interventional pharmacoeconomics: a new discipline for a ... pdx.pdf · interventional...
TRANSCRIPT

Interventional Pharmacoeconomics: A New Discipline for a Cost-Constrained
Environment
Mark J. Ratain, MDThe University of Chicago
Washington State Medical Oncology Society
Seattle, WAMay 3, 2019
1

Mark J. Ratain, MDACCME Conflict of Interest Disclosure
• Expert testimony and patent litigation consulting on behalf of multiple generic pharmaceutical companies
• Research funding (clinical trials) from AbbVie & Genentech
• Director and Treasurer, Value in Cancer Care Consortium
• I WILL DISCUSS OFF-LABEL DOSES AND SCHEDULES 2

Interventional pharmacoeconomics
• Goal is to reduce prescribing costs through development of new therapeutic regimens– Intersection of clinical trials and
pharmacoeconomics• Not about price regulation– “Free market solution” to problem of high
costs of modern therapeutics
3

Potential interventional pharmacoeconomic strategies
1. Substitution of therapeutic alternative (with comparable efficacy)2. Lower dosages (with comparable efficacy)
3. Less frequent dosing (with comparable efficacy)4. Shorter duration (with comparable duration of benefit)
4

5

$2000 vs $50 per dose
6
2011
Funded by NEI

7
Ophthalmol, 2006

8
2017

.
AttardG et al. JCO 2008;;26:4563-4571
©2008 by American Society of Clinical Oncology
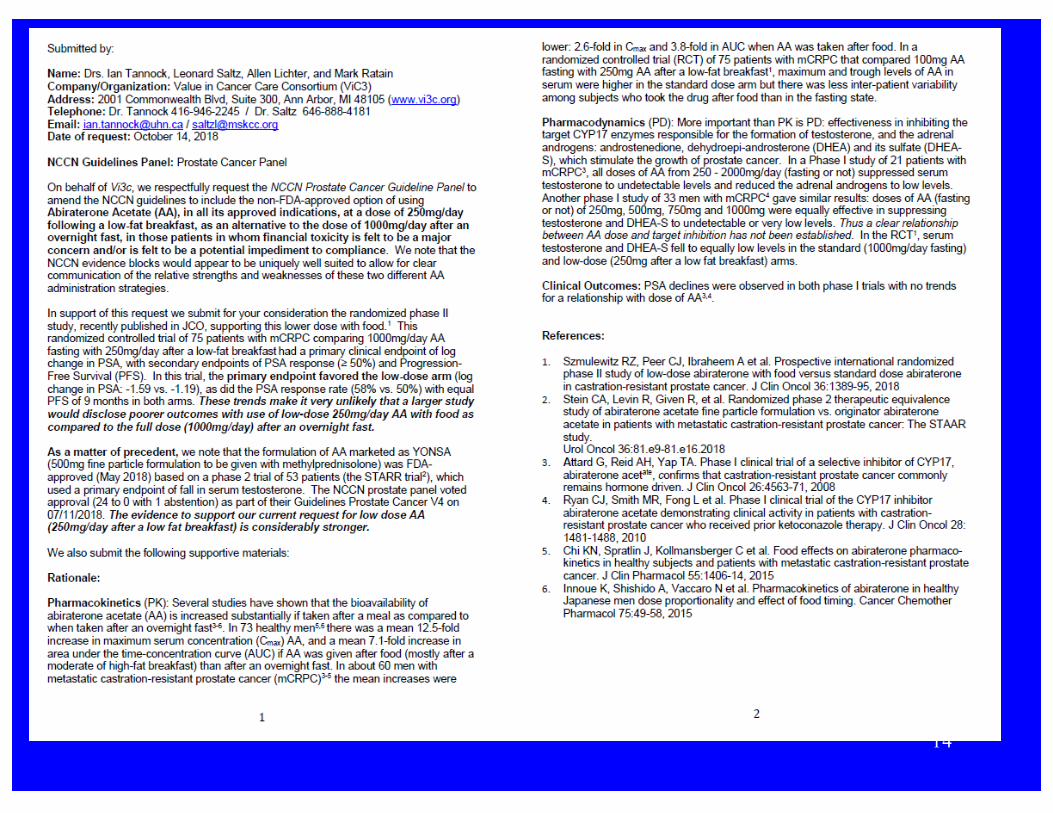
1000 mg dose


