interleukin-1, immune activation pathways, and different
TRANSCRIPT

Annals of the Rheumatic Diseases 1991; 50: 395-400
REVIEW
Interleukin- 1, immune activation pathways, anddifferent mechanisms in osteoarthritis andrheumatoid arthritis
Bruce Kirkham
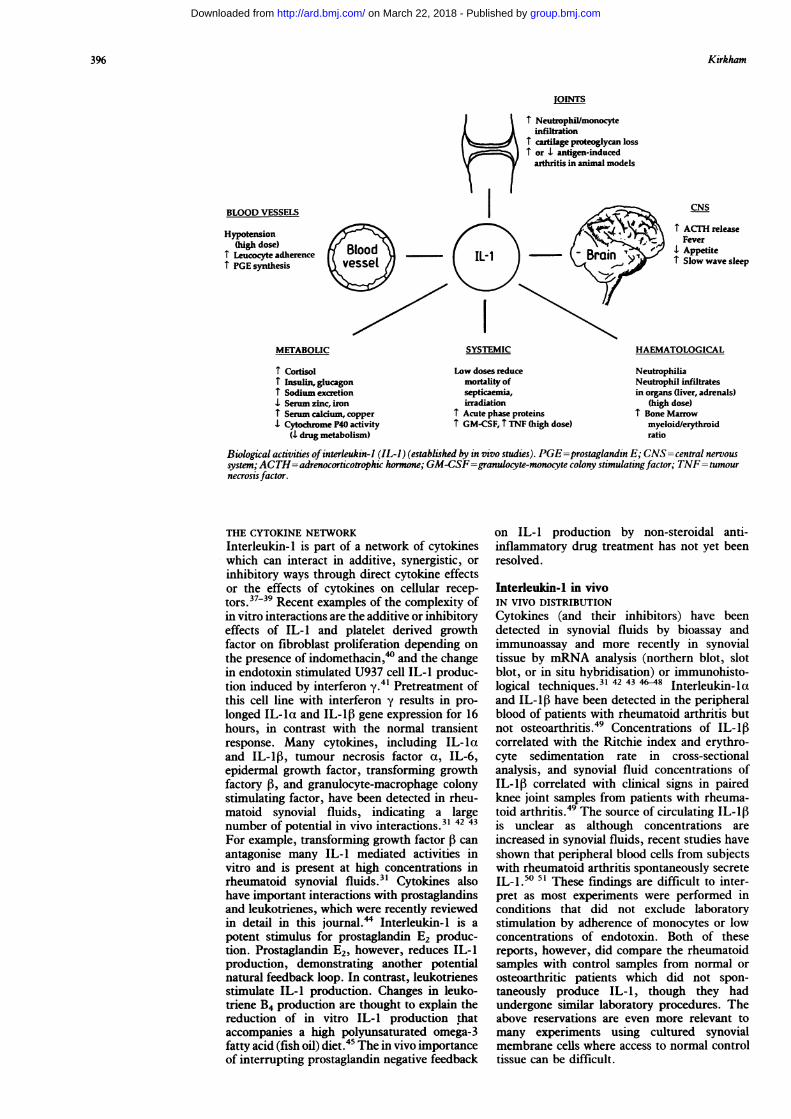
The properties of interleukin-l suggest that ithas a central role in the immunopathology ofmany arthritides (figure). It is now more than10 years since it was realised that numerousbiological activities were due to a single agentcalled interleukin-I (IL-I)' (now known to betwo related proteins, IL-la and IL-l132). Thefunctions of IL-1, such as T cell activation,3stimulation of cellular production of prosta-glandin E2 and I2,4 interleukin-1,5 and inter-leukin-6,6 help for B cell growth,7 induction ofendothelial cell adhesion molecule expression,8stimulation of chondrocyte stromelysin,9 syno-vial cell collagenase, and plasminogen activatorproduction,'0-'2 induction of bone resorption,'3and hepatic acute phase protein synthesis, showits enormous potential for mediating patho-logical processes. The 10th birthday of this 'firstinterleukin' was recently celebrated in a com-prehensive review of our current knowledge bydi Giovine and Duff. 14 In addition to extendingthe role of IL-I as an activator of immunefunction, recent data have provided a morecomplete picture of a physiological system, withnegative feedback pathways and inhibitors ofIL-I activity. This review of IL-I covers recentin vitro findings together with data from in vivostudies and discusses the implications forrheumatoid arthritis and osteoarthritis.
