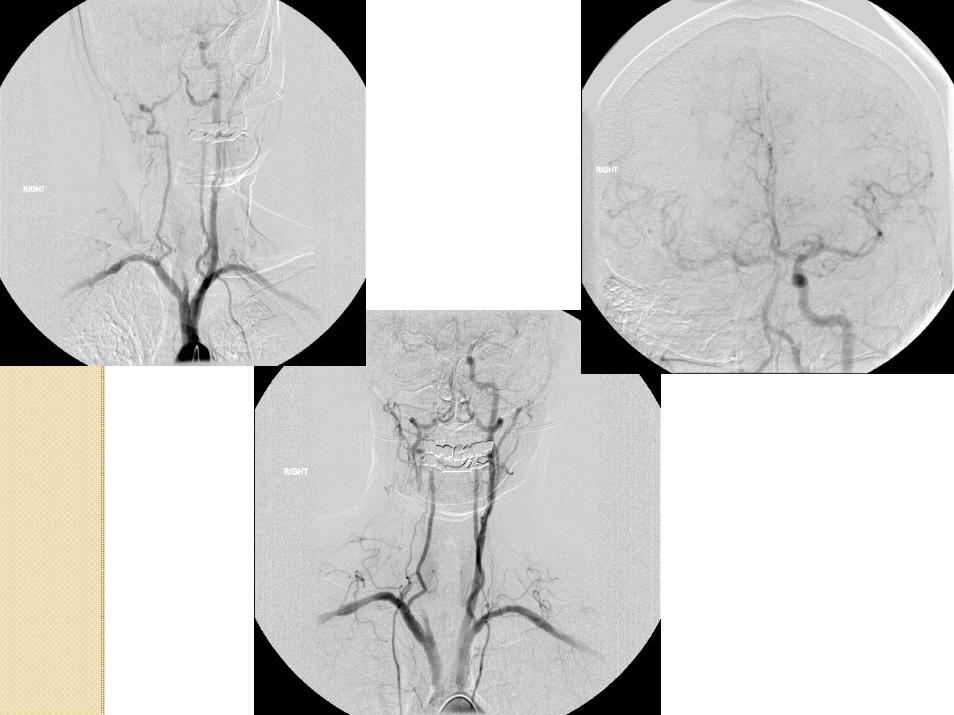
Carotid Angiography
Normal Diseased
Surgical Management of Cerebrovascular Disease, 1995
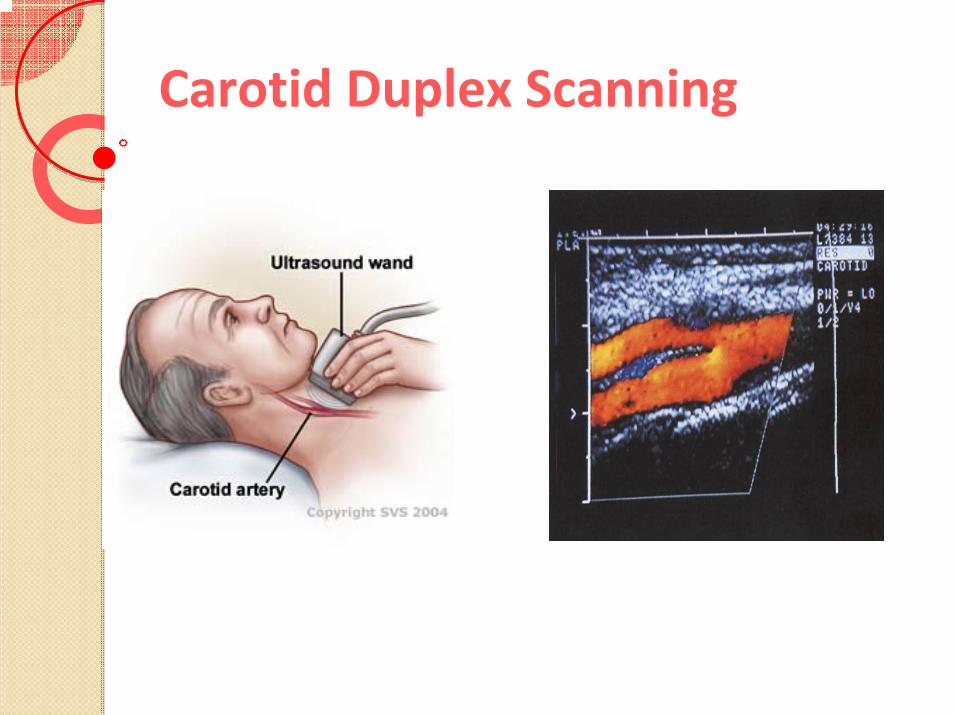
Carotid Duplex Scanning
Treatment options
Ligation
Bypass
Endarterectomy
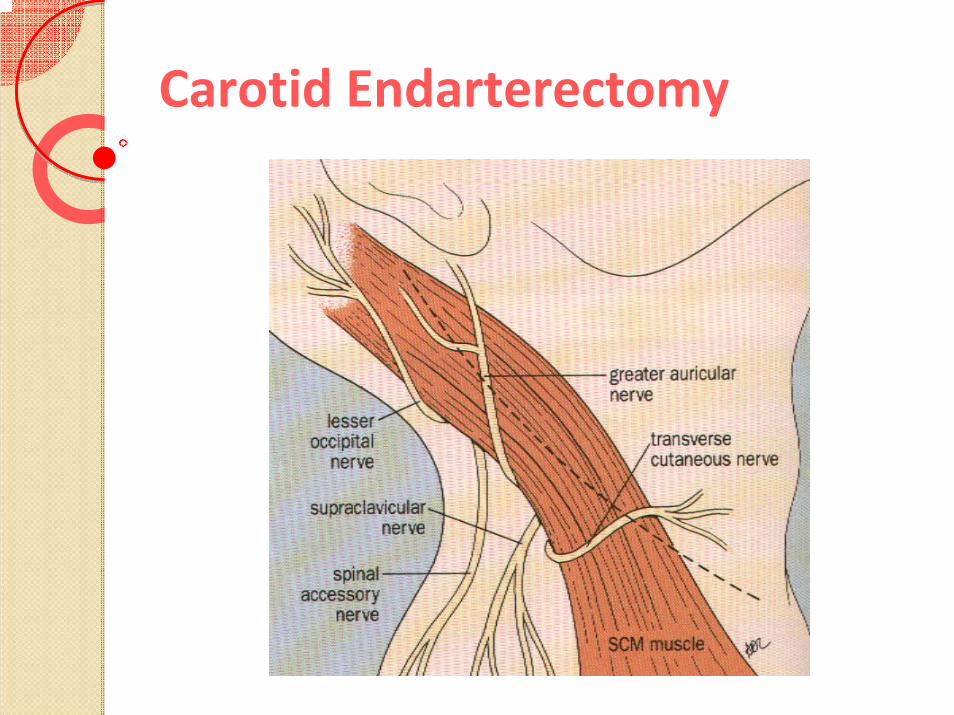
Carotid Endarterectomy
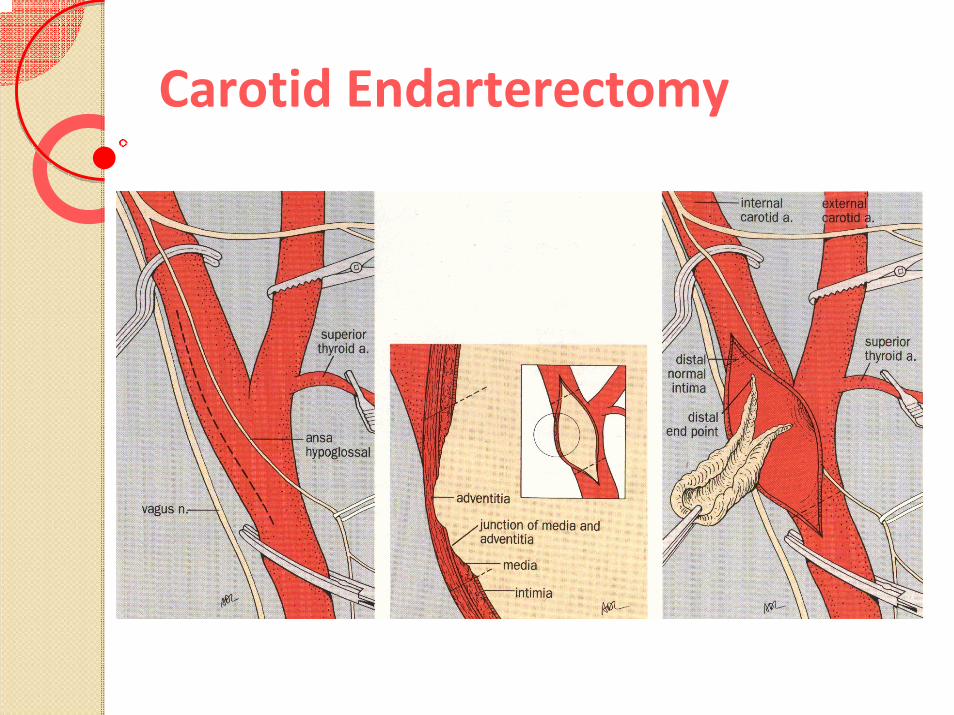
Carotid Endarterectomy
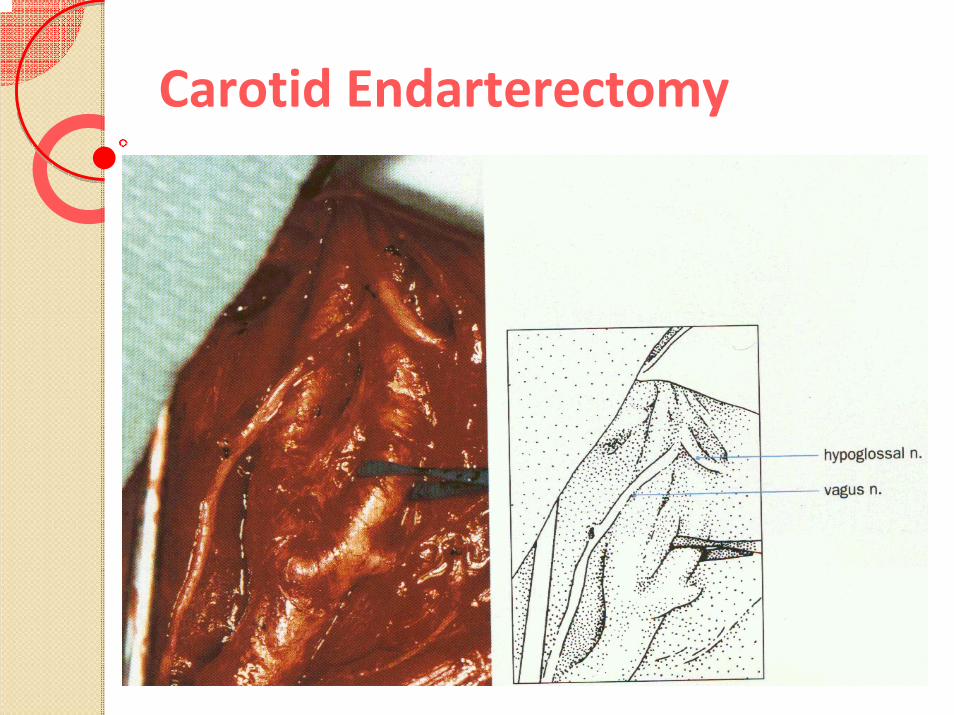
Carotid Endarterectomy
IndicationsUnilateral or bilateral atherosclerotic or restenotic lesions in native carotid arteriesSymptoms + stenosis >50% (NASCET criteria)No Symptoms + stenosis >80% (NASCET criteria)High Risk criteria for CEA◦ CHF◦ Severe COPD◦ Contralateral carotid occlusion◦ Contralateral laryngeal nerve palsy◦ Radical neck surgery/RT◦ Recurrent stenosis after CEA◦ >80 yrs of age

