integumentary system fall 2014 carter & elias. anatomy review
TRANSCRIPT
Integumentary SystemFall 2014
Carter & Elias
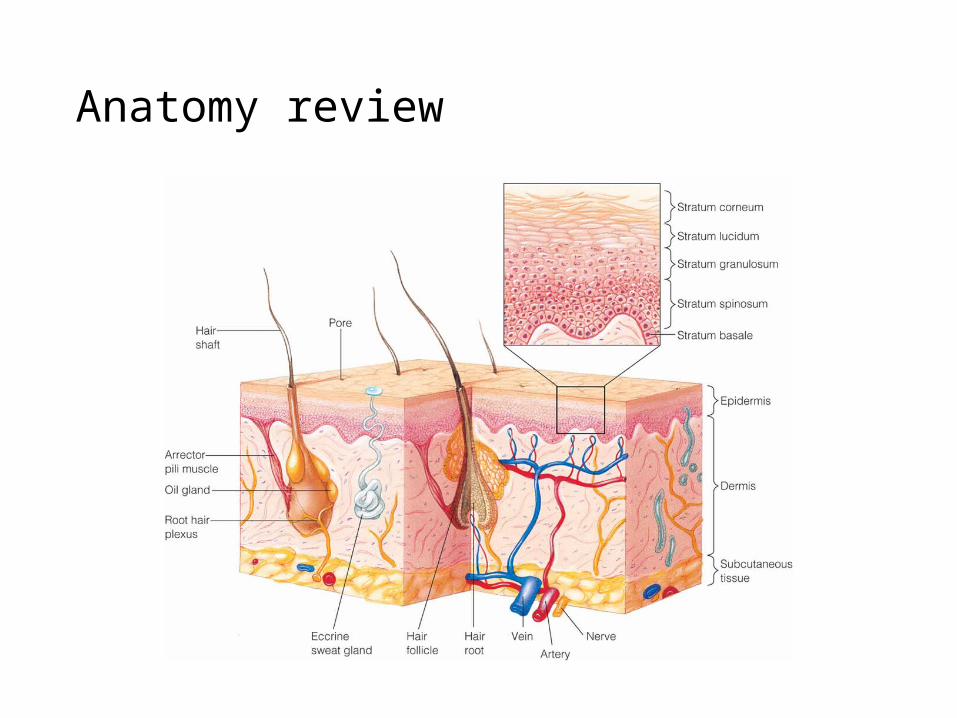
Anatomy review
Functions:
• P____________ _________________• Injury• Microbial Invasion• Fluid & Electrolyte Balance• Temperature control• E__________________• S__________________• V__________________• I __________________
Safe Effective Care Environment: 1. Identify factors that influence injury and disease prevention. Psychosocial Integrity: 4. Discuss psychosocial impact of client’s altered dermatological condition.
C. Matthews MSN, RN, CNE
KP’s
•Assessment• A. Parameters of General Skin Assessment • B. Cultural/Ethnic variations • C. Diagnostic Testing• D. Lesions

Thorough History
•Dx & Tx – realm of practice• Difficult due to similarities in lesions and sx
•Differential dx requires clues
Assessment: Subjective Data
• Past Medical History •T_______________•S_______________•P_______ _______ __________• J__________•D__________ __________ _________•A__________________ •S_______ ________________•R_____________ _____________
Safe Effective Care Environment: 2. Perform thorough dermatological assessment throughout the life span. C. Matthews MSN, RN, CNE
Assessment: History
M___________• Prescription• OTC• Herbals• Name• Length of usage
Safe Effective Care Environment: 1. Identify factors that influence injury and disease prevention ( sun exposure, environmental toxins, etc.). Physiologic Integrity: 5. Describe nursing implications for medications prescribed for clients with dermatologic disorders.
C. Matthews MSN, RN, CNE

