integration of care in management of ckd in resource
TRANSCRIPT

Integration of Care in Management of CKD inResource-Limited Settings
0270-9295/ - see front& 2017 Elsevier Inc. Ahttp://dx.doi.org/10.101
Financial disclosure an
*Division of NephroloTown, Cape Town, S
†Department of MedCanada.
‡Zenith Medical and K
Address reprint requesSchuur Hospital, UnObservatory, 7925,[email protected]
260
Ikechi G. Okpechi, MD, PhD,* Aminu K. Bello, MD, PhD,†
Oluwatoyin I. Ameh, MD, MPhil,‡ and Charles R. Swanepoel, MD, FRCP*
Summary: The prevalence of noncommunicable diseases, including chronic kidney disease (CKD),
continues to increase worldwide, and mortality from noncommunicable diseases is projected to surpasscommunicable disease–related mortality in developing countries. Although the treatment of CKD is expensive,unaffordable, and unavailable in many developing countries, the current structure of the health care system insuch countries is not set up to deliver comprehensive care for patients with chronic conditions, including CKD.The World Health Organization Innovative Care for Chronic Conditions framework could be leveraged toimprove the care of CKD patients worldwide, especially in resource-limited countries where high cost, lowinfrastructure, limited workforce, and a dearth of effective health policies exist. Some developing countriesalready are using established health systems for communicable disease control to tackle noncommunicablediseases such as hypertension and diabetes, therefore existing systems could be leveraged to integrate CKDcare. Decision makers in developing countries must realize that to improve outcomes for patients with CKD,important factors should be considered, including enhancing CKD prevention programs in their communities,managing the political environment through involvement of the political class, involving patients and theirfamilies in CKD care delivery, and effective use of health care personnel.Semin Nephrol 37:260-272 C 2017 Elsevier Inc. All rights reserved.Keywords: CKD, chronic disease management, integrated care, health policyChronic kidney disease (CKD) is prevalentworldwide and increasingly is being recog-nized as an important public health issue with
adverse clinical and economic consequences.1,2 Cost ofCKD treatment and mortality continues to increase inseveral countries.3–6 Part of the problem is related tothe health care approach adopted for the managementof chronic conditions around the world. Althoughhealth systems in developed countries largely haveadopted approaches suitable to manage chronic dis-eases, including CKD, the situation in low- to middle-income countries (LMICs) is very different.
Integrated care in the management of CKD repre-sents an approach to get political leaders, policy-makers, health care practitioners, patients, and thecommunity together to ask important questions andprovide practical solutions toward effective kidney carein their own setting. As health systems around theworld continue to undergo innovation,7,8 including amovement away from the traditional acute care
matterll rights reserved.6/j.semnephrol.2017.02.006
d conflict of interest statements: none.
gy and Hypertension, University of Capeouth Africa.icine, University of Alberta, Edmonton,
idney Centre, Garki, Abuja, Nigeria.
ts to Ikechi G. Okpechi, MD, PhD, Grooteiversity of Cape Town, E13 Renal Unit,Cape Town, South Africa. E-mail: Ikechi.
management process to one that uses integrated meth-ods to provide chronic disease care, there is a need forbuy-in into this approach in LMICs, which are likely tocontinue to experience an increasing burden of CKD inthe coming years.9 This review discusses the concept,barriers, and application of integrated CKD care inLMICs. First, we define the concept of integrated careand link its taxonomy to management of CKD inLMICs. Second, we discuss the perceived barriers toeffective CKD care, and, third, we recommend prac-tical approaches to integration of CKD care in LMICsusing the predefined World Health Organization(WHO) model of care for chronic diseasemanagement.10
MODELS OF CARE FOR CHRONIC DISEASES
In 2002, the WHO proposed the Innovative Care forChronic Conditions (ICCC) as a new model of healthsystems to help manage the global increasing epidemicof chronic diseases, including both communicable andnoncommunicable diseases (Fig. 1).10 The new modelwas based on the chronic care model, a framework forimproving chronic illness care and for improving careat both the individual and population level.11 Knowl-edge that aspects of the chronic care model could notbe applied worldwide, especially in developing coun-tries, gave birth to the ICCC framework based on a setof precepts at 3 levels (Fig. 1).10,12
The micro level highlights partnership betweenfamilies/patients, health care teams, and communities,and functions best when every member at this level isinformed, motivated, and prepared with the skills
Seminars in Nephrology, Vol 37, No 3, May 2017, pp 260–272
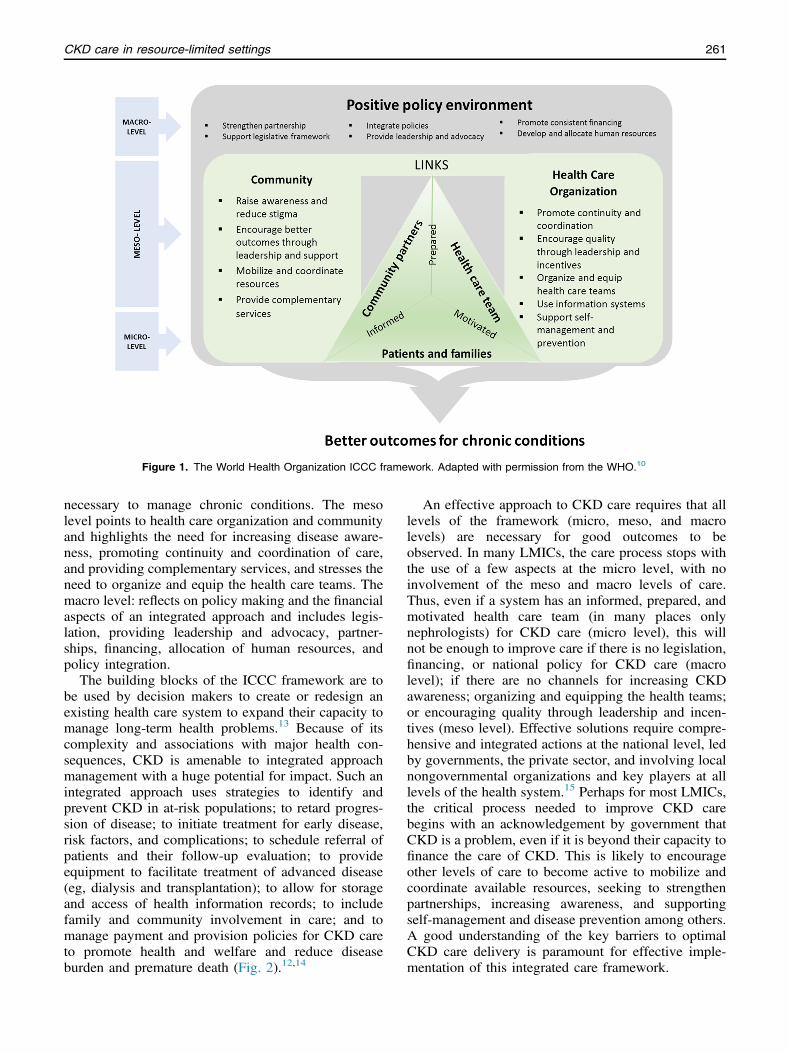
Figure 1. The World Health Organization ICCC framework. Adapted with permission from the WHO.10
CKD care in resource-limited settings 261
necessary to manage chronic conditions. The mesolevel points to health care organization and communityand highlights the need for increasing disease aware-ness, promoting continuity and coordination of care,and providing complementary services, and stresses theneed to organize and equip the health care teams. Themacro level: reflects on policy making and the financialaspects of an integrated approach and includes legis-lation, providing leadership and advocacy, partner-ships, financing, allocation of human resources, andpolicy integration.