ContraindicationsStroke within previous 48 hsIntraluminal thrombusTotal occlusionVascular disease precluding catheterizationIntracranial aneurysm >9mmNeed for more than 2 stentsBleeding disorderOther interventions planned within 30 daysShort life expectancy <1yrOstial lesion of common carotid or brachiocephalic arteries
Pharmacologic ProtocolBefore the Procedure◦ Aspirin (100‐325 mg)◦ Clopidogrel (Plavix) (75mg/day for 2‐3 days)
During the Procedure◦ Heparin IV (70‐100 IU/Kg) ACT 250‐300 seconds◦ Atropine 1 mg/IV (just before dilation)
Post Procedure◦ Dopamine (infusion pump available)
Long term medication◦ Clopidogrel (Plavix) (75mg/day/1month)◦ Aspirin only, if followed by coronary bypass
IIb/IIIa inhibitors not recommended during CAS
Possible ComplicationsAcute◦ Stroke/embolism◦ Carotid occlusion/dissection◦ Carotid spasm (protection device related)◦ Arterial hypotension◦ Bradycardia/asystole◦ Arterial laceration/rupture◦ Intracranial hemorrhageLate◦ Restenosis◦ Occlusion
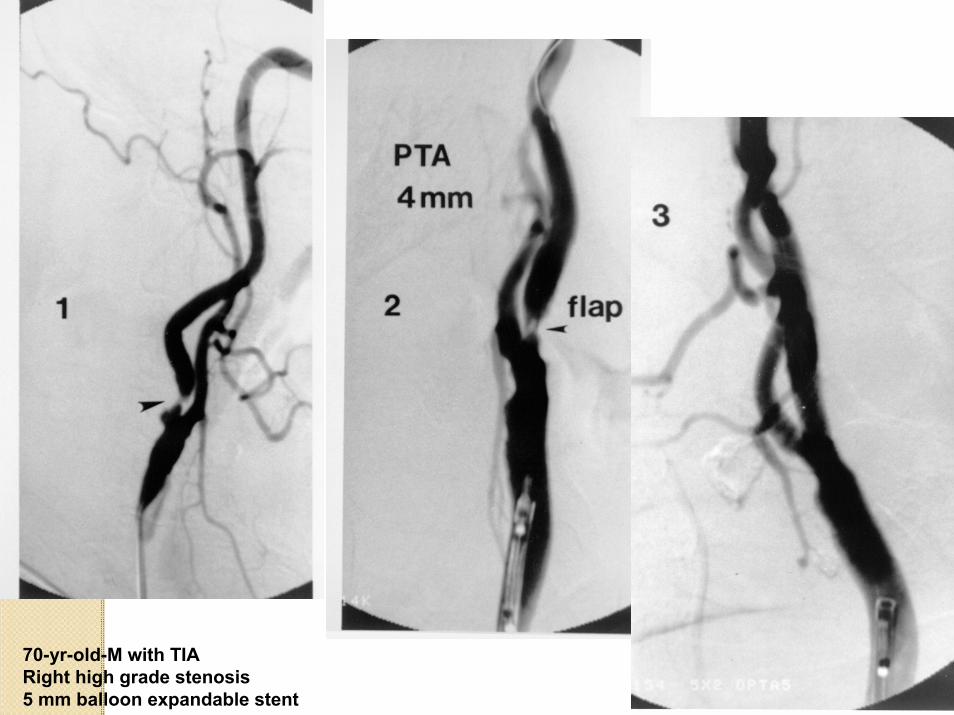
70-yr-old-M with TIARight high grade stenosis5 mm balloon expandable stent
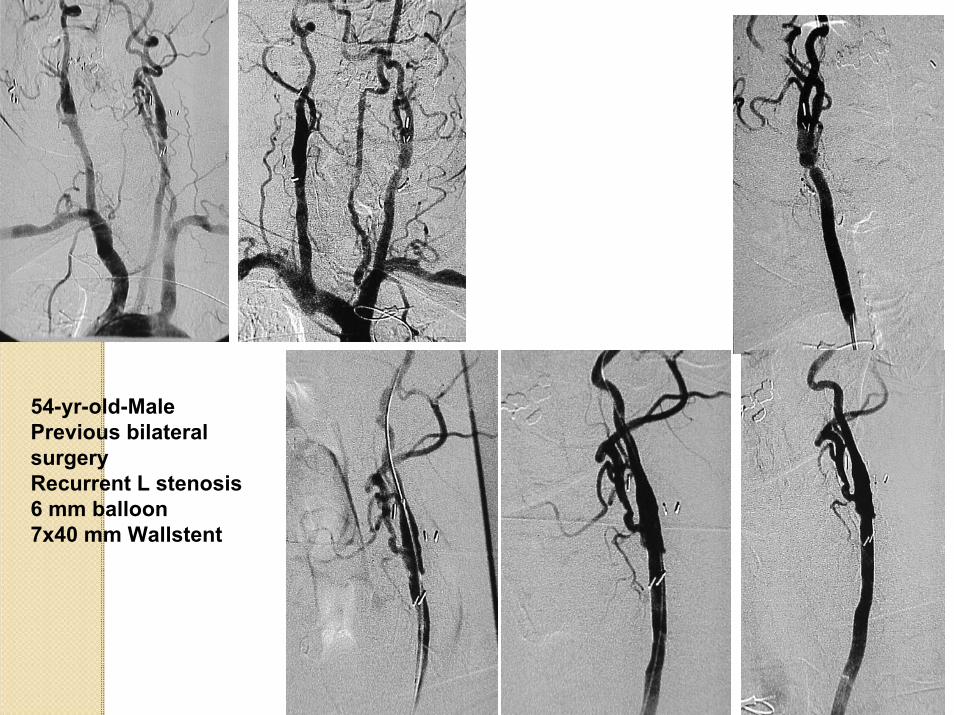
54-yr-old-MalePrevious bilateralsurgeryRecurrent L stenosis6 mm balloon7x40 mm Wallstent
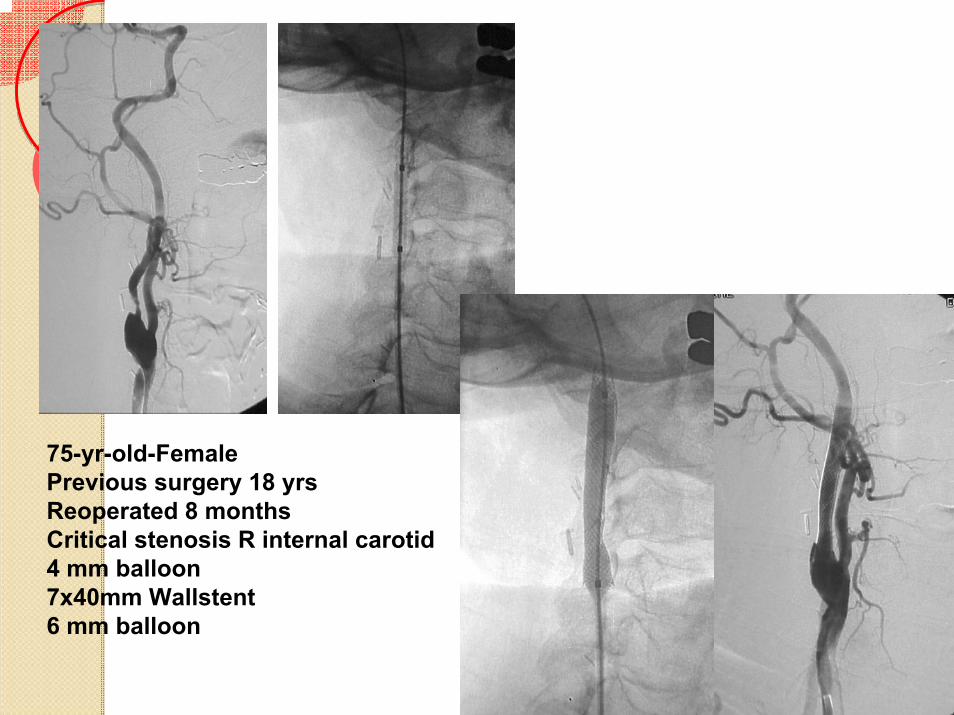
75-yr-old-FemalePrevious surgery 18 yrsReoperated 8 monthsCritical stenosis R internal carotid4 mm balloon7x40mm Wallstent6 mm balloon

