international research journal of … research journal of pharmacy ... hypertension incompliance...
TRANSCRIPT

Biradar S S et al. IRJP 2012, 3 (1)
Page 206
INTERNATIONAL RESEARCH JOURNAL OF PHARMACY www.irjponline.com ISSN 2230 – 8407
Research Article
ASSESMENT OF PHARMACIST MEDIATED PATIENT COUENSILLING ON HYPERTENSION INCOMPLIANCE WITH QUALITY OF LIFE IN SOUTH INDIAN CITY
Biradar S S*1, Kapatae Rajashekhar2, Reddy Srinivas4, Raju S A3 1Research Scholar Pharmacy Practice JJT University Jhunjhunu, India
2Professor and Head of the Department of Community Medicine M R Medical College Gulbarga (Karnataka), India 3Principal HKES College of Pharmacy Gulbarga (Karnataka), India
4Biostatician Department of Community Medicine M R Medical College Gulbarga (Karnataka), India
Article Received on: 15/11/11 Revised on: 29/12/11 Approved for publication: 08/01/12 *Email:[email protected] ABSTRACT To evaluate the effect of counseling in hypertensive patients in terms of their quality of life. A prospective interventional study was conducted in hypertensive patients. Suitably designed and validated Quality of life questionnaire (QOL) of hypertension was used to measure the Quality of life of hypertensive patents. Patients were then counseled at their two follow ups during their two months intervention period. After the completion of intervention score of patients were measured using the same Qol questionnaire. A total of 123 patients were enrolled and randomized into test and control groups, The effectiveness of counseling on test group and control group patients was evaluated by comparing the qol values before and after counseling by applying paired sampled T- test. Pharmacist provided counseling is effective in improving qol of patients towards the Hypertension management. Key words: quality of life, hypertension, stroke, compliance INTRODUCTION Hypertension (HTN) is one of the most common health problems in developed and underdeveloped countries1, 2 Hypertension is an important public health challenge because of the associated morbidity and mortality caused by cardiovascular diseases and the cost to society. Hypertension affects nearly 26 per cent of the adult population worldwide. By 2025 it is projected that 29% of the world’s population (over 1.56 billion adults) will have Hypertension3 In 2000, over 972 million adult populations were estimated to have hypertension and this number is expected to rise to 1.56 billion by the year 2025. Indian population accounts for 66 million hypertensive patients and among these 25% adults are from urban area and 10% from rural area.4. Unfortunately, majority of the patients on antihypertensive medication fail to achieve their recommended target BP and it can lead to a huge adverse impact on quality of life.5 Improved possibilities to treat chronic diseases have increased the interest in measuring quality of life (QOL). Since treatment of chronic diseases is often not curative, but aims to improve function, limit disease progression and ameliorate suffering, any negative influence of the treatment on QOL must be limited as far as possible. Pharmacists, being active members of the healthcare team can use these instruments in their practices to provide better patient care. The aim of measuring quality of life is to provide information about well being of population and it has been a fundamental research topic in health, as its results are important to assess the effectiveness of health care. Quality of-life assessment measures changes in physical, functional, mental, and social health in order to evaluate the human and financial costs and benefits of new programs and interventions6 Quality of life assessment is complicated by the fact that there is no universally accepted definition for QOL. The researchers of this study have adopted the WHO definition of QOL which identifies QOL as a multidimensional concept. It is defined as "individuals' perceptions of their position in life in the
context of the culture and value system in which they live and in relation to their goals, standards, and concerns7. Major medical consequences of stroke concern different physical and psychological aspects such as loss of sense, palsy, disturbance of body image, depression and change in patient's role also affecting HRQL. Despite of side effects of medication (e.g. antidepressant, anti-cholinergic, and anti-adrenergic agents) potentially leading to decreased well-being 8, In a recent population based study, hypertensive individuals were found to have lower health status compared with individuals free from hypertension. Co morbidity with other diseases associated with hypertension may influence how persons with hypertension rate their QOL9 The benefits for hypertensive patients who are adequately treated, antihypertensive medication may produce adverse effects which affect the pleasure of living 10. Poor medication adherence and lack of knowledge and awareness on hypertension are the major reasons for poor BP control which is largely related to deterioration in a patient's quality of life9 The treatment of hypertension is usually long term, and its success will depend on the effects of the drug regimen on the patient's quality of life11
Researchers have attempted to standardize the construct of quality of life to have broad applications in health care policy and management; however, clinical research in hypertension should focus on the components of health-related quality of life that influence patient outcomes with regard to behaviours affecting adherence. Antihypertensive agents that maximize patient acceptance and quality of life are now available. 12 An important aspect in the treatment of hypertension that must be considered is that treatment should not interfere with patient's quality of life13 In this study we measured quality of life, in hypertension patients at government general hospital Gulbarga Karnataka in south Indian city.