Assessment: History• S__________
• Cosmetic• Biopsy
• D__________• H________________
• Hygiene, products• Sunscreen, SPF• Complementary & alternative
medicine
• C/O____________• Known _________ to
carcinogens, chemical irritants, allergens• F_____________
• Alopecia (bald)• Psoriasis• Skin cancer
Safe Effective Care Environment: 1. Identify factors that influence injury and disease prevention ( sun exposure, environmental toxins, etc.). Health Promotion and Maintenance: 3. Identify healthy behaviors by the client and family (screening exams, limiting risk taking behaviors).
C. Matthews MSN, RN, CNE
Assessment: History
• Any changes in the following:
• S_____ condition• H______ condition• N______ condition• M_______membranes
Safe Effective Care Environment: 2. Perform thorough dermatological assessment throughout the life span. C. Matthews MSN, RN, CNE

•Privacy•Carefully describe:• Obvious changes in color and vascularity• Presence or absence of moisture• Edema• Skin Lesions• Skin integrity
•Document properly
Assessment- ObjectiveAssessment- Objective
Parameters of General Skin Assessment- Pgs. 398-400 •c•t•m •e•t •t•o
Physiologic Integrity: 7. Explain the parameters of assessing a lesion. C. Matthews MSN, RN, CNE
Assessment: Inspection
• Consider Cultural and Ethnic variations• Dark skin (pg. 393)
• rates - skin cancer• http://www.cdc.gov/cancer/skin/statistics/race.htm
• wrinkles• Difficult to assess flushing; cyanosis; jaundice• Rashes difficult to observe • Keloids (page 406)
Assessment: Inspection
• Inspection of hair•D•T•Q
• Inspection of nails•G•P•R•C•S
Safe Effective Care Environment: 2. Perform thorough dermatological assessment throughout the life span. Physiologic Integrity: 11. Discuss etiology, clinical manifestations, and interventions for viral, bacterial, fungal, and parasitic skin disorders.
C. Matthews MSN, RN, CNE
MalnutritionAnorexia nervosaAnxietyHygiene DepressionHormonesLiving conditionsCirculatory statusChronic disease

Assessment: Palpation
•E•M•T•T•T
Safe Effective Care Environment: 2. Perform thorough dermatological assessment throughout the life span. C. Matthews MSN, RN, CNE
FeverC-V statusRespiratory statusHormonesHydrationRash/ LesionNutritional status
Diagnostic Testing
Biopsy
• Punch• Incisional• Excisional• Shave
RN Responsibilities
• Informed Consent• Prep site• Assist with procedure• Apply dressing• Post-op instructions• Properly ID specimen

Diagnostic Testing •Cultures• Diagnose fungal, bacteria, viral infections
• KOH (Potassium Hydroxide)• Fungus
•Sample collection• Skin scraping• Swabbing•Meticulous labeling

Diagnostic Testing
•Woods Light• Organisms fluoresce• Pseudomonas• Fungus
•Mineral oil slides• Infestations
•Patch/Scratch test• Allergen testing
Primary Lesions
• Macule, patch• Papule, plaque• Nodule, tumor• Vesicle, bulla• Wheal• Pustule• Cyst

Secondary Lesions
• Atrophy• Erosion• Lichenification• Scales• Crust• Ulcer• Fissure• Scar• Keloid
Lesion Description- pgs. 400-401
• Size•M
• Shape• C• I• R
• Texture• R• s
• Configuration• A• “relating to, or forming
a ring”• L• C _________ r______• C• D
• Effect of pressure
Safe Effective Care Environment: 2. Perform thorough dermatological assessment throughout the life span. Physiologic Integrity: 7. Explain the eight parameters of assessing a lesion. 8. Describe common lesions and rashes utilizing proper terminology
C. Matthews MSN, RN, CNE
Lesion Description
•Distribution•A____________ vs. S_________________•C_____________• “flowing or coming together; also : run together”
•D_____________• L_____________•S_____________•Z______________• “resembling shingles”
•S________________
Safe Effective Care Environment: 2.Perform thorough dermatological assessment throughout the life span. Physiologic Integrity: 7. Explain the eight parameters of assessing a lesion. 8. Describe common lesions and rashes utilizing proper terminology
C. Matthews MSN, RN, CNE
Infections of the skin• Risk factors
• Imbalance between host and microorganism• Broken or damaged skin; Trauma• Systemic disease such as Diabetes• Moisture• Obesity• Systemic corticosteroids, antibiotics
• Prevention• Proper hygiene• Good health