11

12

www.vi3c.org
13
14

15
3/6/2019

Potential for value-based prescribing of oral drugs
Mark J. Ratain, MD Allen S. Lichter, MD
The University of Chicago and the Value in Cancer Care Consortium
European Society of Medical OncologyMunich, GermanyOctober 22, 2018
16

Objectives
1. To identify patent-protected oral oncology agents for which the prescribing costs could be reduced by >33%.
2. To quantify the potential cost-savings for individual drugs and for the oral oncology market as a whole.
17

Results I
• As of 8/2018, 56 patent-protected oral oncology products– 34/56 (61%) have identifiable strategies for significant cost
reduction (range 33-89%)• Dose reduction 21• Frequency reduction (due to flat pricing) 12• Therapeutic substitution 1
– 11/56 (20%) appear optimally dosed– 11/56 (20%) have insufficient information
18

Approaches to interventional pharmacoeconomics
1. Substitution of therapeutic alternative (with comparable efficacy)– Sirolimus for everolimus– Paclitaxel for nab-paclitaxel
19

20

Approaches to interventional pharmacoeconomics
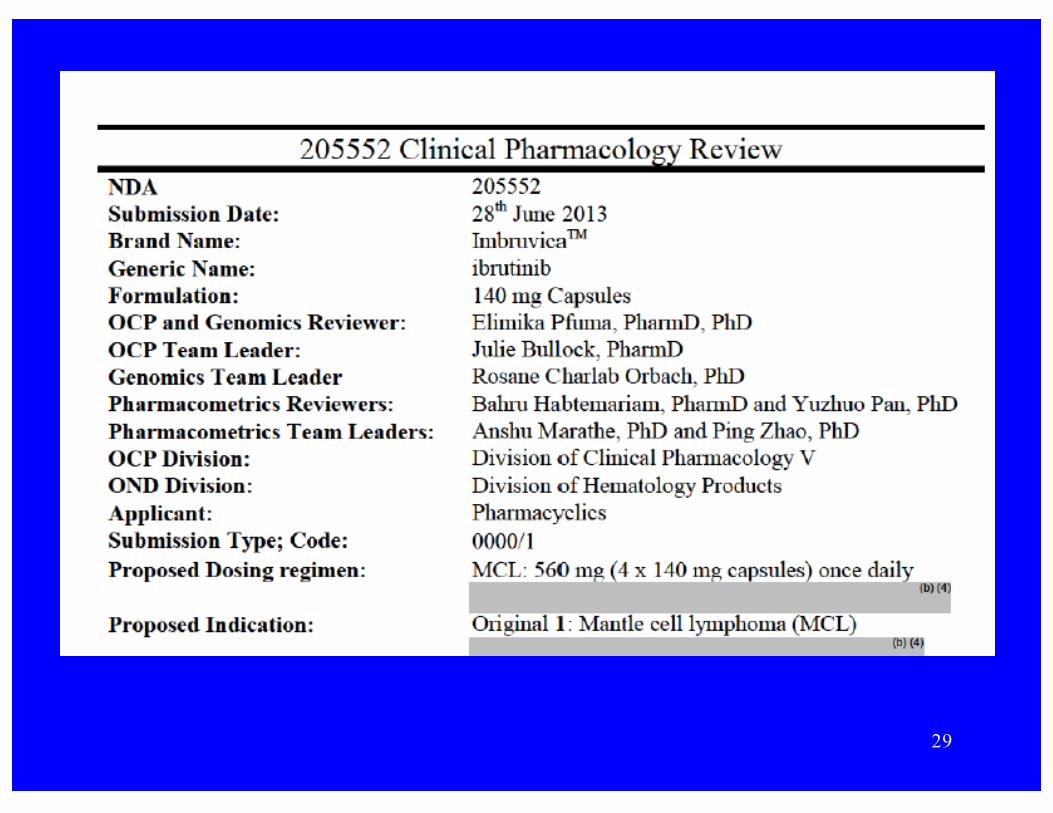
• 2. Lower dosages, with comparable efficacy, and potential reductions in toxicity– Nilotinib– Ibrutinib– Lapatinib– Ceritinib
21

Nilotinib labeled to be taken fasting
22


24

In other words, if you take nilotinibwith breakfast, you might die!!!
25

Remedy = 50% dose reduction taken with food
26


29


31

A pilot study of lower doses of ibrutinib in patients with chronic lymphocytic leukemia
by Lisa S. Chen, Prithviraj Bose, Nichole D. Cruz, Yongying Jiang, Qi Wu, Philip A. Thompson, Shuju Feng, Michael H. Kroll, Wei Qiao, Xuelin Huang, Nitin Jain, William
G. Wierda, Michael J. Keating, and Varsha Gandhi
BloodVolume 132(21):2249-2259
November 22, 2018
©2018 by American Society of Hematology