Biradar S S et al. IRJP 2012, 3 (1)
Page 207
MATERIALS AND METHODS It is a prospective study to determine quality of life in hypertension patients attending outpatient medical department at Government General Hospital, Gulbarga of Karnataka. The survey was done by using structured questionnaires given in below. 1. How would you rate your quality of life? (RATEQL) 2. How much do you enjoy life? (ENJOY) 3. Do you have enough energy for everyday life? (ENERGY) 4. How satisfied are you with your sleep? (SLEEP) 5. How satisfied are you with your access to health services? (HEALTH) The Study group included 123 cases of essential hypertension attending Outpatient department (OPD) who could be followed up as required. They were divided in to two groups as test group and control group. The test group patients received patient counseling regarding lifestyle modifications, diet and other monitoring parameters including the patient information leaflets and control group received only patient information leaflets for their future reference and reading in local language. The follow-up of patients were done from baseline to follow-up -1 follow-up -2 for treatments. The patients were reminded by telephonically for their visits to hospitals. All patients received information regarding the objectives of the study and gave their written informed consent. The data were collected from patients by useable medical records that met our sample frame ted and matched with the questionnaire data. The data was collected from October 2010 to July-2011. Inclusion Criteria: All Patients diagnosed with hypertension of either sex, aged 18 – 70 years and willingness to participate. Exclusion Criteria: Patients with portal hypertension, pre-eclampsia and patients diagnosed with other co‐morbid diseases such as diabetes mellitus, dyslipidemia, heart failure, hepatic dysfunction, psychiatric disorder and cancer. To identify the relationship of Quality of life level on hospital admission, an independent Sample T‐test is used to determine whether there is a significant difference between the average values of the quality of life for hospital admission. RESULTS AND DISCUSSION The total 123 patients were participated in study the patient’s demography were shown in table-1and table-2.The final response rate from 123 patients we tested scores on several dimensions on the Quality of Life Questionnaire against baseline scores using Student’s T test and the results were shown in table-3.Quality of Life With regards to Quality of Life, we tested scores on several dimensions on the Quality of life Questionnaire against Test group scores using Student’s T test. The results were all significant at the .000%
level. The results of the T-test show that the rating for quality of life varied significantly (T was more than twice the standard error and statistically significant at .000 level) for the following aspects of the Quality of Life questionnaire In the study conducted by Vivian EM to assess the treatment outcomes in hypertensive patients showed the improvement in the health related quality of life in the patients with pharmacist Provided education24. CONCLUSION It can be safely assumed that in all dimensions of the Quality of Life questionnaire the baseline results vary significantly from the after counseling results, showing that pharmacist mediated patient counseling had a significant impact on Quality of Life. The study concluded that improving the patients’ quality of life about hypertension can improve the medication adherence behavior, which in turn improves the therapeutic outcomes. ACKNOWLEDGMENTS We express our gratitude to District Surgeon, medical staff outpatient department of Government General Hospital Gulbarga and Patients who helped us to complete this study. REFERENCES 1 Grove C, Laennec NJ. Disorders of the cardiovascular system, New York: McGraw-Hill, Medical Pub; 2005, p. 230. 2 Gascon JJ, Sanchez-Ortuno M, Llor B, Skidmore D, Saturno PJ. Why hypertensive patients do not comply with the treatment: results from a qualitative study. Fam Pract 2004; 21(2): 125-30. 3 Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005; 365: 217-223. 4 Thankappan KA, Sivasankaran S, Khader SA et al., Ind Heart Journal 2005; 57(1): 1-10. 5 Palaian S, Prabhu M, Shankar PR. Patient Counseling By Pharmacist -A Focus on Chronic Illness. Pak. J. Pharm. Sci. 2006; 19(1): 62-65. 6 Testa MA, Simonson DC. Assessment of quality-of life outcomes.N Engl J Med. 1996; 334: 835–840. 7 Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group Psychol Med. 1998; 28 (3): 551-8. 8 Ozer M, Materson R, Caplan L: Management of persons with stroke. Mosby, USA; 1994:41-53. 9 Ogunlana MO, Adedokun B, Dairo MD, Odunaiya NA. Profile and predictor of health-related quality of life among hypertensive patients in south-western Nigeria. BMC Cardiovascular Disorder. 2009; 9:25. 10 Cavalcante MA, Bombig MTN, Filho BL, Carvalho ACC, Paola AAV, Povao R et al. Quality of Life of Hypertensive Patients Treated at an Outpatient Clinic. Arq Bras Cardiol. 2007; 89(4):245-50. 11 Nunes, M.I.,The relationship between quality of life and adherence to treatment.Curr Hypertens Rep, Vol. 3, No. 6, p: 462-465. (2001). 12 Testa, M.A., Methods and applications of quality-of-life measurement during ntihypertensive therapy. Curr Hypertens Rep, Vol. 2, No. 6, p: 530-537. (2000). 13 Fletcher A. Quality of life in the management of hypertension. Clin and Exper Hypertension. 1999; 21:961-72. 14 Coyne KS, Davis D, French F, Hill MN. Health related quality of Life in patients treated for Hypertension. A review of the literature from 1999 to 2000. Clin Ther. 2002;24(1):142‐69 .