Infections: ViralHerpes Simplex Virus, Type I (AKA “cold sores/fever blisters”)
• Contagious• Dormant – Exacerbation
• Triggers
• Symptoms -- 1st episode 3-7 days after exposure• Painful local reaction• Vesicles on erythematous base• Fever, malaise

Herpes Simplex Virus, Type I
• Symptom management•Moist compresses• Petrolatum to lesions• Antiviral agents (Zovirax, Famvir, Valtrex)
•Medical Tx
Infections: ViralHerpes Simplex Virus, Type II
• Genital “Most genital herpes is caused by HSV-2.” (n.l.m.-n.i.h./ Medline plus)
• Recurrence more common than oral• Does not mean re-infection
• Symptoms• Same as Type I
• Treatment• Same as Type I
Infections: ViralHerpes Varicella Virus(chicken pox)
** Highly contagious• No chicken pox or vaccination• Keep those w/active lesions separated until crusted
•Symptoms• Vesicular lesions in successive crops• Face , scalp, spreading to trunk and extremities
• Protect eyes• Do not squeeze pustules or crusts
• Vesicles > pustules > crusts > scars
•Postherpetic neuralgia•Self limiting in children

Herpes Varicella Virus
Medical Tx
• Antivirals• Symptomatic relief

Infections: Viral Herpes Zoster(shingles)
• Activation of varicella zoster virus• Frequent occurrence in immunocompromised• Potentially contagious to immunocompromised
•Symptoms• Linear patches along dermatome• Grouped vesicles on erythematous base• Unilateral on trunk• Burning pain and neuralgia
Herpes Zoster
Medical Tx
• Symptomatic• Wet compresses• White petroleum to lesions
• Antiviral agents

Drug Therapy: Antivirals
• Acyclovir (Zovirax)• Suppresses chicken pox, herpes simplex 1 & 2, shingles• Po, IV, topical
• Valacyclovir (Valtrex)• Herpes zoster (shingles) & genital herpes
• Vaccines • Varivax
• Prevention of chicken pox• Given to children > 12 mo.
• Zostivax• HZU vaccine for adults > 60 y/o
Infections: Viral-WartsVerruca Vulgaris- (common warts)Plantar Warts
• Human papillomavirus- HPV•Mildly contagious
•Symptoms• Circumscribed hypertrophic flesh colored papule
•Treatment• Liquid nitrogen therapy•Medication• Electrodesiccation & Curettage
Infections: Bacterial
•Cellulitis• Staph aureus or strept• Can be primary or secondary infection• Symptoms• Hot• Tender• Erythematous• Edematous• Diffuse borders maybe malaise and fever
• Treatment• Moist heat• Immobilization• Elevation• Systemic antibiotics• Hospitalize if severe
• Can progress to gangrene if untreated
Infections- Bacterial MRSA
•Healthcare-Associated Infections (HA-MRSA)• Rates are decreasing but still over 117,000 cases/yr•MRSA causes infections of wounds, skin, lungs, urinary
system, bacteremia •Community-Associated Infections (CA-MRSA)• Over 15,000 cases/yr• Skin infections, pneumonia(CDC, Case reports for 2011)
Drug Therapy: Antibiotics• OTC
• bacitracin• Polymixin B
• Prescription• mupirocin (Bactroban) (MRSA)• gentamycin (Garamycin) (staph)• erythromycin (staph & strep)• clindamycin (Cleocin) (acne)(MRSA)• Trimethoprim- Sulfamethoxazole (Bactrim)(MRSA)
• Systemic - culture & sensitivity guides selection• Penicillin• Erythromycin• Tetracycline
Infections: Fungal Candidiasis (moniliasis)
• Candida albicans (Fungus)• 50% are symptom free carriers• Immunocompromised >> pathogenic• Likes warm moist areas
• Mouth, vagina, skin
An opportunistic infection