The building blocks of the ICCC framework are tobe used by decision makers to create or redesign anexisting health care system to expand their capacity tomanage long-term health problems.13 Because of itscomplexity and associations with major health con-sequences, CKD is amenable to integrated approachmanagement with a huge potential for impact. Such anintegrated approach uses strategies to identify andprevent CKD in at-risk populations; to retard progres-sion of disease; to initiate treatment for early disease,risk factors, and complications; to schedule referral ofpatients and their follow-up evaluation; to provideequipment to facilitate treatment of advanced disease(eg, dialysis and transplantation); to allow for storageand access of health information records; to includefamily and community involvement in care; and tomanage payment and provision policies for CKD careto promote health and welfare and reduce diseaseburden and premature death (Fig. 2).12,14
An effective approach to CKD care requires that alllevels of the framework (micro, meso, and macrolevels) are necessary for good outcomes to beobserved. In many LMICs, the care process stops withthe use of a few aspects at the micro level, with noinvolvement of the meso and macro levels of care.Thus, even if a system has an informed, prepared, andmotivated health care team (in many places onlynephrologists) for CKD care (micro level), this willnot be enough to improve care if there is no legislation,financing, or national policy for CKD care (macrolevel); if there are no channels for increasing CKDawareness; organizing and equipping the health teams;or encouraging quality through leadership and incen-tives (meso level). Effective solutions require compre-hensive and integrated actions at the national level, ledby governments, the private sector, and involving localnongovernmental organizations and key players at alllevels of the health system.15 Perhaps for most LMICs,the critical process needed to improve CKD carebegins with an acknowledgement by government thatCKD is a problem, even if it is beyond their capacity tofinance the care of CKD. This is likely to encourageother levels of care to become active to mobilize andcoordinate available resources, seeking to strengthenpartnerships, increasing awareness, and supportingself-management and disease prevention among others.A good understanding of the key barriers to optimalCKD care delivery is paramount for effective imple-mentation of this integrated care framework.

Figure 2. Strategies for the prevention of CKD.
I.G. Okpechi et al.262
BARRIERS TO EFFECTIVE CKD CARE DELIVERYIN LMICS
Workforce
Deficiencies in the nephrology workforce includingnurses, general physicians, dialysis technologists, med-ical specialists, and nephrologists for the provision ofadequate kidney care remains a critical problem inseveral LMICs. In developed countries, inadequacy ofthe nephrology workforce has been linked to an agingworkforce, decreasing interest in nephrology amongtrainees, increasing cultural and ethnic disparitiesbetween patients and care providers, inflexible workschedules, and a reduced focus on scholarship andresearch funds; however, in LMICs, inadequate facili-ties for training and loss of trained personnel todeveloped countries largely account for the reducednumbers.15,16 As physicians and nurses leave theirhome countries to seek greener pastures, they leave ahuge workforce gap behind to provide care for arapidly growing and aging population. Such a patternof migration often has been shown to be permanent.17
In many countries in Africa, for example, there areno health care professionals in the rural areas toserve the population.18 Several reports have shownthat the number of nephrology specialists (per millionpopulation) in many countries in Africa is less thanone (Table 1).16,19,20 The continual low workforce
available to provide service to the health care systemwill have a perpetuating effect on weakening the healthcare structures because fewer qualified health careworkers will be available to train the next generation.As a strategy to limit the decreasing nephrologyworkforce, comprehensive and effective nephrologyworkforce planning should be implemented that takesinto consideration the structure and organization of thehealth system, existing care delivery models, nephrol-ogy workforce practices, and the size, quality, andsuccess of internal nephrology training programs.16
A sparse workforce for delivering care is an impor-tant reason to advocate strongly for integrated care inLMICs to improve efficiency, reduce the duplication ofservices, and improve the overall care of patients. Thisprocess could involve a task-shifting approach thatuses trained nonphysician health care workers toperform health tasks to meet the needs of patients.This approach has been used extensively to tackle thehuman immunodeficiency virus (HIV)/acquiredimmune deficiency syndrome epidemic in sub-Saharan Africa. One systematic review on task shiftingfor HIV treatment and care in Africa reported increasedaccess to antiretroviral therapies (ART) throughexpanded clinical capacity, improved cost effective-ness, and good agreement between nonphysician clini-cian decisions with physician decisions.21 Otherstudies also have reported overall good outcomes such

Table 1. Global Health Workforce: Physicians and Nephrologists16,19,20
Physicians (N) Physician Densityper 10,000 Population
Nephrologist Densityper 1,000,000 Population
Population Living inUrban Areas (%)
WHO regionAfrica 33,183 2.7 1 38The Americas 1,981,621 21.5 22 (North America); 80
8 (South America)Europe 2,356,671 32.1 31 71Southeast Asia 1,128,508 5.9 1 35
Income groupLow income* 213,982 2.5 - 30
(24,531)†
Lower middle income‡ 1,991,612 7.9 - 39(323,860)†
Upper middle income§ 3,755,703 16.1 - 62(110,623)†
High income|| 3,186,223 28.7 - 80(153)
*African countries in this category include the following: Benin, Burkina Faso, Burundi, Central African Republic, Chad, DemocraticRepublic of Congo, Eritrea, Ethiopia, Gambia, Guinea, Guinea-Bissau, Kenya, Liberia, Malawi, Mali, Mozambique, Niger, Rwanda,Sierra Leone, Somalia, Togo, Uganda, United Republic of Tanzania, and Zimbabwe.†Number of physicians in African countries is shown in parentheses.‡African countries in this category: Cameroon, Congo, Cote d’Ivoire, Djibouti, Egypt, Ghana, Lesotho, Mauritania, Morocco, Nigeria,Senegal, South Sudan, Sudan, Swaziland, and Zambia.§African countries in this category: Algeria, Angola, Botswana, Gabon, Libya, Mauritius, Namibia, South Africa, and Tunisia.||African countries in this category: Equatorial Guinea.
