interpreting the coagulopathy of trauma-shock
DESCRIPTION
Interpreting the Coagulopathy of Trauma-Shock. Faculty. Bryan A. Cotton, MD, MPH The University of Texas Health Science Center Houston, Texas. Richard P. Dutton, MD, MBA University of Maryland School of Medicine R Adams Cowley Shock Trauma Center Baltimore, Maryland. - PowerPoint PPT PresentationTRANSCRIPT

Interpreting the Coagulopathy of Trauma-Shock
Interpreting the Coagulopathy of Trauma-Shock
FacultyFaculty
2
Bryan A. Cotton, MD, MPH
The University of Texas Health Science Center
Houston, Texas
Richard P. Dutton, MD, MBA
University of Maryland School of Medicine
R Adams Cowley Shock Trauma Center
Baltimore, Maryland
Martin A. Schreiber, MD, FACS
Oregon Health & Science University
Portland, Oregon
Mortality After TraumaMortality After Trauma
Stewart RM, et al. J Trauma . 2003;54:66-71.3
Retrospective review of trauma death at level I trauma center (Stewart et al, 2003)
● Leading causes of death CNS, 51% Shock, 21% CNS + Shock, 16%
Time to DeathTime to Death
• Within 12 h of arrival to ED
50% of trauma patients are dead
• Within 48 h of arrival to ED ≈70% of trauma patients are dead
• Early interventions can impact a patient’s life
Stewart RM, et al. J Trauma. 2003;54:66-71. 4
Coagulopathy and MortalityCoagulopathy and Mortality
• Retrospective review
• N=1867, 24.4% of patients significantly coagulopathic
• Coagulopathy defined as:
1.5 x normal• Mortality
Overall, 19.5% Noncoagulopathic, 10.9% Coagulopathic, 46%
Brohi K, et al. J Trauma. 2003;54:1127–1130. 5

Adapted from Brohi K, et al. J Trauma. 2003;54:1127–1130.
Coagulopathy and Mortality
6
100
80
60
40
20
0
Mortality
0-14 15-29 30-44 45-59 59-64
Injury Severity Score
Per
cen
t M
ort
alit
y
Normal
Coagulopathy