Candidiasis
• Symptoms• Mouth
• White, cheesy plaque (milk curds)• Vagina
• Vaginitis• Red edematous painful vaginal wall • White patches• Vaginal discharge• Pruritis• Painful urination & intercourse
• Skin• Diffuse papular erythematous rash• Pinpoint satellite lesions around edges
Physiologic Integrity: 5. Discuss nursing implications for medications prescribed for clients with dermatologic disorders. 6. Develop plan of care for client with impaired skin integrity.
Candidiasis
Medical Tx: Anti-fungals
• Nystatin (Mycostatin)• Vaginal suppository• Oral lozenge• Powder, cream
• Keep skin clean dry•Diagnosis:
cultureMicroscopic exam (KOH)Wood’s lamp
Picture from cram.com
Infections: FungalDermatophytoses (Tinea)
• Tinea Corporis- AKA ringworm• Tinea Pedis- AKA athlete’s foot• Tinea Cruris- AKA jock itch
• Symptoms• Erythema• Blistering• Pruritis• Pain
• Treatment:• antifungals-miconazole, clotrimazole, butenafine

Insects/Pests/Parasites
• Spiders• Fire Ants• Lice/Scabies• Mosquitoes• Scorpions• “Sand fleas”• Chiggers
• AKA harvest mites or red bugs
Spider bites
• http://www.badspiderbites.com/brown-recluse-spider-bite/

Infestations: Pediculosis
• Head, body or pubic lice (“crabs”)• Parasite excrement and eggs on skin• Nits in hair
• Waxy, don’t fall off easily
• Symptoms• Tiny red points to papular wheal-like lesions• Pruritis – check hairline• Secondary excoriation
Pediculosis
Medical tx
• Pyrethrins (Rid), Permethrin (Nix) or if all other agents fail…Benzene hexachloride (Kwell)• Contact screening• http://www.cdc.gov/lice/head/faqs_treat.html
11. Identify etiology, clinical manifestations, and interventions for viral, bacterial, fungal, and parasitic skin disorders. Physiologic Integrity: 6. Develop plan of care for client with impaired skin integrity.

Infestations: Scabies
• Skin reactions due to eggs, feces, & mite parts• Transmitted by direct contact
•Symptoms• Severe itching especially at HS• Usually not on face• Presence of burrows esp. interdigital webs & flexor surface
of wrists• Redness, swelling, vesiculation

Scabies
Medical tx
• Topical Scabicide• Antibiotics for 2ndary
infection• Treat those in close
proximity• Clothing & linens – hot water
and detergent
Nursing Management: Itchy skin
•Control of pruritis• Break the cycle of itching and scratching• Keep cool• No rubbing•Moisturize• Systemic antihistamines•Wet dressing• Topical steroids•Menthol, Camphor, Phenol numb itch receptors• Oatmeal baths

Nursing Management: Itch
•Baths• For large body areas• Has sedating and antipruritic effect• Oilated oatmeal (Aveeno), potassium permangenate,
sodium bicarb, coal tar derivatives• Temp comfortable to client• Soak 15-20 mins 3-4 times daily• Pat dry, no rubbing• apply moisturizers or meds after baths

Skin problems common in Florida
• Skin cancer• Sunburn-superficial burn• Insects• Plants• Water sports