The Walter and ElizaHail Institute of MedicalResearch, Post Office,Royal MelbourneHospital, Victoria 3050,AustraliaB Kirkham
Interleukin-1: a complex biological systemCONTROL OF PRODUCTIONInterleukin-la and IL-1iB protein production iscontrolled at several levels, including genetranscription, messenger RNA (mRNA) sta-bility, translation to form the 31 kd precursorprotein, and release of the processed mature17-5 kd protein.'5 The complexity of IL-1production is illustrated by the high concentra-tions of IL-1 mRNA that can be stimulated byadherence of monocytes to glass. 6 This mRNAis not translated into protein, however, unless asecond signal (usually endotoxin) is supplied.Human monocytes are very sensitive to endo-toxin and can produce IL-I in response to thelow concentrations commonly found in tissueculture media. 6 Both endotoxin and IL-Istimulate transcription and translation of IL-i.5Glucocorticoids can reduce IL-I transcriptionand translation,17 18 in contrast with prosta-glandins, which reduce translation withoutchanging gene transcription.'9
Unlike most secreted proteins, IL-1 lacks a
distinct cleavage site for the N-terminus, result-ing in much IL-1 remaining cell associated.20Interleukin-li3 is secreted more efficiently thanIL-la and makes up most extracellular IL-1 (incell supernatants and body fluids).2' Inter-leukin-la is found associated with cells and mayform a 'membrane bound' biologically activeIL-1.22 This finding is still in contention,however.23 Despite having only 26% homology,IL-la and IL-1, bind to the same receptors andseem to have similar activity.'5 24 Interleukin-1, is vulnerable to oxidation, in contrast withIL-la, which is a stable molecule.25
INTERLEUKIN-1 INHIBITORSInhibitors of the biological activities of IL-1were noted when it was first detected in bodyfluids, including synovial fluid.2-28 The recentcharacterisation of the 22 kd inhibitor is a majoradvance in IL-1 biology.29 30 This inhibitor isrelated to the interleukin-I family with 26%sequence homology to IL-1iB and 19% homologyto IL-la and competes for the IL-1 receptor.The natural inhibitor has shown functionalinhibition of IL-I induced neutrophil adherenceto endothelial cells and cartilage degradation,3'and the recombinant protein inhibits IL-1stimulated prostaglandin synthesis in vitro.30 Itis produced by monocyte lineage cells withdifferent kinetics and in response to differingstimuli than IL-1. Apparently, immaturemonocytes predominantly secrete IL-1, incontrast with mature macrophage-like cells,which produce the inhibitor.32 It is unclear ifthe same cell can produce both.
Natural inhibitors of cytokines makemeasurement of in vivo cytokine concentrationsdifficult, and this difficulty is increased by thepresence of binding factors in plasma, includinga2 macroglobulin.33 Additionally, specific cyto-kine binding immunoglobulin autoantibodieshave been shown for IL-Ia and tumour necrosisfactor a.3' These antibodies may function asphysiological carriers for cytokines as theirbinding affinity for IL-1 is less than the highaffinity receptor found on T lymphocytes butgreater than the affinity of receptors found oncells such as endothelial cells. Recent findingssuggest that these two forms of the IL-1receptor with low and high affinities for IL-1are expressed on different cell types.35 Highaffinity IL-1 receptors have been identified onsynovial cells from normal subjects and thosewith osteoarthritis and rheumatoid arthritis.36
395
group.bmj.com on March 22, 2018 - Published by http://ard.bmj.com/Downloaded from
Kirkham
BLOOD VESSELS
Hypotension(high dose)
I Leucocyte adherenceI PGE synthesis
METABOLIC
I CortisolI Insulin, glucagonT Sodium excretionI Serum zinc, ironI Senum calcium, copperI Cytochrome P40 activity
(I drug metabolism)
I Neutrophil/monocyteinfiltration
T cartilage proteoglycamT or I antigen-induced
arthritis in animal mo
|IL-t - t Brain
SYSTEMIC
Low doses reducemortality ofsepticaemia,irradiation
I Acute phase proteinsI GM-CSF, I TNF (high dose)
n lossd)dels
CNS
T ACTH releaseFever
I AppetiteT Slow wave sleep
HAEMATOLOGICAL
NeutrophiliaNeutrophil infiltratesin organs (liver, adrenals)
(high dose)1 Bone Marrow
myeloid/erythroidratio
Biological activities ofinterleukin-l (IL-I) (established by in vivo studies). PGE=prostaglandin E; CNS=central nervoussystem; ACTH=adrenocorticotrophic hormone; GM-CSF=granulocyte-monocyte colony stimulating factor; TNF=tumournecrosis factor.
THE CYTOKINE NETWORKInterleukin- is part of a network of cytokineswhich can interact in additive, synergistic, or
inhibitory ways through direct cytokine effectsor the effects of cytokines on cellular recep-tors.3739 Recent examples of the complexity ofin vitro interactions are the additive or inhibitoryeffects of IL-I and platelet derived growthfactor on fibroblast proliferation depending on
the presence of indomethacin,46 and the changein endotoxin stimulated U937 cell IL-I produc-tion induced by interferon y.41 Pretreatment ofthis cell line with interferon y results in pro-longed IL-la and IL-1lB gene expression for 16hours, in contrast with the normal transientresponse. Many cytokines, including IL-laand IL-1,B, tumour necrosis factor a, IL-6,epidermal growth factor, transforming growthfactory ,B, and granulocyte-macrophage colonystimulating factor, have been detected in rheu-matoid synovial fluids, indicating a largenumber of potential in vivo interactions.314243For example, transforming growth factor ,B canantagonise many IL-1 mediated activities invitro and is present at high concentrations inrheumatoid synovial fluids.3' Cytokines alsohave important interactions with prostaglandinsand leukotrienes, which were recently reviewedin detail in this journal." Interleukin-l is a
potent stimulus for prostaglandin E2 produc-tion. Prostaglandin E2, however, reduces IL-1production, demonstrating another potentialnatural feedback loop. In contrast, leukotrienesstimulate IL-1 production. Changes in leuko-triene B4 production are thought to explain thereduction of in vitro IL-1 production thataccompanies a high polyunsaturated omega-3fatty acid (fish oil) diet.45 The in vivo importanceof interrupting prostaglandin negative feedback
on IL-1 production by non-steroidal anti-inflammatory drug treatment has not yet beenresolved.