Use of protectionDevicesReestenosis @ 12mpost CEAFilter WireEPI device

Protection in “Benign Lesion”is Worthwhile

Technique Carotid Stenting
Acculink Stent

Carotid StentingWith Protection Device Accunet



Neck resection & RTMelanomaTIAs

2 previous CEArecurrent stenosisblurred vision+ dizziness

“Top 10”
to avoid complications in CAS.

1. Selection of patients.
High risk Patientsfor carotid Stenting
Know your patient personally
>80 y of age (asymptomatic)Access problemsBaseline large neurological defectMarked cerebral atrophy + microangiopathyDementia / Alzheimer

2. Selection of lesions.
High risk Lesionsfor carotid Stenting.
Obvious filling defect / thrombusVessel occlusion“String” sign ‐ asymptomatic Severe distal loops/kinks/bends Heavy concentric calcifications

Not recommended for stenting.

3. Adjunctive Pharmacology
Dual Antiplatelet RxASA ‐ 325 mg bid.
Plavix (clopidegrel) ‐ 75 mg bid.
Pre treat all patients with AtropineHeparin, Angiomax (Bivalirudin)
Neo‐synephrin (100ug/cc), Dopamine, NGLNo IIB/IIIA agents
or ASA 650mg + 600mg. Plavix /4hrs.Pre
Embolic / Thrombotic complications (peri and post) are avoided with optimal antiplatelet Rx.

4. Sheath placement.
Placing the stent delivery
catheter in a safe and expeditious fashion is the key
to successful carotid stenting .

Sheath doesn’t advance:
Responses may include….
Exchange 0.038 glide for extra stiff glide or 0.035 ‐ 0.038 exchange wireRemove 5F catheter over the stiff exchange wire and reintroduce original dilator; then advance sheath7F sheath instead of 6F
TERMINATE PROCEDURE!!

Remember!Reassess the patient selection process after the sheath is in place !
Decision to proceed is made after sheath placemen!
5F catheter 6F sheath

5. Embolic protection device
1. Find the best projection2. Do not force the filter across the stenosis or tortuosity !
‐Will and does increase chance of an embolic event‐ Kicks out the sheath from the common carotid artery‐ Increases risk of spasm (isolated hemisphere) and dissection of the
distal carotid artery
3. EPD will not pass‐ Stretch neck (extend head), rotate head – reduces tortuosity‐ EPD won’t easily pass Lesion
a. Support the sheath.b. Pan down to make sure it is not going to prolaps into the arch.c. Leave wire tip across lesion.d. Reach for your already prepped “bail out stuff”
Choice PT wire (Buddy wire)1.5 – 2 mm balloon
e. Cross and pre‐dilate alongside EPD wire

Embolic protection device
Can’t place EPD with ample landing zone for stent !
stop procedure!

6. Speed of the Procedure
Equipment ‐ ready and prepped on the table
From bottom to top by a sterile towels:‐ EPD capture device‐ Post dilatation balloon‐ Stent‐ Pre dilatation balloon‐ EPD delivery system
((“Bail out” stuff for very tight lesions)
EPD dwelling time 7 – 10 min.

7. “Minimum touch minimum contrast” technique
• Bony landmarks /roadmap ?• Position EPD• Pre‐dilate – 3.5mm. / 30 or 40mm.• Stent minimum length ‐ 30 mm.
(No contrast with stent deployment)• Post dilate with one inflation (5mm or rarely 5.5mm)• Retrieve EPD• Final Run ‐ “Done”!

