interdependence of evidence-based practice & shared ... · practice & shared decision...
TRANSCRIPT

Interdependence of Evidence-based Practice & Shared Decision Making –
Implications for Quality
Henry H. Ting, MD, MBA
Senior Vice President & Chief Quality Officer,
New York-Presbyterian Hospital
New York Academy of Medicine August 6, 2015

Disclosures A. No relationships with industry
B. Research grants: AHRQ (PI); NHLBI (Co-PI)
C. Foundations, Boards, & Professional Societies: NQF, ABIM, AHA, ACC

Objectives 1. What is shared decision making (SDM)? 2. Why do it?
3. How to do it?

Objectives 1. What is shared decision making (SDM)? 2. Why do it?
3. How to do it?

Evidence-based medicine 1. Make decisions based on all the relevant
research evidence

Confidence in estimates of benefit & risk 1. Bias design 2. Imprecision 3. Inconsistency 4. Indirectness 5. Biased reporting

21
5
10 1
1 2
8
7
8
12
4
3
1
1
2
8
7
2
1
1
1
2
8
1
5
15
6
Not
Men
tione
d
Rou
tine
Exp
erim
enta
l
Rar
e/N
ever
Spe
cific
M
M
M
M
M
Textbook/Review Recommendations
Odds Ratio (Log Scale)
0.5 1.0 2.0
Favors Treatment Favors Control
RCTs Pts
1 23
2 65
3 149
4 316 7 1793
10 2544 11 2651 15 3311 17 3929 22 5452
P<.01
23 5767
27 6125 30 6346 33 6571 43 21 059 54 22 051
67 47 531 65 47 185
70 48 154
P<.001
P<.00001
Cumulative Year
1960
1965
1970
1980
1985
1990
Fibrinolytic Therapy
Lau J. NEJM 1992; 327:248-254

Evidence-based medicine 1. Make decisions based on all the relevant
research evidence 2. Make decisions with more confidence when the
evidence is better

1. 30 year old mother of two and otherwise healthy develops pneumococcal pneumonia.
2. 80 year old man, demented, incontinent, and mute, without family or friends and in apparent discomfort. He develops pneumococcal pneumonia.
3. Woman with terminal cancer and chronic pain has come to terms with her condition, has issues in order, said her goodbyes. She wishes to receive palliative care. She develops pneumococcal pneumonia.
What would you do?

Atrial Fibrillation without treatment:
• In 2 years, 100 patients will have:
10 strokes (5 major, 5 minor)
2 serious upper GI bleeds
Atrial Fibrillation with anticoagulation:
• In 2 years, 100 patients will have:
2 strokes (8 fewer strokes)
How many more serious GI bleeds would you accept in 100 patients and still be willing to use anticoagulation?
What would you do?

Devereaux PJ et al. BMJ 2001;323:1218

Is this real?
530 Physicians 3120 patients with atrial fibrillation + warfarin bleed
90-365 days 90 days
1 afib patient at high risk of stroke
1 afib patient at high risk of stroke

Likelihood of warfarin prescription
1.0
0.79 (0.62-1.00)
0.60 (0.46-0.79)
0.61 (0.46-0.81) 0.72 (0.54-0.97)
1.00 90 d prior 0-90 d post
91-180 d post
181-270 d post
271-360 d post
Odds ratio (95% CI)
Less warfarin after bleeding
Days relative to bleed

Evidence-based medicine 1. Make decisions based on all the relevant
research evidence 2. Make decisions with more confidence when the
evidence is better 3. Evidence based medicine alone is never
sufficient to make a decision

Patient values
and preferences
Research evidence
Context

Patient values, preferences, & context

Parental Clinician-as-perfect agent
Shared decision-making Informed
Choice talk Implicit Clinician Team Patient
Option talk Informed consent Clinician Patient
Deliberation Clinician Clinician Joint Patient
Decision talk Clinician orders
Clinician recommends Consensus Patient
requests
Consistent with EBM principles No Yes Yes Yes
Decision making models
Modified from Charles C et al

Objectives 1. What is shared decision making? 2. Why do it?
3. How to do it?

CEO checklist for high-value health care IOM Roundtable, June 2012
Delos Cosgrove Cleveland Clinic
Micheal Fischer Cincinnati Children’s
Patricia Gabow Denver Health
Gary Gottlieb Partners HealthCare
George Halvorson Kaiser
Brent James Intermountain
Gary Kaplan Virginia Mason
Jonathan Perlin HCA
Robert Petzel Dept Veterans Affairs
Glenn Steele Geisinger
John Toussaint ThedaCare

2011-2012
2014
2016


Shared decision making Why do it?
1. Payment and policy
2. Efficiency – time, cost, utilization
3. Patient Safety
4. Patient Engagement
5. Patient Experience
6. Ethics

Objectives 1. What is shared decision making? 2. Why do it?
3. How to do it?

ACC/AHA cholesterol guidelines
Stone NJ. Circulation. 2014;129(25 Suppl 2):S1-45.