Interleukin-I in vivoIN VIVO DISTRIBUTIONCytokines (and their inhibitors) have beendetected in synovial fluids by bioassay andimmunoassay and more recently in synovialtissue by mRNA analysis (northern blot, slotblot, or in situ hybridisation) or immunohisto-logical techniques.3' 42 43 46 48 Interleukin-laand IL-1,6 have been detected in the peripheralblood of patients with rheumatoid arthritis butnot osteoarthritis.49 Concentrations of IL-1,Bcorrelated with the Ritchie index and erythro-cyte sedimentation rate in cross-sectionalanalysis, and synovial fluid concentrations ofIL-1,B correlated with clinical signs in pairedknee joint samples from patients with rheuma-toid arthritis.49 The source of circulating IL-1,8is unclear as although concentrations areincreased in synovial fluids, recent studies haveshown that peripheral blood cells from subjectswith rheumatoid arthritis spontaneously secreteIL-1.50 5' These findings are difficult to inter-pret as most experiments were performed inconditions that did not exclude laboratorystimulation by adherence of monocytes or lowconcentrations of endotoxin. Both of thesereports, however, did compare the rheumatoidsamples with control samples from normal orosteoarthritic patients which did not spon-taneously produce IL-1, though they hadundergone similar laboratory procedures. Theabove reservations are even more relevant tomany experiments using cultured synovialmembrane cells where access to normal controltissue can be difficult.
396
group.bmj.com on March 22, 2018 - Published by http://ard.bmj.com/Downloaded from

IL-], immune activation pathways, and different mechanisms in OA and RA
By in situ hybridisation analysis of rheuma-toid synovial membrane, Duff and colleaguesshowed tht CD14 positive macrophages containIL-lIU mRNA.49 We detected IL-113, byimmunohistological techniques, in cells scat-tered throughout perivascular aggregates and insome lining layer cells in rheumatoid synovialmembrane.52 These techniques will be increas-ingly applied to assess cytokine production indisease states and models of inflammation andto assess modes of drug action in vivo. Forexample, we showed a significant decrease inIL-1l6 staining after 12 weeks of sodium auro-thiomalate treatment in sequential synovialbiopsy specimens from six patients with rheu-matoid arthritis. This decrease occurred with-out significant changes in the synovial mono-nuclear cell composition.53 These methods willprovide a picture of the cytokine networkpresent in different disease states, and for IL-1at least, an assessment of the balance betweencytokine and inhibitor production may soon bepossible.
IN VIVO FUNCTIONMost of the activities ascribed to IL-l have beendetermined in vitro and must be regarded aspotential functions. The in vivo function ofcytokines can be assessed by the use of recom-binant cytokines and cytokine inhibitors, by theuse of specific anticytokine monoclonal anti-bodies, or by the use of transgenic animalmodels. Henderson and Pettipher showed thatintra-articular administration of IL-la or IL-,13in rabbits causes rapid loss of cartilage proteo-glycan and a rapid increase of neutrophils andmonocytes in the synovial compartment.54Interestingly, synovial fluid prostaglandin con-centrations did not rise and no clinical signs ofinflammation such as swelling or warmth wereseen. Tumour necrosis factor a had less potentbut similar effects and, together, IL-1, andtumour necrosis factor a showed synergisticeffects, confirming in vitro predictions.55Repeated intra-articular injections of IL-1 intothe ankles of normal rats produces a synovialcellular infiltrate and fibrosis in the absence ofcartilage or bone destruction.56 Interleukin-1given intra-articularly or systemically canexacerbate low grade antigen induced arthritisin animal models.56 57 The in vivo picture iscomplicated, however, as the exacerbation seenin collagen induced arthritis varied dependingon the relative timing of disease stimulus andcytokine.58 Jacobs et al reported that intra-articular IL-i1, actually decreased antigeninduced arthritis when given both before orduring the arthritis.59 The timing and dose ofcytokine in relation to a stimulus is crucial.Although high dose IL-1 given intravenouslycauses toxic effects, such as hypotension, fever,and neutrophilia,60 low dose IL-1 given beforenoxious stimuli, such as endotoxin, falciparummalaria, or radiation, can improve survival inanimal models.6' The mechanisms for theseeffects are not known but may involve inductionof cytokine inhibitors, reduction of cytokinereceptor expression, or stimulation of cortisolproduction, and may demonstrate some of the
physiological roles of IL-1. Many of theseprotective effects can be abrogated by pre-treatment with non-steroidal anti-inflammatorydrugs.