“Minimum touch minimum contrast”technique
1. Post dilate only once with a conservative balloon size.The most dangerous part of the procedure.Size conservatively !!!! ‐5mm for most patients and rarely 5.5mm Inflate only once !!!!
For diagnostic study 4 ccm in 6 ccm syringe 50/50 contrast/salineFor sheath injection 6 ccm in 6 ccm syringe
Check syringe, catheter, sheath, Y adapter for air and particlesBack‐bleed and clear after each device is introduced or removedDo not inject contrast during stent deliveryDraw saline and contrast slowly from closed systems !
Creates micro‐bubbles
2. Minimize contrast injections (contrast is toxic to brain)
3. Micro – emboli (air, particles)

Stent
1. Preferably close cell stent2. Release stent slowly3. Oversize stent (better coverage)4. Stent delivery displaces the bifurcation cephalad

8. Hemodynamic mgt. is Key!!
Hold BP meds. in am.Do not anesthetize or sedate at all!Hydrate well.I/A BP monitoringAlways admin. Atropine 0.6 ‐ 1mg.Aggressively treat bradycardia/ hypotensionKnowledge of Coronary status/LV FnHave Neosynepherine bolus ready.BP does not fall ? Rapidly give NTG or Labetalol.

9. Finally
Communicate with the patient“Duck”, Yawning !!
Ignore the Little Issues pos CAS Spasm (wait, NGL)
Residual Ulceration (will disappear)
Residual Stenosis (not significant)
Kinks (pull proximally the sheath)
ECA stenosed or occluded.
A small “tear” (manual compression)

10. C A V E A T
BE SELECTIVE
NOT ALL LESIONS ARE AMENABLE TO CASespecially when using protection devices.
It is proper to recommend surgery or medical treatment rather then to risk complication.

RENAL ARTERY STENOSISRENAL ARTERY STENOSIS

RENAL ARTERY STENOSISRENAL ARTERY STENOSIS

RENAL ARTERY STENOSISRENAL ARTERY STENOSIS

Incidence of Unsuspected RASIncidence of Unsuspected RAS196 consecutive patients referred for coronary angiography for
suspected CAD underwent (drive‐by) renal angiography.
Jean WJ, et al: Cathet Cardiovasc Diagn 1994;32:8‐10.

Atherosclerotic Atherosclerotic Renal Artery StenosisRenal Artery Stenosis
Incidence of RAS in Patients with Peripheral Vascular Disease
Scoble JE. In Renal Vascular Disease 1996:143‐9

Diagnostic TestsDiagnostic Tests
• IVP
• Renal vein renins
• Radionuclide renography
• Renal artery duplex imaging
• Magnetic resonance angiography
• Spiral computed tomography
• Angiography

DriveDrive‐‐By AngiographyBy Angiography
• Renal angiography during cardiac or peripheral angiography in patients at increased risk for having asymptomatic renal artery stenosis:
‐ Atherosclerosis
‐ Hypertension

Routine Screening AngiographyRoutine Screening AngiographyThe FactsThe Facts
• Incidence of RAS is high in this population.
• Progression (silent) with loss of renal mass.
• Risk of screening angiography is minimal.
• RAS independently impacts prognosis.
• Angiography is the “gold standard” for diagnosis.

Goal of Renal Goal of Renal StentingStenting
• Clinical goals
‐ Improves control of HTN
‐ Preserves renal function
‐ Controls of cardiac syndromes (CHF/Angina)

Criteria For Renal Criteria For Renal StentingStenting
• Which lesions, if any, should be treated ?
‐ Solitary ≥ 70% stenosis.
‐ Bilateral ≥ 70% stenoses.
‐ Unilateral ≥ 70% stenosis.

Effect of Renal Artery Effect of Renal Artery StentingStenting ononRenal Function and SizeRenal Function and Size
• 25 patients (mean 20±11 m)
• Renal stenting:
‐ CRI (Cr ≥ 1.5 mg/dL)
‐ Global renal ischemia (≥ 70% stenosis)
‐ Bilateral RAS
‐ Unilateral RAS with solitary kidney
• Before intervention all negative slope
• After intervention, slopes were positive in 18 and less negative in 7 patients
Circulation 2000;102:1671‐7

Kidney Size Following Renal Kidney Size Following Renal StentingStentingKidney size did not changeKidney size did not change
• Pre‐intervention and serial follow‐up sonograms obtained
• Baseline renal length 10.4±1.4 cm
• Follow‐up renal length 10.4 ±1.1 cm (mean follow‐up 19 ±10 months)
Circulation 2000;102:1671‐7

Atherosclerotic Renal Artery Atherosclerotic Renal Artery StenosisStenosis::Who Should Be Who Should Be RevascularizedRevascularized??
• Dialysis‐dependent renal failure with > 70% renal artery stenosis to entire functioning renal mass
‐ Bilateral RAS
‐ RAS to solitary functioning kidney
• Rapid decline in renal function in the 14 weeks prior to starting dialysis is favorable prognostic sign for recovery of renal function (Hansen, 1995)
Circulation 2000;102:1671‐7