Prevention/Education
•Sunscreen- SPF_____ and ______________• Limit exposure•Hat/clothes/sunglasses•Shade• Inspect skin regularly
Safe Effective Care Environment: 1. Identify factors that influence injury and disease prevention ( sun exposure, environmental toxins, etc.). Health Promotion and Maintenance: 3. Identify healthy behaviors by the client and family.
C. Matthews MSN, RN, CNE
Sunburn- Superficial Burns: Education(Protect, Protect, Protect)• Same precautions as for skin cancer.• Don’t let clouds or cool air fool you – Florida sun is damaging then
too.• Get out of the sun before you turn red!• Cool skin off. Immediately!• Hydrate!
Skin cancer - most common cancer!
•Risk factors:
Safe Effective Care Environment: 1. Identify factors that influence injury and disease prevention ( sun exposure, environmental toxins, etc.). Health Promotion and Maintenance: 3. Identify healthy behaviors by the client and family.
C. Matthews MSN, RN, CNE
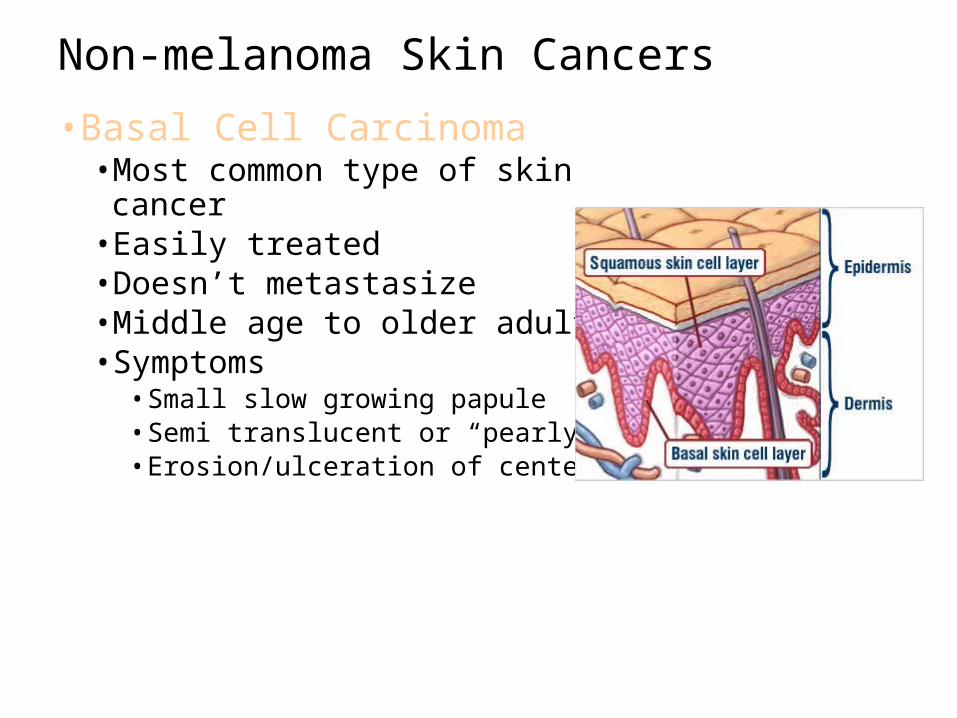
Non-melanoma Skin Cancers
•Basal Cell Carcinoma•Most common type of skin cancer• Easily treated• Doesn’t metastasize•Middle age to older adults• Symptoms• Small slow growing papule• Semi translucent or “pearly”• Erosion/ulceration of center

Basal Cell Carcinoma
Medical Tx
• Excision• Cryosurgery• Radiation• Topical chemotherapy
See illustration, figure 16-14

Non-Melanoma Skin Cancer
•Squamous cell• Less common than BCC• High cure rate with early detection• Can be aggressive, metastasize & be fatal• Common on lips, mouth, face and hands• Pipe, cigar, & cigarette smoking
• Symptoms• Firm nodule• Scaling/ulceration• Opaque
Squamous cell carcinoma
Medical Tx
• Excision• Radiation•Mohs surgery• 5 FU- topical or methotrexate
intralesional
Diagnostic & Surgical Therapy
• Simple Excision• Excision
• Mohs micrographic surgery• Microscopically controlled removal of lesion• Removes tissue in thin layers• Can see all margins of specimen• Preserves normal tissue• Produces smallest wound