These models suggest that IL-1 activity invivo might contribute to cartilage damage andpromote inflammatory changes. This activity,however, will be suppressed by natural in-hibitors. Inhibition of interleukin-I activityincreases over time in antigen induced arthritisin rabbits.62 Two studies of patients withrheumatoid arthritis attempted to correlatesynovial fluid IL-I concentrations with measuresof local joint damage. Saxne and colleaguesshowed that synovial fluid concentrations ofIL-I do not correlate with synovial fluid proteo-glycan fragment concentrations." Miyasakaand colleagues, however, reported that concen-trations of IL-1 secreted by cell cultures fromsynovial biopsy specimens did correlate withradiographic damage.'M A single study reportedmodest short term improvements in patientswith rheumatoid arthritis treated with an IL-1inhibitor.65
Interleukin-1 in osteoarthritisINTERLEUKIN-1 PROPERTIES AND OSTEOARTHRITISAs outlined above, much attention has beenpaid to the role of IL-I in inflammatoryarthropathies such as rheumatoid arthritis.Interleukin- I has also been consistently detectedin synovial fluid samples from patients withosteoarthritis.26 42 6 The processes initiatingosteoarthritis are unknown and it is unclear ifthe end stage of cartilage failure is due mainly toproteoglycan, collagen, subchondral bone, orvascular defects.67 68 It is known that raisedlevels of degradative enzymes, such as col-lagenase and stromelysin, are present in osteo-arthritic cartilage as is plasminogen activator, animportant activator of these enzymes.69 70 Inter-leukin-l has many properties, such as stimu-lation of stromelysin, collagenase and plas-minogen activator secretion, and direct boneresorbing activities, that might account formany of these changes. Tumour necrosis factora produces similar changes and has also beenfound in some osteoarthritic synovial fluids.7' Itis generally found in a lower proportion ofosteoarthritic synovial fluids than is IL-1. Thissuggests that synergistic effects at very lowconcentrations may occur in some patients,contributing to the variable rates of diseaseprogression seen between patients. In additionto its catabolic effects, IL-I has anabolic effects,such as increasing fibroblast collagen synthesis,72which might account for other changes, such asosteophyte formation.
IN VIVO DISTRIBUTION IN OSTEOARTHRITISIt is now clear that infiltrates of mononuclearcells are commonly found in osteoarthriticsynovial membranes, even in patients with earlydisease.73 7" We and other groups investigatedthe distribution of IL-113 in the osteoarthriticsynovium, using immunohistological tech-niques. Pelletier et al reported IL-13 in osteo-arthritic synovial lining layer cells, with some
397
group.bmj.com on March 22, 2018 - Published by http://ard.bmj.com/Downloaded from

Kirkham
staining in the deeper tissues.75 Shinmei et aldemonstrated IL-16 staining in osteoarthriticchondrocytes.76 We detected IL-1lB stainingconsistently in synovial lining layer cells, withalmost no IL-lt being detected in the peri-vascular lymphoid aggregates that were com-monly present.52 This distribution of IL-1,Bstaining was different from that found inrheumatoid arthritis, where it was mainly in theperivascular aggregates. This suggests thatalthough IL-I is present in both the rheumatoidand osteoarthritic synovial compartment, it isstimulated by different processes. The presenceof IL-1 staining in the perivascular cellularinfiltrates in rheumatoid arthritis suggests thatthese infiltrates may be the site of an active cellmediated immune process which interacts withother components of the systemic immunesystem. This is supported by the systemicnature of rheumatoid arthritis, with circulatingIL-149 and IL-1 producing cells,505' raisederythrocyte sedimentation rate, and solubleinterleukin-2 receptor concentrations.77 In con-trast, the localised lining cell activation inosteoarthritis would produce localised increasesof IL-I in the synovial fluid in the absence ofsystemic immune activation. Many cells in theosteoarthritic synovial membrane infiltrate maybe inactive bystander cells, as suggested for therheumatoid synovial membrane by Ziff in1974.78 The suggestion of differing mechanismsof IL-l production in these diseases is sup-ported by the results of Brennan and col-leagues.79 They found that in vitro osteoarthriticsynovial cells produced low concentrations ofIL-l compared with the high concentrationsproduced by rheumatoid synovial cells. Bothgroups produced high concentrations of tumournecrosis factor a. When monoclonal antibodiesto tumour necrosis factor a were added to thesystem, however, IL-l production was reducedonly in the group with rheumatoid arthritis,with no change occurring in IL-l production byosteoarthritic synovial cells.