CKD care in resource-limited settings 263
as reduced rates of loss to follow-up evaluation ofpatients and improved roll out of ARTs when non-physician clinician-based care has been accessed inHIV treatment.22,23 A similar approach could beengaged to improve kidney care delivery using nurse-led care or pharmacist-led care in places where there isa shortage of doctors. Such care could be integratedinto existing hypertension, diabetes clinics, or evenwithin other areas such as HIV clinics. However, suchapproaches will need proper training and retraining ofstaff, adequate referral channels, and support structuresto ensure success. Training can be facilitated byaccessing nephrologists from various countries forhands-on training, setting up community screeningprograms, or staff training for task shifting throughthe International Society of Nephrology EducationalAmbassador program (www.theisn.org/programs).
Infrastructure
Since the introduction of life-saving hemodialysis,nephrology, as a worldwide specialty, has laggedbehind other internal medicine specialties, especiallycardiology and oncology, including the capacity toconduct clinical trials, use of new medicines andtechnologies, and general infrastructure available toensure adequate provision of care.24 Many countriesstill do not have adequate infrastructure necessary forthe provision of basic nephrology services including
laboratories to measure serum creatinine and reportglomerular filtration rate (GFR), pathologic services forreporting kidney biopsy, medications, and treatmentfacilities such as for dialysis for end-stage kidneydisease (ESKD) therapy.25 In Nigeria, for example,with an estimated population of 175 million people anda high prevalence of CKD, growth of hemodialysis(HD) units (each unit capable of supporting 10-20patients at a time), increased from 56 in 2004 to 76 in2014, pointing to a severe shortage of infrastructure fornephrology service provision.26 Limited infrastructurefor manufacturing, transport, and storage of peritonealdialysis (PD) fluids and high costs contribute to the lowutilization of PD compared with HD in manyLMICs.25,27
The lack of such infrastructure is not limited tonephrology services but is widespread, affecting otheraspects of medical care and social life. In Africa, with ahigh prevalence of HIV and despite recommendationsfrom HIV treatment guidelines to estimate kidneyfunction before the initiation of treatment as well asroutinely during follow-up evaluation, especially if thepatient is to be treated with a tenofovir-based regi-men,28,29 this often is not feasible. One large studyfrom Cape Town of 13,168 HIV-positive patients whostarted ART from 2010 to 2012 found a creatininemeasurement for 88.9% at baseline in patients initiatedon tenofovir and for 78.4% at 3 months.30 At baseline,1.9% still were commenced on tenofovir despite an

I.G. Okpechi et al.264
estimated GFR less than 50 mL/min, potentially plac-ing patients at risk of further kidney injury.30 Even inSouth Africa, resources are not always available toperform these tests and where they are performed theremay be infrastructural gaps for physicians to be able toaccess results of tests performed from other institu-tions. The available infrastructure is likely much less inlower-income regions. Although it is not advocated forall institutions, especially at the primary care level, tobe equipped with a laboratory, an opportunity tointegrate CKD care may enhance care in other areas,and could include setting up services for collection ofsamples and mechanisms to ensure that such results arereadily available to caregivers.
Cost of Treatment
Funding for various health care programs such as thosefor HIV, tuberculosis, and malaria in several LMICscome from external donors in developed countries.31
Although such funding is important in stimulatinginnovation and assisting with care in countries thatare unable to meet the needs of the public health sector,the long-term sustainability is often in question. Thecost of renal replacement therapies as well as the costof care to prevent or retard progression of CKDcontinues to increase astronomically worldwide. Datafrom the United States show that treatment costs forESKD in 2010 were 6.3% of the Medicare budget,whereas the costs for earlier stages of CKD werehigher at 27% of the total Medicare budget in 2007.3
In many developed countries, such services are avail-able for free at point of care. Patients in many LMICsoften have to pay out of pocket to receive care forchronic diseases. A study from Cameroon analyzed thecost of diagnostic tests and essential medicines forcardiovascular disease and diabetes care, and showedthat patients often needed to spend from up to onequarter to more than half of their monthly income topay for a month’s supply of individual medicationssuch as angiotensin-converting enzyme inhibitors orantidiabetic medications.32 Another study from Nigeriahas shown that an inability to pay for dialysis was ahuge factor accounting for the number of patientsunable to continue treatment; only 3 of 227 patientswere able to afford renal replacement therapy paymentfor more than 3 months.33 Cost, perhaps more than anyother factor, remains the Achilles heel for CKD servicedelivery in many LMICs at both the primary care andtertiary care level. Therefore, this suggests a need for aradical change in the approach to CKD care indeveloping countries from one that centers on individ-ual care to a population intervention strategy for theprevention of CKD. A population intervention app-roach could involve identifying the most effectiveways of ensuring the availability of medicines to delay
or prevent the progression of CKD (eg, availability ofgeneric drugs, ensuring that only genuine drugs getinto the market, an efficient drug regulatory authorityto oversee the process, consideration of a polypillstrategy).34 Other ways to reduce the overall costs forpatients in places where patients pay out of pocket alsocan include reducing the frequency of unnecessaryclinic visits (to reduce transportation costs) by integra-tion of CKD care with that of other diseases, facilitat-ing community-based care, and to only orderlaboratory tests that will assist in diagnosis and treat-ment. Such approaches will reduce the cost of treat-ment and are likely to improve CKD outcomes.
Emphasis for integration of CKD care in LMICs innoncommunicable disease programs should focus onprevention and early detection. Utilization of WorldKidney Day (www.worldkidneyday.org), whichincreasingly has become an opportunity to screen thegeneral population for CKD in many countries, shouldbe encouraged and broadened to assist with earlydisease detection. Other avenues also should beincluded to meet the goals of early identification ofpatients with risk factors as well as CKD (eg, WorldHypertension Day, World Diabetes Day, and so forth).Research organizations also can assist this process byprioritizing screening and early evaluation of kidneydisease programs or kidney early evaluation programsfor kidney disease research funding in developingcountries. Questions will arise regarding the costeffectiveness of screening or early detection pro-grams,35 or how patients identified with early CKDin this setting will be managed, given that there areother limiting factors to accessing care. In the MAR-EMAR (Maladie Rénale Chronique au Maroc) study ascreening and prevention program in Morocco, clinicalfollow-up visits were scheduled for patients identifiedwith CKD stage 3a, 3b, and 4, and young subjects witha low estimated GFR for their age (othird percentilefor age and sex category) to initiate appropriateinterventions in those identified to be at risk ofworsening kidney function.36 Through such programs,early disease detection and the awareness generatedmay bring about lifestyle changes or improve health-seeking behavior that will slow the progressionof CKD.