Drug Therapy: Topical Fluorouracil (5-FU)
• Selective toxicity for sun damaged cells (cytotoxic)• Indications
• Premalignant skin disease (esp. actinic keratosis)• Systemic absorption minimal
-It causes painful eroded area within 4 days and must use 1-2 times daily 2-4 weeks.-Healing up to 3 weeks after med stopped-Is photosensitizing - avoid sunlight during treatment-Will look worse before it gets better
Non-Melanoma Skin Cancers•Actinic Keratosis (AKA Solar keratosis)•Most common precancerous lesion• Premalignant form of squamous cell carcinoma• Symptoms• Hyperkeratotic papules/plaques on sun exposed areas• Varied appearance
• Irregular shape• Flat• Indistinct borders• Overlying scale
Actinic Keratosis (AKA Solar keratosis)
Medical Tx:
•Cryosurgery•5 FU•Surgical removal•Retin A•Chemical peels
Cryosurgery• Subfreezing temps for surgery (liquid nitrogen)• Lesion becomes red & swollen, blisters, then scabs; falls off in 1-3
weeks• Minimal scarring
• Indications• Genital warts• Seborrheic keratosis• Actinic keratosis

Dysplastic Nevus Syndrome
•Abnormal mole pattern• Increased risk for melanoma• Doubles with dysplastic nevi
•Atypical moles larger than usual (>5mm)• Irregular borders, possibly notched•Various variegated colors•Most common on back
Malignant Melanoma
•Can metastasize ________________!•Most deadly of skin cancers•Causes• U____ _________________• S_____ ________________• G_____________________• H_____________________• S____ _________________•M_________ of gene (B-RAF) 70%
Safe Effective Care Environment: 1. Identify factors that influence injury and disease prevention ( sun exposure, environmental toxins, etc.).
C. Matthews MSN, RN, CNE
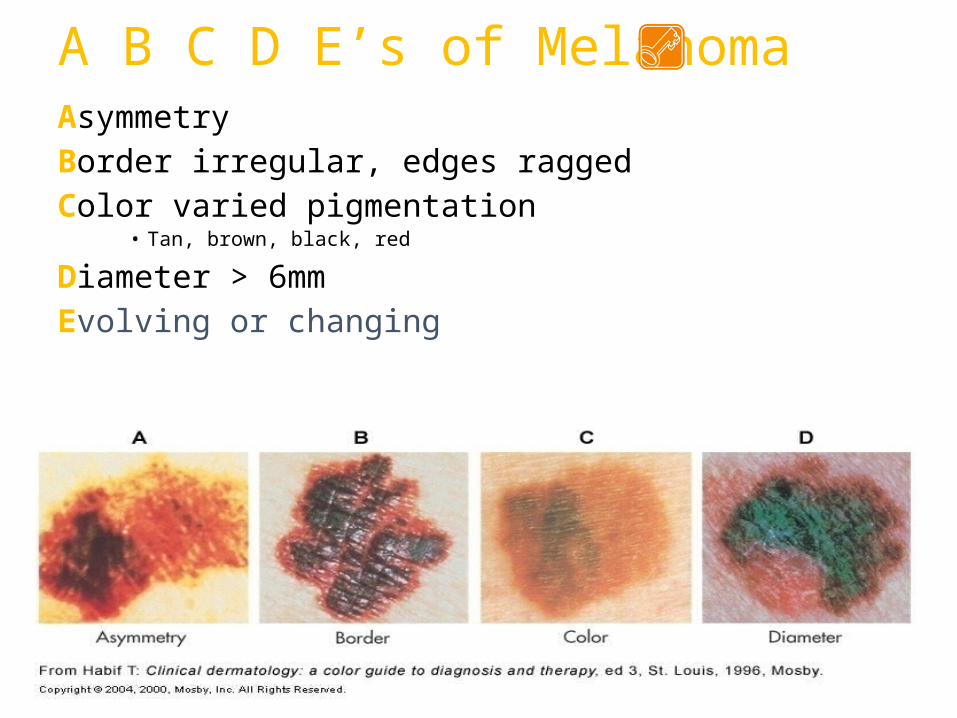
A B C D E’s of MelanomaAsymmetryBorder irregular, edges raggedColor varied pigmentation
• Tan, brown, black, red
Diameter > 6mmEvolving or changing
Melanoma
Medical Tx
Depends on site, stage, age and general health of client• Surgery• Immunotherapy• Interferon, interleukin
• Biologic Therapy• Radiation therapy
Inflammatory Disorders of the Skin
•Contact Dermatitis• Allergic Contact Dermatitis• Delayed hypersensitivity • Lesions 2-7 days after antigen exposure
• Irritant Contact Dermatitis• Inflammation of skin from irritants
•Manifestations• Red, hive-like papules and plaques• Sharply circumscribed• Pruritic Vesicles