A POTENTIAL ROLE IN OSTEOARTHRITISThe detection of IL-l in osteoarthritic synovialmembranes has been in patients with establisheddisease, highlighting the difficulties of studyingearly disease in humans. It is therefore unclearif the lining cell layer production of IL-l is anearly or late development. Goto and colleaguesreported that monocytes can be stimulated toproduce IL-I by fragments of human cartilage,in particular by collagen type 11.80 For osteo-arthritis a possible mechanism relating cyto-kines to disease might be an initial insult tocartilage with release of cartilage fragmentswhich then stimulate synovial lining cell pro-duction of IL-1. The properties of IL-1 maythen contribute to the progress of the lesion. Inthis situation the balance of cytokine andinhibitor would play a crucial part.The importance of IL-I (and other cytokine)
secretion in the early stages of disease will bebest studied in animal models.8' Interleukin-Ihas been detected in the synovial fluid of equineosteoarthritis.82 Two facts suggest this is animportant point to resolve. Glucocorticoids
have been shown to prevent progression ofdisease in osteoarthritis models, in contrast withnon-steroidal anti-inflammatory drugs, whichhave no effect. Glucocorticoids have manyeffects, including reduction of collagenaseproduction, which may mediate this improve-ment. It must be remembered that anotherpowerful activity is the reduction of cytokineexpression. The second fact relates to reportsthat non-steroidal anti-inflammatory drugs,which reduce prostaglandin concentrations,may cause a more rapid deterioration of osteo-arthritis.83 The mechanisms by which thismight occur are unclear but, possibly, suppres-sion of the prostaglandin negative feedbackon IL-1 production may contribute to thisdeterioration
ConclusionThe increasing in vivo definition of cytokineactivities and distribution promises to providethe clinician with explanations of diseasepathology. Important lessons about the ease ofnon-physiological stimulation of cells (recentlyillustrated by the in vitro production of tumournecrosis factor a in patient samples84) mean thatclinical studies must be meticulously plannedand executed if meaningful data are to begained. With the availability of ultrasensitivetechniques using the polymerase chain reactionto detect very low concentrations of cytokinemRNA85 the complex control of production ofmany cytokines must be remembered, andcytokine production should preferably bereported at both the mRNA and peptide level.The recombinant materials, specific monoclonalantibodies, and techniques are now available toensure a continuation of the recent encouragingincrease of studies to define in vivo cytokinefunction.The findings for IL-l described in this review
give an indication of the potential availableinformation but have little meaning in isolation.A more complete picture of the cytokine net-work that operates in many diseases will emergewhen the range of cytokines is assessed at thesite of disease activity. It may become apparentthat there is a hierarchy of cytokines in differentdiseases which might be regulated by inhibitingthe actions of a limited number of cytokines. Atpresent the great overlap of cytokine activitiessuggests to many in this field that this will notbe the case. An interesting hypothesis wouldsuggest that so called 'non-inflammatory'diseases such as osteoarthritis, which may havea limited number of participating cytokines,may be more appropriate targets for theseimmunotherapies of the future.
I am grateful to Professor Gabriel Panayi, London, and Dr JohnHamilton, Melbourne, for their most helpful advice about themanuscript. Dr Kirkham is supported by the Peel MedicalResearch Trust and Arthritis and Rheumatism Council.
1 Mizel S B, Farrar J J. Revised nomenclature of antigen-nonspecific T-cell proliferation and helper factors. CellImmunol 1979; 48: 433-6.
2 Oppenheim J J, Kovacs E J, Matsushima K, Durum S K.There is more than one interleukin 1. Immunol Today 1986;7: 45-56.
3 Herrmann A F, Oster W, Meuer S C, Lindemann A,
398
group.bmj.com on March 22, 2018 - Published by http://ard.bmj.com/Downloaded from
IL-I, immune activation pathways, and different mechanisms in OA and RA
Mertelsmann R H. Interleukin 1 stimulates T lymphocytesto produce granulocyte-monocyte colony-stimulating factor.J Clin Invest 1988; 81: 1415-8.
4 Rossi V, Breviario F, Ghezzi P, Dejana E, Mantovani A.Prostaglandin synthesis induced in vascular cells by inter-leukin-1. Science 1985; 229: 174-6.
5 Dalton B J, Connor J R, Johnson W J. Interleukin-l inducesinterleukin-la and interleukin-li gene expression insynovial fibroblasts and peripheral blood monocytes.Arthritis Rhewn 1989; 32: 279-87.
6 Jirik F R, Podor T J, Hirano T, et al. Bacterial lipopolysac-charide and inflammatory mediators augment IL-6 secre-tion by human endothelial cells. J Immunol 1989; 142:144-7.
7 Giri J G, Kincade P W, Mizel S B. Interleukin-l mediatedinduction of kappa-light chain synthesis and surfaceimmunoglobulin expression on pre-B cells. J Inmnunol1984; 132: 223-8.
8 Mantovani A, Dejana E. Cytokines as communication signalsbetween leukocytes and endothelial cells. Immunol Today1989; 10: 370-5.
9 Hasty K A, Reife R A, Kang A H, Stuart J M. The role ofstromelysin in the cartilage destruction that accompaniesinflammatory arthritis. Arthritis Rhewn 1990; 33: 388-97.
10 Leizer T, Clarris B J, Ash P E, van Damme J, Saklatvala J,Hamilton J A. Interleukin- i and interleukin-la stimubtethe plasminogen activator activity and prostaglandin E2levels of human synovial cells. Arthritis Rhewn 1987; 30:562-6.
11 Dayer J-M, de Rochemonteix B, Burrus S, Demezuks S,Dinarello C. Human recombinant interleukin-I stimulatescollagenase and prostaglandin E2 production by synovialcells. J Clin Invest 1986; 77: 645-8.
12 Dodge G R, Poole A R. Immunohistochemical detection andimmunochemical analysis of type II collagen degradation inhuman nornal, rheumatoid and osteoarthritic articularcartilages and in explants of bovine articular cartilagecultured with interleukin 1. J Clin Invest 1989; 83: 647-61.
13 Rifas L, Shen F, Mitchell K, PeckWA. Macrophage-derivedgrowth factor for osteoblast-like cells and chondrocytes.Proc Natl Acad Sci USA 1984; 81: 4558-62.
14 di Giovine F S, DuffG W. Interleukin 1: the first interleukin.Immunol Today 1990; 11: 13-20.
15 Dinarello C A. Biology of interleukin 1. FASEB J 1988; 2:108-15.
16 Schindler R, Dinarello C A. A method for removinginterleukin-l and tumor necrosis factor-inducing substancesfrom bacterial cultures by ultrafiltration with polysulfone.J Immnol Methods 1989; 116: 159-65.