Health Care Policies, Health Systems, and HealthCare Funding
Effective health systems are strong elements of qualitychronic disease care in all parts of the world.15 Adysfunctional health system will affect all importantaspects in the chain of health provision includingaccess to medicines, availability of workforce, fundsfor new technologies, legislation, and policies forhealth financing. Supporting health systems in LMICs

CKD care in resource-limited settings 265
remains challenging because of the profound impact ofthe double burden of communicable and noncommu-nicable disease epidemics they are facing, fragmenta-tion of the health systems through the running ofparallel programs, poor financing, lack of maintenanceof existing programs, and levels of corruption in thehealth care sectors.15,37–39 Leadership is crucial toidentify opportunities to improve health system func-tioning. It has become clear that the failure of leader-ship in tackling the HIV epidemic has contributed tovarious poor health outcomes including an exacerbatedtuberculosis epidemic with the emergence ofmultidrug-resistant and extensive drug-resistant strainsand thousands of preventable deaths.40 The develop-ment of sound policies targeted to the prevention ofCKD and its risk factors in LMICs, as well asmanagement strategies to improve the efficiency ofhealth care delivery, can help to reduce the increasingburden of disease in these countries.
KIDNEY DISEASES AND INFECTIOUS DISEASESINTERSECTIONS: NEED FOR INTEGRATED HEALTHSYSTEMS
Many LMICs already have effective systems in placeto handle the burden of communicable diseases such asHIV, tuberculosis, and malaria. In many instances,these systems have been supported through extensivefunding from developed countries such as the USPresident’s emergency plan for AIDS relief, whichhas provided significant funding for HIV treatment andresearch in Africa (www.pepfar.gov). Remarkably,several of these infections intersect with kidney diseaseeither directly, by way of shared structural or socio-economic risk factors, or treatment. For example, CKDis an important cause of morbidity and mortality inHIV-positive patients, especially in the elderly, inthose of black ethnicity, and in the presence of hyper-tension or diabetes.41,42 In addition, acute kidneyinjury (AKI) can occur in patients with HIV treatedwith some ART regimens such as tenofovir or relatedto co-infections or use of other antibiotics.30 Similarly,clearly defined links have been established betweentuberculosis, malaria, and hepatitis infections with AKIor CKD.43–45 Kidney disease detection, prevention,and treatment therefore practically could be leveragedon established programs with infrastructure for com-municable diseases care and control given theseintersections with AKI and CKD. Such intersectionshave been identified and described in South Africawhere HIV, tuberculosis, diabetes, and hypertensionaccounted for prescriptions in 45% of patients attend-ing a primary care clinic and 22.6% had multiplemorbidities; diabetes and hypertension were moreprevalent in younger patients on ART than in patients
not receiving ART.46 Because of multimorbidity inHIV patients in South Africa, Oni et al47 suggested amodification to the WHO ICCC model for LMICs tocover gaps in the ICCC framework related to manage-ment of comorbid noncommunicable and infectiouschronic diseases. The proposed framework includes theincreased complexity of treating comorbid noncommu-nicable and infectious chronic diseases patients andhighlights the importance of biological interactions indisease. The framework is based on observations thatpatient experiences such as treatment adherence, healthcare use, and health outcomes are influenced bydemands that the health system places on patients,which are especially difficult to meet for patients livingin significant poverty. Strategies that focus on incor-poration of biological interactions with considerationsof demands placed on patients and health providershold promise to make health systems more effective.47
As an example, South Africa currently is imple-menting the integrated chronic disease managementmodel (including HIV, tuberculosis, diabetes, hyper-tension, asthma, epilepsy, asthma, chronic obstructivepulmonary disease, and mental health illnesses), whichbuilds on the strengths of the HIV/tuberculosis inte-grated program.48 The integrated chronic disease man-agement focuses on restructuring of the primary healthcare system to improve efficiency through the use ofclinical algorithms as well as training of communitycare workers in the prevention, promotion, and treat-ment of these diseases. The multimorbidity modelfurther empowers patients and assists with self-management of their chronic diseases.48 CKD thusfar is not managed within this model, however,integration of CKD care using existing programswould have the potential to reduce costs and improveefficiency for patients with kidney disease given thatthe same facilities are likely to be used, the staffrequirement overall may be reduced (also saving cost),and patients’ engagement with the health system islikely to be improved because care for various chronicdiseases can be accessed in one location, with fewerclinic visits and better provider oversight of the wholepatient.
USING THE EIGHT ESSENTIAL WHO ELEMENTS FORACTION TOWARD CKD INTEGRATED CARE IN LMICS
The ICCC framework outlines eight essential factors inthe course of action to be pursued for integration basedon the level of resources available. These points weredeveloped to highlight elements that decision makersshould be aware of, what the strength of the healthsystem is for each factor considered, what should beperformed to improve care delivery, with useful

I.G. Okpechi et al.266
examples provided that can be applied for each factorin low-, medium-, and high-resource settings.10
It generally is assumed that applying an integratedapproach to chronic disease management can be costeffective; however, there has been a general lack ofcost evaluations of such systems, especially related toCKD care. Although some data suggest that anintegrated approach to care can be cost saving, othershave reported it to be expensive.49,50 Cost is always abarrier for developing countries and the current lack ofdata effectively may limit willingness to adopt anintegrated care approach for CKD care, which isconsidered very expensive. Despite this, using theICCC framework as building blocks for integratedCKD care in LMICs highlights important practicalpoints that should be considered. Table 2 summarizeskey information from the ICCC framework for deci-sion makers that is pertinent to CKD care delivery,what can be performed within a country’s setting, andpractical examples that can be followed. The keyelements for action and information for decisionmakers relevant to CKD care are summarized later.10
SUPPORT A PARADIGM SHIFT ON KIDNEYDISEASES
Policy makers must recognize that incidence andprevalence rates of CKD continue to increase globallyowing to increases in diabetes, hypertension, obesity,and a rapidly aging population.2,51 CKD managementand care is complex, often needing a multidisciplinaryapproach. For this to be effective, it requires a healthsystem approach involving extended and regular healthcare contact to minimize CKD complications and toslow CKD progression.52 Various classes of medica-tions are required to treat CKD adequately and there-fore should be available in the country and affordableto patients to treat the different complications associ-ated with CKD such as hypertension, anemia, mineralbone disease, and dyslipidemia.
MANAGE THE POLITICAL ENVIRONMENT: GETTHE POLITICIANS INVOLVED
The planning and implementation of service deliveryfor effective CKD management will become moreeffective if it takes place within a political context.Given that there is considerable resource limitation inmany countries, thought should be given to criticalaspects of CKD care such as dialysis and kidneytransplantation and governments must develop clearpolicies around access to such care where it is limitedor unavailable. For example, few African countries(Egypt, Libya, Algeria, Tunisia, Morocco, SouthAfrica, Mauritius, and Gabon) have a national dialysis
program that is paid for by the government and capableof accommodating treatment for 100 dialysis patientsper million population.53 In other countries, there hasbeen no government policy or service planning from apolitical context. Planning for integrated CKD manage-ment should not be one-sided (from the policy makers),but must take into consideration health care leaders,patients, families, community members, traditionalhealth practitioners, and organizations that representkidney disease patients. For positive transformationtoward care of CKD, information should be shared andreadily available across groups and a need for politicalcommitment and consensus building among stakehold-ers at each stage.