Inflammatory Disorders of the SkinContact Dermatitis
• Topical corticosteroids• Antihistamines• Skin lubrication• Elimination of allergen• Systemic steroids if severe
• Medical Tx
Inflammatory Disorders of the Skin : Atopic Dermatitis AKA Eczema
• Cause unknown• Begins in infancy and declines with age
•Manifestations• Scaly, red to re-brown, circumscribed lesions• Pruritic• Symmetric eruptions
Inflammatory Disorders of the Skin- Atopic Dermatitis
• Topical corticosteroids• Phototherapy• Coal tarhttp://www.psoriasis.org/netcommunity/sublearn03_mild_otc• Intralesional corticosteroids• Lubrication of dry skin• Antibiotics for secondary infections
• Medical Treatment

Drug Therapy: Antihistamines • Compete with histamine receptor site• Oral or Topical• Cetitizine (Zyrtec)
• PO tabs, syrup QD• Non-sedating
• Diphenahydramine (Benadryl)• PO, IM, topical
• Indications• Urticaria• Pruritis• Allergic reactions
• Adverse effects• Anticholinergic• Sedation (Benadryl)• Use with caution in older adults

Inflammatory Disorder of the Skin- Acne Inflammatory disorder of sebaceous glands
•Symptomscomedones, inflammatory lesions, papules, pustules face, neck, upper back
•Treatment• Comedo extraction• Topical Benzoyl Peroxide• Peeling and irritating agents (retinoic acid)• Antibiotic therapy - long term• Phototherapy• Sun exposure• If severe - isotretinoin (Accutane) CAUTION! Teratogenic
Drug Therapy: Acne Preparations
• Benzoyl peroxide (Benzac, Desquam-X, PanOxyl, etc)• Apply 1-4x day• Effects seen 4-6 weeks• Adverse effects
• Erythema, tenderness, dryness, pruritis, burning• Erythromycin (Eryderm, T-Stat, Erygel)
• Macrolide antibiotic• Adverse effects
• Erythema, tenderness, pruritis, burning
Drug Therapy: Acne Preparations
• Isotretinoin (Accutane)• Pregnancy Category X
• Proven teratogenic• 2 contraceptive methods
• Tretinoin (Retinoic acid, Vitamin A acid, Retin-A)• Stimulates epidermal cell turnover -> skin peeling• Adverse effects
• Red edematous blisters, crusted skin, altered skin pigmentation• Avoid sun, use sunscreen• Apply to dry skin
Chronic Immune Skin Disorder• Psoriasis• Chronic dermatitis due to rapid turnover of epidermal cells• Family predisposition• Manifestations• Sharply demarcated scaling plaques of • Scalp• Elbows• Knees• Palms, soles, and fingernails possible
• Treatment• Retard growth of epidermal cells• Topical corticosteroids• Tar• Anthralin topical• Sunlight, UV light• Alefacept (Amevive) injection• Antimetabolites (methotrexate) or systemic retinoids for difficult cases
Benign Skin Conditions• Seborrheic Keratoses
• Irregularly shaped flat topped papules or plaques• Warty surface• Appearance of being stuck on• Increase in pigmentation• No association with sun exposure• Treatment
• Removal • Curettage• cryosurgery