Lisa S. Chen et al. Blood 2018;;132:2249-2259
©2018 by American Society of Hematology

Lower doses in cycles 2 and 3 reduce inhibition of platelet function by ibrutinib.
Lisa S. Chen et al. Blood 2018;;132:2249-2259
©2018 by American Society of Hematology

35

“Pack splitting” of levantinib – same average daily dose but 50-67% savings
36

Approaches to interventional pharmacoeconomics
• 3. Less frequent dosing (with comparable efficacy)– Nivolumab– Pembrolizumab– Atezolizumab– Trastuzumab
37

38
Predicted trough concentration 18% lower
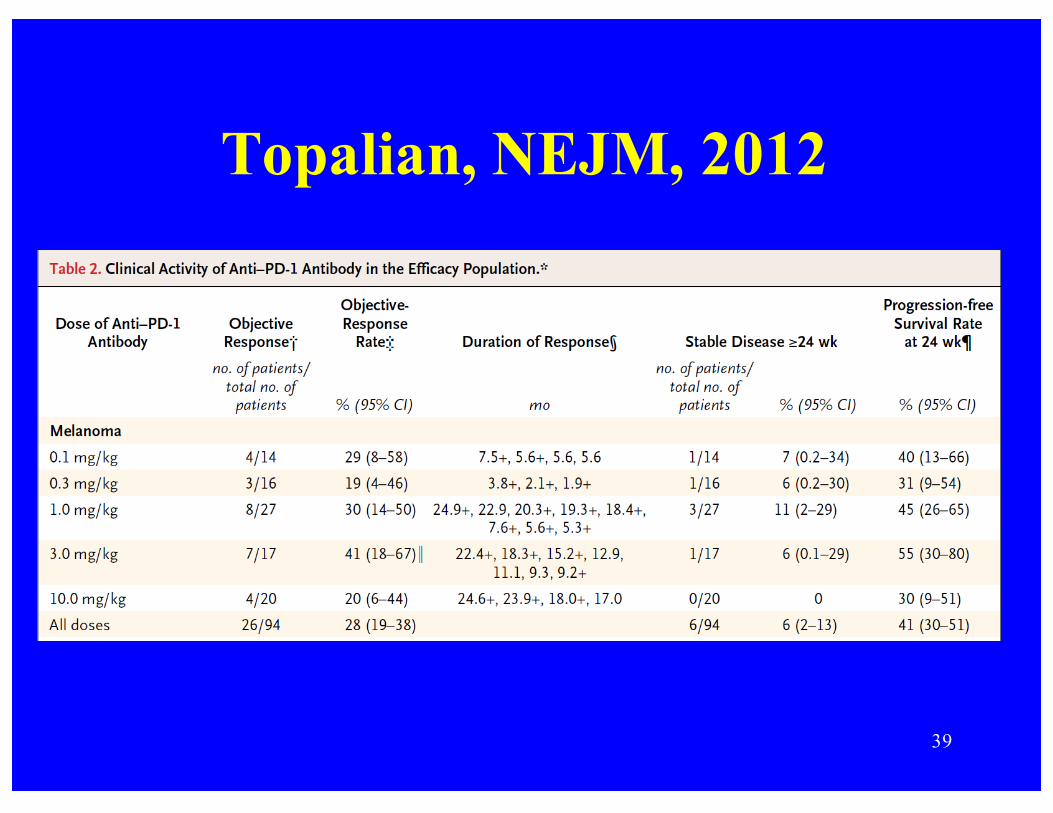
Topalian, NEJM, 2012
39

40

Fig 2. (A) Progression-free and (B) overall survival by treatment arm (randomly assigned patients). Tick marks represent censored observations.
Motzer, JCO, 2015
Nivolumab for metastatic renal cell carcinoma: results of a randomized phase II trial
Flat dose-response over range of 0.3-10 mg/kg q3w

42

43
Observed Cminss at 3 mg/kg Q2W = 52.7 µg/mL
Predicted Cminss at 0.3 mg/kg Q3W = 4.2 µg/mL

44

Interventional pharmacoeconomic studies can save real money!!
45
$4.9
$2.7$1.7
$1.4$0.9$0.9
$0.8$0.7
$0.4
$0.4 $1.6
Potential global savings per year by drug ($B)