BUILD INTEGRATED HEALTH CARE FAVORABLEFOR CKD MANAGEMENT
Effective health systems for CKD care requires inte-gration to ensure shared information across settingsand providers, and across time. For example, systemsshould be in place to have access to electronic healthrecords (eg, serum creatinine levels) from differenthospitals within the same town and banked for accessacross time. Estimated GFR reporting for all laboratoryreporting of serum creatinine levels also should beimplemented because this becomes a useful clinicalvalue for all those assessing or interpreting the resultsand assists in identifying patients with CKD.7,54
Coordinating financing across different arms of healthcare (eg, inpatient, outpatient, and pharmacy services)and incorporation of community resources (eg, trans-portation) that all can improve the efficiency of overallhealth care services.
ALIGN ALL SECTORAL POLICIES TO IMPROVEKIDNEY HEALTH
The policies of all government sectors (eg, national,provincial, and local government) for CKD care shouldbe aligned to maximize health benefits.26 Kidney carepolicies should be aligned with broader legislativeframeworks.
USE HEALTH CARE PERSONNEL MOREEFFECTIVELY FOR CKD PREVENTION ANDMANAGEMENT
Nurses, physicians, dialysis technologists, kidneytransplant coordinators, and nephrologists need to beadequately trained and re-trained using new team caremodels and evidence-based skills for managing CKD.If accompanied by health system restructuring, taskshifting to nonphysician health care workers for certainaspects of CKD prevention and management is a

Table 2. Summary of Eight Essential Elements for Improving CKD Care With Examples for Using an Integrated Care Approach
Essential Element Information for DecisionMakers
What Can Be Done Action Examples
Policy HCO Community LRS MRS HRS
Support a paradigmshift
Incidence and prevalence ratesof CKD continue to increaseglobally owing to diabetesand other risk factors CKDmanagement and carerequires a different healthsystem approach involvingextended and regular healthcare contact to minimizeCKD complications or slowprogression Severalmedications are needed forCKD care and thereforeshould be available andaffordable to effectivelymanage the different aspectsof CKD
Provide leadershipand advocacyIntegratepolicies on CKD
Ensure qualitythrough leadershipand incentivesOrganize andequip health careteam
Increase CKD awarenessin the community
Initiate discussion of thisframework with otherdecision makers aboutchanges to CKD care in thehealth system Obtainpopulation CKD data tohighlight the existingproblem Sensitize policymakers and healthauthorities to the growingburden of CKD and theexistence of effectivestrategies for managingthem
Use the media as a forum foreducation and sensitizingthe general public on kidneydisease issues Use readilyavailable powerful andcredible voices to spread themessage about CKD
Encourage the spread of newideas through localdemonstration projects ofinnovative care models andstrategies Use massmarketing strategies topersuade the population tothink differently aboutkidney diseases
Manage thepoliticalenvironment
Policy making and serviceplanning for CKD care mustbe effective from a politicalcontext Planning forintegrated CKD managementshould not be one-sided(from the political class);other constituents such ashealth care leaders, patients,families, communitymembers, and organizationsthat represent kidney diseasepatients should be involvedNeed for information sharingacross groups and forconsensus and politicalcommitment amongstakeholders at each stage
Provide leadershipand advocacy
Ensure qualitythrough leadershipand incentives
Encourage better CKDoutcomes throughleadership and supportIncrease CKDawareness in thecommunity
Educate and inform patients,families, and otherinfluential people about thegrowing burden of CKD andstrategies for managingCKD in the country’scontext Build a dialoguewith key leaders in thegovernment, health careorganizations, andcommunities to betterunderstand their values andinterests Use health careopinion leaders andcommunity leaders toadvocate for change in localcontexts
Identify organizations andassociations that representdiverse interests in kidneycare debate Includestakeholders in policyformulation and serviceplanning Develop politicalleadership and commitmentto reorient health caretoward CKD
Assemble systematic reviewson the costs and effects ofCKD management Conductlocal research to show thecost effectiveness ofinnovative CKD caremodels and strategies
Build an integratedhealth carefavorable forCKDmanagement
Effective health systems forCKD care cannot remainfragmented but requireintegration to ensure thefollowing:(1) Sharedinformation across settingsand providers, and acrosstime (2) Coordinatingfinancing across differentarms of health care (eg,inpatient, outpatient, and
Integrate policiesStrengthenpartnerships toenhance CKDcare
Use informationsystems
Mobilize and coordinateresources for CKD care
Ensure that policies, plans, andfinancing structures forCKD care are up to dateCollect data on theincidence and prevalence ofCKD Develop kidneydisease registries
Upgrade information systemsto increase coordinationacross public and privatehealth care settings,providers, and time Developinformation-sharingstrategies across health careorganizations andcommunities
Link health care settings via acommon informationsystem
CKD
care
inreso
urce
-limite
dse
ttings
267

Table 2 (continued )
Essential Element Information for DecisionMakers
What Can Be Done Action Examples
Policy HCO Community LRS MRS HRS
pharmacy services)(3) Incorporatingcommunity resources (eg,transportation) Improvedcare of CKD, less waste,less inefficiency, and a lessfrustrating experience forpatients as the final outcomeof an integrated CKD careprocess
Align all sectoralpolicies toimprove kidneyhealth
The policies of all governmentsectors (eg, national,provincial, and localgovernment) for CKD careneed to be aligned tomaximize health benefitsKidney care policies shouldbe aligned with broaderlegislative frameworksIntegrate non–health-relatedpolicies that may impactkidney disease risk (eg,education, water andsanitation, infrastructure)
Integrate policiesStrengthenpartnerships toenhance CKDcare
Foster intersectoralcollaboration
Increase awareness ofstructural risk factorsfor kidney disease
Form links with private sectorhealth workers Form linksto nonhealth governmentsectors that have thepotential to influencepopulation health Supportregulation and legislationthat curbs the marketing ofpublic health risks (eg, high-salt diet, tobacco, andalcohol) Implementpopulation-based preventionactivities in collaborationwith other governmentsectors
Develop patient information–sharing strategies acrosshealth care organizationsand communities
Implement a multisectoralprivate/public governingbody that advocates for thepromotion, prevention, andcomprehensivemanagement of chronicconditions
Use health carepersonnel moreeffectively forCKD preventionand management
Nurses, physicians, dialysistechnologists, kidneytransplant coordinators, andnephrologists need to beadequately trained and re-trained using new, team caremodels and evidence-basedskills for managing CKDImportance of stressing taskshifting to nonphysicianhealth care workers incertain instances of CKDmanagement
Integrate policiesStrengthenpartnerships toenhance CKDcare
Organize and equiphealth care teamSupport self-management andpreventionIntegrate CKDcare with othernoncommunicablediseases or chronicinfections
Community engagementand education Engagecommunity healthworkers, traditionalhealers
Promote basic skills trainingfor health care workers whoare involved in treatingpatients with CKD Wherethere are multipurposehealth workers, studypossibilities of reinforcingtheir decision making vialinkage with specialists
Educate health care workersvia workshops and printedmaterials Mandate CMEs onCKD across a range ofhealth care workersInfluence curriculumdevelopment on CKD atundergraduate andpostgraduate medicalschools
Develop a range of health carepersonnel (eg, self-management counselorsand quality-improvementspecialists) to meetchanging CKD needsReallocate trainingresources in favor of arange of health carepersonnel
Center CKD care onthe patient andfamily
Prevention and management ofCKD requires severallifestyle changes (eg,smoking cessation, use oflow-salt diet, reduction ofalcohol ingestion, weightloss, and so forth), hence theneed for patient involvementin this process to achieve
Public education Organize and equiphealth care teamSupport self-management andprevention
Community engagementand education
Provide basic informationabout CKD management topatients and families Includeself-management supportinstruction during healthcare interactions
Develop educational and skill-building workshops forpatients and families on themanagement of CKD Usewritten educationalmaterials to supplementself-management messages
Provide patients and familiesaccess to information andself-management supportoutside the health caresetting via telephone orInternet Use computerizedpatient self-assessment forthe generation of
I.G.Okp
ech
ietal.