17 Knudsen P J, Dinarello C A, Strom T B. Glucocorticoidsinhibit transcriptional and post-transcriptional expressionof interleukin 1 in U937 cells. I Immunol 1987; 139:4129-34.
18 Kern J A, Lamb R J, Reed J C, Daniele R P, Nowell P C.Dexamethasone inhibition of interleukin 1 beta productionby human monocytes. Post-transcriptional mechanisms.
Clin Invest 1988; 81: 237-44.19 Knudsen P J, Dinarello CA, Strom TB. Prostaglandins post-
transcriptionally inhibit monocyte expression of interleukin1 activity by increasing intracellular cyclic adenosinemonophosphate. J Immunol 1986; 137: 3189-94.
20 Baldari C T, Telford J L. The intracellular precursor of IL-l1 is associated with microtubules in activated U937 cells.J Immunol 1989; 142: 785-91.
21 Libby P, Ordovas J M, Birinyi L K, Auger K R, DinarelloC A. Inducible interleukin-I gene expression in humanvascular smooth muscle cells. J Clin Invest 1986; 78:1432-8.
22 Kurt-Jones E A, Beller D I, Mizel S B, Unanue E R.Identification of a membrane-associated interleukin 1 inmacrophages. Proc NatlAcad Sci USA 1985; 82: 1204-10.
23 Suttles J, Carruth L M, Mizel S B. Detection of IL-la andIL-1i in the supernatants of paraformaldehyde-treatedhuman monocytes. Evidence against a membrane form ofIL-1.JImmwnol 1990; 144: 170-4.
24 Dinarello CA, Clark B D, Puren A J, Savage N, Rosoff PM.The interleukin 1 receptor. Imnunol Today 1989; 10:49-51.
25 Dinarello C A. Interleukin-1 and its biologically relatedcytokines. Adv Immunol 1989; 44: 153-205.
26 Nouri- A M E, Panayi G S, Goodman S M. Cytokines and thechronic inflammation of rheumatic disease. I. The presenceof interleukin- I in synovial fluids. Clin Exp Immunol 1984;55: 295-302.
27 Lotz M, Tsoukas C D, Robinson CA, Dinarello CA, CarsonD A, Vaughan J H. Basis for defective responses ofrheumatoid arthritis synovial fluid lymphocytes to anti-CD3 (T3) antibodies. J Clin Invest 1986; 78: 713-21.
28 Balavoine J-F, Rochemonteix B de, Williamson K, SeckingerP, Cruchard A, Dayer J-M. Prostaglandin E2 and col-lagenase production by fibroblasts and synovial cells isregulated by urine-derived human interleukin 1 andinhibitor(s). J Clin Invest 1986; 78: 1120-4.
29 Hannum C H, Wilcox C J, Arend W P, et al. Interleukin-lreceptor antagonist activity of a human interleukin-1inhibitor. Nature 1990; 343: 336-40.
30 Eisenberg S P, Evans R J, Arend W P, et al. Primarystructure and functional expression from complementaryDNA of a human interleukin- 1 receptor antagonist. Nature1990; 343: 341-6.
31 Arend W P, Joslin F G, Thompson R C, Hannum C H. AnIL-1 inhibitor from human monocytes. Production andcharacterisation of biologic properties. J Immunol 1989;143: 1851-8.
32 ArendW P, Dayer J-M. Cytokines and cytokine inhibitors orantagonists in rheumatoid arthritis. Arthritis Rheum 1990;33: 305-15.
33 James K. Interactions between cytokines and a2-macro-globulin. Immunol Today 1990; 11: 163-6.
34 Bendtzen K, Svenson M, Jonsson V, Hippe E. Autoantibodiesto cytokines-friends or foes? Immunol Today 1990; 11:167-9.
35 Sims J E, March C J, Cosman D, et al. cDNA expressioncloning of the IL-1 receptor, a member of the immuno-globulin superfamily. Science 1988; 241: 585-9.
36 Chin J, Rupp E, Cameron P M, et al. Identification of a high-affinity receptor for interleukin la and interleukin lp oncultured human rheumatoid synovial cells. J Clin Invest1988; 82: 420-6.
37 Balkwill F R, Burke F. The cytokine network. ImmunolToday 1989; 10: 299-304.
38 Guerne P-A, Carson D A, Lotz M. IL-6 production byhuman articular chondrocytes. Modulation of its synthesisby cytokines, growth factors, and hormones in vitro. JImnunol 1990; 144: 499-505.
39 Mielke V, Bauman J G J, Sticherling M, et al. Detection ofneutrophil-activating peptide NAP/IL-8 and NAP/IL8mRNA in human recombinant IL-la- and humanrecombinant tumor necrosis factor-a-stimulated humandermal fibroblasts. 7 Imnunol 1990; 144: 153-61.
40 Kumkumian G K, Lafyatis R, Remmers E F, Case J P, KimS-J, Wilder R L. Platelet-derived growth factor and IL-1interactions in rheumatoid arthritis. Regulation of synovio-cyte proliferation, prostaglandin production and collagenasetranscription. J Immunol 1989; 143: 833-7.
41 Ucla C, Roux-Lombard P, Fey S, Dayer J-M, Mach B.Interferon gamma drastically modifies the regulation ofinterleukin 1 genes by endotoxin in U937 cells. J7 ClinInvest 1990; 85: 185-91.