Acute Coagulopathy of TraumaAcute Coagulopathy of Trauma
7
2.1
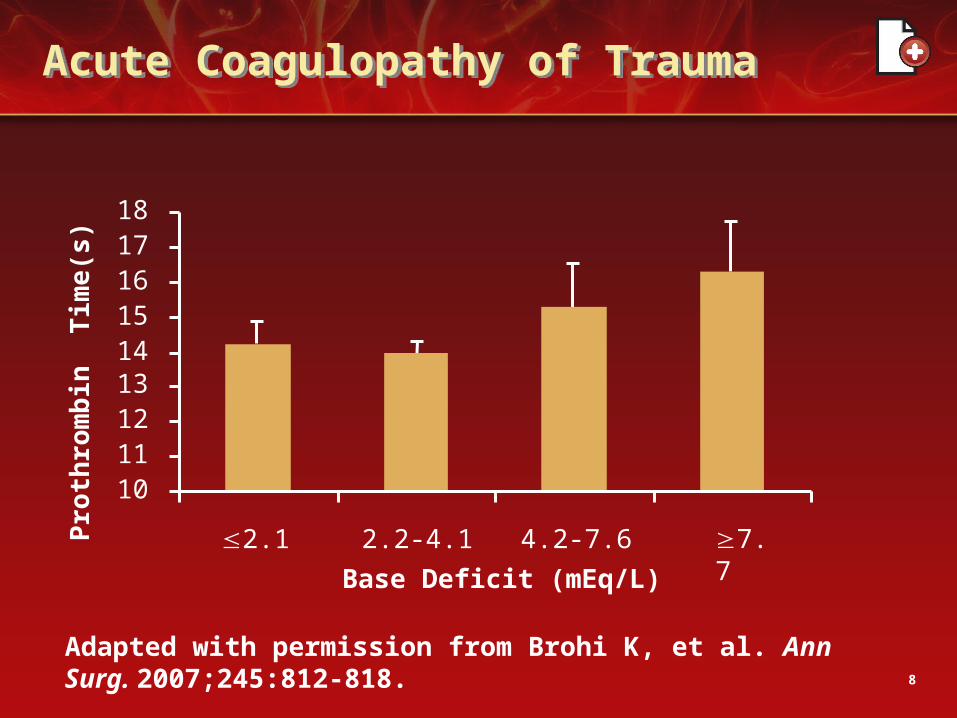
Acute Coagulopathy of TraumaAcute Coagulopathy of Trauma
8
Adapted with permission from Brohi K, et al. Ann Surg. 2007;245:812-818.
101112131415161718
2.2-4.1 4.2-7.6
Base Deficit (mEq/L)
Pro
thro
mb
in T
ime
(s)
7.7
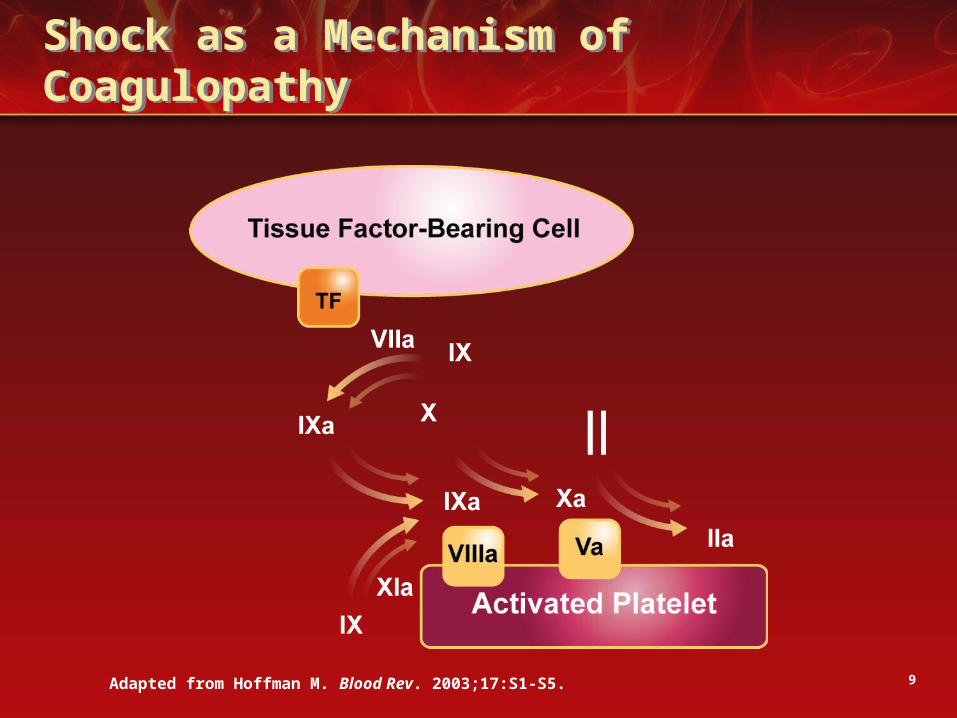
Shock as a Mechanism of CoagulopathyShock as a Mechanism of Coagulopathy
9Adapted from Hoffman M. Blood Rev. 2003;17:S1-S5.
7.72.1
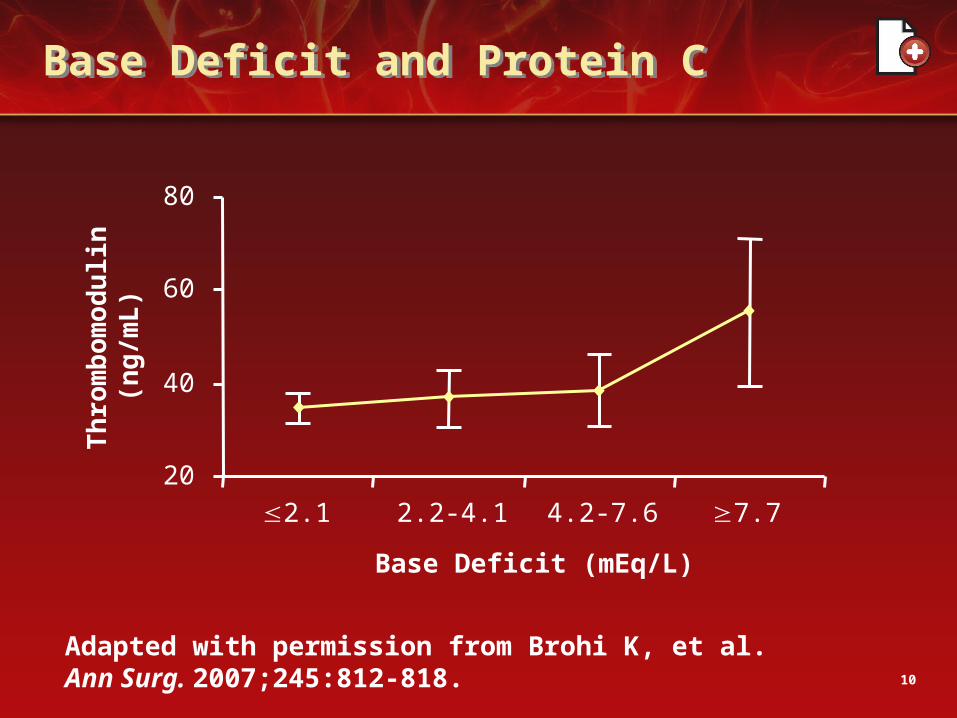
Base Deficit and Protein CBase Deficit and Protein C
10
Adapted with permission from Brohi K, et al. Ann Surg. 2007;245:812-818.
20
40
60
80
2.2-4.1 4.2-7.6
Base Deficit (mEq/L)
Th
rom
bo
mo
du
lin(n
g/m
L)