Techniques of Renal InterventionTechniques of Renal Intervention

Renal Artery Renal Artery StentingStenting ‐‐ 19931993 Renal Artery Renal Artery StentingStenting ‐‐ 20062006

Atheroembolism

Optimal TechniqueOptimal TechniqueSevere atherosclerotic disease of abdominal aortaSevere atherosclerotic disease of abdominal aorta
• Minimize catheter manipulation in the aorta Engage renal artery with softer diagnostic catheter (telescoped inside guide catheter) “No touch” technique
• Consider brachial artery approach for heavily diseased abdominal aorta or extreme downward take‐off of renal artery
• Consider embolic protection for high risk cases with appropriate anatomy

““No TouchNo Touch”” TechniqueTechnique



Optimal TechniqueOptimal TechniqueSevere Baseline Renal InsufficiencySevere Baseline Renal Insufficiency
• Pretreatment for contrast nephropathy:
‐ Hydration
‐Mucormist
‐Sodium Bicarbonate
• Minimize contrast use:
‐ DSA
‐ Low or iso‐osmolar contrast
‐ Strict discipline with injections
‐Intraarterial Gadolinium or CO2 – IVUS
• Distal protection?

Optimal TechniqueOptimal TechniqueOstialOstial DiseaseDisease
• Identify the true ostium –angulated views
• Adequate predilatation
• Leave stent 1‐2 mm into aorta
• Account for stent shortening
• Confirm complete ostialcoverage

Distal Protection During Renal Distal Protection During Renal StentingStenting

Distal ProtectionDistal Protection• Distal protection has a powerful effect on adverse events during SVG intervention
‐ preliminary data suggest that distal protection may prevent renal insufficiency after renal intervention‐ However, anatomy may limit utility in renal application
Edward MS, et al: J Vasc Surg 2006;44:128‐35.

Peripheral Arterial Disease Peripheral Arterial Disease (PAD) (PAD)

Peripheral Arterial Disease (PAD)
Chronic◦ Slow, gradual luminal stenosis 2° plaque enlargement
◦ Collateral development compensates
◦ Symptoms proportional to disease burden
◦ Exertional symptoms may appear first
Acute◦ Sudden occlusion in the absence of adequate collaterals
◦ Embolization (cardiogenic, proximal arteries)
◦ Thrombosis superimposed on occlusive disease plaque rupture
failure of a previous vascular reconstruction
◦ Injury

Distribution of Chronic PAD
Extremities◦ Lower◦ Upper?
Mesenteric◦ Celiac◦ SMA◦ IMA
Renal (limited collateral potential)

Chronic PAD of the Lower Extremities
Aorto‐iliac
Femoropopliteal(SFA most common)
Tibial (especially diabetics)
Vascular Surgery (Rutherford, Ed), 2000

Chronic LE PAD: Symptoms
NoneIntermittent claudication◦ Exertional muscular ischemia (calf, thigh, buttock)◦ Analogous to stable anginaRest pain◦ Blood supply inadequate to meet resting metabolic needs◦ Affects tissue furthest from the heart◦ May be relieved by dependency
Tissue loss ◦ Non‐healing traumatic ulcer◦ Spontaneous gangrene

Chronic LE PAD: Physical Findings
Pulse exam (especially femoral)
◦ Distinguish normal vs abnormal
◦ Symmetry
◦ Bruit or thrill
◦ Aneurysm
◦ Evaluate non‐palpable pulses with CW doppler
Trophic signs (Muscular atrophy, absent hair growth)
Dependent rubor/elevation pallorTissue loss (ulceration, gangrene)

Chronic LE PAOD: Non‐invasive evaluation
Ankle‐Brachial Index (ABI)◦ Best brachial SBP/Ankle SBP
◦ Normal value: ≥ 1.0
◦ Claudication: 0.4 ‐ 1.0
◦ Limb‐threatening: ≤ 0.4
Calcified vessels produce inaccurately high ABI’s◦ Common in diabetes and renal failure
◦ ABI should be consistent with other measures (PE, PVR)
Exercise (treadmill) testing◦ reveals pressure drop in claudication when ABI normal
◦ can identify “pseudoclaudication” (i.e. spinal stenosis)

Ankle‐Brachial Index (ABI)
ABI falls as disease burden increases
Life expectancy falls with ABI
Vascular Surgery (Rutherford, Ed) 2000

PAD is a risk factor for overall cardiovascular mortality
Vascular Surgery (Rutherford, Ed), 2000
PAD patients are much more likely to die of MI than undergo amputation

Chronic LE PAD: Treatment Considerations
PAD is a marker of diffuse atherosclerosisPAD identifies a need for risk factor interventionClaudication is a lifestyle‐limiting (not typically limb‐threatening) problemBe aggressive if ischemia is limb‐threateningRisk/benefit decision