268

good outcomes Patients andfamily members need to beelevated as active players inthe process of provision ofeffective care
individualized self-management materials
Support CKDpatients in theircommunities
CKD care should not start andend in the clinic, dialysisunit, or hospital, but oughtto extend into the home andworking environment (eg,enforcement of smoke-freeareas, provision of cleanwater) Patients and familiesneed services and supportfrom other institutions in thecommunities Communitiescan fill gaps in healthservices that are notprovided by organizedhealth care (eg, transportservices for patientstraveling from remotelocations)
Safe environmentsconducive tohealth
Outreach programs Encourage better CKDoutcomes throughleadership and supportIncrease CKDawareness in thecommunity Mobilizeand coordinateresources for CKD careProvidecomplementaryservices
Support and involvecommunity groups andNGOs in providing care forCKD Establish a structurefor information exchange onpolicies and sharing ofstrategies between healthcare organizations andcommunity-based servicesSupport the roles ofcommunity organizations inpolicy making and serviceplanning
Develop patient information-sharing strategies acrosshealth care organizationsand communities
Ensure employers areinformed about CKDmanagement and take stepsto support prevention andself-management efforts inthe workplace
Emphasize CKDprevention (ie,screening andearly detectionprograms)
CKD can be prevented or itsprogression slowed byadequate control of knownrisk factors such as diabetesand hypertensionComplications of CKD andits risk factors can beminimized through adequateand appropriate initiation oftreatment Early detectionprograms should formcomponents of CKD care
Integrate policiesStrengthenpartnerships toenhance CKDcare Supportlegislativeframework thatcovers CKDcare
Organize and equiphealth care teamSupport self-management andprevention Useinformationsystems
Provide complementaryservices
Ensure that prevention of CKDis addressed in primaryhealth care visits Providehealth workers withinformation and basic skillsto help patients minimizerisks associated with CKDSupport regulation andlegislation that curbs themarketing of public healthrisks Support population-based CKD preventionactivities
Monitor risk factors andidentify persons at risk fordeveloping CKD Assistproviders through educationand tools to put preventionfirst
Ensure that every CKD patientencounter addresses factorsthat can slow progressionAlign provider incentivesso that prevention effortsare rewarded
Abbreviations: CME, continuous medical education; HCO, health care organization; HRS, high-resource setting; LRS, low-resource setting; MRS, medium-resource setting; NGO,non-governmental organization.
CKD
care
inreso
urce
-limite
dse
ttings
269

I.G. Okpechi et al.270
potentially effective and affordable strategy to improveaccess to care. One systematic review foundimproved health outcomes when task shifting wascompared with usual health care, including reductionsin blood pressure, increased uptake of medications, andlower depression scores.55 Task shifting also has beenused effectively in the management of patients withHIV56 and could be leveraged toward the preventionand treatment of CKD, at least within the HIVpopulation in these settings.
CENTER CKD CARE ON THE PATIENT AND FAMILY
Prevention and management of CKD requires severallifestyle changes (eg, smoking cessation, use of low-salt diet, reduction of alcohol ingestion, weight loss),hence the need for patient involvement in this processto achieve good outcomes.57 Patients and familymembers must be involved as active players in theprocess of provision of effective care, for instance,allowing them to make a choice of dialysis modality.58
Shared decision making is an important processbecause it promotes the rights of patients to beinvolved in decision making concerning their health.59
For example, in South Africa, because of dialysisrationing, modality choice often is not discussed withthe patient even when there are open spaces in HD andPD. Discussing modality options with patients raisesthem to a position in which they can participate in theirown management and be better placed to understandthe dynamics and constraints of modality selection.
SUPPORT CKD PATIENTS IN THEIR COMMUNITIES
CKD care should not start and end in the clinic,dialysis unit, or hospital, but ought to extend into thehome and working environments (eg, enforcement ofsmoke-free areas, provision of clean water). Patientsand families need services and support from otherinstitutions in the communities. Communities can fillgaps in health services that are not provided byorganized health care (eg, transport services forpatients traveling from remote locations). A cross-sectional study of patients receiving hemodialysis inthe hospital and in the community in Hong Kong foundthat patients receiving dialysis in the communitysetting had a better health-related quality of life.60
Although the reason for this was not clear, it doessuggest a positive impact and a positive role of thecommunity on patients with CKD.
EMPHASIZE CKD PREVENTION: SCREENING ANDEARLY DETECTION PROGRAMS
CKD can be prevented or its progression slowed byadequate control of known risk factors. Complications
of CKD and its risk factors can be minimized throughadequate and appropriate initiation of treatment. Earlydetection programs are important components of CKDcare, especially in LMICs where ESKD treatment isnot accessible. Few countries have screening pro-grams,53 and although there are no randomized con-trolled studies, some data suggest that early CKDidentification and initiation of treatment for risk factorscan slow progression and improve patient out-comes.61,62 CKD awareness is low and the preventionof CKD can occur through improving awareness; amedical screening program in Taiwan reported that lessthan 4% of patients with CKD (ie, 12% of the surveyedpopulation) were aware of their condition.63 Aware-ness of CKD risk factors such as diabetes and hyper-tension also have been reported by several studies to below.64–67
CONCLUSIONS
Integrated care for chronic diseases is a challenge formost LMICs. Application of the ICCC framework,however, may be adapted to the needs in the popula-tion and can have a positive impact on CKD care andmanagement including early disease detection and useof a variety of health care workers to maximallyimprove outcomes. It is possible for countries withestablished and functioning programs dedicated to thetreatment and control of communicable diseases toleverage existing infrastructure to integrating kidneydisease screening and care in their population. ForCKD in particular, a focus on prevention should be akey strategy in many countries where care for laterstages of CKD is prohibitively expensive, and effortsto establish screening and monitoring programs forearly detection of CKD as well as risk factors shouldbe prioritized.