42 Hopkins S J, Humphreys M, Jayson M I V. Cytokines insynovial fluid. I. The presence of biologically active andimmunoreactive IL-1. Clin Exp Immunol 1988; 72: 422-7.
43 Shiozawa S, Shiozawa K, Tanaka Y, et al. Human epidermalgrowth factor for the stratification of synovial lining layerand neovascularisation in rheumatoid arthritis. Ann RheumDis 1989; 48: 820-8.
44 Hopkins S J. Cytokines and eicosanoids in rheumaticdiseases. Ann Rheun Dis 1990; 49: 207-11.
45 Endres S, Ghorbani R, Kelley V E, et al. The effect of dietarysupplementation with n-3 polyunsaturated fatty acids onthe synthesis of interieukin-l and tumor necrosis factor bymononuclear cells. N EngII Med 1989; 320: 265-71.
46 Buchan G, Barrett K, Turner M, Chantry D, Maini R N,Feldmann M. Interleukin-I and tumour necrosis factormRNA expression in rheumatoid arthritis: prolongedproduction of IL-la. Clin Exp Immunl 1988; 73: 449-55.
47 Firestein G, Xu W-D, Townsend K, et al. Cytokines inchronic inflammatory arthritis. I. Failure to detect T celllymphokines (interleukin 2 and interleukin 3) and presenceof macrophage stimulating factor (CSF-1) and a novel mastcell growth factor in rheumatoid synovitis. J Exp Med1988; 168: 1573-86.
48 Husby G, Williams R C. Synovial localisation of tumornecrosis factor in patients with rheumatoid arthritis. JAutoimmun 1988; 1: 363-71.
49 Duff G W. Peptide regulatory factors in non-malignantdisease. Lancet 1989; i: 1432-5.
50 Koch B, Baum W, Burmester G R, et al. Prostaglandin E2,interleukin 1 and gamma interferon production of mono-nuclear cells of patients with inflammatory and degenerativejoint diseases. Z Rheumatol 1989; 48: 194-9.
51 Goto M, Fujisawa M, Yamada A, et al. Spontaneous releaseof angiotensin converting enzyme and interleukin l1 fromperipheral blood monocytes from patients with rheumatoidarthritis under a serum free condition. Ann Rhewn Dis1990; 49: 172-6.
52 Kirkham B W, Navarro F J, CorkillM M, Barbatis C, PanayiG S. Immunohistochemical localization of interleukin 1 inrheumatoid and osteoarthritis synovial membrane[Abstract]. BrJ Rhewmatol 1989; 28 (suppl 2): 47.
53 Kirkham B W, Navarro F J, Corkill M M, Gibson T, PanayiG S. Change in interleukin 1 beta expression in rheumatoidsynovial membrane after treatment with gold and gluco-corticoid [Abstract]. Clin Rheumatol 1990; 9: 11-9.
54 Henderson B, Pettipher E R. Comparison of the in vivoinflammatory intra-articular injection of natural andrecombinant IL-1 alpha and IL-1 beta in the rabbit.Biochem Pharnacol 1988; 37: 4171-6.
55 Henderson B, Pettipher E R. Arthritogenic actions ofrecombinant IL-1 and tumour necrosis factor a in therabbit: evidence for synergistic interactions between cyto-kines in vivo. Clin Exp Immunol 1989; 75: 306-10.
56 Stimpson S A, Dalldorf F G, Otterness I G, Schwab J H.Exacerbation of arthritis by IL-1 in rat joints previouslyinjured by peptidoglycan-polysaccharide. J Immunol 1988;140: 2964-9.
57 Staite N D, Richard K A, Aspar D G, Franz K A, GalinetL A, Dunn C J. Induction of an acute erosive monarticulararthritis in mice by interleukin-I and methylated bovineserum albumin. Arthritis Rheum 1990; 33: 253-60.
58 Killar L M, Dunn C J. Interleukin-1 potentiates thedevelopment of collagen-induced arthritis in mice. Clin Sci1989; 76: 535-8.
59 Jacobs C, Young D, Tyler S, Callis G, Gillis S, Conlon P J. Invivo treatment with IL-I reduces the severity and durationof antigen-induced arthritis in rats. J Imnunol 1988; 141:26T7-74.
60 Okusawa 5, Gelfand J A, Ikejima T, Connolly R J, Dinarello
399
group.bmj.com on March 22, 2018 - Published by http://ard.bmj.com/Downloaded from

Kirkham
C A. Interleukin 1 induces a shock-like state in rabbits.Synergism with tumor necrosis factor and the effect ofcyclooxygenase inhibition.J Clin Invest 1988; 81: 1162-72.
61 Cominelli F, Nast C C, Lierena R, Dinarello C A, ZipserR D. Interleukin 1 suppresses inflammation in rabbitcolitis. Mediation by endogenous prostaglandins. ClinInvest 1990; 85: 582-6.
62 Henderson B, Rowe F M, Bird C R, Gearing A J H.Production of interleukin 1 in the joint during thedevelopment of antigen-induced arthritis in the rabbit. ClinExp Immunol 1988; 74: 371-6.
63 Saxne T, Di Giovine F S, Heinegard D, DuffG W, WollheimF A. Synovial fluid concentrations of interleukin- I beta andproteoglycans are inversely related. Autoimmun 1988; 4:373-80.