1. Four high risk groups • Secondary prevention in patients with prior ACS,
revascularization, stroke/TIA, PAD
• Primary prevention for LDL ≥190
• Primary prevention for diabetes (age 40-75) and LDL 70-189
• Primary prevention if 10-year risk ≥7.5% 2. Treat to risk, not treat to target LDL 3. Use of statins
ACC/AHA cholesterol guidelines
Stone NJ. Circulation. 2014;129(25 Suppl 2):S1-45.

ACC/AHA cholesterol guidelines
Pencina MJ. NEJM. 2014; 370(15):1422-31

ACC/AHA Cholesterol Guidelines
Ionannidis JAMA . 2014; 311:463-464.

Glasziou and Haynes ACP JC 2005

Jackevicius CA. JAMA 2002; 288:462.
% Patients taking statins as prescribed
0
20
40
60
80
100
0.00 0.25 0.50 0.75 1.00 1.25 1.50 1.75 2.00Follow-up (yr)
Patie
nts
taki
ng s
tatin
s (%
)
Coronary artery disease
Acute coronary syndrome
Primary prevention
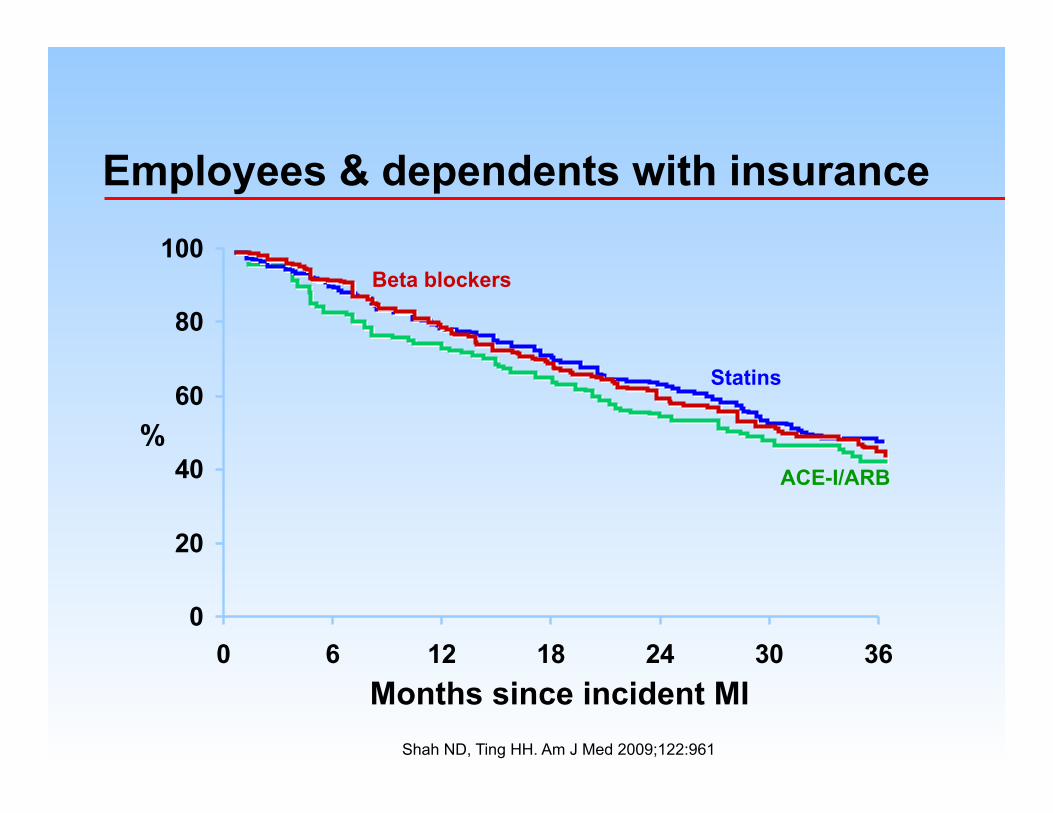
Shah ND, Ting HH. Am J Med 2009;122:961
Employees & dependents with insurance
0
20
40
60
80
100
0 6 12 18 24 30 36Months since incident MI
%
Statins
Beta blockers
ACE-I/ARB

ACC/AHA cholesterol guidelines
Montori VM, Ting HH. JAMA . 2014; 311:465-466.

Coylewright M, Ting HH. PLoS One 2012; 7(11):e49827
Participatory research

Web
Statin choice

Web
Statin choice

Video / Web
Diabetes Medication Choice

The Body of Evidence Systematic review of 115 RCTs
Compared to usual care, decision aids:
Increase patient involvement by 34%
Increase patient knowledge of options by 13%
Increase consultation time by ~2.6 minutes
Reduce decisional conflict by ~7%
Reduce % undecided by 40%
No consistent effect on choice, adherence,
health outcomes or costs
Stacey D et al. Cochrane review 2014

SDM and SES
Coylewright MC, Ting HH. Circulation CQO 2014; 7:360-367.

Opportunities for SDM in practice
1. When pros and cons are closely balanced
2. When pros>cons only if patients adhere
3. When pros and cons are not well known
