interpretation of cognitive tests - home - british … iq, reading/writing/age left school. •...
TRANSCRIPT

Interpretation of Cognitive Tests Workshop for BGS Trainees Conference 6th February 2016 Dr Vicki Osman-Hicks, Consultant in Old Age Psychiatry [email protected]
BGS Traine
es w
eeke
nd 20
16

Plan for Workshop • Checking level of experience/confidence • Principles for interpretation of tests • Refresher on different cognitive functions • Different cognitive tests and when to use each one. • Cognitive Tests in context of a community/OPD assessment for
suspected dementia • Cognitive Tests in different conditions • Round up and questions
BGS Traine
es w
eeke
nd 20
16

Checking level of experience High level of experience
Highly confident
BGS Traine
es w
eeke
nd 20
16
Shared Tips vs What’s hard?
BGS Traine
es w
eeke
nd 20
16

Principles for Interpreting Cognitive Tests • Caution with screening tests
• Why Assess now- it is timely and appropriate?
• Assessment: Cognitive test only as part of full ‘memory clinic style’ assessment (history +mental state + collateral history+ risk assessment + bloods+ physical examination +neuroimaging*). • On it’s own means nothing. Patient not the score.
• Assessment for What- Dementia vs MCI? Alz vs. FTD? • Link the history taking with the appropriate cognitive tests
• Pre-morbid abilities: 1st Language, IQ, Reading/Writing/Age Left
School.
• Disabilities: Sight/Hearing/ Tremor/Weakness
BGS Traine
es w
eeke
nd 20
16
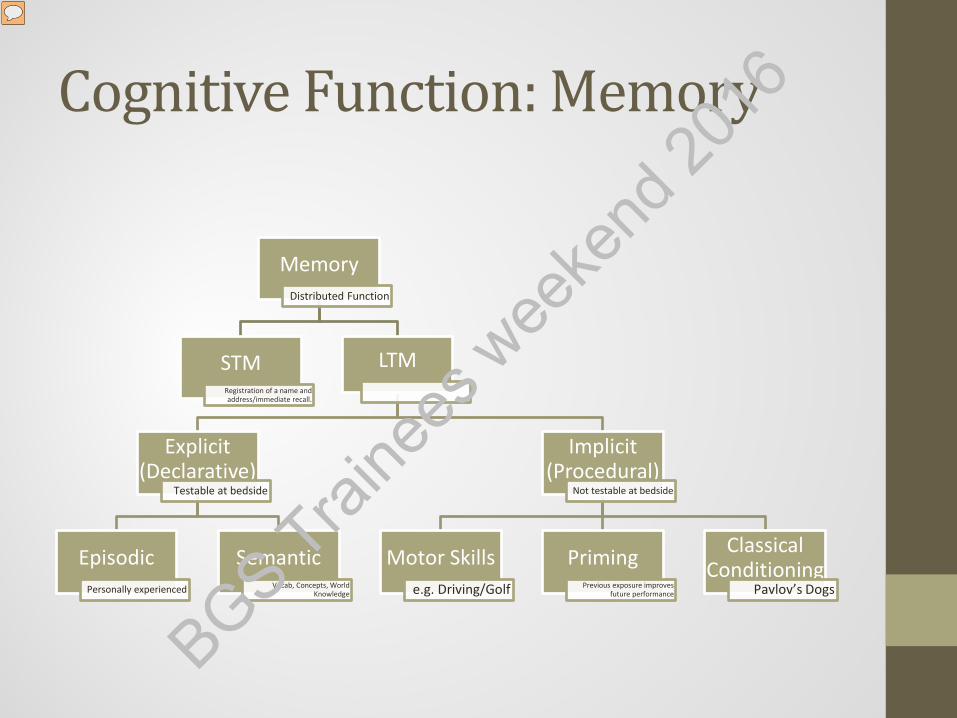
Cognitive Function: Memory
Memory Distributed Function
STM Registration of a name and address/immediate recall.
LTM
Explicit (Declarative)
Testable at bedside
Episodic Personally experienced
Semantic Vocab, Concepts, World
Knowledge
Implicit (Procedural)
Not testable at bedside
Motor Skills e.g. Driving/Golf
Priming Previous exposure improves
future performance
Classical Conditioning
Pavlov’s Dogs
BGS Traine
es w
eeke
nd 20
16

Cognitive Function: Attention and Executive Function
Responsivity Or Alertness
Sustained Attention
Divided Attention (more
than 1 task at once)
Selective Attention (focus on 1, suppress
another stimuli) Personality, Social Behaviour, Affect, Theory
of Mind, Motivation
Problem Solving, Sequencing and
Planning
Abstract Thinking
Set Shifting
Initiation and
Decision Making
Inhibitory Control
BGS Traine
es w
eeke
nd 20
16

Different Cognitive Tests MMSE ACE-III MOCA 6-CIT
Screening/ Staging for Dementia
Assessment for MCI and Dementia
Assessment for MCI not dementia
Screening for Dementia in Primary Care
Cut off 24/30 87% Sensitive 82% Specific Sensitivity depends on care setting. Cut off 27/30 in highly educated.
Cut Off 88/100 100% Sensitive 96% Specific 82/100 93% Sensitive 100% Specific for Dementia
Cut off 26/30 94% Sensitive 80% Specific
8+/28 Abnormal 79% Sensitive 100% Specific Culturally unbiased.
Takes 5-10 mins Takes 16 mins Takes 10 mins Takes <5 mins
Validated in: GP and Secondary Care
Validated in memory clinic, psych & neuro.
Validated in memory clinics,
Validated in Memory Clinics
Copyrighted ACE 3 Online 6CIT Online BGS Trai
nees
wee
kend
2016
Exercise: Cognitive Tests • You will be given a number of cognitive tests. In pairs: 1. Name the cognitive deficits on the test and rate the severity, if indeed it is dementia. 2. Link the one depression scale with the most likely MMSE. 3. Link the one ‘back of an MMSE’ with the most likely MMSE. 4. Think about the differential diagnosis for each one. 5. Finally describe the most likely history/mental state for your preferred diagnosis for each cognitive test?
BGS Traine
es w
eeke
nd 20
16
Exercise: Your Service • Design a flow chart of how you would manage a good quality
assessment of dementia including interpretation of cognitive tests in your clinic/service/future consultant job/ward?
BGS Traine
es w
eeke
nd 20
16

Round Up & Key Learning Points • Caution with screening tests
• Why Assess now- it is timely and appropriate?
• Assessment: Cognitive test only as part of full ‘memory clinic style’ assessment (history +mental state + collateral history+ risk assessment + bloods+ physical examination +neuroimaging*). • On it’s own means nothing. Patient not the score.
• Assessment for What- Dementia vs MCI? Alz vs. FTD? • Link the history taking with the appropriate cognitive tests
• Think about how you design your service to interpret them
well. BGS Traine
es w
eeke
nd 20
16

Further Reading • MOCA (how to do) You Tube MOCA • Stroop Test You Tube Stroop • ACE 3 Training (Free) ACE Training Online • Review of Brief
Cognitive Tests Velayudham L et al 2014
BGS Traine
es w
eeke
nd 20
16