64 Miyasaka N, Sato K, Goto M, et al. Augmented interleukin- 1
production and HLA-DR expression in the synovium ofrheumatoid arthritis patients. Possible involvement in jointdestruction. Arthritis Rheum 1988; 31: 480-6.
65 Seibel M J, Bruckle W, Respondek M, Beveridge T,Schnyder J, Muller W. Initial clinical experiences in thetreatment of chronic polyarthritis with a new monokinerelease inhibitor. Z Rheumatol 1989; 48: 147-51.
66 Smith J B, Bocchieri M H, Sherbin-Allen L, Borofsky M,Abruzzo J L. Occurrence of interleukin- I in humansynovial fluid: detection by RIA, bioassay and presence ofbio-assay inhibiting factors. Rheumatol Int 1989; 9: 53-8.
67 Hamerman D. The biology of osteoarthritis. N Engl Med1989; 320: 1322-30.
68 Brown R A, Weiss J B. Neovascularisation and its role in theosteoarthritic process. Ann Rheum Dis 1988; 47: 881-5.
69 Arner E C, Pratta M A. Independent effects of interleukin-1on proteoglycan breakdown, proteoglycan synthesis, andprostaglandin E2 release from cartilage in organ culture.Arthritis Rheum 1989; 32: 288-97.
70 Campbell I K, Piccoli D S, Roberts M J, Muirden K D,Hamilton J A. Effects of tumour necrosis factor a and P onresorption of human articular cartilage and production ofplasminogen activator by human articular chondrocytes.Arthritis Rheum 1990; 33: 542-52.
71 di Giovine F, Nuki G, Duff G W. Tumour necrosis factor insynovial exudates. Ann Rheum Dis 1988; 47: 768-72.
72 Goldring M B, Birkhead J, Snadell L J, et al. Interleukin 1
suppresses expression of cartilage specific types II andIX collagens and increases type I and III collagens inhuman chondrocytes. J Clin Invest 1988; 82: 2026-37.
73 Lindblad S. Arthroscopic and synovial correlates of pain inosteoarthritis. Semin Arthritis Rheum 1989; 18 (suppl 2):91-3.
74 Revell P A, Mayston V, Lalor P, Mapp P. The synovialmembrane in osteoarthritis: a histological study includingthe characterisation of the cellular infiltrate present ininflammatory osteoarthritis using monoclonal antibodies.Ann Rheum Dis 1988; 47: 300-7.
75 Pelletier J-P, Martel-Pelletier J. Evidence for the involvementof interleukin I in human OA cartilage degradation:protective effect of NSAID. 7 Rheumatol 1989; 16 (suppl18): 19-27.
76 Shinmei M, Masuda K, Kikuchi T, Shimomura Y. Inter-leukin 1, tumour necrosis factor and interleukin 6 asmediators of cartilage destruction. Semin Arthritis Rheum1989; 18 (suppl 2): 27-32.
77 Campen D H, Horwitz D A, Quismorio F P, EhresmannG R, Martin W J. Serum levels of interleukin-2 receptorand activity of rheumatic diseases characterized by immunesystem activation. Arthritts Rheum 1988; 31: 1358-64.
78 Ziff M. Relation of cellular infiltration ofrheumatoid synovialmembrane to its immune response. Arthritis Rheum 1974;17: 313-9.
79 Brennan F M, Chantry D, Jackson A, Maini R, FeldmannM. Inhibitory effect of TNFa antibodies on synovial cellinterleukin-1 production in rheumatoid arthritis. Lancet1989; ii: 244-7.
80 Goto M, Yoshinoya S, Miyamoto T, et al. Stimulation ofinterleukin-1 alpha and interleukin-1 beta release fromhuman monocytes by cyanogen bromide peptides of type IIcollagen. Arthritis Rheum 1988; 31: 1508-14.
81 Altman R D, Dean D D. Osteoarthritis research: animalmodels. Semin Arthritis Rheum 1990; 19 (suppl 1): 21-5.
82 Morris E A, McDonald B S, Webb A C, Rosenwasser L J.Identification of interleukin-I in equine osteoarthritic jointeffusions. Am Vet Res 1990; 51: 59-64.
83 Rashad S, Revell P, Hemingway A, Low F, Rainsford K,Walker F. Effect of non-steroidal anti-inflammatory drugson the course of osteoarthritis. Lancet 1989; ii: 519-22.
84 Freeman R, Wheeler J, Robertson H, Paes M L, Laidler J. Invitro production of TNF-a in blood samples. Lancet 1990;336: 312-3.
85 Brenner C A, Tam A W, Nelson P A, et al. Messageamplification phenotyping (MAPPing): a technique tosimultaneously measure multiple mRNAs from smallnumbers of cells. Biotechniques 1989; 7: 1096-103.
400
group.bmj.com on March 22, 2018 - Published by http://ard.bmj.com/Downloaded from
and rheumatoid arthritis.and different mechanisms in osteoarthritis Interleukin-1, immune activation pathways,
B Kirkham
doi: 10.1136/ard.50.6.3951991 50: 395-400 Ann Rheum Dis
http://ard.bmj.com/content/50/6/395.citationUpdated information and services can be found at:
These include:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on March 22, 2018 - Published by http://ard.bmj.com/Downloaded from