REFERENCES1. Levey AS, Atkins R, Coresh J, et al. Chronic kidney disease as
a global public health problem: approaches and initiatives - aposition statement from Kidney Disease Improving GlobalOutcomes. Kidney Int. 2007;72:247-59.
2. Perico N, Remuzzi G. Chronic kidney disease: a research andpublic health priority. Nephrol Dial Transplant. 2012;27 (Suppl3):iii19-26.
3. U.S. Renal Data System. 2014 annual data report: an overviewof the epidemiology of kidney disease in the United States.Bethesda, MD: National Institutes of Health, National Instituteof Diabetes and Digestive and Kidney Diseases, 2014.
4. Mayosi BM, Lawn JE, van Niekerk A, et al. Health in SouthAfrica: changes and challenges since 2009. Lancet.2012;380:2029-43.
5. Liyanage T, Ninomiya T, Jha V, et al. Worldwide access totreatment for end-stage kidney disease: a systematic review.Lancet. 2015;385:1975-82.
6. Kerr M, Bray B, Medcalf J, O'Donoghue DJ, Matthews B.Estimating the financial cost of chronic kidney disease to the

CKD care in resource-limited settings 271
NHS in England. Nephrol Dial Transplant. 2012;27 (Suppl 3):iii73-iii80.
7. Stevens PE, O'Donoghue DJ. The UK model for systemredesign and chronic kidney disease services. Semin Nephrol.2009;29:475-82.
8. Levey AS, Schoolwerth AC, Burrows NR, Williams DE, StithKR, McClellan W. Comprehensive public health strategies forpreventing the development, progression, and complications ofCKD: report of an expert panel convened by the Centers forDisease Control and Prevention. Am J Kidney Dis.2009;53:522-35.
9. WHO. Global status report on non-communicable diseases2010. Description of the global burden of NCDs, their riskfactors and determinants. Available from: http://www.who.int/nmh/publications/ncd_report2010/en/. Accessed 05.09.16.
10. WHO. Innovative care for chronic conditions: building blocksfor action. Global report. Geneva: WHO/NMC/CCH, 2002.Available from: http://www.who.int/chp/knowledge/publications/icccreport/en/. Accessed 05.09.16.
11. Wagner EH, Austin BT, Von Korff M. Organizing care forpatients with chronic illness. Milbank Q. 1996;74:511-44.
12. Epping-Jordan JE, Pruitt SD, Bengoa R, Wagner EH. Improv-ing the quality of health care for chronic conditions. Qual SafHealth Care. 2004;13:299-305.
13. Epping-Jordan JE. Integrated approaches to prevention andcontrol of chronic conditions. Kidney Int Suppl. 2005;98:S86-S88.
14. Almaguer M, Herrera R, Alfonso J, Magrans C, Manalich R,Martinez A. Primary health care strategies for the prevention ofend-stage renal disease in Cuba. Kidney Int Suppl. 2005;97:S4-S10.
15. Katz IJ, Gerntholtz T, Naicker S. Africa and nephrology: theforgotten continent. Nephron Clin Pract. 2011;117:c320-7.
16. Sharif MU, Elsayed ME, Stack AG. The global nephrologyworkforce: emerging threats and potential solutions! ClinKidney J. 2016;9:11-22.
17. Eastwood JB, Conroy RE, Naicker S, West PA, Tutt RC,Plange-Rhule J. Loss of health professionals from sub-SaharanAfrica: the pivotal role of the UK. Lancet. 2005;365:1893-900.
18. Isla RAT, Mapiye D, Swanepoel CR, Rozumyk N, Hubahib JE,Okpechi IG. Continuous ambulatory peritoneal dialysis inLimpopo Province, South Africa: predictors of patient andtechnique survival. Perit Dial Int. 2014;34:518-25.
19. WHO. Global health workforce statistics 2014 update. Avail-able from: http://www.who.int/hrh/statistics/hwfstats/en/.Accessed 05.09.16.
20. WHO. World health statistics 2015. Available from: http://www.who.int/gho/publications/world_health_statistics/2015/en/.Accessed 05.09.16.
21. Callaghan M, Ford N, Schneider H. A systematic review oftask-shifting for HIV treatment and care in Africa. Hum ResourHealth. 2010;8:8.
22. Emdin CA, Chong NJ, Millson PE. Non-physician clinicianprovided HIV treatment results in equivalent outcomes asphysician-provided care: a meta-analysis. J Int AIDS Soc.2013;16:18445.
23. Wouters E, Van Damme W, van Rensburg D, Masquillier C,Meulemans H. Impact of community-based support services onantiretroviral treatment programme delivery and outcomes inresource-limited countries: a synthetic review. BMC HealthServ Res. 2012;12:194.
24. Ortiz A. Translational nephrology: what translational researchis and a bird's-eye view on translational research in nephrology.Clin Kidney J. 2015;8:14-22.
25. Swanepoel CR, Wearne N, Okpechi IG. Nephrology in Africa—not yet uhuru. Nat Rev Nephrol. 2013;9:610-22.
26. Bamgboye EL. The challenges of ESRD care in developingeconomies: sub-Saharan African opportunities for significantimprovement. Clin Nephrol. 2016;86 (Suppl):18-22.
27. Okpechi IG, Rayner BL, Swanepoel CR. Peritoneal dialysis inCape Town, South Africa. Perit Dial Int. 2012;32:254-60.
28. Department of Health South Africa. National consolidatedguidelines for the prevention of mother-to-child transmissionof HIV (PMTCT) and the management of HIV in children,adolescents and adults. 2015. http://www.health.gov.za/index.php/2014-03-17-09-09-38/policies-and-guidelines/category/230-2015p. (Accessed 05.09.16).
29. Gupta SK, Eustace JA, Winston JA, et al. Guidelines for themanagement of chronic kidney disease in HIV-infectedpatients: recommendations of the HIV Medicine Associationof the Infectious Diseases Society of America. Clin Infect Dis.2005;40:1559-85.
30. De Waal R, Cohen K, Fox MP, et al. Clinician compliance withlaboratory monitoring and prescribing guidelines in HIV-1-infected patients receiving tenofovir. S Afr Med J. 2016;106:52-3.
31. McCoy D, Chand S, Sridhar D. Global health funding: howmuch, where it comes from and where it goes. Health PolicyPlan. 2009;24:407-17.
32. Jingi AM, Noubiap JJ, Ewane Onana A, et al. Access todiagnostic tests and essential medicines for cardiovasculardiseases and diabetes care: cost, availability and affordabilityin the West Region of Cameroon. PLoS One. 2014;9:e111812.
33. Okunola Y, Ayodele O, Akinwusi P, Gbadegesin B, OluyomboR. Haemodialysis practice in a resource-limited setting in thetropics. Ghana Med J. 2013;47:4-9.