Chronic LE PAD: Treatment Options
Risk factor modification (almost always)
Exercise (for claudication)
Pharmacotherapy ◦ rarely for claudication
◦ not effective for limb‐threatening ischemia
Revascularization◦ Endovascular (balloon angioplasty/stenting)
◦ Surgery
Amputation◦ failed revascularization
◦ may occasionally be appropriate 1° treatment

Intermittent Claudication
Generally not limb‐threatening◦ Usually represents single‐level disease (SFA most common)
◦ ABI ~ 0.7
◦ Risk factors for progression to limb‐threatening ischemiaSmoking
Diabetes
Low ABI at presentation (<0.50)
First‐line treatment◦ Exercise
◦ Risk factor modification (especially smoking)
Pharmacotherapy? (Good in theory, poor in practice)
Revascularization? (Intolerable lifestyle limitation in good risk patient)

Claudication & Smoking
Risk factor for progression to limb‐threatening ischemia
Shortens walking distance at any given ABI
Cessation will predictably double walking distance

Effect of exercise on claudication
Gardner et al, J Cardiopulm Rehabil, 2002
Predictably doubles walking distance
The sedentary, smoking claudicant could quadruple walking distance with smoking cessation and exercise

Pharmacotherapy for claudication
Dawson et al, Am J Med, 2000
Cilostazol (Pletal®) better than pentoxifylline (Trental®)
~ 50% improvement in walking distance with cilostazol
Minimal benefit vs smoking cessation or exercise

Limb‐threatening ischemia
Rest pain or tissue loss◦ Usually multi‐level disease (Aorto‐iliac, fem‐pop, tibial)
◦ ABI typically <0.4
Nearly absolute indication for revascularization ◦ some type of operation is in the patient’s future
◦ Frail elderly patients poor candidates for prosthetic ambulation
◦ ?Primary amputationNon‐ambulators
Healthy with excellent potential for prosthetic function

Diabetes and PAD
Risk factor for limb‐threatening ischemia◦ Higher likelihood of tibial artery disease
◦ Neuropathy predisposes to foot wounds
◦ Severe deep space foot infections
Wound healing poorer at any given ABI vs non‐diabetics
Vascular calcification may artifactually elevate ABI
Dismal prospects for limb‐salvage if combined with renal failure

Chronic LE PAOD: Role of Angiography?
NOT for diagnostic purposesUsed for planning therapy after decision to intervene has been made

Lower extremity revascularization:endovascular options
Balloon angioplasty/stenting◦ Most commonly applied to aortoiliac segment◦ Favorable lesion: short, concentric stenosis◦ Unfavorable lesion: long, eccentric stenosis or occlusion
Atherectomy (rarely)

Lower extremity revascularization: surgical options
Aorto‐bifemoral bypassVascular Surgery (Rutherford, Ed) 2000

Lower extremity revascularization: surgical options
Wylie’s Atlas of Vascular Surgery, 1992

Lower extremity revascularization: Graft patency & limb salvage
Graft patency (80‐90% @ 5 yrs)
Limb salvage (~90% @ 5 yrs)
Taylor, J Vasc Surg, 1990

Lower extremity revascularization: Survival
Limb‐threatening ischemia is a marker for a “malignant” disease
Taylor, J Vasc Surg, 1990

Summary
Vascular surgeons diagnose and treat atherosclerosis in non‐coronary vascular territories (carotid, lower extremities, renal, mesenteric) using both endovascular and surgical techniques.
Complete clinical evaluation possible in most patients with H&P supplemented with vascular laboratory (common sense hemodynamic approach)
CEA can prevent strokes in patients with >50% stenosis (Level 1 evidence)
Lower extremity PAD (ABI) is a marker for heavy systemic atherosclerotic disease burden >> treat risk factors
Primary treatment for claudication: exercise, stop smoking
Limb‐threatening ischemia >> revascularization

Basic PAD Facts
Which of the following statements regarding peripheral arterial disease is NOT true?
A. PAD is a manifestation of atherosclerosis and has become recognized as a “coronary disease equivalent”
B. PAD has a distinct set of risk factors that separate it from coronary artery disease.
C. Vulnerable plaques are characterized by large necrotic cores and thin fibrous caps
D. Lesions causing symptoms of PAD typically occur at major arterial bifurcations.

LOWERLOWER‐‐LIMB INTERVENTIONS:LIMB INTERVENTIONS:TASC II 2007 vs. TASC 2000TASC II 2007 vs. TASC 2000

IMPORTANCE OF SUBINTIMAL IMPORTANCE OF SUBINTIMAL ANGIOPLASTY FOR LOWERANGIOPLASTY FOR LOWER‐‐LIMB PTALIMB PTA

BTK PTA: TOOLS OF THE TRADEBTK PTA: TOOLS OF THE TRADE
Biondi‐Zoccai et al, J Endovasc Ther 2009

112 2 Choices Choices 33
STENTSTENT

THANK YOUTHANK YOU