Base Deficit and Protein CBase Deficit and Protein C
11Brohi K, et al. Ann Surg. 2007;245:812-818.
● Activated protein C is potent anticoagulant Activates fibrinolysis
• In shock state, protein C activation→coagulopathy
• Decrease in protein C concentration associated with marked increase in mortality
12
Protein C Pathway
● Thrombomodulin increased
● Binds protein C
● Produces activated protein C
● Inhibits factors V, VIII
● Accelerates fibrinolysis

Rate of Heat TransferRate of Heat Transfer
Gentilello LM. In: Maull KI, et al, eds. Advances in Trauma and Critical Care. Vol 9. St Louis, MO: Mosby; 1994:39-79.
Q=mc(T2 - T1)
Rewarming TechniqueHeat Transfer (kcal/hr)
Airway rewarming 8-12
Overhead radiant warmer 17
Heating blankets 20
Convective warmers 15-26
Body cavity lavage 36
Continuous arteriovenous rewarming 92-139
Cardiopulmonary bypass 710
13

Effect of Hypothermia and DilutionEffect of Hypothermia and Dilution
Gubler KD, et al. J Trauma. 1994;36:847-851.14
Dilution
No Dilution
PT
(se
c)
Temperature (°C)
13
15
17
19
21
23
25
27
28 30 32 34 36 38
Martini WZ, et al. J Trauma. 2005;58:1002-1010.
Changes of Plasma Fibrinogen Concentration and Platelet Count
15
• Porcine trauma model
• HCI-induced hypothermia and acidosis pH, 7.1 Temperature, 32°C
• Results: Increased hypothermia and acidosis significantly decreased fibrinogen concentration and PLT counts