Table -1 Gender Frequency Percent Valid Percent Cumulative Percent
Valid female 55 44.7 49.1 49.1 male 57 46.3 50.9 100.0 Total 112 91.1 100.0
Missing System* 11 8.9 Total 123 100.0
*Missing system for drop outs during the study (because of unknown reasons) Roughly equal numbers of men and women participated in the study with about
50% of each sex represented.

Biradar S S et al. IRJP 2012, 3 (1)
Page 208
55
57
54
56
58
Female Male
Gender wise distribution of study population
Table 3: Distribution of study population according to education status
Frequency Percent Valid Percent Cumulative Percent Valid 13 10.6 10.6 10.6
Illiterate 30 24.4 24.4 35.0 Under Graduate 74 60.2 60.2 95.2
Graduate 3 2.4 2.4 97.6 Post Graduate 3 2.4 2.4 100.0
Total 123 100.0 100.0
Table-3 Paired Samples Test Paired Differences
t-Value df Sig. (2-tailed)
95% Confidence Interval of the Difference
Mean
Std. Deviation
Std. Error Mean Lower Upper
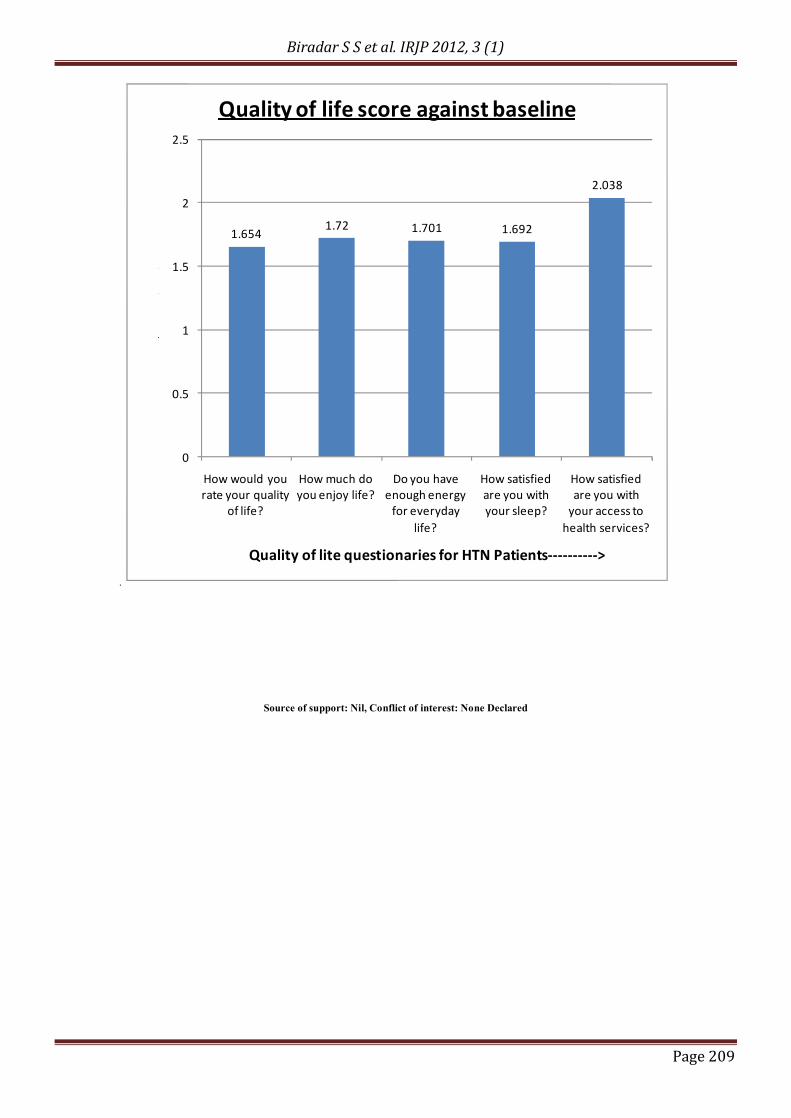
Pair 1 brategl - Rateql -1.654 1.117 .108 -1.868 -1.440 -15.322 106 .000 Pair 2 benjoy - enjoy -1.720 .989 .096 -1.909 -1.530 -17.994 106 .000 Pair 3 benergy - Energy -1.701 .983 .095 -1.889 -1.513 -17.899 106 .000 Pair 4 bsleep - sleep -1.692 .905 .087 -1.865 -1.518 -19.334 106 .000 Pair 5 bhealth - health -2.038 .872 .085 -2.206 -1.870 -24.058 105 .000
Biradar S S et al. IRJP 2012, 3 (1)
Page 209
.
1.6541.72 1.701 1.692
2.038
0
0.5
1
1.5
2
2.5
How would you rate your quality
of life?
How much do you enjoy life?
Do you have enough energy
for everyday life?
How satisfied are you with your sleep?
How satisfied are you with
your access to health services?
Scores
-----
>
Quality of lite questionaries for HTN Patients---------->
Quality of life score against baseline
Source of support: Nil, Conflict of interest: None Declared