Potential industry responses to interventional pharmacoeconomic studies
1. Raise prices2. Encourage physicians to prescribe
according to the label3. Threaten legal and/or regulatory action
46

47

48
April 13, 2018

49
April 18, 2018

50
May 15, 2018 (company made announcement on May 11)
51
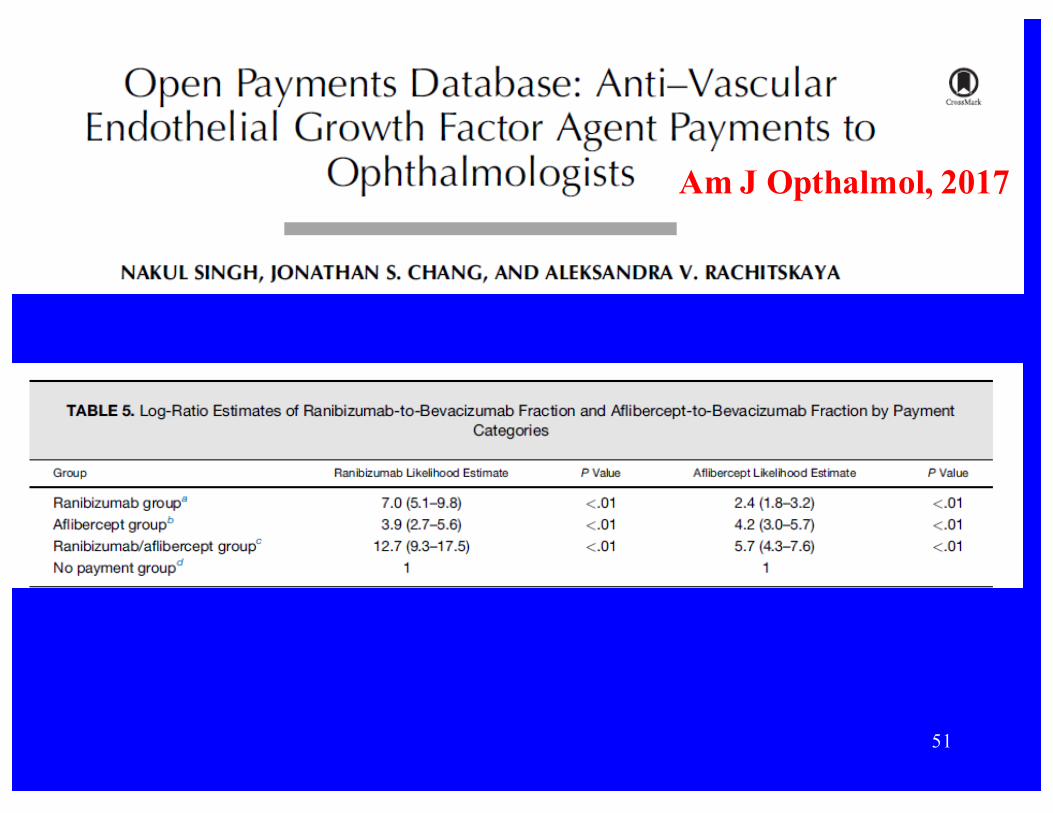
Am J Opthalmol, 2017

52

53
Funding models for interventional pharmacoeconomic studies
1. Direct government support2. Philanthropic contributions3. Repurposing of drug costs within a
single closed health care system4. Consortia studies funded per patient by
select payers
54

Within a single closed health care system, IVPE studies are self-funding
• Standard care, ibrutinib 420 mg qd– Cost $480/day
($14,400/mo)• Experimental arm,
ibrutinib 140 mg qd– Cost $160/day
($4,800/mo)
• Clinical trial, 50% standard and 50% experimental– Mean cost $320/day
($9,600/mo)– Savings on drugs
$160/day ($4,800/mo) covers research costs
55

Creating a consortium focused on IVPE studies
• General concept is similar to that for a single closed system
• In consortium, eligibility requires payer approval– And payer funding per case!!
• Payers can be HMOs, insurance companies, self-insured corporations and even states (for Medicaid patients)
56

Conclusions
• Interventional pharmacoeconomics can reduce prescribing costs without price regulation.
• There are numerous strategies to fund and conduct interventional pharmacoeconomic studies in the context of community oncology practices and health maintenance organizations.
57