Thrombin GenerationThrombin Generation
Posted with permission from Martini WZ, et al. J Trauma. 2005;58:1002–1010.
Control
Hypothermic
Acidotic
Combined
*P.05, different from normal value at the same quench time point.
16
0
1500
3000
4500
6000
7500
9000
0 1 2 3 4 5 6 7Quench Time (min)
[TAT
] (µg
/L)
*
*
* **
*
*
**
*
*
*
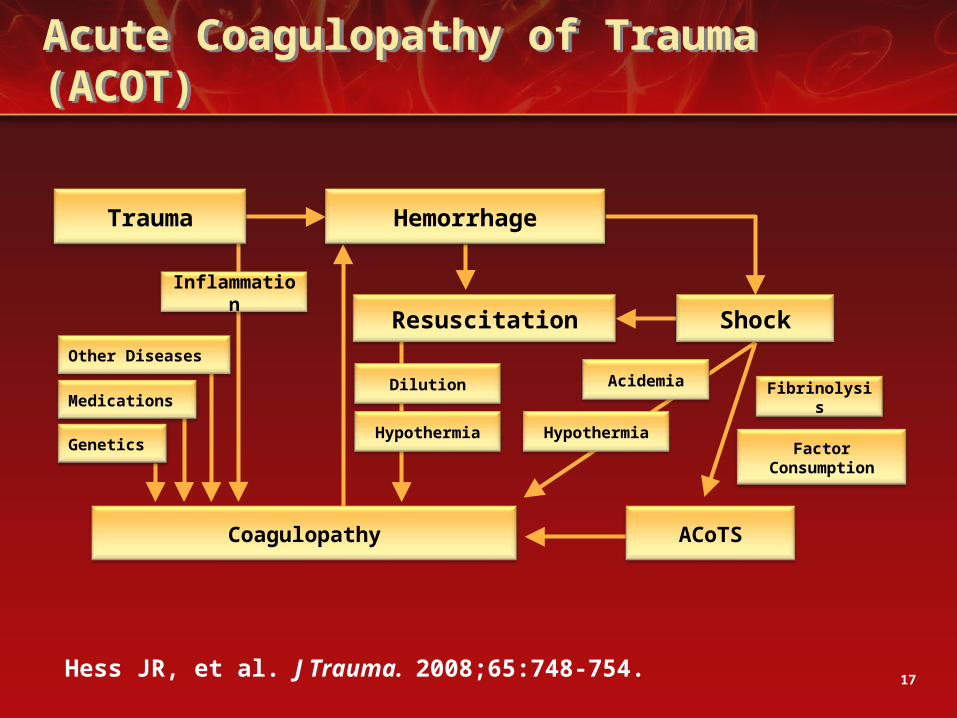
Acute Coagulopathy of Trauma (ACOT)Acute Coagulopathy of Trauma (ACOT)
Hess JR, et al. J Trauma. 2008;65:748-754. 17
Trauma Hemorrhage
ShockResuscitation
Coagulopathy ACoTS
FactorConsumption
FibrinolysisAcidemia
HypothermiaHypothermia
Dilution
Inflammation
Other Diseases
Medications
Genetics
ConclusionsConclusions
• Coagulopathy following trauma is complex
• Severely injured are coagulopathic immediately following injury
• Most of what we do makes it worse
• Early treatment should focus on stopping bleeding and correcting coagulopathy
18
19
Bryan A. Cotton, MD, MPH
Associate Professor of Surgery
The University of Texas
Health Science Center and
Center for Translational Injury Research
Houston, Texas
Has the way in which you manage the coagulopathy of trauma changed considerably over the course of your career as a surgeon?
20

Historically
• Treatment delayed
• Resuscitation emphasized
Currently
• Arrest bleeding
• Correct coagulopathy early
• Downplay resuscitation
• Adequate organ perfusion
• Limit fluids
21
22
Richard P. Dutton, MD, MBA
Professor of Anesthesiology
University of Maryland School of Medicine
Attending Anesthesiologist
R Adams Cowley Shock Trauma Center
Baltimore, Maryland
In the upcoming year, what types of research can we expect to see disseminated in the medical literature concerning resuscitation methods and strategies for managing the coagulopathy of trauma, and what will be the focus of those papers?
23
• Papers on role of recombinant factor VIIa in trauma
Results from prospective, randomized trial expected ≈600 patients enrolled
Third or fourth largest trauma study ever conducted
• Papers on plasma:red cell ratio
Match therapy to patient
Base ratio on needs of particular patient
Prospective and randomized trials24

Thank you for participating in this CE activity.
To receive credit for this activity, please complete the posttest and evaluation by clicking the “posttest” tab located above and following the instructions.
To download the reference list or supplemental slides for this program, please click the appropriate link on the home page of this activity.
www.bloodcmecenter.org
25