34. Okpechi IG, Swanepoel CR, Venter F. Access to medicationsand conducting clinical trials in LMICs. Nat Rev Nephrol.2015;11:189-94.
35. Manns B, Hemmelgarn B, Tonelli M, et al. Population basedscreening for chronic kidney disease: cost effectiveness study.BMJ. 2010;341:c5869.
36. Benghanem Gharbi M, Elseviers M, Zamd M, et al. Chronickidney disease, hypertension, diabetes, and obesity in the adultpopulation of Morocco: how to avoid "over"- and "under"-diagnosis of CKD. Kidney Int. 2016;89:1363-71.
37. Lewis M. Governance and corruption in public health caresystems. Available from: http://www1.worldbank.org/publicsector/anticorrupt/Corruption%20WP_78.pdf. Accessed 05.09.16.
38. Adegboyega K, Abdulkareem S. Corruption in the Nigeria publichealth care delivery system. Sokoto J Soc Sci. 2012;2:98-114.
39. Suter E, Oelke ND, Adair CE, Armitage GD. Ten keyprinciples for successful health systems integration. HealthcQ. 2009;13:16-23.
40. Chopra M, Lawn JE, Sanders D, et al. Achieving the healthmillennium development goals for South Africa: challenges andpriorities. Lancet. 2009;374:1023-31.
41. Szczech LA, Gupta SK, Habash R, et al. The clinicalepidemiology and course of the spectrum of renal diseasesassociated with HIV infection. Kidney Int. 2004;66:1145-52.
42. Winston J, Deray G, Hawkins T, Szczech L, Wyatt C, YoungB. Kidney disease in patients with HIV infection and AIDS.Clin Infect Dis. 2008;47:1449-57.
43. Arogundade FA, Hassan MO, Omotoso BA, et al. Spectrum ofkidney diseases in Africa: malaria, schistosomiasis, sickle celldisease, and toxins. Clin Nephrol. 2016;86 (Suppl):53-60.
44. Wearne N, Okpechi IG. HIV-associated renal disease - anoverview. Clin Nephrol. 2016;86 (Suppl):41-7.
45. Barsoum RS. Burden of end-stage kidney disease: NorthAfrica. Clin Nephrol. 2016;86 (Suppl):14-7.
46. Oni T, Youngblood E, Boulle A, McGrath N, Wilkinson RJ,Levitt NS. Patterns of HIV, TB, and non-communicable disease

I.G. Okpechi et al.272
multi-morbidity in peri-urban South Africa- a cross sectionalstudy. BMC Infect Dis. 2015;15:20.
47. Oni T, McGrath N, BeLue R, et al. Chronic diseases and multi-morbidity–a conceptual modification to the WHO ICCC modelfor countries in health transition. BMC Public Health.2014;14:575.
48. Oni T, Unwin N. Why the communicable/non-communicabledisease dichotomy is problematic for public health controlstrategies: implications of multimorbidity for health systemsin an era of health transition. Int Health. 2015;7:390-9.
49. Lanzeta I, Mar J, Arrospide A. Cost-utility analysis of anintegrated care model for multimorbid patients based on aclinical trial. Gac Sanit. 2016;30:352-8.
50. Prinja S, Bahuguna P, Mohan P, et al. Cost effectiveness ofimplementing integrated management of neonatal and child-hood illnesses program in District Faridabad, India. PLoS One.2016;11:e0145043.
51. Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease:global dimension and perspectives. Lancet. 2013;382:260-72.
52. Fenton A, Sayar Z, Dodds A, Dasgupta I. Multidisciplinarycare improves outcome of patients with stage 5 chronic kidneydisease. Nephron Clin Pract. 2010;115:c283-8.
53. Barsoum RS, Khalil SS, Arogundade FA. Fifty years of dialysisin Africa: challenges and progress. Am J Kidney Dis.2015;65:502-12.
54. Johnson DW, Jones GR, Mathew TH, et al. Chronic kidneydisease and automatic reporting of estimated glomerular filtra-tion rate: new developments and revised recommendations.Med J Aust. 2012;197:224-5.
55. Joshi R, Alim M, Kengne AP, et al. Task shifting for non-communicable disease management in low and middle incomecountries–a systematic review. PLoS One. 2014;9:e103754.
56. Rustagi AS, Manjate RM, Gloyd S, et al. Perspectives of keystakeholders regarding task shifting of care for HIV patients inMozambique: a qualitative interview-based study with Ministryof Health leaders, clinicians, and donors. Hum Resour Health.2015;13:18.
57. Galbraith L, Hemmelgarn B, Manns B, et al. The associationbetween individual counselling and health behaviour change:the See Kidney Disease (SeeKD) targeted screening programme
for chronic kidney disease. Can J Kidney Health Dis.2016;3:35.
58. Walker RC, Howard K, Morton RL, Palmer SC, Marshall MR,Tong A. Patient and caregiver values, beliefs and experienceswhen considering home dialysis as a treatment option: a semi-structured interview study. Nephrol Dial Transplant. 2016;31:133-41.
59. Legare F, Stacey D, Turcotte S, et al. Interventions forimproving the adoption of shared decision making by health-care professionals. Cochrane Database Syst Rev. 2014;9:CD006732.
60. Wan EY, Chen JY, Choi EP, et al. Patterns of health-relatedquality of life and associated factors in Chinese patientsundergoing haemodialysis. Health Qual Life Outcomes.2015;13:108.
61. Katz IJ, Gerntholtz TE, van Deventer M, Schneider H, NaickerS. Is there a need for early detection programs for chronickidney disease? Clin Nephrol. 2010;74 (Suppl 1):S113-8.
62. Komenda P, Ferguson TW, Macdonald K, et al. Cost-effectiveness of primary screening for CKD: a systematicreview. Am J Kidney Dis. 2014;63:789-97.
63. Wen CP, Cheng TY, Tsai MK, et al. All-cause mortalityattributable to chronic kidney disease: a prospective cohortstudy based on 462 293 adults in Taiwan. Lancet. 2008;371:2173-82.
64. Lau SL, Debarm R, Thomas N, et al. Healthcare planning innorth-east India: a survey on diabetes awareness, risk factorsand health attitudes in a rural community. J Assoc Phys India.2009;57:305-9.
65. Liu X, Li Y, Li L, et al. Prevalence, awareness, treatment,control of type 2 diabetes mellitus and risk factors in Chineserural population: the RuralDiab study. Sci Rep. 2016;6:31426.
66. Dzudie A, Kengne AP, Muna WF, et al. Prevalence, awareness,treatment and control of hypertension in a self-selected sub-Saharan African urban population: a cross-sectional study. BMJOpen. 2012;2:4.
67. Wang J, Zhang L, Wang F, Liu L, Wang H. Prevalence,awareness, treatment, and control of hypertension in China:results from a national survey. Am J Hypertens. 2014;27:1355-61.